integrated pet/ct in differentiated thyroid cancer: diagnostic accuracy and impact on patient...
TRANSCRIPT

Integrated PET/CT in Differentiated Thyroid Cancer: Diagnostic
Accuracy and Impact on Patient Management
J Nucl Med 2006; 47:616–624
報告者 : 蘇惠怡

IntroductionIntroduction Differentiated thyroid cancer (DTC): occur
s in 3–5 per 100,000 people and represents about 1% of all malignant tumors
most cases : prognosis is favorable treatment consisting of primary surgery and ablative radioiodine administration achieves a 10-y survival rate of 80%–90% .

IntroductionIntroduction special subgroups : less favorable with m
uch lower survival rates. Risk factors :
(1) age > 45 y, (2) histopathologic grading, (3) poor radioiodine accumulation . Those patients without sufficient radioiodine uptake in the tumor cells have a significantly lower survival rate if distant metastases are present .

IntroductionIntroduction
Patients with DTC may have only iodine-negative tumor lesions or both iodine-negative and iodine-positive tumor tissue . →” the presence of iodine-negative tumor tissue decreases the accuracy of iodine scintigraphy “

IntroductionIntroduction
tumor tissue is not detected by iodine scintigraphy and will remain without further treatment
For the treatment of iodine-negative tumor tissue, surgery is the only curative therapy option. Exact localization of 18F-FDG tumor foci is mandatory for successful resection of cancer in these cases.

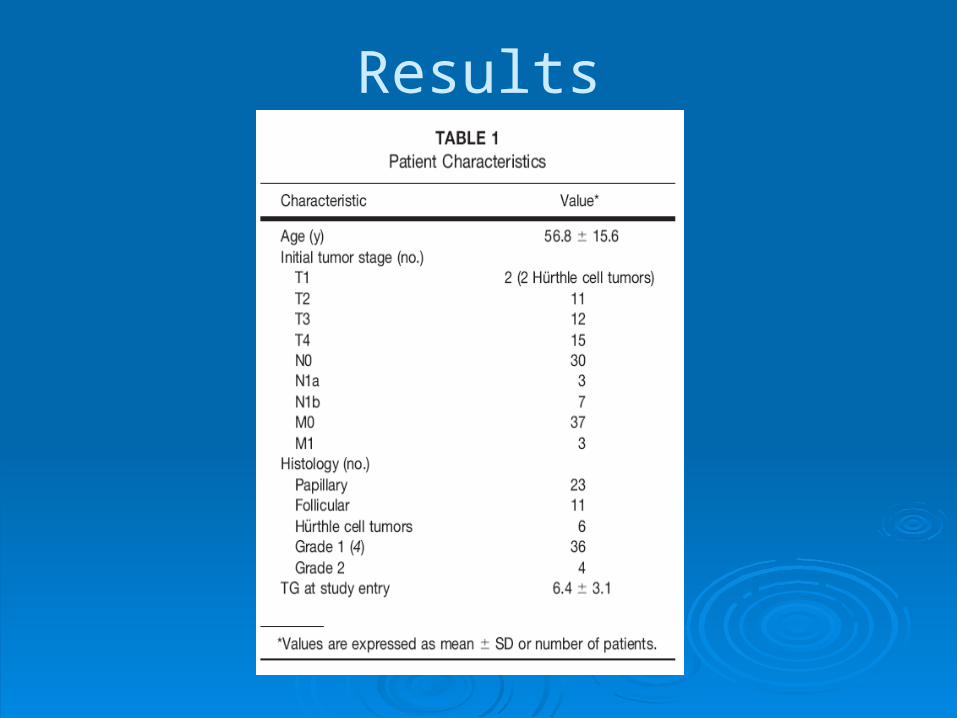
Materials and Methods 40 patients : (1)
elevated TG level in the euthyroid (2)the hypothyroid state or (3)morphologically suspected tumor disease (sonography, CT, MRI),
(1)L-thyroxin withdrawal for 4 wk before 131I whole-body scintigraphy, (2)low-iodine diet during this period, (3)thyroid-stimulating hormone increase of >30 mU/L

Materials and Methods Exclusion criteria : (1)positiv
e test for TG antibodies, (2)administration of CT contrast medium within the previous 6 mo, (3)positive iodine urine test performed on the day of scintigraphy, (4)pregnancy, (5)age <18 y.

Materials and Methods
(1)fasted at least 4 h before injection of 370 MBq 18F-FDG. (2)Blood glucose : <150 mg/dL (8.3 mmol/L). (3)Intravenous contrast agent: not administered. (4)the supine position with arms elevated, (5)CT scanning was started at the level of the cervicothoracic region
Scanning was started 60–90 min after the injection .

Materials and Methods
5-point scale was used: 0 : the lesion was normal; 1 : the lesion was probably normal; 2 : the lesion was equivocal; 3 : the lesion was probably abnormal; 4 : the lesion was abnormal.

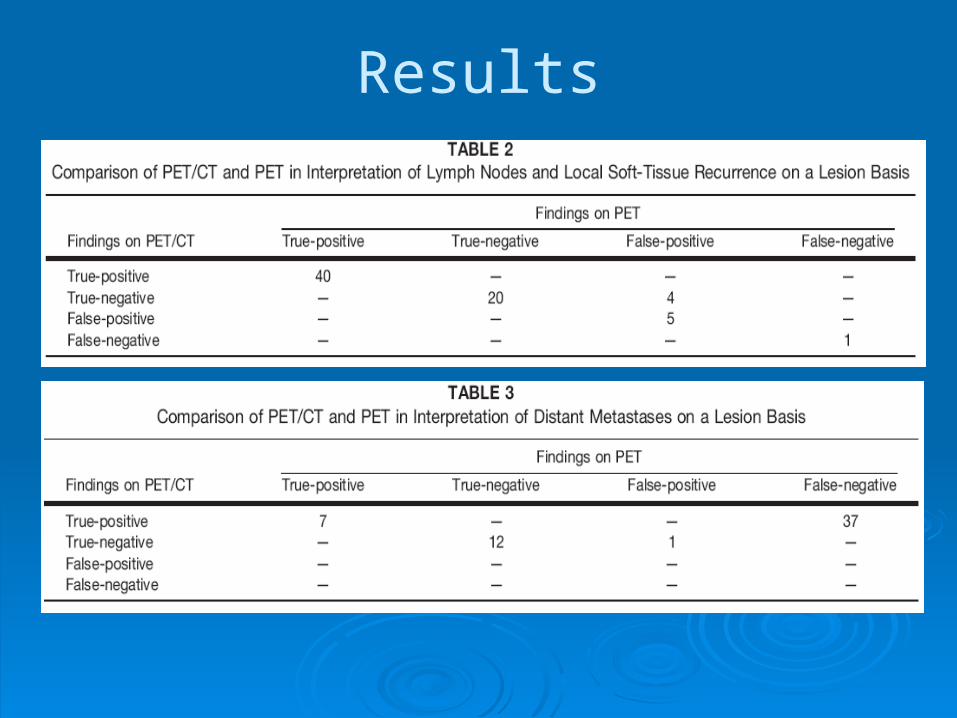
Materials and Methods true-positive : score was 2–4 and histopathology was po
sitive or if it showed progression at follow-up sessions. true-negative :score was 0–1 and histology was negative
or if follow-up examinations did not show any pathologic result in the region of concern for at least 18 mo.
false-positive : score was 2–4 and if histopathology was negative or if it showed no progression at follow-up sessions.
false-negative : score was 0–1 and if histology was positive or if follow-up examinations showed growth of the lesion(s).
Results
Results

Results

Results

Results
(A) Preoperative PET showed intense 18F-FDG uptake in the suspected, left cervical lymph node as demonstrated on the coronal slice. (B) However, PET detected a second tumor focus that was located more caudally. For this second tumor, shown On the transverse PET slice. (C ) no corresponding abnormality could be localized on CT images . (D) Only by fusion of PET andCT images could the second lesion be precisely identified (located between esophagus and dorsolateral trachea) and be removed surgically.

DiscussionDiscussion Three patients were identified on PET/CT
as having a physiologic or nontumoral cervical 18F-FDG accumulation that was classified as lymph node metastases by PET alone and side-by-side PET and CT.
One limitation of 18F-FDG PET is especially in the region of the neck. →Specificity for detecting lymph node metastases could be increased by PET/CT

(A) pathologic 18F-FDG uptake in the right lower cervical region. (B) Corresponding CT slices did not reveal any abnormality. (C) PET/CT images clearly showed that the PET finding was located on the right vocal cord and corresponded to benign, muscular uptake. No surgery was scheduled and follow-up confirmed this benign finding.

DiscussionDiscussion This was achieved in 3 patients by PET/CT dete
ction of small and miliary lung metastases that were not diagnosed by PET alone.
This confirms the findings of previously reported studies showing that 18F-FDG PET is not able to adequately assess miliary lung metastases smaller than 6 mm. It is unclear whether this is generated from motion artifacts on inspiration and expiration or from a lower metabolic activity of the lung metastases .
DiscussionDiscussion
One important aspect of our study was evaluation of the therapeutic relevance of PET/CT.

DiscussionDiscussion

DiscussionDiscussion
One limitation of our study seems to be that CT was performed without a contrast agent. → avoid blockage of iodine uptake.
Another limitation of the study is that the minimal time for follow-up of patients was 18 mo.

Conclusion
By precisely localizing tumor tissue, image fusion by integrated PET/CT is clearly superior to side-by-side interpretation of PET and CT images.
Integrated PET/CT is able to improve diagnostic accuracy in a therapeutically relevant way in patients with iodine-negative DTC.

Thank you for your attention ! Thank you for your attention !