unisys insured hmo...about this supplement this supplement describes the benefits provided through...
TRANSCRIPT

UNISYS
SELF-INSURED MANAGED-CARE OPTION
FOR UNISYS PARTICIPANTS
IN DESIGNATED GEOGRAPHIC LOCATIONS
January 2001
Supplement to the Summary Plan Description
for Medical Plans Sponsored by Unisys

ABOUT THIS SUPPLEMENT
This supplement describes the benefits provided through the self-insured managed-care medical options
made available in designated geographic locations to eligible Unisys employees, eligible former Unisys
employees and their eligible dependents. This supplement amends the Summary Plan Description (SPD)
booklet referenced below, that applies to you based on your employment status.
�� For active employees eligible to participate in the Unisys Flexible Benefits Program — SPD for health
and welfare benefits, including amendments as may be made from time to time.
�� For eligible retired or disabled former employees — SPD for the Unisys Post-Retirement and Extended
Disability Medical Plan (PRM Plan), including amendments as may be made from time to time.
Except where otherwise noted, this supplement modifies only the medical plan provisions for covered/non-
covered services and administrative procedures reflected in your SPD. Refer to your SPD for general
information on eligibility, enrollment, changing your medical elections, when coverage begins and ends, and
other important information, including the “additional information” section.
Throughout this supplement, “you” generally refers to covered employees, covered former employees and
covered dependents. The term “you” also is interchangeable, depending on the context of the sentence, with
an eligible employee, eligible former employee or an eligible dependent. “Retiree” generally refers to Unisys
retirees or disabled former Unisys employees and their covered dependents.
Keep this supplement handy as an ongoing reference. This supplement, your SPD, and any amendments
constitute your health plan documents. This supplement contains Plan provisions as of January 1, 2001,
unless otherwise noted.
FOR QUICK REFERENCE, KEEP THESE NUMBERS HANDY
Your primary care physician or clinic (PCP)
your first contact for all of your health-care needs
(does not apply to
SelectAdvantage for services
on or after July 1, 2001)
(Fill in the name and telephone number above)
Member Services �� general information
regarding the Plan �� help you identify network
providers
�� respond to inquiries on
claims
For Aetna, HealthPartners and Medica Self-Insured members,
also use these numbers to:
�� report treatment for a
medical emergency within
24 hours of treatment; also
contact your PCP/PCC �� precertify services
Aetna U.S. Healthcare® Members:
�� 1-800-238-3488
HealthPartners Members:
�� 952-883-5000 in the Minneapolis/St. Paul metro area
�� 1-800-883-2177
To report a medical emergency or urgent medical need after clinic daytime operating hours
�� 612-339-3663 in the Minneapolis/St. Paul metro area
�� 1-800-551-0859 outside the metro area
Medica Self-Insured Members:
�� 1-800-962-9497
�� 952-992-3190 or 1-800-841-6753 for TTY connections for the hearing impaired
To report a medical emergency or urgent medical need after clinic daytime operating hours
�� call your PCC after-hours telephone number
United Behavioral Health (UBH) for treatment of mental-health or substance abuse disorders
�� 1-800-848-8327
SelectAdvantage Members, through June 30, 2001:
�� 1-248-637-6777
�� 1-888-302-0767
For treatment of mental-health or substance abuse disorders
�� 1-800-888-9037
SelectAdvantage Members, on and after July 1, 2001:
�� 1-800-521-1321

Self-Insured HMO 2001 — i
CONTENTS
Introduction .................................................................................................................................................2
How the Plan Works....................................................................................................................................6
NETWORK PROVIDERS.............................................................................................................................6
Your Primary Care Physician (PCP) for Aetna U.S. Healthcare........................................................7
Your Primary Care Clinic (PCC) for HealthPartners and Medica Self-Insured.................................7
Your Primary Care Physician (PCP) for SelectAdvantage .................................................................7
Role of your PCP/PCC........................................................................................................................8
Selecting your PCP/PCC.....................................................................................................................8
Changing your PCP/PCC ** ..............................................................................................................9
Network Specialists ............................................................................................................................9
IF YOUR PHYSICIAN OR CLINIC LEAVES THE NETWORK.......................................................................10
WHAT TO DO FOR A MEDICAL EMERGENCY OR AN URGENT MEDICAL NEED......................................10
WHAT TO DO IF YOU OR YOUR DEPENDENT IS OUTSIDE THE SERVICE AREA WHEN MEDICAL CARE IS
OBTAINED..............................................................................................................................................11
Aetna U.S. Healthcare Cost-Sharing Table ...............................................................................................16
HealthPartners Cost-Sharing Table............................................................................................................23
Medica Self-Insured Cost-Sharing Table...................................................................................................30
SelectAdvantage Cost-Sharing Table ........................................................................................................40
Definitions .................................................................................................................................................50
Precertification...........................................................................................................................................62
EMERGENCY SERVICES .........................................................................................................................62
NON-EMERGENCY SERVICES.................................................................................................................62
Covered Expenses/Services .......................................................................................................................66
Exclusions .................................................................................................................................................84
Special Programs .......................................................................................................................................96
How to File a Claim...................................................................................................................................98
INFORMATION NEEDED FOR A CLAIM ....................................................................................................98
ADDRESS FOR CLAIMS SUBMISSIONS.....................................................................................................98
SOME EXPENSES ARE NOT REIMBURSABLE ...........................................................................................98
FILING LIMITATIONS ..............................................................................................................................99
PAYEES ..................................................................................................................................................99
DELAYED PAYMENTS.............................................................................................................................99
RIGHT TO RECOVER EXCESS PAYMENTS................................................................................................99
Complaint and Appeals Procedure ............................................................................................................99
REGISTERING A COMPLAINT OR DISAGREEMENT WITH A DETERMINATION .........................................99
APPEALS OF PRECERTIFICATION DETERMINATIONS ...........................................................................101
Additional Information About the Plan ...................................................................................................104
FUNDING..............................................................................................................................................104
RIGHT TO RECEIVE AND RELEASE NEEDED INFORMATION.................................................................104
RIGHT TO DEVELOP GUIDELINES .........................................................................................................104
ACCESS TO RECORDS AND CONFIDENTIALITY .....................................................................................105
AMENDMENTS TO THIS SUPPLEMENT..................................................................................................105
CASE REVIEW ......................................................................................................................................105
EXTENSION OF BENEFITS .....................................................................................................................105
Index........................................................................................................................................................108


INTRODUCTION
Self-Insured HMO 2001 –– 1
INTRODUCTION

INTRODUCTION
2 — Self-Insured Managed-Care Option 2001
INTRODUCTION
Unisys offers this self-insured managed-care option in designated geographic locations to eligible Unisys
employees, former employees, and their dependents.
Under a fully-insured plan, Unisys pays fixed monthly premiums set by the plan. The plans bear the risk
that expenses will not exceed the premiums collected. The premiums include projected benefit payments,
state insurance taxes, administrative costs, and a profit margin. The benefits provided under the plan are
subject to mandates specific to the states in which they operate.
Under a self-insured plan, Unisys makes benefit payments as services occur, including a fee for the use of
the third-party administrator’s network and the third-party administrator’s services noted below. Costs are
variable rather than fixed because Unisys, not the plans, bears the risk of volatility of expenses. State
insurance taxes and state mandates do not apply. Instead, the plan is subject to the federal Employee
Retirement Income Security Act.
Unisys has contracted with the following third-party administrators (TPAs) for claims processing,
precertification, utilization review, member services, grievance resolution, and a provider network under
the Plan. Use the group number noted below when asking questions about benefits under the Plan.
Third-party administrators
(TPAs)
Group ID Number
active employees and their
covered dependents
Group ID number
retired or disabled former employees and
their covered dependents or survivors
Aetna U.S. Healthcare® #00176C #00176C NOT eligible for Medicare
HealthPartners
Administrators, Inc.
(owner: HealthPartners, Inc.)
#3493 #3493
Medica Self-Insured (MSI) �� #45935 non-bargaining
�� #45936 bargaining
�� #45936 bargaining to age 65
�� #45937 non-bargaining NOT eligible for
Medicare
�� #45938 non-bargaining eligible for Medicare
SelectCare Systems
Corporation through 6/30/01
(product: SelectAdvantage)
Select Advantage on and
after 7/01/01
�� PPOM networks
�� ABS third-party
administrator
�� #095625-0001
�� #095625-0002 COBRA
�� #095625-0004 NOT eligible for Medicare
�� #095625-0003 eligible for Medicare
Each third-party administrator:
�� Has a network of physicians, hospitals and health-care centers that are available as part of the Plan;
�� Follows a credentialing process before a provider is admitted to their network; and
�� Monitors the performance of their network providers.
Neither Unisys nor any of the TPAs engage in the performance or delivery of medical, hospital services, or
other types of health-care services. The TPAs have contractual agreements with their network providers to
furnish covered services within the scope of their licenses to plan members. Neither Unisys nor any of the
TPAs guarantee the professional services of the providers. The selection of a provider and the decision to
receive or decline health-care services is solely your decision and responsibility.
This Supplement to your Summary Plan Description (SPD) booklet includes: a description of how the Plan
works, a description of benefits available under the Plan; procedures for submitting requests for
reimbursement, and procedures for appealing a denied request for benefits. Refer to the appropriate SPD

INTRODUCTION
Self-Insured Managed-Care Option 2001 — 3
referenced inside the front cover under “About This Supplement” for:
�� General information on eligibility;
�� Covered dependents;
�� Coordination of benefits with other group plans;
�� When coverage begins and ends;
�� Your continuation options (if any) when coverage ends; and
�� General additional Plan information, such as your rights under the Employee Retirement Income
Security Act (ERISA) of 1974, as amended, and third-party liabilities.
Read this supplement and your SPD. Many provisions are interrelated; reading just one or two provisions
may give you a misleading impression. Some terms in this supplement have a particular meaning under the
Plan and are defined, beginning on page 49.
Unisys maintains this Plan for the exclusive benefit of covered employees, covered former employees, and
their covered dependents. Each covered person's rights under the Plan are legally enforceable.


Self-Insured Managed-Care Option 2001 — 5
HOW THE PLAN WORKS

HOW THE PLAN WORKS
6 — Self-Insured Managed-Care Option 2001
HOW THE PLAN WORKS
To understand how the Plan works, it is important to know how to use the “Network” providers and
benefits. In order to use this Plan, you will need to know about the most important network provider of
them all — your PCP, your “primary care physician” (for HealthPartners or Medica Self-Insured, your
PCC, your “primary care clinic”).
Network Providers
Network providers are doctors, hospitals, and other health-care providers who belong to the third-party
administrator’s network of contracted providers.
A directory of Network physicians and providers who have agreed to provide covered services to Plan
members is available to you before you enroll. This directory is updated regularly. You also can access the
websites as noted below for the most up-to-date information:
Third-party administrator
(TPA) Website Feature for provider directory
Aetna U.S. Healthcare www.aetnaushc.com Click on DocFind®; then search under
�� Type of provider
�� HMO, if an active employee
�� HMO, if a retiree not eligible for
Medicare
�� Medicare Golden Plan, if a retiree
eligible for Medicare
HealthPartners www.healthpartners.com �� Click on Consumer Choice
�� Choose HealthPartners Primary Clinic
�� Choose from providers, care networks,
clinics, and hospitals
Medica Self-Insured www.allina.com Click on the Medica.com tab
�� Visitors Center
�� Provider Directory
�� Continue
�� Medica Premier
�� Continue
�� Search Options
SelectCare – for
SelectAdvantage through
6/30/01
www.selectcare.com Physicians, hospitals and other services
�� SelectCare Physician Search for non-
hospital providers
�� HMO/HMO Plus/
SelectAdvantage POS for network
hospitals
SelectAdvantage – on and
after 7/01/01
www.abs-tpa.com �� Click on Members button
�� Choose the Unisys button for providers
and other search options

HOW THE PLAN WORKS
Self-Insured Managed-Care Option 2001 — 7
Your Primary Care Physician (PCP)
for Aetna U.S. Healthcare
At the core of the Plan is your PCP. The Plan promotes the PCP as your personal medical-care coordinator.
When you enroll in the Plan, you choose a PCP for yourself and for each covered family member. You
choose from the licensed network physicians who practice in one of the following areas of medicine:
�� Family/General Practice: Family/general practitioners have special medical training in prevention,
diagnosis, and management of the medical needs of adults and children. Many family/general
practitioners perform minor surgery, obstetrics and gynecology services.
�� Internal Medicine: Internists have specialized training in the prevention, diagnosis, and management
of illness in adults. Many internists also have specialized areas of interest, called subspecialties, in
which they have further training. These include endocrinology, cardiology, gastro-enterology, and so
on.
�� Pediatrics: Pediatricians have specialized training in the medical management of children from birth
through late teen years. Besides treating illnesses, these physicians are interested in seeing that their
patients undergo normal growth and development.
Women age 16 or older have the option of choosing an OB/GYN in addition to their medical PCP. If you
choose to do so, you can see that OB/GYN for routine obstetrical and gynecological care without a referral
from your PCP. More complicated situations and surgeries will be coordinated by both your network
OB/GYN and your PCP.
Your Primary Care Clinic (PCC)
for HealthPartners and Medica Self-Insured
At the core of the Plan is your PCC. The Plan promotes the PCC as your personal medical care
coordinator. When you enroll in the Plan, you choose a PCC for yourself and for each covered family
member. You choose from the primary care clinics listed in the Provider Directory. Refer to page 6 to learn
how to obtain the list of primary care clinics.
The PCCs are either:
�� Owned, operated, and staffed by the third-party administrators, or
�� Contracted with the third-party administrators to provide primary care services and ambulatory medical
care.
Within the clinics are licensed network physicians who practice in one of the primary care areas of
medicine defined above as Family/General Practice, Internal Medicine, or Pediatrics.
Your Primary Care Physician (PCP)
for SelectAdvantage
For services on or before June 30, 2001, SelectAdvantage requirements for PCP selection and referrals are
the same as those noted above for Aetna U.S. Healthcare.
On and after July1, 2001, SelectAdvantage does not require the selection of a PCP. You may seek services
from any PPOM network provider without referrals, including network specialists. Traditionally this type
of network-based plan is considered an open-access HMO.

HOW THE PLAN WORKS
8 — Self-Insured Managed-Care Option 2001
Role of your PCP/PCC
You become a partner with your PCP/PCC in preventive medicine. Helping you maintain good health
through preventive care is one of the goals of the Plan. Periodic evaluations, examinations, x-rays and lab
work all contribute to keeping you in good health and are provided when your PCP/PCC so advises. These
services also help your PCP/PCC detect potential problems early, preventing complications later.
Consult your PCP/PCC whenever you have questions about your health. Your PCP/PCC is your guide
through today’s complex medical-care system.
When medically necessary, your PCP/PCC refers you to other doctors or facilities for treatment. To receive
coverage, you must have a prior written or electronic referral from your PCP/PCC for all non-emergency
services and any necessary follow-up. The referral is important because:
�� It is how your PCP arranges for you to receive the necessary, appropriate care and follow-up treatment.
�� It guarantees payment to network specialists and hospitals for referred covered services, so you will
only be responsible for applicable copayments. (Note: not all services are covered under the Plan.
When you receive a referral, check with Member Services to be sure that the services requested by the
referral are covered under the Plan.)
�� It is required for services to be considered for payment.
Even when your PCP/PCC refers you to a specialist or hospital, it is important that your PCP/PCC
continues to monitor your progress.
Note for Medica Self-Insured
Medica Self-Insured allows you to refer yourself to network providers without referral from your PCC.
This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. Copayments
and coinsurance are higher under Tier II than when you obtain a referral from your PCC (Tier I).
Note for SelectAdvantage on and after July 1, 2001
SelectAdvantage allows you to refer yourself to network providers without referral for services on and after
July 1, 2001. This is called “self-referral.”
Selecting your PCP/PCC
When you enroll for coverage, you must select a network PCP/PCC to manage the care of each family
member. You may select a different PCP/PCC for yourself and for each of your covered dependents.
For more information about a specific doctor or clinic you can access the information through the websites
noted on page 6 or call Member Services at the telephone number listed inside the front cover of this
Supplement. It also may be helpful to schedule a meeting with your prospective PCP/PCC to ask questions
and determine your personal comfort level with the provider.
After you enroll, you and each family member will receive a medical ID card.
Newborns or new adoptions: To enroll a newborn or newly adopted child for coverage, you must notify
the Unisys Benefits Service Center of the addition of the child by calling 1-800-600-4015 within 30 days
of the date of birth or adoption. Then indicate your child’s PCP/PCC by calling Member Services at the
telephone number listed inside the front cover of this supplement. An ID card for the child is then sent to
you.
Note for SelectAdvantage on and after July 1, 2001: No PCP selection is required for any covered family
member. After you enroll in the Plan, you receive a medical ID card for yourself and one to share with
other covered family members. If you need additional ID cards, call Member Services

HOW THE PLAN WORKS
Self-Insured Managed-Care Option 2001 — 9
Changing your PCP/PCC* **
You may change your PCP/PCC by calling Member Services at the telephone number listed inside the
front cover of this Supplement. Some third-party administrators allow you to change your PCP/PCC over
the Internet by accessing their websites (see page 6).
If you use Member Services to change your PCP/PCC, give the Member Services representative the new
PCP/PCC office ID number (this is available in the paper directory, the online directory, or by calling the
provider’s office). Ask your current PCP/PCC to transfer your medical records to your new PCP/PCC.
If you need to see the new PCP/PCC immediately, tell Member Services so verification of the new
designation can be coordinated with the PCP/PCC’s office before you make your appointment.
Referrals from your prior PCP do not carry forward. You need to obtain new referrals from your new PCP.
Network Specialists ** ***
Your PCP/PCC provides most of your care. However, if your PCP/PCC determines that you need specialty
care, your PCP/PCC will issue a written or electronic referral to one of the specialists who belong to the
Plan’s Network. As long as you remain a Plan participant, referrals are valid for:
�� The services specified on the referral
�� The provider noted on the referral
�� The time frame noted on the referral; in most cases, this will not exceed 90 days from the date the
referral is issued
When your PCP/PCC refers you to a network specialist for covered services, the Plan provides full
coverage, after applicable copayments, up to the benefit limits shown in the cost-sharing chart for the
appropriate plan. The charts begin on the following pages:
�� Aetna U.S. Healthcare, see page 15
�� HealthPartners, see page 21
�� Medica Self-Insured, see page 29
�� SelectAdvantage, see page 39
To avoid personal responsibility for the full charge for costly and unnecessary specialist bills:
1. Always consult your PCP/PCC first when you need medical care. If it is medically necessary, your
PCP/PCC will provide a written or electronic referral to provider.
2. Take a moment to review the referral with your PCP/PCC. Understand what specialist services are
being recommended and why.
3. Present the written referral to the specialist. In the case of an electronic referral, reference the referral
date and your PCP/PCC’s name. The referral is necessary to have the noted services approved for
payment. Without the referral, you are responsible for payment for these services.
4. If the referral provider suggests any treatments or tests not listed in the referral, another written or
electronic referral from your PCP/PCC is required in order for the services to be covered.
* Note for HealthPartners and Medica Self-Insured: Changes in your primary care clinic made by the 20th of the
month are effective the 1st of the following month. Changes made after the 20th are effective the 1st of the next
following month. For example, a change requested May 15th is effective June 1st. A change requested May 22nd is
effective July 1st. You cannot access your new primary care clinic for services before the effective date of the
change.
** Note for Medica Self-Insured: Medica allows you to refer yourself to network providers without referral from
your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. Copayments and
coinsurance are higher under Tier II than when you obtain a referral from your PCC (Tier I).
*** Note for SelectAdvantage on and after July 1, 2001: You are not required to notify anyone for care by network
providers.

HOW THE PLAN WORKS
10 — Self-Insured Managed-Care Option 2001
Note: If your condition does not meet the definition of emergency (see page 52) or urgent medical need
(see page 59), and you go directly to any doctor or facility without a written or electronic referral from your
PCP/PCC* **, you must pay the entire bill yourself.
If Your Physician or Clinic Leaves the Network
Doctors or clinics sometimes leave the network. They may leave because they are relocating, or because
they no longer meet the standards and requirements for network membership, or for other reasons. If your
PCP/PCC leaves the network, you will be notified and asked to select a new network PCP/PCC.
What to Do for a Medical Emergency or an Urgent Medical Need
Medical emergency is defined on page 52. Urgent medical need is defined on page 59. All emergency care
and urgent medical care is reviewed on a case-by-case basis. To avoid unforeseen problems, it is essential
that you understand what to do in case of a medical emergency or an urgent medical need.
If you have a medical emergency or an urgent medical need while outside the network service area, follow
these steps**:
1. Call your PCP/PCC for help. Explain the symptoms that are occurring and give your PCP/PCC any
other information necessary to help determine the appropriate action.
2. If directed by your PCP/PCC, if you cannot reach your PCP/PCC or a covering physician***, or if a
delay would endanger your health:
a. In a medical emergency — seek care at the nearest emergency treatment facility and have the
emergency room contact your PCP/PCC immediately, so your PCP/PCC can contribute to the
treatment you require
b. In an urgent medical situation — seek care at the nearest emergency treatment facility,
private practice physician, walk-in clinic, or surgicenter and have the provider contact your
PCP/PCC immediately, so your PCP/PCC can contribute to the treatment you require
3. If you are admitted to an inpatient facility, you, a family member, a treating physician, or the facility
should contact your PCP/PCC AND Member Services within 24 hours.
4. If you are not admitted to an inpatient facility, you or a family member must notify your PCP/PCC
within 24 hours after treatment is received.
Participating PCP/PCCs are required to provide coverage 24 hours a day, including weekends and
holidays. Chronic or less severe problems should be handled during routine office hours, but your
physician provides around-the-clock coverage to help deal with emergencies and urgent medical needs.
Care for a medical emergency is covered, no matter where, no matter when. If you have an urgent medical
need while inside the network service area, your PCP/PCC* ** must coordinate your care in order for
benefits to be payable. Urgently needed care may also be covered while out of the network service area, if
you follow the steps indicated above and your PCP/PCC refers you for immediate care.
The appropriate third-party administrator makes the initial coverage determination. If the third-party
administrator determines that the situation meets the Plan requirements for emergency care or urgent
* Note for Medica Self-Insured: Medica allows you to refer yourself to network providers without referral from
your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. Copayments and
coinsurance are higher under Tier II than when you obtain a referral from your PCC (Tier I).
** Note for SelectAdvantage on and after July 1, 2001: You are not required to notify anyone for care by network
providers. If you obtain care from a non-network provider due to a medical emergency or urgent medical need
occurring outside the network service area, you must contact Member Services within one business day after services
are received.
*** Note for HealthPartners: After regular PCC hours, call the HealthPartners After Hours CareLine at the number
on your ID card. Or you may visit any of the plan-wide network urgent care clinics.

HOW THE PLAN WORKS
Self-Insured Managed-Care Option 2001 — 11
medical care, benefits are payable whether or not network providers are used. However, the Plan may limit
reimbursement to expenses incurred up to the time you are determined to be medically able to travel or to
be transported to a network provider.
Treatment in hospital emergency rooms is not covered for conditions that are determined not to be an
emergency or urgent medical need. If it is determined that your condition does not meet the requirements
to be classified as an emergency or urgent medical need by the Plan, you are not entitled to reimbursement.
Note: A number of situations in which emergency rooms have traditionally been used are not generally
considered a medical emergency or urgent medical need. If you are in doubt about whether your situation
constitutes a medical emergency or urgent medical need, call your PCP/PCC or call Member Services
at the telephone number listed inside the front cover of this supplement.
Follow-up care after emergency or urgently needed treatment (for example, suture removal, cast removal,
x-rays, clinic/office revisits, or emergency room revisits) is covered only when provided by your PCP/PCC
or when authorized by a written or electronic referral by your PCP/PCC*.
What to Do if You or Your Dependent Is Outside the Service Area
when Medical Care Is Obtained
Benefit payments for services you receive depend on a number of factors if:
��You are traveling outside the service area for some purpose other than:
�� The receipt of medical care,
OR
��Your primary residence is outside the service area;
��You or a covered dependent is a student residing outside the service area while away at school.
Benefits are available only in the following situations:
�� If the treatment is for a medical emergency (as defined on page 52) and the steps noted beginning on
page 10 have been followed — in other words, benefits are payable for treatment in a medical
emergency no matter where you are or whether treatment is from network or non-network providers.
�� If the treatment is for an urgent medical need (as defined on page 59), the steps noted beginning on
page 10 have been followed and your PCP/PCC has referred you for immediate care.
�� For routine and preventive services, benefits apply only if your designated network PCP/PCC*
provides these services — all routine and preventive care must be provided by your designated
network PCP/PCC in order to have any coverage at all.
�� For treatment of mental/nervous conditions** ***, including substance abuse, benefits apply only if
they are arranged in accordance with the provisions of the Plan and are received from a designated
network provider.
* Note for Medica Self-Insured: Medica allows you to refer yourself to network providers without referral from
your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. Copayments and
coinsurance are higher under Tier II than when you obtain a referral from your PCC (Tier I).
** Note for Medica Self-Insured: All mental-health and/or substance abuse treatments must be coordinated by
United Behavioral Health (UBH), a separate specialized organization, in order to be covered. The telephone number
is on the inside front cover of this booklet.
*** Note for SelectAdvantage: All mental-health and/or substance abuse treatments on or before June 30, 2001, ust
be coordinated by Value Options, a separate specialized organization, in order to be covered. The telephone number
is on the inside front cover of this booklet.

HOW THE PLAN WORKS
12 — Self-Insured Managed-Care Option 2001
For HealthPartners, call 1-800-530-4966. This will connect you with PHCS, an affiliated group that can
provide you with the names and telephone numbers for participating PHCS providers or, in the U.S. and
Canada, call After Hours CareLine at the telephone number listed on your ID card for assistance in
directing your care. Outside the U.S. and Canada, contact MCI and ask to be connected on a collect-call
basis to After Hours CareLine at 952-883-7789. Services received from PHCS providers are allowed on a
discounted fee-for-service basis and you are responsible for payment.
For Aetna U.S. Healthcare, there is added flexibility for employees residing in one Aetna U.S. Healthcare
HMO service area offered through Unisys while dependents reside in a different Aetna U.S. Healthcare
HMO network area offered through Unisys (for example, children residing with a former spouse or
children while away at school). In this case, a PCP for the dependent can be selected in the network area
where the dependent resides and the full range of covered services is available to the dependent within that
network.
To determine if a dependent resides in an HMO service area:
�� Call Member Services at the toll-free number listed inside the front cover of this booklet, or
�� Visit the Aetna U.S. Healthcare website at www.aetnaushc.com.
�� Select the HMO product
�� Enter the ZIP code for the dependent
�� If providers are listed, then the ZIP code is in an Aetna U.S. Healthcare HMO service area

COST SHARING TABLES
Self-Insured Managed-Care Option 2001 — 13
COST-SHARING TABLES


AETNA U.S. HEALTHCARE COST-SHARING TABLE
Self-Insured Managed-Care Option 2001 — 15
AETNA U.S. HEALTHCARE
COST-SHARING TABLE
��ACTIVE EMPLOYEES AND THEIR COVERED DEPENDENTS
��RETIREES, DISABLED FORMER EMPLOYEES AND THEIR COVERED DEPENDENTS
NOT ELIGIBLE FOR MEDICARE

AETNA U.S. HEALTHCARE COST-SHARING TABLE
16 — Self-Insured Managed-Care Option 2001
AETNA U.S. HEALTHCARE COST-SHARING TABLE
The following chart outlines benefits for those enrolled in the Aetna U.S. Healthcare self-insured option as
an active employee, including enrolled eligible dependents. It also applies to those not eligible for
Medicare who enroll as an eligible retiree or disabled former employee, including their enrolled
dependents not eligible for Medicare. All care must be provided by or coordinated by your PCP for you to
receive benefits. This chart is just a summary of the benefits. Some services may have limits. Specific
conditions, limits and exclusions are detailed in the pages that follow the cost-sharing charts.
AETNA U.S. HEALTHCARE COST-SHARING TABLE
Feature Cost-Sharing
Annual Deductible None
Annual Out-of-Pocket Limit None
Lifetime Maximum Benefit None
Precertification
PCP handles for you, except treatment for medical
emergency or urgent medical need
not provided or directed by PCP
Network Physician Visits for Preventive Services
��Well-child care; frequency/type based
on Aetna U.S. Healthcare guidelines
You pay $10/visit to PCP,
then Plan pays 100%
��Routine visits, age 18 and older (annual) You pay $10/visit to PCP,
then Plan pays 100%
��Well-woman exam (annual); no referral
required
You pay $10/visit to network OB/GYN,
then Plan pays 100%
�� Prenatal care You pay $15 for first office visit to network OB/GYN,
then Plan pays 100% for all prenatal care thereafter
�� Cancer screenings (physician services
only); frequency/type based on Aetna
U.S. Healthcare guidelines
You pay $10/visit to PCP or $15/visit to referral specialist,
then Plan pays 100%
��Vision
�� Examination by network optometrist
or ophthalmologist; no referral
required; frequency based on Aetna
U.S. Healthcare guidelines
You pay $15/visit,
then Plan pays 100%
�� Eyewear Not covered;
Discount arrangements are available through the Plan

AETNA U.S. HEALTHCARE COST-SHARING TABLE
Self-Insured Managed-Care Option 2001 — 17
AETNA U.S. HEALTHCARE COST-SHARING TABLE
Feature Cost-Sharing
Network Physician Visits Other Than Preventive Services
�� Treatment of illness or injury You pay $10/visit to PCP or $15/visit to referral specialist,
then Plan pays 100%
��Office surgery You pay $10/visit to PCP or $15/visit to referral specialist,
then Plan pays 100%
��Office lab and x-ray
�� Billed with office visit
�� No office visit when services
rendered
Plan pays 100%
You pay $15/test or x-ray;
then Plan pays 100%
��Allergy testing and treatment You pay $10/visit to PCP or $15/visit to referral specialist,
then Plan pays 100%
Inpatient Network Hospital Services
��Hospital semi-private room & board and
ancillary services
You pay $250/admission,
(not applicable for re-admission within 30 days for the
same condition; $750 maximum/person/year),
then Plan pays 100%
�� Lab and x-ray Plan pays 100% after the hospital copayment
�� Surgeons' charges Plan pays 100% after the hospital copayment
�� Physician hospital visits Plan pays 100% after the hospital copayment
��Anesthesia Plan pays 100% after the hospital copayment
��Delivery — normal or C-section Plan pays 100% after the hospital copayment
Network Alternatives to Inpatient Care: Precertification and referral by PCP required
��Skilled nursing facility (maximum of 90 days/lifetime)
Plan pays 100% after the hospital copayment
���Home-health care Plan pays 100%
��Home IV therapy Plan pays 100%
�� Inpatient hospice for palliative care of
terminally ill
Plan pays 100% after the hospital copayment

AETNA U.S. HEALTHCARE COST-SHARING TABLE
18 — Self-Insured Managed-Care Option 2001
AETNA U.S. HEALTHCARE COST-SHARING TABLE
Feature Cost-Sharing
Outpatient Services (treatment and services by network providers performed in a network
facility other than in the physician’s office or as an inpatient in a hospital)
�� Surgery, including surgeon and facility You pay $100/procedure for PCP or referral specialist,
then Plan pays 100%
�� Independent lab and x-ray facilities You pay $15/test or x-ray,
then Plan pays 100%
��Hospital emergency room (medical
emergency defined on page 52)
�� For treatment of a medical
emergency
You pay $50/visit
(waived if admitted within 24 hours for the same
condition),
then Plan pays 100%
�� For non-emergency care not
authorized in advance by PCP
Not covered
��Hospital observation room for up to 24
hours without admission
Same as outpatient hospital emergency room services
�� Follow-up care with PCP or referral
specialist�
You pay $10/visit for PCP or $15/visit for referral
specialist,
then Plan pays 100%
��Ambulance (ambulance defined on
page 50; medical emergency defined on
page 52)�
�� For a medical emergency
Plan pays 100%
�� For non-emergency transportation
approved by Aetna U.S. Healthcare
and recommended by the PCP
Play pays 100%;
otherwise, not covered

AETNA U.S. HEALTHCARE COST-SHARING TABLE
Self-Insured Managed-Care Option 2001 — 19
AETNA U.S. HEALTHCARE COST-SHARING TABLE
Feature Cost-Sharing
Treatment for Mental Health Conditions by Network Providers
��Inpatient hospital or specialized
treatment facility
You pay hospital copayment,
then Plan pays 100%;
up to 30 days/year, up to 90 days/lifetime;
annual and lifetime maximums include inpatient care for
detoxification and treatment of substance abuse conditions
��Physician inpatient visits Plan pays 100%,
up to 30 days/year, up to 90 days/lifetime;
annual and lifetime maximums include inpatient care for
detoxification and treatment of substance abuse conditions
��Office/outpatient visits You pay $15/visit for referral specialist,
then Plan pays 100%;
up to 30 visits/year
(individual, family, group or other visits count as one visit)
Treatment for Substance Abuse Conditions by Network Providers
��Detoxification You pay hospital copayment,
then Plan pays 100%
�� Inpatient hospital or specialized
treatment facility
You pay hospital copayment,
then Plan pays 100%;
up to 30 days/year, up to 90 days/lifetime;
annual and lifetime maximums include inpatient care for
detoxification and treatment of mental health conditions
�� Physician inpatient visits Plan pays 100%;
up to 30 days/year, up to 90 days/lifetime;
annual and lifetime maximums include inpatient care for
detoxification and treatment of mental health conditions
��Outpatient rehabilitation You pay $15/visit for referral specialist,
then Plan pays 100%;
up to 30 visits/year;
(individual, family, group or other visits count as one visit)

AETNA U.S. HEALTHCARE COST-SHARING TABLE
20 — Self-Insured Managed-Care Option 2001
AETNA U.S. HEALTHCARE COST-SHARING TABLE
Feature Cost-Sharing
Other Network Services and Supplies
��Acupuncture only when provided by a physician for
anesthesia in connection with a covered surgery
Plan pays 100%
��Chiropractic services �� only for short-term treatment when there is
a reasonable expectation that a condition
will improve over a short-predictable
period of time
�� does not include maintenance or palliative
care
You pay $15/visit for referral specialist,
then Plan pays 100%;
up to 15 visits within 60 consecutive days/incidence,
measured from start of treatment;
Aetna U.S. Healthcare Medical Director can authorize
additional therapy, provided the conditions noted to the left
continue to apply
��Dental services You pay $100/procedure for surgical removal of partial or
fully bony impacted wisdom tooth or tumors, then Plan
pays 100%; other dental procedures are not covered
��Diabetes self-management training and
education
�� Educational tools
��Blood glucose monitor
�� Program consistent with national
standards established by the
American Diabetes Association
You pay $10/visit to PCP or $15/visit to referral specialist,
then Plan pays 100%
��Durable medical equipment (DME) Plan pays 100% for precertified DME when obtained from
network DME vendors
�� Infertility treatments: limited to the diagnosis and treatment of
medical conditions resulting in infertility and
treatment to return the body to normal bodily
function
Covered the same as treatment for other conditions
��Nutritional supplements for the
treatment of PKU
Plan pays 100%
�� Prosthetic devises; limited to items
noted on pages 68 and 69.
Plan Pays 100% for precertified covered prosthetic devices
when obtained from network vendors;
Covered wigs limited to $350 per year
��Reconstructive and restorative surgery
that is not cosmetic in nature
Same as other surgery
��Rehabilitative services: cognitive,
physical, occupational, pulmonary, and
speech therapy �� only for short-term treatment when there is
a reasonable expectation that a condition
will improve over a short, predictable
period of time
�� only to restore function lost through illness
or injury
�� does not include maintenance or palliative
care
You pay $15/visit for referral specialist,
then Plan pays 100%;
up to 60 consecutive days/condition, measured from start
of treatment;
Aetna U.S. Healthcare Medical Director can authorize
additional therapy,
provided the conditions noted to the left continue to apply

HEALTHPARTNERS COST-SHARING TABLE
Self-Insured Managed-Care Option 2001 — 21
HEALTHPARTNERS
COST-SHARING TABLE
��ACTIVE EMPLOYEES AND THEIR COVERED DEPENDENTS
��RETIREES, DISABLED FORMER EMPLOYEES AND THEIR COVERED DEPENDENTS
NOT ELIGIBLE FOR MEDICARE
��RETIREES, DISABLED FORMER EMPLOYEES AND THEIR COVERED DEPENDENTS
ELIGIBLE FOR MEDICARE


HEALTHPARTNERS COST-SHARING TABLE
Self-Insured Managed-Care Option 2001 — 23
HEALTHPARTNERS COST-SHARING TABLE
The following chart outlines benefits for those enrolled in the HealthPartners self-insured option as an
active employee, a retiree, a disabled former employee, or an enrolled dependent of an active employee,
retiree or disabled former employee. All care must be provided by or coordinated by your PCC for you to
receive benefits.
For retirees, disabled former employees and their covered dependents eligible for Medicare, plan benefits
are payable after copayments and Medicare payments are considered.
This chart is just a summary of the benefits. Some services may have limits. Specific conditions, limits and
exclusions are detailed in the pages that follow the cost-sharing charts.
HEALTHPARTNERS COST-SHARING TABLE
Feature Cost-Sharing
Annual Deductible
None
Annual Out-of-Pocket Limit per
Individual None
Lifetime Maximum Benefit None
Precertification
PCC handles for you,
except treatment for medical emergency or urgent medical
need
not provided or directed by PCC
Network Physician Visits for Preventive Services
�� Well-child care; frequency/type based
on HealthPartners guidelines
You pay $10/visit to PCC,
then Plan pays 100%
�� Routine visits (annual) You pay $10/visit to PCC,
then Plan pays 100%
�� Well-woman exam (annual); no referral
required
You pay $10/visit to PCC or network OB/GYN,
then Plan pays 100%
�� Prenatal care You pay $10 for first office visit to network OB/GYN,
then Plan pays 100% for all prenatal care thereafter
�� Cancer screenings (physician services
only); frequency/type based on
HealthPartners guidelines
You pay $10/visit to PCC or referral specialist, then plan
pays 100%
��Vision
�� Examination by network
optometrist or ophthalmologist; no
referral required; frequency based
on HealthPartners guidelines
You pay $10/visit,
then Plan pays 100%
�� Eyewear Not covered;
Discount arrangements are available through the Plan

HEALTHPARTNERS COST-SHARING TABLE
24 — Self-Insured Managed-Care Option 2001
HEALTHPARTNERS COST-SHARING TABLE
Feature Cost-Sharing
Network Physician Visits Other Than Preventive Services
�� Treatment of illness or injury You pay $10/visit to PCC or referral specialist, then Plan
pays 100%
�� Office surgery You pay $10/visit to PCC or referral specialist, then Plan
pays 100%
��Office lab and x-ray
�� Billed with office visit
�� No office visit when services
rendered
Plan pays 100%
Plan pays 100%
�� Allergy testing and treatment You pay $10/visit to PCC or referral specialist, then Plan
pays 100%
Network Convenient/Urgent Care Centers
�� Services after normal PCC hours; no
referral required
You pay $10 per visit,
then Plan pays 100%
Inpatient Network Hospital Services
��Hospital semi-private room & board
and ancillary services
You pay $250/admission
(not applicable for re-admission within 30 days for the same
condition; $750 maximum/person/year),
then Plan pays 100%
�� Lab and x-ray Plan pays 100% after the hospital copayment
�� Surgeons' charges Plan pays 100% after the hospital copayment
�� Physician hospital visits Plan pays 100% after the hospital copayment
��Anesthesia Plan pays 100% after the hospital copayment
��Delivery — normal or C-section Plan pays 100% after the hospital copayment
Network Alternatives to Inpatient Hospital Care
��Skilled nursing facility (maximum of 90 days/lifetime)
Plan pays 100% after the hospital copayment
��Home-health care You pay $10/visit,
then Plan pays 100%
��Home IV therapy You pay $10/visit,
then Plan pays 100%
�� Inpatient hospice for palliative care of
terminally ill Plan pays 100% after the hospital copayment
��Outpatient hospice Plan pays 100%

HEALTHPARTNERS COST-SHARING TABLE
Self-Insured Managed-Care Option 2001 — 25
HEALTHPARTNERS COST-SHARING TABLE
Feature Cost-Sharing
Outpatient Services (treatment and services by network providers performed in a network
facility other than in the physician’s office or as an inpatient in a hospital)
�� Surgery, including
surgeon and facility
You pay $10 for PCC or referral specialist, then Plan pays
100%
�� Independent lab and
x-ray facilities
Plan pays 100%
��Hospital emergency room (medical
emergency defined on page 52)
�� For treatment of a medical
emergency in the service area
You pay $50/visit
(waived if admitted within 24 hours for the same
condition),
then Plan pays 100%
�� For treatment of a medical
emergency outside the service area
You pay 20%, the Plan pays 80% of the first $2,500;
then Plan pays 100%
�� For non-emergency care not
authorized in advance by PCP
Not covered
��Hospital observation room for up to 24
hours without admission
Same as outpatient hospital emergency room services
�� Follow-up care with PCC or referral
specialist�
You pay $10/visit for PCC or referral specialist, then Plan
pays 100%
��Ambulance (ambulance defined on
page 50; medical emergency defined on
page 52)�
�� For a medical emergency
You pay 20%
then Plan pays 80%
�� For non-emergency transportation
approved by HealthPartners and
recommended by the PCC
You pay 20%;
then Plan pays 80%;
otherwise, not covered

HEALTHPARTNERS COST-SHARING TABLE
26 — Self-Insured Managed-Care Option 2001
HEALTHPARTNERS COST-SHARING TABLE
Feature Cost-Sharing
Treatment for Mental Health Conditions by Network Providers
��Inpatient hospital or specialized
treatment facility
You pay hospital copayment,
then Plan pays 100%;
up to 30 days/year or 90 days/lifetime;
annual and lifetime maximums include inpatient care for
detoxification and treatment of substance abuse conditions
��Physician inpatient visits Plan pays 100%,
up to 30 days/year or 90 days/lifetime;
annual and lifetime maximums include inpatient care for
detoxification and treatment of substance abuse conditions
��Office/outpatient visits You pay $10/visit,
then Plan pays 100%;
up to 30 visits/year
(individual, family, group or other visits count as one visit)
Treatment for Substance Abuse Conditions by Network Providers
��Detoxification You pay hospital copayment
then Plan pays 100%;
up to 30 days/year or 90 days/lifetime;
annual and lifetime maximums include inpatient care for
detoxification and treatment of mental health conditions
�� Inpatient hospital or specialized
treatment facility
You pay hospital copayment,
then Plan pays 100%;
up to 30 days/year or 90 days/lifetime;
annual and lifetime maximums include inpatient care for
detoxification and treatment of mental health conditions
�� Physician inpatient visits Plan pays 100%;
up to 30 days/year or 90 days/lifetime;
annual and lifetime maximums include inpatient care for
detoxification and treatment of mental health conditions
��Outpatient rehabilitation You pay $10/visit;
then Plan pays 100%;
up to 30 visits/year
(individual, family, group or other visits count as one visit)

HEALTHPARTNERS COST-SHARING TABLE
Self-Insured Managed-Care Option 2001 — 27
HEALTHPARTNERS COST-SHARING TABLE
Feature Cost-Sharing
Other Network Services and Supplies
��Acupuncture (for pain relief or anesthesia only)
You pay $10/visit to referral network acupuncturist, then
Plan pays 100%
��Chiropractic services �� only for short-term treatment when there is
a reasonable expectation that a condition
will improve over a short, predictable
period of time
�� does not include maintenance or palliative
care
You pay $10/visit to referral network provider, then Plan
pays 100%;
up to 15 visits;
HealthPartners Medical Director can authorize additional
therapy,
provided the conditions noted to the left continue to apply
��Communication or interpretation
services for a ventilator-dependent
patient during an inpatient stay
Plan pays 100%
��Dental
��Medical conditions requiring oral
surgery
You pay $10 to referral network provider,
then Plan pays 100%
�� Treatment of accidental injuries to
sound natural teeth
You pay 20% to network provider,
then Plan pays 80%
��Diabetes self management training and
education �� Medical nutrition therapy
�� Referral from PCP
�� Program consistent with national standards
established by the American Diabetes
Association
You pay $10/visit,
then Plan pays 100%
��Durable medical equipment (DME) Plan pays 100% for precertified DME when obtained from
network DME vendors
�� Infertility treatments: limited to the diagnosis and treatment of
medical conditions resulting in infertility and
treatment to return the body to normal bodily
function
Covered the same as treatment for other conditions
��Nutritional supplements for the
treatment of PKU
You pay 20%,
then Plan pays 80%
�� Prosthetic devices; limited to items
noted on pages 68 and 69
Plan Pays 100% for precertified covered prosthetic devices
when obtained from network vendors; Covered wigs limited
to $350 per year
��Reconstructive and restorative surgery
that is not cosmetic in nature
Same as other surgery

HEALTHPARTNERS COST-SHARING TABLE
28 — Self-Insured Managed-Care Option 2001
HEALTHPARTNERS COST-SHARING TABLE
Feature Cost-Sharing
Other Network Services and Supplies
��Rehabilitative services: cognitive,
physical, occupational, pulmonary, and
speech therapy �� only for short-term treatment when there is
a reasonable expectation that a condition
will improve over a short, predictable
period of time
�� only to restore function lost through
illness or injury
�� does not include maintenance or palliative
care
You pay $10/visit to referral network specialist, then Plan
pays 100%;
up to 15 visits/therapy/condition;
HealthPartners Medical Director can authorize additional
therapy,
provided the conditions noted to the left continue to apply

MEDICA COST-SHARING TABLE
Self-Insured Managed-Care Option 2001 — 29
MEDICA SELF-INSURED
COST-SHARING TABLE
��ACTIVE EMPLOYEES AND THEIR COVERED DEPENDENTS
��RETIREES, DISABLED FORMER EMPLOYEES AND THEIR COVERED DEPENDENTS
NOT ELIGIBLE FOR MEDICARE
��RETIREES, DISABLED FORMER EMPLOYEES AND THEIR COVERED DEPENDENTS
ELIGIBLE FOR MEDICARE

MEDICA COST-SHARING TABLE
30 — Self-Insured Managed-Care Option 2001
MEDICA SELF-INSURED COST-SHARING TABLE
The following chart outlines benefits for those enrolled in Medica Self-Insured option as an active
employee, a retiree, a disabled former employee, or an enrolled dependent of an active employee, retiree or
disabled former employee. All care must be provided by or coordinated by your PCC for you to receive
Tier I benefits.
Medica Self-Insured allows you to refer yourself to network providers without referral from your PCC.
This is called “self-referral.” Tier II benefits apply for all covered services received directly from the self-
referral provider, as well as all covered services ordered or coordinated by the self-referral provider.
For retirees, disabled former employees, and their covered dependents eligible for Medicare, plan benefits
are payable after copayments and Medicare payments are considered.
This chart is just a summary of the benefits. Some services may have limits. Specific conditions, limits and
exclusions are detailed in the pages that follow the cost-sharing charts.
MEDICA SELF-INSURED COST-SHARING TABLE
Feature
Tier I Cost-Sharing
All covered services provided by or
coordinated by your PCC
Tier II Cost-Sharing All covered services provided by or
coordinated by self-referral network
provider
Annual Deductible None None
Annual Out-of-Pocket
Limit per Individual None
$750/person;
$5,000/family;
applies only to Tier II benefits;
copayments for Tier I services and
prescription drugs are not included
Lifetime Maximum
Benefit None None
Precertification
PCC or self-referral network provider handles for you,
except treatment for medical emergency or urgent medical need
not provided or directed by PCC
Network Physician Visits for Preventive Services
�� Well-child care; frequency
and type based on Medica
guidelines
You pay $10/visit to PCC,
then Plan pays 100%
Not covered
�� Routine visits (annual) You pay $10/visit to PCC,
then Plan pays 100%
You pay $25/visit,
then Plan pays 100%
�� Well-woman exam
(annual)
You pay $10/visit to a network OB/GYN,
then Plan pays 100%
�� Prenatal care You pay $10/visit,
then Plan pays 100%
You pay $25/visit,
then Plan pays 100%
�� Cancer screenings (physician services only);
frequency and type based on
Medica guidelines
You pay $10/visit to PCC or referral
specialist,
then Plan pays 100%
You pay $25/visit,
then Plan pays 100%

MEDICA COST-SHARING TABLE
Self-Insured Managed-Care Option 2001 — 31
MEDICA SELF-INSURED COST-SHARING TABLE
Feature
Tier I Cost-Sharing
All covered services provided by or
coordinated by your PCC
Tier II Cost-Sharing All covered services provided by or
coordinated by self-referral network
provider
Network Physician Visits for Preventive Services (continued)
��Vision
��Examination by
network optometrist or
ophthalmologist; no
referral required;
frequency based on
Medica schedule
You pay $15/visit,
then Plan pays 100%
��Eyewear Not covered; discount arrangements are available through the Plan
Network Physician Visits Other Than Preventive Services
�� Treatment of illness or
injury
You pay $10/visit to PCC or referral
specialist, then Plan pays 100%
You pay $25/visit,
then Plan pays 100%
�� Office surgery You pay $10/visit to PCC or referral
specialist, then Plan pays 100%
You pay $25/visit
then Plan pays 100%
��Office lab and x-ray
�� Billed with office
visit (you already
paid office visit
copayment)
�� No office visit billed
when services
rendered
Plan pays 100%
You pay $10,
then Plan pays 100%
Plan pays 100%
You pay $25,
then Plan pays 100%
�� Allergy testing and
treatment
You pay $10/visit to PCC or referral
specialist, then Plan pays 100%
You pay $25/visit,
then Plan pays 100%
Network Convenient/Urgent Care Centers
�� Services after normal
PCC hours; no referral
required
You pay $10 per visit,
then Plan pays 100%
Not covered
Inpatient Network Hospital Services
��Hospital semi-private
room & board and
ancillary services
You pay $250/admission
(copayment waived for re-admission
within 30 days for the same condition;
$750 maximum/person/year),
then Plan pays 100%
You pay $500/admission
and 30% (up to $450),
then Plan pays balance of network
facility charges
�� Lab and x-ray Plan pays 100% after the hospital
copayment All included in the above hospital
copayment and coinsurance
�� Surgeons' charges Plan pays 100% after the hospital
copayment
You pay 30%, then Plan pays 70%
(not subject to the $450 maximum if
billed separately from facility charge)

MEDICA COST-SHARING TABLE
32 — Self-Insured Managed-Care Option 2001
MEDICA SELF-INSURED COST-SHARING TABLE
Feature
Tier I Cost-Sharing
All covered services provided by or
coordinated by your PCC
Tier II Cost-Sharing All covered services provided by or
coordinated by self-referral network
provider
Inpatient Network Hospital Services (continued)
�� Physician hospital visits Plan pays 100% after the hospital
copayment
You pay 30%, then Plan pays 70%
(not subject to the $450 maximum if
billed separately from facility charge)
�� Anesthesia Plan pays 100% after the hospital
copayment
All included in the above hospital
copayment and coinsurance, provided
billed with the facility charge;
otherwise, you pay 30%, then Plan
pays 70%
(not subject to the $450 maximum)
�� Delivery — normal or
C-section physician
charges
Plan pays 100% after the hospital
copayment
You pay 30%, then Plan pays 70%
(not subject to the $450 maximum)
Network Alternatives to Inpatient Hospital Care: must be precertified. Call 1-800-962-9497
�� Skilled nursing facility (maximum of 90 days/lifetime
of Tier I and Tier II benefits
combined)
You pay 20%,
then Plan pays 80%
You pay 30% (no maximum),
then Plan pays 70%
�� Home-health care You pay 20%,
then Plan pays 80%;
For high-risk prenatal care, Plan pays
100%
You pay 30% (no maximum),
then Plan pays 70%
�� Home IV therapy You pay 20%,
then Plan pays 80%
You pay 30% (no maximum),
then Plan pays 70%
�� Inpatient hospice for
palliative care of
terminally ill
Plan pays 100% Not covered

MEDICA COST-SHARING TABLE
Self-Insured Managed-Care Option 2001 — 33
MEDICA SELF-INSURED COST-SHARING TABLE
Feature
Tier I Cost-Sharing
All covered services provided by or
coordinated by your PCC
Tier II Cost-Sharing All covered services provided by or
coordinated by self-referral network
provider
Outpatient Services (treatment and services by network providers performed in a network
facility other than in the physician’s office or as an inpatient in a hospital)
�� Surgery
�� Facility
You pay $100,
then Plan pays 100%
You pay 30% (up to $450),
then Plan pays 100%
�� Surgeon� Plan pays 100% You pay 30% (no maximum),
then Plan pays 70%
�� Independent lab and x-ray
facilities billed outside the
PCC system
You pay $15/test or x-ray,
then Plan pays 100%
You pay $25/test or x-ray,
then Plan pays 100%
��Hospital emergency room
facility charge (medical
emergency defined on
page 52)
�� For treatment of a
medical emergency
You pay $50/visit
(waived if admitted within 24 hours for the same condition),
then Plan pays 100%
�� For non-emergency
care not authorized in
advance by PCC
Not covered
��Hospital observation
room for up to 24 hours
without admission
You pay $100,
then Plan pays 100%
You pay 30% (up to $450),
then Plan pays 100%
�� Follow-up care� You pay $10/visit for PCC or referral
specialist,
then Plan pays 100%
You pay $25/visit,
then Plan pays 100%
��Ambulance (see
definitions of ambulance,
page 50, and medical
emergency, page 52)�
�� For a medical
emergency
You pay 20%,
then Plan pays 80%
�� For non-emergency
transportation
approved by Medica
and recommended by
the PCC/self-referral
network provider
You pay 20%,
then Plan pays 80%;
otherwise, not covered
You pay 30% (no maximum),
then Plan pays 70%;
otherwise, not covered

MEDICA COST-SHARING TABLE
34 — Self-Insured Managed-Care Option 2001
MEDICA SELF-INSURED COST-SHARING TABLE
Feature
Tier I Cost-Sharing
All covered services provided by or
coordinated by your PCC
Tier II Cost-Sharing All covered services provided by or
coordinated by self-referral network
provider
Network Treatment for Mental Health Conditions by Network Providers:
must be precertified by UBH @ 1-800-848-8327
�� Inpatient hospital,
inpatient specialized
treatment facility or
partial program
You pay standard inpatient hospital
copayment, then Plan pays 100%;
up to 30 days/year, up to 90
days/lifetime; annual and lifetime
maximums include inpatient care for
detoxification and treatment of
substance abuse conditions
Not covered
��Physician inpatient visits Plan pays 100%;
up to 30 days/year, up to 90
days/lifetime; annual and lifetime
maximums include inpatient care for
detoxification and treatment of
substance abuse conditions
Not covered
��Office/outpatient visits You pay $15/visit,
then Plan pays 100%;
up to 30 visits/year
(individual, family, group or other
visits count as one visit)
Not covered

MEDICA COST-SHARING TABLE
Self-Insured Managed-Care Option 2001 — 35
MEDICA SELF-INSURED COST-SHARING TABLE
Feature
Tier I Cost-Sharing
All covered services provided by or
coordinated by your PCC
Tier II Cost-Sharing All covered services provided by or
coordinated by self-referral network
provider
Treatment for Substance Abuse Conditions by Network Providers:
must be precertified byUBH @ 1-800-848-8327
��Detoxification You pay standard inpatient hospital
copayment, then Plan pays 100%;
up to 30 days/year, up to 90
days/lifetime; annual and lifetime
maximums include inpatient care for
detoxification and treatment of mental
health conditions
Not covered
�� Inpatient hospital,
inpatient specialized
treatment facility, or
partial program
You pay standard inpatient hospital
copayment, then Plan pays 100%;
up to 30 days/year, up to 90
days/lifetime; annual and lifetime
maximums include inpatient care for
detoxification and treatment of mental
health conditions
Not covered
�� Physician inpatient visits Plan pays 100%;
up to 30 days/year, up to 90
days/lifetime; annual and lifetime
maximums include inpatient care for
detoxification and treatment of mental
health conditions
Not covered
�� Outpatient rehabilitation You pay $15/visit,
then Plan pays 100%;
up to 30 visits/year (individual,
family, group or other visits count as
one visit)
Not covered

MEDICA COST-SHARING TABLE
36 — Self-Insured Managed-Care Option 2001
MEDICA SELF-INSURED COST-SHARING TABLE
Feature
Tier I Cost-Sharing
All covered services provided by or
coordinated by your PCC
Tier II Cost-Sharing All covered services provided by or
coordinated by self-referral network
provider
Other Network Services and Supplies: call 1-800-962-9497
��Acupuncture (only for medically necessary
services)
You pay $15/visit
then Plan pays 100%
You pay $25/visit,
then Plan pays 100%
��Chiropractic services �� only for short-term
treatment when there is a
reasonable expectation
that a condition will
improve over a short,
predictable period of time
�� does not include
maintenance or palliative
care
You pay $15/visit,
then Plan pays 100%;
up to 15 visits
(maximum includes Tier II benefits);
Medica Medical Director or designee
can authorize additional therapy,
provided the conditions noted to the
left continue to apply
You pay $25/visit
then Plan pays 100%;
up to 15 visits
(maximum includes Tier I benefits);
Medica Medical Director or designee
can authorize additional therapy,
provided the conditions noted to the
left continue to apply
�� Communication or
interpretation services for
a ventilator-dependent
patient during an
inpatient stay
Plan pays 100%,
up to 120 hours/lifetime
(maximum includes Tier II benefits)
You pay 30% (no maximum),
then Plan pays 70%,
up to 120 hours/lifetime
(maximum includes Tier I benefits)
�� Dental Limited to the surgical procedures
commonly viewed as medical rather
than dental in nature (same benefits as
other outpatient surgery) and certain
services or supplies for an accidental
injury to sound natural teeth if the
service is done or supply provided as
part of the initial emergency treatment
(same benefits as other emergency
treatment)
Limited to the surgical procedures
commonly viewed as medical rather
than dental in nature (same benefits as
other outpatient surgery) and certain
services or supplies for an accidental
injury to sound natural teeth if the
service is done or supply provided as
part of the initial emergency treatment
(same benefits as other emergency
treatment)
��Diabetes self management
training and education �� Medical nutrition therapy
�� Referral from PCP
�� Program consistent with
national standards
established by the
American Diabetes
Association
You pay $15/visit,
then Plan pays 100%
You pay $25/visit,
then Plan pays 100%

MEDICA COST-SHARING TABLE
Self-Insured Managed-Care Option 2001 — 37
MEDICA SELF-INSURED COST-SHARING TABLE
Feature
Tier I Cost-Sharing
All covered services provided by or
coordinated by your PCC
Tier II Cost-Sharing All covered services provided by or
coordinated by self-referral network
provider
Other Network Services and Supplies (continued): must be precertified. Call 1-800-962-9497
�� Durable medical
equipment (DME)
Plan pays 100% for initial DME;
precertification required if cost is
$1,500 or greater
For replacement, repair, or revision of
artificial eyes, limbs, and breast
prosthesis made necessary by normal
wear and usage, you pay 20%,
then Plan pays 80%
You pay 30% (no maximum) for initial
DME, then Plan pays 70%;
precertification required if cost is
$1,500 or greater
�� Infertility treatments: limited to the diagnosis and
treatment of medical
conditions resulting in
infertility and treatment to
return the body to normal
bodily function
Covered the same as treatment for
other conditions
Covered the same as treatment for
other conditions
��Nutritional supplements
for the treatment of PKU
You pay 20%,
then Plan pays 80%
You pay 30% (no maximum),
then Plan pays 70%
�� Prosthetic devices;
limited to items noted on
pages 68 and 69
Plan Pays 100% for precertified
covered prosthetic devices when
obtained from network vendors;
Covered wigs limited to $350 per year
You pay 30%,
then plan pays 70%;
Covered wigs limited to $350 per
year
��Reconstructive and
restorative surgery that is
not cosmetic in nature
Plan pays 100% You pay 30% (no maximum) for
precertified surgery,
then plan pays 70%
��Rehabilitative services:
cognitive, physical,
occupational, pulmonary,
and speech therapy �� only for short-term
treatment when there is a
reasonable expectation
that a condition will
improve over a short,
predictable period of time
�� only to restore function
lost through illness or
injury
�� does not include
maintenance or palliative
care
You pay $15/visit,
then Plan pays 100%;
up to 15 visits/therapy/condition
(maximum includes Tier II benefits);
Medica Medical Director or designee
can authorize additional therapy,
provided the conditions noted to the
left continue to apply
You pay $25/visit,
then Plan pays 100%
up to 15 visits/therapy/condition
(maximum includes Tier I benefits);
Medica Medical Director or designee
can authorize additional therapy,
provided the conditions noted to the
left continue to apply
�� Treatment to lighten or
remove the coloration of a
port wine stain
You pay $10/visit,
then Plan pays 100%
You pay $25/visit,
then Plan pays 100%


SELECTADVANTAGE COST-SHARING TABLE
Self-Insured Managed-Care Option 2001 — 39
SELECTADVANTAGE
COST-SHARING TABLE
��ACTIVE EMPLOYEES AND THEIR COVERED DEPENDENTS
��RETIREES, DISABLED FORMER EMPLOYEES AND THEIR COVERED DEPENDENTS
NOT ELIGIBLE FOR MEDICARE
��RETIREES, DISABLED FORMER EMPLOYEES AND THEIR COVERED DEPENDENTS
ELIGIBLE FOR MEDICARE

SELECTADVANTAGE COST-SHARING TABLE
40 — Self-Insured Managed-Care Option 2001
SELECTADVANTAGE COST-SHARING TABLE
The following chart outlines benefits for those enrolled in the SelectAdvantage self-insured option as an
active employee, a retiree, a disabled former employee, or an enrolled dependent of an active employee,
retiree or disabled former employee. For services on or before June 30, 2001, all care must be provided by
or coordinated by your PCP for you to receive benefits. For services on or after July 1, 2001, all care must
be provided by a network provider, but need not be directed by a PCP.
For retirees, disabled former employees, and their covered dependents eligible for Medicare, plan benefits
are payable after copayments and Medicare payments are considered.
This chart is just a summary of the benefits. Some services may have limits. Specific conditions, limits and
exclusions are detailed in the pages that follow the cost-sharing charts.
SELECTADVANTAGE COST-SHARING TABLE
Feature Cost-Sharing
Annual Deductible None
Annual Out-of-Pocket Limit per
Individual None
Lifetime Maximum Benefit None
Precertification
PCP handles for you,
except treatment for medical emergency or urgent medical
need
not provided or directed by PCP
Network Physician Visits for Preventive Services
�� Well-child care
frequency/type based on
SelectAdvantage guidelines
�� For services on and before 6/30/01
�� For services on and after 7/01/01
You pay $10/visit to PCP,
then Plan pays 100%
You pay $10/visit,
then Plan pays 100%
�� Routine visits (annual)
�� For services on or before 6/30/01
�� For services on and after 7/01/01
You pay $10/visit to PCP,
then Plan pays 100%
You pay $10/visit,
then Plan pays 100%
�� Well-woman exam (annual)
�� For services on or before 6/30/01
�� For services on and after 7/01/01
You pay $10/visit to PCP or network OB/GYN,
then Plan pays 100%; no referral required
You pay $10/visit.
then Plan pays 100%
�� Prenatal care You pay $10 for first office visit
to network OB/GYN,
then Plan pays 100% for all
prenatal care thereafter

SELECTADVANTAGE COST-SHARING TABLE
Self-Insured Managed-Care Option 2001 — 41
SELECTADVANTAGE COST-SHARING TABLE
Feature Cost-Sharing
Network Physician Visits for Preventive Services (continued)
��Cancer screenings
(physician services only)
frequency and type based
on SelectAdvantage guidelines
�� For services on or before 6/30/01
�� For services on or after 7/01/01
You pay $10/visit to PCP or $15/visit to referral specialist,
then plan pays 100%
You pay $10/visit,
then Plan pays 100%
��Vision
�� Examination by network
optometrist or ophthalmologist no
referral required; frequency based
on SelectAdvantage guidelines
�� For services on or before
6/30/01
�� For services on or after 7/01/01
You pay $15/visit,
then Plan pays 100%
You pay $10/visit,
then Plan pays 100%
�� Eyewear Not covered;
Discount arrangements are available through the Plan
Network Physician Visits Other Than Preventive Services
�� Treatment of illness or injury
�� For services on or before 6/30/01
�� For services on or after 7/01/01
You pay $10/visit to PCP or $15/visit to referral specialist,
then Plan pays 100%
You pay $10/visit,
then Plan pays 100%
��Office surgery
�� For services on or before 6/30/01
�� For services on or after 7/01/01
You pay $10/visit to PCP or $15/visit to referral specialist,
then Plan pays 100%
You pay $10/visit,
then Plan pays 100%
��Office lab and x-ray
�� Billed w. office visit
�� No office visit when services
rendered
Plan pays 100%
You pay $10,
then Plan pays 100%
Note: retirees, disabled former employees, and their
covered dependents eligible for Medicare have no
copayment for office lab and x-ray services
��Allergy testing and treatment
�� For services on or before 6/30/01
�� For services on or after 7/01/01
You pay $10/visit to PCP or $15/visit to referral specialist,
then Plan pays 100%
You pay $10/visit,
then Plan pays 100%

SELECTADVANTAGE COST-SHARING TABLE
42 — Self-Insured Managed-Care Option 2001
SELECTADVANTAGE COST-SHARING TABLE
Feature Cost-Sharing
Inpatient Network Hospital Services
�� Hospital semi-private room & board
and ancillary services
You pay $250/admission,
(not applicable for re-admission within 30 days for the
same condition; maximum $750/person/year),
then Plan pays 100%;
�� Lab and x-ray Plan pays 100% after hospital copayment
�� Surgeons' charges Plan pays 100% after hospital copayment
�� Physician hospital visits Plan pays 100% after hospital copayment
�� Anesthesia Plan pays 100% after hospital copayment
�� Delivery — normal or C-section Plan pays 100% after hospital copayment
Network Alternatives to Inpatient Hospital Care
�� Skilled nursing facility (maximum of 90 days/lifetime)
Plan pays 100% after hospital copayment
Note: retirees, disabled former employees, and their
covered dependents eligible for Medicare have no hospital
copayment for approved skilled nursing care facilities
���Home-health care Plan pays 100%
�� Home IV therapy Plan pays 100%
�� Inpatient hospice for palliative care of
terminally ill Plan pays 100% after hospital copayment

SELECTADVANTAGE COST-SHARING TABLE
Self-Insured Managed-Care Option 2001 — 43
SELECTADVANTAGE COST-SHARING TABLE
Feature Cost-Sharing
Outpatient Services (treatment and services by network providers performed in a network
facility other than in the physician’s office or as an inpatient in a hospital)
�� Surgery, including
surgeon and facility
You pay $100/procedure,
then Plan pays 100%
Plan pays 100%
�� Independent lab and x-ray
facilities
�� For services on or before 6/30/01
�� For services on or after 7/01/01
You pay $15/test or x-ray,
then Plan pays 100%
You pay $10/test or x-ray,
then Plan pays 100%
Note: retirees, disabled former employees, and their
covered dependents eligible for Medicare have no
copayment for independent lab and x-rays; the Plan pays
100%
��Hospital emergency room (medical
emergency defined on page 52)
�� For treatment of a medical
emergency
You pay $50/visit
(waived if admitted within 24 hours for the same
condition),
then Plan pays 100%
Note: retirees, disabled former employees, and their
covered dependents eligible for Medicare have a $35/visit
copayment
�� For non-emergency care Not covered
��Hospital observation room for up to 24
hours without admission
Same as outpatient hospital emergency room services
�� Follow-up care�
�� For services on or before 6/30/01
�� For services on or after 7/01/01
You pay $10/visit for PCP or $15/visit for referral
specialist, then Plan pays 100%
You pay $10/visit,
then Plan pays 100%
��Ambulance (see definitions of
ambulance, page 50, and medical
emergency, page 52)�
�� For non-emergency approved by
SelectAdvantage
Plan pays 100%;
otherwise, you pay 100%

SELECTADVANTAGE COST-SHARING TABLE
44 — Self-Insured Managed-Care Option 2001
SELECTADVANTAGE COST-SHARING TABLE
Feature Cost-Sharing
Treatment for Mental Health Conditions by Network Providers
��Inpatient hospital or specialized
treatment facility
You pay hospital copayment
then Plan pays 100%;
up to 30 days/year, up to 90 days/lifetime;
annual and lifetime maximums include inpatient care for
detoxification and treatment of substance abuse conditions
��Physician inpatient visits Plan pays 100%;
up to 30 days/year, up to 90 days/lifetime;
annual and lifetime maximums include inpatient care for
detoxification and treatment of substance abuse conditions
��Office/outpatient visits
up to 30 visits/year (individual, family
group or other visits count as one visit,
except retirees, disabled former
employees, and their covered dependents
eligible for Medicare have up to 20
visits/year
�� For services on or before 6/30/01
�� For services on or after 7/01/01
You pay $15/visit,
then Plan pays 100%
Note: retirees, disabled former employees, and their
covered dependents eligible for Medicare have a $10/visit
copayment
You pay $10/visit
then Plan pays 100%

SELECTADVANTAGE COST-SHARING TABLE
Self-Insured Managed-Care Option 2001 — 45
SELECTADVANTAGE COST-SHARING TABLE
Feature Cost-Sharing
Treatment for Substance Abuse Conditions from Network Providers
��Detoxification You pay hospital copayment,
then Plan pays 100%
�� Inpatient hospital or specialized
treatment facility
You pay hospital copayment,
then Plan pays 100%;
up to 30 days/year, up to 90 days/lifetime;
annual and lifetime maximums include inpatient care for
detoxification and treatment of mental health conditions
�� Physician inpatient visits Plan pays 100%,
up to 30 days/year, up to 90 days/lifetime;
annual and lifetime maximums include inpatient care for
detoxification and treatment of mental health conditions
��Outpatient rehabilitation
up to 30 visits/year (individual, family
group or other visits count as one visit),
except retirees, disabled former
employees, and their covered dependents
eligible for Medicare have up to 20
visits/year
�� For services on or before 6/30/01
�� For services on or after 7/01/01
You pay $15/visit,
then Plan pays 100%
Note: retirees, disabled former employees, and their
covered dependents eligible for Medicare have a $10/visit
copayment
You pay $10/visit
then Plan pays 100%

SELECTADVANTAGE COST-SHARING TABLE
46 — Self-Insured Managed-Care Option 2001
SELECTADVANTAGE COST-SHARING TABLE
Feature Cost-Sharing
Other Network Services and Supplies
��Acupuncture (for treatment of pain or anesthesia only) �� For services on or before 6/30/01
�� For services on or after 7/01/01
You pay $15/visit to referral specialist,
then Plan pays 100%
You pay $10/visit,
then Plan pays 100%
Note: acupuncture is not covered for retirees, disabled
former employees, and their covered dependents eligible
for Medicare
��Chiropractic services �� Only for short-term treatment when there is
a reasonable expectation that a condition
will improve over a short, predictable
period of time;
�� does not include maintenance or palliative
care �� For services on or before 6/30/01
�� For services on or after 7/01/01
up to 15 visits within 60 consecutive days/incidence,
measured from start of treatment; SelectAdvantage Medical
Director can authorize additional services, provided the
conditions noted to the left continue to apply
You pay $15/visit to referral specialist,
then Plan pays 100%
You pay $10/visit,
then Plan pays 100%
Note: chiropractic services are not covered for retirees,
disabled former employees, and their covered dependents
eligible for Medicare
��Communication or interpretation
services for a ventilator-dependent
patient during an inpatient stay
Plan pays 100%
��Dental Not covered
��Diabetes self management training and
education
��Medical nutrition therapy
��Referral from PCP
�� Program consistent with national
standards established by the
American Diabetes Association
Plan pays 100% when services are obtained at a network
hospital.
��Durable medical equipment (DME),
prosthetics, etc.
Plan pays 100% for precertified
DME when obtained from network DME vendor
�� Infertility treatments: limited to the diagnosis and treatment of
medical conditions resulting in infertility and
treatment to return body to normal bodily
function
Covered the same as treatment for other conditions
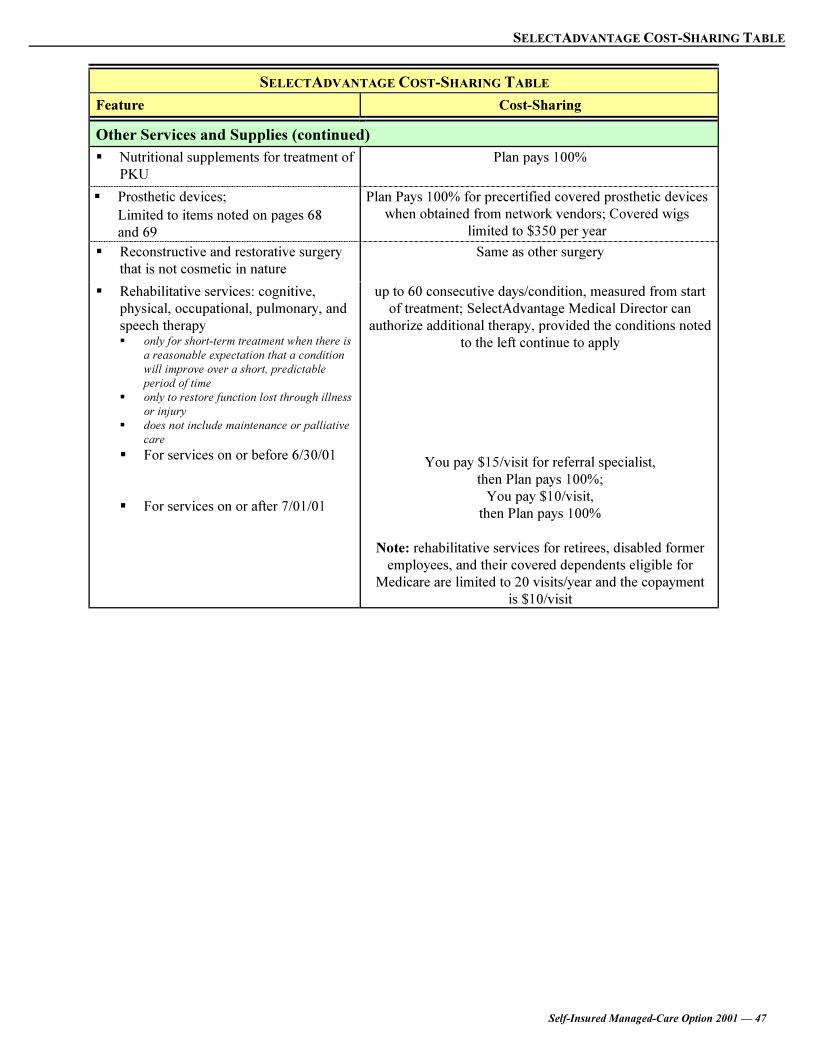
SELECTADVANTAGE COST-SHARING TABLE
Self-Insured Managed-Care Option 2001 — 47
SELECTADVANTAGE COST-SHARING TABLE
Feature Cost-Sharing
Other Services and Supplies (continued)
��Nutritional supplements for treatment of
PKU
Plan pays 100%
�� Prosthetic devices;
Limited to items noted on pages 68
and 69
Plan Pays 100% for precertified covered prosthetic devices
when obtained from network vendors; Covered wigs
limited to $350 per year
��Reconstructive and restorative surgery
that is not cosmetic in nature
Same as other surgery
��Rehabilitative services: cognitive,
physical, occupational, pulmonary, and
speech therapy �� only for short-term treatment when there is
a reasonable expectation that a condition
will improve over a short, predictable
period of time
�� only to restore function lost through illness
or injury
�� does not include maintenance or palliative
care
�� For services on or before 6/30/01
�� For services on or after 7/01/01
up to 60 consecutive days/condition, measured from start
of treatment; SelectAdvantage Medical Director can
authorize additional therapy, provided the conditions noted
to the left continue to apply
You pay $15/visit for referral specialist,
then Plan pays 100%;
You pay $10/visit,
then Plan pays 100%
Note: rehabilitative services for retirees, disabled former
employees, and their covered dependents eligible for
Medicare are limited to 20 visits/year and the copayment
is $10/visit


DEFINITIONS
Self-Insured Managed-Care Option 2001 — 49
DEFINITIONS

DEFINITIONS
50 — Self-Insured Managed-Care Option 2001
DEFINITIONS
A number of the terms used in this supplement have the specific meanings noted here.
Alternative care means care and services instead of continued inpatient care in an acute care hospital. The
alternative care must be recommended to you by your physician, tailored to your specific health needs, and
approved by the appropriate third-party administrator. Such care is designed to provide special assistance if
you have a catastrophic or chronic illness. Nurses work with you and your family members, your physician,
appropriate hospital staff and other providers to develop a plan of care specific to your health needs.
Alternative care might include a home-care program or transfer from an inpatient hospital setting to a
rehabilitation facility or extended care facility. Alternative benefits may be provided on a case-by-case
basis, subject to determinations made by the appropriate third-party administrator.
Ambulance means the following requirements are met:
�� Provided by an authorized agency in a vehicle staffed by trained personnel, equipped to handle
medical emergencies, and
�� Transport you from the place where you are injured or stricken by illness/disease to the nearest hospital
where treatment can be provided, or
�� Transport you from a hospital unable to treat your physical condition to the nearest hospital that can
treat your physical condition or hospital affiliated with your care network, or
�� Transport you from a hospital to the nearest convalescent or rehabilitation facility or hospice with
available space to which you are moved upon discharge, or
�� Transport you from a hospital, a convalescent, or rehabilitation facility to your home, or a hospice, or
�� Transport you from a non-network hospital to a network hospital if approved in advance by the third-
party administrator.
Ambulatory surgical facility or surgery center means a licensed facility equipped and operated
primarily for the purpose of performing surgical procedures. The facility must have:
�� Continuous physician services and registered professional nursing services whenever a patient is in the
facility;
�� A certified anesthesiologist attending whenever general or spinal anesthesia is performed;
�� Full-time skilled nursing services in the operating and recovery rooms, and personnel and equipment to
handle medical emergencies; and
�� A written agreement with a nearby hospital for the immediate transfer of patients in case of an
emergency.
The facility must not provide services or accommodations for overnight stays.
Birthing center means a facility operated under the direction of at least one doctor specializing in
obstetrics and gynecology, with a doctor or legally qualified midwife present at all births and during the
immediate postpartum period. Full-time skilled nurses must be present in the delivery and recovery rooms.
In addition, the birthing center must have:
��At least two beds or birthing rooms;
�� The equipment and trained personnel needed to handle medical emergencies related to complications
of labor and newborn abnormalities; and
��A written agreement with a nearby hospital for the immediate transfer of patients in case of emergency.
Benefits for services at a network birthing center are the same as those for outpatient hospital care.

DEFINITIONS
Self-Insured Managed-Care Option 2001 — 51
Convenient/Urgent Care Center means a health-care facility whose primary purpose is to offer and
provide immediate, short-term medical care for minor, immediate medical conditions. For HealthPartners
and Medica Self-Insured participants, access to these centers is considered the same as a PCC office visit
when the care is required on an urgent basis after normal PCC clinic hours.
Copayment means a fixed dollar amount that you must pay each time you receive a particular covered
service. If the Unisys plan is the secondary plan, copayments required by the primary plan are not
reimbursed through this Plan when this Plan is secondary payer.
The copayments that apply to specific services under your plan are noted in the Cost-Sharing Table for
your Plan. Refer to the information beginning on:
�� Page 15 for Aetna U.S. Healthcare
�� Page 21 for HealthPartners
�� Page 29 for Medica Self-Insured
�� Page 39 for SelectAdvantage
Cosmetic services and procedures improve physical appearance but do not correct or improve a
physiological function and are not medically necessary. These services are not covered under the Plan.
Course of treatment means a planned program of services or supplies furnished by a health-care provider
or team of providers. The program must be:
�� Developed in connection with the diagnosis or treatment of an illness or injury,
�� Of a definite duration, and
�� Approved by your PCP/PCC* **.
Custodial supportive care means services and supplies that are primarily for meeting personal needs in
conducting the activities of daily living. Some examples of custodial supportive care are:
�� Services and supplies furnished mainly to train or assist in personal hygiene and other activities of
daily living rather than to provide therapeutic treatment (activities of daily living include, but are not
limited to: bathing, feeding, taking oral medications, walking, getting in and out of bed, and dressing).
�� Preparation of special diets and supervision of medications that are ordinarily self-administered.
�� Services and supplies that can safely and adequately be provided by persons without the technical
skills or professional training of a covered health-care provider.
Custodial supportive care is not covered under the Plan.
Designated transplant facility means a hospital that has entered into a separate contract with the
appropriate third-party administrator to provide certain transplant-related health services to members
receiving transplants. Once you have been evaluated and listed as a potential recipient at a designated
transplant facility, you are required to remain with that designated transplant facility, unless it is medically
necessary for the transplant to be rendered at another facility. If you choose independently to be listed at
additional transplant facilities, any charges incurred for services provided by the additional facility(ies) are
not covered under the Plan.
* Note for Medica Self-Insured: Medica allows you to refer yourself to network providers without referral from
your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. Copayments and
coinsurance are higher under Tier II than when you obtain a referral from your PCC (Tier I).
** Note for SelectAdvantage for services on or after July 1, 2001: SelectAdvantage allows you top refer yourself to
any network provider. This is called “self-referral.”

DEFINITIONS
52 — Self-Insured Managed-Care Option 2001
Diabetic supply means insulin and disposable supplies used for the treatment and control of diabetes.
Covered disposable supplies include glucose and ketone test strips, lancettes, syringes, and supplies for
insulin pumps, such as tubing. They do not include alcohol swabs that have a use other than the treatment
of diabetes or a medical condition.
Diabetic supplies are covered under the separate Prescription Drug Program offered through Unisys.
Glucometers and insulin pumps are considered durable medical equipment and are covered under the
medical portion of the Plan described in this booklet.
Drugs or medicines dispensed by a pharmacy are payable under the separate Prescription Drug Program
offered through Unisys.
Take-home drugs billed by the hospital as part of your confinement or outpatient services, and drugs
dispensed by your doctor’s office for which there is a charge are considered under the appropriate benefit
(that is, inpatient care, outpatient hospital care, or office visit) and are subject to the appropriate copayment
rates noted in the cost-sharing charts beginning on the following pages:
�� Page 15 for Aetna U.S. Healthcare
�� Page 21 for HealthPartners
�� Page 29 for Medica Self-Insured
�� Page 39 for SelectAdvantage
Elective admission means an admission that is scheduled in advance.
Elective surgery means a surgical procedure that is scheduled in advance.
Emergency means a condition for which symptoms are severe and occur suddenly, resulting in the need
for immediate medical attention, that is found to be necessary, generally provided within four (4) hours of
onset of the condition, to:
�� Preserve life, or
�� Prevent serious impairment to bodily function, organs, or parts, or
�� Prevent placing your physical or mental health in serious jeopardy.
Examples of medical emergencies include, but are not limited to:
�� Difficulty swallowing
�� Fractures
�� Heart attach or suspected
heart attack
�� High fever in infants
�� Loss of consciousness
�� Poisoning
�� Severe burns
�� Severe shortness of breath
�� Suspected overdose of
medication
�� Uncontrolled bleeding
Medically necessary treatment in these cases is considered emergent care and is covered, regardless of
where you are or what covered provider renders the care. Treatment may include the use of a hospital's
emergency room and emergency transportation by an ambulance. Follow-up care, however, must be
provided by or coordinated by your PCP/PCC* ** in order for benefits to be payable.
When reviewing services for coverage as emergency services, the appropriate third-party administrator
imposes the standard that a reasonable layperson would believe that the circumstances required immediate
medical care that could not wait until the next working day or next available office hours.
* Note for Medica Self-Insured: Medica allows you to refer yourself to network providers without referral from
your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. Copayments and
coinsurance are higher under Tier II than when you obtain a referral from your PCC (Tier I).
** Note for SelectAdvantage for services on or after July 1, 2001: SelectAdvantage allows you top refer yourself to
any network provider. This is called “self-referral.”

DEFINITIONS
Self-Insured Managed-Care Option 2001 — 53
The steps you should take in a medical emergency are provided beginning on page 10.
If you are in doubt about whether your situation constitutes a medical emergency, call your PCP/PCC
or call Member Services at the telephone number listed inside the front cover of this supplement.
Health-care providers means providers who are: not members of your household or family members; and
are practicing within the scope of their applicable licenses or, in the absence of licensing requirements, are
certified by the appropriate professional association. For benefits to be payable, the services provided must
be covered services under the Plan. Covered health-care providers include, but are not limited to:
�� Certified Nurse Anesthetist — CNA.
�� Doctor or physician — Doctor of Medicine
(MD), Doctor of Osteopathy (DO), Doctor of
Podiatry (DPM), Doctor of Chiropractic
(DC), Doctor of Optometry (OD), or
Christian Science Practitioner
�� Mental disorder providers — licensed
masters social worker (MSW), licensed
masters psychiatric nurse (MSN), doctoral
psychologist (PhD, PsyD, or EdD), and
Doctor of Medicine (MD)
�� Midwife — legally qualified midwife
�� Nurse — licensed practical nurse (LPN),
licensed vocational nurse (LVN), or
registered nurse (RN)
�� Physical therapist
�� Physician’s Assistant (PA), if legally
qualified
�� Physiologist
�� Physiotherapist
�� Registered Physical Therapist (RPT)
�� Speech pathologist
Homebound means that leaving the home would directly and negatively impact the patient’s physical
health. The home could mean the patient’s own dwelling, a relative’s home, an apartment complex that
provides assisted living services, or some other type of institution. However, an institution is not
considered to be the home if it is a hospital or skilled nursing facility.
Home-health agency means a licensed agency or organization specializing in providing medical care and
treatment in the home. To be covered, the agency and the services must be precertified by the appropriate
third-party administrator and:
�� Be primarily engaged in providing skilled nursing services and other therapeutic services;
�� Have policies established by a professional group associated with the agency; this professional group
must include at least one physician and at least one registered graduate nurse to govern the services
provided;
�� Have a full-time administrator and provide full-time supervision of services by a physician or
registered graduate nurse;
�� Maintain a complete medical record on each individual; and
�� Be licensed to operate in the state in which the facility is located.
Hospice care means a defined inpatient or outpatient program of care for individuals with a terminal
condition whose life expectancy is six months or less. To be covered, the program must be precertified by
the appropriate third-party administrator. Although palliative care and respite care normally are excluded
from any benefits coverages, they may be considered when approved by the appropriate third-party
administrator through a precertified hospice program.
Hospice services are comprehensive palliative medical care and supportive social, emotional, and spiritual
services that are provided to the terminally ill and their families, primarily in the patient’s home.
A hospice interdisciplinary team, composed of professionals and volunteers, coordinates an individualized
plan of care for each patient and family. The goal of hospice care is to make patients as comfortable as
possible to enable them to live their final days to the fullest in the comfort of their own homes and with
loved ones.
Respite care is a form of hospice services that gives the patient’s uncompensated primary caregivers (that

DEFINITIONS
54 — Self-Insured Managed-Care Option 2001
is, family members or friends) rest and/or relief when necessary to maintain a terminally ill covered patient
at home.
Hospital means an institution that is engaged primarily in providing medical care and treatment of sick and
injured persons on an inpatient basis at the patient’s expenses and fully meets these criteria:
�� Is accredited as a hospital by the Joint Commission on accreditation of Healthcare Organizations;
�� Is approved by Medicare as a hospital;
�� Maintains inpatient diagnostic and treatment services for surgical and medical patients;
�� Provides treatment and care of injured and sick persons by or under the supervision of physicians; and
�� Provides 24-hour nursing service by or under the supervision of registered nurses..
The following are not considered to be hospitals; care at these facilities is not payable as hospital care:
�� Convalescent homes or similar institutions; or
�� Institutions primarily for custodial care, rest or as domiciles; or
�� Health resorts, spas, sanitariums, or tuberculosis hospitals; or
�� Other facilities and institutions which are not classified in general usage as short-term acute care
general hospitals.
Inpatient means an uninterrupted stay of 24 hours or more in a hospital, skilled nursing facility, or
licensed acute care facility.
Investigative refers to procedures, tests, medical treatments, drugs, devices, or other services that are not
supported by reliable medical evidence permitting conclusions concerning its safety, effectiveness, or
effect on health outcomes.
The Medical Director for the appropriate third-party administrator determines if one of the above is
investigational. In making this determination, the Medical Director considers the following reliable
evidence, none of which is determinative in and of itself:
�� Whether there is final approval from the appropriate U.S. government regulatory agency, if required.
This includes whether a drug or device can be lawfully marketed for its proposed use by the U.S. Food
and Drug Administration (FDA); if the drug or device or medical treatment or procedure is the subject
of ongoing Phase I, II, or III clinical trials; or if the drug, device or medical treatment or procedure is
under study, or if further studies are needed to determine its maximum tolerated dose, toxicity, safety,
or efficacy as compared to standard means of treatment or diagnosis; and
�� Whether there are consensus opinions and recommendations reported in relevant scientific and medical
literature, peer-reviewed journals, or the reports of clinical trial committees, and other technology
assessment bodies; this includes consideration of whether a drug is included in the American Hospital
Formulary Service as appropriate for its proposed use; and
�� Whether there are consensus opinions of national and local health-care providers in the applicable
specialty or subspecialty that typically manages the condition as determined by a survey or poll of a
representative sampling of these providers, including whether there are protocols used by the treating
facility or another facility studying the same drug, device, medical treatment or procedure.
The Medical Director also evaluates:
�� The patient’s medical record,
�� Medical protocols for treatment,
�� Informed consent documents, and
�� Authoritative medical literature.

DEFINITIONS
Self-Insured Managed-Care Option 2001 — 55
The Medical Director's determination is a question of professional judgment.
With respect to medications, investigational also means medications with no approved FDA indications,
medications used for investigational indications, and/or medications used for investigational dosage
regimens or delivery routes.
Notwithstanding the above, a procedure, test, treatment, drug, device, or other service will not be
considered investigative when it is the subject of ongoing Phase III clinical trials and the third-party
administrator determines on a case-by-case basis that:
�� Reliable evidence demonstrates that it is safe and efficacious; and
�� Network providers practicing in the applicable specialty or subspecialty conclude that it is not
investigative; and
�� If applicable, the FDA has indicated that the approval of the drug or device for the proposed use, dose,
and delivery route is pending and likely to occur.
Life-threatening illness or injury means a condition resulting from an illness or traumatic accidental
injury which, if not immediately diagnosed and treated, would result in permanent physical disability or
loss of life. (Also see page 52 for the definition of medical emergency.)
Maintenance care means services and supplies furnished mainly to:
�� Maintain, rather than improve, a level of physical or mental function; or
�� Provide a protected environment free from exposure that can worsen a physical or mental condition.
No benefits are payable for services which are mainly maintenance in nature.
Medically necessary care means services which are:
�� Appropriate for the diagnosis, treatment or prevention of the illness or health problem;
�� Consistent with medical standards and accepted practice parameters of the community as determined
by health-care providers in the same or similar general specialty as typically manage the condition,
procedure, or treatment;
�� Require the skills of a covered health-care provider;
�� Help to restore, improve, or maintain the patient’s health;
�� Provided in the appropriate setting; and
�� Not for the convenience of the patient, the patient's family, or the patient's physician or other provider.
Generally, benefits are available under the Plan only for covered services that are medically necessary. The
fact that your physician prescribes care or services does not automatically mean the care or services qualify
for benefits under the Plan. The final decision of whether or not a service is medically necessary is made
by the Medical Director for the appropriate third-party administrator or the director's designee.
However, even though the following services do not fit the above definition of medically necessary care,
they are covered services under the Plan:
�� Certain voluntary procedures (such as circumcision, tubal ligation, vasectomy and elective termination
of pregnancy);
�� Preventive services administered by your designated network PCP/PCC or designated network
OB/GYN that are consistent with local medical practice for your age and sex;
�� Detection services administered by your designated network PCP/PCC or designated network
OB/GYN that are consistent with local medical practice for your age and sex; and
�� Specific wellness care provided by your designated network PCP/PCC or designated network
OB/GYN.
DEFINITIONS
56 — Self-Insured Managed-Care Option 2001
Medical supplies mean small and often disposable items that are part of medical treatment for an illness or
injury. To be covered under the Plan, the supply must be consistent with the diagnosis and generally must
not be useful in the absence of illness or injury. Covered medical supplies include, but are not limited to:
ostomy bags and skin bond for a colostomy, surgical support stockings for a diagnosis of phlebitis or other
circulatory condition.
Over-the-counter products are not covered. Examples of excluded over-the-counter products include, but
are not limited to: band aids, bandages, pads for incontinence, ankle braces, wrist braces, elbow braces,
knee braces, or neck braces.
Mental disorder means a condition having an emotional or psychological origin as defined in the current
edition of the Diagnostic and Statistical Manual of Mental Disorders. It includes conditions commonly
understood to be mental disorders whether based on a physiological or organic origin and for which
treatment is generally provided by or under the direction of a mental-health professional, such as a
psychiatrist or psychologist.
The precertified care the Plan covers include, but are not limited to treatment of the following mental
disorders:
�� Alcoholism and drug
abuse
�� Attention deficit disorder
�� Bipolar disorder
�� Major depressive disorder
�� Obsessive compulsive
disorder
�� Panic disorder
�� Pervasive Mental
Developmental Disorder
(Autism)
�� Psychotic depression
�� Schizophrenia
Coverages available and limitations are noted in the cost-sharing table for the appropriate third-party
administrator beginning on the following pages:
�� Page 15 for Aetna U.S. Healthcare
�� Page 21 for HealthPartners
�� Page 29 for Medica Self-Insured
�� Page 39 for SelectAdvantage
Morbid obesity means a body weight of greater than 150 percent of expected body weight according to
the MetLife Tables for sex, age, height, and body build. A medical condition must be directly exacerbated
by the obesity before the Plan considers the limited treatments that are covered (see page 73). The types of
medical conditions that could be directly exacerbated by the obesity include hypertension, cardiac disease,
respiratory disease, or Type I diabetes mellitus.
Negotiated fee means the maximum amount a network provider may be paid for covered services and
supplies in accordance with a contract between the provider and the appropriate third-party administrator.
Network provider means any hospital, physician, specialist, or other provider under agreement with the
appropriate third-party administrator to make covered services available under the Plan for a negotiated fee
or reimbursement arrangement.
Palliative care means care that relieves pain or symptoms immediately following treatment, but does not
result in permanent improvement. In general, no benefits are available for any care considered to be
palliative in nature. However, benefits may be payable for precertified palliative care provided through a
covered hospice program.

DEFINITIONS
Self-Insured Managed-Care Option 2001 — 57
Prenatal care means a comprehensive package of medical and psychosocial support provided throughout
a pregnancy and related directly to the care of the pregnancy, including risk assessment, serial surveillance,
prenatal education, and use of specialized skills and technology, when needed, as defined by Standards for
Obstetric-Gynecologic Services issued by the American College of Obstetricians and Gynecologists.
Psychologically necessary care means care which is:
�� Appropriate and essential for the diagnosis, evaluation or treatment of a mental disorder, including
substance abuse, other than mental retardation;
�� In line with U.S. standards of mental-health professional practices (psychiatry, clinical psychology,
clinical social work);
�� Provided at the appropriate level of care based on the severity of the illness and capacity to respond to
professional treatment;
�� Within the professional competence of the provider; and
�� Reasonably expected to improve the condition or level of functionality, or at least prevent further
deterioration.
Reasonable and Customary (R&C) means the amount that the Plan uses to determine payment for a
particular service when it is rendered by a covered provider, based on the usual, customary and reasonable
fee in the area. Charges received are considered only up to the R&C limit established by the Plan. The
R&C limit is:
�� The amount customarily charged for the service by other providers in the geographical area where the
service is provided;
�� Reasonable considering the type of service provided;
�� Determined solely by the appropriate third-party administrator; and
�� Subject to change at any time.
Some providers may charge a fee that is higher than R&C. Any difference between R&C and the amount
billed by a non-network provider is always your responsibility. The difference is not considered for
reimbursement under the Plan. Under the terms of their contracts, network providers never bill amounts in
excess of R&C.
Covered emergency care by non-network providers are paid at the billed rates.
Reconstructive refers to surgery to rebuild or correct:
�� A body part when such surgery is incidental to or following surgery resulting from injury, sickness, or
disease of the involved body part; or
�� A functional defect determined by a physician to have been present at birth and that adversely affects
your ability to perform routine activities of daily living.
Surgery that is primarily cosmetic in nature is not considered to be reconstructive and is not covered under
the Plan. For covered reconstructive surgery, refer to page 76.

DEFINITIONS
58 — Self-Insured Managed-Care Option 2001
Referral* ** means a specific written or electronic authorization from your designated network PCP/PCC
to seek medically necessary services from another provider when such services are not available from your
PCP/PCC. Your PCP/PCC must issue a written or electronic referral according to specific referral
guidelines that include:
�� The time period during which services must be received,
�� The specific services to be provided, and
�� The provider to whom you are referred.
A general statement by your PCP/PCC that you should seek a particular type of service or provider is not
considered a referral under the Plan.
Respite care means care rendered by individuals other than your primary caregivers (primary caregivers
may be family members or friends) to give them rest and/or relief when necessary in order to maintain you
at home. In general, no benefits are available for any care considered to be respite care. However, respite
care may be covered under a hospice program, if approved through the Plan’s precertification process.
Restorative surgery means surgery to rebuild or correct a physical defect that has direct adverse effect on
the physical health of a body part and the restoration or correction is determined to be medically necessary.
Surgery that is cosmetic is not considered to be restorative under the Plan.
Self-insured means that the Plan sponsor, Unisys in this case, makes benefit payments as services occur,
including a fee for the use of the third-party administrator’s network and the third-party administrator’s
services. Costs are variable rather than fixed because Unisys, not the plans, bears the risk of volatility of
expenses. State insurance taxes and state mandates do not apply. Instead, the plan is subject to the federal
Employee Retirement Income Security Act.
Skilled nursing convalescent facility means a licensed, Medicare-approved facility other than a hospital
and meets all of the following requirement:
�� Maintains permanent and full-time facilities for bed care of ten or more resident patients;
�� Has available at all times the services of a physician;
�� Has a registered nurse or physician on full-time duty in charge of patient care, and one or more
registered nurses or licensed practical nurses on duty at all times;
�� Maintains a daily medical record for each patient;
�� Is primarily engaged in providing continuous skilled nursing care for ill or injured persons during the
convalescent stage of their illness or injury and is not, other than incidentally, a place for rest, the aged,
drug addicts, alcoholics, or a nursing home. Nor is it a place providing custodial care, educational care,
or the care of mental disorders or mental retardation; and
�� Has transfer arrangements with one or more hospitals and a utilization review plan in effect.
Coverage under the Plan is limited to precertified, medically necessary treatments provided as an
alternative to inpatient hospital services and the cost is less than inpatient hospital care. Custodial or
maintenance services are not covered.
* Note for Medica Self-Insured: Medica allows you to refer yourself to network providers without referral from
your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. Copayments and
coinsurance are higher under Tier II than when you obtain a referral from your PCC (Tier I).
** Note for SelectAdvantage for services on or after July 1, 2001: SelectAdvantage allows you to refer yourself to
any network provider. This is called “self-referral.”

DEFINITIONS
Self-Insured Managed-Care Option 2001 — 59
Specialized licensed treatment facility means a facility that specifically treats mental health conditions,
including substance abuse conditions. In order to be covered under the Plan, the facility must meet local
licensing standards for the effective treatment of mental health or substance abuse conditions.
Specialized mental health facilities also must provide:
�� All normal infirmary-level medical services required during the treatment period, whether or not
related to the mental health condition, and an agreement with a hospital in the area to provide any
other medical services required;
�� Continuous supervision by a psychiatrist who has the overall responsibility for coordinating patient
care and who is at the facility on a regularly scheduled basis; and
�� Staff psychiatrists who are directly involved in the treatment program, at least one of whom is present
at all times during the treatment day, and the continuous services of a psychiatric nurse.
Specialized substance abuse facilities also must provide:
�� A full-time inpatient or outpatient program for the diagnosis, evaluation, and rehabilitation of
alcoholism or drug abuse;
�� 24-hour medical detoxification services;
�� Normal medical services (unless the treatment facility has an agreement with a nearby hospital to
provide other medical services);
�� Skilled nursing services by licensed nurses under the direction of a full-time registered graduate nurse
— all under the supervision of a staff of doctors; and
�� A prepared written plan of treatment for each patient which is followed under a doctor’s supervision.
Surgical procedures include, but are not limited to procedure in the following categories:
�� Incision or excision of any part of the body;
�� Electrocauterization;
�� Manipulative reduction of a fracture or dislocation;
�� Suturing of a wound (removal of sutures by a physician who is not the operating physician also is
considered part of a surgical procedure); or
�� Endoscopic removal of a stone or foreign object from the larynx, bronchus, trachea, esophagus,
stomach, urinary bladder, or ureter.
Urgent care center (See Convenient/Urgent Care Center on page 51.)
Urgent medical need means an acute, non-life-threatening medical condition which could not have been
anticipated and for which a delay in treatment would be detrimental to your health. Some examples of
urgent medical need include, but are not limited to:
�� Earache
�� Respiratory or flu-like symptoms with high fever
�� Severe abdominal cramps
�� Severe diarrhea
�� Severe sore throat
�� Severe vomiting
To be covered, urgent-care treatment must be coordinated by your PCP/PCC* **. The steps you should
take in case of an urgent medical need are provided beginning on page 10.
* Note for Medica Self-Insured: Medica allows you to refer yourself to network providers without referral from
your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. Copayments and
coinsurance are higher under Tier II than when you obtain a referral from your PCC (Tier I).
** Note for SelectAdvantage for services on or after July 1, 2001: SelectAdvantage allows you to refer yourself to
any network provider. This is called “self-referral.”


PRECERTIFICATION
Self-Insured Managed-Care Option 2001 — 61
PRECERTIFICATION

PRECERTIFICATION
62 — Self-Insured Managed-Care Option 2001
PRECERTIFICATION
When your PCP/PCC* coordinates your care with network providers, precertification generally is handled
for you by your PCP/PCC. In emergency situations involving an inpatient stay outside your network
service area, you are required to initiate the precertification process. If a network referral specialist directs
services, you should verify with the provider and Member Services to ensure that the required
precertification process is completed.
* Note for Medica Self-Insured and for SelectAdvantage: If you self-refer to a network provider, you should verify
with the provider and Member Services that the required precertification process is completed for the services noted
in this section that require precertification.
Emergency Services
If you are admitted to a facility due to a medical emergency (see page 52 for the definition of medical
emergency) or urgent medical need (see page 59 for the definition of urgent medical need), you , a family
member, or the attending physician should call Member Services within 24 hours after the emergency
occurs. If your plan includes a PCP or PCC, you also should notify your PCP/PCC.
If the appropriate third-party administrator considers your admission to be the result of a medical
emergency or urgent medical need, the Plan will approve payment for the care, regardless of the network
status of the providers involved in your emergency care. You must pay the appropriate copayments or
coinsurances.
Your PCP/PCC must provide or coordinate your follow-up care (or a network self-referral specialist, in the
case of Medica Self-Insured, or any network provider in the case of SelectAdvantage for services on or
after July 1, 2001).
For additional information on what to do in the event of an emergency, refer to page 10.
Non-Emergency Services
The following chart indicates services also requiring precertification. Follow up with Member Services
within one week before the date services are to be provided to verify that the precertification process has
been completed.
Type of non-emergency
services requiring
precertification Network Provider Role Your role
Inpatient stay Obtain certification for inpatient
admissions for any reason,
including medical, surgical, or
maternity admissions.
��Verify that services have
been approved in advance of
admission.
��Comply with any
requirements resulting from
the precertification process.
Durable Medical Equipment Obtain certification for durable
medical equipment items that fall
under certification review
procedure.
�� If approved, purchase the
equipment from the approved
network vendor.
��Comply with any
requirements resulting from
the precertification process

PRECERTIFICATION
Self-Insured Managed-Care Option 2001 — 63
Type of non-emergency
services requiring
precertification Network Provider Role Your role
Home Health Care Obtain certification for home
health care services.
��Verify that services have
been approved in advance of
receiving services.
��Comply with any
requirements resulting from
the precertification process.
Home IV therapy Obtain certification for Home IV
therapy.
��Verify that services have
been approved in advance of
admission.
��Comply with any
requirements resulting from
the precertification process.
Hospice Obtain certification for hospice
care.
��Verify that services have
been approved in advance of
admission.
��Comply with any
requirements resulting from
the precertification process.
Mental Health or Substance
Abuse Treatments
For Aetna U.S. Healthcare, your
PCP obtains certification for
mental health/substance abuse
treatments.
�� For HealthPartners, you can
self refer for outpatient
services from network
behavioral health providers.
�� For Medica Self-Insured,
specialized precertification
vendors apply to these types
of treatments. You must
precertify these services.
Refer to the telephone
number on the front cover of
this booklet for the
appropriate contact.
�� For SelectAdvantage
members for services on and
before June 30, 2001,
specialized precertification
vendors apply to these types
of treatments.
��Comply with any
requirements resulting from
the precertification process.
��Note the limitations for
coverage.

PRECERTIFICATION
64 — Self-Insured Managed-Care Option 2001
Type of non-emergency
services requiring
precertification Network Provider Role Your role
Organ or Tissue Transplants Obtain certification for the organ
or tissue transplants.
�� The third-party
administrators designate
specialized facilities for
organ or tissue transplants.
��Verify that services have
been approved in advance of
receiving treatments.
��Comply with any
requirements resulting from
the precertification process.
Rehabilitative services: cognitive,
physical, occupational,
pulmonary, and speech therapy
Provide the referral for the
treatments.
�� If approved, obtain services
from designated provider.
��Comply with any
requirements resulting from
the precertification process.
��Note the limitations for
coverage.
Skilled Nursing Care Obtain certification for skilled
nursing care services.
��Verify that services have
been approved in advance of
admission.
��Comply with any
requirements resulting from
the precertification process.
Skilled Nursing Facility Obtain certification for inpatient
admissions to a skilled nursing
facility.
��Verify that services have
been approved in advance of
admission.
��Comply with any
requirements resulting from
the precertification process.
Surgery Obtain certification for any
surgical procedures requiring
certification.
��Verify that services have
been approved in advance of
admission.
��Comply with any
requirements resulting from
the precertification process.

COVERED EXPENSES/SERVICES
Self-Insured Managed-Care Option 2001 — 65
COVERED EXPENSES/SERVICES

COVERED EXPENSES/SERVICES
66 — Self-Insured Managed-Care Option 2001
COVERED EXPENSES/SERVICES
If medically necessary, charges from network providers for the supplies or services listed in this section are
covered under the Plan.
Even if they are not medically necessary, the following voluntary services/procedures are covered under
the Plan when provided by your PCP/PCC* ** or referral specialist:
�� Certain voluntary procedures (such as circumcision, tubal ligation, vasectomy, and elective termination
of pregnancy);
�� Preventive services administered by your designated network PCP/PCC* ** or designated network
OB/GYN that are consistent with local medical practice for your age and sex;
�� Detection services administered by your designated network PCP/PCC* ** or designated network
OB/GYN that are consistent with local medical practice for your age and sex; and
�� Specific wellness care provided by your designated network PCP/PCC* ** or designated network
OB/GYN.
Unless otherwise specified, the copayment levels apply as described in the Cost-Sharing Table for the
appropriate third-party administrator beginning on the following pages:
�� Page 15 for Aetna U.S. Healthcare
�� Page 21 for HealthPartners
�� Page 29 for Medica Self-Insured
�� Page 39 for SelectAdvantage
If services are not medically necessary, they are not covered. The Plan also does not cover chiropractic or
rehabilitative services if they are custodial, maintenance, or palliative in nature.
Acupuncture
Refer to the Cost Sharing Table for the appropriate third-party administrator. Coverage for these services
generally is limited to specific circumstances.
In no event is acupuncture covered for maintenance or palliative care.
Ambulance
Refer to page 50. The covered services are noted in the definition.
Ambulatory surgical facility or surgery center
The Plan covers services provided by a network ambulatory surgical facility or surgery center in the same
manner as applies to outpatient surgery in a hospital.
Amniocentesis and chromosomal analysis
These services are covered only when medically necessary as determined by the network physician in
accordance with guidelines established by the appropriate third-party administrator.
* Note for Medica Self-Insured: Medica allows you to refer yourself to network providers without referral from
your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. Copayments and
coinsurance are higher under Tier II than when you obtain a referral from your PCC (Tier I).
** Note for SelectAdvantage for services on or after July 1, 2001: SelectAdvantage allows you to refer yourself to
any network provider. This is called “self-referral.”

COVERED EXPENSES/SERVICES
Self-Insured Managed-Care Option 2001 — 67
Anesthetic services
The Plan covers expenses for the administration of anesthetics when rendered by a licensed
anesthesiologist or certified registered anesthetist in connection with a covered surgical procedure or
maternity care.
The Plan does not provide additional payment for the administration of anesthetics if the physician who
administers the anesthesia also performs the care (or assists the physician who performs the care) and
receives payment under any other part of the Plan.
Assistant surgeons
Services of assistant surgeons are covered only when the assistance by another physician is medically
necessary during the course of an operation.
Birthing centers
The Plan covers expenses for birthing centers in the same manner in which expenses are covered for
outpatient services at a hospital (see page 71).
Cancer screenings
The Plan supports the early detection of breast cancer, prostate cancer, ovarian cancer, and colorectal
cancer by covering testing to identify individuals that are at higher risk for these diseases. The physician
fees associated with the screenings done in a doctor’s office are covered the same as any office visit. The
professional laboratory or x-ray fees are covered the same as independent lab and x-rays. Scoping
procedures are handled the same as surgical fees.
Chemotherapy
The Plan covers medically necessary, non-investigational chemotherapy regimens. The Plan does not cover
investigative services associated with chemotherapy or investigative dosage regimens. (See page 54 for a
definition of investigative and page 75 for information on radiation.)
Contact lenses/prescription lenses (eyeglasses)
The Plan covers the initial prescription for contact lenses or eyeglasses following cataract surgery*.
For all other purposes, contact lenses or eyeglasses are not covered under the Plan. The third-party
administrator may offer a discount that applies to any purchase of prescription contact lenses or eyeglasses.
If not, Unisys provides discounted eyewear through the Cole Vision Program that is described on the
Unisys Employee Network at iwww.unisys.com/employee.
* Note for Medica Self-Insured: Medica does not cover contact lenses or eyeglasses following cataract surgery.

COVERED EXPENSES/SERVICES
68 — Self-Insured Managed-Care Option 2001
Dental services and treatment
In general, dental services and treatment are not covered. However, the Plan does cover oral surgeries that
typically are considered medical rather than dental in nature or are medically necessary for the treatment of
an underlying medical condition. Some examples include, but are not limited to:
�� Surgical removal of unerupted impacted wisdom teeth
��Removal of tumors or non-dental cysts and lesions
��Repair of cleft palate
��Removal of teeth to complete radiation treatment for cancer of the jaw
In addition, the Plan covers certain services or supplies for the repair of sound natural teeth damaged as the
result of an accidental injury, if the service is done or supply provided as part of the initial emergency
treatment or within the guidelines established by the third-party administrator.
The Plan covers precertified facility charges (but not the surgical charges) for outpatient surgical services
in a hospital or surgicenter for dental surgeries only if the patient is:
��Under the age of 5, or
�� Severely disabled, or
��Has a medical condition requiring outpatient hospital care or general anesthesia for dental treatment.
Coverage for similar services under a dental plan is primary to coverage under this Plan.
Diabetic supplies
Glucometers and insulin pumps are covered as durable medical equipment (see below). Insulin and
disposable diabetic supplies, such as syringes, test strips, and lancettes are covered separately under the
Unisys Prescription Drug Program.
Diagnostic services
The Plan covers radiology and pathology procedures done by, or ordered by your network physician to
determine the nature and/or extent of a condition or illness for which you show symptoms. The Plan does
not cover diagnostic services done for research, study, or investigational programs. (See page 54 for a
definition of investigational.)
Dialysis treatment
The Plan covers dialysis treatment for acute or chronic kidney ailments.
Drugs or medicines dispensed by a pharmacy
Drugs or medicines requiring a prescription and dispensed by a pharmacy are covered separately under the
Unisys Prescription Drug Program.
Durable medical equipment (DME) and prosthetic devices
The Plan covers certain durable medical equipment and some prosthetics, provided they meet Medicare
guidelines for coverage. Some DME also requires advance approval by the third-party administrator.
Contact Member Services at the number listed on the inside cover of this booklet to determine if prior
approval is required by the Plan.
Durable medical equipment: Requests for any type of durable medical equipment for prolonged use and
for treatment of an illness or an injury, must be made in writing by your PCP/PCC and coordinated with a
DME coordinator in Member Services. If approved, the DME or prosthetic device is ordered through the
designated DME vendor identified by the third-party administrator.
The Plan covers the rental or purchase of approved DME, including expenses related to necessary repair
and maintenance. The third-party administrator determines whether rental or purchase will be covered.
Glucometers and insulin pumps are included as covered DME for patients diagnosed with diabetes.

COVERED EXPENSES/SERVICES
Self-Insured Managed-Care Option 2001 — 69
Supplies for glucometers and insulin pumps are covered separately under the Unisys Prescription Drug
Program.
Replacement equipment is covered only if it can be shown that replacing the equipment is required due to
a change in physical condition or purchasing new equipment is less expensive than the repair of existing
equipment.
Charges for more than one item of equipment for the same or similar purposes are not covered.
Note: Even if prescribed by a physician, a number of items are not covered under the Plan. Items not
covered include, but are not limited to: air conditioners, air filter systems, air purifiers, arch supports, bath
chairs, bathtub rails, breast pumps, corsets, dehumidifiers, exercise equipment, humidifiers, jobst
stockings, molded shoes, orthotics, raised toilet seats, shoe inserts, shower stools, stair glides, swimming
pools, toilet rails, or tub benches.
Prosthetic devices: The Plan covers the original placement and fitting of approved devices which replace
all or part of an absent body part. The Plan also covers the original placement and fitting of approved
devices that replace all or part of the function of a permanently inoperable or malfunctioning body part.
Coverage for prosthetic devices is determined by the Medical Director for the appropriate third-party
administrator or the director's designee, unless otherwise required by law.
Also included are charges for the repair or replacement of a prosthesis. However, replacement is covered
only if the appropriate individual plan administrator is shown that both of the following conditions have
been met:
�� It is needed due to a change in physical condition, and
�� It is likely to cost less to purchase a new one than to repair the existing one.
Further, the Plan covers only one repair or replacement per year, unless more than one repair or
replacement is medically necessary due to a change in physical condition.
The Plan does not cover the repair or replacement of a prosthetic device due to loss or misuse of the
device.
Wigs or artificial hairpieces: The Plan covers wigs or artificial hairpieces when they are required as a
result of illness, injury, or treatments for a medical condition. These include alopecia areata and hair loss
following chemotherapy. Wigs and artificial hairpieces are covered when coordinated through the
appropriate plan administrator. The annual maximum for these supplies is $350.
Elective termination of pregnancy
The Plan covers expenses related to the elective termination of a pregnancy, regardless of medical
necessity for the procedure.
Enteral formula
The Plan covers nutritional supplements specifically associated with therapeutic treatment of
phenylketonuria (PKU), branched chain ketonuria, galactosemia, and homocystinuria, if administered
under the direction of a physician.

COVERED EXPENSES/SERVICES
70 — Self-Insured Managed-Care Option 2001
Home-health care
Home-health services are covered if approved and coordinated in advance by the appropriate third-party
administrator and provided upon the prior written or electronic referral by your PCP/PCC* **.
The following services for the homebound may be covered, provided that the primary purpose of the care
is skilled in nature:
�� Part-time or intermittent skilled nursing services provided by or under the supervision of a registered
professional nurse;
�� Part-time or intermittent services of a home-health aide under the supervision of a registered
professional nurse, or if appropriate, a qualified speech or physical therapist;
�� Medical social services by or under the supervision of a qualified medical or psychiatric social worker
in conjunction with other home-health services, if your PCP/PCC* **certifies that such services are
essential for the effective treatment of the medical condition;
�� Short-term physical or speech therapy provided by or under the supervision of a qualified speech
pathologist or physical therapist in connection with other home-health services, provided your
PCP/PCC* ** certifies that such services are likely to result in significant improvement within a 60-
day period;
�� Short-term occupational therapy (except vocational rehabilitation or employment counseling) rendered
by or under the supervision of a qualified occupational therapist in connection with other home-health
services, provided the PCP/PCC* ** certifies that such services are likely to result in significant
improvement within a 60-day period.
No benefits are payable for home-health services:
�� That are not ordered or coordinated by your PCP/PCC* **, or
�� That are of a maintenance or custodial nature, or
�� That are used as respite for primary caregivers.
Hospice
The Plan covers inpatient hospice services for the palliative care of a terminal illness, provided the care has
been requested in writing by your PCP/PCC* **, precertified in advance, and is provided by a designated
hospice program.
To qualify, the patient must be considered to be terminally ill, as indicated in a written medical prognosis
by the attending physician, with a life expectancy of six (6) months or less if the terminal illness runs its
normal course. The patient must have chosen a palliative treatment focus (that is, one that emphasizes
comfort and supportive services) rather than treatment attempting to cure the condition. If you elect to
receive hospice services, you do so in lieu of curative treatment for the terminal illness for the period you
are enrolled in the hospice program.
* Note for Medica Self-Insured: Medica allows you to refer yourself to network providers without referral from
your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. Copayments and
coinsurance are higher under Tier II than when you obtain a referral from your PCC (Tier I).
** Note for SelectAdvantage for services on or after July 1, 2001: SelectAdvantage allows you to refer yourself to
any network provider. This is called “self-referral.”

COVERED EXPENSES/SERVICES
Self-Insured Managed-Care Option 2001 — 71
Hospital (acute care general hospital)
Emergency room expenses: The Plan covers services performed in a hospital emergency room only in the
case of care rendered to treat a medical emergency or properly referred treatment for an urgent medical
need (see page 52 for a definition of medical emergency and page 59 for a definition of urgent medical
need), or if your designated PCP/PCC* ** authorizes the care. If care is received in a hospital emergency
room for situations not meeting the definition of medical emergency (or your designated PCP/PCC* ** did
not authorize the use of the emergency room), no benefits are payable.
Inpatient expenses: The Plan covers medically necessary services customarily furnished by an acute care
general hospital when you are a registered inpatient. These include, but are not limited to:
* Note for Medica Self-Insured: Medica allows you to refer yourself to network providers without referral from
your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. Copayments and
coinsurance are higher under Tier II than when you obtain a referral from your PCC (Tier I).
** Note for SelectAdvantage for services on or after July 1, 2001: SelectAdvantage allows you to refer yourself to
any network provider. This is called “self-referral.”
�� Administration and processing of whole
blood, blood products and blood derivatives
�� Anesthesia and anesthesia services
�� Cardiography/encephalography
�� Drugs, medications, biologicals
�� General nursing care
�� Intensive care or coronary care
�� Intravenous injections and solutions
�� Labor and delivery room services
�� Laboratory and x-ray testing and services
�� Magnetic resonance imaging (MRI)
�� Medical social work
�� Nuclear medicine
�� Oxygen and oxygen therapy
�� Pathology
�� Physical and rehabilitation therapy as
described beginning on page 76
�� Pre- and post-operative care, and operating
room services
�� Semi-private room and board
If you occupy a private room, you must pay the full difference between the hospital's charges for a private
room and the hospital's most common charge for a semi-private room. However, if it is medically necessary
that you have a private room, or if a semi-private room is not available, the Plan will cover the private-
room rate.
The Plan does not cover expenses associated with personal convenience items. These include, but are not
limited to: telephone and television rentals, guest trays, or guest accommodations.
Note: each person’s confinement, including that of a newborn, is treated separately and distinctly from the
confinement of any other person. In other words, an inpatient admission for childbirth will generally result
in two (or more) independent and separately determined hospital benefits. For the newborn to be covered,
you must call the Unisys Benefits Services Center at 1-800-600-2015 within 30 days of the birth.
Outpatient expenses: The Plan covers services performed in the outpatient department of a hospital. Also
covered as if they are outpatient hospital expenses are services performed at birthing centers, ambulatory
surgical centers, or hemodialysis centers, provided the facility possesses all licenses, permits, certifications,
and approvals required by applicable state, local, and federal law.

COVERED EXPENSES/SERVICES
72 — Self-Insured Managed-Care Option 2001
Hospital visits
Medical visits by a physician while you are a registered inpatient in a hospital are covered, provided the
visits are for care of illnesses or conditions other than those related to surgery or maternity care (these visits
generally are included in the physician's surgical or delivery fee). The maximum covered is one visit per
day per diagnosis per physician, unless more visits are determined to be medically necessary.
Medical consultations in a hospital: Medical consultations in a hospital are covered if all of the following
apply:
�� Your physician calls in another physician for a medically necessary consultation, and
�� The physician who is called in is a specialist in your illness or disease, and
�� The consultation takes place while you are a registered inpatient in a hospital.
Newborn care: The initial examination of an enrolled newborn child in a hospital is covered when the
examination is done by a physician other than the delivering physician. If the newborn is not enrolled in
the plan within 30 days of the date of birth, these services and the hospital stay for the newborn are not
covered. To enroll the newborn, call the Unisys Benefits Services Center at 1-800-600-2015.
Second physician: Visits by a second physician are covered if it is determined by the appropriate third-
party administrator that an “exceptional complication” in your surgery, maternity, or inpatient hospital
stays warrants a second physician. An exceptional complication is a condition that is either:
�� Not related to that for which you were admitted to the hospital, or
�� So unusual that it requires more than the customary surgical, maternity or medical care.
Infertility treatments
The Plan covers only limited services for the diagnosis and treatment of infertility to restore normal bodily
function. It does not cover artificial insemination, in vitro fertilization, GIFT, ZIFT, surrogates, storage of
eggs or semen, embryo implants, or fetal implants.
Mental health services
Services for mental disorders (see page 56 for a definition of mental disorder) are covered only when
provided by network providers under the terms required by the appropriate third-party administrator. For
example, treatment for mental-health services may require precertification and/or the oversight of a
separate utilization review group affiliated with the third-party administrators.
Outpatient: The Plan covers a maximum of 30 outpatient visits per year to a psychiatrist, clinical
psychologist, or psychiatric social worker in individual, group, or family therapy sessions.
For retirees, disabled former employees, and their covered dependents eligible for Medicare and
participating in the SelectAdvantage option, the Plan covers a maximum of 20 outpatient visits per year.
Inpatient: The Plan covers a maximum of 30 days of inpatient care per year for the treatment of mental or
nervous disorders, up to 90 days in a lifetime. Covered services include:
�� Pre- and post-hospital planning, including treatment and discharge planning,
�� Referral to (but not payment for) community health and social welfare agency services, and
�� Referral to (but not payment for) related family counseling services except as specified under
Substance Abuse Services.
Inpatient non-hospital residential facility: The Plan covers medical, nursing, counseling or therapeutic
services for substance abuse or dependency in an approved residential facility licensed by the Department
of Health, according to an individual treatment plan, subject to the following limitations:
�� Up to 30 days per year, and
�� Up to 90 days per lifetime.
Covered services include, but are not limited to, the following for non-hospital residential facilities:

COVERED EXPENSES/SERVICES
Self-Insured Managed-Care Option 2001 — 73
�� Drugs, medicines, equipment and supplies provided by the facility;
�� Family counseling and intervention;
�� Physician, psychologist, nurse, certified addictions counselor and trained staff services;
�� Psychiatric, psychological and medical laboratory testing;
�� Rehabilitation therapy and counseling; and
�� Room charges.
Consideration of treatments for substance abuse conditions: Services for treatment of mental-health
conditions and substance abuse conditions are combined when determining if annual and/or lifetime
maximum benefits have been reached.
Morbid obesity treatments
The Plan covers certain medical and/or surgical treatment for morbid obesity (refer to page 56 for a
definition of morbid obesity.
Surgery for morbid obesity is covered only if referral is from a legitimate eating disorder program, under
physician supervision, and in circumstances that fulfill medical necessity, and only if precertified by the
appropriate third-party administrator.
Covered outpatient treatment of morbid obesity includes the following elements:
��Must be physician-directed;
��May involve modified fasting;
��Must include exercise (however, no benefits are payable for the cost of exercise equipment or
programs); and
��Must include a psychological assessment (not necessarily ongoing psychotherapy).
Note: Self-help programs (food supplements, nutri/system, Optifast and store-front diet centers), exercise
equipment, health club dues, or spa treatments are not covered.
Nursing home
See skilled nursing facility on page 79.

COVERED EXPENSES/SERVICES
74 — Self-Insured Managed-Care Option 2001
Office visits/services
The following office services are covered at the benefit levels noted in the cost-sharing charts. Note: a
number of the services are payable only if they are provided by your PCP/PCC* **.
Allergy testing and treatment: Covered services include tests to determine the nature of allergies, test
materials, desensitization treatment (allergy shots), and treatment materials (syringes, serum) to alleviate
allergies. To be covered, services must by provided by your PCP/PCC* ** or requested by a written or
electronic referral by your PCP/PCC* ** to a network specialist.
Chemotherapy/radiation therapy: Non-investigative chemotherapy or radiation therapy services are
covered under the applicable benefit levels.
Diagnosis and treatment: Covered are the services of physicians and other medical staff for the diagnosis
and treatment of illness, injury, or other conditions, as well as emergency and urgent care. This includes
surgical procedures done in a physician's office, consultations with specialists, and a diagnostic workup to
confirm a diagnosis of infertility.
Medication and supplies for use in the physician's office: Covered services include medically necessary
medications, injectables, radioactive materials, dressings, and casts when administered or applied by your
physician in the physician's office for treatment purposes.
Medication or supplies for preventive purposes are covered only when provided by your PCP/PCC* **.
Obstetrical/gynecological services: Routine well-woman examinations are covered only when performed
by your PCP/PCC* ** or network OB/GYN. You do not need a referral for your routine visit (one/calendar
year). This direct access apples to general OB/GYN care from a network OB/GYN only, not subspecialty
care, such as perinatology care, or gynecologic oncologic care* **. Expenses related to pregnancy are
covered under the applicable benefit levels. The Plan also covers the diagnosis and treatment of medical
conditions resulting infertility and treatment to return the body to normal bodily function. Note, however,
that the Plan does not cover artificial insemination or other infertility procedures.
Office surgery: All provisions noted on page 81 with respect to surgical procedures also apply to surgery
done in a physician's office, with the exception of the differences in copayments.
Preventive health services: Each of the third-party administrators establishes the type and frequency of
routine preventive services that are covered based on their internal policies and local market practices.
X-ray and laboratory services: These services, when performed in a network doctor's office, are included
in the appropriate PCP/PCC or specialist office visit copayment (for a network specialist, a PCP/PCC* **
referral is required). Covered services include non-investigative diagnostic x-rays, x-ray therapy,
electrocardiograms, laboratory tests, and diagnostic clinical isotope services which are medically necessary
and ordered by your physician. Routine x-ray and laboratory services performed in your doctor's office are
covered only when provided by your PCP/PCC* ** ***. A separate copayment applies if services are
provided by an independent x-ray or laboratory service***.
* Note for Medica Self-Insured: Medica allows you to refer yourself to network providers without referral from
your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. Copayments and
coinsurance are higher under Tier II than when you obtain a referral from your PCC (Tier I). ** Note for SelectAdvantage for services on or after July 1, 2001: SelectAdvantage allows you to refer yourself to
any network provider. This is called “self-referral.” *** Note for HealthPartners: No copayment applies for network x-ray and lab services, regardless of the setting
where services are rendered.

COVERED EXPENSES/SERVICES
Self-Insured Managed-Care Option 2001 — 75
Organ and tissue transplants
Transplant procedures that are covered include only precertified non-investigative human transplants
performed at hospitals specifically approved and designated to perform these procedures by the appropriate
third-party administrator. Some examples of covered transplants include, but are not limited to:
�� Bone marrow transplants or stem cell
recoveries for certain conditions, specifically
aplastic anemia, leukemia, severe combined
immunodeficiency disease and Wiskott-
Aldrich Syndrome
�� Corneal transplants
�� Heart transplants
�� Kidney transplants
�� Liver transplants for children with biliary
atresia
Additional transplants are covered when they are deemed by the appropriate third-party administrator, in
their sole discretion, no longer to be investigative in nature. (See page 54 for the definition of
investigative.)
Outpatient surgery
See surgical procedures on page 81.
Oxygen and oxygen equipment
See durable medical equipment on page 68.
Pap tests
The Plan covers expenses associated with Pap tests performed as often as medically necessary when
symptoms indicate possible cancer.
In addition, routine Pap tests are covered, even if there are no symptoms of cancer, provided they are
ordered by your designated network PCP/PCC* ** or your network OB/GYN.
Phenylketonuria (PKU) nutritional supplements
The Plan covers nutritional supplements specifically associated with therapeutic treatment of
phenylketonuria (PKU), branched chain ketonuria, galactosemia, and homocystinuria, if administered
under the direction of a physician. Nutritional supplements for any other conditions are not covered.
Physical therapy
See rehabilitative services on page 76. Note that there are limitations as noted in the cost-sharing tables.
Preadmission testing
The Plan covers these expenses when performed in conjunction with a scheduled hospital admission or
outpatient surgical procedure.
Prescription drugs and medicines dispensed by a pharmacy
These are covered separately under the Unisys Prescription Drug Program described in the appropriate
Summary Plan Description booklet noted on the inside cover of this booklet as revised from time-to-time
in the annual Summary of Plan Changes booklet issued each fall.
Radiation services
The Plan covers medically necessary, non-investigative radiation services, including the use of x-rays,
radiation, or radioactive isotopes. The Plan does not cover radiation services associated with investigative
uses or dosage regiments of radiation therapy. (See page 54 for a definition of investigative.)
* Note for Medica Self-Insured: Medica allows you to refer yourself to network providers without referral from
your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. Copayments and
coinsurance are higher under Tier II than when you obtain a referral from your PCC (Tier I).
** Note for SelectAdvantage for services on or after July 1, 2001: SelectAdvantage allows you to refer yourself to
any network provider. This is called “self-referral.”

COVERED EXPENSES/SERVICES
76 — Self-Insured Managed-Care Option 2001
Reconstructive surgery
The Plan covers reconstructive surgery, including plastic surgery, only to:
�� Correct a severe birth defect or congenital abnormality which is accompanied by a functional medical
disorder;
�� Repair damage caused by an injury or covered surgery that occurred while covered under a medical
plan sponsored by Unisys;
�� Reconstruct breast after a total mastectomy performed following the diagnosis of cancer and/or
reconstruct the other breast to produce symmetrical appearance; or
�� Restore a body part that is injured or deformed by acute trauma, infection or other pathological disease
such that the essential function of that body part is compromised.
The Plan covers plastic or reconstructive surgery expenses only when the procedure is expected to improve
the function of a body part. Improvement in the function of a body part is considered to occur only if:
�� The surgery is expected to partially or fully restore or improve the physiological function, passive
function or normal function of an organ, a tissue or a body part; or
�� The surgery is expected to eliminate or substantially reduce an impairment causing pain or discomfort
to a body part or a body area resulting from an illness, injury or previous covered surgery.
Improvement in function does not include the repair of body changes associated with the aging process or
congenital deformities of a generalized nature which are not causing a restorable loss of function.
Other services and supplies that improve, alter, or enhance appearance, whether for psychological or
emotional reasons, are not covered.
Rehabilitation services
The Plan covers the rehabilitation services noted below. Be sure to note the limitations indicated on the
cost-sharing tables. The Plan does not cover any of these services if they are for maintenance care or are
palliative in nature.
Cardiac rehabilitation: Benefits for cardiac rehabilitation are available only as part of an inpatient stay.
Cognitive therapy: Benefits for short-term cognitive therapy are available upon referral by your
PCP/PCC* **. To be covered, the treatment must be approved by the Medical Director for the appropriate
third-party administrator or the director’s designee. In all cases, the network provider must certify that the
treatment is expected to result in a significant improvement in your condition within a short time frame,
generally 60 days or less.
For Aetna U.S. Healthcare and SelectAdvantage members (other than retirees, disabled former employees,
and their covered dependents eligible for Medicare and participating in the SelectAdvantage option, as
noted below), covered services include precertified treatment within a 60-day period per incident of illness
or injury. The 60-day period is measured from the first day of treatment for the incident.
For retirees, disabled former employees, and their covered dependents eligible for Medicare and
participating in the SelectAdvantage option, covered services are limited to 20 visits per calendar year.
For HealthPartners and Medica Self-Insured, covered services are limited to 15 visits per condition.
* Note for Medica: Medica allows you to refer yourself to network providers without referral from your PCC. This
is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral provider, as well
as all covered services ordered or coordinated by the self-referral provider. Copayments and coinsurance are higher
under Tier II than when you obtain a referral from your PCC (Tier I).
** Note for SelectAdvantage for services on or after July 1, 2001: SelectAdvantage allows you to refer yourself to
any network provider. This is called “self-referral.”

COVERED EXPENSES/SERVICES
Self-Insured Managed-Care Option 2001 — 77
Manipulative therapy: Benefits for short-term manipulative therapy are available upon referral by your
PCP/PCC* ** to a licensed network chiropractor or a network osteopathic physician. Alternately, you may
select a network osteopathic PCP/PCC* ** who performs these services. To be covered, the treatment must
be approved by the Medical Director for the appropriate third-party administrator or the director's designee.
In all cases, the network provider must certify that the treatment is expected to result in a significant
improvement in your condition within a short time frame, generally 60 days or less.
For Aetna U.S. Healthcare and SelectAdvantage members (other than retirees, disabled former employees,
and their covered dependents eligible for Medicare and participating in the SelectAdvantage option, as
noted below), covered services include precertified treatment within a 60-day period per incident of illness
or injury. The 60-day period is measured from the first day of treatment for the incident.
For retirees, disabled former employees, and their covered dependents eligible for Medicare and
participating in the SelectAdvantage option, covered services are limited to 20 visits per calendar year.
For HealthPartners and Medica Self-Insured, covered services are limited to 15 visits per condition.
Occupational therapy: Benefits for short-term occupational therapy are available upon referral by your
PCP/PCC* **. To be covered, the treatment must be approved by the Medical Director for the appropriate
third-party administrator or the director’s designee. In all cases, the network provider must certify that the
treatment is expected to result in a significant improvement in your condition within a short time frame,
generally 60 days or less.
For Aetna U.S. Healthcare and SelectAdvantage members (other than retirees, disabled former employees,
and their covered dependents eligible for Medicare and participating in the SelectAdvantage option, as
noted below), covered services include precertified treatment within a 60-day period per incident of illness
or injury. The 60-day period is measured from the first day of treatment for the incident.
For retirees, disabled former employees, and their covered dependents eligible for Medicare and
participating in the SelectAdvantage option, covered services are limited to 20 visits per calendar year.
For HealthPartners and Medica Self-Insured, covered services are limited to 15 visits per condition.
Physical therapy: Benefits for short-term physical therapy are available upon referral by your
PCP/PCC* **. To be covered, the treatment must be approved by the Medical Director for the appropriate
third-party administrator or the director’s designee. In all cases, the network provider must certify that the
treatment is expected to result in a significant improvement in your condition within a short time frame,
generally 60 days or less.
For Aetna U.S. Healthcare and SelectAdvantage members (other than retirees, disabled former employees,
and their covered dependents eligible for Medicare and participating in the SelectAdvantage option, as
noted below), covered services include precertified treatment within a 60-day period per incident of illness
or injury. The 60-day period is measured from the first day of treatment for the incident.
For retirees, disabled former employees, and their covered dependents eligible for Medicare and
participating in the SelectAdvantage option, covered services are limited to 20 visits per calendar year.
* Note for Medica Self-Insured: Medica allows you to refer yourself to network providers without referral from
your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. Copayments and
coinsurance are higher under Tier II than when you obtain a referral from your PCC (Tier I).
** Note for SelectAdvantage for services on or after July 1, 2001: SelectAdvantage allows you to refer yourself to
any network provider. This is called “self-referral.”

COVERED EXPENSES/SERVICES
78 — Self-Insured Managed-Care Option 2001
For HealthPartners and Medica Self-Insured, covered services are limited to 15 visits per condition.
Pulmonary rehabilitation: Benefits for short-term pulmonary rehabilitation services are available upon
referral by your PCP/PCC* **. To be covered, the treatment must be approved by the Medical Director for
the appropriate third-party administrator or the director’s designee. In all cases, the network provider must
certify that the treatment is expected to result in a significant improvement in your condition within a short
time frame, generally 60 days or less.
For Aetna U.S. Healthcare and SelectAdvantage members (other than retirees, disabled former employees,
and their covered dependents eligible for Medicare and participating in the SelectAdvantage option, as
noted below), covered services include precertified treatment within a 60-day period per incident of illness
or injury. The 60-day period is measured from the first day of treatment for the incident.
For retirees, disabled former employees, and their covered dependents eligible for Medicare and
participating in the SelectAdvantage option, covered services are limited to 20 visits per calendar year.
For HealthPartners and Medica Self-Insured, covered services are limited to 15 visits per condition.
Speech therapy: Benefits for short-term speech therapy are available to restore speech lost due to an
illness, accident, or surgery upon referral by your PCP/PCC* **. To be covered, the treatment must be
approved by the Medical Director for the appropriate third-party administrator or the director’s designee.
In all cases, the network provider must certify that the treatment is expected to result in a significant
improvement in your condition within a short time frame, generally 60 days or less.
For Aetna U.S. Healthcare and SelectAdvantage members (other than retirees, disabled former employees,
and their covered dependents eligible for Medicare and participating in the SelectAdvantage option, as
noted below), covered services include precertified treatment within a 60-day period per incident of illness
or injury. The 60-day period is measured from the first day of treatment for the incident.
For retirees, disabled former employees, and their covered dependents eligible for Medicare and
participating in the SelectAdvantage option, covered services are limited to 20 visits per calendar year.
For HealthPartners and Medica Self-Insured, covered services are limited to 15 visits per condition.
Scoping procedures
Medical necessary scoping procedures to determine the nature and/or extent of an illness or an injury are
covered in the same manner as surgery (see page 81). The copayments vary, depending on where the
procedure is performed. Refer to the cost-sharing tables.
* Note for Medica Self-Insured: Medica allows you to refer yourself to network providers without referral from
your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. Copayments and
coinsurance are higher under Tier II than when you obtain a referral from your PCC (Tier I).
** Note for SelectAdvantage for services on or after July 1, 2001: SelectAdvantage allows you to refer yourself to
any network provider. This is called “self-referral.”

COVERED EXPENSES/SERVICES
Self-Insured Managed-Care Option 2001 — 79
Second surgical opinions
Charges associated with a second opinion for a proposed surgery which are obtained at your request are
covered under the following conditions:
�� The second opinion is given by a network specialist who, by specialty, is an appropriate physician to
consider the surgical procedure; and
�� The proposed surgery is of a non-emergency nature and is a covered procedure under the Plan; and
�� The physician who renders the second opinion does not perform the surgery; and
�� A written or electronic referral by your PCP/PCC* ** is issued.
Skilled nursing facility
If daily skilled care is medically necessary, the Plan covers up to 90 days of precertified care per lifetime
provided at:
�� Nursing homes,
�� Skilled nursing facilities,
�� Transitional care facilities, and
�� Rehabilitation facilities.
Coverage is limited to skilled nursing care as defined by Medicare and subject to precertification by the
appropriate third-party administrator.
Services from these types of facilities are covered when room, board and miscellaneous services for
medically necessary treatment are an alternative to higher cost inpatient hospital services, the charges are
less than inpatient hospital care, and the care has been precertified by the appropriate third-party
administrator.
Charges for custodial supportive care or maintenance care are not covered (see page 51 for a definition of
custodial supportive care and page 55 for a definition of maintenance care).
Sterilization surgeries
Tubal ligations and vasectomies are covered regardless of medical necessity for the procedure. Surgical
reversals of voluntary sterilizations are not covered.
* Note for Medica Self-Insured: Medica allows you to refer yourself to network providers without referral from
your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. Copayments and
coinsurance are higher under Tier II than when you obtain a referral from your PCC (Tier I).
** Note for SelectAdvantage for services on or after July 1, 2001: SelectAdvantage allows you to refer yourself to
any network provider. This is called “self-referral.”

COVERED EXPENSES/SERVICES
80 — Self-Insured Managed-Care Option 2001
Substance abuse treatments
Substance abuse treatments are covered only when provided by network providers under the terms required
by the appropriate third-party administrator. For example, treatment for substance abuse conditions may
require precertification and the oversight of a separate utilization review group affiliated with the third-
party administrator.
The substance abuse treatments noted below are covered, provided treatment is obtained under the terms
proscribed by the appropriate third-party administrator.
Outpatient: The Plan covers diagnostic services, medical treatment, and medical referral services for the
abuse of or addiction to alcohol or drugs.
The Plan covers a maximum of 30 outpatient visits per year for treatment of substance abuse or
dependency. However, for retirees, disabled former employees, and their covered dependents eligible for
Medicare and enrolled in the SelectAdvantage option, a maximum of 20 outpatient visits per year applies
for treatment of substance abuse or dependency.
Covered services include, but are not limited to:
�� Services by a physician, psychologist, certified addictions counselor and trained staff;
�� Rehabilitation therapy and counseling,
�� Family counseling and intervention,
�� Psychiatric, psychological and medical laboratory tests, and
�� Drugs, medicines, equipment use and supplies dispensed by the outpatient provider.
Inpatient hospital: The Plan covers a maximum of 30 days of inpatient care per year for detoxification,
medical treatment and referral services for substance abuse or addiction, up to 90 days in a lifetime.
Covered services include, but are not limited to:
�� Room charges;
�� Physician, psychologist, nurse, certified addictions counselor and trained staff services;
�� Diagnostic x-rays;
�� Psychiatric, psychological and medical laboratory testing; and
�� Drugs, medicines, equipment and supplies dispensed by the facility.
Inpatient non-hospital residential facility: The Plan covers medical, nursing, counseling or therapeutic
services for substance abuse or dependency in an approved residential facility licensed by the Department
of Health, according to an individual treatment plan, subject to the following limitations:
�� Up to 30 days per year, and
�� Up to 90 days per lifetime
For non-hospital residential facilities, covered services include, but are not limited to:
�� Drugs, medicines, equipment and supplies dispensed by the facility;
�� Family counseling and intervention;
�� Physician, psychologist, nurse, certified addictions counselor and trained staff services;
�� Psychiatric, psychological and medical laboratory testing;
�� Rehabilitation therapy and counseling; and
�� Room charges.
Consideration of treatments for mental-health: Services for treatment of mental-health conditions and
substance abuse conditions are combined when determining if annual and/or lifetime maximum benefits
have been reached.

COVERED EXPENSES/SERVICES
Self-Insured Managed-Care Option 2001 — 81
Surgical procedures
The Plan covers medically necessary procedures which involve an incision or puncture of the skin or tissue
requiring the use of surgical instruments. In addition, the Plan covers the following voluntary surgical
procedures which are not medically necessary: circumcision, elective termination of pregnancy, tubal
ligation, and vasectomy.
Covered surgical procedures include, but are not limited to, medically necessary:
�� D&C procedures;
�� Electrocauterization;
�� Endoscopic removal of a stone or other foreign object from the larynx, bronchus, trachea, esophagus,
stomach, urinary bladder or ureter;
�� Manipulative reduction of a fracture or dislocation;
�� Normal delivery, Caesarean section delivery, procedures resulting from complications of pregnancy,
and procedures required following a miscarriage;
�� Scoping procedures; and
�� Suturing of a wound (removal of sutures by a physician who is not the operating physician also is
considered part of a surgical procedure).
Note: Surgical procedures and related expenses, including hospital care, that are not covered include, but
are not limited to: procedures to alter sex from one gender to the other; radial keratotomy; in vitro
fertilization; elective reversal of sterilization; treatment of obesity (other than treatment for morbid obesity
as noted on page 73); investigational procedures.
TMJ (temporomandibular joint) syndrome treatments
Only precertified medically necessary surgery for TMJ is covered under the Plan. Services not covered
include, but are not limited to: appliances and the x-rays related to the appliance, x-rays related to covered
surgery for TMJ, therapy, and other medical supplies.
Transitional care facility
See skilled nursing facility on page 79.
X-ray and laboratory services
See X-ray and laboratory services on page 74.


EXCLUSIONS
Self-Insured Managed-Care Option 2001 — 83
EXCLUSIONS

EXCLUSIONS
84 — Self-Insured Managed-Care Option 2001
EXCLUSIONS
The Plan does not cover expenses for services which are not medically necessary. Medical necessity is
discussed on page 55.
Care that may be personally desirable, but not medically necessary, is not covered. Some examples of
personal necessity which are not considered medically necessary are cosmetic care, in vitro fertilization,
and artificial insemination.
Further, the Plan does not cover:
��Any expense for which no services are provided;
��Any care, treatment, service, or supply furnished, paid for, or for which benefits are provided or
required by reason of past or present service of any family member in the armed forces of a
government;
�� Services not provided by a covered health-care provider; and
��Care for conditions that state or local law require be treated in a public facility, including, but not
limited to, commitments due to mental disorders, including substance abuse conditions.
Other exclusions are noted below and on the following pages.
Acupressure, or hypno-therapy
Acupressure and hypno-therapy are not covered under any circumstances.
Admission to a hospital before you become covered under the Plan
If you are admitted as a registered inpatient before the date you become covered under the Plan, the Plan
will not cover any charges associated with your stay.
Adoption expenses
Expenses not covered include, but are not limited to: adoption fees; court costs; expenses related to the
natural mother; and all expenses for the child prior to the date the child begins to reside with you in a
regular parent/child relationship.
Air conditioners, dehumidifiers, humidifiers, or other equipment to alter the air or temperature
These are not covered under any circumstances. Refer to pages 68 and 86.
Annual maximums
Services in excess of annual maximums are not covered under any circumstances, with the exception of
Tier II benefits through Medica Self-Insured.
Appointments missed/canceled
Charges for missed or canceled appointments are not covered under any circumstances.
Artificial insemination
Artificial insemination is not covered under any circumstances.
Autologous blood donations/storage
The Plan does not cover charges related to donating and storing your own blood for any reason, even if the
services are performed prior to a planned surgical procedure that would generally require a blood
transfusion.
Autopsy
The Plan does not cover the expenses associated with an autopsy.

EXCLUSIONS
Self-Insured Managed-Care Option 2001 — 85
Blood or blood plasma
The Plan does not cover expenses related to the acquisition of blood or blood plasma (it does, however,
cover the cost of transfusions).
Chelating agents
Any service, supply or treatment for which chelating agents are used are not covered, except for treatment
of heavy metal poisoning.
Complications arising from any non-covered surgery
If the initial surgery is not covered, treatments for complications arising from the surgery are not covered.
Confinement in an institution not covered under the Plan
The Plan does not cover charges for confinement in an institution which is not covered under the Plan.
Contact lenses/prescription lenses (eyeglasses)*
Except as noted on page 67 for the first pair of corrective lenses immediately following cataract surgery,
charges for contact lenses or eyeglasses are not covered.
Convenience items
Convenience items are not covered under any circumstances. Such items include, but are not limited to:
telephone and television rental, guest meals, and guest accommodations.
Correction of structural imbalance, distortion, or subluxation
The Plan does not cover the diagnosis, detection, and correction (by manual or mechanical means) of
structural imbalance, distortion, or subluxation to remove nerve interference and its effects. This exclusion
applies when the nerve interference is the result of or related to distortion, misalignment, or subluxation of
or in the vertebral column.
Cosmetic or plastic surgery
The Plan does not cover any procedure, service, equipment or supply which improves, alters, or enhances
appearance, whether or not for psychological or emotional reasons, except as noted on page 76.
Court appearances
The Plan does not cover costs related to any court appearance, proceeding or hearing.
Custodial supportive care or maintenance care (including sanitorium care, rest care, unskilled
nursing, or unskilled rehabilitation services)
These types of care are not covered under any circumstances. (See page 51 for the definition of custodial
supportive care and page 55 for the definition of maintenance care.)
* Medica Self-Insured does not cover contact lenses or eyeglasses following cataract surgery.

EXCLUSIONS
86 — Self-Insured Managed-Care Option 2001
Dental services or treatment
The Plan does not cover any dental services or treatment other than those noted on page 68. Services not
covered include, but are not limited to:
��Alveolectomy
��Apicoectomy (dental root
resection)
��Care of gums or bones
supporting teeth
��Dental cleanings or
fillings
��Dental implants
��Dental prosthesis, braces,
and in-mouth appliances
�� False teeth
�� Frenectomy
�� Incision and drainage of
cellulitis
�� Incision of sinuses,
salivary glands, or ducts
��Myofunctional alteration
��Orthodontics, including
braces
��Orthognathic surgery
�� Placement of
subperiosteal orthopedic
bone plates
�� Planing or scaling
��Removal of exostosis
��Repair, removal or
replacement of teeth
��Root canal therapy
�� Simple tooth extractions
�� Soft tissue impactions
�� Treatment of cavities
�� Treatment of injuries to
or diseases of the teeth or
gums other than the
initial emergency
treatment
�� Treatment of periodontal
abscess or dentigerous
cysts
�� Treatment of
temporomandibular joint
(TMJ) syndrome, unless
precertified as medically
necessary (see page 81)
Discount
The Plan does not cover the portion of any charge which represents a discount.
Durable medical equipment (DME) and other equipment
The following items are not covered:
��Air conditioners
��Air filter systems
��Air purifiers
��Arch supports
��Back-up generators
��Bath chairs
��Bathtub rails
��Breast pumps
��Corsets
��Dehumidifiers
�� Environmental control
equipment
�� Exercise equipment,
including but not limited
to weight training
equipment
�� Foot orthotics or
special/corrective shoes
��Humidifiers
�� Jobst stockings
��Raised toilet seats
�� Shoe inserts
�� Shower stools
�� Stair glides
�� Swimming pools
�� Toilet rails
�� Tub benches
��Whirlpools
Education, special education, or job training
These services are not covered, even if provided in a facility that also provides treatment for medical,
mental disorders or substance abuse conditions.
Educational, vocational, or other training services, counseling or supplies
These are not covered for any purpose, including speech, language, learning deficiencies or behavioral
problems. (Diabetic education is covered, however, as noted in the cost-sharing charts.)
Embryo implants
Embryo implants are not covered under any circumstances.
Eyeglasses*
Except as noted on page 67 for the first pair of corrective lenses immediately following cataract surgery,
charges for contact lenses or eyeglasses are not covered.
* Medica Self-Insured does not cover contact lenses or eyeglasses following cataract surgery.

EXCLUSIONS
Self-Insured Managed-Care Option 2001 — 87
Family members/household members
The Plan does not cover expenses associated with care you get from an individual who normally resides in
your household or is a member of your immediate family. Your immediate family includes parents,
siblings, spouses, children, grandparents, aunts, uncles, nieces and nephews, as well as similar family
members related to you by marriage.
Fetal implants
Fetal implants are not covered under any circumstances.
First aid supplies
Common first aid supplies and medical supplies for home use are not covered under any circumstances.
Food supplements, or food substitutes/nutritional supplements
These are not covered under any circumstances, except as noted on pages 69 and 75 for treatment of PKU
and related conditions.
Free care
The Plan does not cover any care if the care is given to you without charge or would normally be given to
you without charge. This exclusion applies if the care would have been given to you with no charge if you
had not been covered under the Plan or under any other health-benefit plan or insurance.
Gender reassignment
Services for gender reassignment are not covered under any circumstances. Also not covered are any
complications arising from procedures to alter your sex from one gender to the other. Further, other
services related to gender reassignment or disturbance of gender identification or circumstances are not
covered.
Genetic testing or genetic counseling
Charges for genetic testing or genetic counseling are not covered.
Government hospitals
Except for payment for non-military service connected disabilities, the Plan does not pay for care or
supplies in any hospital or other institution which is owned, operated, or maintained by the Veterans
Administration or the federal government, unless the hospital is a network hospital. The Plan does not
cover any other care or supplies in any other hospital or other institution which is owned, operated, or
maintained by the federal government. (The Plan does cover, however, services in such a hospital if,
because of serious injury or sudden illness, you are taken there for emergency care because it is the closest
facility to the place where you were injured or became ill that can render care. In that case, the Plan covers
the services which are considered to be medically necessary as emergency care, provided it was not
possible for you to be sent to another hospital.)
Government programs
The Plan does not cover:
�� Services to the extent that such services are payable by Medicare as the primary payer, or any other
federal, state, or local government program;
�� Treatment of disabilities from diseases contracted or injuries sustained as a result of military service or
war, declared or undeclared, or any act of war, for which you are legally entitled to services at
government facilities, where available;
�� Services or supplies that any school system is required by law to provide; or
�� Services or supplies required by law to be covered under the provisions of any Workers'
Compensation, no-fault automobile insurance, or similar law.
Hearing aids and related supplies
These are not covered under any circumstances.

EXCLUSIONS
88 — Self-Insured Managed-Care Option 2001
Hospice services that are not covered
The following hospice services are not covered:
�� Services by volunteers or persons who do not normally charge for their services;
�� Services by a licensed pastoral counselor to a congregation member in the normal course of duties as a
pastor or minister;
��Charges for funeral arrangements;
��Charges for financial or legal counseling, including estate planning and the drafting of a will;
��Homemaker or caretaker services; and
��Bereavement counseling in excess of Plan maximums determined by the third-party administrators as
consistent with local practice.
Illegal acts
The Plan does not cover expenses arising as the result of or in the course of the patient committing an
illegal act.
Infertility treatment
The Plan does not cover artificial insemination, in vitro fertilization, fertility drugs, GIFT, ZIFT, charges
involving surrogates, storage of eggs or semen, fetal implants, embryo implants, sonograms, or other
infertility or surgical procedures. (The Plan does, however, cover the diagnostic workup to confirm a
diagnosis of infertility.)
Instructional programs
The Plan does not cover instructional or educational programs (such as, but not limited to, childbirth
classes, vocational training and testing, weight-loss or smoking cessation – some of the plans do offer
optional specialized programs for certain of these conditions). Diabetic education is covered, however, as
noted in the cost-sharing tables.
Investigative procedures, tests, treatments, drugs, devices, or services
These are not covered under any circumstances. (See page 54 for the definition of investigative.)
In vitro fertilization
Expenses related to in vitro fertilization are not covered under any circumstances.
Lasix surgery
Charges related to Lasix eye surgery are not covered under any circumstances.
Learning disorders, developmental delays or mental retardation, defects and deficiencies
Expenses related to services, treatment, educational testing, or training for learning disorders,
developmental delays, or mental retardation, defects and deficiencies are not covered. This exclusion does
not apply, however, to covered mental health services or to medical treatment of those with these listed
conditions which would otherwise be covered under the Plan.
Lifetime maximums
Expenses in excess of lifetime maximums are not covered under any circumstances.
Mammaplasty
The Plan does not cover mammaplasty done for augmentation, reduction, asymmetry, or removal of
silicone implants unless it is determined by the appropriate third-party administrator’s Medical Director to
be medically necessary or is required by law to achieve symmetry following a covered mastectomy.

EXCLUSIONS
Self-Insured Managed-Care Option 2001 — 89
Mandated or court-ordered care
The Plan does not cover any medical, psychological, or psychiatric care which is the result of a court order
or mandated by a third party (such as your employer, licensing board, recreation council, or school). The
Plan does not cover care for conditions that state or local law requires to be treated in a public facility,
including but not limited to, commitment due to mental disorders.
Massage therapy
The Plan does not cover charges for massage therapy under any circumstances.
Medical reports
The Plan does not cover charges for medical reports or for provider appearances at hearings or court
proceedings.
Motor-vehicle-accident-related services
The Plan does not cover services that are eligible for payment under the provisions of an automobile
insurance contract or pursuant to any federal or state law which mandates indemnification for such services
to persons suffering bodily injury from motor vehicle accidents, where permitted by state law.
Nutritional counseling
The Plan does not cover dietary control counseling or weight maintenance programs.
Obesity
The Plan does not cover any surgery, medical service or supply meant for the control of obesity or morbid
obesity (such as dietary control, counseling or weight maintenance programs), even if the obesity or
morbid obesity aggravates another condition or illness, except as noted under “Covered expenses/supplies”
on page 73.
Occupational therapy supplies
The Plan does not cover occupational therapy supplies, even if the occupational therapy itself is covered.
Organ and tissue transplant services
The Plan does not cover artificial organs, artificial parts, non-human donors, implantation services, and
other related services. Only transplant expenses as specified on page 75 are covered.
Medical expenses of an organ donor are typically charged to the organ recipient. The Plan does not cover a
non-Unisys donor in a transplant procedure unless the recipient of the transplant is a Unisys participant in
this Plan or another Unisys health plan. If the Unisys Plan participant is the recipient, coverage is provided
only for a live donor, to the extent benefits are unavailable from any other source.
Palliative care
See the definition on page 56. The Plan excludes treatments which are solely of a palliative nature, with
the exception of precertified palliative care given to the terminally ill through a covered hospice program.
Personal convenience items
The Plan does not cover expenses associated with personal convenience items. Excluded items include,
but are not limited to, telephone and television rentals, guest trays, or guest accommodations.
Plastic or reconstructive surgery
See pages 57 and 76.
Premarital laboratory work
Premarital laboratory work is not covered under any circumstances.

EXCLUSIONS
90 — Self-Insured Managed-Care Option 2001
Preparation of itemized bills or benefits requests
The Plan does not cover expenses associated with the preparation of itemized bills, benefits requests or
claim forms.
Preventive or routine care
Preventive or routine examinations, immunizations, and inoculations are covered only if the services are
provided by your PCP/PCC* ** or network OB/GYN, subject to the frequency and services deemed
appropriate by the third-party administrator for the patient’s age, sex and geographic location.
Private duty nurses
Private duty nurses generally are not covered. The few exceptions are described elsewhere in this booklet
and must be approved by the Medical Director for the appropriate third-party administrator or the
director’s designee.
Private room
If you occupy a private room, you must pay the difference between the hospital's charges for a private room
and the hospital's most common charge for semi-private accommodations. If the appropriate third-party
administrator determines that it was medically necessary for you to have a private room, or if a semi-
private room was not available, however, the Plan will cover the private room.
Refractive eye procedures
Charges for refractive eye procedures to improve/correct vision are not covered under any circumstances.
The excluded procedures include, but are not limited to: radial keratotomy, laser eye surgery, and lasix
surgery.
Required examinations
The Plan does not cover examinations for obtaining or maintaining employment, insurance or professional
or other licenses. Further, the Plan does not cover examinations before athletic or recreational activities or
for school, camp, or other program unless it is coincidentally the periodic routine examination by your
designated PCP/PCC* ** or network OB/GYN.
Resident physician or intern
The Plan does not cover services provided by a resident physician or intern rendered in that capacity.
These typically are billed as part of the inpatient or outpatient care from the facility.
Respite care
Respite care is not covered with the exception of precertified respite care given to temporarily relieve the
primary caregiver of the terminally ill through a covered hospice. To be covered, the respite care must be
precertified.
Reversal of any sterilization procedure
The reversal of any sterilization procedure is not covered, even if the sterilization procedure was covered.
Routine foot care
The Plan does not cover routine foot care for the cutting or removal of corns or calluses, or the trimming of
nails (including mycotic nails) when not medically necessary. (Note: Diabetic foot care coordinated by
your PCP/PCC* ** is covered, as well as routine foot care if you have a peripheral vascular disease,
peripheral neuropathies, or blindness.)
* Note for Medica Self-Insured: Medica allows you to refer yourself to network providers without referral from
your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. Copayments and
coinsurance are higher under Tier II than when you obtain a referral from your PCC (Tier I).
** Note for SelectAdvantage for services on or after July 1, 2001: SelectAdvantage allows you to refer yourself to
any network provider. This is called “self-referral.”

EXCLUSIONS
Self-Insured Managed-Care Option 2001 — 91
Safe surrounding
Charges for care furnished mainly to provide a surrounding free from exposure that can worsen a medical
condition or mental disorder are not covered.
Second surgical opinion and consultation with specialist
The Plan does not cover both a second surgical opinion and a consultation with the same specialist for the
same surgical procedure.
Self-referred services* **
The Plan does not cover most services obtained without prior written or electronic referral by your
PCP/PCC* **. The exceptions are:
�� Routine gynecological care by a network specialist;
�� Covered vision examinations by a network specialist; and
�� Self-referral services that the third-party administrator endorses throughout their network – if in doubt,
contact Member Services at the telephone number on the inside front cover of this booklet to
determine if self-referral is available for the services you require
Speech therapy
Except as noted on page 78, the Plan does not cover speech therapy, evaluation, diagnosis, or treatment.
The Plan does not cover the diagnosis and correction of speech impediments (stuttering or lisps, for
example), assistance in the development of verbal clarity, or treatment of children diagnosed with learning
disorders, developmental delays or non-severe communication deficits.
Surrogate mother's expenses
Expenses related to surrogate mothers are not covered under any circumstances.
Telephone calls
The Plan does not cover charges for telephone calls, including calls made by your provider to another
provider or to a health-care plan. The telephone expenses and provider's time spent on the phone are
excluded.
Transfer to a different hospital
The Plan does not cover admission to a different hospital when care for the condition is available at the
network hospital where you were first admitted.
Travel, transportation, or living expenses
The Plan does not cover the travel, transportation, or living expenses of a physician or a covered person
except professional ambulance services as listed under “Covered Expenses” or travel expenses for
treatment authorized through the case management programs of the third party administrator. These
programs generally are limited to situations involving highly specialized care at designated treatment
facilities or for organ or tissue transplants at designated treatment facilities. In those situations, the case
manager will indicate what travel expenses may be reimbursed.
* Note for Medica Self-Insured: Medica allows you to refer yourself to network providers without referral from
your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. You pay more under
Tier II than when you obtain a referral from your PCC (Tier I).
** Note for SelectAdvantage for services on or after July 1, 2001: SelectAdvantage allows you to refer yourself to
any network provider. This is called “self-referral.”

EXCLUSIONS
92 — Self-Insured Managed-Care Option 2001
Travel-related immunizations
Travel-related immunizations are not covered.

EXCLUSIONS
Self-Insured Managed-Care Option 2001 — 93
Treatment not prescribed or recommended by a physician
Treatment not prescribed or recommended by a physician is not covered under any circumstances.
Vaccinations, inoculations, or immunizations
These services are covered only if provided by your PCP/PCC* ** and not done strictly for travel
requirements.
Vision training therapy or vision perception training
These services are not covered under any circumstances.
Voice training and voice therapy
Except as noted on page 78, the Plan does not cover voice or speech therapy, evaluation, diagnosis, or
treatment. The Plan does not cover the diagnosis and correction of speech impediments (stuttering or lisps,
for example), assistance in the development of verbal clarity, or treatment of children diagnosed with
learning disorders, developmental delays or non-severe communication deficits.
Work-related condition or disability treatments
The Plan does not cover any service, supply, or treatment due to a condition or disability that would entitle
you to any benefit under a Workers' Compensation act or similar legislation.
* Note for Medica Self-Insured: Medica allows you to refer yourself to network providers without referral from
your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-referral
provider, as well as all covered services ordered or coordinated by the self-referral provider. Copayments and
coinsurance are higher under Tier II than when you obtain a referral from your PCC (Tier I).
** Note for SelectAdvantage for services on or after July 1, 2001: SelectAdvantage allows you to refer yourself to
any network provider. This is called “self-referral.”


SPECIAL PROGRAMS
Self-Insured Managed-Care Option 2001 — 95
SPECIAL PROGRAMS

SPECIAL PROGRAMS
96 — Self-Insured Managed-Care Option 2001
SPECIAL PROGRAMS
In addition to the numerous benefits described earlier in this booklet, the third-party administrators provide
a number of special programs designed to:
�� Enhance your life style,
�� Keep you healthy, or
�� Assist you when you have complex special health-care needs.
Some offer discounts on alternative medical treatments that are not covered by the Plan.
These programs are described separately in literature provided by the appropriate third-party administrator,
in newsletters, and on their websites (see page 6 for URL addresses). You are encouraged to read literature
you receive at home and to access the websites frequently.
CLAIMS, COMPLAINTS, APPEALS
Self-Insured Managed-Care Option 2001 — 97
CLAIMS AND COMPLAINT/APPEALS
PROCEDURE

CLAIMS, COMPLAINTS, APPEALS
98 — Self-Insured Managed-Care Option 2001
HOW TO FILE A CLAIM
Network providers submit benefits requests for all services they perform. You are required to submit a
written request for payment of expenses associated with services you receive from non-network providers
— for example, for treatment of a medical emergency.
Information needed for a claim
Your written request should include all of the following information:
��Name and Social Security number of the Unisys employee or former Unisys employee;
��Contract number shown on your medical ID card (not your Paid Prescription Drug ID card); and
�� Itemized statement from the provider showing the dates of service, the diagnosis code, the procedure
codes for their services, the full name and address of the provider, and the charge for each service.
Address for claims submissions
Your written request with the information noted above, should be forwarded to the appropriate third-party
administrator at one of the following addresses:
Aetna U.S. Healthcare
Member Services
980 Jolly Road
PO Box 129
Blue Bell PA 19422-0770
HealthPartners, Inc.
Claims Department
8100 – 34th Avenue South
PO Box 1289
Minneapolis MN 55440-1289
Medica Self-Insured
Route 2901
PO Box 169061
Duluth MN 55816-8310
For services on and before 6/30/01
SelectCare, Inc.
PO Box 369
Troy MI 48007
For services on and after 7/01/01
Select Advantage
ABS, Inc.
PO Box 37506
Oak Park MI 48237-0506
You will receive an explanation of benefits (EOB) statement that indicates payments and the balance of
submitted expenses for which you are responsible.
Some expenses are not reimbursable
Following are some examples of situations for which benefits may not be payable. The list is not all-
inclusive.
��You receive treatment from a provider other than your PCP/PCC* ** in a non-emergency situation
without a prior written or electronic referral from your PCP/PCC* **.
��You obtain services in the emergency room of a hospital and your condition did not meet the
requirements for a medical emergency or urgent medical need.
��You receive post-emergency (or post-urgency) follow-up treatment without a prior written or electronic
referral from your PCP/PCC* **.
��You receive services not covered under the Plan.
* Note for Medica Self-Insured members: Medica allows you to refer yourself to network providers without referral
from your PCC. This is called “self-referral.” Tier II benefits apply for all covered services directly from the self-
referral provider, as well as all covered services ordered or coordinated by the self-referral provider. You pay more
under Tier II than when you obtain a referral from your PCC (Tier I).
** Note for SelectAdvantage for services on or after July 1, 2001: SelectAdvantage allows you to refer yourself to
any network provider. This is called “self-referral.”

CLAIMS, COMPLAINTS, APPEALS
Self-Insured Managed-Care Option 2001 — 99
Following are some examples of situations for which part, but not all, of the submitted expenses may be
payable. The list is not all-inclusive:
�� Part or all of the expenses are payable under other coverage which pays before this Plan.
�� The expenses submitted exceed R&C (see page 57 for a definition of R&C).
�� Services exceed benefit maximums (for example, chiropractic care, physical therapy, treatment for
mental health or substance abuse, or home-health care).
Filing limitations
Your request for payment should be submitted as early as possible, and in no event later than 12 months
after you receive the service. If the Plan is ever terminated, final benefits requests must be received within
90 days of the date the Plan is terminated.
Payees
Payment is made directly to the provider.
Delayed payments
In the event that a benefit is denied in whole or in part and a complaint is filed or an appeal is made, the
Plan is not obligated to pay any part of the disputed expense until a final determination has been made
under the complaint and appeals procedure described below.
Right to recover excess payments
If payments are made in excess of the benefits due under the Plan, Unisys has the right to recover these
excess payments from any person or organization to whom the excess payments are made. If excess
payments are made to you, and upon request to do so you fail to return the excess payments, further
payments are withheld until the full excess payment amount is recovered.
COMPLAINT AND APPEALS PROCEDURE
You have the right to register complaints and appeal determinations made by the third-party administrator.
The Plan is obligated to hear and resolve complaints, according to the procedures described in this section.
This includes complaints about network providers and disagreements with benefit determinations.
Registering a Complaint or Disagreement with a Determination
If you submit a request for medical benefits and your request is denied in whole or in part, you will receive
a determination explaining why your request has been denied, and advising you of your right to appeal the
determination.
The following pages outline the informal process to resolve disagreements and the formal process for
submitting complaints or appealing medical benefit determinations under the Plan.
1. Contact Member Services
If you have a complaint, or a benefit has been denied in part or in full and you disagree
with this determination, call Member Services at the telephone number listed inside the
front cover of this supplement. To assist in the investigation of your complaint or
disagreement, provide as many of the pertinent details relating to your complaint as
possible. For example, be sure to include the full names of the persons involved, the dates
involved, and the chronological sequence of events.
If your complaint involves issues relating to quality of health care rendered by a network
provider, you also should attempt to discuss the quality of care issues with the provider.
The Member Services representative will assist you in trying to resolve the complaint or

CLAIMS, COMPLAINTS, APPEALS
100 — Self-Insured Managed-Care Option 2001
disagreement on an informal basis. The representative also will document the complaint.
Most disagreements can be resolved at this level.
2. Submit missing information or an informal written complaint
The written notice explaining why a benefit request is denied refers to the provision upon
which the denial is based. If the denial is because you did not submit all the required
information, the written notice will tell you what is missing so that you can resubmit the
request. The written notice also explains the review procedure.
If discussions with the Member Services Department are not satisfactory, you may submit
a written complaint or disagreement with a benefits determination to the appropriate plan
administrator at:
Aetna U.S. Healthcare
Member Services
MidAtlantic Grievance Appeals
PO Box 936, Mail Stop U296
Blue Bell PA 19422
Fax 215-775-5168
Member Services
HealthPartners, Inc.
8100 – 34th Avenue South
PO Box 1309
Minneapolis MN 55440-1309
Medica Self-Insured
Customer Services
Route 0501
PO Box 9310
Minneapolis MN 55440-9310
SelectAdvantage
ABS, Inc.
PO Box 37506
Oak Park MI 48237-0506
You will receive a reply within 45 days of receipt of the written request unless additional
information is necessary from you or the provider, in which case, the reply will be
forwarded within 45 days of receipt of the additional information.
It will be assumed that the complaint has been satisfactorily resolved unless you file a
formal grievance within 60 days of the date of the reply to your initial complaint.
3. Submit a formal grievance for review by the third-party administrator
The grievance committee or equivalent group for each of the third-party administrators
reviews and investigates all formal grievances within 30 days of receipt unless additional
information required to resolve the grievance is not received from you or the provider
during the 30-day period. The decision of the grievance committee or equivalent group is
final and binding unless you appeal to the Unisys Employee Benefits Administrative
Committee within 30 days of the date of the decision by the grievance committee.
4. Request review by the Unisys Employee Benefits Administrative Committee
If a request for benefits is denied in whole or in part by the third-party administrator’s
grievance committee, and you disagree with the determination, you have the right to
appeal the determination and request a review by the Unisys Employee Benefits
Administrative Committee, which is responsible for ensuring that the Plan is administered
in accordance with the terms of the Plan and for interpreting the Plan provisions.
Your appeal must be in writing and should be sent to the appropriate third-party
administrator within 60 days after you receive the determination from the grievance
committee. Your appeal should include all information, evidence, and documents that may
support your request, and you may review pertinent documents the third-party
administrator may have.
The third-party administrator will ensure that no mistake has been made at an earlier level

CLAIMS, COMPLAINTS, APPEALS
Self-Insured Managed-Care Option 2001 — 101
of review, and will forward your appeal to the Unisys Benefits Administrative Committee
on your behalf.
You will be notified of the Unisys Employee Benefits Administrative Committee's
decision within 60 days after your appeal is received. This period may be extended if you
are required to submit additional information, or if special circumstances require delay. In
any event, you will be notified of the Committee's decision no later than 120 days after
your appeal is received.
If your appeal is denied, the decision will be written in a manner calculated to be
understood by you and will specify the particular reasons for the decision.
A determination by the Unisys Employee Benefits Administrative Committee exhausts
your appeal rights under the Plan.
Appeals of Precertification Determinations
If you or your physician disagree with a precertification determination, you or your physician may appeal
by writing to the appropriate third-party administrator within 60 days of the date the decision is made.
Your case will be reviewed by a Medical Director or physician consultant different from the one who
originally determined that the care was not medically necessary.
Circumstances which may have prevented you from following the precertification guidelines and
procedures also are taken into consideration.
The third-party administrator will reach a decision within 30 days from the date your appeal of a
precertification determination is received. The administrator will tell you, your physician and any other
provider involved in your care of the decision. If you continue to disagree with the determination, you can
request that your appeal be heard by the Unisys Benefits Administrative Committee by following the
guidelines described in the preceding pages.
Appeals for the denial of a precertification when there is a serious medical emergency requiring rapid
processing, are handled in an expedited appeal process upon request.


ADDITIONAL INFORMATION
Self-Insured Managed-Care Option 2001 — 103
ADDITIONAL INFORMATION
ABOUT THE PLAN

ADDITIONAL INFORMATION
104 — Self-Insured Managed-Care Option 2001
ADDITIONAL INFORMATION ABOUT THE PLAN
Refer to the Summary Plan Description (SPD) booklet referenced on the inside front cover of this
supplement for general information about the Official Plan Name, Plan Number, Plan Sponsor, Employer
Identification Number, Plan Year, Plan Administration and Named Fiduciary, Type of Plan,
Administration, Right of Recovery, Third Party Liability, Agent for Legal Process, Conflicts with Existing
Law, and Your Rights Under ERISA. In addition, the following is important information about the Plan.
In addition, the following information about the Plan is important.
Funding
Benefits are funded by Unisys Corporation and contributions by employees, former Unisys employees, and
their dependents.
Right to Receive and Release Needed Information
Certain facts are needed to apply some of the provisions of the Plan. The third-party administrators rely
mainly upon the information that you provide. The administrators also may collect information from other
sources to perform its functions with regard to application of the provisions of the Plan.
The third-party administrators have the right to decide which facts are needed.
Consistent with applicable state and federal law, needed facts may be obtained from or given to any other
organization or person, without your further approval or consent unless applicable federal or state law
prevents disclosure of the information without your consent. Information may be made available to:
�� The third-party administrators and their representatives in connection with benefits requests and
financial administration of the Plan. This includes Plan audits.
��Other health-care coverage providers, if the possibility of other coverage exists or there is a need to
preserve the continuity of your coverage.
�� Peer Review Organizations and other agencies to determine whether or not health-care services were
medically necessary or reasonably priced.
��Government regulators of health-care businesses and to others as required by law.
�� Law enforcement authorities when necessary to prevent or prosecute fraud or other illegal activities.
Right to develop guidelines
The third-party administrators have the right to develop or adopt guidelines that establish in more detail the
instances and procedures when the Plan will pay for services. Examples of the use of the guidelines are to
determine whether care was:
��Medically necessary,
��Covered or excluded emergency care in the outpatient department of a hospital, or
��Of a custodial, maintenance or palliative nature.
These guidelines interpret and illustrate the Plan provisions and will not be contrary to any term or part of
the Plan.

ADDITIONAL INFORMATION
Self-Insured Managed-Care Option 2001 — 105
Access to records and confidentiality
By receiving benefits under the Plan, you authorize access to any health records and medical information
held by any health-care provider who delivers services to you under the Plan. You also authorize use of
your health records, when necessary, for: claims processing, including claims made for reimbursement or
subrogation; quality of care assessment; referrals to other providers; performance of case management;
underwriting; utilization review; utilization information to your treating providers; and evaluation of
potential or actual coverage under the Plan.
Medical records and information about your care that the Plan gets from providers are confidential. The
Plan will disclose information to others only as required to coordinate benefits, or with your written
consent. State and federal laws governing the confidentiality of medical records are followed at all times.
Amendments to this Supplement
Amendments included in this supplement, or sent to you at a later date, are incorporated and fully made a
part of the Plan.
Case review
The services of professional medical reviewers may be retained to examine and render expert opinions
regarding any charges, records or other documentation relating to expenses submitted to the Plan for
determination of benefits payable.
Extension of benefits
If you are confined in any institution in which benefits are available under the Plan when coverage ends,
benefits for the facility continue to be paid for the stay until the earlier of 90 days, the date of discharge
from the institution, or the date upon which the Plan's maximum benefit is reached.


INDEX
Self-Insured Managed-Care Option 2001 — 107
INDEX

INDEX
108 — Self-Insured Managed-Care Option 2001
INDEX
A
Abortion, legal ..............................55, 66, 69, 81
Access to records ..........................................105
Acupresure......................................................84
Acupuncture ...................................................66
Aetna U.S. Healthcare ................................20
HealthPartners ............................................27
Medica ........................................................36
SelectAdvantage .........................................46
Adoption.....................................................8, 84
Air conditioner....................................69, 84, 86
Air filter ....................................................69, 86
Air purifier................................................69, 86
Allergy testing and treatment..........................74
Aetna U.S. Healthcare ................................17
HealthPartners ............................................24
Medica ........................................................31
SelectAdvantage .........................................41
Alternates to hospital care...............................50
Aetna U.S. Healthcare ................................17
HealthPartners ............................................24
Medica ........................................................32
Precertification............................................62
....................................................................42
Alternatives to hospital care
SelectAdvantage .........................................42
Ambulance......................................................66
Aetna U.S. Healthcare ................................18
Covered services.........................................50
Definition....................................................50
HealthPartners ............................................25
Medica ........................................................33
SelectAdvantage .........................................43
Ambulatory surgical center.................50, 66, 71
Amendments.................................................105
Amniocentesis ................................................66
Anesthesia ......................................................71
Covered services.........................................67
Dental treatment .........................................68
Anesthesia, inpatient
Aetna U.S. Healthcare ................................17
HealthPartners ............................................24
Medica ........................................................32
SelectAdvantage .........................................42
Arch support .............................................69, 86
Artificial insemination ..................72, 74, 84, 88
Autologous blood donations ...........................84
Automobile accidents .....................................89
Autopsy ..........................................................84
B
Bath chair ................................................. 69, 86
Bathtub rail............................................... 69, 86
Birthing center.......................................... 67, 71
Definition ................................................... 50
Blood/blood plasma.................................. 71, 85
Breast pump ............................................. 69, 86
C
Cancer screening ...................................... 67, 75
Aetna U.S. Healthcare................................ 16
................................................................... 23
Medica........................................................ 30
SelectAdvantage......................................... 41
Cardiac rehabilitation ..................................... 76
Cardiography.................................................. 71
Case review .................................................. 105
Cataract .................................................... 85, 86
Cataracts......................................................... 67
Chelating agents ............................................. 85
Chemotherapy .......................................... 67, 74
Chiropractic services ...................................... 77
Aetna U.S. Healthcare................................ 20
HealthPartners ............................................ 27
Medica........................................................ 36
SelectAdvantage......................................... 46
Chromosomal anlaysis.................................... 66
Circumcision ...................................... 55, 66, 81
Claims ............................................................ 98
Filing limitations ........................................ 99
Cognitive therapy ........................................... 76
Aetna U.S. Healthcare................................ 20
HealthPartners ............................................ 28
Medica........................................................ 37
SelectAdvantage......................................... 47
Complaints and appeals.................. 99, 100, 101
Contact lenses..................................... 67, 85, 86
Convenient/urgent care center
Definition ................................................... 51
HealthPartners ............................................ 24
Medica........................................................ 31
Copayment
Definition ................................................... 51
Corset ....................................................... 69, 86
Cosmetic................................. 51, 58, 76, 84, 85
Cost-sharing tables ......................................... 13
Aetna U.S. Healthcare.. 15, 16, 17, 18, 19, 20
HealthPartners ........ 21, 23, 24, 25, 26, 27, 28

INDEX
Self-Insured Managed-Care Option 2001 — 109
Medica ..............29, 30, 31, 32, 34, 35, 36, 37
SelectAdvantage39, 40, 41, 42, 43, 44, 46, 47
Custodial supportive care .51, 54, 58, 66, 70, 79,
85, 104
D
Deductible
Aetna U.S. Healthcare ................................16
HealthPartners ............................................23
Medica ........................................................30
SelectAdvantage .........................................40
Dehumidifier.......................................69, 84, 86
Delivery
Aetna U.S. Healthcare ................................17
HealthPartners ............................................24
Medica ........................................................32
SelectAdvantage .........................................42
Dental .......................................................55, 86
Aetna U.S. Healthcare ................................20
Covered ......................................................68
HealthPartners ............................................27
Medica ........................................................36
Not covered ................................................86
SelectAdvantage .........................................46
Developmental delays.....................................88
Diabetes self-management ........................86, 88
Aetna U.S. Healthcare ................................20
HealthPartners ............................................27
Medica ........................................................36
SelectAdvantage .........................................46
Diabetic supply
Glucometer ...........................................52, 68
Insulin pump...............................................68
Insulin pump supplies...........................52, 68
Lancettes...............................................52, 68
Syringes ................................................52, 68
Test strips .............................................52, 68
Dialysis .....................................................68, 71
Directory of network providers.........................6
Drugs and medicines, fertility.........................88
Drugs and medicines, inpatient...........71, 73, 80
Drugs and medicines, investigative ..........54, 88
Drugs and medicines, prescription......52, 68, 75
Drugs and medicines, take-home........52, 74, 80
Durable medical equipment (DME)
Aetna U.S. Healthcare ................................20
Covered ......................................................68
HealthPartners ............................................27
Medica ........................................................37
Not covered ................................................86
Precertification............................................62
SelectAdvantage .........................................46
E
Education ....................................................... 86
Elective admission.......................................... 52
Elective surgery.............................................. 52
Embryo implant.................................. 72, 86, 88
Emergency........................ 10, 11, 52, 62, 71, 98
Emergency room .................. 11, 52, 62, 71, 104
Aetna U.S. Healthcare................................ 18
HealthPartners ............................................ 25
Medica........................................................ 33
SelectAdvantage......................................... 43
Encephalography............................................ 71
Environmental equipment .............................. 86
Exercise equipment ............................ 69, 73, 86
Extension of benefits .................................... 105
Eyeglasses .......................................... 67, 85, 86
F
Family or household members........................ 87
Fee, negotiated ............................................... 56
Fetal implant....................................... 72, 87, 88
First aid supplies ............................................ 87
Food supplements/substitutes......................... 87
Foot care......................................................... 90
Funding ........................................................ 104
G
Gender reassignment ...................................... 87
Generator, back-up ......................................... 86
Genetic testing/counseling.............................. 87
GIFT......................................................... 72, 88
Glucometer ........................................68, 69. See
Government programs.................................... 87
Guideline development................................. 104
H
Health club dues............................................. 73
Hearing aid ..................................................... 87
Home health care............................................ 53
Aetna U.S. Healthcare................................ 17
Covered ...................................................... 70
HealthPartners ............................................ 24
Medica........................................................ 32
Not covered ................................................ 70
Precertification ........................................... 63
SelectAdvantage......................................... 42
Home IV therapy
Aetna U.S. Healthcare................................ 17
HealthPartners ............................................ 24

INDEX
110 — Self-Insured Managed-Care Option 2001
Medica ........................................................32
Precertification............................................63
SelectAdvantage .........................................42
Homebound ....................................................53
Hospice...........................................................53
Aetna U.S. Healthcare ................................17
Covered ......................................................70
HealthPartners ............................................24
Medica ........................................................32
Not covered ................................................88
Precertification............................................63
SelectAdvantage .........................................42
Hospital ..........................................................54
Government ................................................87
Inpatient......................................................71
Transfer ......................................................91
Hospital emergency room .............11, 52, 62, 71
Aetna U.S. Healthcare ................................18
HealthPartners ............................................25
Medica ........................................................33
SelectAdvantage .........................................43
Hospital services
Covered ......................................................71
Precertification............................................62
Private room .........................................71, 90
Hospital services, inpatient
Aetna U.S. Healthcare ................................17
HealthPartners ............................................24
Medica ..................................................31, 32
SelectAdvantage .........................................42
Hospital services, outpatient .............68, 71, 104
Aetna U.S. Healthcare ................................18
HealthPartners ............................................25
Medica ........................................................33
SelectAdvantage .........................................43
Hospital visits
Aetna U.S. Healthcare ................................17
Covered ......................................................72
HealthPartners ............................................24
Medica ........................................................32
SelectAdvantage .........................................42
Humidifier ..........................................69, 84, 86
Hypno-therapy ................................................84
I
In vitro fertilization.............................72, 84, 88
Infertility diagnosis .............................72, 74, 88
Aetna U.S. Healthcare ................................20
HealthPartners ............................................27
Medica ........................................................37
SelectAdvantage .........................................46
Infertility treatment .............................72, 74, 88
Aetna U.S. Healthcare ................................20
HealthPartners ............................................ 27
Medica........................................................ 37
SelectAdvantage......................................... 46
Infertility treatments ....................................... 88
Inpatient ......................................................... 54
Instructional.................................................... 88
Insulin pump ............................................ 52, 68
Intern .............................................................. 90
Investigative/investigational ......... 54, 55, 68, 88
Itemized bill preparation................................. 90
J
Jobst stockings.......................................... 69, 86
L
Lab and x-ray ................................. 8, 68, 81, 89
Lab and x-ray, in office .................................. 74
Aetna U.S. Healthcare................................ 17
HealthPartners ............................................ 24
Medica........................................................ 31
SelectAdvantage......................................... 41
Lab and x-ray, independents..................... 67, 74
Aetna U.S. Healthcare................................ 18
HealthPartners ............................................ 25
Medica........................................................ 33
SelectAdvantage......................................... 43
Lab and x-ray, inpatient...................... 71, 73, 80
Aetna U.S. Healthcare................................ 17
HealthPartners ............................................ 24
Medica........................................................ 31
SelectAdvantage......................................... 42
Lab and x-ray, outpatient.......................... 74, 80
Laser eye surgery............................................ 90
Lasix surgery ............................................ 88, 90
Learning disorders.......................................... 88
Life-threatening .............................................. 55
Lifetime maximum ......................................... 88
Aetna U.S. Healthcare................................ 16
HealthPartners ............................................ 23
Medica........................................................ 30
SelectAdvantage......................................... 40
M
Maintenance care...... 55, 58, 66, 70, 79, 85, 104
Mammaplasty ................................................. 88
Mandated care ................................................ 89
Massage therapy ............................................. 89
Medical necessity ................. 52, 58, 66, 71, 104
Definition ................................................... 55
Medical report ................................................ 89

INDEX
Self-Insured Managed-Care Option 2001 — 111
Medical supplies .............................................56
Mental disorder...............................................56
Mental health treatments...........................72, 80
Aetna U.S. Healthcare ................................19
HealthPartners ............................................26
Medica ........................................................34
Precertification............................................63
SelectAdvantage .........................................44
Missed appointments ......................................84
N
Newborn ...............................................8, 71, 72
Nutritional counseling ....................................89
O
Obesity............................................................89
Obesity, morbid ........................................56, 73
Occupational therapy ......................................77
Aetna U.S. Healthcare ................................20
Covered ......................................................70
HealthPartners ............................................28
Medica ........................................................37
SelectAdvantage .........................................47
Supplies ......................................................89
Office visits ....................................................74
Aetna U.S. Healthcare ................................17
HealthPartners ............................................24
Medica ........................................................31
SelectAdvantage .........................................41
........................................................................75
Orthotics ...................................................69, 86
Out-of-pocket maximum.................................84
Aetna U.S. Healthcare ................................16
HealthPartners ............................................23
Medica ........................................................30
SelectAdvantage .........................................40
Outside the service area ..................................11
Aetna U.S. Healthcare ................................12
HealthPartners ............................................12
Oxygen ...........................................................75
P
Palliative care ...........53, 56, 66, 70, 76, 89, 104
Aetna U.S. Healthcare ..........................17, 20
HealthPartners ................................24, 27, 28
Medica ............................................32, 36, 37
SelectAdvantage .............................42, 46, 47
Pathology........................................................68
Personal convenience..........................71, 85, 89
Physical therapy........................................75, 77
Aetna U.S. Healthcare................................ 20
Covered ...................................................... 70
HealthPartners ............................................ 28
Medica........................................................ 37
SelectAdvantage......................................... 47
PKU.......................................................... 69, 75
Aetna U.S. Healthcare................................ 20
HealthPartners ............................................ 27
Medica........................................................ 37
SelectAdvantage......................................... 47
Port wine stain
Medica........................................................ 37
Preadmission testing....................................... 75
Precertification ............................................... 62
Aetna U.S. Healthcare................................ 16
HealthPartners ............................................ 23
Medica........................................................ 30
SelectAdvantage......................................... 40
Premarital lab ................................................. 89
Prenatal care
Aetna U.S. Healthcare................................ 16
Definiton .................................................... 57
HealthPartners ............................................ 23
Medica........................................................ 30
SelectAdvantage......................................... 40
Private duty nurse........................................... 90
Prosthetic devises
Aetna U.S. Healthcare................................ 20
Covered ...................................................... 69
HealthPartners ............................................ 27
Medica........................................................ 37
SelectAdvantage......................................... 47
Provider, network ........................................... 56
Providers, covered .......................................... 53
Psychologically necessary care....................... 57
Pulmonary therapy.......................................... 78
Aetna U.S. Healthcare................................ 20
HealthPartners ............................................ 28
Medica........................................................ 37
SelectAdvantage......................................... 47
R
Radial keratotomy .......................................... 90
Radiation ........................................................ 75
Radiology ....................................................... 68
Reasonable and customary (R&C) ..... 57, 66, 99
Reconstructive surgery ................................... 76
Aetna U.S. Healthcare................................ 20
Definition ................................................... 57
HealthPartners ............................................ 27
Medica........................................................ 37
SelectAdvantage......................................... 47
Referral

INDEX
112 — Self-Insured Managed-Care Option 2001
Definition....................................................58
Refractive eye procedure ................................90
Rehabilitative services ....................................76
Aetna U.S. Healthcare ................................20
HealthPartners ............................................28
Medica ........................................................37
Precertification............................................64
SelectAdvantage .........................................47
Release of information..................................104
Resident physician..........................................90
Respite care ..................................53, 58, 70, 90
Restorative......................................................58
Reversal of sterilization ..................................90
Routine exams
Aetna U.S. Healthcare ................................16
HealthPartners ............................................23
Medica ........................................................30
SelectAdvantage .........................................40
S
Safe surrounding.............................................91
Scoping procedures.............................67, 78, 81
Second surgical opinion..................................91
Second surgical opinions ................................79
Self-insured managed-care option ....................2
Self-referral.....................................................91
Shoes, corrective.............................................86
Shoes, insert....................................................69
Shoes, inserts ..................................................86
Shoes, molded.................................................69
Shower stool .............................................69, 86
Skilled nursing..................50, 53, 58, 59, 70, 85
Precertification............................................64
Skilled nursing facility..................54, 73, 79, 81
Aetna U.S. Healthcare ................................17
Definition....................................................58
HealthPartners ............................................24
Medica ........................................................32
Precertification............................................64
SelectAdvantage .........................................42
Spa..................................................................73
Specialized treatment facility....................72, 80
Aetna U.S. Healthcare ................................19
Definition....................................................59
HealthPartners ............................................26
Medica ..................................................34, 35
SelectAdvantage ...................................44, 45
Speech therapy....................................78, 91, 93
Aetna U.S. Healthcare ................................20
Covered ......................................................70
HealthPartners ............................................28
Medica ........................................................37
SelectAdvantage .........................................47
Stair glide ....................................................... 69
Stair glides...................................................... 86
Storage of eggs or semen.......................... 72, 88
Substance abuse treatments ...................... 73, 80
Aetna U.S. Healthcare................................ 19
HealthPartners ............................................ 26
Medica........................................................ 35
Precertification ........................................... 63
SelectAdvantage......................................... 45
Surgery ........................................................... 81
Definition ................................................... 59
Precertification ........................................... 64
Surgery, assistants .......................................... 67
Surgery, inpatient
Aetna U.S. Healthcare................................ 17
HealthPartners ............................................ 24
Medica........................................................ 31
SelectAdvantage......................................... 42
Surgery, office ................................................ 74
Aetna U.S. Healthcare................................ 17
HealthPartners ............................................ 24
Medica........................................................ 31
SelectAdvantage......................................... 41
Surgery, outpatient ......................................... 75
Aetna U.S. Healthcare................................ 18
HealthPartners ............................................ 25
Medica........................................................ 33
SelectAdvantage......................................... 43
Surgical center.................................... 50, 66, 68
Surrogate ............................................ 72, 88, 91
Swimming pool ........................................ 69, 86
T
Telephone calls............................................... 91
Third-party administrators ................................ 2
TMJ................................................................ 81
Toilet rail .................................................. 69, 86
Toilet seat, raised...................................... 69, 86
Transplant
Covered ...................................................... 75
Designated facility...................................... 51
Not covered ................................................ 89
Precertification ........................................... 64
Travel ............................................................. 91
Tub bench................................................. 69, 86
Tubal ligation ............................... 55, 66, 79, 81
U
Urgent medical need......... 10, 11, 59, 62, 71, 98
Definition ................................................... 59

INDEX
Self-Insured Managed-Care Option 2001 — 113
V
Vascetomy ..........................................55, 66, 79
Vasectomy ......................................................81
Vision
Aetna U.S. Healthcare ................................16
HealthPartners ............................................23
Medica ........................................................31
SelectAdvantage .........................................41
Vision training ................................................93
Vocational rehabilitation.................................70
W
Well-child care
Aetna U.S. Healthcare ................................16
HealthPartners ............................................ 23
Medica........................................................ 30
SelectAdvantage......................................... 40
Well-woman exams
Aetna U.S. Healthcare................................ 16
HealthPartners ............................................ 23
Medica........................................................ 30
SelectAdvantage......................................... 40
Whirlpool ....................................................... 86
Wigs and artificial hairpieces ......................... 69
Work-related................................................... 93
Z
ZIFT ......................................................... 72, 88

INDEX
114 — Self-Insured Managed-Care Option 2001



