integrated pharmacotherapy i drug targets, ligands ... · pdf file1 integrated pharmacotherapy...
TRANSCRIPT
1
Integrated Pharmacotherapy I
Drug Targets, Ligands, Receptors, and
Mechanisms of Drug Action
Required reading: Chapters 1 and 2, Basic and Clinical
Pharmacology, 10th Ed., Katzung BG, McGraw Hill, 2007.
Edward Fisher, Ph.D., R.Ph. Professor and Associate Dean for Academic Affairs
Professor and Associate Dean for Academic Affairs
University of Hawaii at Hilo College of Pharmacy [email protected]
2
Learning Objectives
After attending these lectures, completing the required reading, &
studying these handouts, you should be able to describe the basic
principles of drug receptors & pharmacodynamics including:
The dose-response relationship
Signaling mechanisms and drug action
The relationship between dose and clinical response
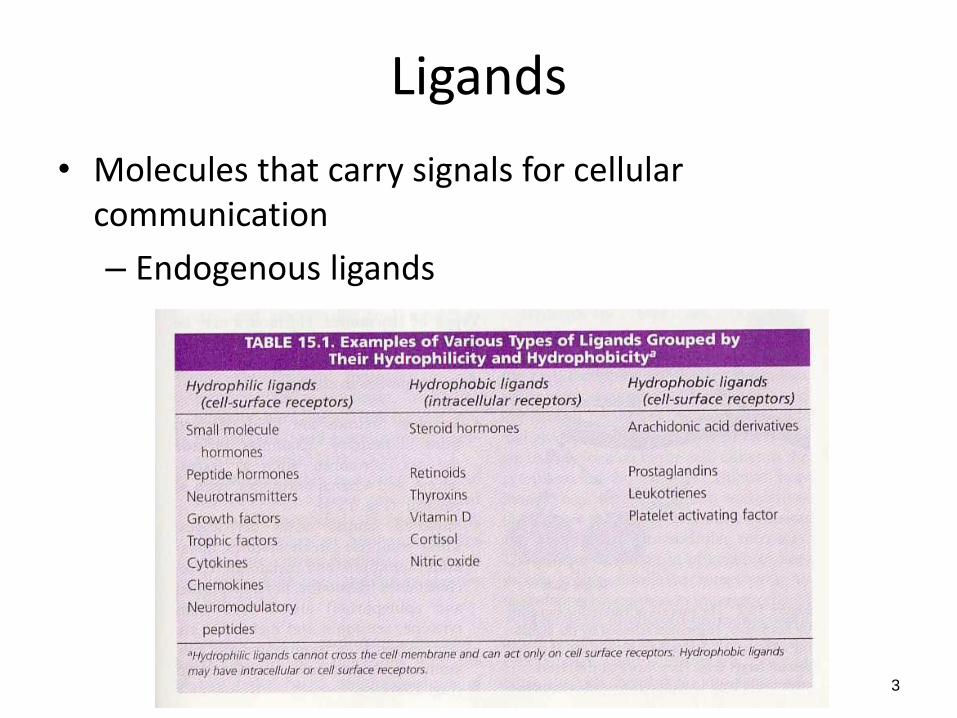
Ligands
• Molecules that carry signals for cellular communication
– Endogenous ligands
3
Ligands
• Endogenous ligands
– Neurotransmitters
– Hormones - secreted from endocrine glands
• Ductless and located in connective tissue
• Secreted into blood and have effects at distant sites, they are released:
– In steady amounts (e.g. thyroid hormone)
– Based on specific cycle
» Circadian rhythms (e.g. glucocorticoids)
» 4-week cycle – female hormones
4
Types of Hormones
• Steroid hormones– derived from cholesterol • Amino acid derivatives
– Catecholamines – Histamine – Serotonin – Melatonin
• Peptides and proteins – Neuropeptides (vasopressin, oxytocin) – Pituitary hormones (corticotropin, gonadotropins) – Gastrointestinal hormones (insulin)
• Eicosanoids – Derived from polyunsaturated fatty acids especially arachidonic acid
• Prostaglandins, prostacyclins, leukotrienes, thromboxanes
5
Types of Hormones
• Hydrophobic hormones – Receptors found in the cell – Act by affecting gene expression – Examples
• Sex hormones – Androgens and estrogens
• Adrenal hormones – Mineralocorticoids and glucocorticoids
• Hydrophilic hormones – Receptors on cell surfaces – Examples
• Catecholamines • Peptide hormones • Eicosanoids
6
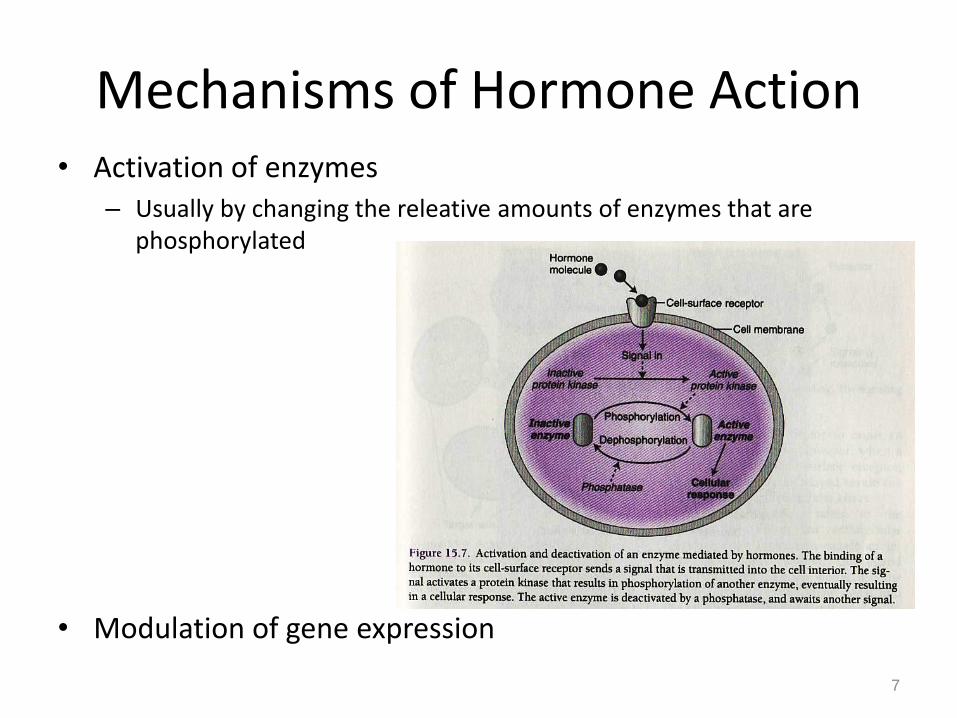
Mechanisms of Hormone Action • Activation of enzymes
– Usually by changing the releative amounts of enzymes that are phosphorylated
• Modulation of gene expression
7
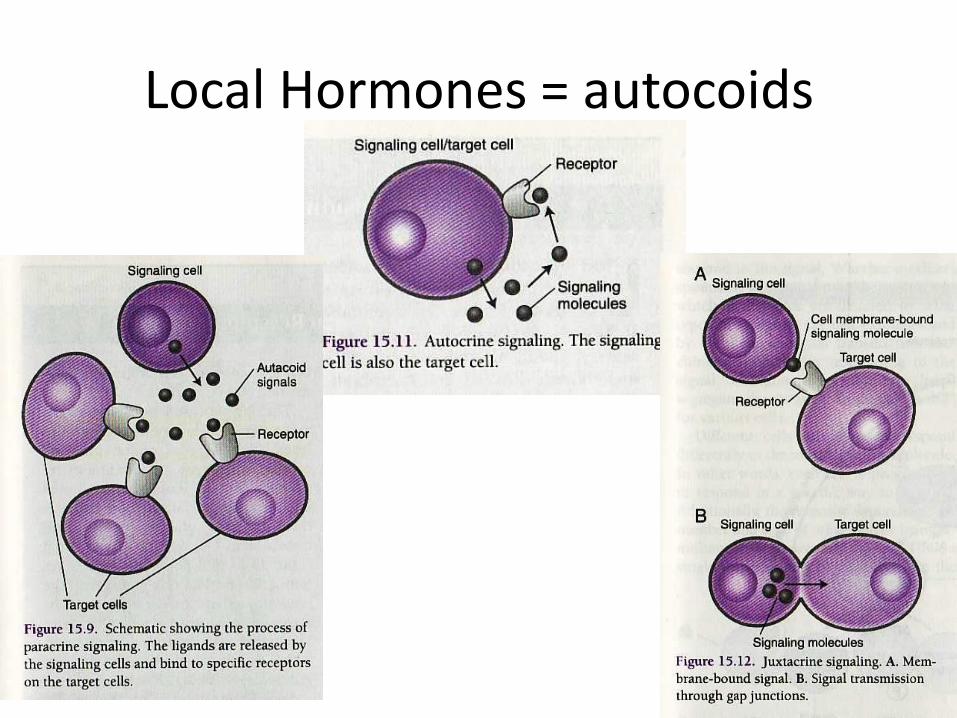
Local Hormones = autocoids
• Characteristics – Transport via blood is not necessary – Have local effects – Short duration of action
• Functions – Defense – Repair – Classifications
• Paracrine – act on neighboring cells – Synaptic transmission – special type of paracrine
• Autocrine – also act on the cell that secreted them – Influence a group of cells to act the in the same way
• Juxtacrine – direct contact is necessary – Gap junctions
8
Local Hormones = autocoids
9
Introduction to Pharmacology
10
Pharmacology: the study of substances that interact with living
systems through chemical processes.
Medical pharmacology – therapeutic application
Toxicology – undesirable effects of chemicals on living systems
Pharmacodynamics: the actions of the drug on the body.
Biochemical effects, mechanism of action (MOA)
Drug classification
Pharmacokinetics: the actions of the body on the drug.
Absorption, distribution, metabolism, & excretion
Involved with the time course of the drug in the body
How the drug effects you
How you effect the drug
Introduction to Pharmacology
11
Receptor: part of an organism or cell (macromolecule) that
interacts with a ligand (drug, endogenous molecule) causing a
chain of biochemical events leading to an observable response. Active states vs. inactive states
Drug: any substance that brings about a change in biologic
function through its chemical actions.
Endogenous – synthesized in the body (hormones)
Xenobiotics – chemicals not synthesized by the body
Drug: Pharmacy definition: Articles intended for use in the
diagnosis, cure, mitigation, treatment or prevention of disease in
man or other animals
.
Introduction to Pharmacology
12
Drug targets – biomolecules that have a role in the disease
process and are considered to be the site of action for drug
therapy (receptors, enzymes, DNA, ion channels, transport
proteins)
Agonist: a drug that binds to and activates a receptor which
brings about an effect.
Albuterol – β2-selective adrenoceptor agonist
Introduction to Pharmacology
13
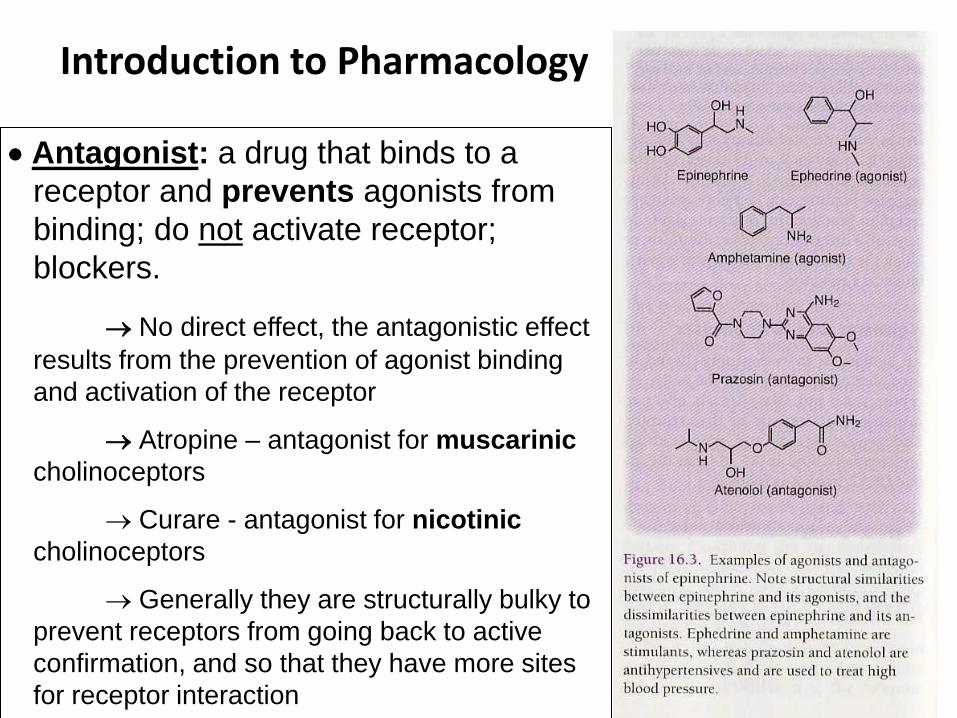
Antagonist: a drug that binds to a
receptor and prevents agonists from
binding; do not activate receptor;
blockers.
No direct effect, the antagonistic effect
results from the prevention of agonist binding
and activation of the receptor
Atropine – antagonist for muscarinic
cholinoceptors
Curare - antagonist for nicotinic
cholinoceptors
Generally they are structurally bulky to
prevent receptors from going back to active
confirmation, and so that they have more sites
for receptor interaction
Introduction to Pharmacology
14
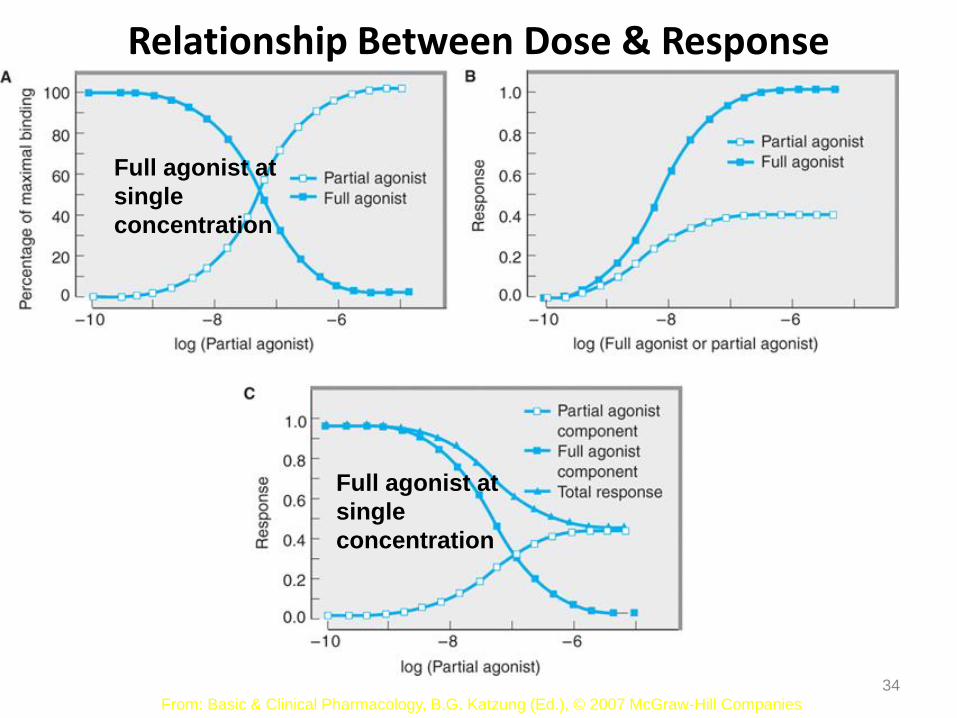
Partial Agonist: a drug that binds to a receptor and activates it,
but the effect is not as great as with a full agonist.
Are agonists if no full agonist is present; are antagonists if a full
agonist is present
Pindolol – partial β receptor agonist
Inverse Agonist: a drug that binds to a receptor and stabilizes it
in the inactive conformation.
Constitutively active receptors – active without binding to agonist
Many drugs that act as competitive antagonists
are really partial agonists
Introduction to Pharmacology
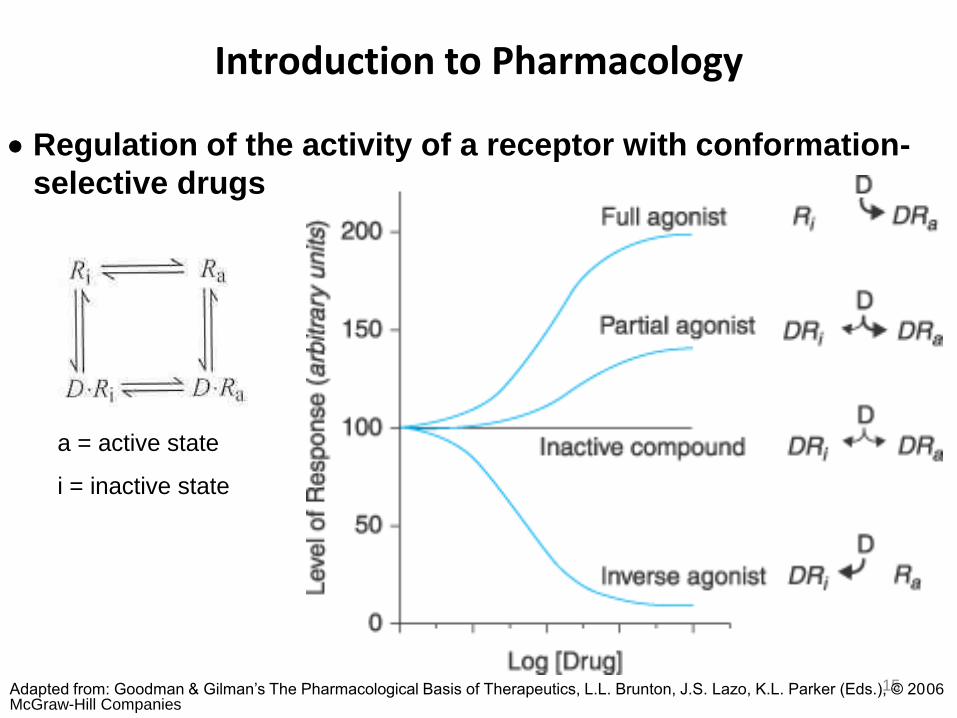
15 Adapted from: Goodman & Gilman’s The Pharmacological Basis of Therapeutics, L.L. Brunton, J.S. Lazo, K.L. Parker (Eds.), © 2006 McGraw-Hill Companies
Regulation of the activity of a receptor with conformation-
selective drugs
a = active state
i = inactive state
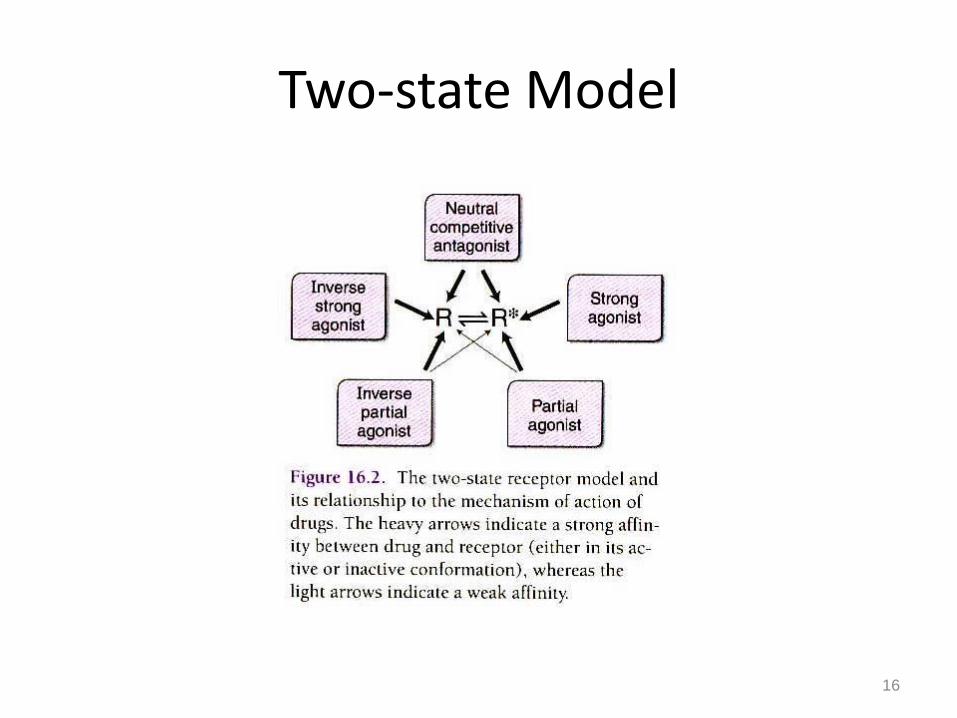
Two-state Model
16
A Little Background on Drugs
17
A drug is a substance that brings about a change
in biologic function through its chemical actions.
Sources
Endogenous
Exogenous (xenobiotics)
States
Solids
Liquids
Gases
Size
Vast majority of drugs have a MW between 100 – 1000
MW 100 helps achieve selective receptor binding
MW 1000 inhibits diffusion-mediated distribution
= Chemicals foreign to the
biological system in question
Drugs do not create effects they modulate function
A Little Background on Drugs
18
Chirality: stereoisomerism, R or S – “handedness”
Over 50% of all useful drugs are chiral
In the majority of cases, one enantiomer will have different
pharmacodynamics, pharmacokinetics than the other enantiomer
Labetalol (2 chiral centers, 4 enantiomers)
(S,R) – α-blocker
(R,R) – -blocker
(S,S) and (R,S) – inactive
Eutomer – isomer with desired activity
Distomer – isomer with undesired activity
Prototype drug: a member of a drug group that typifies the
most important characteristics of the group.
There are several thousand drugs that are currently available
arranged into ~ 70 groups
Drug Receptors & Pharmacodynamics
19
Receptors:
1.) Determine the quantitative relations between dose or
concentration of drug and pharmacologic effects
receptor number in various target tissues
2.) Are responsible for selectivity of drug action
Affinity – determined by chemical forces that cause drug
to bind to the receptor
Efficacy – change in confirmation toward the active state
Intrinsic activity – ability to evoke maximal effect after
binding
3.) Mediate the actions of both pharmacologic agonists and
antagonists
receptor classes, subtype, and isoforms
Some drug’s MOA do not involve receptors: antacids, osmotics.
Receptor:
Class α β
Subtype α1 α2
Isoforms α1a α1b
20
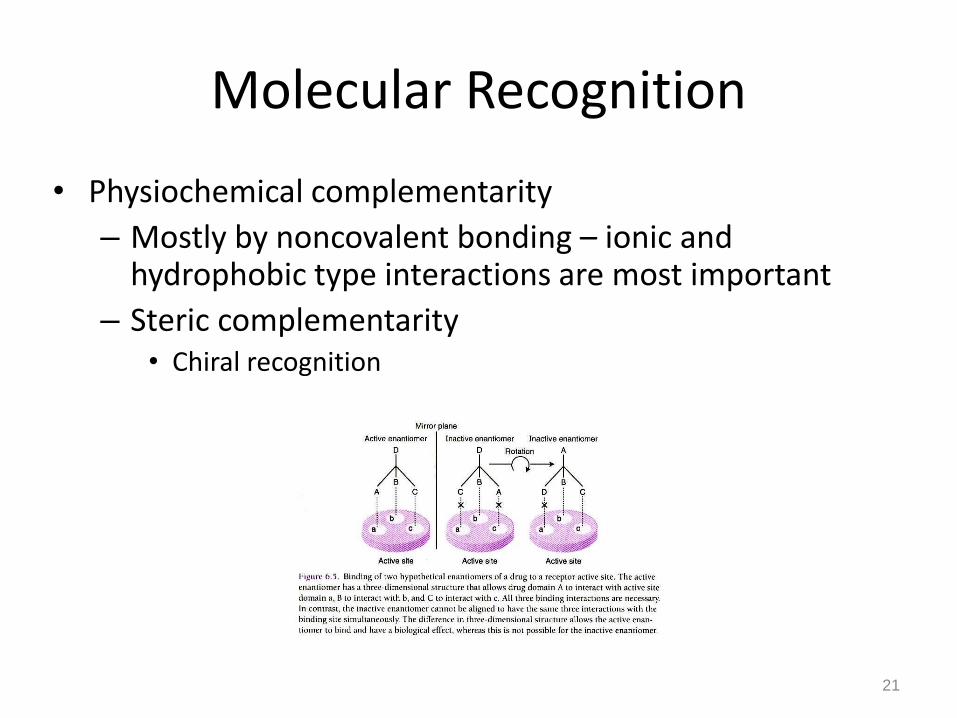
Molecular Recognition
• Physiochemical complementarity
– Mostly by noncovalent bonding – ionic and hydrophobic type interactions are most important
– Steric complementarity • Chiral recognition
21
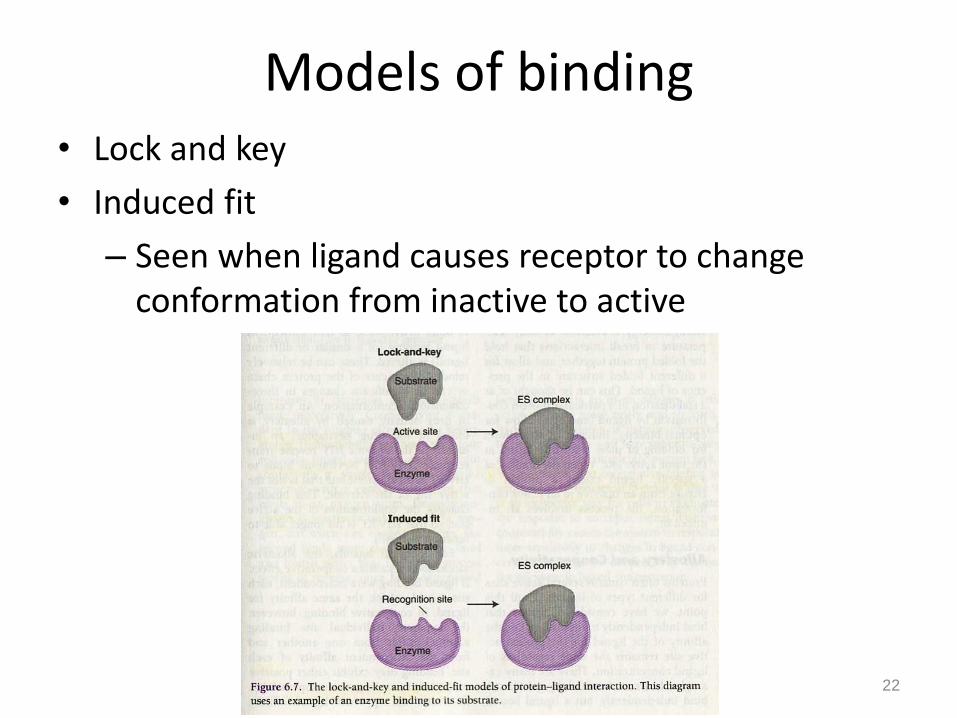
Models of binding • Lock and key
• Induced fit
– Seen when ligand causes receptor to change conformation from inactive to active
22
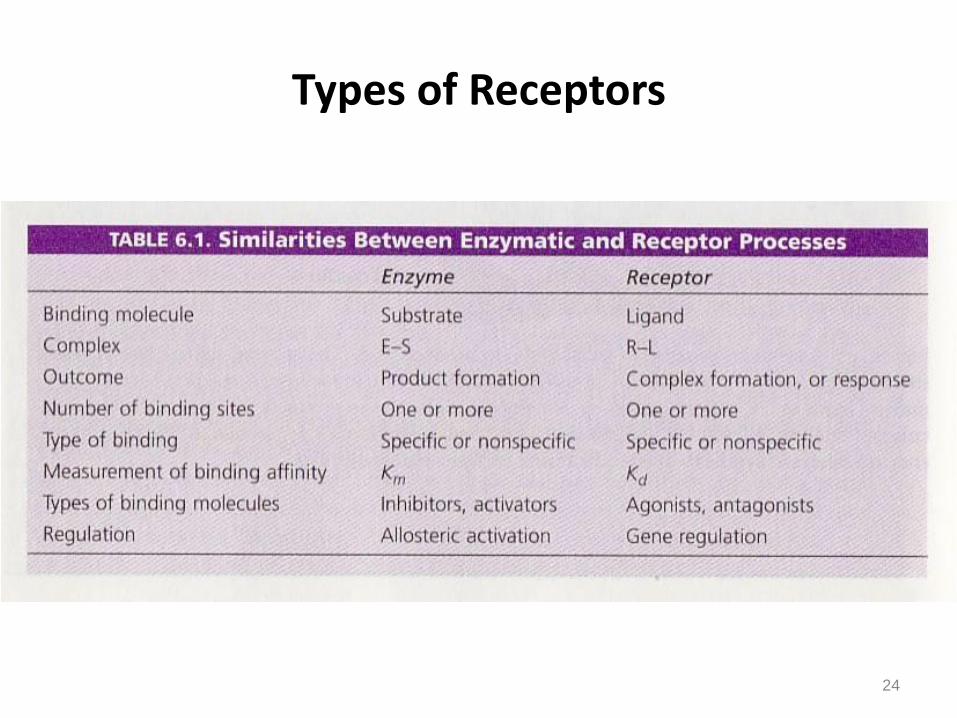
Types of Receptors
23
Regulatory Proteins:
Mediate actions of most drugs and endogenous chemicals
(neurotransmitters, hormones, autocoids)
Best characterized
Enzymes:
Usually through inhibition
Methotrexate inhibits dihydrofolate reductase
Transport Proteins:
Digoxin inhibits Na+, K+ ATPase
Structural Proteins:
Colchicine inhibits tubulin Prevents polymerization of microtubules
Types of Receptors
24
Aspects of Drug Receptor Function
25
1.) Relationship between drug concentration (dose)
& pharmacologic response
2.) Signaling mechanisms and drug action
3.) Relationship between dose and clinical response
Relationship Between Dose & Response
26
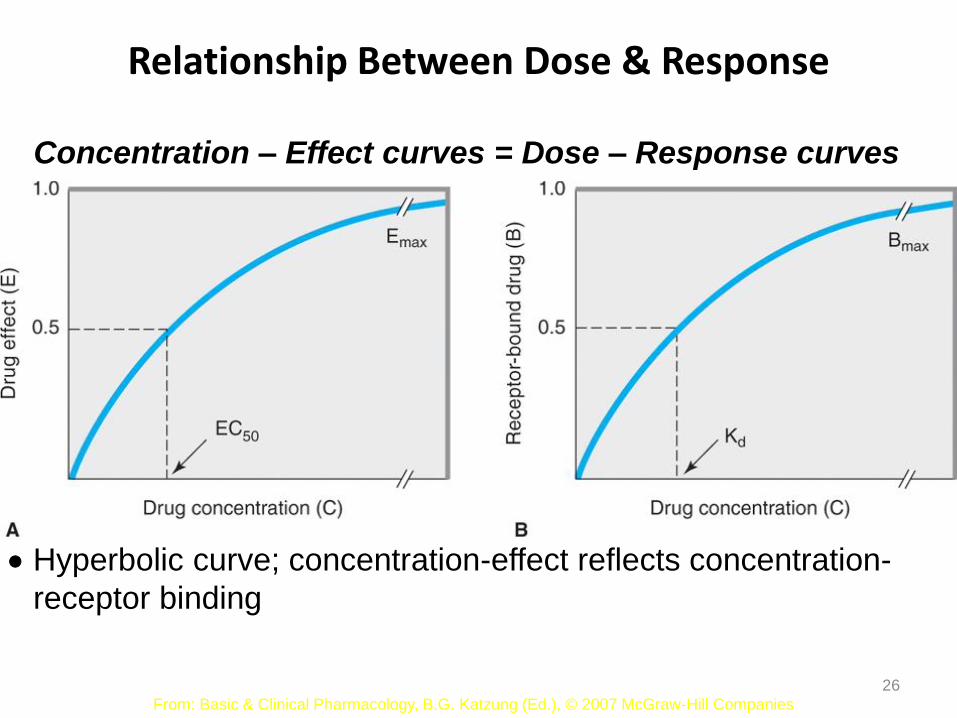
Concentration – Effect curves = Dose – Response curves
From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), © 2007 McGraw-Hill Companies
Hyperbolic curve; concentration-effect reflects concentration-
receptor binding
Occupation theory
Magnitude of pharmacological effect is proportional to percentage of
receptors occupied
27
Relationship Between Dose & Response
28
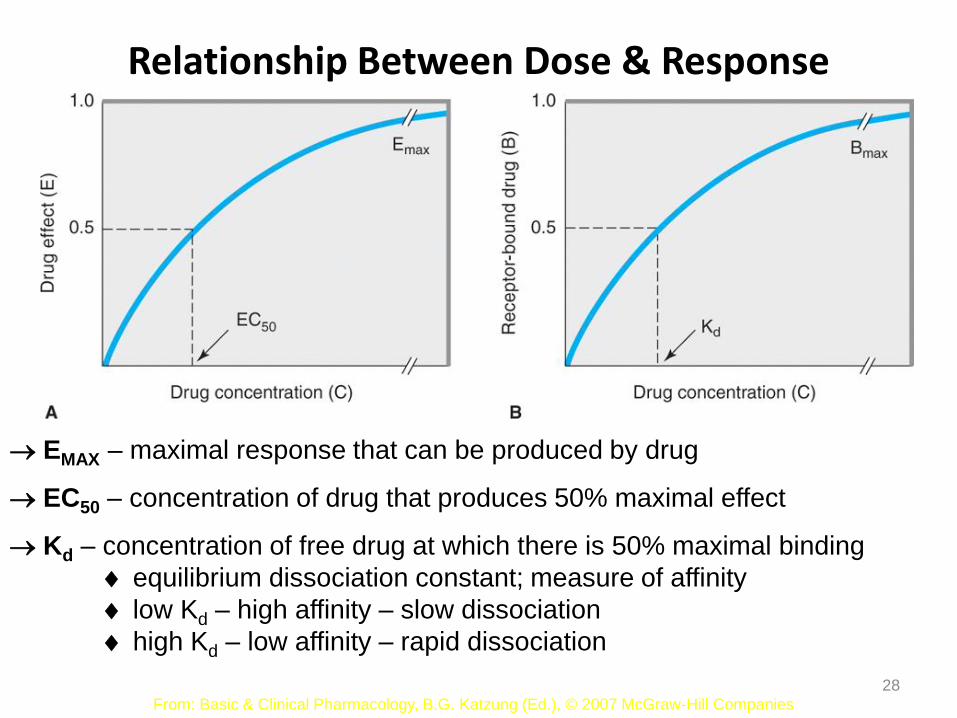
EMAX – maximal response that can be produced by drug
EC50 – concentration of drug that produces 50% maximal effect
Kd – concentration of free drug at which there is 50% maximal binding
equilibrium dissociation constant; measure of affinity
low Kd – high affinity – slow dissociation
high Kd – low affinity – rapid dissociation
From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), © 2007 McGraw-Hill Companies
Relationship Between Dose & Response
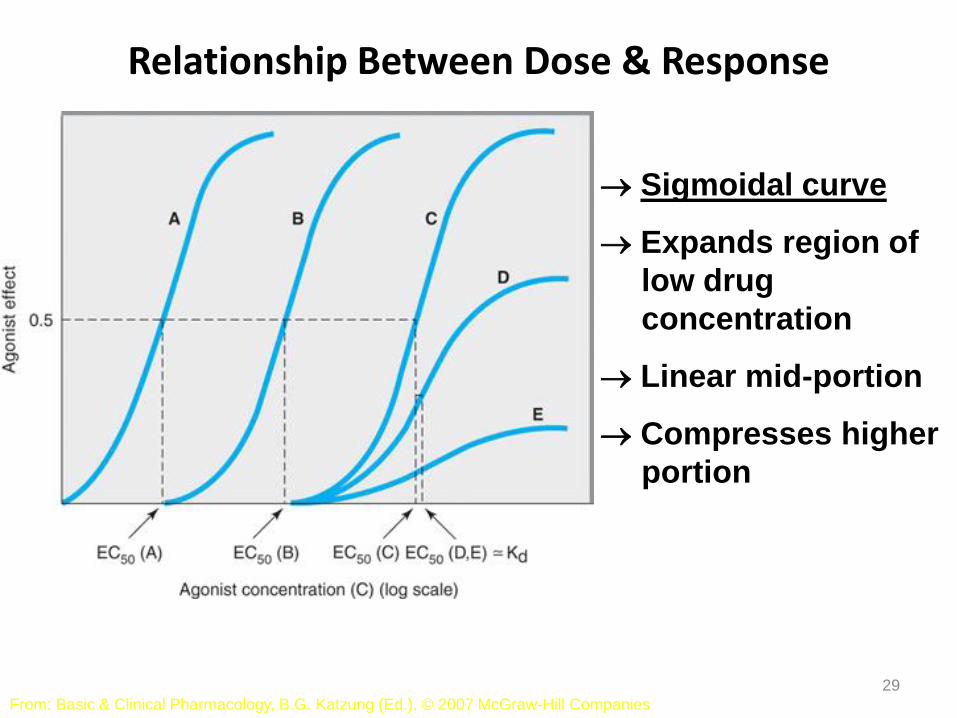
29
From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), © 2007 McGraw-Hill Companies
Sigmoidal curve
Expands region of
low drug
concentration
Linear mid-portion
Compresses higher
portion
Relationship Between Dose & Response
30
From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), © 2007 McGraw-Hill Companies
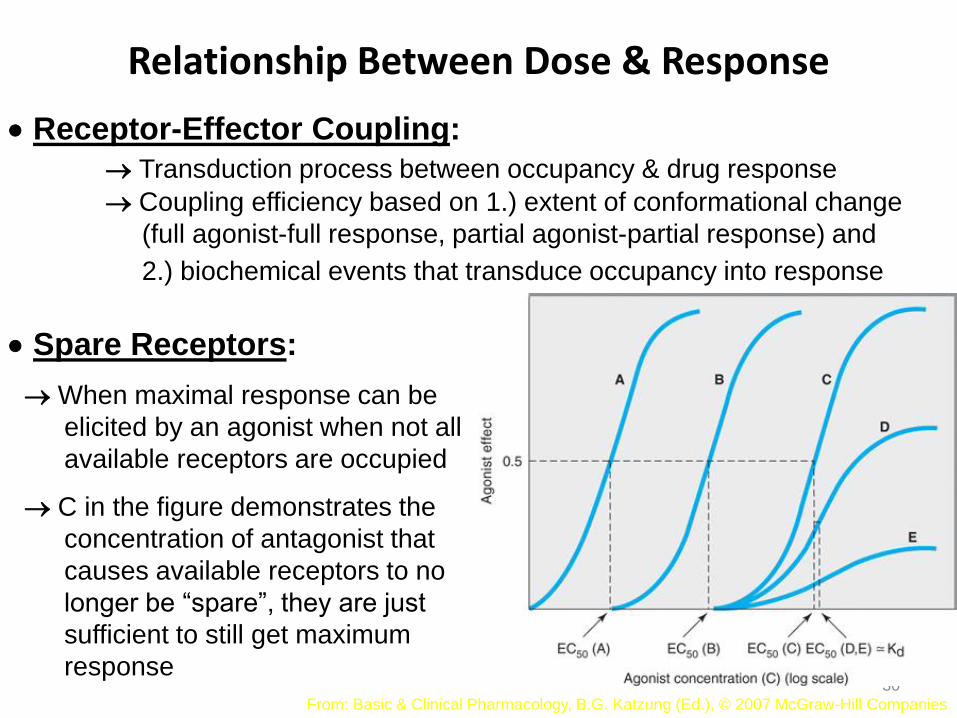
Receptor-Effector Coupling:
Transduction process between occupancy & drug response
Coupling efficiency based on 1.) extent of conformational change
(full agonist-full response, partial agonist-partial response) and
2.) biochemical events that transduce occupancy into response
Spare Receptors:
When maximal response can be
elicited by an agonist when not all
available receptors are occupied
C in the figure demonstrates the
concentration of antagonist that
causes available receptors to no
longer be “spare”, they are just
sufficient to still get maximum
response
Relationship Between Dose & Response
31
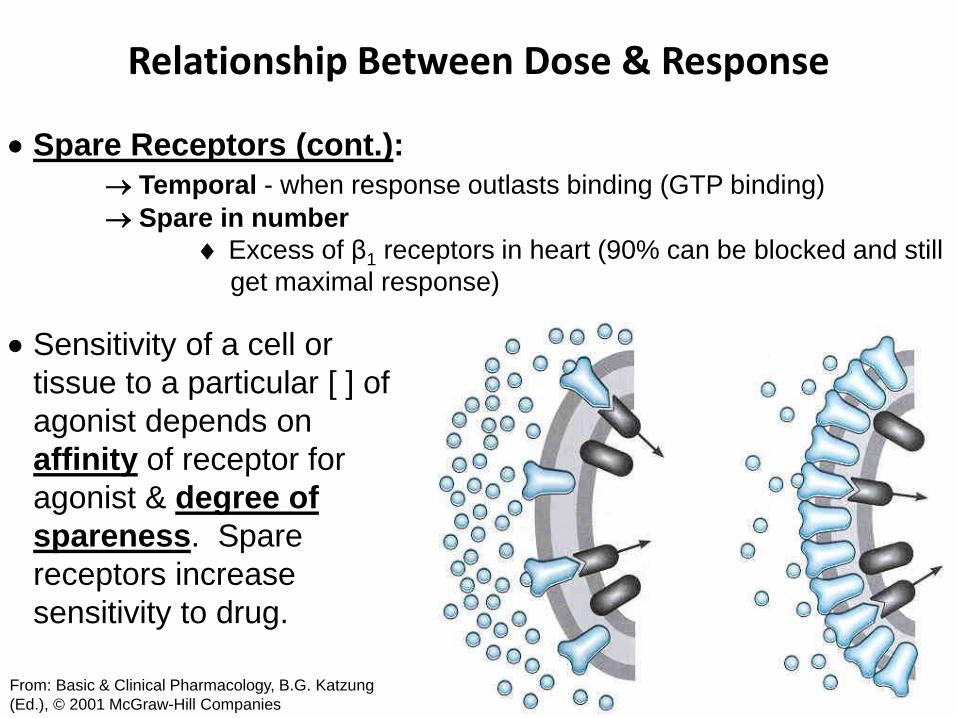
Spare Receptors (cont.):
Temporal - when response outlasts binding (GTP binding)
Spare in number
Excess of β1 receptors in heart (90% can be blocked and still
get maximal response)
From: Basic & Clinical Pharmacology, B.G. Katzung
(Ed.), © 2001 McGraw-Hill Companies
Sensitivity of a cell or
tissue to a particular [ ] of
agonist depends on
affinity of receptor for
agonist & degree of
spareness. Spare
receptors increase
sensitivity to drug.
Relationship Between Dose & Response
32 From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.),
© 2007 McGraw-Hill Companies
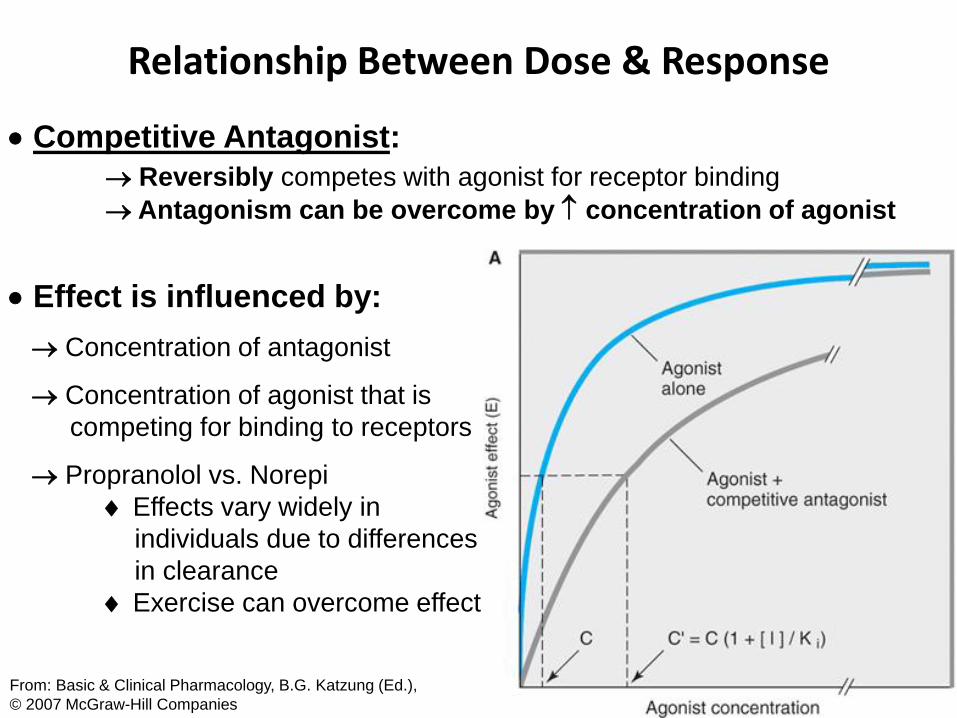
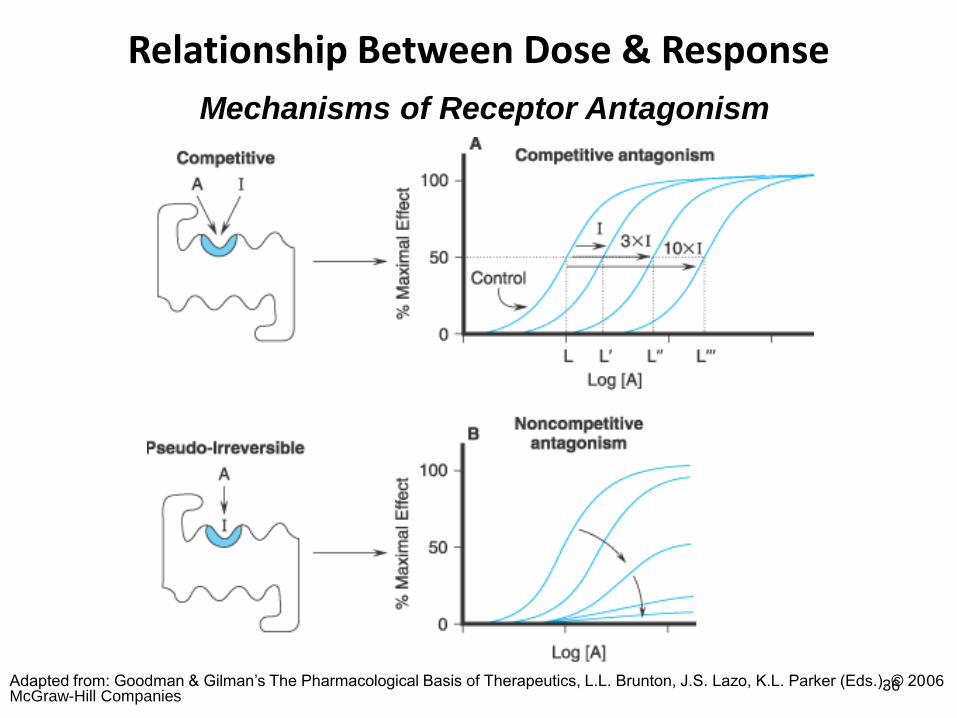
Competitive Antagonist:
Reversibly competes with agonist for receptor binding
Antagonism can be overcome by concentration of agonist
Effect is influenced by:
Concentration of antagonist
Concentration of agonist that is
competing for binding to receptors
Propranolol vs. Norepi
Effects vary widely in
individuals due to differences
in clearance
Exercise can overcome effect
Relationship Between Dose & Response
33 From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.),
© 2007 McGraw-Hill Companies
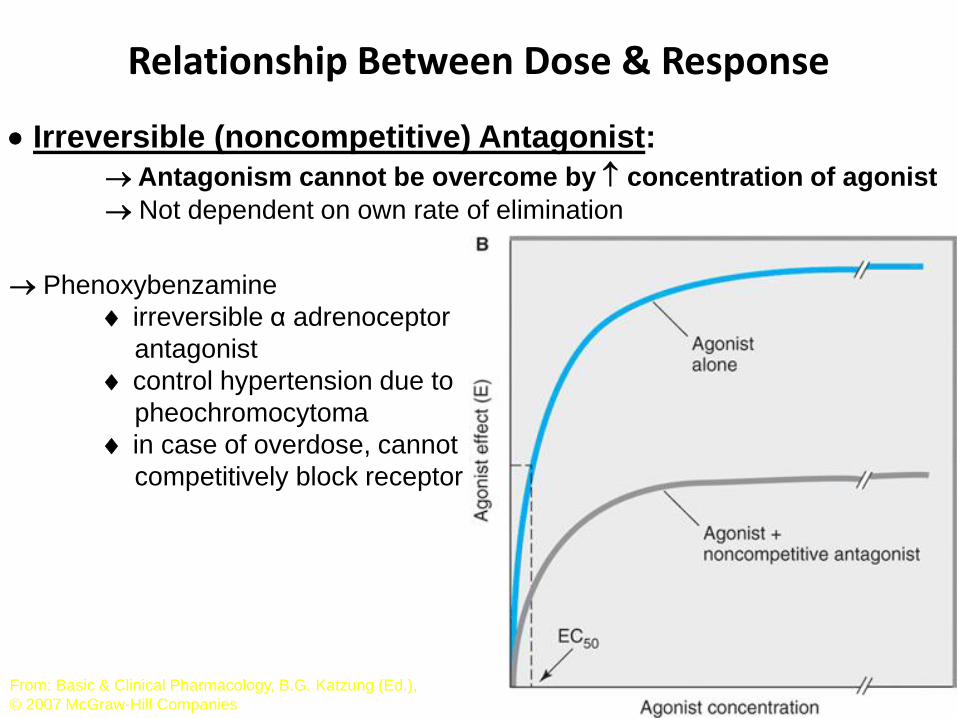
Irreversible (noncompetitive) Antagonist:
Antagonism cannot be overcome by concentration of agonist
Not dependent on own rate of elimination
Phenoxybenzamine
irreversible α adrenoceptor
antagonist
control hypertension due to
pheochromocytoma
in case of overdose, cannot
competitively block receptor
Relationship Between Dose & Response
34
From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), © 2007 McGraw-Hill Companies
Full agonist at
single
concentration
Full agonist at
single
concentration
Relationship Between Dose & Response
35
Allosteric Antagonist:
Binds to another part of the molecule
Chemical Antagonist:
A drug may bind to and inactivate another drug
Protamine used to counteract heparin
Desferrioxamine chelates iron
Physiological Antagonist:
One type of functional antagonism – agonists that oppose via action
on a different receptor or system
Use of a separate endogenous regulatory pathway
Glucocorticoids vs. insulin in controlling blood glucose
Effects are less specific & more difficult to control
Relationship Between Dose & Response
36
Mechanisms of Receptor Antagonism
Adapted from: Goodman & Gilman’s The Pharmacological Basis of Therapeutics, L.L. Brunton, J.S. Lazo, K.L. Parker (Eds.), © 2006 McGraw-Hill Companies
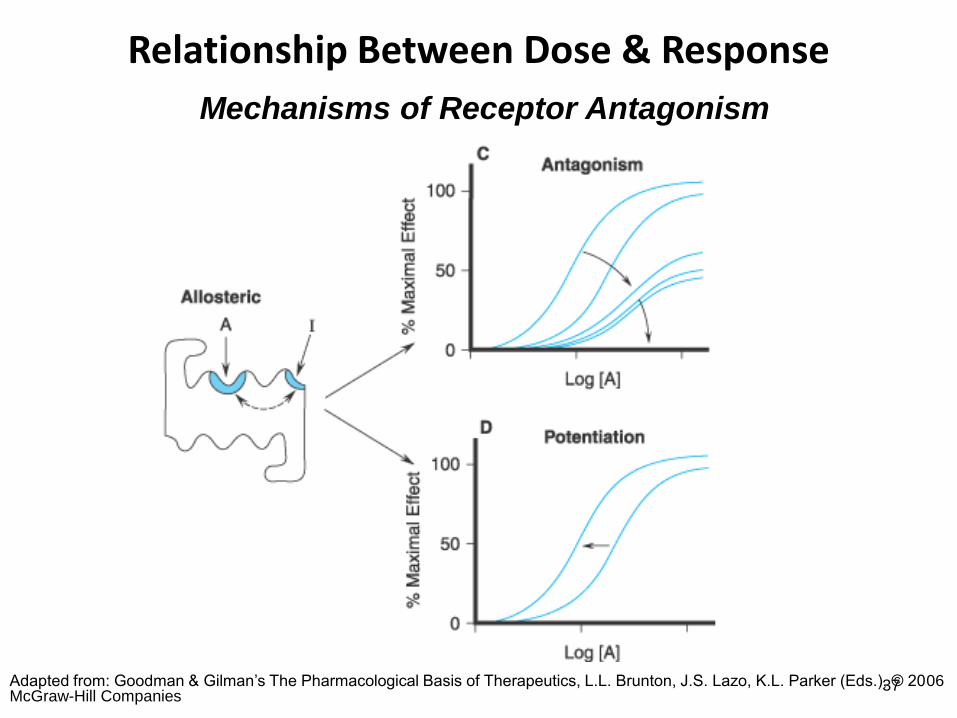
Relationship Between Dose & Response
37
Mechanisms of Receptor Antagonism
Adapted from: Goodman & Gilman’s The Pharmacological Basis of Therapeutics, L.L. Brunton, J.S. Lazo, K.L. Parker (Eds.), © 2006 McGraw-Hill Companies
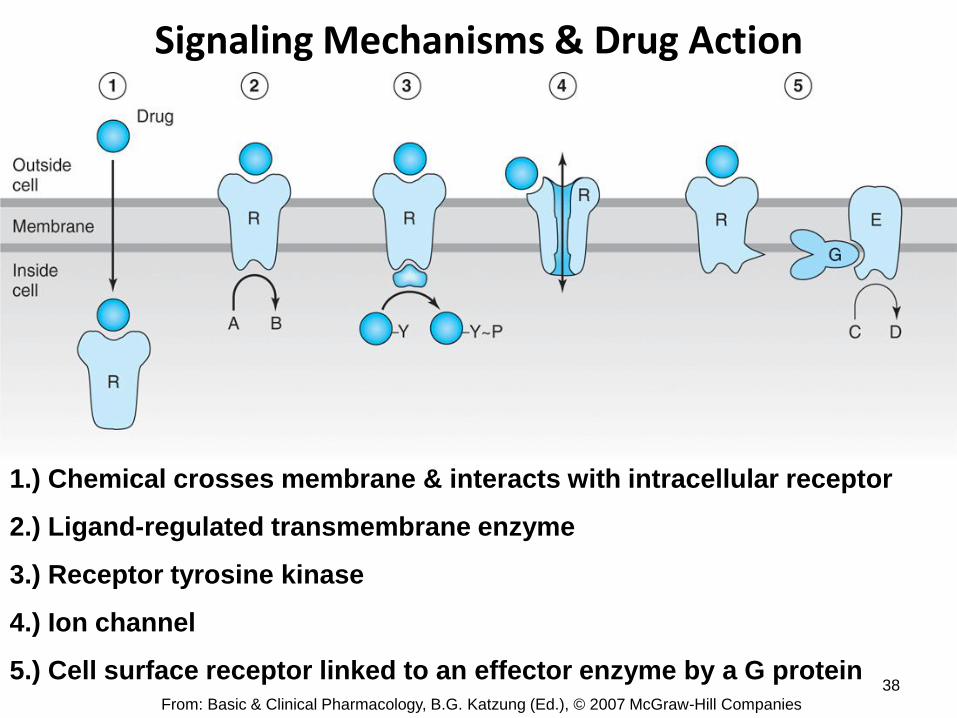
Signaling Mechanisms & Drug Action
38
1.) Chemical crosses membrane & interacts with intracellular receptor
2.) Ligand-regulated transmembrane enzyme
3.) Receptor tyrosine kinase
4.) Ion channel
5.) Cell surface receptor linked to an effector enzyme by a G protein From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), © 2007 McGraw-Hill Companies
Signaling Mechanisms & Drug Action
39 From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), © 2007
McGraw-Hill Companies
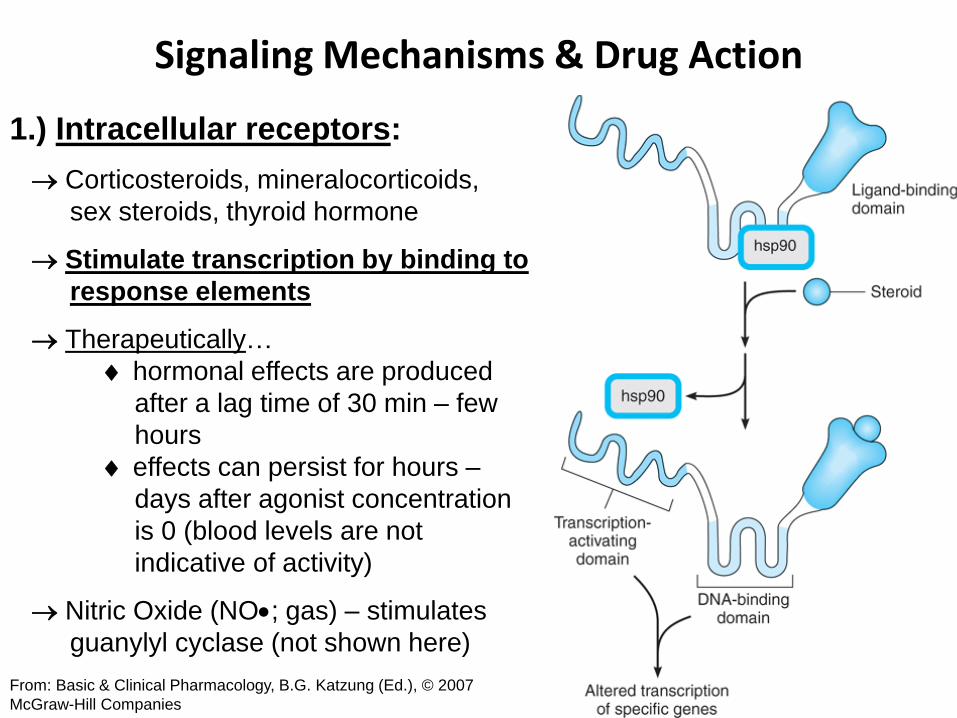
1.) Intracellular receptors:
Corticosteroids, mineralocorticoids,
sex steroids, thyroid hormone
Stimulate transcription by binding to
response elements
Therapeutically…
hormonal effects are produced
after a lag time of 30 min – few
hours
effects can persist for hours –
days after agonist concentration
is 0 (blood levels are not
indicative of activity)
Nitric Oxide (NO; gas) – stimulates
guanylyl cyclase (not shown here)
Signaling Mechanisms & Drug Action
40
2.) Ligand Regulatory Transmembrane Enzymes:
Ligand activates enzymatic activity of cytoplasmic domain
Similar to tyrosine kinases
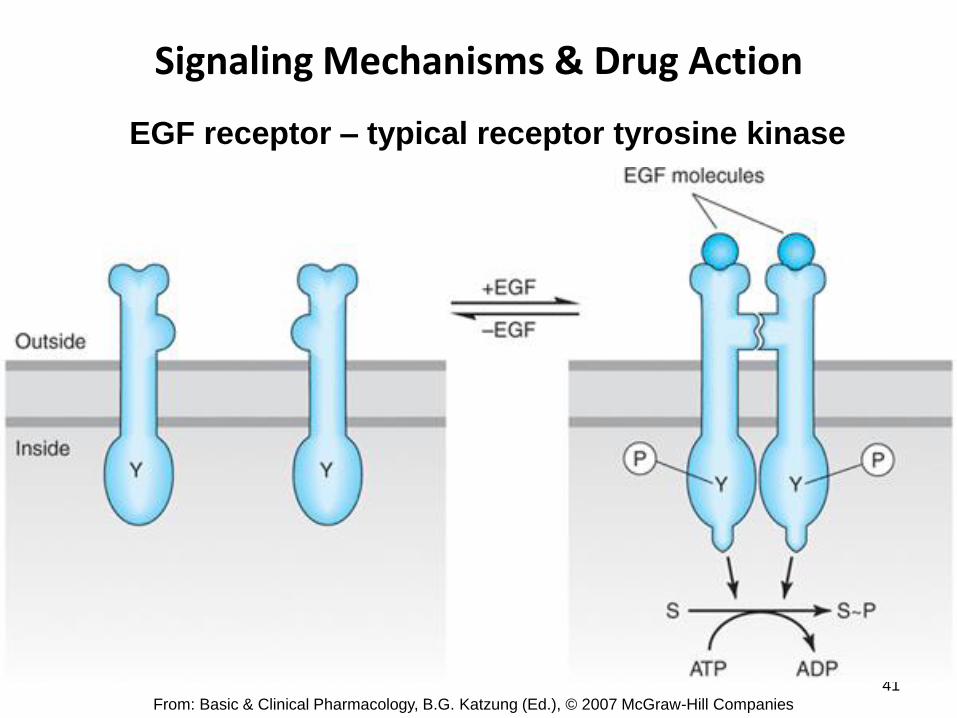
3.) Receptor Tyrosine Kinases:
Ligand activates enzymatic activity of bound protein tyrosine kinase
Insulin, epidermal growth factor (EGF), platelet-derived growth
factor (PDGF), atrial natriuretic peptide (ANP), transforming
growth factor- (TGF-)
Mechanism:
autophosphorylation
varied substrate phosphorylation
Activity outlasts receptor binding
Down-regulation
agonist continually binding to receptor causes increased
endocytosis of receptor
Site for drug action for growth factors, cancer
Signaling Mechanisms & Drug Action
41
From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), © 2007 McGraw-Hill Companies
EGF receptor – typical receptor tyrosine kinase
Signaling Mechanisms & Drug Action
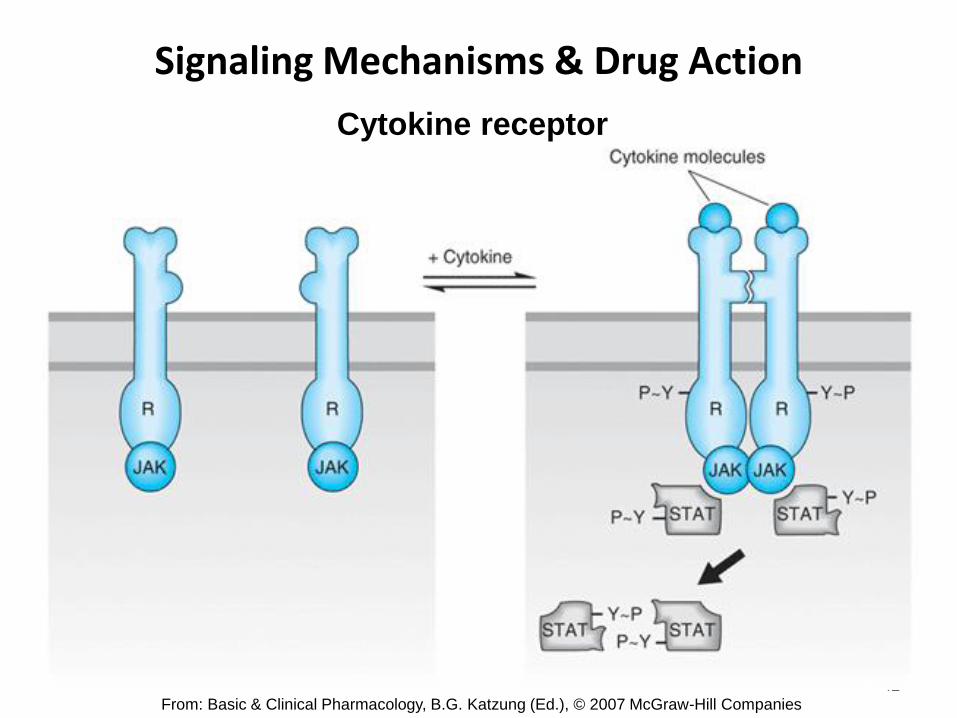
42
From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), © 2007 McGraw-Hill Companies
Cytokine receptor
Signaling Mechanisms & Drug Action
43 From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), © 2007
McGraw-Hill Companies
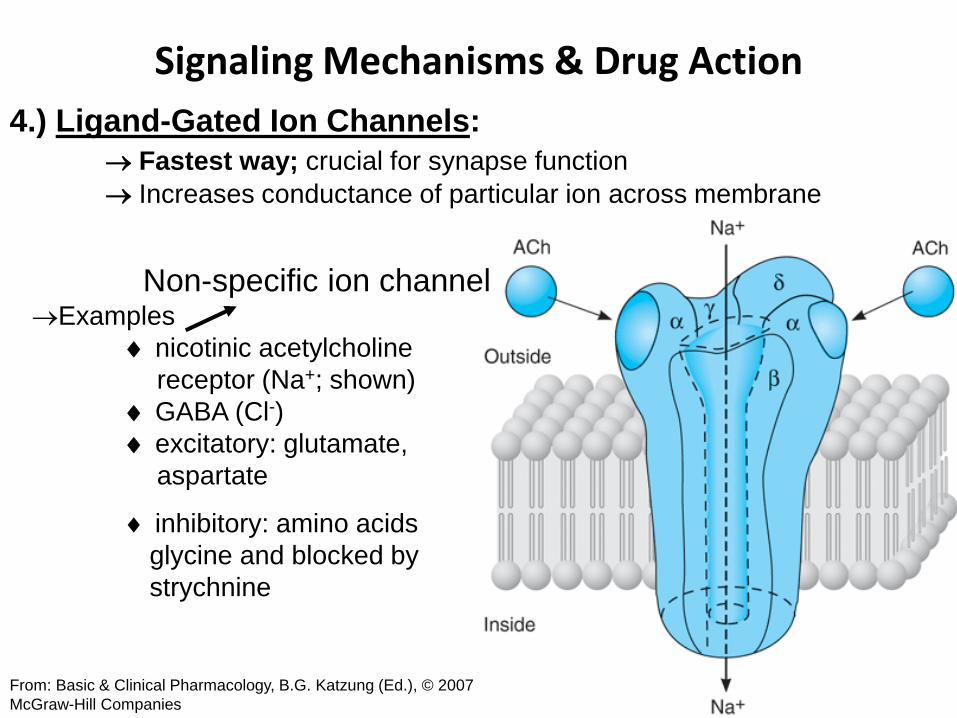
4.) Ligand-Gated Ion Channels:
Fastest way; crucial for synapse function
Increases conductance of particular ion across membrane
Examples
nicotinic acetylcholine
receptor (Na+; shown)
GABA (Cl-)
excitatory: glutamate,
aspartate
inhibitory: amino acids
glycine and blocked by
strychnine
Non-specific ion channel
Signaling Mechanisms &
Drug Action
44
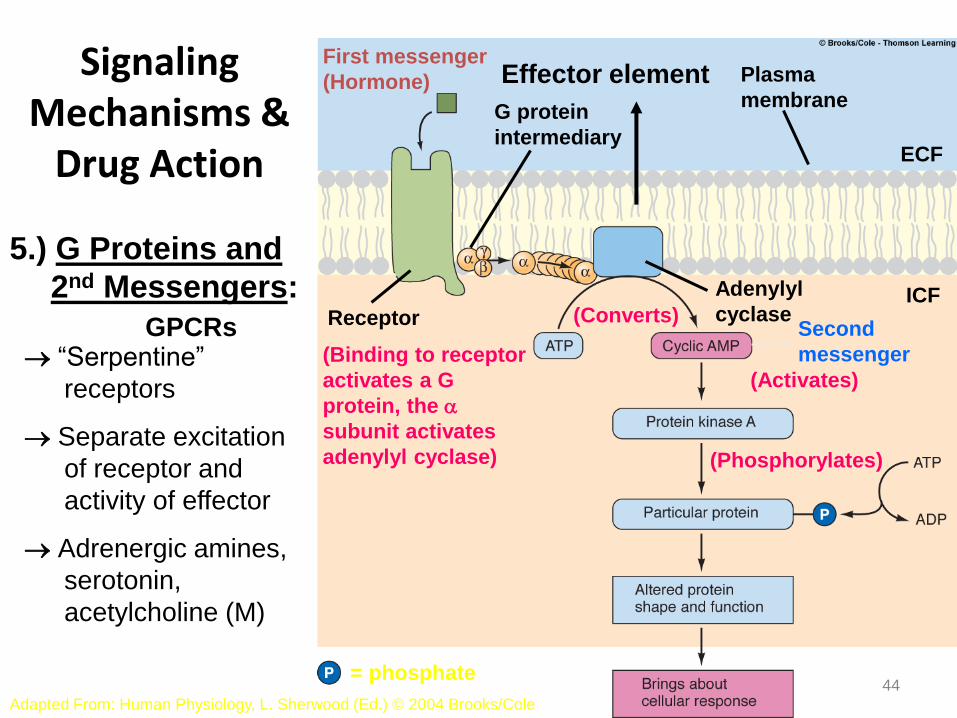
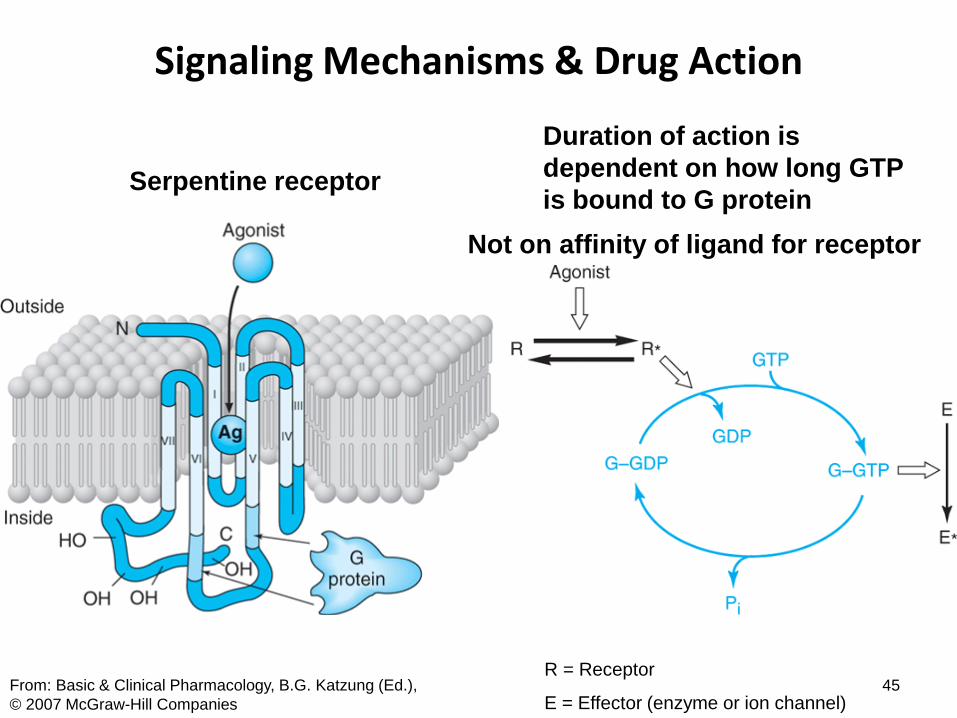
5.) G Proteins and
2nd Messengers:
“Serpentine”
receptors
Separate excitation
of receptor and
activity of effector
Adrenergic amines,
serotonin,
acetylcholine (M)
Adapted From: Human Physiology, L. Sherwood (Ed.) © 2004 Brooks/Cole
First messenger
(Hormone)
G protein
intermediary
Plasma
membrane
ECF
Receptor
(Binding to receptor
activates a G
protein, the a
subunit activates
adenylyl cyclase)
(Converts)
(Activates)
(Phosphorylates)
Second
messenger
= phosphate
ICF Adenylyl
cyclase GPCRs
Effector element
Signaling Mechanisms & Drug Action
45 From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.),
© 2007 McGraw-Hill Companies
Duration of action is
dependent on how long GTP
is bound to G protein
R = Receptor
E = Effector (enzyme or ion channel)
Serpentine receptor
Not on affinity of ligand for receptor
Signaling Mechanisms & Drug Action
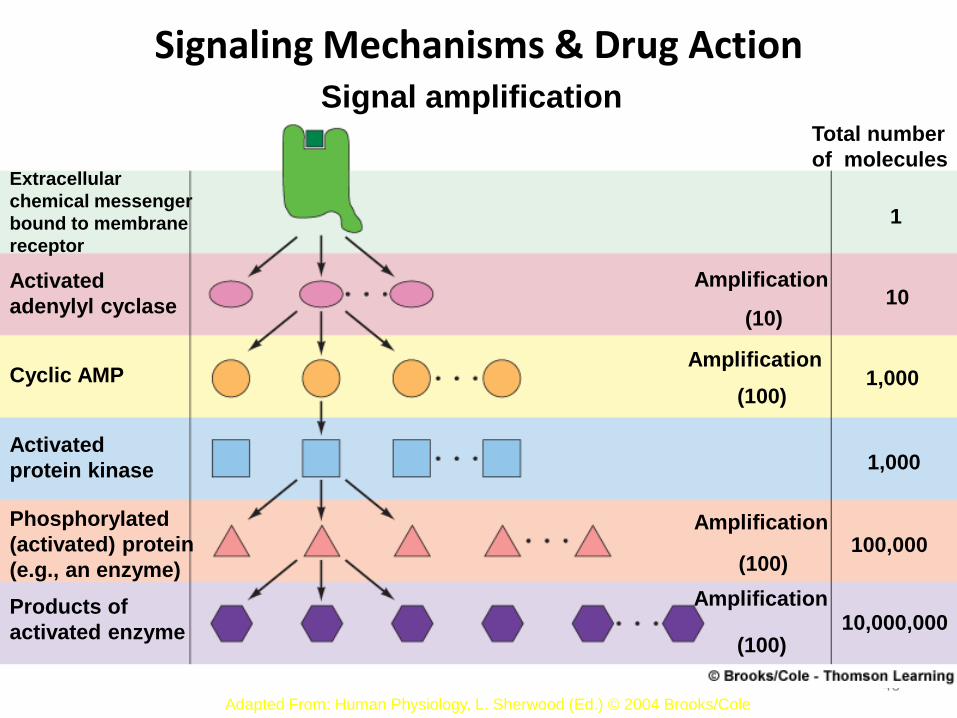
46 Adapted From: Human Physiology, L. Sherwood (Ed.) © 2001 Brooks/Cole
Signal amplification
Extracellular
chemical messenger
bound to membrane
receptor
Activated
adenylyl cyclase
Cyclic AMP
Activated
protein kinase
Phosphorylated
(activated) protein
(e.g., an enzyme)
Products of
activated enzyme
Amplification
(10)
(100)
Total number
of molecules
1,000
100,000
10,000,000
Amplification
Amplification
Amplification
(100)
(100)
1
10
1,000
Adapted From: Human Physiology, L. Sherwood (Ed.) © 2004 Brooks/Cole
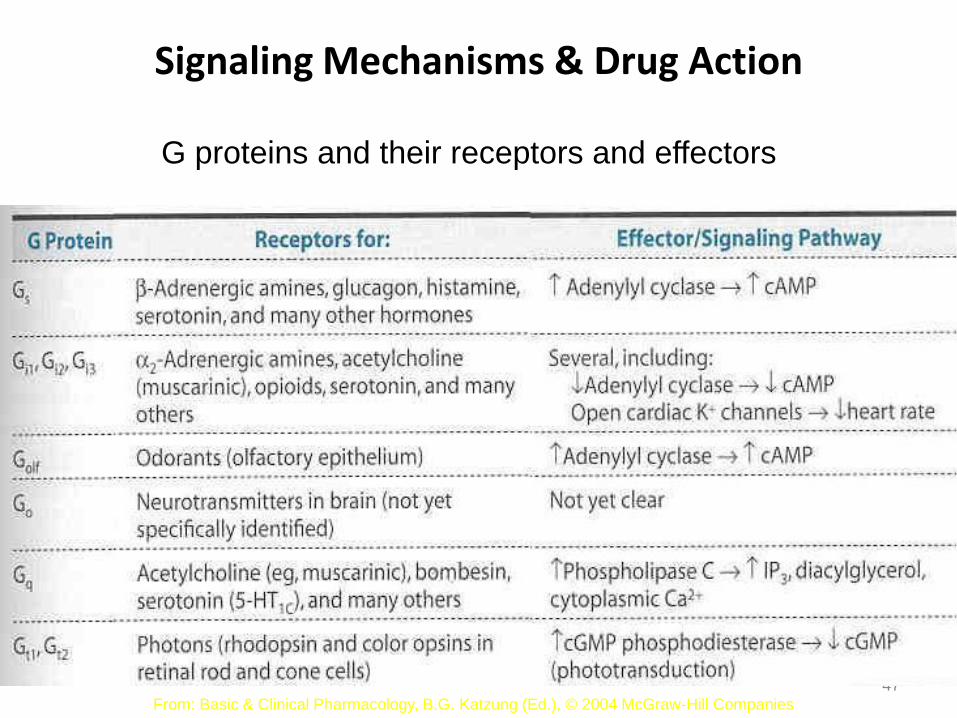
Signaling Mechanisms & Drug Action
47
From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), © 2004 McGraw-Hill Companies
G proteins and their receptors and effectors
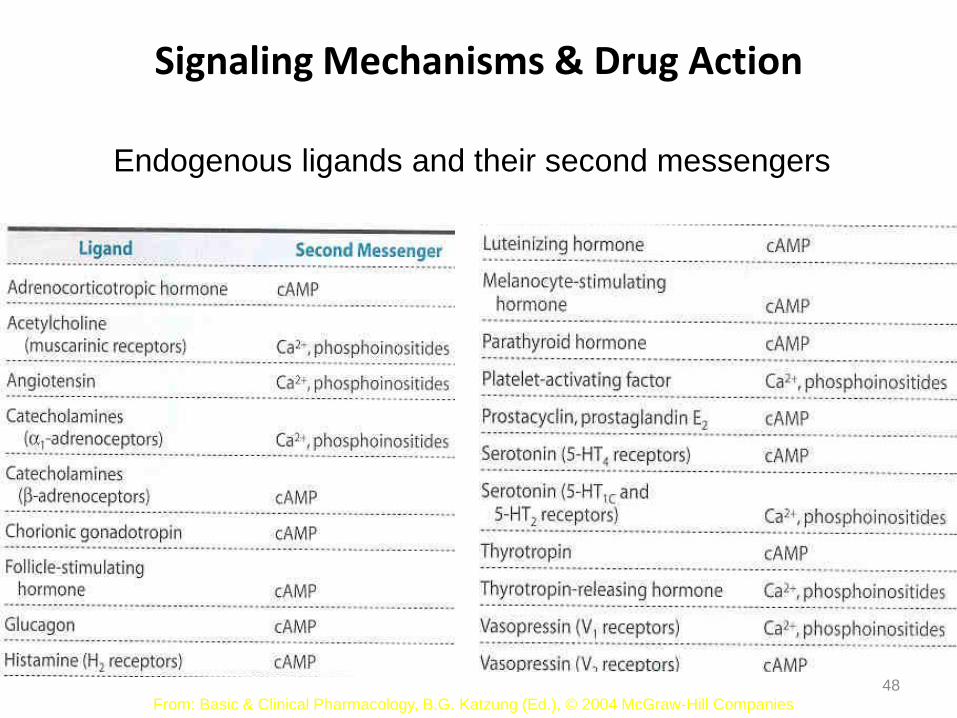
Signaling Mechanisms & Drug Action
48
From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), © 2004 McGraw-Hill Companies
Endogenous ligands and their second messengers
Signaling Mechanisms & Drug Action
49
Fro
m:
Ba
sic
& C
linic
al P
ha
rma
colo
gy,
B.G
. K
atz
un
g (
Ed
.), ©
20
07
McG
raw
-Hill
Co
.
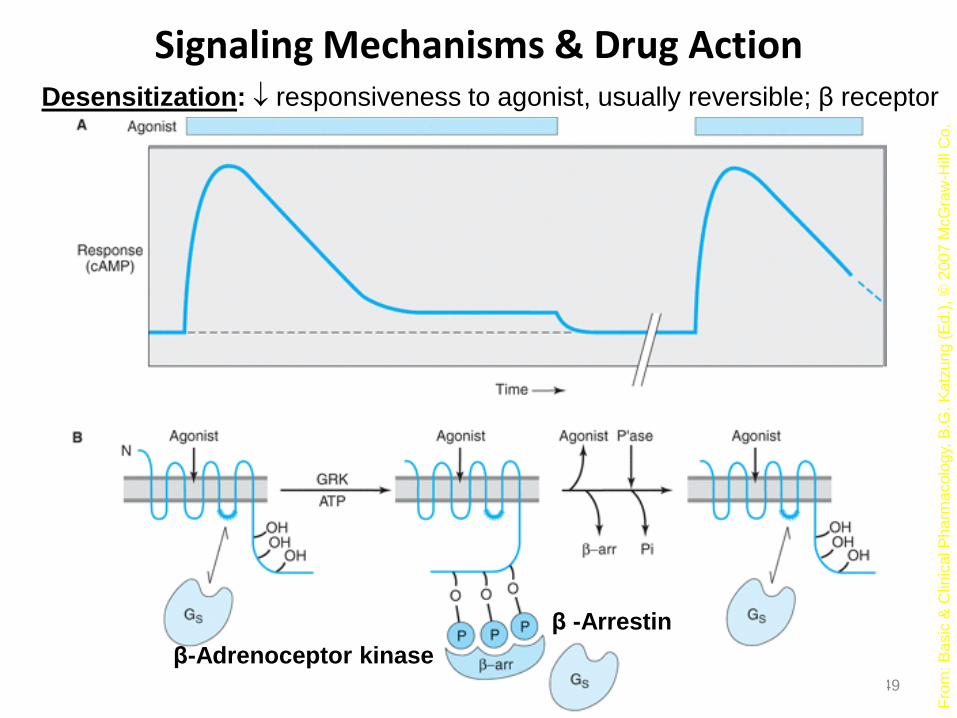
Desensitization: responsiveness to agonist, usually reversible; β receptor
β-Adrenoceptor kinase
β -Arrestin
Signaling Mechanisms & Drug Action
50
Fro
m:
Ba
sic
& C
linic
al P
ha
rma
colo
gy,
B.G
. K
atz
un
g (
Ed
.), ©
20
07
McG
raw
-Hill
Co
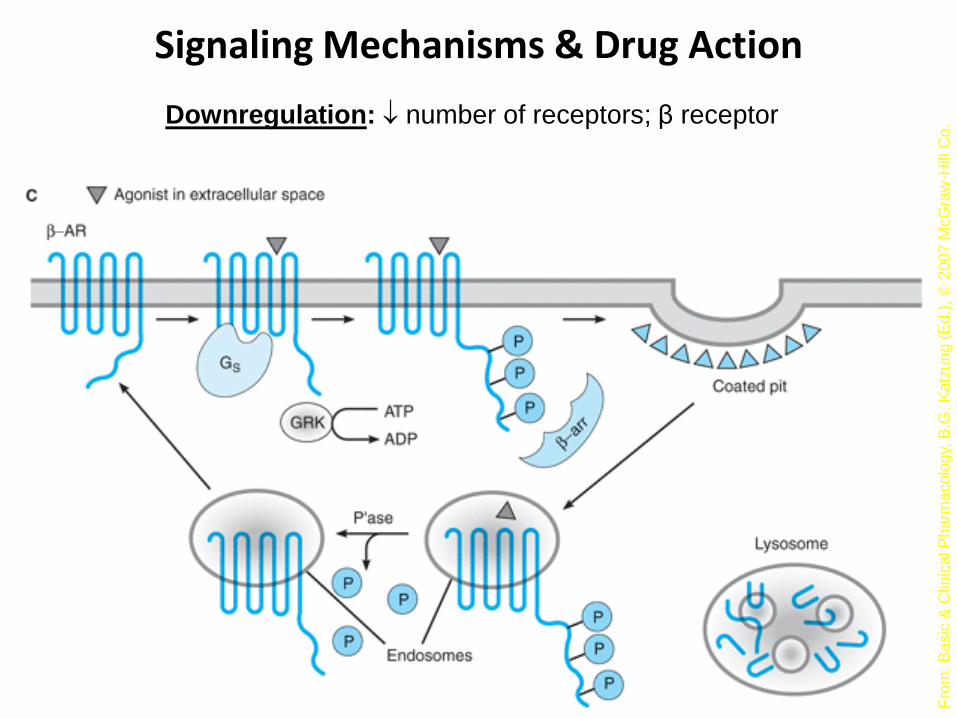
. Downregulation: number of receptors; β receptor
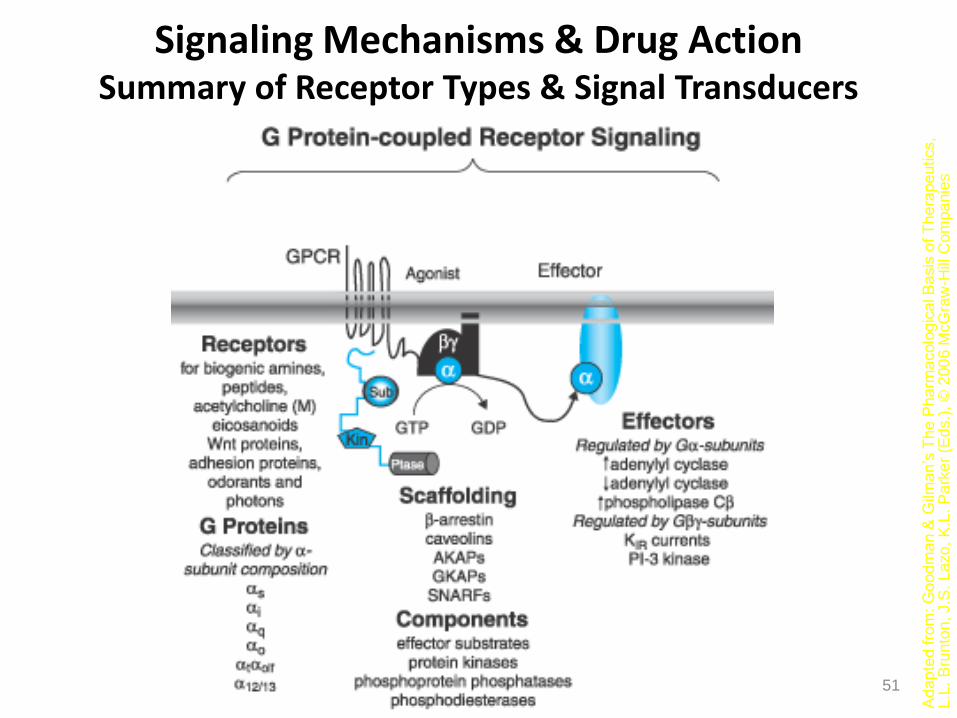
Signaling Mechanisms & Drug Action Summary of Receptor Types & Signal Transducers
51
Ad
ap
ted fro
m: G
oo
dm
an &
Gilm
an
’s T
he
Ph
arm
acolo
gic
al B
asis
of T
he
rape
utics,
L.L
. B
run
ton
, J.S
. L
azo
, K
.L. P
ark
er
(Ed
s.)
, ©
20
06
McG
raw
-Hill
Co
mp
anie
s
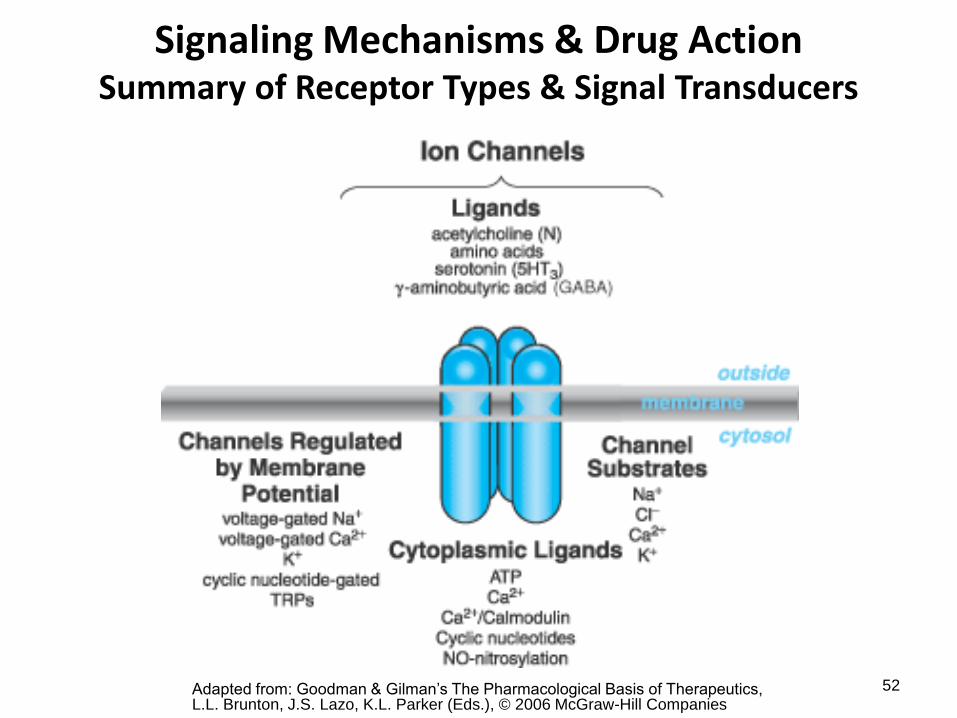
Signaling Mechanisms & Drug Action Summary of Receptor Types & Signal Transducers
52 Adapted from: Goodman & Gilman’s The Pharmacological Basis of Therapeutics, L.L. Brunton, J.S. Lazo, K.L. Parker (Eds.), © 2006 McGraw-Hill Companies
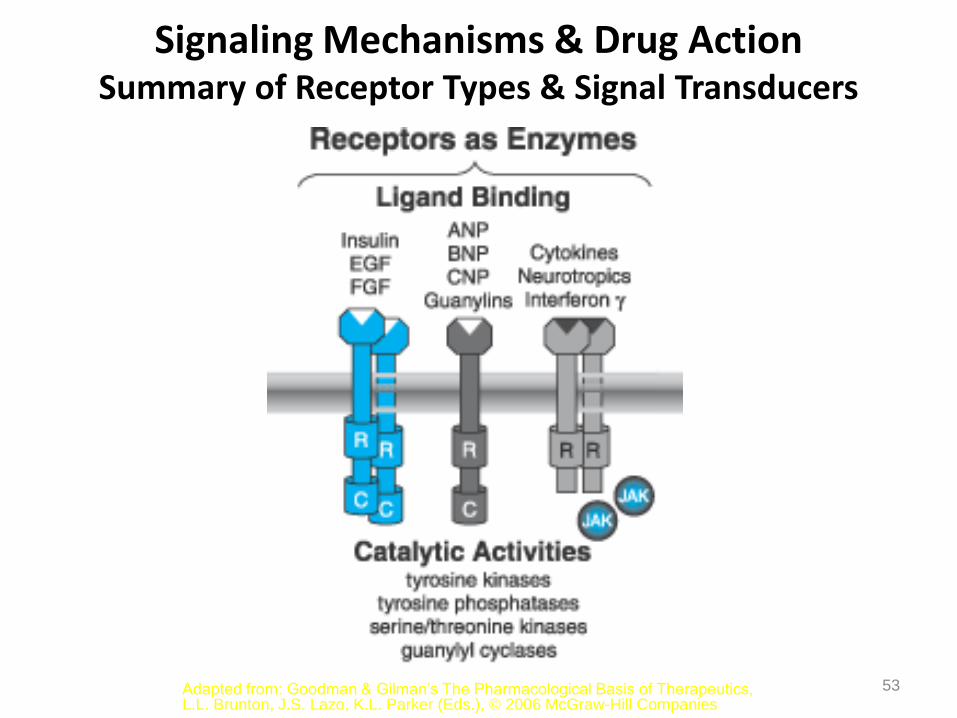
Signaling Mechanisms & Drug Action Summary of Receptor Types & Signal Transducers
53 Adapted from: Goodman & Gilman’s The Pharmacological Basis of Therapeutics, L.L. Brunton, J.S. Lazo, K.L. Parker (Eds.), © 2006 McGraw-Hill Companies
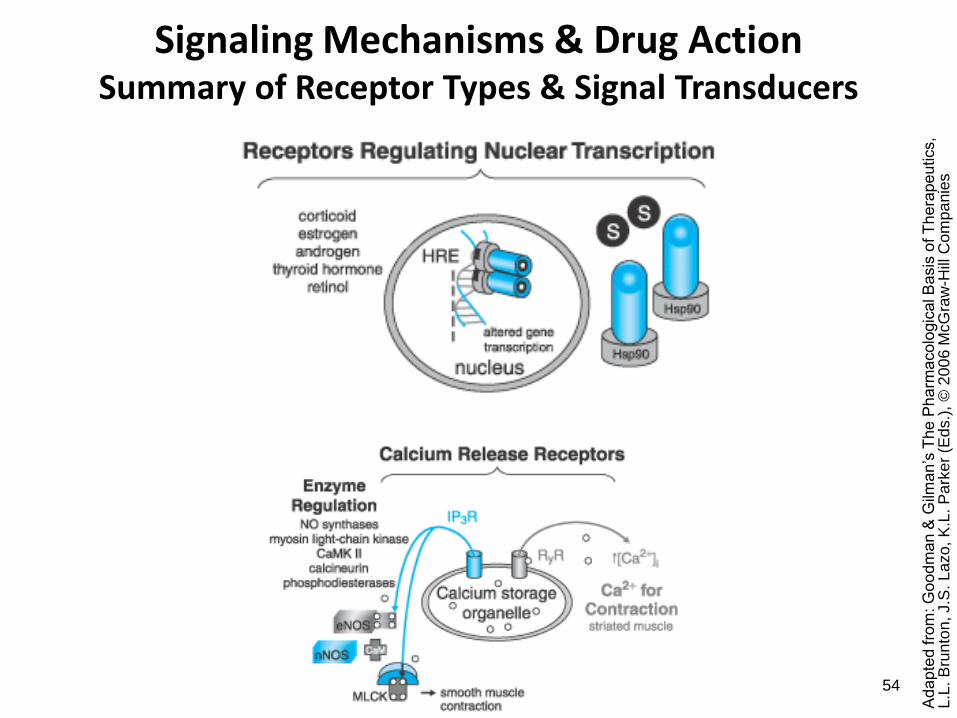
Signaling Mechanisms & Drug Action Summary of Receptor Types & Signal Transducers
54
Ad
ap
ted fro
m: G
oo
dm
an &
Gilm
an
’s T
he
Ph
arm
acolo
gic
al B
asis
of T
he
rape
utics,
L.L
. B
run
ton
, J.S
. L
azo
, K
.L. P
ark
er
(Ed
s.)
, ©
20
06
McG
raw
-Hill
Co
mp
anie
s
Signaling Mechanisms & Drug Action
55
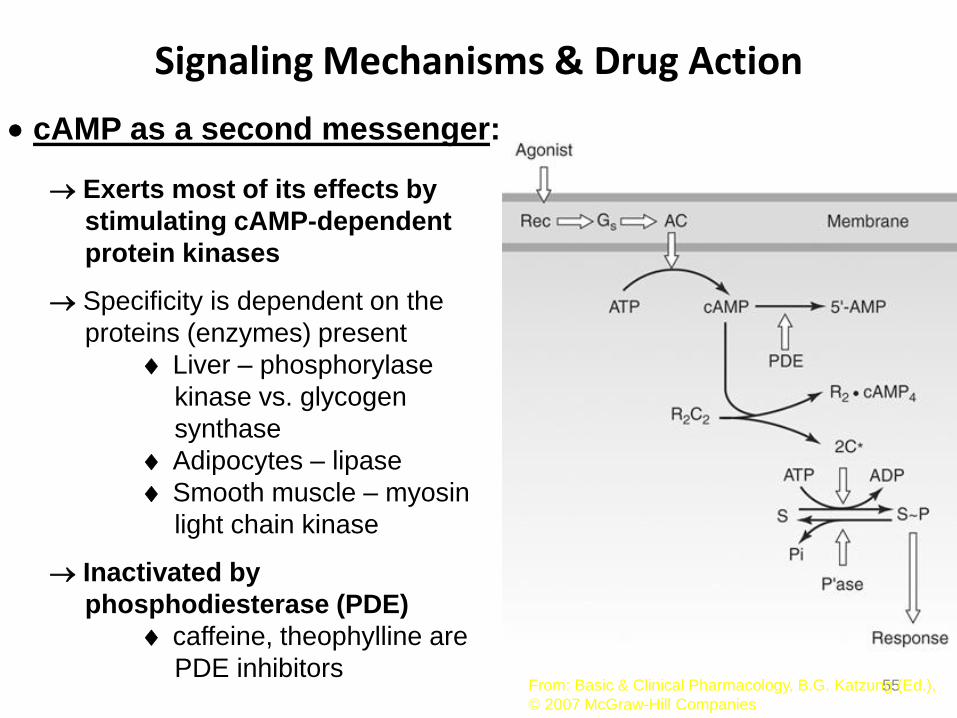
cAMP as a second messenger:
From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.),
© 2007 McGraw-Hill Companies
Exerts most of its effects by
stimulating cAMP-dependent
protein kinases
Specificity is dependent on the
proteins (enzymes) present
Liver – phosphorylase
kinase vs. glycogen
synthase
Adipocytes – lipase
Smooth muscle – myosin
light chain kinase
Inactivated by
phosphodiesterase (PDE)
caffeine, theophylline are
PDE inhibitors
Signaling Mechanisms & Drug Action
56
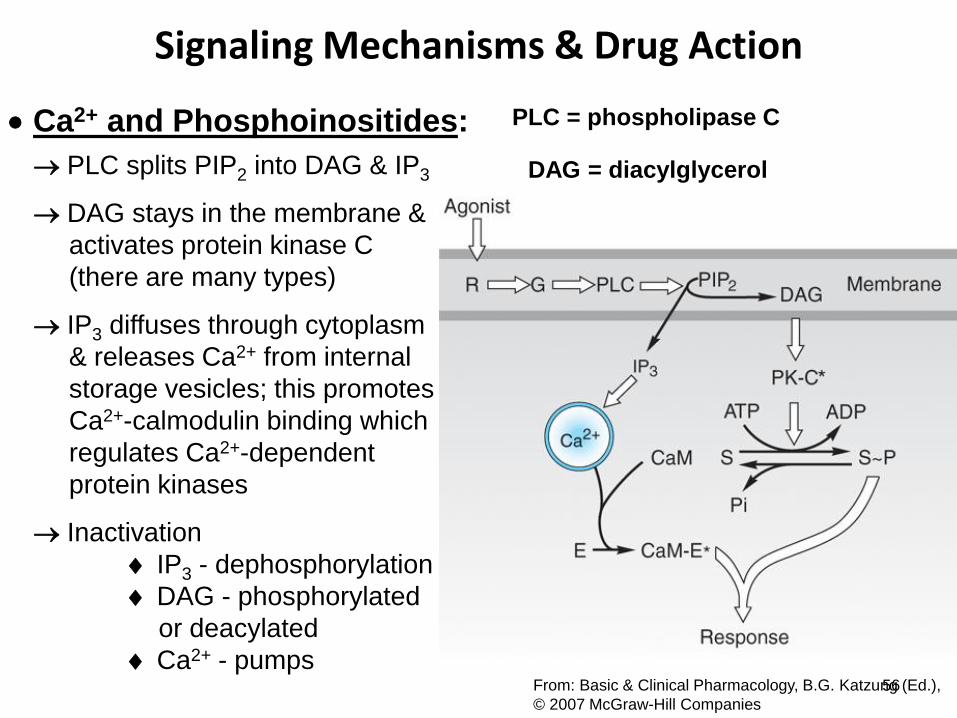
Ca2+ and Phosphoinositides:
From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.),
© 2007 McGraw-Hill Companies
PLC splits PIP2 into DAG & IP3
DAG stays in the membrane &
activates protein kinase C
(there are many types)
IP3 diffuses through cytoplasm
& releases Ca2+ from internal
storage vesicles; this promotes
Ca2+-calmodulin binding which
regulates Ca2+-dependent
protein kinases
Inactivation
IP3 - dephosphorylation
DAG - phosphorylated
or deacylated
Ca2+ - pumps
PLC = phospholipase C
DAG = diacylglycerol
Signaling Mechanisms & Drug Action
57 From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), ©
2007 McGraw-Hill Companies
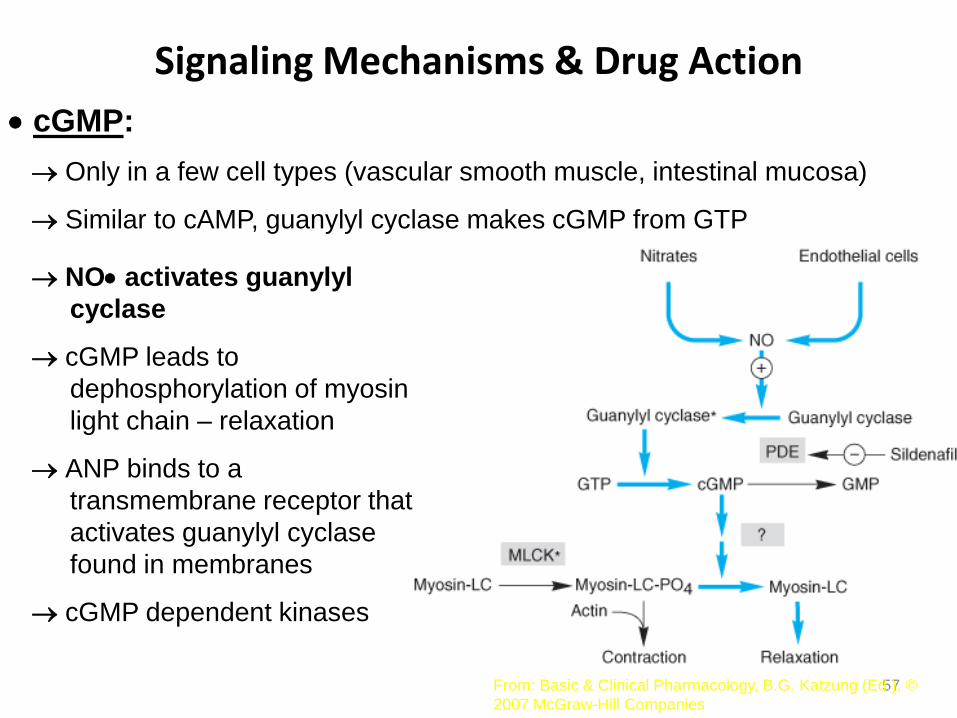
cGMP:
Only in a few cell types (vascular smooth muscle, intestinal mucosa)
Similar to cAMP, guanylyl cyclase makes cGMP from GTP
NO activates guanylyl
cyclase
cGMP leads to
dephosphorylation of myosin
light chain – relaxation
ANP binds to a
transmembrane receptor that
activates guanylyl cyclase
found in membranes
cGMP dependent kinases
Signaling Mechanisms & Drug Action
58
Phosphorylation:
Reversible
Amplification: records a molecular memory of the pathway that
has been activated, dephosphorylation erases
the memory
Flexible regulation: differing substrate specificities of the
multiple protein kinases regulated by 2nd
messengers provide branch points that
may be independently regulated
Receptor classes & drug development:
Structure activity relationships give clues about drug receptors
Limited number of regulatory molecules
Overall effects are due to receptors
Diversity of receptors allows for selectivity of drugs
Relationship Between Dose & Clinical Response
59
Maximal benefit with minimal toxicity
Graded dose-response relationship:
Potency – EC50 or ED50 (dose needed for 50% of drug’s effect)
dependent on affinity (Kd) and
efficiency of coupling response
Maximal efficacy – limit of the dose-response relationship;
important for clinical effectiveness
dependent on ability to reach relevant receptors
route of administration, absorption, site of action
Relationship Between Dose & Clinical Response
60 From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), ©
2007 McGraw-Hill Companies
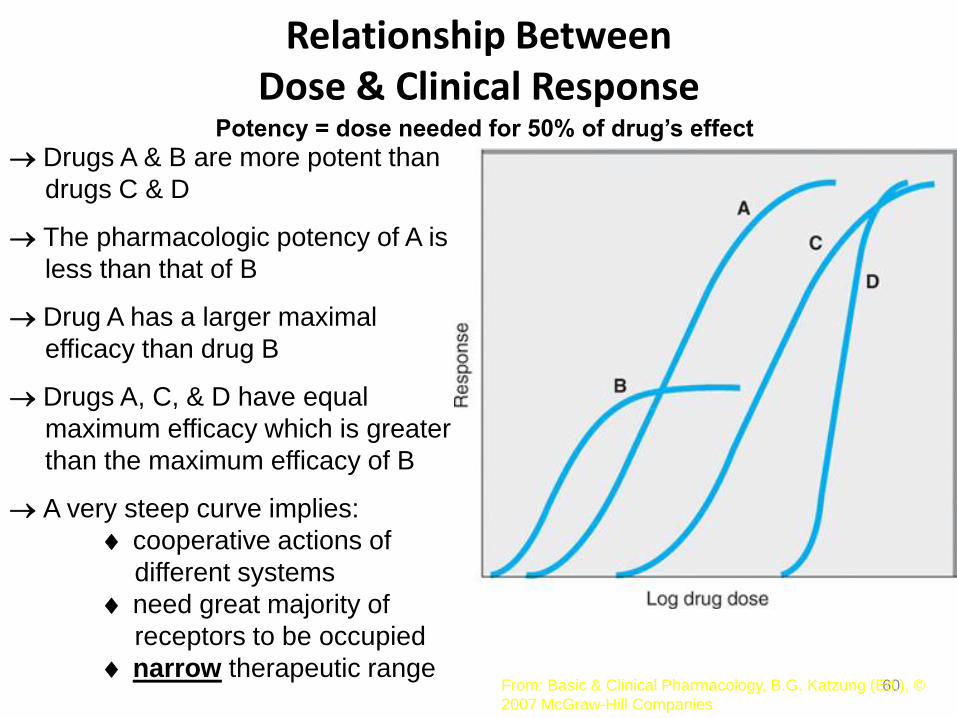
Drugs A & B are more potent than
drugs C & D
The pharmacologic potency of A is
less than that of B
Drug A has a larger maximal
efficacy than drug B
Drugs A, C, & D have equal
maximum efficacy which is greater
than the maximum efficacy of B
A very steep curve implies:
cooperative actions of
different systems
need great majority of
receptors to be occupied
narrow therapeutic range
Potency = dose needed for 50% of drug’s effect
Relationship Between Dose & Clinical Response
61
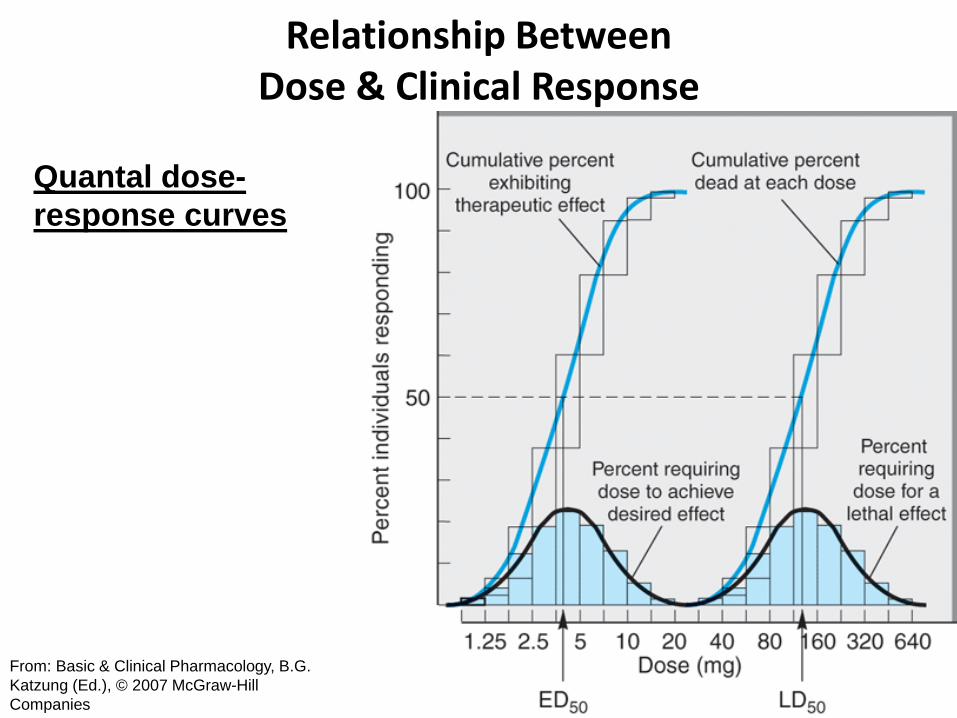
Quantal dose-response curves:
All or none
Determine the dose required to produce an effect in a large number
of individual patients and plotting the cumulative frequency
distribution
ED50 - dose at which 50% of individuals respond (different than
ED50 defined above)
TD50 - dose required to produce a toxic effect in 50% of individuals
(LD50 if death is endpoint)
Therapeutic index – TD50 / ED50
Digoxin – narrow
Benzodiazepines and antipsychotics - wide
The clinically acceptable risk of toxicity depends
critically on the severity of the disease being
treated.
Relationship Between Dose & Clinical Response
62
From: Basic & Clinical Pharmacology, B.G.
Katzung (Ed.), © 2007 McGraw-Hill
Companies
Quantal dose-
response curves
Relationship Between Dose & Clinical Response
63
Variation in drug responsiveness:
Clinical response in individual patients
Idiosyncratic – infrequently observed in most patients
genetic differences in metabolism
immunological differences
Hypersensitivity – true allergy (uncommon)
Hyperreactive – intensity of effect is increased vs. that in most
individuals
Hyporeactive – intensity of effect is decreased vs. that in most
individuals
Tolerance – responsiveness decreases as a consequence of
continued drug administration
Tachyphylaxis – decreased responsiveness that occurs rapidly
after administration of a drug
Relationship Between Dose & Clinical Response
64
Four mechanisms contribute to
variation in drug responsiveness
1.) Alteration in concentration of drug that reaches receptor
2.) Variation in concentration of endogenous receptor ligand
3.) Alteration in number or function of receptors
Up-regulation (thyroid hormone increases receptors in heart;
antagonists like -blockers also do this)
stop antagonist – increase in receptor number - response
to endogenous ligand (need to wean)
Down-regulation
stop agonist – may have too few receptors to get
effective stimulation
2.) Variation in concentration of endogenous receptor ligand
• Saralasin – weak partial agonist at angiotensin II
• Angiotensin II is a potent vasoconstrictor – What would be its effect on blood pressure up or down?
• What would be the effect on blood pressure of giving saralasin to a patient with high levels of angiotensin?
• What would be the effect on blood pressure of giving saralasin to a patient with low levels of angiotensin?
65
Relationship Between Dose & Clinical Response
66
Pharmacogenetics: identification of genetic factors that contribute
to a particular drug response; may allow the
design of the most appropriate individualized
pharmacologic therapy for patients
4.) Change in responsiveness distal to receptor
Largest and most important class of mechanisms that cause
variation in responsiveness to drug therapy
Age
General health
Severity & pathophysiology of disease
Wrong diagnosis
Compensatory mechanisms – (baroreceptor reflex after
administration of an anti-hypertensive agent)
Relationship Between Dose & Clinical Response
67
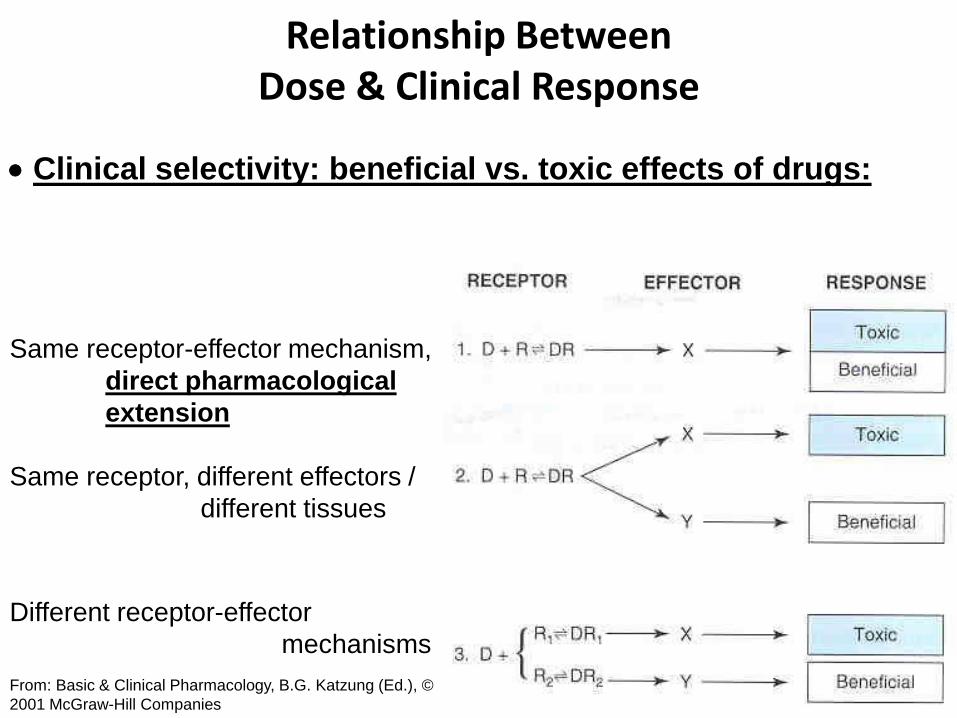
Clinical selectivity: beneficial vs. toxic effects of drugs:
From: Basic & Clinical Pharmacology, B.G. Katzung (Ed.), ©
2001 McGraw-Hill Companies
Same receptor-effector mechanism,
direct pharmacological
extension
Same receptor, different effectors /
different tissues
Different receptor-effector
mechanisms
Relationship Between Dose & Clinical Response
68
Strategies for lowering adverse effects:
Use lowest dose possible
Add an adjunctive drug that acts on a different receptor mechanism
Anatomical selectivity – refine administration to get more drug to site
of action
No drug causes only a single, specific effect
69
Drugs are only selective, not specific
70