insert publication title here
TRANSCRIPT

COVID-19
Palliative Care
Toolkit

Palliative Care Toolkit, version 2.2
2
Purpose The purpose of this palliative care toolkit is to provide Health Board planners with
support for local resilience planning during the COVID-19 pandemic. It is not
intended to replace existing palliative care processes and guidance documents but
instead it offers a range of practical approaches and tools that can be considered
and adapted locally in order to strengthen any local response to the COVID-19
situation.
The toolkit has been shared with a range of stakeholders for comment and has
been approved by the Scottish Government Professional Advisors Group (PAG) for
application during the COVID-19 outbreak.
The content of the toolkit will be reviewed post COVID-19 and consideration given
as to whether an adapted version should continue to be made available.
Version History Version Date Summary of changes
2.2 30/04/2020 Updated Appendix N title
Further Information For more information on COVID-19 see the COVID-19 guidance section of our
website, www.gov.scot/coronavirus

Palliative Care Toolkit, version 2.2
3
Contents Purpose .......................................................................................................................................2
Version History .........................................................................................................................2
Further Information .................................................................................................................2
Contents ......................................................................................................................................3
Executive Summary..................................................................................................................5
Section one: COVID-19 Contingency Plan – Scottish Palliative Care Pharmacy
Association 9
Section two - Strengthening Primary Care........................................................................15
Section three - Accessing oral palliative care medicines from Emergency
Departments during COVID-19 ............................................................................................18
Section four - Accessing palliative care medicines in care homes ..............................24
Appendix A: Prescribing dose ranges for COVID-19 palliative care patients during
the pandemic ...........................................................................................................................31
Appendix B: Single Nurse Administration (SNA) of Controlled Drugs .........................35
Appendix C: the SPOT clinical decision prescribing support tool .................................39
Appendix D: Example of Guidance for Prescribing and Administering PRN
medication when a Person is Imminently Dying from COVID-19 Lung disease .......42
Appendix E: SAMPLE Drug Administration Instruction Chart (courtesy of NHS
Tayside) .....................................................................................................................................43
Appendix F: SAMPLE Medication Administration Record ..............................................46
Appendix G: SAMPLE Communications Sheet ...................................................................48
Appendix H: Example of Just in Case Box prescribing from NHS Tayside ................49
Appendix I: Patient Group Direction (PGD) template - supply of paracetamol
500mg oral solid dosage form to patients with COVID-19 approaching the end of
life requiring relief from pain or fever, by appropriate registered healthcare
professionals in NHSScotland...............................................................................................53
Appendix J: Patient Group Direction (PGD) template - supply of morphine sulfate
10mg/5ml oral solution to patients with COVID-19 approaching the end of life
requiring relief from pain, breathlessness or cough by appropriate registered
healthcare professionals in NHSScotland. .........................................................................61
Appendix K: Patient Group Direction (PGD) template - supply of lorazepam 1mg
tablets, to patients with COVID-19 approaching the end of life requiring relief
from anxiety and distress, by appropriate registered healthcare professionals in
NHS Scotland. ...........................................................................................................................70
Appendix L: Patient Leaflet - Supply of medicines for control of symptoms ...........78
Appendix M: Coronavirus in care homes – visual............................................................83

Palliative Care Toolkit, version 2.2
4
Appendix N: Administration of palliative care medicine for care home residents at
end of life (courtesy of SPCPS based on a Model of Care developed by NHSGG&C)
....................................................................................................................................................84
Appendix O – Summary of issues to be considered to support care home residents
accessing palliative care medicines during the COVID-19 pandemic (courtesy of
SPCPS)........................................................................................................................................87
Appendix P – Members of Working Group for the Palliative Care Toolkit ................89

Palliative Care Toolkit, version 2.2
5
Executive Summary The aim of this toolkit is to help improve access to supportive and palliative care
medicines, within the scope of the Human Medicines Regulations 2012, including
the flexibilities provided during a pandemic situation, and the Misuse of Drugs
Regulations 2001. The toolkit provides Health Board planners with options that
can be adapted and utilised locally in their response to COVID-19. To assist with
this, several exemplars of documentation, policies, charts and flow diagrams have
been included in the appendices.
Guidelines
The appropriate reduction of suffering for those who are very ill or dying from
COVID-19 is paramount. Normally, the Scottish Palliative Care guidelines are the
reference point for the management of adults with life limiting illness. More
recently, temporary guidelines for symptom management for when a person is
imminently dying from COVID-19 and for supporting end of life care when
alternatives to medication normally given through syringe pumps are required
have been developed.
The first of these two new guidelines describes the symptoms of COVID-19 and
the palliative care medicines to help alleviate symptoms, at the end of life. The
second guideline describes alternative palliative care medicines that that can be
prescribed in the event that there is a shortage of essential palliative care
medicines, syringe pumps or district nursing staff to administer sub-cutaneous
medicines. It aims to support professionals, who are already skilled in providing
generalist palliative care, in identifying alternatives medicines and routes of
administration, when usual medicines or syringe drivers are not available.
This toolkit aligns with these two temporary Scottish Palliative Care guidelines in
order to strengthen the response across primary and secondary care and in the
various care settings where people require palliative care.
Sections
The toolkit comprises the following four sections:
Section one: palliative care contingency planning overview;
Section two: strengthening Primary Care in-hours and out-of-hours;
Section three: discharge from an Emergency Department; and
Section four: providing medicines to care homes.

Palliative Care Toolkit, version 2.2
6
Section one contains a palliative care contingency plan which describes a series of
priority areas and potential solutions which Health Board planners may wish to
consider in order to build a tiered approach to strengthening the palliative care
pathway. The contingency plan takes into account the different care settings, the
varying demographic and geographic profiles of communities and any existing
palliative care service provision. It suggests who should lead on any actions and
timescales. Some of these activities are described in more detail in sections two,
three and four.
Section two describes a range of measures that can be used to strengthen the
response from primary care services both in-hours and out-of-hours as well as
securing and protecting the medicine supply chain in order to reduce any
preventable waste. Appendices A-H contain a number of practical tools to support
this.
Section three outlines a new alternative of ‘To Take Out’ (TTO) packs for oral
palliative medicines as a discharge option for an Emergency Department. This will
support a quick discharge home and allow a carer or relative to administer oral
medicines to help alleviate symptoms. This may provide a suitable bridge before
a ‘Just in Case Box’ (JICB) can be arranged in the community, if required. There is
also a one page quick reference guide. In addition, appendices I-L include three
Patient Group Direction (PGD) templates for local adoption to facilitate the supply
of the TTO medicines and a Patient Information Leaflet (PIL) for supply with the
medicines.
Section four describes a number of ways to support access to medicines in care
homes. In particular, there are options to consider how to expand the use of
homely remedies to provide symptomatic relief, ways to increase access to
certain Prescription Only Medicines (POMs) using health board approved protocols
and approaches such as using anticipatory prescriptions for JICBs for residents to
minimise the waste of critical medicines. Appendices M-O provide specific tools
to support this.
Appendices
Underpinning each of these sections are appendices which provide existing
exemplar guidance documents and templates that a number of Health Boards
have developed and agreed to share. These include, in addition to what has been
described above, information on the Safer Prescribing of Opioids Tool (SPOT), a
summary of the sample Medication Administration Record (MAR) charts, guidance

Palliative Care Toolkit, version 2.2
7
on single nurse administration; guidance on the use of dose ranges; sample
communication sheets and district nurse administration sheets.
Reducing the risk of waste and avoidable medicine shortages
As a result of the global impact of COVID-19 there may be significant constraints
on the availability of a number of palliative care medicines. Throughout the
toolkit, there is an emphasis on approaches that minimise waste and reduce the
risk of avoidable medicine shortages. In addition, NHS England is developing
guidance on the repurposing of medicines in Care Homes and Hospices and NHS
Scotland will consider the outcome of this work when it is available.
Training
Additional guidance, training and support materials are available both through
Turas (NHS Education for Scotland) and various Royal Colleges and professional
bodies. One such example is the Royal College of General Practitioners’ guide on
Community Palliative, End of Life and Bereavement Care in the COVID-19
Pandemic.
Legislative considerations
There is an option to allow the supply of POMs to patients during the COVID-19
pandemic within the existing legislative provisions in the Human Medicines
Regulations 2012. Regulation 214 means a person may not supply a POM except
in accordance with a prescription given by an appropriate practitioner. However,
the Regulations also set out various exceptions to this rule. For example,
regulation 247 allows the supply of a POM without a prescription in a pandemic
situation, provided certain conditions are met. For example, the supply must be
made whilst a disease is, or in anticipation of a disease being imminently
pandemic and a serious risk, or potentially serious risk to human health. The
supply must be made under a disease specific protocol that specifies the
symptoms of and the treatment of that disease. The protocol must also be
approved by UK Ministers or an NHS body. “NHS body” includes territorial Health
Boards in Scotland. Any Health Board considering this approach will want to
satisfy themselves that any protocol complies with regulation 247 and the
legislation which sets out the requirements for controlled drugs, for example the
Misuse of Drugs Regulations 2001. The Central Legal Office (CLO) will be able to
provide Health Boards with advice on this.
Palliative Care Toolkit, version 2.2
8
Local adoption
Health Boards may wish to consider establishing a group of key stakeholders to
provide a whole system approach to reviewing and revising local process to
ensure that the medicines required for end of life care can continue to be
available to those who need them, when they need them.
The exemplars from Health Boards included in this toolkit will need adaption and
agreement for local implementation in line with local Health Board clinical
governance processes. Consideration should also be given to any additional
training required to support health and social care professionals in undertaking
any new or extended roles.
In view of concerns around medicines shortages during COVID-19, Health Boards
will also want to support national and local approaches to maintaining the supply
chain of palliative care medicines, discouraging the over-ordering of these
medicines and minimising the waste of relevant medicines.
Summary
This palliative care toolkit provides health and social care planners and healthcare
professionals with a range of options and tools to help them to identify
appropriate and effective measures to improve access to supportive and palliative
care medicines across different health and social care settings.

Palliative Care Toolkit, version 2.2
9
Section one: COVID-19 Contingency Plan – Scottish Palliative Care Pharmacy Association
Summary
There are a number of people who are at a higher risk of developing severe illness with COVID-19, including people who are aged
70 years or older (regardless of medical conditions) and people under 70 years of age with an underlying health condition,
including those given the flu vaccination each year on medical grounds. The COVID-19 response has raised a number of concerns
about the availability of both supportive and palliative care medicines across all care settings, and in particular those in care
homes and their own homes. Some of the concerns raised apply to all dying patients and not just those affected by COVID-19.
The following contingency plan outlines a range of actions, some of which have already been completed at a national level and
others which are for local consideration. The Scottish Palliative Care Pharmacy Association (SPCPA) have a key role in
development and implementation of these actions.
Priority area Solution Action by Timescale
1. Access to
palliative care
medicines –
primary and
secondary care
settings
Palliative Care Community Pharmacies and Community
Pharmacies
Each Health Board will have local arrangements for
the prescribing, supply and administration of
palliative care medicines.
Consider stock of Just in Case Box (JICB) medicines
Add stock of alternative palliative care medicines as
per national guidance.
Consider palliative care medicine stock levels in
community pharmacies that supply to care homes.
Local arrangements by
SPCPA members/each Health
Board/primary and
secondary care teams
As soon as
possible
(ASAP)

Palliative Care Toolkit, version 2.2
10
Acute services
Consider stock of palliative care medicines as
required.
List of medicines on the COVID-19 end of life care
and alternative palliative care medicines emailed to
stores/distribution.
GP bags
Ask GPs to consider the stock of JICB medicines in
the GP bag.
Out of Hours (OOH) services
Consider stock in in OOH centres.
Hospice
Consider stock of essential palliative care
medicines. Consider strengthening local prescribing.
Consider arrangements in the community, including
the use of non-medical and HBP prescriptions.
Consider the use of a ‘Hospice palliative care bag’
for Hospice medical staff to administer to
community patients.
Any additional holding sites for palliative care
medicines needed e.g. COVID-19 Assessment Centres
Consider stock holdings.
2. COVID-19
education and
training
required
Two national COVID-19 palliative care guidelines ‘End
of life care guidance in COVID-19 patients’ and
‘Alternatives to regular medication normally given via
a syringe pump when this is not available’ have been
published.
SPCPA Complete

Palliative Care Toolkit, version 2.2
11
Guidelines available at
https://www.palliativecareguidelines.scot.nhs.uk.
Palliative care training resources available on Turas.
NHS Education for Scotland (NES) have circulated
palliative care training available with the 2 national
guidelines.
NES Complete
Training delivered locally. Local arrangement ASAP
3. Shortage of
essential
palliative care
medicines
Alternative palliative care medicine guideline written.
Ensure stock of these medicines.
Local arrangement ASAP
SPCPA, working with National Procurement (NP), will
continue to provide information on medicines
shortages and recommend alternatives.
SPCPA/NP/ current board
approach
Ongoing
List of medicines included in both national palliative
care guidelines emailed to NP.
SPCPA Complete
Consideration is being given at a UK level to the
repurposing of medicines in care homes and hospices
NHS England and the
Devolved Administrations
Ongoing
Consider approaches to reducing waste.
Some health boards reducing quantity of JICB
medicines prescribed (for example 5 amps rather
than 10).
Raise awareness of the potential shortages in all
settings to discourage over-ordering and minimise
waste of palliative care medicines
Local
arrangement/SPCPA/primary
care team
ASAP
Minimise waste of critical injectable medicines.
Guidance available from Specialist Pharmacy Services.
Local arrangement ASAP
4. COVID-19
ACP
COVID-19 Anticipatory Care Planning (ACP) being
developed in all areas.
Local arrangement ASAP

Palliative Care Toolkit, version 2.2
12
5. Discharging
COVID-19
palliative care
patients home
from
Emergency
Departments
(ED)
National approach agreed.
Three key oral medicines (morphine 10mg/5ml liquid,
lorazepam and paracetamol) to be given as TTOs to
alleviate symptoms until a JICB/syringe pump/district
nurse is available where appropriate.
Healthcare Improvement
Scotland (HIS)/ SPCPA/
National Acute Pharmacy
Group Scotland
Complete
6. JICB
prescription
charts
Ensure extra supply of JICB medicine charts. Local arrangement ASAP
Extra to be distributed to the Hospice, Acute/ED, care
homes and community settings.
7. Care homes There are several approaches that can be taken
including:
strengthening the primary care prescribing
pathway.
use of extended home remedies.
use of protocols under regulation 247 of the
Human Medicines Regulations 2012 to support
supply and administration of medicines.
prescribing of ‘just in case’ boxes in anticipation.
NHS GG & C has produced a COVID-19 Strategy for
Palliative Care Drug Provision in Care Homes with
associated protocols. Health Boards considering the
use of protocols should seek advice from CLO.
Local arrangements ASAP
8. Not enough
district nurses
Most Health Boards have their own ‘informal carers
administering s/c medicines’ policy.
Local arrangement Complete
Palliative Care Toolkit, version 2.2
13
to administer
subcutaneous
(s/c) medicines
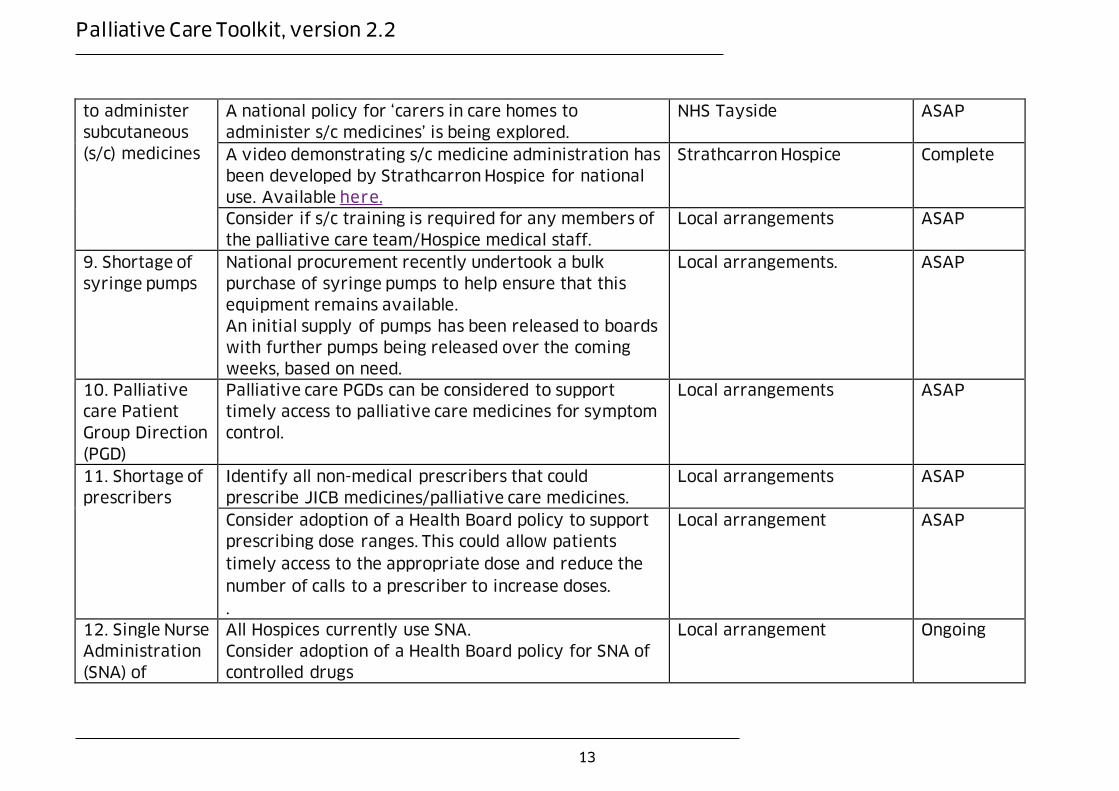
A national policy for ‘carers in care homes to
administer s/c medicines’ is being explored.
NHS Tayside ASAP
A video demonstrating s/c medicine administration has
been developed by Strathcarron Hospice for national
use. Available here.
Strathcarron Hospice Complete
Consider if s/c training is required for any members of
the palliative care team/Hospice medical staff.
Local arrangements ASAP
9. Shortage of
syringe pumps
National procurement recently undertook a bulk
purchase of syringe pumps to help ensure that this
equipment remains available.
An initial supply of pumps has been released to boards
with further pumps being released over the coming
weeks, based on need.
Local arrangements. ASAP
10. Palliative
care Patient
Group Direction
(PGD)
Palliative care PGDs can be considered to support
timely access to palliative care medicines for symptom
control.
Local arrangements ASAP
11. Shortage of
prescribers
Identify all non-medical prescribers that could
prescribe JICB medicines/palliative care medicines.
Local arrangements ASAP
Consider adoption of a Health Board policy to support
prescribing dose ranges. This could allow patients
timely access to the appropriate dose and reduce the
number of calls to a prescriber to increase doses.
.
Local arrangement ASAP
12. Single Nurse
Administration
(SNA) of
All Hospices currently use SNA.
Consider adoption of a Health Board policy for SNA of
controlled drugs
Local arrangement Ongoing

Palliative Care Toolkit, version 2.2
14
controlled
drugs
13. Reducing
risk/governance
SPCPA hold a risk register for the national work.
All SPCPA members encouraged to complete a risk
register on an individual basis, for personal use.
SPCPA Ongoing
14. SPCPA
members
support
Weekly zoom meetings scheduled for support.
Make contact with any SPCPA member if struggling.
If SPCPA member is off - Any pharmacist/technician
can be added to the SPCPA email distribution list or
WhatsApp group, if urgent palliative care advice is
needed.
SPCPA members Ongoing

Palliative Care Toolkit, version 2.2
15
Section two - Strengthening Primary Care
In Hours
Access to Medicines
There are risks associated with the global medicines supply chain of medicines,
both in the short and medium term. The Department for Health and Social Care
(DHSC) has asked NHS England (NHSE) to lead, on behalf of the UK, on sourcing as
much of the affected medicines as possible. National Procurement is working
closely with colleagues in NHSE to reinforce the supply chain for palliative care
medicines, as well as other supportive and critical care medicines.
Health Boards are asked to support the national approach to managing the supply
chain of palliative care medicines. Locally, there is also a need for measures which
discourage over-ordering of medicines and minimise waste. Health Boards should
consider the following steps:
• strengthening the current prescribing pathway by considering the
management of stock holdings of palliative care medicines across the
community pharmacy palliative care network, in GP practices, COVID-19
assessment centres, hospices and at community hospitals. For the COVID-
19 assessment centres, Health Boards may choose to mirror the
arrangements described under the Emergency Department section;
restricting the supply of ‘just in case’ boxes (JICBs) by improving
mechanisms to allow just in time dispensing of JICBs to preserve the stock
of critical medicines and reduce any unnecessary waste;
reducing, if appropriate, the quantity of anticipatory palliative care
medicines prescribed from ten to five ampoules or less;
minimising the waste of other critical injectable medicines based on the
guidance from Specialist Pharmacy Services.
supplying a ten day rather than a seven day supply of any subcutaneous
infusion medicines at discharge from secondary care to relieve the pressure
on the primary care teams; if appropriate.
strengthening arrangements for hospital pharmacy departments to support
community pharmacies in accessing critical medicines that are in short
supply; and
considering the use of:
o the prescribing of dose ranges in COVID-19 palliative care patients
taking account of the risks and benefits (Appendix A).
o the use of a single nurse administration policy (Appendix B).

Palliative Care Toolkit, version 2.2
16
o the SPOT clinical decision prescribing support tool (Appendix C);
o prescribing flow diagram for symptom management adapted from the
Scottish Palliative Care temporary guidelines for symptom
management for when a person is imminently dying from COVID-19
(Appendix D);
o pre-filled district nurse drug administration charts, MAR charts and
Communication Sheets (Appendices E, F and G);
o a JICB prescribing template (Appendix H).
Syringe drivers
Portable infusion pumps are normally used in palliative care to deliver a
continuous subcutaneous infusion of medication over 24 hours. Some acute areas
also use non-ambulatory pumps. Health Boards will want to ensure healthcare
professional know which device(s) are available for use and the current local
protocols for setting up and monitoring the syringe pump that is being used.
National Procurement has procured additional supplies of syringe pumps
however, Health Boards will also want to ensure that they have local strategies to
address circumstances when syringe pumps or associated consumables may not
be available.
Other measures
Alongside the legislative flexibilities described in the Executive Summary, there
are some legislative changes to the Misuse of Drugs Regulations 2001 that are
currently being considered at a UK level and which may become available during
the COVID-19 pandemic that will support the emergency supply of controlled
drugs from community pharmacies in certain circumstances. In addition, NHS
England is also considering the repurposing of previously dispensed but unused
medicines from Care Homes and Hospices and NHS Scotland will consider the
outcome of this work when it is available.
Out-of-hours
Health Boards should consider strengthening the current prescribing pathway by
considering the stock holdings in out-of-hours locations. This could include
increasing the availability of JICBs and/or the TTO packs of oral palliative care
medicines developed for the Emergency Department section. Community
pharmacists can accept a faxed or emailed prescription for Prescription Only
Medicines (POMs), but not controlled drugs from Schedules 1, 2 and 3, with the
exception of phenobarbitone or phenobarbital sodium for the treatment of
epilepsy, as long as it is followed up within 72 hours with a signed

Palliative Care Toolkit, version 2.2
17
prescription. Regulation 214 of the Human Medicines Regulations 2012 requires
that POMs are supplied in accordance with a prescription, however there is an
exception in regulation 224 which reflects the 72 hour requirement. This allows a
POM to be supplied where it has been “requested by a relevant prescriber who by
reason of an emergency is unable to provide a prescription immediately” and is
followed up with a prescription within 72 hours. An out-of-hours request for
either an acute or a repeat prescription would meet the definition under the
“urgent or emergency” criterion.

Palliative Care Toolkit, version 2.2
18
Section three - Accessing oral palliative care medicines from Emergency Departments during COVID-19

Palliative Care Toolkit, version 2.2
19
Accessing palliative care medicines from Emergency Departments during COVID-19 for palliative care patients that are still able to take medicines orally
Summary
Generally, a palliative care patient, who wishes to die at home, or in a homely
setting, is prescribed ‘just in case’ box (JICB) medicines as part of the normal
discharge process from hospital. In order to complement this, and in situations
where the patient is not dying imminently, a range of alternative palliative care
medicines for oral use have been agreed and ‘To Take Out’ (TTO) packs will be
provided by NHS Scotland Pharmaceutical Specials Service (NHS PSS). This will
support a quick discharge home and allow a carer or relative to administer oral
medicines to help alleviate symptoms. Supplying these medicines may also
provide a bridge to a JICB which can be arranged in the community, as and when
required. In addition, to support this approach there are three Patient Group
Direction (PGD) templates (appendices I-K) for local adoption to facilitate the
supply of the TTO medicines and a Patient Information Leaflet (PIL) (Appendix L)
for supply with the TTO packs.
The flow chart at the start of this section may provide a protocol in the ED setting
for Health Boards to adapt for their use.
Background
The Scottish Palliative Care guidelines is the key source of information on the
management of adults with life limiting illness and is available at:
https://www.palliativecareguidelines.scot.nhs.uk. To complement the standard
end of life care guidelines, two temporary guidelines have been developed for
symptom management in the context of:
End of life care guidance when a person is imminently dying from COVID-19
lung disease
This guideline describes the symptoms of COVID-19 and the palliative care
medicines prescribed to help alleviate symptoms, at end of life. It was developed
using COVID-19 information from Scotland, worldwide and a consensus of
palliative care professional expertise across Scotland.
Alternative to regular medication normally given via a syringe pump when this
is not available
This guideline describes alternative palliative care medicines that that could be
prescribed in a crisis where there is a shortage of essential palliative care
medicines, syringe pumps or district nurses in the community to administer

Palliative Care Toolkit, version 2.2
20
subcutaneous (s/c) medicines. These medicines could, if appropriate, be
administered by a relative or carer.
Generally, palliative care patients discharged home for end of life care, are
prescribed ‘Just in case box’ (JICB) medicines as recommended in the Scottish
Palliative Care guidelines.
For palliative care patients that are imminently dying, and wish to die at home,
JICB medicines should be prescribed via the normal discharge process. However,
if the patient is not imminently dying and the patient wishes to return to a
homely setting then a range of alternative palliative care medicines for oral use
have been agreed by the Scottish Palliative Care Pharmacy Association (SPCPA)
and COVID-19 Palliative Guidelines Development Group. This will allow a quick
discharge home and allow the carer/relative to administer oral medicines to help
alleviate symptoms. Supplying these medicines may also provide a bridge to JICB
which can be arranged in the community, when required.
To assist in the management of patients who require palliative care at this time an
option is described on the supply of alternative medicines to help control patient
symptoms. This option for the supply of medicines at Emergency Departments
(EDs) has been developed considering the following factors:
Palliative care patients approaching end of life and still able to take oral
medicines
Arrangements for JICB cannot be accessed in a timely way to support
discharge of the individual
The medicines to be provided are oral medicines providing ease of
administration to patients by their carers
The medicines aim to help alleviate symptoms at end of life
Supply of these medicines will give ease of access to symptom relief and
may provide a bridge to the availability of JICB, where appropriate
Treatments described in this document are for adults (aged 16 years and
older)
This option help to ensure palliative care medicines are available to help alleviate
symptoms for end of life care, allowing individuals to be given access if required,
without unnecessary delay to manage the predictable and distressing symptoms
that can occur.

Palliative Care Toolkit, version 2.2
21
Medicines
Medicine Symptom Dose Quantity to be
supplied
paracetamol
500mg
tablets/caplets
/ soluble
tablets
Pain/fever 500mg-1g (1 or 2)
tablets to be taken
every 4 to 6 hours.
Maximum 4g (8 tablets)
in 24 hours
32
tablets/caplets
Or
24 soluble
tablets
morphine
10mg/5mL
oral solution
Pain/breathlessn
ess/cough
2mg (1mL) to be taken
every 1 to 2 hours
when required
Maximum of 3 doses in
4 hours and 6 doses in
24 hours
1 x100mL
lorazepam
1mg tablets
(Genus, PVL or
Teva brands) –
tablets should
be scored and
blue in colour
Anxiety/distress
500 micrograms (half a
tablet) to be taken
sublingually every 4
hours when required.
Maximum of 4 doses in
24 hours.
10
In addition to this, where lorazepam is unavailable, then diazepam may be used as
an alternative. Dose information can be found in the Scottish Palliative Care
Guidelines: Alternative to regular medication normally given via a syringe pump
when this is not available.
Hyoscine hydrobromide patches may be supplied if secretions are problematic as
per the COVID-19 guidelines.
Where a prescriber chooses to give alternative medicines to the TTO packs
available then these should be prescribed and supplied as per normal discharge
medicines.
The medicines and dose have been reviewed and agreed by the SPCPA and
COVID-19 Palliative Guidelines Development Group.

Palliative Care Toolkit, version 2.2
22
Pre-packing of stock
NHS PSS are facilitating the availability of pre-packs for the three medicines
described above. Details for ordering of stock will be communicated as soon as
they are available.
In the interim, arrangements for the local over labelling and pack down may need
to be put in place for supply into the local EDs.
Health Boards will be aware of the following interim advice:
As discussed at the Scottish Unlicensed Medicines Advisory Board (SUMAB) given
the current position it would be prudent to allow relaxation of the rules around
the number of packs which can be over labelled/packing down provided there are
safe systems of work in place, please refer to the attached guidance document for
recommendations on the systems that should be in place.
SPQAG
Repackaging overlabelling guidance Version 2 May 2019 (2).pdf
Supply at Emergency Departments
Prescriptions for these medicines would be generated by prescribers in EDs using
local systems e.g. admission card/document, HEPMA protocols. In line with a
prescription the patient/carer will be provided with TTO supplies of the medicines
and the medicines supplied should be recorded following usual processes.
Information on the medicines prescribed should be included in any discharge
communication to GPs/primary care as per usual practice stating the medicines
that have been provided. The Key Information Summary (KIS) can be accessed in
EDs. A COVID-19 Anticipatory Care Plan is available as a word document which
can be completed or updated and sent to GP practices to be copied into KIS as
required. A digital service with electronic form is planned to be available shortly.
Further information on Anticipatory Care Planning can been found here.
A patient/carer information leaflet (Appendix L) providing information on the
medicines supplied should be provided to the patient/carer as well as advice on:
How to arrange further medicines if required
What to do if the condition changes or deteriorates further
What to do if admitted to hospital or another care setting
How to dispose of medicines that are no longer needed
Palliative Care Toolkit, version 2.2
23
Stock top up arrangements to EDs should follow local processes.
Patient follow up
Communication to allow timely patient follow up is essential. The usual
mechanisms for updating Primary Care on other medicines and/or clinical
decisions made at ED should be utilised to share information in relation to
medicines provided for palliative care. Local palliative care services should be
contacted for advice to ensure patient follow up.
Primary care teams should ensure patient follow up to provide re-assessment and
where necessary make arrangements for access to Just In Case Boxes via normal
routes as appropriate for the patient.
Accessing palliative care medicines from COVID-19 Assessment Centres when
access to the JICB arrangement is unavailable/inappropriate for adults
While this section focusses on supply arrangements from EDs, the same factors
can be taken into account when considering the options for the supply of
palliative care medicines from COVID-19 assessment centres.
The patient information leaflet relating to the medicines is also appropriate for
use within the assessment centre setting.
Mechanisms for the supply, prescribing, administration and stock top up of
palliative care medicines will need to be established in line with the local
processes to access other medicines for use at the centres. Likewise the standard
processes for communication of key patient information to the primary care
teams should be used to convey palliative care issues.
The PGD templates are included in Appendices I-K for paracetamol, morphine and
lorazepam for local adoption, as required, as a potential option to support patient
access in this setting.

Palliative Care Toolkit, version 2.2
24
Section four - Accessing palliative care medicines in care homes

Palliative Care Toolkit, version 2.2
25
Access to palliative care medicines for care home residents
during the COVID-19 pandemic
Summary
Health Boards may wish to consider the following approaches to strengthening
access to medicines in care home settings:
preparing anticipatory prescriptions for Just in Case Boxes (JICBs) for
residents which are only dispensed if needed for that individual
resident. These can be repeated every 28 days as necessary. This approach
will minimise the waste of specific medicines;
expanding the use of homely remedies to include a number of Pharmacy
Only (P) and General Sales List (GSL) medicines to provide symptomatic
relief;
using the To Take Out (TTO) packs of medicines that are being provided to
Emergency Departments (EDs) as a bridge to alleviate symptoms; and
making use of the supply and administration of certain Prescription Only
Medicine (POM) medicines under a specific protocol which has been
approved by a Health Board.
The flow chart at the start of this section provides a protocol for care home
settings for Health Boards to adapt for their use.
Introduction
The COVID-19 pandemic raises challenges for care home staff, their families and
the staff looking after them. Care home residents are particularly vulnerable to
COVID-19 as they are increasingly frail and elderly with complex co-morbidities.
The symptoms of COVID-19 can be aggressive and escalate quickly, therefore care
home residents will need quick access to palliative care medicines to help
alleviate symptoms and reduce suffering.
It is predicted that with the escalation of COVID-19, the healthcare system will be
under immense pressure which may result in a reduced number of carers and
healthcare professionals. In addition to this, it is anticipated that there may be a
shortage of essential palliative care medicines and syringe pumps. This guideline
describes how care home residents can access palliative care medicines
throughout the COVID-19 pandemic.

Palliative Care Toolkit, version 2.2
26
Care Homes
There are over 35,000 residents in over 1,000 care homes in Scotland. There are
many different types of care home (care of the elderly, children, nursing,
residential etc.) that are managed by the NHS, local authority, voluntary or private
organisations. All these residents access care through the carers, their GP,
pharmacists, nursing staff (either on site nursing or district nurses) and other
healthcare professionals. Appendix M provides a visual that captures the wide
range of activities that should be considered as part of a package of care to care
home residents in the context of COVID-19. There is also a video explaining the
visual available here.
The recent guidance from the British Geriatrics Society ‘Managing the COVID-19
pandemic in care homes’ states that ‘care homes should work with GPs and local
pharmacists to ensure that they have a stock of anticipatory medications and the
community prescription chart, to enable, at short notice, palliative care for
residents’.
Current process for care home residents accessing palliative medicines
Currently, GPs prescribe JICB medicines (morphine, midazolam, hyoscine
butylbromide and levomepromazine ampoules), on an individual patient basis, to
help alleviate symptoms, at the end of life. These medicines are prescribed in
advance of symptoms, so they are available when required. With the escalation
of COVID-19, this approach has the potential to result in a very large volume of
JICB medicines being prescribed for care home residents. While it is essential that
care home residents have access to this medication, it is likely that many of these
individually prescribed medicines will not be used and this will result in the
potential waste of medication that may be in short supply.
JICB medicines are administered subcutaneously, therefore are currently
administered by nursing staff.
Anticipated problems accessing palliative care medicines during COVID-19
With the expected strain on the healthcare system and carers, there may be
delays in care home residents accessing palliative care medicines due to:
shortage of carers looking after care home residents;
shortage in prescribers to prescribe palliative care medicines;
medicine supply issues with essential palliative care medicines;

Palliative Care Toolkit, version 2.2
27
delays in dispensing medicines in Community Pharmacy due to staff
shortages (potential for pharmacy closures), increased workload and
medicine supply issues; and
limited nursing staff available to review residents and administer
subcutaneous medicines.
Supporting access to palliative care medicines for care home residents
Ways to support care home residents accessing palliative care medicines include:
Shortage of GPs/prescribers to prescribe the palliative care medicines.
In the event of limited access to GPs to prescribe palliative care medicines, ways
to support this are:
allowing dose ranges to be prescribed, to allow effective titration of
palliative care medicines, to reduce suffering, for resident’s experiencing
severe COVID-19 symptoms. This is described in detail in Appendix A;
identifying other non-medical prescribers (for example advanced nurse
practitioners (ANP’s), independent pharmacist prescribers etc.) who could
prescribe these medicines; and
distribution of JICB kardexes to all care homes so they are available for
immediate access, if required.
Access to palliative care medicines
Care home residents can access palliative care medicines via the:
Homely remedy policy
Many care homes have a homely remedy medicines policy. This allows care
homes to stock medicines for minor ailments such as paracetamol for pain, senna
for constipation and simple linctus for cough. Such homely remedy policies can be
updated to include other General Sales List (GSL) and Pharmacy (P) medicines that
may provide relief of the COVID-19 symptoms. For example:
P or GSL palliative care medicine COVID-19 symptom
Paracetamol tablets/liquid/suppositories Pain, fever
Codeine linctus 15mg/5mL liquid Cough
Prochlorperazine 3mg buccal tablets Nausea and vomiting
Hyoscine hydrobromide 300mcg tablet Respiratory secretions
Hyoscine 1.5mg patches Respiratory secretions
All these medicines are listed in the temporary palliative care guideline
‘Alternatives to regular medication normally given via a syringe pump when this

Palliative Care Toolkit, version 2.2
28
is not available’ and would enable a carer to administer these medicines, to help
alleviate symptoms and reducing suffering, until the resident could be reviewed
by a health care professional.
Community Pharmacy
Generally, care home residents access medicines through community pharmacy.
They are not currently eligible for the Minor Ailment Service. Care home
residents can obtain alternative palliative care medicines, via a GP10 prescription,
which a carer can then administer. For example, a patient in pain, who is opioid
naïve, can be prescribed morphine sulfate oral solution and/or a buprenorphine
patch, rather than a morphine syringe pump, which needs to be administered by a
nurse on a daily basis. This empowers the carer to administer medicines to help
relieve symptoms and allows the nursing team to be able to prioritise patients
and focus on the residents who remain symptomatic. Details of alternative
medicines that can be prescribed are described in the national palliative care
guideline ‘Alternatives to regular medication normally given via a syringe pump
when this is not available’, available at
https://www.palliativecareguidelines.scot.nhs.uk/. These are also listed in
Appendix O.
Anticipatory prescribing JICB medicines
All JICB medicines are prescribed on an individual patient basis. This may result in
a significant volume JICB medicines being prescribed and subsequently wasted if
they are not used. This is a particular concern in the context of potential supply
challenges for palliative care medicines. Where COVID-19 is confirmed in a care
home, JICB medicines could be prescribed on a GP10 prescription but not
dispensed in community pharmacy until they are required – a form of delayed
prescribing. This could save on wastage, however, it will take some GP time to
prescribe all the individual JICB medicines. Some Health Boards are also reducing
the number of ampoules prescribed in a JICB to reduce wastage.
All palliative care medicines
A full list of all the palliative care medicines available, including how to access
them and who they can be administered by, is listed in Appendix N which outlines
an approach based on a Model of Care developed by NHSGG&C. This provides
clarity on which palliative care medicines can be administered by a carer. This
empowers carers to help relieve symptoms and allows nursing staff to prioritise
patients, who remain symptomatic.

Palliative Care Toolkit, version 2.2
29
Advice on managing symptoms in palliative care is available on the Scottish
Palliative Care guidelines website.
Two temporary palliative guidelines on caring for palliative care patients dying of
COVID-19, ‘End of life care when a person is imminently dying from COVID-19
lung disease’ and ‘Alternatives to regular medication normally given via a syringe
pump when this is not available’ are available at
https://www.palliativecareguidelines.scot.nhs.uk/.
Care Homes holding stocks of POMs
In the event of a pandemic, there are options to allow the supply of POMs to
patients within the existing legislative provisions in the Human Medicines
Regulations 2012. As described in the Executive Summary, the 2012 Regulations
set out various exemptions to regulation 214 which specifies that a person may
not supply a POM except in accordance with a prescription given by an
appropriate practitioner. For example, regulation 247 allows the supply of a POM
without a prescription in a pandemic situation, provided certain conditions are
met. These conditions include that the supply must be made whilst a disease is, or
in anticipation of a disease being imminently pandemic and a serious risk, or
potentially serious risk to human health. It must also be made under a disease
specific protocol which must be approved by UK Ministers or an NHS body. “NHS
body” includes territorial Health Boards in Scotland. The protocol must specify the
symptoms of and the treatment of that disease. Any Health Board considering
putting a protocol in place which relates to the supply of medicines in care homes
will want to satisfy themselves that any protocol complies with regulation 247 of
the Human Medicine Regulation 2012 as well as the legislation which sets out the
requirements for controlled drugs, for example the Misuse of Drugs Regulations
2001. The Central Legal Office (CLO) will be able to provide Health Boards with
advice on this.
This type of approach would allow a care home to stock medicines such as:
Medicine Symptom of COVID-19
Hyoscine Butylbromide 20mg/mL amps Respiratory secretions
Levomepromazine 25mg/mL amps Agitation/delirium
Haloperidol 5mg/mL amps – second line Agitation/delirium
This supports timely access to palliative care medicines, to help alleviate
symptoms, for end of life care. NHS Greater Glasgow & Clyde (GGC) have adopted
this approach and their COVID 19 Palliative Care Medicines Policy for Care Homes
can be found here, This provides an example of one Health Board’s approach

Palliative Care Toolkit, version 2.2
30
using the pandemic exemption in Regulation 247 of the Human Medicines
Regulations 2012.
In line with the NHSGGC protocol, relevant Prescription Only Medicines are pre-
authorised by a prescriber for individual patients. In the event of symptoms
arising, a nurse is required to discuss the patient’s symptoms and confirm their
care plan with a prescriber before the medicine is administered for 48 hours.
Thereafter a regular prescription is required to support ongoing treatment.
Any Health Board using the pandemic flexibilities pandemic to allow the supply of
POMs to patients within the existing legislative provisions in the Human
Medicines Regulations 2012 will need to ensure that they have an exit strategy
from those arrangements when the pandemic status is withdrawn.
Shortage of essential palliative care medicines
Palliative care medicine shortage advice
It is anticipated that there will be shortages of essential palliative care medicines,
due to the increase in demand. Currently, community pharmacists and local Health
Board arrangements provide advice on medicine supply issues and palliative care
pharmacists recommend alternative medicines, for symptom control.
Re-using care home residents JICB medicines
If a resident’s JICB medicines are not used and they die, it is current practice to
destroy these medicines. This may result in the destruction of many JICB
medicines that have been dispensed for individual residents. There is work being
considered at a UK level on the repurposing of certain medicines from care homes
and hospices and NHS Scotland will consider this work and its practical application
when it becomes available.
Conclusion
This section describes different options to support timely access to palliative care
medicines for care home residents, despite the potential challenges presented by
COVID-19. Appendix O provides a summary of all issues to be considered and
potential approaches.
Palliative Care Toolkit, version 2.2
31
Appendix A: Prescribing dose ranges for COVID-19 palliative care patients during the pandemic
Situation
The symptoms of COVID-19 can be aggressive and escalate quickly, therefore
palliative care patients need quick access to palliative care medicines, to help
alleviate symptoms and reduce suffering. It is predicted that with the escalation
of COVID-19, the healthcare system will be put under immense pressure which
may result in a reduced number of healthcare professionals. This appendix
outlines an approach to the prescribing of dose ranges in COVID-19 palliative care
patients and outlines the risks and benefits of such an approach.
Background
The standard palliative care medicines, ‘Just in case box’ (JICB) medicines
(morphine, midazolam, hyoscine butylbromide and levomepromazine amps), as
recommended in the Scottish Palliative Care guidelines, are prescribed to help
alleviate symptoms at the end of life. These medicines are prescribed in advance
of expected symptoms developing and the doses are correspondingly low.
A national palliative care guideline, ‘End of life care guidance when a person is
imminently dying from COVID-19 lung disease’ has been developed, using COVID-
19 information from Scotland, worldwide and a consensus of palliative care
professional expertise across Scotland. This guideline describes higher doses of
standard palliative care medicines that may be required to control the COVID-19
symptoms, experienced at the very end of life.
Therefore, a palliative care patient suffering from COVID-19 symptoms, may
require higher doses than those prescribed on a standard JICB Kardex, to control
their symptoms. Fixed dose prescribing would therefore result in a call to the
prescriber to authorise an increase in dose. This takes time and delays the patient
receiving the most appropriate dose, to control symptoms.
Assessment
The legal and professional guidance on dose ranges is set out as follows, with the
associated advantages and disadvantages.
British National Formulary
Prescribing dose ranges is legally acceptable, and this is detailed in the British
National Formulary (BNF) and the palliative care formulary. However, the
guidance is very clear that dose ranges are only legally acceptable when part of
an instruction to administer. In the prescription writing requirements in the BNF,
it states that ‘Use of decimal points is acceptable to express a range’.

Palliative Care Toolkit, version 2.2
32
Misuse of Drugs Regulations 2001
Under the Misuse of Drugs Regulations 2001, Regulation 7 describes the
administration of drugs in Schedules 2, 3, 4 and 5
(1) Any person may administer to another any drug specified in Schedule 5.
(2) A doctor or dentist may administer to a patient any drug specified in Schedule
2, 3 or 4.
(3) Any person other than a doctor or dentist may administer to a patient, in
accordance with the directions of a doctor or dentist, any drug specified in
Schedule 2, 3 or 4.
Home Office
Previous correspondence from the Home Office in 2011* stated:
‘Where an instruction to administer is given the prescriber has flexibility
to instruct a range of doses to be used’.
‘Where a dose range is prescribed it should be suitable for the patient's
condition and previous opioid use and should not be sufficiently wide to
allow overdose to occur’.
Nursing and Midwifery Council (NMC) standards
Previously Standard 13 from the NM standards for Medicines Management stated,
"Where medication has been prescribed within a range of dosages it is acceptable
for registrants to titrate dosages according to patient response and symptom
control, and to administer within the prescribed range”.
Whilst these standards have been withdrawn, they contain useful detailed
guidance which is often referred back to support the current professional
overview guidance.
Royal College of Nursing (RCN) and Royal Pharmaceutical Society (RPS)
Dose ranging is not specifically mentioned in the RCN/RPS Professional guidance
on the administration of medicines in healthcare settings (2019).
Palliative Care Formulary
Prescribing a range of permitted dose ranges allows nurses to increase the
amount given on their own initiative. In practice, nurses tend to start with the
lower dose, but increase to the top of the range if necessary.
Advantages of prescribing dose ranges for COVID-19 palliative care patients
The potential advantages of prescribing dose ranges are that they:
enable a nurse to use their professional judgement to administer the most
appropriate dose, to alleviate symptoms and reduce suffering;
support timely access to the patient receiving the most appropriate dose to
alleviate symptoms, especially as symptoms can escalate quickly;
Palliative Care Toolkit, version 2.2
33
reassure the family that if symptoms don’t settle, then further medication
doses can be administered safely;
may be beneficial if there is a shortage of syringe pumps and symptoms
need to be controlled with subcutaneous ‘as required’ medicines; and
reduce the number of calls to the GP/OOH/prescriber to increase doses.
Disadvantages of prescribing dose ranges for COVID-19 palliative care patients
The potential disadvantages of prescribing dose ranges are that an inexperienced
nurse administering an inappropriately high dose for a patient resulting in patient
harm.
Ways to reduce the risk of patient harm
Only allow a small range (for example 2mg to 5mg of morphine, midazolam)
for prescribing dose ranges.
Write both doses in full (for example 2mg to 5mg rather than 2-5mg) to
minimise the risk of misreading (2-5mg could be misread as 25mg).
If the nurse hasn’t any knowledge of the previous response to the drug, the
lowest dose within the range should be used.
Where knowledge of previous response suggests that an increase in dose
may be required the nurse would need to judge the risks of potential
adverse effects against the potential to gain symptom relief.
Where prior response is unknown or where new clinical factors require
consideration, starting at higher doses within the range prescribed would
normally be implemented only after consultation with an experienced
colleague, prescriber or member of the specialist palliative care team.
There will be maximum number of doses permitted in a specific time frame,
following which a prescriber needs to be contacted.
If the highest dose within the range has been administered, and the patient
is still suffering from symptoms a doctor/experienced nurse needs to be
contacted
Safeguarding approaches
The medicine will already be prescribed by a prescriber that has clinically
assessed the patient and there are no contraindications.
Prescribing dose ranges is only suitable for medicines for which the
prescriber considers there is a clinical indication.
Only a small dose range (for example 2mg to 5mg) is allowed.
Information will be provided by the prescriber detailing when a higher dose
(within the dose range) can be given
A maximum number of doses per 24 hours must be stated.
Good communication between the prescriber and nurse is essential.
It must be clear to the nurse when medical advice must be obtained (for
example, when a second dose, from top of the range, has been given).

Palliative Care Toolkit, version 2.2
34
Recommendation
Some health boards, particularly in remote and rural areas, for example NHS
Highland, have supported the prescribing of dose ranges since 2011. This
approach can be used nationally to reduce the pressure on prescribers, allow
nursing staff to use their professional judgement to administer the most
appropriate dose to care for the patient and most importantly, support the patient
to receive timely access to medicines, to reduce suffering.
Any Health Board wanting to support the prescribing of dose ranges, will want to
consider gaining agreement for implementation in line with local Health Board
clinical governance processes and local guidance will need to be widely
communicated to all members of the healthcare professionals involved (doctors,
nurses and pharmacists) to highlight the change in practice.
*Correspondence from Jane Smith. Principal Pharmacist Medicines Management. Home Office 2011.

Palliative Care Toolkit, version 2.2
35
Appendix B: Single Nurse Administration (SNA) of Controlled Drugs
Situation
With impending widespread staff shortages, the current process of dual nurse
(person) administration and checking of some medicines has the potential to
impact on service delivery, symptom management and patient care.
Background
A brief review of policies from different settings has identified that there is mixed
practice both across and within settings within respect to single and dual nurse
(person) administration of CDs.
Hospice setting
SNA is undertaken by nurses in majority of hospices in Scotland. Those hospices
which have not adopted SNA are NHS facilities following local hospital/acute
policies. Rigorous nurse training involves self-assessment as well as assessment
and supervision by other healthcare professionals. The time required for training
varies between hospices but it has been reported that for some staff, the training
can be undertaken in a single shift. The time required is dependent on the level of
experience of individual nurses.
Acute setting
In the acute setting it would appear that the administration of CDs (including
recording in CD Register) is routinely undertaken by two nurses. Only
exceptionally is SNA current practice where a risk assessment has been
undertaken. The administration of other oral medicines and IV medicines may be
carried out by one nurse with necessary calculations being checked by an
additional healthcare professional where practicable.
It is noted that SNA of CDs by district nurses is standard practice in the
community setting. However administration is undertaken in line with patient
specific directives using patient’s own stock from a community pharmacy.
Prison setting
Nurses, healthcare assistants or pharmacy assistants are employed to administer
the majority of medicines which are supplied as individually named patient items.
However, 500 items per week are supplied to prisons as stock items, including
methadone, opioid substitution therapy and diazepam and dihydrocodeine for
safe management of withdrawal. Two people, one of whom is always a nurse, are
required to sign CDs out of the CD register and these two people then undertake
administration of the CDs (generally methadone and buprenorphine).

Palliative Care Toolkit, version 2.2
36
Assessment
Legislative position
Royal Pharmaceutical Society/Royal College of Nursing Guidance
The current RPS/RCN Professional Guidance on the Administration of Medicines in
Healthcare Settings, aimed at registered healthcare professionals administering
medicines, advises that ‘the organisation’s administration procedure is followed’.
The Guidance states ‘Risk assessments must be undertaken to inform
organisational policies/procedures for second signatories, witness requirements,
and delegating’ and also recommends that ‘any calculations are double checked
where practicable by a second person and uncertainties raised with the prescriber
or pharmacy professional’.
CEL 2008 (07)
CEL2008_07 is the main guiding legislation in Scotland and it provides a guide to
good practice in secondary care on the safer management of controlled drugs. It
requires healthcare practitioners to adhere to relevant local policies. It advises
that the healthcare organisation may wish to stipulate that receipt of CDs and
updating of the register should be witnessed by a second competent person.
Additionally the administration of CDs within secondary care should normally be
done via two-person administration process. Any departure from the double
check process should be considered exceptional and carry with it a specific risk
assessment to support this practice
In summary, it would appear that there is no legislative barrier to SNA of CDs if
local policies can be updated to support the change. A risk assessment is required
for individual settings before this practice could be adopted to minimise the risk
of error and/or criminal activities which could have significant consequences for
patients, staff and the healthcare organisation.
Minimising any associated risk
Factors to be considered before adoption of SNA for CDs are set out in the
following table.
Factor Comment
Legislative requirements
for
records in CD register
safe custody
Only need to record schedule 2 CDs (recording of
Schedule 3 CDs is custom and practice in some
settings)
The nurse administering the CD must record the
activity in the CD register
Balance checks can be undertaken by a single
person (not necessarily a nurse)
Only schedule 2 CDs and a limited range of
schedule 3 CDs require safe custody

Palliative Care Toolkit, version 2.2
37
Risk of misuse/theft
Fear of censure in the
event CDs go missing
CD register balance checks required for only for
schedule 2 CDs with the frequency depending on
risk assessment e.g. frequency of use and
previous CD related incidents
Regulatory bodies have advised that they are
adopting a supportive approach during the
current crisis
Clinical use An incremental approach with initial adoption of
SNA for CD doses/formulations that nurses are
experienced using in their specialist clinical
practice setting would be preferred. However it is
noted that higher initial doses of CDs are required
for the control of COVID-19 symptoms.
There may be specific circumstances 2 individuals
should still be involved and this need considered
as part of the appropriate risk assessment
Competence of nursing
staff
Training packages are available to support nurses
to increase competence and confidence whilst
ensuring that they remain within their scope of
practice
The Strathcarron Hospice has given permission
for their package to be used by all hospices.
The timing to introduce such a change in policy
and procedures is challenging in view of the
number of new and returning nurses moving into
clinical practice. However this change in practice
is only appropriate for those nurses that are
confident and competent to undertake SNA of
CDs.
Proposals for consideration
With reference to these factors it is proposed that SNA may be considered for a
limited time period subject to review as follows:
Hospice setting
In view of the current high level of experience of handling CDs, it is proposed that
further steps should be taken to explore rolling out SNA of CDs to the NHS
hospices. Use of established hospice training packs could empower those nurses
that can demonstrate their competence and have the confidence to work in this
way. This proposed change is supported by information from local hospice audits
which suggest no increase in error rate, post introduction of SNA procedures.
Acute settings
The resource required to supervise and assess the nurses in training is noted, but
training packages in hospices are readily available and could be shared and
adapted/adopted for use in acute settings.
Palliative Care Toolkit, version 2.2
38
Nurses currently working in high risk clinical areas such as critical care, high
dependency and coronary care units already operate with a degree of autonomy
and level of expertise in the administration of high risk medicines and may be
best placed to undertake SNA of CDs in the first instance. It is proposed that
further steps should be taken to explore the adoption of SNA of CDs in these
areas. Thereafter boards could consider roll out to other clinical areas e.g.
respiratory, A&E etc. Any potential resistance from nurses, managers and
pharmacy to adopt this change will need to be overcome to support
implementation.
Prison settings
The resource required to supervise and assess the nurses in training is noted but
it is proposed that SNA of CDs should be explored in the prison setting.
Recommendation
There are a range of circumstances where the use of singe nurse administration of
CDs may be possible in the hospice, acute and prison settings to alleviate
pressures.
Any Health Board wanting to support single nurse administration prescribing will
want to gain consensus agreement for implementation in line with local Health
Board clinical governance processes and local guidance will need to be widely
communicated to all members of the healthcare professionals involved (doctors,
nurses and pharmacists) to highlight the change in practice.

Palliative Care Toolkit, version 2.2
39
Appendix C: the SPOT clinical decision prescribing support tool
Situation
The COVID19 pandemic is creating an increased demand for opioids and leading to
a shortage of first-line opioids that are familiar to prescribers. This creates
uncertainty around opioid prescribing and conversion between one opioid or
route of administration and another to ensure equal potency and avoid the harms
associated with over- or under-dosing.
The solution is the Safer Prescription of Opioids Tool (SPOT). SPOT is a novel
Clinician Decision Support Digital Health CE-marked medical device. In a real
world, cross setting and multi-professional study1 across NHS Tayside, it is proven
to significantly improve the confidence of opioid prescribing in users and
adherence to best practice guidelines. SPOT has undergone large-scale testing in
an NHS Board and is now ready for national level deployment to support the
COVID pandemic.
Background
SPOT is designed to reduce unwarranted variation and primary and secondary
harms when prescribing opioids whilst supporting warranted variation of choice
to align to individual situations, values and side effect profiles. It supports
prescribers when their usual first line choice of opioid is not available or
inappropriate for the clinical situation.
SPOT was created and trialed in NHS Tayside over a four year period across
primary, secondary and tertiary care by a multi-professional interdisciplinary
team including independent prescribers, pharmacists, a clinical pharmacologist
and director of research, the RCGP Executive Officer (Quality Improvement), the
Palliative Medicine Special advisor to the Scottish Government Health & Social
care Directorate and the Chief Medical Officer and National Clinical Lead for
Palliative and End of Life Care for Health Improvement Scotland. Since July 2019,
SPOT has been used in day-to-day practice in NHS Borders.
1 https://doi.org/10.3390/ijerph16111926

Palliative Care Toolkit, version 2.2
40
SPOT enables clinicians to independently and remotely double-check their
equianalgesic opioid conversions safely, quickly and conveniently at the patient’s
bedside, whilst providing access to nationally adopted best-practice Scottish
Palliative Care Guidelines. This helps to reduce and mitigate risk, preventing
conversion errors leading to harm and increasing spread of opioid options for
each individual to have personalised analgesia approaches implemented.
Following an Innovate UK funded development programme, SPOT is ready for
deployment at scale. It is available in web-app, iOS and Android hybrid-app
format. SPOT has been assessed and meets the standards of the NHS Scotland
Quality Assurance Framework for Medical Device Apps, and is linked on
https://rightdecision.scot.nhs.uk. The Scottish Palliative Care Guideline Group and
Chair of this group have reviewed and endorsed SPOT.
At present there is currently no clinically validated opioid prescribing clinician
decision support tool available internationally.
Assessment
SPOT provides the following functionality:
• SPOT uses an algorithm based on the equianalgesic tables from best practice
guidelines.
• Conversion of equianalgesic doses of opioids, allowing simple conversion from
one opioid and route of administration to another. Independently validating
drug conversions, at the patient’s bedside.
• All drug preparations in the pharmacy are listed bespoke to each drug, aiding
drug selection.
• Links to gold-standard reference to inform prescribers.
• All conversions are auditable centrally, providing a clinical governance and
audit trail.
• SPOT promotes consistency of opioid conversion throughout whole system
through supporting individual clinical decisions, widening opioid repertoire for
individual clinicians and educates in real-time through both these
mechanisms.
The intended users are junior doctors, any trainee doctor/consultant prescribing
opiates in a palliative patient, pharmacists supporting safe prescribing in settings
with palliative patients, independent prescribers, GPs and GP trainees both in
hours and out of hours.

Palliative Care Toolkit, version 2.2
41
Furthermore, research into SPOT has identified that not only is SPOT proven to
improve prescriber confidence when performing opioid conversion, but it has the
ability to improve prescriber performance.
Using machine learning, we have identified that when adopted at scale SPOT can
be used to simultaneously harness information that could help the development
of guidelines for pain management and also monitor prescriber performance to
ensure safe and effective treatment of pain. Not only this, but SPOT can identify
the magnitude of an error, whether that is likely to cause harm, and identify the
calculations that colleagues find most taxing.
The aim of SPOT is to support prescribers in using first, second and third line
opioids throughout the COVID19 pandemic and beyond into normal business-as-
usual practice.
Recommendation
SPOT is the only CE-Marked, clinically-validated equianalgesic opioid converter in
clinical practice, assessed against the NHS Scotland Quality Assurance Framework
for Medical Device Apps, based upon the Scottish Palliative Guidelines, proven to
improve adherence to guidelines and confidence in prescribers which is ready for
national-level adoption and is currently rolled out in an NHS Board. It is designed
to support prescribers during shortages associated with the COVD19 pandemic
and prescribers using unfamiliar opioids. It comes with the mandated software
support, updates, indemnity and ongoing clinical appraisal to continue to fulfil this
the National Assurance Framework.
Author of Report: Dr Deans Buchanan, Clinical Lead and. Consultant Palliative
Medicine, Palliative Medicine Special advisor to the Scottish Government Health &
Social care Directorate and the Chief Medical Officer and Dr Scott Jamieson,
Prescribing Lead, Angus HSCP
Updated 13/4/20 - Dr Roger Flint GP Registrar
Date: 13/04/20
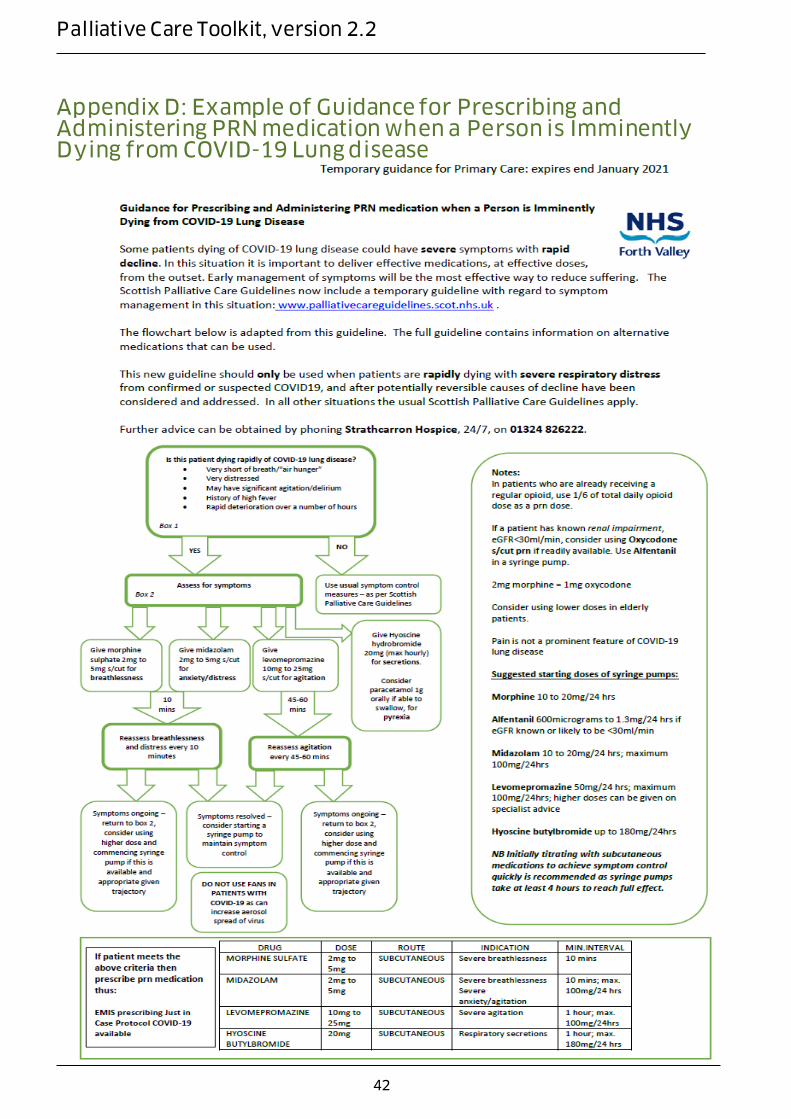
Palliative Care Toolkit, version 2.2
42
Appendix D: Example of Guidance for Prescribing and Administering PRN medication when a Person is Imminently Dying from COVID-19 Lung disease

Palliative Care Toolkit, version 2.2
43
Appendix E: SAMPLE Drug Administration Instruction Chart (courtesy of NHS Tayside)
«PATIENT_Title»
«PATIENT_Forename1»
«PATIENT_Surname»
CHI: «PATIENT_CHI_Number»
«PATIENT_House»«PATIENT_Road»
«PATIENT_Town»
«PATIENT_Postcode»
DRUG ADMINSTRATION INSTRUCTION CHART (ADAPTED FOR ANTICIPATORY MEDICATION)
Sheet No : ______________
Date/Time Name of Drug Dose to be Administered
and Frequency
Method of
Administration
Prescribed By
(signature)
Date
Stopped
Stopped by
(Signature)
Date/Time Name of As Required
Drug
Dose to be Administered
and Frequency
Method of
Administration
Prescribed By
(Signature)
Date
Stopped
Stopped By
(Signature)
Morphine Sulfate
Injection 10mg/1ml
2 mg hourly as needed for
pain or breathlessness SC injection
Midazolam Injection
10mg/2ml
2 mg hourly as needed for SC injection

Palliative Care Toolkit, version 2.2
44
Patient Name: ………………………………………………………… CHI No: ………………………………………………….
«PATIENT_Title»
«PATIENT_Forename1»
«PATIENT_Surname»
CHI: «PATIENT_CHI_Number»
«PATIENT_House»«PATIENT_Road
» «PATIENT_Town»
«PATIENT_Postcode»
DRUG ADMINISTRATION
INSTRUCTION CHART
Sheet No ……..
Date/Time Name of Drug Dose to be
Administered
and Frequency
Method of
Administration
Prescribed By
(signature)
Date
Stopped
Stopped by
(Signature)
anxiety/ distress/
myoclonus
Hyoscine
Butylbromide
Injection 20mg/1ml
20 mg hourly as needed
(max 120mg/24hrs) for
respiratory secretions
SC injection
Levomepromazine
25mg/1ml injection
*.........mgs
*............hourly as needed
for nausea
SC injection

Palliative Care Toolkit, version 2.2
45
Date/Time Name of As
Required Drug
Dose to be
Administered and
Frequency
Method of
Administration
Prescribed By
(Signature)
Date
Stopped
Stopped By
(Signature)
Morphine
10mg/ml
injection
2mg every hour as
required for pain or
breathlessness
SC injection
Midazolam
10mg/2ml
injection
2mg hourly as
required for
anxiety, distress or
myoclonus
SC injection
Hyoscine
butylbromide
20mg/ml
20mg hourly as
required for
excessive
respiratory
secretions up to a
maximum of
120mg in 24 hours
SC injection
Haloperidol 5mg
/ml
0.5ml injected sc
every 12 hours for
nausea/ vomiting
as required
SC injection

Palliative Care Toolkit, version 2.2
46
Appendix F: SAMPLE Medication Administration Record Pharmacy Check
Patient/Client Name
CHI
Address
GP Practice Start Date End Date
Medication Name,
Strength, Form
Time Dose
C/F: Qty: Qty Rec: By: Date: Qty Ret: Date: By:
C/F: Qty: Qty Rec: By: Date: Qty Ret: Date: By:

Palliative Care Toolkit, version 2.2
47
C/F: Qty: Qty Rec: By: Date: Qty Ret: Date: By:
C/F: Qty: Qty Rec: By: Date: Qty Ret: Date: By:
C/F: Qty: Qty Rec: By: Date: Qty Ret: Date: By:
C/F: Qty: Qty Rec: By: Date: Qty Ret: Date: By:
Please refer to their dispensed label for full medication instructions
Codes to be used if medication is not taken R: refused O: See Overleaf please see carer medication notes for detail
1 of X
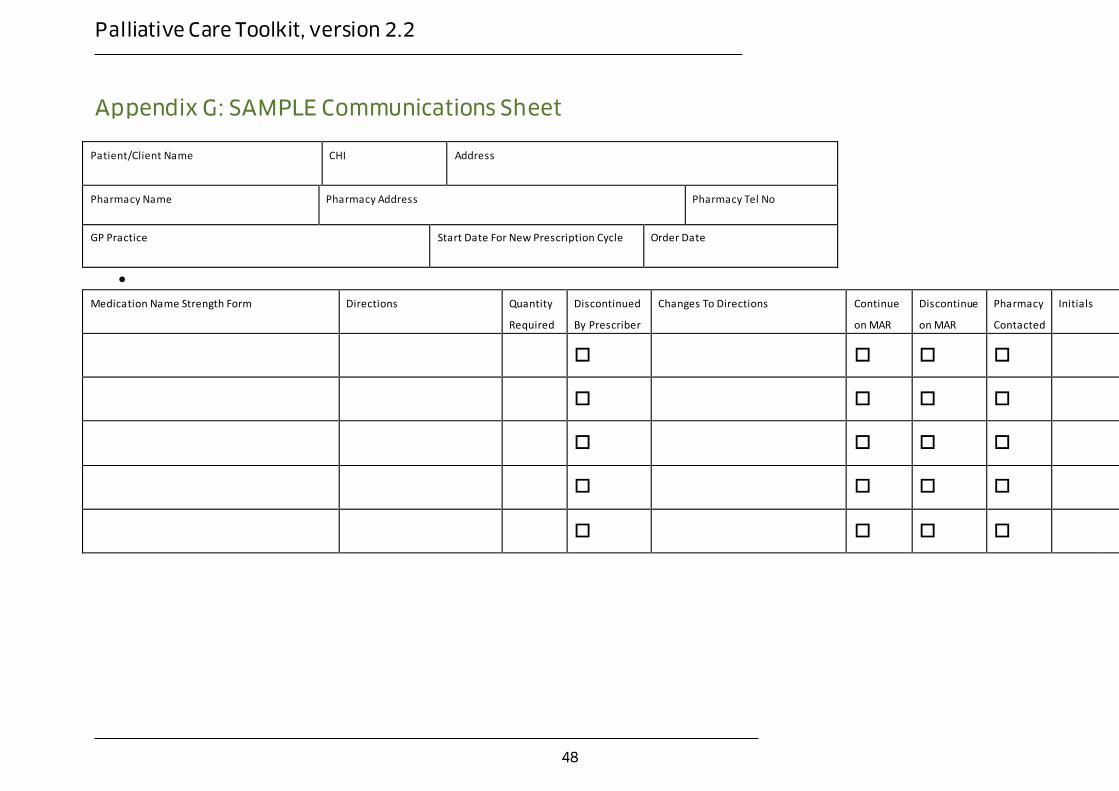
Palliative Care Toolkit, version 2.2
48
Appendix G: SAMPLE Communications Sheet
Patient/Client Name
CHI
Address
Pharmacy Name Pharmacy Address Pharmacy Tel No
GP Practice
Start Date For New Prescription Cycle
Order Date
Medication Name Strength Form Directions Quantity
Required
Discontinued
By Prescriber
Changes To Directions
Continue
on MAR
Discontinue
on MAR
Pharmacy
Contacted
Initials

Palliative Care Toolkit, version 2.2
49
Appendix H: Example of Just in Case Box prescribing from NHS Tayside

Palliative Care Toolkit, version 2.2
50

Palliative Care Toolkit, version 2.2
51

Palliative Care Toolkit, version 2.2
52

Palliative Care Toolkit, version 2.2
53
Appendix I: Patient Group Direction (PGD) template - supply of paracetamol 500mg oral solid dosage form to patients with COVID-19 approaching the end of life requiring relief from pain or fever, by appropriate registered healthcare professionals in NHSScotland.
The purpose of the PGD is to help patients by providing them with more convenient access to treatment during the period of responding to COVID-19. It cannot be used until Appendix 1 is completed for each clinical area.
This PGD authorises appropriate registered healthcare professionals (see section titled:
Characteristics of staff authorised under the PGD) to supply paracetamol 500mg oral solid
dosage form to patients 16 years and older approaching the end of life with pain or fever,
and who meet the criteria for inclusion under the terms of the document.
Change history Person or group
responsible for changes
Date changes authorised Version number

Palliative Care Toolkit, version 2.2
54
Patient Group Direction for the supply of paracetamol 500mg oral solid dosage form
Authorisation
This PGD has been produced by the Area Drugs and Therapeutics Committee Collaborative and (insert group here) to assist NHS Boards to introduce this new service model in a uniform way across NHSScotland. NHS boards should ensure that the final PGD is
considered and approved in line with local clinical governance arrangements for PGDs. The qualified health professionals who may supply paracetamol 500mg oral solid dosage form under this PGD can only do so as named individuals. It is the responsibility of each
professional to practice within the bounds of their own competence and in accordance with their own Code of Professional Conduct, and to ensure familiarity with the marketing authorisation holder’s summary of product characteristics (SPC) for all medicines supplied in accordance with this PGD.
NHS board governance arrangements will indicate how records of staff authorised to operate this PGD will be maintained. Under PGD legislation there can be no delegation. Supply of the medicine has to be by the same practitioner who has assessed the patient
under the PGD. This PGD has been reviewed for NHS insert Board name by:
Doctor Click or tap here to enter text. Signature Click or tap here to enter text.
Pharmacist Click or tap here to enter text. Signature Click or tap here to enter text.
Nurse Click or tap here to enter text. Signature Click or tap here to enter text.
Approved on behalf of NHS insert Board name by:
Medical Director Click or tap here to enter
text. Signature Click or tap here to enter text.
Director of Pharmacy/Senior Pharmacist
Click or tap here to enter text. Signature Click or tap here to enter text.
Clinical
Governance Lead
Click or tap here to enter text. Signature Click or tap here to enter text.
Date Approved Click or tap to enter a date.
Effective from Click or tap to enter a date. Review Date
Click or tap to enter a date.
Clinical Situation
Definition of clinical situation/condition
Patients with COVID-19 approaching the end of life requiring symptomatic relief from pain or fever.

Palliative Care Toolkit, version 2.2
55
Clinical criteria for inclusion
Patients aged 16 years or older
Patient assessed as being in the end-of-life phase by an appropriately trained medical doctor.
Confirmed or suspected COVID-19
Informed consent by patient or patient advocate/carer
Patient or patient advocate/carer must be present at consultation (or involved remotely as appropriate)
Clinical criteria for
exclusion
Regularly takes another product which contains
paracetamol
Hypersensitivity to paracetamol and/or other constituents– review Summary of Product Characteristics of the products
under consideration
No valid consent
Lack of appropriate support/ability to administer oral paracetamol as instructed
Criteria for seeking
further clarification from doctor or independent prescriber
Any doubt as to inclusion/exclusion criteria being met.
Patients at increased risk of liver toxicity include:
Frail elderly
Adults with body weight <50kg
Chronic malnutrition/anorexia For the control of symptom at the end of life, the cautions listed in the BNF of manufacturer’s Summary of Product
Characteristics should not necessarily be a deterrent to the use of paracetamol.
Action if patient excluded from
treatment
Refer to medical doctor/non-medical independent prescriber and document in patient’s medical notes
Action if patient
declines`
Refer patient to medical doctor. The reason why the patient
declined treatment under the PGD will be documented in the patient’s medical notes
Description of Treatment
Name, form and strength of medicine
Paracetamol 500mg tablets, caplets, soluble tablets, effervescent tablets and capsules
Legal status GSL, P
Indicate any off-label use (if relevant)
Route/method of administration
Oral
Dose 500mg to 1000mg, 1 to 2 units of oral solid form dosage.

Palliative Care Toolkit, version 2.2
56
Consider reducing dose to 500mg in frail elderly, adults with body weight <50kg, and chronic malnutrition/ anorexia
Frequency of dose
Every 4 to 6 hours; maximum of 4 doses in 24 hour period
Duration of
treatment
While symptoms persist
Quantity to supply 1x32 of tablets, caplets or capsules, or 1x24 of soluble or effervescent tablets
Maximum or minimum treatment period
Not applicable
Advice to be given to patient before
treatment
Dosing information should be carefully explained and patient/carer understanding checked.
Do not take anything else containing paracetamol while taking this medicine.
Do not exceed the maximum of 4 doses in a 24 hour period
Written information
to be given to the patient or carer
The medicine manufacturer’s Patient Information Leaflet
should be given.
Follow-up advice to be given to patient or carer
If an adverse reaction is causing distress or there is insufficient relief from symptoms following treatment - seek medical advice from a General Practitioner or NHS 24 on 111
Identifying and managing possible
adverse reactions
Refer to BNF or Summary of Product Characteristics for a full list of side-effects.
If an adverse reaction does occur and continues to cause patient distress inform relevant medical practitioner as soon as possible. Report the reaction to the MHRA using the Yellow Card
System. https://yellowcard.mhra.gov.uk/ where appropriate.
Referral for medical advice
Appearance or suspicion of an adverse reaction or patient distress
Facilities and supplies required
Appropriate storage facilities for medicines Appropriately labelled supply Patient information leaflets
Special
considerations / additional information
Details of records required
Click or tap here to enter text.
References BNF No. 78 Available from: https://www.medicinescomplete.com/mc/bnf/current/
accessed on 02 April 2020 SPCs Available at: http://www.medicines.org.uk/emc accessed on: 02 April 2020

Palliative Care Toolkit, version 2.2
57
Scottish Palliative Care Guidelines. Available from https://www.palliativecareguidelines.scot.nhs.uk/ accessed on 02 April 2020
Palliative Care Formulary. Available from https://www.medicinescomplete.com/#/browse/palliative accessed on 02 April 2020
Characteristics of staff authorised under the PGD
Professional
qualifications
Appropriate healthcare professionals for supplying include:
[Boards to adapt this list as appropriate]
Registered pharmacists.
Registered chiropodists and podiatrists.
Registered dental hygienist.
Registered dental therapist.
Registered dietitians.
Registered midwives.
Registered nurses.
Registered occupational therapists.
Registered optometrists.
Registered orthoptists.
Registered orthotists and prosthetists.
Registered paramedics.
Registered physiotherapists.
Registered radiographers.
Registered speech and language therapists. Under PGD legislation there can be no delegation. Supply of the medication has to be by the same practitioner who
has assessed the patient under this PGD. Specialist
competencies or qualifications
Able to assess the person’s (or advocate’s) capacity to
understand the nature and purpose of the medication in order to give or refuse consent. Must be familiar with the relevant paracetamol 500mg oral solid dosage form Summary of Product Characteristics (SPC).
Continuing
education and training
Aware of local treatment recommendations.
Attends approved training and training updates as appropriate.
Audit Trail
Record/Audit Trail
All records must be clear, legible and in an easily retrieval format.
Additional references
British National Formulary (BNF) current edition
MHRA guidance, Patient Group Direction: Who can use them.
Available on https://www.gov.uk/government/publications/patient-group-directions-pgds/patient-group-directions-who-can-use-them accessed on 02 April 2020
National Institute for Health and Care Excellence. Medicines
Practice Guideline: Patient Group Directions. Available on

Palliative Care Toolkit, version 2.2
58
https://www.nice.org.uk/guidance/mpg2/chapter/Recommendations#developing-patient-group-directions accessed on 02 April 2020
Appendix 1 Health professionals approved to provide care under the direction
The lead nurse/professional of each clinical area is responsible for maintaining records of all
clinical areas where this PGD is in use, and to whom it has been disseminated.
The manager who approves a healthcare professional to supply and/or administer medicines under
the patient group direction, is responsible for ensuring that he or she is competent, qualified and trained to do so and for maintaining an up-to-date record of such approved persons in conjunction with the Head of Profession.
The healthcare professional who is approved to supply and/or administer medicines under the
direction is responsible for ensuring that he or she has completed the PGD learnPro module,
understands and is qualified, trained and competent to undertake the duties required. The approved person is also responsible for ensuring that administration or supply is carried out within the terms of the direction, and according to his or her code of professional practice and conduct.
PATIENT GROUP DIRECTION : Supply of paracetamol 500mg oral solid dosage form from Community assessment centres or Emergency departments to patients with COVID-19 approaching the end of life requiring symptomatic relief from pain; by appropriate registered health professional in NHSScotland
Local clinical area(s) where these healthcare professionals will operate this PGD:
Name of Healthcare Professional
Signature Date Tick to confirm PGD learnPro module is completed
Name of Manager Signature Date

Palliative Care Toolkit, version 2.2
59
Name of Healthcare Professional
Signature Date Tick to confirm PGD learnPro module is completed
Name of Manager Signature Date

Palliative Care Toolkit, version 2.2
60

Palliative Care Toolkit, version 2.2
61
Appendix J: Patient Group Direction (PGD) template - supply of morphine sulfate 10mg/5ml oral solution to patients with COVID-19 approaching the end of life requiring relief from pain, breathlessness or cough by appropriate registered healthcare professionals in NHSScotland. Version – 1.0
The purpose of the PGD is to help patients by providing them with more convenient access to treatment during the period of responding to COVID-19. It cannot be used until Appendix
1 is completed for each clinical area.
This PGD authorises appropriate registered healthcare professionals (see section titled: Characteristics of staff authorised under the PGD) to supply morphine sulfate 10mg/5ml oral solution packs of 100ml to patients 16 years and older approaching the end of life with pain,
breathlessness or cough and who meet the criteria for inclusion under the terms of the document.
Change history
Person or group responsible for changes
Date changes authorised Version number

Palliative Care Toolkit, version 2.2
62
Authorisation
This PGD has been produced by the Area Drugs and Therapeutics Committee
Collaborative Click or tap here to enter text. to assist NHS Boards to introduce this
new service model in a uniform way across NHSScotland. NHS boards should
ensure that the final PGD is considered and approved in line with local clinical
governance arrangements for PGDs.
The qualified health professionals who may supply morphine sulfate 10mg/5ml
oral solution under this PGD can only do so as named individuals. It is the
responsibility of each professional to practice within the bounds of their own
competence and in accordance with their own Code of Professional Conduct, and
to ensure familiarity with the marketing authorisation holder’s summary of
product characteristics (SPC) for all medicines supplied in accordance with this
PGD.
NHS board governance arrangements will indicate how records of staff authorised
to operate this PGD will be maintained. Under PGD legislation there can be no
delegation. Supply of the medicine has to be by the same practitioner who has
assessed the patient under the PGD.
This PGD has been reviewed for NHS insert Board name by:
Doctor Click or tap here to enter
text. Signature
Click or tap here to
enter text.
Pharmacist Click or tap here to enter
text. Signature
Click or tap here to
enter text.
Nurse Click or tap here to enter
text. Signature
Click or tap here to
enter text.
Approved on behalf of NHS insert Board name by:
Medical Director Click or tap here to
enter text. Signature
Click or tap here to
enter text.
Director of
Pharmacy/Senior
Pharmacist
Click or tap here to
enter text. Signature
Click or tap here to
enter text.
Clinical
Governance Lead
Click or tap here to
enter text. Signature
Click or tap here to
enter text.
Date Approved Click or tap to enter
a date.
Effective from Click or tap to enter
a date.
Review
Date
Click or tap to enter a
date.
Clinical Situation

Palliative Care Toolkit, version 2.2
63
Definition of
clinical
situation/condition
Patients with COVID-19 approaching the end of life
requiring symptomatic relief from pain, breathlessness
or cough.
Clinical criteria for
inclusion
Patients aged 16 years or older
Patient assessed as being in the end-of-life phase by
an appropriately trained medical doctor.
Confirmed or suspected COVID-19
Informed consent by patient or patient
advocate/carer
Patient or patient advocate/carer must be present at
consultation (or involved remotely as appropriate)
Clinical criteria for
exclusion
Known opioid hypersensitivity
No valid consent
Lack of appropriate support/ability to administer
morphine sulfate as instructed
The following are listed as contra-indications to
morphine in the BNF, however none of the
contraindications are absolute if treatment is titrated
carefully against a patient's symptoms.
Acute respiratory depression
Comatose patients
Head injury (opioid analgesics interfere with
pupillary responses vital for neurological
assessment)
Raised intracranial pressure (opioid analgesics
interfere with pupillary responses vital for
neurological assessment)
Risk of paralytic ileus
Acute abdominal conditions
Delayed gastric emptying
Heart failure secondary to chronic lung disease
Phaeochromocytoma
Criteria for
seeking further
clarification from
doctor or
independent
prescriber
Any doubt as to inclusion/exclusion criteria being met.
For the control of symptoms at the end of life, the
cautions listed in the BNF or manufacturer’s Summary
of Product Characteristics should not necessarily be a
deterrent to the use of morphine sulfate.
Action if patient
excluded from
treatment
Refer to medical doctor/non-medical independent
prescriber and document in patient’s medical notes

Palliative Care Toolkit, version 2.2
64
Action if patient
declines`
Refer patient to medical doctor. The reason why the
patient declined treatment under the PGD will be
documented in the patient’s medical notes
Description of Treatment
Name, form and
strength of
medicine
Morphine sulfate oral solution 10mg/5ml
Legal status POM (Prescription Only Medicine), Controlled Drug
Schedule 5
Indicate any off-
label use (if
relevant)
Breathlessness and cough are off-label use
Route/method of
administration
Oral
Dose 2mg (1mL)
Frequency of
dose
Every 1 to 2 hours as required for symptoms. Maximum
of 3 doses in 4 hours and total maximum of 6 doses in 24
hour period
Duration of
treatment
While symptoms persist
Quantity to
supply
1 x 100mL
Maximum or
minimum
treatment period
Not applicable
Advice to be
given to patient
before
treatment
Dosing information should be carefully explained and
patient/carer understanding checked.
An oral syringe with appropriate graduations should be
supplied.
Morphine oral solution usually takes approximately 15
minutes to take effect.
Inform of possible side effects including nausea,
vomiting, and constipation and that supportive
treatments can manage these effects.
Morphine may cause confusion and drowsiness, if this
happens do not drive.

Palliative Care Toolkit, version 2.2
65
Written
information to
be given to the
patient or carer
The medicine manufacturer’s Patient Information Leaflet
should be given and the additional PIL associated with
the use of the medicine in this situation.
Follow-up
advice to be
given to patient
or carer
If an adverse reaction is causing distress or there is
insufficient relief from symptoms following treatment
instructions seek medical advice from a General
Practitioner or NHS 24 on 111
Identifying and
managing
possible adverse
reactions
Nausea, vomiting, constipation, drowsiness and confusion
are common side effects of morphine. Refer to BNF or
Summary of Product Characteristics for a full list of side-
effects. If an adverse reaction does occur and continues to cause
patient distress inform relevant medical practitioner as
soon as possible.
Report the reaction to the MHRA using the Yellow Card
System. https://yellowcard.mhra.gov.uk/ where
appropriate.
Referral for
medical advice
Appearance or suspicion of an adverse reaction or
patient distress.
Subtle hallucinations should be reported to your doctor
as these may indicate the dose of morphine requires
reviewed.
Facilities and
supplies
required
Appropriate storage facilities for medicines
Appropriately labelled supply of morphine oral solution
10mg/5ml.
Patient information leaflets
Special
considerations /
additional
information
Details of
records required
Click or tap here to enter text.
References BNF No. 78 Available from:
https://www.medicinescomplete.com/mc/bnf/current/
accessed on 02 April 2020
SPCs Available at: http://www.medicines.org.uk/emc
accessed on: 02 April 2020
Scottish Palliative Care Guidelines. Available from
https://www.palliativecareguidelines.scot.nhs.uk/
accessed on 02 April 2020
Palliative Care Formulary. Available from
https://www.medicinescomplete.com/#/browse/palliative
accessed on 02 April 2020

Palliative Care Toolkit, version 2.2
66
Characteristics of staff authorised under the PGD
Professional
qualifications
Appropriate healthcare professionals for supplying a
POM CD5 include: [Boards to adapt this list as
appropriate]
Registered pharmacists.
Registered chiropodists and podiatrists.
Registered midwives.
Registered nurses.
Registered occupational therapists.
Registered optometrists
Registered orthoptists.
Registered orthotists and prosthetists.
Registered paramedics.
Registered physiotherapists
Registered radiographers
Under PGD legislation there can be no delegation. Supply of the medication has to be by the same practitioner who has assessed the patient under this
PGD. Specialist
competencies or
qualifications
Able to assess the person’s capacity to understand the
nature and purpose of the medication in order to give
or refuse consent.
Must be familiar with the relevant morphine sulfate
10mg/5ml oral solution Summary of Product
Characteristics (SPC).
Continuing
education and
training
Aware of local treatment recommendations.
Attends approved training and training updates as
appropriate.
Audit Trail
Record/Audit
Trail
All records must be clear, legible and in an easily retrieval
format.
Additional
references
British National Formulary (BNF) current edition
MHRA guidance, Patient Group Direction: Who can use
them. Available on
https://www.gov.uk/government/publications/patient-
group-directions-pgds/patient-group-directions-who-can-
use-them accessed on 02 April 2020
National Institute for Health and Care Excellence.
Medicines Practice Guideline: Patient Group Directions.
Available on
https://www.nice.org.uk/guidance/mpg2/chapter/Recomm

Palliative Care Toolkit, version 2.2
67
endations#developing-patient-group-directions accessed
on 02 April 2020
Specialist Pharmacy Services. Patient Group Direction.
Available from https://www.sps.nhs.uk/articles/who-can-
supply-or-administer-controlled-drugs-under-the-terms-
of-a-patient-group-direction-and-under-what-
circumstances/ accessed on 02 April 2020
Appendix 1
Health professionals approved to provide care under the direction
The lead nurse/professional of each clinical area is responsible for maintaining records of
all clinical areas where this PGD is in use, and to whom it has been disseminated.
The manager who approves a healthcare professional to supply and/or administer
medicines under the patient group direction, is responsible for ensuring that he or she is
competent, qualified and trained to do so and for maintaining an up-to-date record of
such approved persons in conjunction with the Head of Profession.
The healthcare professional who is approved to supply and/or administer medicines
under the direction is responsible for ensuring that he or she has completed the PGD
learnPro module, understands and is qualified, trained and competent to undertake the
duties required. The approved person is also responsible for ensuring that administration
or supply is carried out within the terms of the direction, and according to his or her code
of professional practice and conduct.
PATIENT GROUP DIRECTION : Supply of morphine sulfate oral solution 10mg/5ml from
Community assessment centres or Emergency departments to patients with COVID-19
approaching the end of life requiring symptomatic relief from pain, breathlessness or
cough; by appropriate registered health professional in NHSScotland
Local clinical area(s) where these healthcare professionals will operate this PGD:
Name of Healthcare Professional
Signature Date Tick to confirm PGD learnPro module is completed
Name of Manager Signature Date

Palliative Care Toolkit, version 2.2
68
Name of Healthcare Professional
Signature Date Tick to confirm PGD learnPro module is completed
Name of Manager Signature Date

Palliative Care Toolkit, version 2.2
69
Palliative Care Toolkit, version 2.2
70
Appendix K: Patient Group Direction (PGD) template - supply of lorazepam 1mg tablets, to patients with COVID-19 approaching the end of life requiring relief from anxiety and distress, by appropriate registered healthcare professionals in NHS Scotland.
Version – 0.1
The purpose of the PGD is to help patients by providing them with more convenient access to treatment during the period of responding to COVID-19. It cannot be used until Appendix
1 is completed for each clinical area.
This PGD authorises appropriate registered healthcare professionals (see section titled: Characteristics of staff authorised under the PGD) to supply lorazepam 1mg tablets packs of 10 tablets to patients 16 years and older approaching the end of life with anxiety or
distress and who meet the criteria for inclusion under the terms of the document.
Change history
Person or group responsible for changes
Date changes authorised Version number

Palliative Care Toolkit, version 2.2
71
Patient Group Direction for the supply of lorazepam 1mg tablets (manufactured by Genus, PVL or TEVA); pack size 10 tablets, legally classified as a Prescription Only Medicine Controlled Drug Schedule 4 Part 1
Authorisation
This PGD has been produced by the Area Drugs and Therapeutics Committee Collaborative Click or tap here to enter text. to assist NHS Boards to introduce this new service model in a
uniform way across NHSScotland. NHS boards should ensure that the final PGD is
considered and approved in line with local clinical governance arrangements for PGDs. The qualified health professionals who may supply lorazepam 1mg tablets under this PGD can only do so as named individuals. It is the responsibility of each professional to practice
within the bounds of their own competence and in accordance with their own Code of Professional Conduct, and to ensure familiarity with the marketing authorisation holder’s summary of product characteristics (SPC) for all medicines supplied in accordance with this PGD.
NHS board governance arrangements will indicate how records of staff authorised to operate this PGD will be maintained. Under PGD legislation there can be no delegation. Supply of the medicine has to be by the same practitioner who has assessed the patient
under the PGD. This PGD has been reviewed for NHS insert Board name by:
Doctor Click or tap here to enter text. Signature Click or tap here to enter text.
Pharmacist Click or tap here to enter text. Signature Click or tap here to enter text.
Nurse Click or tap here to enter text. Signature Click or tap here to enter text.
Approved on behalf of NHS insert Board name by:
Medical Director Click or tap here to enter
text. Signature Click or tap here to enter text.
Director of Pharmacy/Senior Pharmacist
Click or tap here to enter
text. Signature Click or tap here to enter text.
Clinical
Governance Lead
Click or tap here to enter text. Signature Click or tap here to enter text.
Date Approved Click or tap to enter a date.
Effective from Click or tap to enter a date. Review Date
Click or tap to enter a date.

Palliative Care Toolkit, version 2.2
72
Clinical Situation
Definition of clinical situation/condition
Patients with COVID-19 approaching the end of life requiring symptomatic relief from anxiety or distress.
Clinical criteria for
inclusion Patients aged 16 years or older
Patient assessed as being in the end-of-life phase by an appropriately trained medical doctor.
Confirmed or suspected COVID-19
Informed consent by patient or patient advocate/carer
Patient or patient advocate/carer must be present at consultation (or involved remotely as appropriate)
Clinical criteria for exclusion
Known benzodiazepine hypersensitivity
No valid consent
Lack of appropriate support/ability to administer lorazepam as instructed
The following are listed as contra-indications to
benzodiazepines and lorazepam in the BNF, however none of the contraindications are absolute if treatment is titrated carefully against a patient's symptoms.
Acute pulmonary insufficiency
Marked neuromuscular respiratory weakness
chronic psychosis
Sleep apnoea syndrome
Unstable myasthenia gravis
CNS depression
Compromised airway
Respiratory depression
Criteria for seeking further clarification from doctor or independent
prescriber
Any doubt as to inclusion/exclusion criteria being met.
Action if patient excluded from treatment
Refer to medical doctor/non-medical independent prescriber and document in patient’s medical notes
Action if patient declines`
Refer patient to medical doctor. The reason why the patient declined treatment under the PGD will be documented in the patient’s medical notes
Description of Treatment
Name, form and strength of medicine
Lorazepam 1mg tablets for sublingual use (manufactured by Genus, PVL or TEVA)

Palliative Care Toolkit, version 2.2
73
Legal status Prescription Only Medicine, Controlled Drug Schedule 4 part 1
Indicate any off-label use (if relevant)
Sublingual route is off-label use
Route/method of administration
Sublingual, put half a tablet under the tongue and leave to dissolve.
If mouth dry, moisten first with sips of water, otherwise tablet will not dissolve.
Dose Half of a 1mg tablet (500 micrograms)
Frequency of dose
Every 4 hours as required for symptoms; maximum of 4 doses in 24 hour period
Duration of treatment
While symptoms persist
Quantity to supply 10
Maximum or minimum treatment period
Not applicable
Advice to be given to patient before
treatment
Dosing information should be carefully explained and patient/carer understanding checked.
Inform of possible side effects including decreased alertness, confusion, drowsiness, paradoxical increase in anxiety, agitation or aggression, and how to manage these effects.
Lorazepam may cause confusion and drowsiness, if this happens do not drive.
Written information
to be given to the patient or carer
The medicine manufacturer’s Patient Information Leaflet
should be given and the additional PIL associated with the use of the medicine in this situation.
Follow-up advice to be given to patient or carer
If an adverse reaction is causing distress or there is insufficient relief from symptoms following treatment instructions seek medical advice from a General Practitioner or NHS 24 on 111.
Identifying and
managing possible adverse reactions
Confusion, drowsiness, dizziness and decreased alertness
are common side effects of lorazepam. Refer to BNF or Summary of Product Characteristics for a full list of side-effects. If an adverse reaction does occur and continues to cause
patient distress inform relevant medical practitioner as soon as possible. Report the reaction to the MHRA using the Yellow Card System. https://yellowcard.mhra.gov.uk/ where appropriate.
Referral for medical advice
Appearance or suspicion of an adverse reaction or patient distress
Facilities and supplies required
Appropriate storage facilities for medicines Appropriately labelled supply of lorazepam tablets. Patient information leaflets

Palliative Care Toolkit, version 2.2
74
Special considerations / additional
information
Details of records required
Click or tap here to enter text.
References BNF No. 78 Available from: https://www.medicinescomplete.com/mc/bnf/current/ accessed on 03 April 2020 SPCs Available at: http://www.medicines.org.uk/emc
accessed on: 03 April 2020 Scottish Palliative Care Guidelines. Available from https://www.palliativecareguidelines.scot.nhs.uk/ accessed on 03 April 2020
Palliative Care Formulary. Available from https://www.medicinescomplete.com/#/browse/palliative accessed on 03 April 2020
Characteristics of staff authorised under the PGD
Professional
qualifications
Appropriate healthcare professionals for supplying lorazepam
(a POM CD4 Part 1 medicine) include: [Boards to adapt this list as appropriate]
Registered pharmacists.
Registered chiropodists and podiatrists.
Registered midwives.
Registered nurses.
Registered occupational therapists.
Registered optometrists
Registered orthoptists.
Registered orthotists and prosthetists.
Registered paramedics.
Registered physiotherapists
Registered radiographers Under PGD legislation there can be no delegation.
Supply of the medication has to be by the same practitioner who has assessed the patient under this PGD.
Specialist competencies or qualifications
Able to assess the person’s capacity to understand the nature and purpose of the medication in order to give or refuse consent.
Must be familiar with the relevant lorazepam 1mg tablets Summary of Product Characteristics (SPC).
Continuing education and training
Aware of local treatment recommendations. Attends approved training and training updates as appropriate.

Palliative Care Toolkit, version 2.2
75
Audit Trail
Record/Audit
Trail
All records must be clear, legible and in an easily retrieval format.
Additional references
British National Formulary (BNF) current edition
MHRA guidance, Patient Group Direction: Who can use them. Available on https://www.gov.uk/government/publications/patient-group-directions-pgds/patient-group-directions-who-can-use-
them accessed on 03 April 2020
National Institute for Health and Care Excellence. Medicines Practice Guideline: Patient Group Directions. Available on https://www.nice.org.uk/guidance/mpg2/chapter/Recommendatio
ns#developing-patient-group-directions accessed on 03 April 2020
Specialist Pharmacy Service Coronavirus (COVID-19) Available at
https://www.sps.nhs.uk/articles/who-can-supply-or-administer-controlled-drugs-under-the-terms-of-a-patient-group-direction-and-under-what-circumstances/ accessed on 03 April 2020
Appendix 1 Health professionals approved to provide care under the direction
The lead nurse/professional of each clinical area is responsible for maintaining records of all
clinical areas where this PGD is in use, and to whom it has been disseminated.
The manager who approves a healthcare professional to supply and/or administer medicines under
the patient group direction, is responsible for ensuring that he or she is competent, qualified and trained to do so and for maintaining an up-to-date record of such approved persons in conjunction with the Head of Profession.
The healthcare professional who is approved to supply and/or administer medicines under the
direction is responsible for ensuring that he or she has completed the PGD learnPro module,
understands and is qualified, trained and competent to undertake the duties required. The approved person is also responsible for ensuring that administration or supply is carried out within the terms of the direction, and according to his or her code of professional practice and conduct.
PATIENT GROUP DIRECTION : Supply of lorazepam 1mg tablets from Community
assessment centres or Emergency departments to patients with COVID-19 approaching the end of life requiring symptomatic relief from anxiety or distress; by appropriate registered health professional in NHSScotland
Local clinical area(s) where these healthcare professionals will operate this PGD:

Palliative Care Toolkit, version 2.2
76
Name of Healthcare Professional
Signature Date Tick to confirm PGD learnPro module is completed
Name of Manager Signature Date
Name of Healthcare Professional
Signature Date Tick to confirm PGD learnPro module is completed
Name of Manager Signature Date

Palliative Care Toolkit, version 2.2
77

Palliative Care Toolkit, version 2.2
78
Appendix L: Patient Leaflet - Supply of medicines for control of symptoms
What are ‘Just in case’ medicines?
Just in case medicines are a range of medicines that can be given to take home to
help relieve pain or other symptoms.
You will have been told if you should continue to take your usual medicines. Your
usual oral medicines (e.g. painkillers) should be tried first to see if they help to
relieve your symptoms.
What are the ‘Just in case’ medicines for?
You may not need any of these medicines right now, however, they have been
prescribed for you because your healthcare team think that they may be needed
at some point in the coming days to help with:
pain relief
cough/ breathlessness or breathing (especially if you're unable to clear
your own throat)
anxiety or restlessness
The healthcare professional who gives you the ‘just in case’ medicines will assess
you and will agree a plan with you and your carer about what to do if your usual
medicines need to be changed or if another dose of the ‘Just in case’ medicine is
needed.
Who can/should give you ‘Just in case’ medicines?
These ‘just in case’ medicines can be taken by you or given to you by your carer.
The medicines that are supplied are for oral use (to be swallowed). The medicines
will either have a dispensing label with instructions (similar to what you would
receive from a community pharmacy) or instructions will be available from the
patient information leaflet provided with the medicine.
Information below provides further details on how to take these medicines in
addition to the Patient Information Leaflets (PIL) that are provided with the
medicines.
Your doctor / clinician will supply you with enough medicine at this time to treat
your symptom. If a further supply of medicines is required you or your carer
should let you GP know. If your condition changes, you or your carer should let
your GP practice or community nurse (in hours)/the NHS 24 111 service (out of
hours) know so that they can reassess you and make sure your regular medicines,
the ‘Just in case’ medicines, and their doses, are still right for you.
If you are admitted to hospital or another care setting, the medicines can go with
you as they have been prescribed for you. If you're unable or do not wish to do
this, please let the staff know that you have them in the house.

Palliative Care Toolkit, version 2.2
79
If ‘Just in case’ medicines or any other medicines are no longer needed, they
should be returned to your community pharmacy or dispensing doctor in a plastic
bag. Further information on returning unused medicines can be found at -
https://www.nhsinform.scot/illnesses-and-conditions/infections-and-poisoning/coronavirus-
covid-19/coronavirus-covid-19-general-advice#common-questions
Morphine and Lorazepam for Treatment of Shortness of Breath, Cough and
Anxiety.
All medicines are supplied with a manufacturer’s ‘Patient Information Leaflet’. This
can provide a great deal of information about the medicine, its normal uses and
side effects. However, most medicines have more than one effect on the body and
for many years, it has been known that certain medicines are safe and effective
for the treatment of symptoms other than those specified by the medicine’s
manufacturer and there is now plenty of evidence to confirm such use.
We are providing you with this extra information to inform you of the reason(s)
why you are taking this medicine and to highlight any other information. This
should be read in conjunction with the attached manufacturer’s patient
information leaflet.
Lorazepam 1mg tablets
Lorazepam is sometimes used for anxiety or distress, which may feel worse if you
are short of breath. Instead of swallowing the tablet you allow it to dissolve under
your tongue.
Frequently asked questions
Q. What form(s) of this medicine are there and how is it usually taken?
A. This medicine is normally available as a tablet. The dose prescribed is normally
between half a 1mg tablet (0.5mg or 500 micrograms) to one 1mg tablet. It has
been prescribed to be taken when needed for shortness of breath or anxiety. You
usually place this dose under your tongue. Under the tongue (sublingual)
lorazepam tablets start to work within 10 to 20 minutes of taking a dose for
breathlessness and usually last for about eight hours. You can place a dose under
the tongue every four to six hours, however you may not need as much as this.
The maximum number of doses that you can take is 4 doses in 24 hours.
Because the medicine gets into your body easily from the soft tissue in your
mouth, you should place the tablet under your tongue and keep it there until it
has fully dissolved. Before taking this medicine, make sure your mouth is moist by
taking some water. This will help the tablet dissolve better under your tongue. The
tablets can be swallowed instead of placing under the tongue, but will take a little
longer to get into your body to have the same effect.
Note: Always follow the dose indicated on the label or advised by a healthcare
professional.

Palliative Care Toolkit, version 2.2
80
Q. What are the most common side effects I might experience?
A. Lorazepam might make you sleepy (drowsy) shortly after you take it. Because
of this, we advise you to rest for a while in a comfortable chair or bed
immediately after you take the dose. You should not drive immediately after
taking lorazepam or if it makes you sleepy. Drowsiness is more likely to occur if
you are taking other medicines that cause sleepiness. Please inform your doctor
or pharmacist of any other medicines you are taking.
Occasionally, you may also experience light headedness (dizziness) and a dry
mouth. If you do experience light headedness which lasts for a long time, let your
doctor or pharmacist know.
Drinking alcohol may also make these side effects worse.
Q. What do I do if I forget to take a dose?
A. Take a dose as soon as you remember. Do not take a double dose to make up
for the missed one. If you are sick and bring up the medicine within 30 minutes of
taking it, repeat the dose as soon as you feel better.
Safe storage
Your medication needs to be kept in a safe place out of the reach of children. It
needs to be stored in the original container. Return unused medication to a
pharmacy in a plastic bag. For further information on returning unused medicines
please see the link to NHS Inform above.
Morphine Sulfate Oral Solution 10mg/5ml
Morphine has been used as a treatment for breathlessness for many years and is
proven to be effective and safe. It can also be useful to treat a very persistent
cough.
If you have been prescribed the morphine to use for pain, follow the directions
you have been given and read the manufacturer’s Patient Information Leaflet
supplied with it.
Frequently asked questions
Q. What form(s) of this medicine are there and how is it usually taken?
A. Morphine works quickly to relieve coughing and the feeling of being breathless.
You will usually be started on a small dose of morphine, around 2mg which is 1ml
of the oral solution. This will start to work within 10 to 20 minutes after taking a
dose for breathlessness. Usually the effect of the morphine will last between 2 to
3 hours. You may need to take the morphine every 1 to 2 hours initially to help

Palliative Care Toolkit, version 2.2
81
relieve symptoms. If you need to take more than 3 doses of morphine in 4 hours
or 6 doses of morphine in 24-hours, please contact your GP, nurse or pharmacist
for advice as your dose may need to be increased. Measure the morphine solution
(liquid) out from the bottle with an oral syringe (a syringe which is specially
designed to use with medicines you take by mouth) and squeeze it gently into
your mouth and swallow.
Q. What are the most common side effects I might experience?
A. As with all medicine there may be side effects which can include:
Constipation – it may be useful to take a laxative while taking morphine
Nausea and vomiting
• Drowsiness (sleepiness), if you do feel drowsy it is important that you do
not drive
Skin itching, and
Dry mouth.
Nausea, itching and drowsiness usually go away over time and with continued use
of morphine. If any of these symptoms are making you feel unwell contact your
GP. If you are taking other medicines which make you sleepy or have drunk
alcohol, this may make you even sleepier.
Dry mouth
Try to keep your mouth and lips clean and moist. Brush your teeth regularly
morning and night with fluoride toothpaste, preferably not immediately after
taking a dose of morphine. Frequent cool drinks, sips of water and ice cubes may
help. If your mouth becomes sore, please see your healthcare professional for
advice and help.
Q. Is morphine dangerous, will I become addicted?
A. Some people may feel concerned at the thought of using morphine for several
reasons:
• Some people may recognize this as a medicine used for pain including
when someone has cancer or is dying. This is absolutely not why morphine
is used for breathlessness.
• Some people may think that using morphine will make you addicted. The
small amount of morphine used to treat breathlessness does not cause
addiction. The morphine can be safely reduced and stopped if it does not
benefit you, or if you no longer need it.
• You might notice that the packet information leaflet includes a warning
that states that it is dangerous to take morphine when you have a breathing
condition. This is only a possible problem if you need to take very large
doses of morphine to treat pain. It is safe and helpful to you in the low
doses prescribed for treating breathlessness.

Palliative Care Toolkit, version 2.2
82
It is important to let your doctor know if you feel the morphine is not helping, as
it may be that you need a larger dose regularly, or other medicines may help. If
you are taking more frequent doses of morphine you may feel unwell in one or
more of these ways:
more sleepy than usual
feeling sick more of the time
restlessness or jumpiness, and
bad dreams and/or confusion.
Should this happen, please tell your prescriber as they may want to review your
medicine for breathlessness.
Safe storage
Your medication needs to be kept in a safe place out of the reach of children. It
needs to be stored in the original container. Please return unused medication to a
pharmacy in a plastic bag. For further information on returning unused medicines
please see the link to NHS Inform above.

Palliative Care Toolkit, version 2.2
83
Appendix M: Coronavirus in care homes – visual

Palliative Care Toolkit, version 2.2
84
Appendix N: Administration of palliative care medicine for care home residents at end of life (courtesy of SPCPS based on a Model of Care developed by NHSGG&C)
Symptom of COVID-19
Medicines administered by a carer Medicines administered by nursing staff/trained staff (subcutaneous administration)

Palliative Care Toolkit, version 2.2
85
Homely remedy – stock in care
home
Prescribed on a GP10 -
access via community
pharmacy
Medication stocked
in care homes – via
protocol
Just in case box
medicines/palliative
care amps – via
GP10
Pain Paracetamol tablets/soluble tablets
(500mg)/liquid
(250mg/5ml)/suppositories(500mg/1g)
Morphine 10mg/5ml liquid
Buprenorphine patch
Fentanyl patch
Diclofenac suppositories
Morphine/oxycodone/
alfentanil injection
Nausea &
vomiting
Prochlorperazine 3mg tabs
Hyoscine hydrobromide
300microgram tablets
Hyoscine hydrobromide 1.5mg patch
Can be given orally or
sublingually
Levomepromazine 6mg
tablets
Ondansetron 4mg
orodispersible tablets
Olanzepine orodispersible
tablets
Levomepromazine
injection
Breathlessness Non-pharmacological measures Morphine 10mg/5ml liquid
Buccal midazolam
Midazolam injection
Morphine injection
Cough Codeine linctus 15mg/5ml liquid Morphine 10mg/5ml liquid Morphine injection
Respiratory
secretions
Hyoscine hydrobromide
300microgram tabs
Hyoscine hydrobromide 1.5mg patch
Ipratropium inhaler Hyoscine
butylbromide
Hyoscine
hydrobromide/
Hyoscine
butylbromide/
Glycopyrronium
Anxiety and
distress
- Lorazepam 1mg tablets -
sublingual
Buccal midazolam
Diazepam rectal tubes
Levomepromazine
injection
Midazolam injection

Palliative Care Toolkit, version 2.2
86
Delirium and
agitation
- Levomepromazine tablets -
sublingual
Olanzepine oro-dispersible
tablets (sublingual)
Buccal midazolam
Levomepromazine
injection
Haloperidol injection
Haloperidol injection
Midazolam amps
Levomepromazine
amps
Seizures - Buccal midazolam
Diazepam rectal tubes
Carbamazepine suppositories
Midazolam

Palliative Care Toolkit, version 2.2
87
Appendix O – Summary of issues to be considered to support care home residents accessing palliative care medicines during the COVID-19 pandemic (courtesy of SPCPS)
Priority area Action
Shortage of GP prescribers Support the prescribing of dose ranges (see
Appendix A)
Local arrangement
Identify any other prescribers non-medical
prescribers
Local arrangements
Access to JICB medicines Distribute JICB kardexes to all care homes – local
arrangement
Prescribe anticipatory JICB medicines to all
residents in advance, when COVID-19 is confirmed.
Do not dispense until needed to reduce wastage.
Ensure timely access to palliative care medicines
via palliative care pharmacies or local
arrangements for OOH
Care homes Update the homely remedy policy to include GSL/P
medicines that a carer could give to a care home
resident to help alleviate symptoms
Update the homely remedy policy.
See sample protocols from NHS GG&C.
Care homes may stock prescription only medicines
for symptoms of COVID-19 (for example hyoscine
butylbromide for secretions) if the requirements of
the pandemic exemption (Medicines Regulation
247) are met
New policy required to support this which includes
the development of board approved disease
protocols. See sample protocols from NHS GG&C.
Care homes can stock two of the medicines in the
JICB (levomepromazine and hyoscine
butylbromide) in the care home to improve access
to these medicines, for end of life care
New policy required to support this which includes
the development of board approved disease
protocols. See sample protocols from NHS GG&C.

Palliative Care Toolkit, version 2.2
88
Community Pharmacy Care Home residents can access standard palliative
care medicines and alternative palliative care
medicines that a carer could administer on a GP10
via the community pharmacy.
See the ‘alternatives to regular medication normally
given via a syringe pump when this is not available’
guideline at
www.palliativecareguidelines.scot.nhs.uk.
Local arrangement
Just in Case Boxes Need to be prescribed on a GP10 and dispensed by
community pharmacy
All JICB medicines are given subcutaneously so
need to be administered by a nurse/trained staff.
Shortage of essential
palliative care medicines
Care home staff being able to access information
about medicine supply issues
SPCPA/ community pharmacists/ local
arrangements to provide advice and recommend
alternatives

Palliative Care Toolkit, version 2.2
89
Appendix P – Members of Working Group for the Palliative Care Toolkit
Name Surname Role Organisation
Alison Strath Principal
Pharmaceutical
Officer
Scottish Government
Anne Wilson Palliative Care
Pharmacist
NHS Forth Valley
Joanne Barton Technical Manager,
Operations and
Medicines
Management
NHS Greater Glasgow and Clyde
Morgan Reilly Senior Policy
Manager
Scottish Government
Noreen Downes Principal
Pharmacist
Scottish Medicine Consortium,
Healthcare Improvement Scotland
Scott Hill National Clinical
Lead (Pharmacy)
Area Drug and Therapeutics
Committee Collaborative and
Scottish Medicines Consortium,
Healthcare Improvement Scotland
Members of the Scottish Palliative Care Pharmacy Association (SPCPA) and
colleagues from across health and social care who provided advice and feedback
on the development of the toolkit are thanked for their contribution.
Queries or comments related to the toolkit can be sent to: [email protected]

Palliative Care Toolkit, version 2.2
90
© Crown copyright 2020
You may re-use this information (excluding logos and images) free of charge in
any format or medium, under the terms of the Open Government Licence. To view
this licence, visit http://www.nationalarchives.gov.uk/doc/opengovernment-
licence/ or e-mail: [email protected]. Where we have identified any
third party copyright information you will need to obtain permission from the
copyright holders concerned.
The Scottish Government, St Andrew’s House, Edinburgh, EH1 3DG