integration inp 3
TRANSCRIPT

Name: Dave Jay S. Manriquez INP 3 (Integration) Class 201509Case Scenario 1 (Setting: at the health clinic)
Sienna RandallGrade 12 student – around 16 to 17 years old
Diagnosis DehydrationBP is low and below her ideal body weightAnorexia NervosaBinge Eating and Purging
StatisticsHeight – 5’7Weight – 108 pounds
Note: 13 pounds under the desired body weight for height and body buildDieting began in 9th gradeFirst month lost 25 poundsMaintained a daily rigorous exercise program and continues to dietBegun binge eating and purging Claims that food, losing weight and exercising on her mindMotivated to stop binge eating and purging but doesn’t know howFeels helplessOver-achiever academically and in sports, she is shy and doesn’t have many friendsWell behaved and strived for perfection
Medications:Sienna is on NO regular medication
Laboratory Values Results Normal MeaningPotassium 3.2 mEq/L 3.5-5.0 mEq/L Causes: dehydration,
Intervention: potassium rich food
Sodium 146 mEq/L 135-145 mEq/L Causes: dehydration, Intervention: increase fluid intake
Chloride 105 mmol/L 96-106 mmol/L NormalHemoglobin 125 g/L Female: 120-155 g/L NormalPrealbumin 100 mg/L 150-350 mg/L Causes: protein-calorie
malnutritionIntervention: Lower than 110 needs aggressive nutrition therapy as enteral feedings or total parental nutrition

The physician orders Sienna to be given the following medication: Potassium acetate 10 mEq PO qid for 4 days, give 1 dose now
1. Written Research
Knowledge about Anorexia Nervosa - An emotional disorder characterized by an obsessive desire to lose weight by refusing to eat. It is a serious, potentially life-threatening eating disorder.
Signs and symptoms of Anorexia Nervosa: Inadequate food intake leading to a weight that is clearly too low. Intense fear of weight gain, obsession with weight and persistent behavior to prevent weight
gain. Self-esteem overly related to body image. Abnormally slow heart rate and low blood pressure, which mean that the heart muscle is
changing. The risk for heart failure rises as heart rate and blood pressure levels sink lower and lower.
Reduction of bone density (osteoporosis), which results in dry, brittle bones. Muscle loss and weakness. Severe dehydration, which can result in kidney failure. Fainting, fatigue, and overall weakness. Dry hair and skin, hair loss is common. Growth of a downy layer of hair called lanugo all over the body, including the face, in an effort
to keep the body warm. Binge-Eating/Purging Type involves binge eating and/or purging behaviors during the last three
months. Restricting Type does not involve binge eating or purging.
Warning Signs Dramatic weight loss. Preoccupation with weight, food, calories, fat grams, and dieting. Refusal to eat certain foods, progressing to restrictions against whole categories of food (e.g. no
carbohydrates, etc.). Frequent comments about feeling “fat” or overweight despite weight loss. Anxiety about gaining weight or being “fat.” Denial of hunger. Development of food rituals (e.g. eating foods in certain orders, excessive chewing, rearranging
food on a plate). Consistent excuses to avoid mealtimes or situations involving food. Excessive, rigid exercise regimen--despite weather, fatigue, illness, or injury, the need to “burn
off” calories taken in. Withdrawal from usual friends and activities. In general, behaviors and attitudes indicating that weight loss, dieting, and control of food are
becoming primary concerns.
Signs and symptoms of binge eating and purging:Binge eating signs and symptoms:Binging – eating an amount of food that is larger than most people would eat.
Lack of control over eating – Inability to stop eating. Eating until the point of physical discomfort and pain.

Secrecy surrounding eating – Going to the kitchen after everyone else has gone to bed. Going out alone on unexpected food runs. Wanting to eat in privacy.
Eating unusually large amounts of food with no obvious change in weight. Disappearance of food, numerous empty wrappers or food containers in the garbage, or hidden
stashes of junk food. Alternating between overeating and fasting – Rarely eats normal meals. It’s all-or-nothing when
it comes to food.Purging signs and symptoms:Purging – evacuation of food from GI; self-induced vomiting or excessive use of laxatives and diuretics.
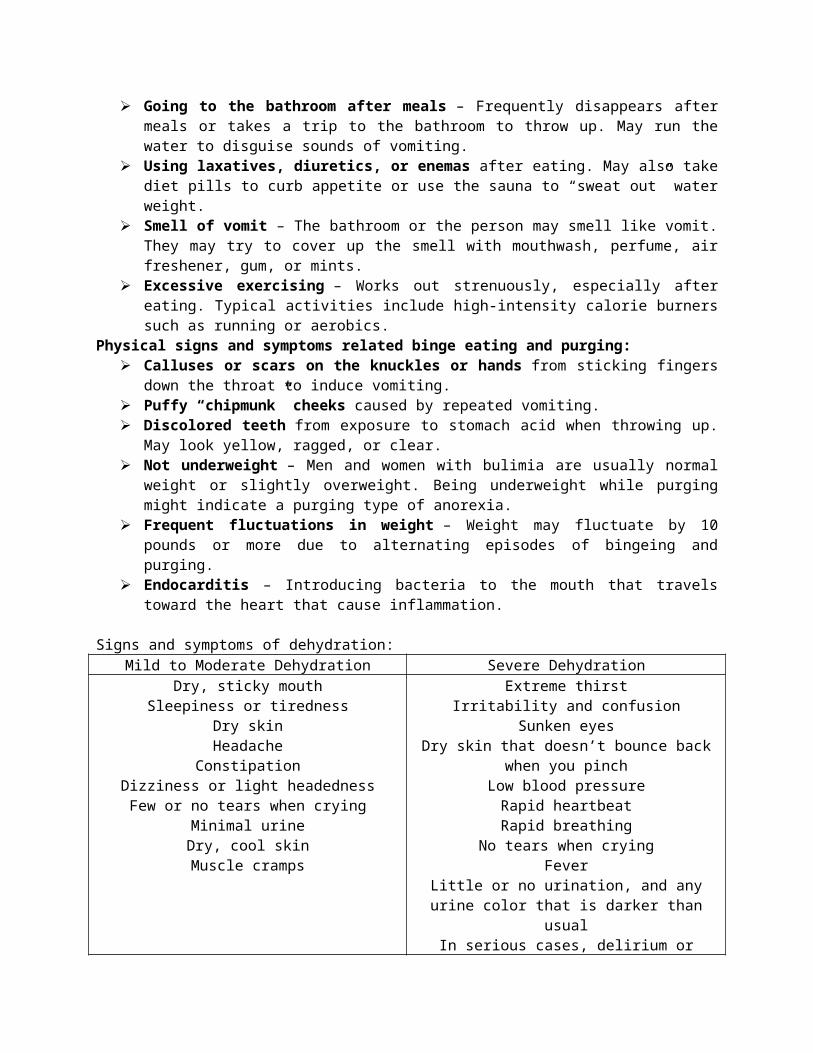
Going to the bathroom after meals – Frequently disappears after meals or takes a trip to the bathroom to throw up. May run the water to disguise sounds of vomiting.
Using laxatives, diuretics, or enemas after eating. May also take diet pills to curb appetite or use the sauna to “sweat out” water weight.
Smell of vomit – The bathroom or the person may smell like vomit. They may try to cover up the smell with mouthwash, perfume, air freshener, gum, or mints.
Excessive exercising – Works out strenuously, especially after eating. Typical activities include high-intensity calorie burners such as running or aerobics.
Physical signs and symptoms related binge eating and purging: Calluses or scars on the knuckles or hands from sticking fingers down the throat to induce
vomiting. Puffy “chipmunk” cheeks caused by repeated vomiting. Discolored teeth from exposure to stomach acid when throwing up. May look yellow, ragged, or
clear. Not underweight – Men and women with bulimia are usually normal weight or slightly
overweight. Being underweight while purging might indicate a purging type of anorexia. Frequent fluctuations in weight – Weight may fluctuate by 10 pounds or more due to
alternating episodes of bingeing and purging. Endocarditis – Introducing bacteria to the mouth that travels toward the heart that cause
inflammation.
Signs and symptoms of dehydration:Mild to Moderate Dehydration Severe Dehydration
Dry, sticky mouthSleepiness or tiredness
Dry skinHeadache
ConstipationDizziness or light headednessFew or no tears when crying
Minimal urineDry, cool skin
Muscle cramps
Extreme thirstIrritability and confusion
Sunken eyesDry skin that doesn’t bounce back when you pinch
Low blood pressureRapid heartbeatRapid breathing
No tears when cryingFever
Little or no urination, and any urine color that is darker than usual
In serious cases, delirium or unconsciousness
Further information I need to know to help understand of Sienna’s diagnoses and health related issues. Underlying causes
Neuroimaging - process of producing images of the structure or activity of the brain or other part of the nervous system by techniques such as magnetic resonance imaging or computerized tomography.
Resources Anxiety level – convulsive disorder? Depression – Quick Depression Assessment Checklist Food preferences: electrolytes, normal growth and development for grade 12 student (starting to
form relationship), culture, amenorrhea.
Associated medical conditions that present as a risk for Sienna. Dehydration Malnutrition Low potassium (Hypokalemia) Constipation, dry skin, dental problems, lethargy, calluses on dorsal hand surface (Russell’s sign),
arrhythmias, cardiac arrest, and death.
Sienna’s strengths Well-behaved, over-achiever, strives for perfection Adolescent- high in resilience , young age Motive to stop binge eating and purging Mother (Support?), friends Intelligence (over-achiever academically)
Treatments and nursing care CBT (Cognitive-behavioral physiotherapy) - revolve around reversal of the restrictive or mal
adaptive patterns of eating and thinking about food, develop healthy eating habit Gradual caloric intake Medication – antidepressants, antianxiety Check – Self-inventory of eating, binging and purging behavior, Depression scale (Beck’s) anxiety
scale Encourage Sienna to verbalize feelings of fear/anxiety r/t achievement, family relationships, intense
need for independence Help the client to achieve realistic view of norms for HT & WT Assist the client in setting practical limits Promote independent decision making as appropriate establish a sense of control Provide ways to reinforce the client’s strengths & attributes Encourage family to participate in education Weigh daily before breakfast Establish rapport/ gain client’s trust Gather information/ data about diet intake and patterns insomnia, fatigue, increased feeling of
anxiety and intolerance to cold temperature, change in bowel elimination and urine output related to laxative or diuretics use.
Asking client how many times she induces vomiting? Use non-confrontational and non-judgmental approach

Use active listening and open-ended questions Head to toe assessment: observe signs of inadequate nutrition, increased hair growth, brittle dry
nails or skin, erosion of tooth enamel
Sienna lab results:Not normal range, identify possible causes and interventions.See notes above…
Meds: Potassium Acetate (Potassium Supplements)Action: Supplements. Treatment/prevention of potassium depletion. Essential to transmission of nerve impulses; contraction of cardiac, skeletal, and smooth muscle.Route: PO; peak 1-2 hoursUsual dose: 40-80 meq/dayAdverse side effects: Arrhythmias, abdominal pain, diarrhea, flatulence, nausea and vomiting Nursing Consideration: Assess for signs and symptoms of hypokalemia such as weakness and fatigue. Monitor pulse, BP, and ECG periodically. Assess for signs and symptoms of toxicity such as slow irregular heartbeat, confusion, and cardiac arrhythmiasClient teaching: Explain the purpose of the medication and the need to take it as directed. Take missed doses as soon as remembered within 2 hour. Do not double dose.
Based on Sienna’s history and diagnoses, what would you assess first? What are your focused assessment? QPA : skin, calluses Abdominal V/S, weight
2. Demonstrate Assessments Demonstrate a QPA1. Introducing myself to client with name and purpose. 2. QPA
General appearance-Looking at her skin, colour weight, body built, hair, nails, lanugo, callus fingers, scared or shy.
Airway Breathing Circulation LOO/LOC In/Out Pain Any Sign of pain? Safety
3. Take note of baseline data: v/s, wt, ht, allergies, medical history Demonstrate focused assessments
1. Vitals 2. Weight 3. If feeling pain, Pain Assessment (PQRST)4. Nutrition Assessment

5. Psychological Assessment : Anxiety scale, Beck’s depression scale6. Head to toe assessment: Dry, brittle, falling hair; Dry skin; Lanugo on the face, upper arms
and shoulder; Dry lips and mouth; Dental problems; Nails are brittle; Low energy; Muscle wasting
7. Abdominal assessment – use of diuretics or laxatives
3. Demonstrate Therapeutic Communication Skillsa. Therapeutic nursing approach with Sienna.
How often do you induce vomiting after eating? How do you feel after binge eating? What makes you feel that way? Is there anybody in your
family has the same condition? Tell me how you feel about your body? How do you feel after eating? What happens after you eat?
b. Therapeutic questions for both Sienna and her mother, questions that help gather assessment data.For Sienna: Mention to her that everything that is discuss is confidential and can be shared only to the member of the health care team that will care for her.
How often do you eat in a day? What food you usually eat? How much do you eat? (Let her describe) small or big portion? How much fluid do you drink in a day? How is your appetite? What activities you are doing to make you feel good? How do you cope up with stress in your life?
For Sienna’s Mother: What do you know about you daughter eating habit? What do you observe about your daughter behavior?
c. Demonstrate asking these questions.
4. Administer Medication: Potassium Acetate POSee notes above… Medication Administration Checklists p. 6 (Oral Med Administration)
5. Demonstrate Client Teaching Inform to divide food to small frequent meals.
a. Signs and symptoms of dehydration and the importance of being hydrated.Sign and symptoms of dehydration see above…Importance of being hydrated
The body depends on water to survive. Every cell, tissue, and organ in the body needs water to work correctly. For example, the body uses water to maintain its temperature, remove waste, and lubricate joints. Water is needed for good health.
b. Manifestations of binge eating and purging.See notes above…c. How to manage keeping an ideal weight relative to height and body size. BMI < 18.5 : underweight range 18.5 =< BMI < 24.9 : normal or healthy weight range
25.0 =< BMI <29.9 : overweight range BMI => 30.0 : obese range
Metric BMI Formula
BMI = Mass (Kilograms)__ (Height (Meters))2
Imperial BMI Formula
BMI = Mass (pounds)____ x 703 (Height (Inches))2
Sienna BMI = 108 LBS______ x 703 = 16.91 or 17, Sienna is underweight. She need to eat and inc fluid. 5’7 (67 inches)2To be in normal weight, she needs to be: 118 lbs to 159 lbs for a 5’7 height.
PLAN OF CAREUrgent and Important Not Urgent but Important
QPAVital Signs – included current WT and HT
Assess hydration status – Skin AssessmentAssess abnormal lab valuesSuicidal thought/depressionMedical Administration – PO
PsychosocialMenstruation
Bowel PatternsBinge/purging behavior
NutritionIdentify knowledge
Willingness/perception to change
References:Lewis; Moodle Slides/ Classroom Notes; Handouts; Leifer; Womble; Davis Drug GuideInternet Sources:http://www.mayoclinic.org/diseases-conditions/anorexia/home/ovc-20179508http://www.helpguide.org/articles/eating-disorders/bulimia-nervosa.htmhttp://www.mayoclinic.org/diseases-conditions/dehydration/basics/symptoms/con-20030056
Name: Dave Jay S. Manriquez INP 3 (Integration) Class 201509Case Scenario 2 (Setting: Home Visit)
Rachel Rogers17 years old
Diagnosis (Baby)Born prematurelyFebrile Seizure - scared Rachel a lot. Feels helpless and unsure of what to do to help her baby.
Note:Complication of Postpartum Hemorrhage – experienced a large blood volume loss and her Hgb is 115 gm/L. Normal: Female: 120-155 g/LDelivered a preterm female infant at 32 weeks gestation on Feb. 2, 2016 via SVDContinued to smoke periodically throughout pregnancyHas an unplanned pregnancyHas been drinking alcohol but had stopped when her pregnancy was confirmedLives with her parentsStruggle in graduating from high schoolConcerned that her baby not meeting her milestonesExperience difficulty in breastfeeding and frustrated
LPN role: Work for community based nursing company, has been assigned to visit Rachel and her baby who is four months old now. Assist any challenges that she may be facing. Complete an assessment on Rachel and her baby by identifying priorities of care and provide appropriate health teaching.
1. Written Research
Rachel risk factors in being a 17 year old mother?1.) Nutritional intake:
Inadequate nutrition as adolescent about their body image so they don’t eat enough to maintain body weight.
Adolescent diet to control weight She may be affected by media definition of a beautiful body Poor nutrition can lead to birth deficit, gestational HTN, low birth weight and prematurity Dietary contains “empty calories” consists of fad diets
2.) Sexual Activity: Multiple partners/unprotected sex STI,s STI,s increase risk to fetus and new born
3.) Age at which pregnancy occurs: Young adolescents have immature vascular development in the uterus It can lead to gestational HTN and fetal perfusion problems that results in prematurity and low
birth weight

Pelvis does not reach adult size and diminishes 3 years after the start of menstruation Small pelvis can cause problem during delivery and labour Long bone growth is incomplete Poor pregnancy outcome such as prematurity and low birth weight
4.) Limited access to health care services: Adolescents may fear revealing pregnancy to parents and other people which can cause result in
problems for mother and fetus Delayed prenatal care that results to problems for mother and fetus Limit access to health care
5.) History of smoke: History of smoke and alcohol can lead to complication during the pregnancy Some fetal complication e.g. fetal alcohol syndrome Lack of experience how to handle baby
6.) Knowledge deficit/self/support Doesn't know anything knowledge deficit Self-esteem problems/peer pressure Financial support/resources Emotional support lack of support
Questions to ask Rachel about her support system? At home, who usually help you taking care of your baby? Is the father of the child involve in the care or any sort of support? Are your parents happy to see your baby? How’s your relationship with the father of the baby? How is your relationship with your parents? Do you have any siblings? Who else lives with you at
home? While you’re in school, who’s going to look after your child? Have you had contact with the social worker yet? Have you reach out to a support group?
Assessments and nursing interventions required to appropriately assess Rachel’s health.Assessments:
Resources/financial support? Nutritional status - kind of foods she eats, (carbo, proteins, fruits, veggies including any
supplements). Educating her about healthy food choices, especially iron as she had large amount of blood loss, as well as for breastfeeding.
Sleeping patterns (rest or have a nap when the baby is sleeping). Adequate rest period (fatigue/tiredness related to post-partum depressive symptoms and breastfeeding).
How she breastfeed her baby or mixed feeding; sore in the breast, engorgement Emotional -exploring her feelings towards a new role; (have someone to talk to, ask help is
needed) Coping skills- her attitude and insights about being a new mom and her strengths Plans for graduating high school

Interventions: Encourage the adolescents to develop positive self-image and feelings of self-worth to help
them adopt the coping skills with the changes after the delivery. Educate the client about seriousness of substance abuse. Educate the client about the effects of substances use on the baby e.g. the children with
substance abuse parents are at high risk of abuse, they are confused, may feel isolated and embarrassed, aggressive, child may try to gain love by never causing any trouble. They may have delayed developmental and growth milestones. They may suffer from some mental illness also. Attention deficit/hyper activity disorder.
Tell her about how to breast feed and different positions of breast feeding. Demonstrated how to bath the newborn and care of the new born baby. Tell her about the care of the episiotomy and about the maintenance of the personal hygiene. Connect her with the support services. Give information about the growth and developmental milestones of the baby and not all the
babies have those milestones at the same time. Provide privacy and ensure confidentiality and respect are basic to adolescent communication. Be careful while communicating with adolescent because they may perceive your behaviour as
phoney. Give her teaching about: nutrition, dental care, personal care, accident prevention like falls in
baby, positioning of the baby. Do not lay the baby on side or on tummy until the tummy time starts. The baby may have sudden infant death syndrome. Do not put so many clothes on the baby, and do not cover with heavy blanket. Do not put toys in the crib. Tell her how to manage time as she also needs rest. Encourage her to ask questions and express her feelings. Give her instructions how to care a baby with seizures. Tell her about the maintenance of temperature.
Further information I need to know to help understand of Rachel’s health related issues. How many packs she smokes before? How much alcohol can she consume before? About breastfeeding problem - proper positioning and holding the baby. Her coping and psychological status.
Associated medical conditions that present as a risk for Rachel’s baby. Premature baby, lungs are not developed, may have respiratory problem and prone to infection. Premature babies lack fat and immature thermoregulation, so may have low body temperature Lack of reflexes for sucking and swallowing, so may lead to feeding difficulty FAS- due to mother’s history of alcohol and smoke Premature babies have immature gastrointestinal systems. The potentially serious conditions, in
which the cell lining the bowel wall are injured, can occur in pre-mature babies after they start feeding.
Blood problem- They are at risk of anemia and infant jaundice. All new born experience a slow drop in RBC count during the first month of life, the decrease may be more in premature baby.
Metabolic problem. Premature babies may develop on abnormally low level of blood sugar (hypoglycemia) because they have smaller stores of glycogen and their liver have trouble converting stored glycogen into glucose.

Immune system problem: Undeveloped immune system common in premature babies, can lead to infection. Infection in premature baby can quickly spread to blood stream causing sepsis, a life threatening condition.
Cerebral palsy: It is a disorder of movement, muscle tone and posture that can be caused by infection, inadequate blood flow or injury to premature baby’s developing brain either during pregnancy or while the baby is still young and mature
Impaired cognitive skills: Premature babies are more likely to log behind their developmental milestones.
Behaviour and physical problems- they can have ADHD (attention deficit hyperactivity disorder. Having a febrile seizure. Low birth weight. Delayed brain development. Fetal Alcohol Syndrome Sudden Infant Death Syndrome
Corrected gestational age for the baby?(40 – 32 weeks = 8 weeks or 2 months)Baby is 4 months old now – 2 months = 2 months Gestational corrected age.
Milestones the baby be meeting.Physical DevelopmentPosterior fontanelle closes tears appear. Can hold head in erect in mid position. Follows moving light with eyes. Holds a rattle briefly. Legs are active Sleep. Develops own pattern, may sleep from feeding to feedingDiet: Breast milk or formulaExercise: Provide a safe, flat place to kick and be active. Do not leave infant alone, particularly on any raised surface. Physical examination by the family doctor or pediatrician.Immunization: First diphtheria, tetanus and whooping cough (DTaP), injectable polio vaccine (IPV) , Haemophilus influenza type b (Hib) and second hepatitis B virus (HBV) vaccine. Still completely depends on adult for physical care. Needs a flexible routine throughout infancy and childhood.Pacifier: If used, select for safety, choose one – piece construction and loop handle to prevent aspiration.Hiccups: are normal and subside with treatment. Small amounts of water may help.Colic: Consists of paroxysmal abdominal pain, irritable, crying. Usually disappears after 3 months. Place infant prone over arms
15-16 hrs of sleep/day can see people from up to 18 inches follow movements when walk close by enjoys listening to the sound of moms voice presence of reflexes on 0-2mons old Effective feeding patterns Predictable Sleep-wake patterns Reflexes: Moro reflex (startle reflex) birth to 3 – 6 months.
Tonic neck reflex birth to 5 – 7 months. Palmar grasp – birth to 4 months Babinski reflex / Plantar – birth until before infant begins walking.
Responses to sound: blinking and turning response – birth
Food reflexes: rooting response – birth to 3 – 4 months Sucking response – birth to 7 – 12 months
Locomotion: Chin up (1), Chest up and elevates self with arms (2), rolls over at will (4). Perception: (1) able to focus on sharply contrasted objects, (2) Selectively responds to patterns,
colors, (3) imitates expressions, prefers to look at familiar sight. (4) Perceives differences in facial expressions.
Pseudo menstruation (girl) - withdrawal of hormone
Interview question that help gather assessment data from Rachel and her baby. Did you use any contraceptive methods in the past? How many partners? Were there any
violence or did you experience abuse? When did you start smoking and stopped smoking during pregnancy? When exactly was the time you stopped drinking alcohol? When was the time you realized you had to go to the clinic to get checked for pregnancy? Were
you able to come to your prenatal check-ups from first to third trimester? Are you breast-feeding or bottle-feeding? (Use one to prevent nipple confusion) What’s the position as you breast-feed your child? Are you experiencing any pain on your
breast? You experienced heavy bleeding after the delivery of the child, are you still having bleeding up
to this day? Do you have wound or an episiotomy? Are you experiencing any pain? (In your abdominal area or your perineum?) How many pads per day? What color is it? Is there any odor to it?
You mentioned that you’re concerned about the child not meeting her milestones. Could you give me an example? (Or what is your baseline?)
How are the infant’s sleep patterns? Would you say he is irritable or restless during the day? Difficulty with breast-feeding: Did you notice any significant weight changes to the baby? What
are the baby’s birth and his weight now? Are you expressing enough milk for the infant’s feeds? Is she able to take in any feeds? Is the child vomiting? How many times in a day? What’s the
amount? What type of stool is it (hard or constipation or soft or watery). What are the color and the
amount of stool? How many diaper pads each day? Febrile Seizure: Was the baby feverish? Which part of the body was seizing? Were you able to
take note for how long the seizure episode was? Could you describe what did you do when your infant was having a seizure? Was he breathing after the seizure?
Client teaching appropriate for Rachel and her baby.Febrile Seizure teaching:
If your child has a febrile seizure, stay calm and:• Make sure your child is on a safe surface, such as the floor, and cannot fall down or hit
something hard.• Lay your child on his or her side to prevent choking. This is especially important if your
child has a lot of saliva coming out of the mouth.• Watch for breathing problems, including any color change in your child's face.• If the seizure lasts more than 5 minutes, or your child turns blue, it may be a more
serious type of seizure — call 911 right away. It's also important to know what you should not do during a febrile seizure:
• Do not try to hold or restrain your child.
• Do not put anything in your child's mouth.• Do not try to give your child fever-reducing medicine.• Do not try to put your child into cool or lukewarm water to cool off.
Proper Breastfeeding techniques Correct the baby’s latch so that the baby can obtain as efficiently as possible the milk that the
mother has available. Correcting the latch may be all that is necessary to change a situation of “not enough milk” to one of “plenty of milk”.
Use breast compression to increase the intake of milk. Use milk expression after feedings to increase the supply. Correct sucking problems by stopping the use of artificial nipples (Using a Lactation Aid,
and Finger Feeding) and other stratagems.
For Rachel: Visit the pediatrician in dealing with the baby’s milestones. Take note of any signs of bleeding including amount or discharge; bruising. Check labs because
hemoglobin is low. Eat legumes and green leafy vegetables essential for iron. Drink Vitamin C or oranges for better absorption of iron-enriched foods.
What information can you assess in regards to the seizure activity Rachel’s baby exhibited? What assessments and health teaching can you provide?Febrile Seizure:
A febrile seizure can be very frightening for any parent or caregiver. Does not cause any harm and the child usually does not have a more serious long-term health
problem. Most febrile seizures occur in the first 24 hours of an illness, and may not occur when the fever
is highest. Ear infections, a cold or viral illness may trigger a febrile seizure. A febrile seizure may be as mild as the child's eyes rolling or limbs stiffening. A simple febrile seizure stops by itself within a few seconds to 10 minutes. It is often followed by a brief period of drowsiness or confusion.
Assessments: Ask Rachel, How often and how long was it? Was only part of the body shaking or was the entire
body shaking? Temperature greater than 102.2 F (39C). If seizure lasts greater than 5 minutes. Call for help, emergency. Look for signs and symptoms of shock like dry mucous membranes, pale and clammy skin,
tachycardia, tachypnea and abnormal mental status. Assess for neurological problem may have either led to the fever or been caused by the seizure. Assessing the respiratory system, look and listen for the lower airway congestion and
constriction, as well as upper airway swelling. Focus on ABC support, which may include airway positioning, suctioning secretions, vomit and
applying oxygen. Skin assessment like bruising or injuries. S/S: tonic and clonic movement, vomit, eye roll back, body shake, soil or wet themselves.
Treatment: usually stop on its own; side lying to prevent choking then can use bulb syringe to suction.
Febrile seizure teachings: See notes above…
Rachel Baby:Weight – 7.2 kgLength – 64 cmHead Circumference – 39 cmNot gained weight in the past 2 monthsWhere does the baby fall on the Growth Chart for her Corrected Gestational Age?Head Circumference – 85th percentileLength and weight – 95th percentile
Identify three major risks to her health that you can address? Anemia Low self esteem Depression
Due to young age and first birth, she may find it difficult to adopt with the changes. Trying to complete high school Due to delayed milestones of the baby Febrile seizure
Alcohol
Meds: Domperidone acetate, Motilium (gastric stimulant)Action: Improved GI motility, Nausea/Vomiting associated with dopamine agonist, stimulate lactation as it increases prolactin levels.Route: PO; peak 30 minsUsual Dose: 10 mgAdverse side effects: Headache, insomnia, dry mouthNursing Consideration: Monitor for symptoms related to hyperprolactinemia (menstrual abnormalities, galactorrhea, and sexual dysfunction). Monitor serum prolactin prior to therapy.Client teaching: Advise patient to notify health care professional if galactorrhea, menstrual irregularities, palpitations, irregular heartbeat, dizziness, or fainting occur.
Based on Rachel’s history and diagnoses, what would you assess first? What are your focused assessment? Rachel:Sign and symptoms of anemia – Extreme fatigue, pale skin, weakness, shortness of breath, chest pain, frequent infections, headache, dizziness or light-headedness.2. Demonstrate Assessments:
Demonstrate QPA for both mother and baby, V/SDemonstrate focused assessments: Rachel: Respiratory assessment, Pain assessment, Peripheral Vascular assessment, Psychosocial assessmentBaby: Pediatric assessment – head to toe, includes: height, weight, head and chest circumference, fontanels, eyes, ears, nose, mouth, milia, Mongolian spot rise and fall of chest, apical pulse, capillary <2 secs in the chest, skin turgor pinch abdomen, startle reflex, rooting/sucking reflex, Babinski reflex, hip sound, cord care, how many times diaper is change per day.
3. Demonstrate Therapeutic Communication Skills
a. Demonstrate a therapeutic nursing approach with Rachel and her baby.See notes above…b. Develop therapeutic questions for Rachel’s mother Allison. What would you ask her, when you enter the home?Rachel:
Is the father of the baby around and supportive? Is your family supportive? How are you coping to this challenges? How many times you feed the baby? Do you feed your baby with formula milk? How do you breastfeed the baby? Can you show me?
Rachel Mother Allison: What support you provide to Rachel and the baby? What do you do for living? What kind of relationships you have with your daughter?
c. Demonstrate asking Allison these questions.
4. Administer Medication: Domperidone Acetate PO 3 tablets TIDSee Medication Administration Checklist for PO Meds p. 6…
5. Demonstrate Client Teaching for Rachel and her babyClient teaching
Immunization Vitamin D Crib safety Seizure precaution Burp frequently, avoid over feeding or underfeeding Fall prevention If fever give antipyretic
Client Teaching for Rachel and her baby Educate Rachel the importance of breastfeeding for her baby. Explain to Rachel the
breastfeeding is most complete source up to 6 months of age. Breast milk contains protein, fats and carbohydrates and Immunoglobulins to resist her baby from infection. Also breastfeeding enhances cognitive development and decreased frequency of respiratory tract illnesses, gastroenteritis, otitis media and food allergies.
Teach Rachel some ways to increase her hemoglobin level like taking iron supplements, increase intake of iron rich foods (eggs, spinach, beans, lean meats and seafood. Food rich in vitamin B12, folic acid and Vitamin C.
Refer Rachel to the physician to discuss the iron supplements. Refer Rachel to Community support services for young mother or first time mother like
breastfeeding, bonding with other mother and their baby. Educating Rachel regarding the effect of smoking and alcohol to her well-being and health as
well as to her baby. Exploring issues such as family supports, potential parenting disorders, depression, coping
mechanisms and possible financial, career or housing problems. Educate Rachel about the seven “S” to calming the infant (Swaddle, Swing / rock“Shhh-Shhh” Sounds, Gentle swats (taps) to the back or bottom, Sugar water (evidence suggests it minimizes
pain), Sing, Soother (pacifier) / suck. Inform about PURPLE cry and what it is. Inform about immunization, and the next schedule is 6 months.

Inform to read the book baby best chance. Newborn teaching: baby bath, diaper change, cord care, proper sleep position, using of bulb
syringe, soothing and swaddling.
PLAN OF CAREUrgent and Important Not Urgent but Important
QPANewborn Assessment
Febrile Seizure TeachingsBreastfeeding Teachings
Abnormal Lab Values – low hemoglobinMedical Administration – PO
NutritionSmoking and drinking cessation
Identify KnowledgeWillingness to change
References:Lewis; Moodle Slides/ Classroom Notes; Handouts; Leifer; Womble; Davis Drug GuideInternet Sources:http://www.webmd.com/parenting/baby/baby-development-2-month-old?page=2http://www.cdc.gov/growthcharts/data/set1clinical/cj41l018.pdfhttp://kidshealth.org/en/parents/febrile.htmlhttp://www.webmd.com/a-to-z-guides/understanding-anemia-symptoms

Name: Dave Jay S. Manriquez INP 3 (Integration) Class 201509Case Scenario 3 (Setting: Home Visit)
Anita Sidhu
Note:Gave birth vaginally to an eight pound baby boy 4 days ago and went homeGot last dose of IV antibiotics for an infected episiotomy Started to experience signs and symptoms of postpartum bluesTaking antipsychotic medicationsFeeding her baby boy formula using bottle
History:Diagnose with SchizophreniaMonthly depot injections of Fluphenazine Decanoate 12.5mg IM
LPNMaking home visit to Anita and her newborn baby boyNoticed that Anita has a Saline Lock insertedAccording to MAR and nurse’s notes, Anita received her last dose of IV antibiotic medication.
1. Written Research
Anita Diagnoses and health related issues: A. Infected Episiotomy An episiotomy is an incision made in the perineum — the tissue between the vaginal opening and
the anus — during childbirth As in other incisions, infection is the primary risk in an episiotomy or laceration. An additional risk is extension of the episiotomy with a laceration into or through the rectal
sphincter (3rd or 4th degree), which can cause prolonged perineal discomfort and stress incontinence
Signs and symptoms of infection: REEDA to do assessment of infected episiotomy Possibility of fever and pain Swelling and hardening of the incision Pain with urination Heat at the incision site Assessing the perineum :
o Ask woman to turn on side and flex upper leg, lower perineal pad, and lift up upper buttock; if necessary, use flashlight to inspect perineum.
o Observe for edema, bruising, and hematomao Examine episiotomy or laceration for REEDA
REEDA is redness, edema, ecchymosis, discharge, approximation Redness without excessive tenderness is probably the normal inflammation
associated with healing, but pain with the redness is more likely to indicate infection.
Mild edema is common, but severe edema interferes with healing.

A few small superficial bruises (ecchymosis) are common. Large bruises interfere with normal healing.
No discharge from the perineal suture line should be present Approximation (intactness of the suture line). The suture line should not be
separated. If intact, it is almost impossible to distinguish the laceration or episiotomy from surrounding skin folds.
Warmth around the area, foul odour, fever, Loss of appetite, lethargy, restlessness. Healing will take longer time probably by secondary intention.
Treatments and Nursing Interventions / Client Teaching: Comfort and hygienic measures are the focus of nursing care and patient teaching An ice pack or chemical cold pack is applied for the first 12 to 24 hours to reduce edema and
bruising and to numb the perineal area A disposable rubber glove filled with ice chips and taped shut at the wrist can also be used. The cold
pack should be covered with a paper cover or a washcloth to prevent tissue damage. When the ice melts, the cold pack is left off for 10 minutes before applying another for maximum effect
In some cultures, women believe that heat has healing properties and may resist the use of an ice pack.
After 24 hours, heat in the form of a chemical warm pack, or a sitz bath increases circulation and promotes healing. The sitz bath may circulate either cool or warm water over the perineum to cleanse the area and increase comfort. Sitting in a cool sitz bath and adding ice cubes and remaining in the water for 20 minutes often provides immediate pain relief.
The woman is taught to do perineal care after each voiding or bowel movement to cleanse the area without trauma. A plastic bottle (peribottle) is filled with warm water, and the water is squirted over the perineum in a front-to-back direction. The perineum is blotted dry. Perineal pads (peripads) should be applied and removed in the same front-to-back direction to prevent fecal contamination of the perineum and vagina.
B. Postpartum Blues 50-90% of post-partum affective disorder peak onset: postpartum days 4 and 5 and typically resolves by day 10-14 days Also called the “baby blues” Time of emotional change due to quick drop in hormones after birth
Signs & Symptoms: Mood vacillates between periods of joy and periods of emotional letdown
Happy one minute, sad the next Feelings of fatigue, irritability, cry easily, mood swings, tearfulness, anxiety, hopelessness,
overwhelmed, poor concentration Symptoms generally involve mood lability, tearfulness, and some mild anxiety and depressive
symptoms. This is as a result in drop of hormones after delivery and exhaustion from childbirth. It usually disappears after 7-10 days.
Describe signs and symptoms of postpartum blues? Postpartum blues start after birth to two weeks Women has periods of let down Roller coaster emotions are usually self-limiting Normal after birth and very important to educate the parents Instead of celebrating, you feel like crying.

You were prepared for joy and excitement, not exhaustion, anxiety, and weepiness Moodiness, sadness, difficulty sleeping, irritability, appetite changes, concentration problems.
Risks: Misinterpreting postpartum blues and postpartum depression Postpartum depression starts with in four weeks after delivery
Treatment & Nursing Interventions / Client Teaching: Teaching regarding this phenomenon prior to conception and throughout pregnancy (anticipatory
teaching and planning) Engage partner or other supports, as required. Allow for time to rest and recover without guilt Return to daily activity / exercise and well-balanced diet (blood sugar fluctuations can increase
affective symptoms) Assess for progression to worsening state Explain to her that it is a normal condition which most mothers have after giving birth. Reassurance
is necessary. Support for child. Proper nutrition and staying active. Teaching mother and family that it’s common due to hormonal changes. Hormones level drops
causing these symptoms Support system is important It goes away on its own within two weeks, emotional support is important If symptoms don’t go away, It could be Postpartum depression Contact Doctor
C. Schizophrenia A form of psychosis in which there are disorganized thoughts, perceptual alterations,
inappropriate affect, and decreased emotional response as the links to reality are lost. It is a chronic and disabling mental illness that causes the person to withdraw into a world of
delusional thoughts and misperceptions The word schizophrenia derives from Greek, meaning “split mind” The person’s ability to distinguish real from unreal becomes painfully disordered. Symptoms typically emerge in adolescence or early 30s – usually before psychotic episode Complex biochemical brain disorder affects a person’s ability to determine what reality is and
what is not.
Signs and Symptoms of Schizophrenia:People with schizophrenia are affected by delusions (fixed false beliefs that can be terrifying to the person experiencing them), hallucinations (sensory experiences, such as hearing voices talking about them when there is no one there), social withdrawal and disturbed thinking. Psychosis: a severe mental disorder in which thought and emotions are so impaired that contact is lost with external reality.
Positive Symptoms – evidenced early in the progress of the disorder. Called acute schizophrenia involving alterations in thinking, perception, and behavior.
Delusions (fixed, false ideas or beliefs) Word salad (Jumble of unconnected and disorganized thoughts) Clang associations (Insignificant rhyming of words) Thought broadcasting (Believes that his/her thoughts can be heard by others) Thought insertion (Believes the thoughts of others can be inserted into his/her mind)

Loose associations or derailment (Content is off-track) Neologism (New words made up by the person that have special personal meaning) Hallucinations (false sensory perceptions that have no relation to reality) Illusions (Sensory stimuli actually exist but are misinterpreted by the person) Depersonalization (One’s thoughts and feelings seem unreal or not to belong to oneself, or
in which one loses all sense of identity) Bizarre behavior Agitation Catatonia (decreased reaction to environmental stimuli)
Negative Symptoms – develop slowly over time and are reflected in the person’s inability to deal with the way their illness affects their life. Result in isolation and withdrawal from the uncomfortable inability to interact with others in a meaningful way.
Blunt or flat affect - expressionless Bizarre / inappropriate affect (giggling, smiling, mumbling in odd situations. Referred to
as“autistic”behaviours.) Anergia – low energy/ambition Avolition – decreased motivation for self-care Poor interactive ability - isolation Substance use – alcohol, marijuana, cocaine etc. Depression with suicidal end (10% attempt or commit suicide)
Treatments: • Medication: Haloperidol, Risperidone, And Clozapine Individual family and group psychotherapy, Cognitive behaviour therapy (CBT), Electro-
convulsive Therapy (ECT)
PSYCHOSIS Makes reference to a set of symptoms, including perceptual disturbances, disorganized
thinking, and behavior alterations, that demonstrate disorganization in the mental processes. Symptoms reflect the behavior, emotional response, and thought processes of the person who
has lost contact with realityProdromal Signs & Symptoms (Start of a disease prior to onset of psychosis): Increasing anxiety Inability to concentrate Distraction Distortion of reality Paranoia Delusional thinking Deteriorating relationships
Signs & Symptoms:Perceptual Disturbances Hallucinations
o False sensory perceptions that have no relation to reality and are not supported by actual environmental stimuli
o When a hallucination occurs, the person has the perception of seeing (visual), hearing (auditory), smelling (olfactory), feeling (tactile), or tasting (gustatory), although there is no stimulus present

o Although all of these may occur, auditory hallucinations are the most common (i.e.; voices or sounds heard only by the person experiencing them).
o Inside or outside the person’s head, talking to the person, commenting on his/her behavior.
o Voices are commanding, telling the person to harm himself or others and are very frightening to the person
o Studies show that those who experience the command hallucinations may react in panic or demonstrate violence toward themselves or others.
o Visual hallucinations are less common but may involve seeing people or images that are not actually present. (i.e.; feeling that something is crawling on the skin or moving inside the body parts
Illusions o Experienced when sensory stimuli actually exist but are misinterpreted by the
person (i.e.; person may refer to spots on the floor as insects or to an electric cord as snake)
Disorganized Thinking Thought processes become confused and disrupted, leaving the person with an inability to
carry on a logical conversation. Delusion – consists of fixed, false ideas or beliefs without appropriate external stimuli that
are inconsistent with reality and that cannot be changed by reasoning. Thought usually involve a theme that is dominant in the mind (i.e.; the client who thinks
someone is trying to kill him will demonstrate this both verbally and behaviorally)Behavior Alterations Psychotic behavior may be described as agitated, aggressive, childlike, inappropriate, silly,
and unpredictable Wild, purposeless, agitated movements are described as frenzied motor activity Disorganized behavior can lead to an inability to perform activities of daily living or carry out
goal directed activity. The person may appear very unkempt and dress inappropriately for the situation.
Treatments & Nursing Interventions / Client Teaching: Combined approach:
Medicationso Antipsychotic drugso Symptom managemento No cure
Psychotherapyo Individual, group, family therapy
Case Management Life-long treatment and support Medical Tx: Antipsychotics to manage symptoms such as haloperidol
Patient Anita Meds: Fluphenazine – phenothiazines or neuroleptic, works by affecting the balance of natural chemicals (neurotransmitters) in the brain.
Psychotherapy, support groups, stress management, getting enough sleep, regular exercise and avoiding alcohol and drugs.
Client teaching appropriate for Anita.

If postpartum blues continue for more than 10 days it could lead to depression and if more than 1 month it could lead to psychosis. Consult doctor immediately.
Never stop taking medications for schizophrenia and complete antibiotics. Monitor for signs of systemic infection such as fever, chills, loss of appetite, severe pain. Proper
perineal hygiene (clean from front to back) No strenuous exercise and no lifting of heavy objects. Moderate activity. Good nutrition. Watch
for extreme mood swings and if there are any suicidal thoughts, contact physician immediately.
Further research do I need to help my understanding of Anita’s diagnoses and health related issues? Past Health History Family Health History (find out if there is history of schizophrenia and psychosis in the family) Suicide risk tool, depressions assessment, side effects of antipsychotics (extrapyramidal
symptoms)
Meds: Fluphenazine Decanoate, Apo – Fluphenazine, (antipsychotics/ phenothiazines)Action: Alters the effects of dopamine in the CNS. Diminished signs and symptoms of psychoses. Route: IMUsual Dose: 12.5-25mg, maybe repeated q 3 wks.Adverse side effects: Neuroleptic Malignant Syndrome, extrapyramidal reactions, sedation, tardive dyskinesia.Nursing Consideration: Assess mental status (LOO, LOC, mood, behaviour) before and periodically during therapy. Monitor BP, pulse, RR, ECG. Monitor for onset of akathisia (restlessness or desire to keep moving) and extrapyramidal side effects (parkinsonian - difficulty speaking or swallowing, loss of balance control, pill rolling, mask-like face, shuffling gait, rigidity, tremors; dystonic - muscle spasms, twisting motions, twitching, inability to move eyes, weakness of arms or legs). Monitor for development of neuroleptic malignant syndrome (fever, respiratory distress, tachycardia, seizures, diaphoresis, arrhythmias, hypertension or hypotension, pallor, tiredness, severe muscle stiffness, loss of bladder control.) Report immediately. Client teaching: Report immediate to physician if signs of adverse effects occur.
Sites/ Needle gauge for administrating medication:Site Amount to be injected Gauge Length
Deltoid R and L(ask for dominant hand)
Ventro- Gluteal Vastus Lateralis
1 ml
3 ml3 ml
22-25
22-2522-25
5/8 to 1 inch
5/8 to 1 inch5/8 to 1 inch
Note: deltoid = three fingers below acromion process, then form a triangle Ventro-Gluteal = fingers on iliac crest and anterior superior iliac spine, hand on greater trochanter Vastus Lateralis = Greater trochanter of femur and lateral femoral condyle at the middle
Based on Anita’s history and diagnoses, what would you assess first? What are your focused assessment? Identify the components of the focused assessments?
Focused assessments? Components of focused assessments? QPA Vitals Signs Episiotomy ( REEDA) BUBBLEHE
Psychosocial assessment Saline lock ( DRIPS) Meds administration IM Baby: Head to toe infant assessment ( weight, length, head circumference)
2. Perform Assessments QPA BUBBLE – HE Mental Health Status: Postpartum Blues and Psychosis
QPAa. ABC
i. Vital Signs – RR, BP, Apical pulse, Temperature, O2 Satb. LOC, LOOc. Pain
i. PQRSTd. Input
i. Increase 2000-2500 ml fluid intake/daye. Output
i. Monitor output – lochia, bowel, urine, Focus Assessments
1. Pain Assessment2. BUBBLE-HE3. Mental Health Status: Postpartum Blues & Psychosis
3. Demonstrate Therapeutic Communication Skills Demonstrate a therapeutic nursing approach with Anita.Therapeutic Nursing Approach
Gain the trust of the client Use active listening and open-ended questions to encourage the client to communicate freely
Develop therapeutic questions for Anita.Therapeutic Questions for Anita
How are you feeling? How do you feel right now about your life? How is your mood? How are you feeling about yourself? How do you see yourself? Are you taking your medications consistently? What are the things you do to take care of yourself? How are the things you used to enjoy at the moment? How is your energy level? How is your appetite like? How is your sleeping pattern? How is your husband? How is your relationship with the baby now? How about your husband? Do you have any other support network?
Demonstrate asking Anita these questions.
4. Administer Medication: Fluphenazinne Decanoate injection. Remove Saline Lock.See Medication Administration Checklist – IM Injection, p. 38

5. Demonstrate Client Teaching:a. Identify the sign and symptoms of infection.See notes above…b. Describe what the client needs to do if she suspects an infection.Report to nurse or to go a clinic/hospital for treatment.CLIENT TEACHING Infection: Identify the signs & symptoms of infection.
Describe what the client needs to do if she suspects an infection. Medication Administration: Why is it important for Anita to take her monthly injection of
Fluphenazine Decanoate? Identify client teaching on the importance of Anita receiving her injections on a regular basis.
It is important for Anita to receive her monthly injection of Fluphenazine to maintain a therapeutic blood level. Also Anita is previously diagnose with Schizophrenia which put her at risk of developing postpartum psychosis.
Newborn AssessmentVital Signs: Apical pulse 110-160 bpm; temperature 36.2-37.7 (axilla); respiration 30-60 cpmBirthmarks: Mongolian spotsHair: Cradle cap/ scalp hair presentFontanels: Anterior – diamond shape, should be flat and soft (bulging may indicate increased ICP, sunken fontanelle may indicate dehydration), closes 12-18 month; Posterior – triangular shape, closes by 3 months.Molding: Cephalhematoma – blood collects between surface of cranial bone and periostimal membrane doesn’t cross suture line disappears in 2-3 weeks; Caput succedaneum – collection of fluid under the scalp caused by edema disappear 3-4 days.Eyes: NystagmusEars: Startle to loud noise (Moro reflex)Umbilical cord: usually falls off within 10-14 daysReflexes: should be present; Rooting/Sucking; Gaggling/Swallowing; Babinski/Plantar Flex; Tonic Neck
PLAN OF CARE:Urgent and Important Not Urgent but Important
QPABUBBLE-HE
Suicidal Thought/ DepressionSafety
SBAR for a possible pain meds and removal of Saline Lock
Newborn AssessmentMedication Administration - IM
Mental health statusPsychosocial
NutritionSupport system
Health teaching on notifying signs and symptoms of infection
References:Lewis; Moodle Slides/ Classroom Notes; Handouts; Leifer; Womble; Davis Drug GuideInternet Sources:http://www.healthpages.org/surgical-care/episiotomy/http://www.helpguide.org/articles/schizophrenia/schizophrenia-signs-types-and-causes.htmhttp://www.earlypsychosis.ca/pages/curious/symptoms-of-psychosis

http://www.mayoclinic.org/diseases-conditions/postpartum-depression/basics/symptoms/con-20029130http://www.webmd.com/drugs/2/drug-14460/fluphenazine-decanoate-injection/details