integrated coloproctology
TRANSCRIPT

HOW THE ANAL SPHINCTER WORKS?
A NEW MATHEMATICAL APPROACH
BYProf .Dr. Ahmed Farag.MD.
Faculty of Medicine – Cairo University

Maintenance of continence appears to be a complex phenomenon
achieved by the combination of Anatomic and physiologic factors, the relative contribution of each
being unclear. (Sangwan and Coller Surg.Clin North Am
1994)

Faecal Incontinence May be multi-factorial due to altered stool
consistency, increased rate of delivery of contents to the
rectum, abnormal rectal capacity and compliance, decreased AR sensations and pelvic f loor or
anal sphincter dysfunction(Jorge and Wekner Dis Colon Rectum 1993)

Using traditional research methodology, the reported data
had been described as being disseminated research data by some authors and by the others as being adding to the confusion experienced in the world of Anal
Incontinence.
(Varma et al Dis colon Rectum 1999 – editors comment)

The role of Anismus detected on defecation proctography in idiopathic constipation was doubted by some authors due to the high incidence of this condition in their normal controls.
Schouten WR, Briel JW, Auwerda JJ, Van Dam JH, Gossl ink MJ, Giani AZ, Hop WC: Anismus: fact or fict ion? Dis Colon Rectum 1997 Sep 40:1033-41.

In addition very little is known about what symptoms or defecographic findings should be considered as an indication for surgery in patients suffering from large Rectocele (> 2m ) and impaired rectal emptying.
Karlbom U, Graf W, Nil lson S, Pahlman L: Does Surgical repair of a Rectocele improve rectal emptying? Dis Colo Rectum 1996 Nov 39:1296-1302.

The lack of answers to the question on how the anal sphincter works is mainly due to the fact that, the AR segment is functionally highly integrated and should be studied
using an integrated approach.
(Farag A. Dis Colon Rectum 2000 – Letter)

The flow equation had been used successfully previously in
medicine in order to understand and study:
1. Urodynamics.2. Hemodynamics.
Recently the flow equation had been applied for the integration of Anorectal
physiology trying to understand how the anal sphincter works, Which
should be our information highway for the investigation and treatment of
patients suffering from A.I. and other functional A.R. disorders.
Farag A. Eur Surg. Res. 1998Farag A. Dis Colon Rectum 2000 – Letter.
www.integratedcoloproctology.com

Definition of A.I.
Abnormal (involuntary) f low of gas or stools during rest or during
squeeze (voluntary or reflex).

Types of A.I.
1. Passive. (Engel et al 1995)
2. Urgency. (Engel et al 1995)
3. Stress. (Swash 1990)

Similarly Constipation can be defined as: A low flow rate of the stools or gases
during defecation per unit time.

The Flow Equation
intrarectal PressureFlow (A.I.) = ----------------------------------------- Anal canal Resistance

The Resistance Equation
128 x Dynamic Viscosity x A.C. LengthA.C. Resistance =
------------------------------------------------ 3.14 x (A.C. Diameter ) 4

A.C.L.
A.C.D.

Structure – Function relationship
Rest Sq. (X8) Strain (/88)

Primary Mechanical Factors
3.14 x (A.C. Diameter ) 4
Flow (A.I.)= intrarectal Pressure X ----------------------------
128 x D.V. x A.C. Length
Dynamic Viscosity of Air:Water:Barium sulphate paste = 1 : 38 : 68

Controversies in A.I.
3.14 x (A.C. Diameter ) 4
Flow (A.I.)= intrarectal Pressure X ----------------------------
128 x D.V. x A.C. Length
1. Anal Canal Pressure?
2. Anorectal Angle?3. Perineal Descent?4. Frequency of A.I.?

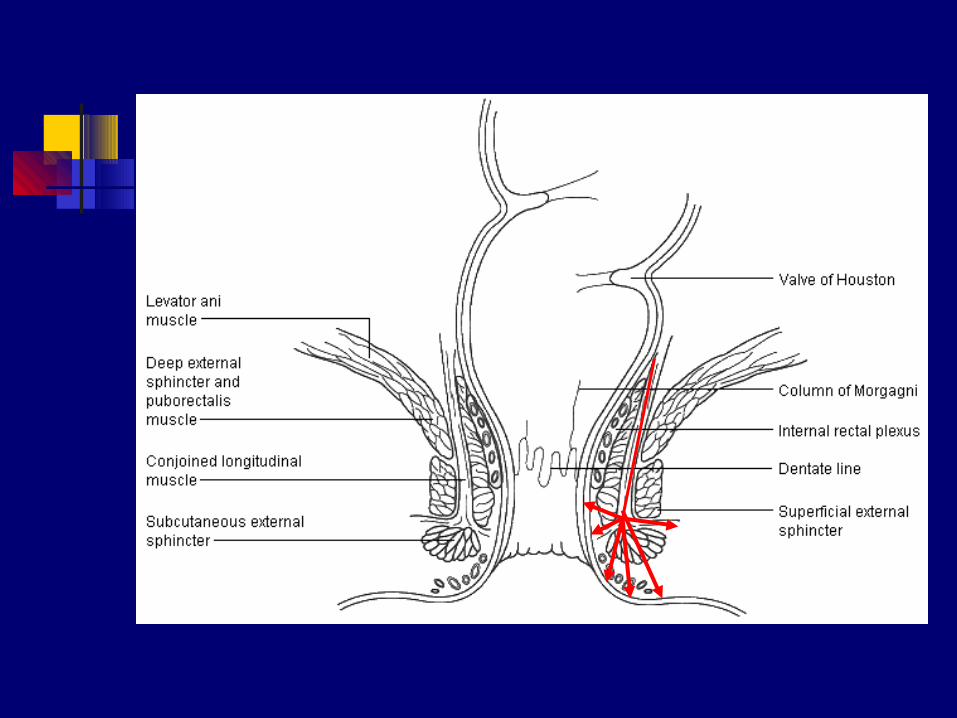

Longitudinal muscle
Internal A. sphincter
External A. sphincter
Puborectalis muscle
A.C. Length •It forms a supportive
framework for the IAS and EAS during
rest and squeeze.
• It decreases the A.C length
during defecation
Maintains A.C.L. during
rest (++)
Maintains ACL during rest (+)
and during Squeeze (+)
Maintains ACL during rest (++) and during squeeze (++) and relaxes to decrease ACL
during defecation (+
+)
A.C. Diameter •Forms a supportive
framework for the IAS and EAS during
rest and squeeze.•Opens the A.C. during defecation
Maintains A.C.D. during rest (++) and
relaxes to increase ACD
during defecation (+
+)
Maintains ACD during
rest (+), decreases
ACD during squeeze (++) and relaxes to increase ACD
during defecation (+
+)
Maintains ACD during rest (+) and
during squeeze (+)
and relaxes to increase ACD
during defecation (+)

Sensory & Reflex Factors
Flow (A.I.) = intrarectal Pressure / Anal canal
Resistance
Sensory Reflexes

THE HYBRID LAW IN COLOPROCTOLOGY
Since two thirds of continent individuals still have normal anal pressures as
seen on manometry, and two thirds of patients with AI have low anal pressures, can the anal canal
pressure show itself in the flow equation?

THE HYBRID LAW IN COLOPROCTOLOGY
As was suggested by many authors, the anal canal pressure measured is the resistance of the anal canal to distension by the measuring probes and is proportionate to the probe diameter.
Keighley MRB. Constipation in: Keighley MRB, Wil l iams(eds). Surgery of the Anus Rectum and Colon. London, Saunders 1993; 609 – 938.

According to the law of Laplace:
Distending Pressure (p) X Radius (R)
Wall Tension (T) = ––––––––––––––––––––––––––––––– Anal Canal Wall Thickness (δ)

Accordingly:
R (Inside) = Tδ/Anal Canal P
& Since the ACD = 2R

THE HYBRID LAW IN COLOPROCTOLOGY
3.15 (Tδ) 4
Flow = IR –––––––––––––––– 8 X DV (ACP) 4


The Flow Calculator.

Flow Index (Anal Incontinence)
< 0.1 - 1 cc/Sec. <
Fluid StoolsSoft Stools
GasFluid stoolsSoft Stools
Normal Soiling Incontinent

Passive A.I. (Mechanical Factors)
IRP (rest)Flow (A.I.)= ------------------------------------- A.C. Resistance (rest)

Passive A.I. (Sensory Deficit)
Flow (A.I.)= ------------------------------
SensoryFactors

Passive A.I. (Reflex Factors)
Flow (A.I.)= ------------------------
ReflexDeficit

Stress A.I. (Mechanical Factors)
IRP (cough)
Flow (A.I.)= -------------------------------------
A.C. Resistance (sq.)

Stress A.I. (Reflex Factors)
IRP (cough)
Flow (A.I.)= -----------------------------------------
A.C. Resistance (Rest)

Urgency A.I. (Mechanical Factors)
IRP (urgency) Flow (A.I.) = ------------------------------------- A.C. resistance (sq.)

Urgency A.I. (Sensory and reflex Factors)
IRP (urgency)Flow (A.I.)= --------------------------------------
A.C. Resistance (Strain.)

Knowing how the Anal Sphincter Works Wil l
help us in:
1. The relative contribution of factors responsible for A.I. i f they coexist
The relative contribution of sensory or reflex factors
= Flow after correction – Flow before correction

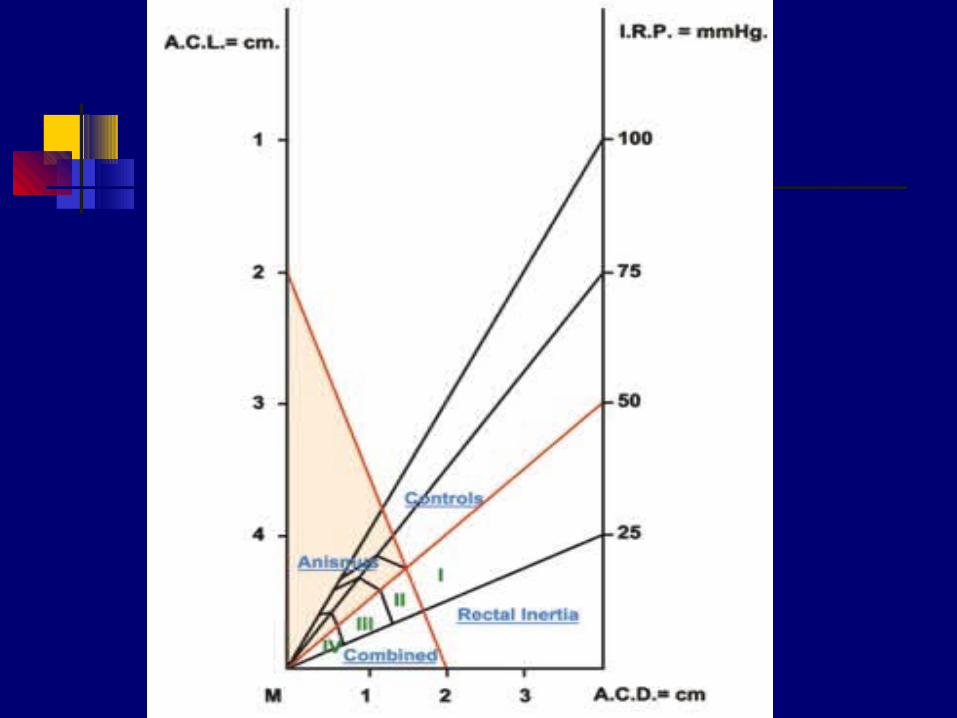
Zone 1: Normal defecationZone II, III&IV: Obstructed Def.II: for soft well formed stools.III: for fluid stools.IV: For Gas.
Defecation norm gram
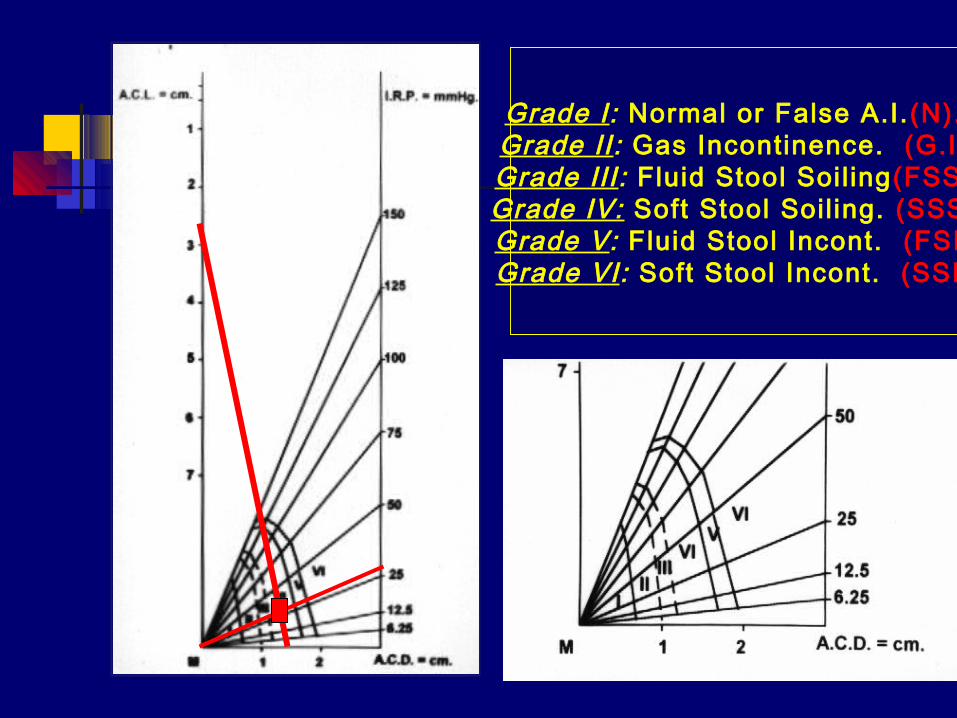
Grade I: Normal or False A.I. (N).Grade II : Gas Incontinence. (G.I)Grade III : Fluid Stool Soil ing(FSS)Grade IV: Soft Stool Soil ing. (SSS)Grade V: Fluid Stool Incont. (FSI)Grade VI: Soft Stool Incont. (SSI)

The mathematic scoring, diagrammatic scoring showed statistically significant correlation with clinical severity scoring at the level of 0.01.
Mathematic scoring could diagnose fecal incontinence irrespective to its severity in 59/63 patients (93.65%) and could accurately match the clinical severity in 39/63 patients (61.9%) using 6 points severity scoring and grading system. Farag A. III rd International Congress on Pelvic Floor
Surgery 2001

Mathematic scoring could diagnose fecal incontinence irrespective to its severity in 59/63 patients (93.65%) and could accurately match the clinical severity in 39/63 patients (61.9%) using 6 points severity scoring and grading system. Farag A. III rd International Congress on Pelvic Floor
Surgery 2001
The overall correlation between clinical scores, functional scores using flow equation (=0.732) and functional scores using continence normogram (=0.668) had revealed statistical significance at 0.01 level using Pearson’s correlation.

Similarly correlation between mathematical scoring using the flow equation and diagrammatic scoring using the continence normogram (=0.841) revealed statistical significance at 0.01 level using the same statistical analysis.

2. Patient selection for treatment.
Flow (A.I.)= ------------------------
S

2. Patient selection for treatment.
It helps to select patients for direct sphincter repair of their sphincter
defects seen on imaging by correlation between the anatomically lost sphincter length & decreased A.C. resistance to
flow

Anal sphincter repairs should not be offered to the patients with normal anal canal
resistance where:

The minimum AC dimensions during rest were set as ACL = 3.0 cm and ACD = 0.8 (AC
resistance = 5639.6 and tolerating IRP up to 42 mmHg).

and the minimum AC resistance during squeeze was taken as ACL = 3.5 cm and ACD = 0.6 cm ( AC resistance = 20794.7), tolerating IRP up to 155 cm) as calculated from the flow calculator..

Results O = successful
cases.
x = Failures.
Rectocele Group

How the A. Sphincter Works Can also Help in:
Predicting outcome. Operator independent assessment of
treatment. Assessment of different treatment
modalit ies if used simultaneously. Planning for New treatment
modalit ies.

Diseases of the colon and RectumVolume Number42 Cozox R crvM 4APRIL 1999CENTENNIAL ARTICLES IN COLON AND RECTAL
SURGERY
One Hundred Years of RectalProlapse SurgeryRobert D. Madoff, M.D., Anders Mellgren, M.D., Ph.D.From the Division of Colon and Rectal Surgery, University of
Minnesota, Minneapolis, Minnesota

One may reasonably expect that the coming centurywill provide further incremental gains in ourunderstanding of the pathophysiology of prolapseand its related disorders as laboratory investigationcontinues to be performed. However, one cannotdiscount the notion that an entirely novel and, onemight hope, unifying concept may emerge that radicallyalters our understanding of the disease.

Could It be the Flow equation and the Hybrid Law in Coloproctology the answer to the visionary question of Robert Madoff and his co-workers?

Knowledge Is Power
Thank You
www.integratedcoloproctology.com