integrated quality improvement programme 2020-21 update
TRANSCRIPT
Integrated Quality Improvement Programme 2020-21 Update Page 1 of 6
Cover Sheet
Trust Board Meeting in Public: Wednesday 13 January 2021
TB2021.08
Title: Integrated Quality Improvement Programme 2020-21 Update
Status: For Information
History: Regular reporting
Board Lead: Chief Operating Officer
Author: Peter Fry, Deputy Director of Clinical Services
Confidential: No
Key Purpose: Assurance

Oxford University Hospitals NHS FT TB2021.08
Integrated Quality Improvement Programme 2020-21 Update Page 2 of 2
Executive Summary
1. The Trust Wide Integrated Quality Improvement Programme (IQIP) continues to
support clinical and managerial staff to inspire, support and create a culture that
improves and delivers quality care for our patients.
2. The paper includes a programme level update for each of the Programmes within
the IQIP in Phase 1.The Board are asked to note the updates for December 2020.
3. There are no formal escalations for December 2020.
4. The OUH Improvement Team new structure went live on 1st December 2020.
Recruitment has commenced for the Head of Quality Improvement. Despite a high
number of vacancies progress continues to be made in the majority of the
programmes being supported. In December 2020, the IQIP team has moved into
supporting the vaccination programme so some areas have not progressed as
much as planned. We are currently reviewing any opportunities with NHS
professionals/bank for additional support into vacant posts to help sustain
programmes along with supporting other critical programmes
Recommendations
5. The Trust Board is asked to:
Review the detail within the paper and note the progress made.

Start Out Define & Scope Measure & Understand
Design & Plan Implement Sustain 1
OUH – Integrated Quality Improvement Programme 2020-21 Trust Board Update – December 2020
• Integrated Quality Improvement Programme Phase 1
Summary Updates (2020/21) (slides 2 - 3)
• Programme Dashboards (slides 4 - 9)
OU
H –
Inte
grat
ed Q
ual
ity
Imp
rove
men
t Pr
ogr
amm
e

Programme Update
Urgent and Emergency Care Executive Sponsor: Sam Foster Accountable Officer: Lily O’Connor
• Home First (HF) now introduced countywide from 19th October 2020 • Every month since the Home First Service has launched, it has exceeded the
National Target of 75% of patients discharged from reablement being discharged with no ongoing support or a reduced level of support. However it did reduce from 82% to 76% in month, additional domestic care agencies have been sourced to mitigate this drop.
• JR and HGH ED’s have gone live with NHS 111 Appointments , 24/7 for both Adults and Children with additional slots from 15:00 – 17:00 also agreed
• The Childrens Assessment Unit is now live for GP referrals and imminently for SCAS 999 referrals
• LLOS average daily numbers dropped from 121 in October to 102 in November, with last 2 weeks hitting below the 90 target.
• Escalation: N/A
Outpatients Executive Sponsor: David Walliker Accountable Officer: Sharon Barrington
• Increase in clinic utilisation of JR (Blue) but below target at HGH. • Non F2F - % of non F2F appointments increased slightly in last month. New
letter production system (live Jan 21) will produce correct info for video appts • Ophthalmology SPA business case in final stages – 30% of referrals + 18% FU
for community management via Hub • 9,626 letters to patients via DrDoctor in Dermatology. Roll out to all areas • Brackley development on track. ENT to start clinics on 14.1.21, other to follow • Escalation: N/A
Planned Care Executive Sponsor: Sara Randall Accountable Officer: Matt Dooley
• Tumour Site Recovery – Top 2/3 priorities identified for LGI, H&N, Lung and Breast, developed with MDT Leads
• RTT Recovery – Supporting workstreams following weekly meetings with Divisions, ensuring escalation process and feedback in place
• IS Transfers – 1st list planned at Circle Reading for Orthopaedics • Inpatient stratification: OUH met the national submission deadline 11.12.20.
Next due 9.1.21 • Endoscopy Improvement Plan developed, key metrics to be finalised • Cancellations: review of Trustwide cancellation process, regional sitrep being
developed • Escalation: N/A
Underpinned by the OUH Quality Improvement Methodology, Quality Service Improvement and Redesign (QSIR), embedded across the organisation
Ow
nersh
ip w
ithin
services, led b
y Executive Sp
on
sors an
d A
ccou
ntab
le Officers
Executive Directors Team Objectives – Linked to all Programmes within the
IQIP
Building a sustainable workforce and improving Staff
Experience
Identifying and Managing Talent
Building a culture of clinical effectiveness, Quality
Improvement (QI) and Safety
Delivering High Quality
Delivering Sustainable Services
Providing an integrated care population and well being
Integrated Quality Improvement Programme 2020/21 – Phase 1 Update O
UH
– In
tegr
ated
Qu
alit
y Im
pro
vem
ent
Pro
gram
me

Programme Update
Theatre Productivity Executive Sponsor: Meghana Pandit Accountable Officers: Christopher Palin, Andrew Prince, Mark Scarfe and Jaideep Pandit
• Theatres Digital and Theatres Metrics Standardisation Groups have been established and supporting steering group
• Trauma and Orthopaedic activity at NOC is more than the activity recorded in previous year
• West Wing Emergency Theatres utilised 106% ( Capacity 10,640, used 11,319)
• Electronic requesting order form prioritised with IM&T • Escalation: N/A
Quality Improvement (QI) & Safety (No further update from November 2020, IQI resource supporting Vaccine programme)
Executive Sponsor: Meghana Pandit Accountable Officer: Anny Sykes
• Integration of QI across OUH – IQI Team involved with supporting workshops with latest QI Hub cohort and Oxford Brookes Masters Students
• QSIR V – Planned to start in January and applications open, run with BOB ICS faculty and support to sessions from IQI Team
• GIRFT – IQI Team actively supporting Trust GIRFT Lead Nov 2020 • GIRFT – Priority to support Divisions with an infrastructure to ensure
reporting from Divisional Action Plans • GIRFT – Active support to 6 challenged specialities (Ophthalmology,
Gynaecology, Urology, Breast, T&O and OMFS) supporting local GIRFT Leads
• Escalation: N/A
Non Clinical Improvement Programme (no update from November 2020, awaiting data for December -15th January 2021)
Executive Sponsor: Jason Dorsett Accountable Officers: Andrew Carter / Jon Evans
• Agency expenditure has decreased from an average of £1.8m to £1.1m per month
• Incentive scheme for increasing Nursing and Midwifery capacity has been implemented, options 1 and 2 went live on the 2nd of November. Option 3 will go live in December.
• The availability of temporary workers has reduced, it is expected that the reduction in monthly expenditure will continue or remain at a lower level than previous months expenditure.
• Escalation: N/A
Underpinned by the OUH Quality Improvement Methodology, Quality Service Improvement and Redesign (QSIR), embedded across the organisation
Ow
nersh
ip w
ithin
services, led b
y Executive Sp
on
sors an
d A
ccou
ntab
le Officers
Executive Directors Team Objectives – Linked to all Programmes within the
IQIP
Building a sustainable workforce and improving Staff
Experience
Identifying and Managing Talent
Building a culture of clinical effectiveness, Quality
Improvement (QI) and Safety
Delivering High Quality
Delivering Sustainable Services
Providing an integrated care population and well being
Integrated Quality Improvement Programme 2020/21 – Phase 1 Update O
UH
– In
tegr
ated
Qu
alit
y Im
pro
vem
ent
Pro
gram
me
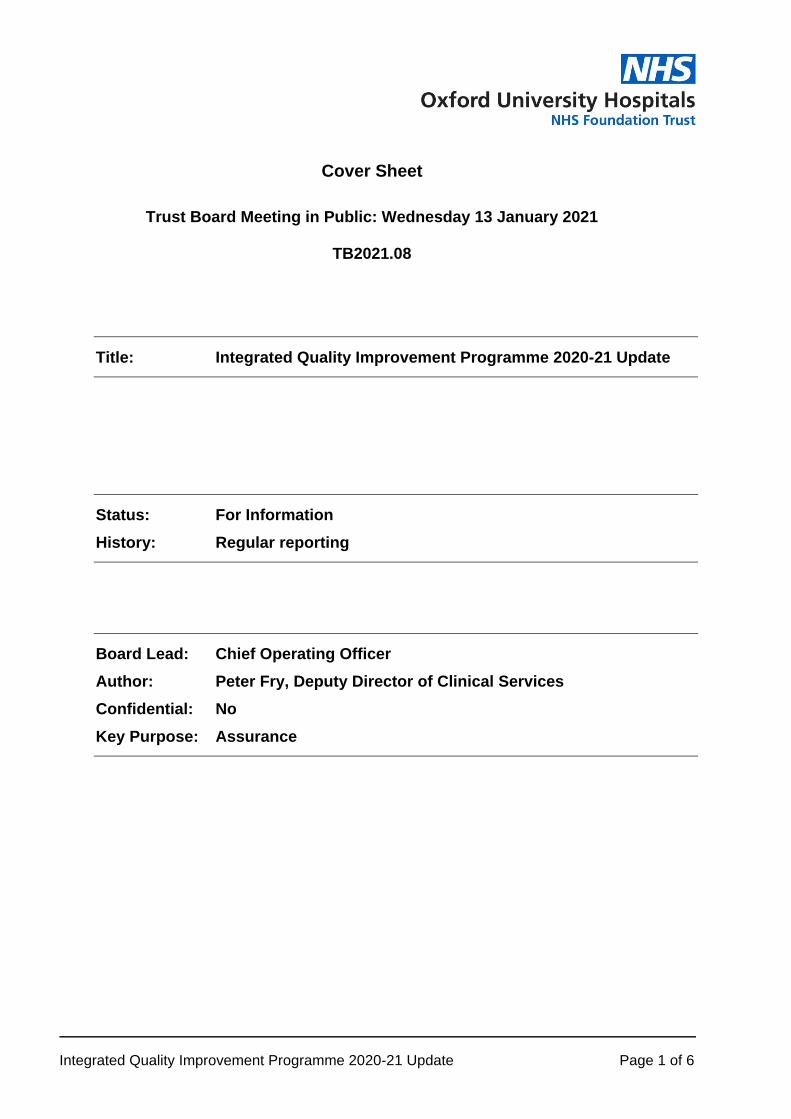
• In November the average daily LLOS numbers decreased to 102. Although this is above the target of 90, this was a drop on the previous two months. In the last two weeks of November the numbers have been below the target of 90. When compared with November-19 there has been a 26% drop YOY in the average daily LLOS numbers
• In November there started to be an increased LOS in respiratory and infectious diseases due to the prolonged stay of patients admitted with Covid.
• The Horton General Hospital continues to have an increased LOS with Northamptonshire. The Northamptonshire delays had reduced in October but have increased back up in November.
• The Oxfordshire system is currently reviewing all discharge delays to determine what additional support is required to support more patients going directly home, especially those on a delirium pathway who have an extended LOS.
• NHS 111 can now book directly to the JR and HGH ED’s 24/7 with additional slots from 15:00-17:00hrs
• Mental Health workers are now in 111 • Following regular audit it was identified that the national pathway questions
for people with eye problems needed to be reviewed to prevent unnecessary ED attendances. Work on this has commenced.
• A head injury virtual pathway is being developed • The Childrens Assessment Unit is now live for GP referrals and imminently for
SCAS 999 referrals • Localised Oxfordshire comms are being drafted for dissemination in January
2020 to enhance the National comms campaign as the visibility of this material has been limited
• The management process for unheralded patients is being finalised
OU
H –
Urg
ent
and
Em
erge
ncy
Car
e P
rogr
amm
e Executive Sponsor: Sam Foster Accountable Officer: Lily O’Connor
Urgent and Emergency Care Improvement Programme Dashboard - Dec 2020
Every month the service has exceeded the National target of 75% of patients discharged from reablement being discharged with no ongoing support or a reduced level of support. The number of pick-ups per week has exceeded the trajectory throughout November. However, this additional case load, and an increase in number of patients on contingency whilst long term care is sourced has led to an increase in LOS within the service and delays in patient pick-ups. In November 76% of patients referred into the service were picked up within 7 days, which was a drop from 82% in October. The service has though continued to perform above baseline in the % of patients picked-up within 7 days. To mitigate this dom care agencies have been commissioned to become involved within Home First. 2 agencies commenced pick-ups in November and 3 further agencies have been commissioned by OCC (Start dates to be confirmed) Increased therapy capacity to manage demand through both short term means (redeployment of staff etc) and long term have been explored. A Gap analysis has been undertaken, a minimum requirement for Therapy input has been drafted to ensure that Oxfordshire’s OT resource is only used where absolutely necessary. It has been agreed that remote therapy reviews can be undertaken and use of Attend anywhere for this is being piloted.
Home First NHS 111 First Patients with a LLOS
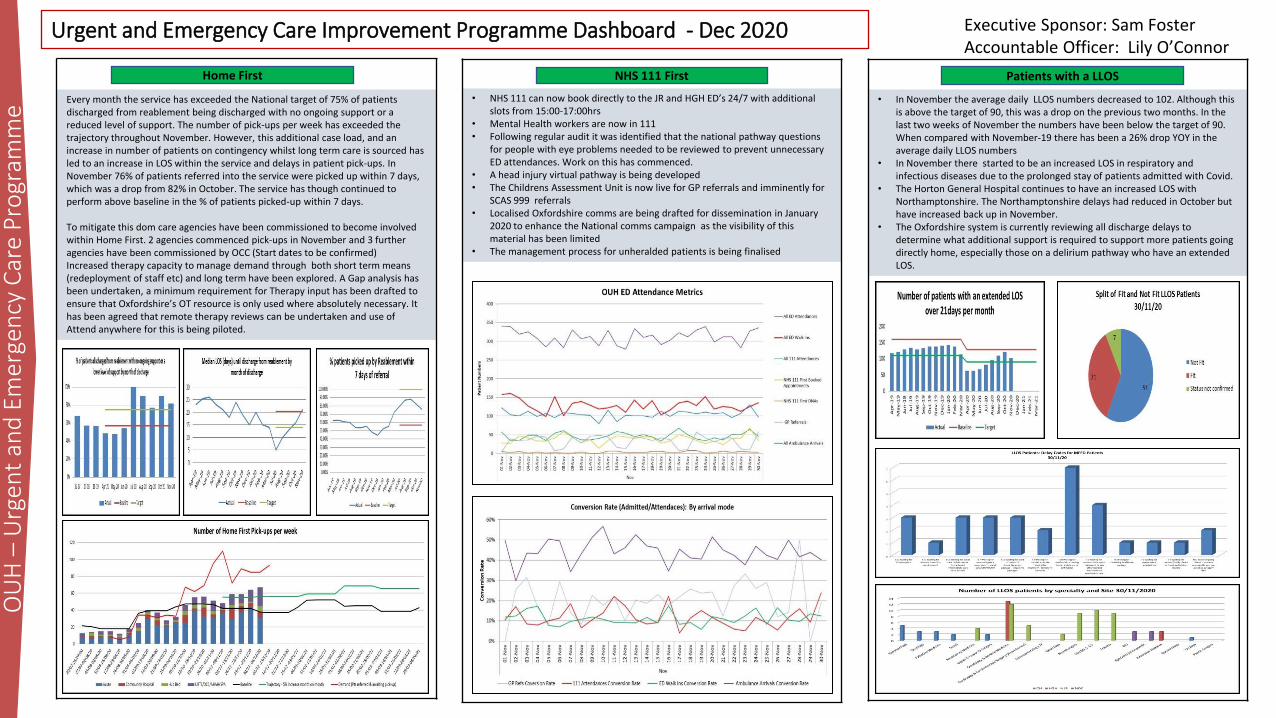
Implementation of electronic checkout delayed. Coding process being looked into by EPR, Commissioning & Informatics – needs to be done in PowerChart so consultants can record as part of electronic checkout process (currently done in HIM Coding). Dermatology are also clearing PMFU backlog. Dermatology now using Revenue Cycle & Consultants now using Ambulatory Organiser in PowerChart – implementation gone well & this is now imbedded.
Outpatient Improvement Programme Dashboard - Dec 2020 Executive Sponsor: David Walliker Accountable Officer: Sharon Barrington
• Utilisation increased in Blue Area (83%) but HGH still below target (47%). • Booking SOP being tested – services to confirm room bookings with 6 weeks’ notice. • Services given access to clinic schedules on O Drive to view available clinic rooms for booking. • Weekly dashboard being shared with DDOs, OSMs and service staff showing utilisation data, short notice cancellations & no shows • BookWise for JR Blue + HGH – b/c approved by Business Planning – final sign off required by Sara Randall & David Walliker.
Usage, Clinic Build, Governance • In November, 11.9% of 95,066 appts were carried out Non F2F, compared
to target NHSE of 25% • Services have submitted their requirements for 212 treatment functions
(TF), of the 253 in total. Each TF has multiple clinics types to be set up in EPR, so far 794 clinics have been built and ready for service to use
• Project structure encompassing; user groups, service level teams, OPT task & finish group has now been established
Issues and Mitigations • Existing letter production software unable to support Attend Anywhere
clinics, requiring services to locally manage letters for video appts. This caused issues with letters sent to some patients, which has now been addressed and communications sent to GP’s.
• New letter production system scheduled to go-live on 13th Jan 2021, will support video appointment letter production.
• Existing EPR clinic builds did not support video appts, forcing services to book video appts in F2F slots, resulting in under reporting.
• Revised prioritisation now in place to convert clinics to the required templates, based on activity and readiness to provide Non F2F appts.
• Data shows ~1,840 patients per week attend OUH for an Outpatient blood test
• Manual audits being carried out to determine % of these who attend for bloods only
• ~48 pts per week attend their GP surgery for a blood test which was requested by OUH
• B/c being worked up to compare options for providing phlebotomy in community including bus, static units, drive-through marquees
On hold whilst clarification on the use of NHS mail accounts at OUH is clarified.
Digital Dermatology
Clinic Utilisation
Remote blood testing
Directorate NHSmail accounts
Performance of DrDoctorto date in Dermatology (22/12/20 ref Leopard report) • Total letters 9,626 • Total immediate prints 2080 • Delayed prints 2377 • Electronic views 5104 • Too late for printing 65
Digital
c30% of referrals could be managed virtually and a further 18% of FUs by community optometrists, freeing up space and time (capacity) in OPs. A diagnostic hub would provide diagnostics for all referred patients with triage using OUH consultants . Diagnostics would be using the same equipment as eye hospital to ensure repeatability and comparison and shared and stored digitally. Business case in final stages; due to be completed by mid January 2021. To be signed off by OUH and OCCG.
Ophthalmology SPA Brackley Hospital
Ventilation has been installed and throughput improved by the service. This project is no longer required.
MaxFax
OU
H –
Ou
tpat
ien
ts P
rogr
amm
e
Gynae Oncology: Start date 1.12.20 pushed back as awaiting feedback on patient leaflet from patient panel. Likely to start in Feb 2021 Info video to be filmed in Jan 21. Trigger card signed-off. SOP signed-off. 9 x KPIs signed-off. Patient experience survey devised + review meeting to sign-off first wk of Jan 2021. Pts will be tracked manually.
Baseline shows 8 services already offer a form of PIFU mostly as ‘open access or SOS appointments’. These are not being tracked so data on patients who revert to a routine FU pathway is not easily extracted. Tracking for PIFU patients via EPR to be explored in Jan 2021.
Patient Initiated FU (PIFU)
0
0.05
0.1
0.15
0.2
0.25
0.3
0
20000
40000
60000
80000
100000
120000
Total Non-F2F Activity
Total Optattendedappts
NHSETarget(25% ofALLappts)
Total %NonF2Fappts
Non F2F
Three clinic rooms and one minor ops room with 25 air changes/hour available from early January for exclusive OUH use Specialities involved: ENT, Plastics, Cardiology, Ophthalmology, Gynaecology, Audiology/SLT Official start date: ENT to commence full day clinics on 14 January 2021 (30 patients/week) , other specialities to follow
Outstanding work: -Finalization of OUH-Brackley legal agreement -Development of business case and cost centre to hire full-time HCA and additional equipment
Trust wide opportunity ~ 85% of patients have SMS capability (mobile # but may be out of date) ~ 4,800 letters printed per day With 51% uptake = 2805 letters read digitally/day With 253 working days = 619K letters viewed digitally Next steps; • Plan roll out of DrDoctor digital letters to all areas • Wider digital by default programme to include mapping of system solutions
and communications with patients and stakeholders.

Project 4: BOB ICS Cancer Dashboard (Productivity)
TVCA dashboard has been developed pan-alliance, and a hybrid dashboard is in development with OUH
Project 1: Tumour site recovery
Monthly meetings with LGI, H&N and Lung / Weekly meetings with Breast Performance to be reported via Cancer strategy group
Top 2/3 priorities identified for LGI, H&N and Lung with MDT leads H&N Priorities: 1: Surgical capacity for diagnostics and treatments – From 4th Jan additional theatre capacity at Churchill, awaiting confirmation of exact capacity. 2: Insertion of PEG’s prophylactically - inc H&N/ nutritional nursing and gastro services LGI Priorities: 1: Audit of the use of FIT testing / impact on 2ww referrals – in progress 2: Ownership of patients early in pathway 3: Current Colorectal cancer pathway mapped now to review against National TVCA pathway. Lung Priorities: 1: Increase access to neck lump clinic to exclude metastatic disease or assist with diagnosis – Process agreed to initiate direct access for neck lump fine needle aspiration in line with respiratory appointment. To be confirmed 18 Dec 2020 for start date in new year. 2: Increase biopsy capacity 3: Increase theatre capacity Breast: 1: Review of joint clinic/radiology availability 2: Improved clinic room availability/provision in line with Radiology support Endoscopy: 1: Recover plan identified in Project 2 will incorporate cancer pathways. 2: TVCA project manager. Initial meeting to discuss job description and advert in December . This post will go out to advert in 2020 . To partly support Endoscopy with specific focus on Cancer pathway.
6
Planned Care Programme – Dashboard December 2020 Executive Sponsor: Sara Randall Accountable Officer(s): Matt Dooley
Project 2 and 3: RTT recovery and Diagnostic
Weekly meeting with Divisions to review recovery plan • Monitor of actions against submitted plan / Monitor of actions against funding and mitigations Weekly escalations and feedback loop • Timely escalation and feedback to services – working very well with positive response from divisions Weekly Elective care recovery group • Oversight of performance / Review of Orbit reports for Activity against Phase 3 plan
Identified work streams 1: All patients contacted by CSU. Patients now under review with Independent sector. All relevant information sent to Independent sector. • 1 full time member of staff to support admin process • 13 Orthopaedic patients and 3 Gynaecology patients with TCI at Circle, • 11 Orthopaedic patients with TCI at Berkshire Independent Hospital 2: Improvement plans • Urology – Referral to admission for patient pathway at the Horton. Action plan provided to service, expect first project
group meeting January 2021. Linked to theatre improvement project • Therapies –Aim to reduce length of wait and breach patients within Therapies. Urogynae/Therapies plan provided to
service, expect first project group meeting in January 2021 • Genetics – Patient pathway mapped pre and post clinic. Project plan shared with service for agreement Dec 2020 3: Endoscopy Improvement • Plan provided to service, performance metrics to be added. Themes identified are Manage Demand, Increase Capacity,
Improve Utilisation 4: Cancellations • Review of cancellation process Trust wide. Draft document circulated for feedback. • Region requires daily sit rep for cancellations in the past 14 days for Non clinical reasons. • Initial information report pulled and a sub group identified of the ECRG to review the cancellations reasons and how
they are logged on EPR to ensure that reports are relevant to support services as well as local an national reporting
OU
H –
Pla
nn
ed C
are
Pro
gram
me
Inpatient Stratification
Retrospective work: All RCS codes pull through from EPR to PTL . A column on the PTL shows the expiry date of the review. Admin teams have transposed 7,022 patient reviews into on EPR as of 4.12.20 as compared to 3 reviews recorded on EPR on 22.10.20. The proxy arrangement for admin to transpose consultant RCS codes into Powerchart has been extended. EPR enhancements: Traffic light flag + free text added to EPR consultant list. 2 questions added to lead consultants to harm review Powernote and Ulysses incident form if moderate harm. Prospective review: Roll out starting in NOTTSCaN Jan 21 for consultants to enter RCS codes into EPR. National submission: OUH met the national submission deadline 11.12.20. Next due 9.1.21

Executive Sponsor Meghana Pandit Accountable
Officers
Jaideep Pandit - NOTTSCaN Theatres Mark Scarfe – SUWON Theatres Andrew Prince – NOC Theatres Christopher Palin – Cardiac Theatres
Project Facilitator Arnold Victor
KPI’s reporting period : July 2020 - November 2020 Project start date: Recommenced in August 2020
OU
H –
Th
eatr
e P
rod
uct
ivit
y P
rogr
amm
e
Theatres Improvement Programme Dashboard - December 2020
0
500
1000
1500
2000
2500
Jul Aug Sep Oct Nov
Sessions
0
1000
2000
3000
4000
5000
Jul Aug Sep Oct Nov
Cases
55% 59% 57% 58% 57%
0%
20%
40%
60%
80%
100%
Jul Aug Sep Oct Nov
Avg. Efficiency Target
60% 63% 62% 61% 62%
0%
20%
40%
60%
80%
100%
Jul Aug Sep Oct Nov
Average Utilisation Target
48.25 49.25 37.75
114.25
38.4
-96.75 -98.25 -98.25 -90.5 -94.8 -150
-100
-50
0
50
100
150
Jul Aug Sep Oct NovAverage Overrun Minutes Average of Underrun
Cases Delivered Sessions Delivered Efficiency Overrun / Underrun Utilisation
The above chart shows the current Trauma and Orthopaedic activity at NOC is more than the activity recorded in Jan 2020
All 8 theatres, all specialties
T & O : Theatres 3 to 8
T &O and plastics
West Wing Emergency Provision Background : • Emergency main case of elective cancellations ( 25%
- Pre Covid) • Nov 2019 - 23 adult cancellations and 6 paediatric
cancellations, excluding cancellations associated to staff and overruns
Introduction of New Emergency provision • 3 days a week for general adult emergencies • .5 day for 5 days a week for NEL Paediatrics • SOP for use of WW lists and lead clinician to oversee
governance
Result • In hours utilised 106% ( Capacity 10,640, used 11,319) • 96 cases delivered , 2 to 13 per day ( 50 adults & 46
paeds) • Only 2 elective cases cancelled for emergency ( adults) • No paediatric elective cases cancelled to
accommodate emergency procedure
Increase in T &O activity
Highlight Progress Update
Improvements to POA • Development of Electronic - Pre-Op assessment forms have been
completed, a step towards standardising workflows across OUH • Electronic POA tracking board has been developed to improve scheduling
appointments • Steps to unify trust governance and POA standards is in progress SUWON Improvement Plans • SOP for 6-4-2 implemented, session allocation by specialty under review • Engagements with specialities in progress to improve list planning • Review of day DCU capacity and workflow at HGH in progress • Deep dive analysis on Urology completed and improvement plans agreed NOC Improvement Plans • Process to manage 6-4-2 and SOP implemented • Theatre performance group established to monitor list planning • Changes to theatre start and end time implemented to address delayed
start and SOP of Golden Patient initiated • Recording time-stamps process • New pathway for theatres 7 & 8 to handle day cases introduced • Pooled pathway for Hip and Knee surgery introduced

Project 3
GIRFT / 7 Day Services
• Development of existing GIRFT support • Progress GIRFT action plans • Engagement with local GIRFT team systems • Progress Financial Benefits - QI activities • Completion of 7 Day Services audit and support for
transition to BAU
Project 2
Integration of Quality Improvement across OUH
• Integration of all QI activities across the OUH • Introduction of Ulysses QI Form – recording of all QI
projects at OUH • Intranet page for OUH QI – access for all • Collaboration between QSIR faculty and QI Hub team
Project 1
Quality Service Improvement and Redesign (QSIR)
• Embedding QSIR methodology across OUH • Building capability using QSIR • Introduction of QSIR Virtual at OUH • Collaboration with BOB ICS QSIR Faculty
OU
H –
Qu
alit
y Im
pro
vem
ent
& S
afet
y Pr
ogr
amm
e
Executive Sponsor Meghana Pandit Accountable Officer Anny Sykes Programme Managers Jo McMahon / Arnold Victor
Underpinned by the OUH Quality Improvement Methodology, Quality Service Improvement and Redesign (QSIR), embedded across the organisation
Project 1 Update - November 2020
Quality Service Improvement and Redesign (QSIR)
• QSIR Virtual (QSIR V) Programme – planned to launch across BOB ICS in January 2021 • Current QSIR Practitioner Cohort due to complete by 23rd November
Project 2 Update – November 2020
Integration of Quality Improvement across OUH
• IQI Team supporting bi-weekly workshops as part of the current QI Hub cohort (Sept to Dec 2020) • Support to individual students on the QI Hub using various Improvement tools • Support to Oxford Brookes Masters Students within developing Compassionate Care Modules – four sessions per year on
transformational and change management • Ulysses QI form due to be launched end Nov 2020 during Clinical Audit Awareness Week
Project 3 Update – November 2020
GIRFT / 7 Day Services
• IQI Team actively supporting Trust GIRFT Lead (November 2020) • Supporting Divisions with consolidating all specialty level GIRFT Action Plans into Divisional Plans. Designing the infrastructure for
formal reporting on progress of all GIRFT actions (included Performance and Finance teams) • Active support from IQI Team to six challenged specialties following GIRFT Deep Dives (Ophthalmology, Gynaecology, Urology,
Breast, T&O and OMFS) • Ongoing engagement with local GIRFT Implementation representatives and supporting GIRFT across ICS • Development of Board Assurance Framework and 7DS paper to Integrated Assurance Committee (December 2020)
Quality Improvement and Safety Programme Dashboard - Nov 2020

Highlights (highlights only)
Progress in last period
• Agency spend has decreased from an average of £1.8m in 2019/20 to £1.1m per month . This is
• Standing up of new departments at short notice • Fast tracking of recruitment of new posts to support increasing
demand levels.
Escalation for TME to note
• There is a significant decrease in the availability of temporary workers via commercial agencies. This should not be relied up upon as a source of workforce
Project Trajectories
Improvement Workstreams Projects Target Baseline Data source Last Month
(Oct-20) This Month
(Nov-20) Trend
Target Achievement Date
Lead/Owner
P1 Premium Capacity
To reduce agency expenditure to meet the ceiling provided by NHSI
£16.4m (£1.3m per month)
£22m Finance/
Workforce
£1.29 (A) £1.02M (A)
31-Mar-21 Jason Dorsett
To reduce premium staff volume TBC 1,012 WTE 128 WTE (A) 118 WTE (A)
P2 Temporary staffing To reduce temporary staffing expenditure (Bank)
£33m £39m Finance/
Workforce
£4.23M (B) £4.53 M (B) 31-Mar-21 Jason Dorsett
To reduce temporary staffing volume (Bank) 872 WTE (B) 903 WTE (B)
P3 In year savings Achievement of the procurement savings in line with
tracker £9M N/A
Procurement Tracker
£1.5m Target YTD £0.4m Actual YTD
TBC 31-Mar-21 Gary Welch
G: On track A: Progress with some issues, close monitor R: Serious issues, recovery plan required
Project Goal To instigate and implement non-clinical projects which will support the operational efficiencies of the Trust Executive Sponsor Jason Dorsett
Project start & end dates April 2020 to March 2021 Accountable Officer (s) Jon Evans, Andrew Carter
Programme Update Fortnightly Project team meetings Daily Improvement Facilitator Samantha Parker
OU
H –
No
n C
linic
al Im
pro
vem
ent
Pro
gram
me
Non Clinical Improvement Programme Dashboard - Nov 2020