inpatient glycemic management
TRANSCRIPT

8/5/2015
1
Robert J. Rushakoff, MD
Medical Director, Inpatient DiabetesProfessor of Medicine
Division of Endocrinology and MetabolismUniversity of California, San FranciscoSan Francisco, CA 94115
Disclosures
Conflict of Interest (COI) and Financial
Relationship Disclosures:
–none
Inpatient Glycemic Management:How We Get Others To Follow Our Lead
August 5th, 2015New Orleans, LA
Objectives1) State current inpatient glycemic control goals
2) Discuss several strategies to improve insulin safety
3) Describe several ways to decrease clinical inertia in
acute care
4) State innovative ways to educate health care
professionals in the hospital setting using technology
"Each blind man perceived the elephant as something different: a
rope, a wall, tree trunks, a fan, a snake, a spear..."

8/5/2015
2
EducationNurses
Physicians
Students
Patient Education
TransitionsOutpatient to Inpatient
Inpatient to Inpatient
Inpatient to Outpatient
Data Collection
Medical Errors
Glucometrics
Diabetes Management
Order Entry
Smart Orders
Dosing Calculators
Jargon
CQI
Patient Assessment of Skills, Education
Diabetes Assessment Form
1.-----------------------------------------------------------------------------
2.-----------------------------------------------------------------------------
3.-----------------------------------------------------------------------------
4.-----------------------------------------------------------------------------
5.-----------------------------------------------------------------------------
6.-----------------------------------------------------------------------------
7.-----------------------------------------------------------------------------
8.-----------------------------------------------------------------------------
9.-----------------------------------------------------------------------------
10.----------------------------------------------------------------------------
11.----------------------------------------------------------------------------
12.----------------------------------------------------------------------------
13.----------------------------------------------------------------------------
14.----------------------------------------------------------------------------
15.----------------------------------------------------------------------------
16.----------------------------------------------------------------------------
17.----------------------------------------------------------------------------
18.----------------------------------------------------------------------------
19.----------------------------------------------------------------------------
20.----------------------------------------------------------------------------
21.----------------------------------------------------------------------------
22.----------------------------------------------------------------------------
23.----------------------------------------------------------------------------
Page 1 of 6
Coordination of Outpatient Care
Home care services
Outpatient diabetes classes
Medical Errors
JCAHO
ICU ProtocolsPeriopManagement
Secondary Diagnosis
Insulin Administration
• Order Written
• Order Sent to
Pharmacy
• Order Entry by
Pharmacist
• Drug Preparation by
pharmacy
• Insulin delivery to unit
• Medication
Administration
• Documentation
Inpatient Diabetes Goals
Who Cares
Just get patient
home
Sliding Scales are
fine
Avoid that scary hypoglycemia
Inpatient Diabetes Goals
Normal glucoses
for everyone
A high glucose
means failure
Sliding Scales are
banned
Some
hypoglycemia is
acceptable
Inpatient Diabetes Goals
Appropriate Glucose
Control Based on
physiology and
outcome studies
Target Glucose Levels
Alive
No DKA or
Hyperosmolar
Coma
Target Glucose Levels
No hypo- or
hyperglycemia
•Prevent fluid and electrolyte
abnormalities secondary to
osmotic diuresis
•Improve WBC function
•Improve gastric emptying
•Decrease surgical complications
•Earlier hospital dischange
•Decreased post-MI mortality
•Decreased post-CABG
morbidity and mortality
Target Glucose Levels

8/5/2015
3
Normal
Glucoses
Decreased Morbidity and
Mortality
Target Glucose Levels
Problems With
High Glucoses
Glucose and Post-CABG: Morbidity and Mortality
Diabetes and Coronary Artery Bypass Surgery
An examination of perioperative glycemic control and outcomes
• Retrospective review of 291 patients surviving 24 h post-op
• 40% with retinopathy, nephropathy, or neuropathy
Inpatient complications:
For each 1 mmol/l (18 mg/dL) increase in post-op day 1 over 6.1 mmol/l (110 mg/dL), a 17% increased risk of complications
McAlister FA et al.
Diabetes Care. 2003; 26:1518-1524.
High Blood Glucose Levels Associated With Increased Mortality in ICU
• Retrospective review of 259,040 critically ill patients conducted by the Veterans Affairs Inpatient Evaluation Center based in Cincinnati
• Hyperglycemia was an independent predictor of
mortality starting at 111 mg/dL
• Effect was greatest with acute myocardial
infarction, unstable angina, and stroke
– Raised MI risk from 1.7 to 6 times
– Raised stroke risk from 1.8 to 29 times
– Raised unstable angina from 1.4 to 3 times
Falciglia M et al. Crit Care Med. 2009; 37:3001-3009.
• A significant but weaker effect was seen in patients with sepsis, pneumonia, and pulmonary embolism
• Hyperglycemia was not found to be associated with mortality in diseases such as COPD and hepatic failure, hip fractures
• In diabetes patients, the increase in mortality risk was not seen until mean glucose was >146 mg/dL
Hyperglycemia–related mortality in critically ill patients varies with admission diagnosis
Falciglia M et al. Crit
Care Med. 2009; 37:3001-3009.
Intervention
Studies

8/5/2015
4
Decreased InfectionsInsulin infusion improves neutrophil function
in diabetic cardiac surgery patients
Perioperative IV insulin infusion
Neutrophil phagocytic activity
% baseline
Control 47
Insulin 75
Rassias AJ et al.
Anesth Analg. 1999; 88:1011-
1016.
Decreased InfectionsGlucose control lowers the risk of wound
infection in diabetics after open-heart operations
Perioperative IV insulin infusion
Protocol to maintain glucoses <200 mg/dL
Incidence of Deep Wound Infections (%)
1997 1999
Routine Control 2.4 2.0“Tight” Control 1.5 0.8
Zerr KJ et al. Ann Thorac Surg. 1997;63:356-361. Furnary AP et al. Ann Thorac Surg. 1999;67:352-360.
Furnary AP et al. J Thorac Cardiovasc Surg. 2003;125:1007-1021.
Decreased Morbidity and MortalityIntensive Insulin Therapy in Critically Ill Patients
• Patients (all) on mechanical ventilation in ICU
• Randomly assigned to IV insulin maintaining glucoses between 80-
110 mg/dL or conventional treatment (IV insulin if glucose >215
mg/dL then maintain glucose between 180-200)
Van den Berghe G et al. N Engl J Med. 2001;345:1359-1367.
% given insulin 24-hour dose AM glucose
Intensive 99 71 units 103
Conventional 39 33 units 153
12 month mortality
Intensive 4.6%
Conventional 8.6%
Main effect on patients
in ICU >5 days
NICE-SUGAR
• 6104 adults who were expected to require treatment in the ICU
on 3 or more consecutive days randomized to intensive blood
glucose control (target range, 81 to 108 mg/dL) or conventional
blood glucose control (<180 mg/dL)
• Primary endpoint death from any cause within 90 days after
randomization
• Baseline characteristics similar
The NICE-SUGAR Study Investigators. N Engl J Med. 2009;360:1283-1297.
Data on Blood Glucose Level, According to Treatment
Group
The NICE-SUGAR Study Investigators. N Engl J Med. 2009;360:1283-1297.
Probability of Survival and Odds Ratios for Death, According to Treatment Group
Problems
With Low
Glucoses

8/5/2015
5
Hypoglycemia and Mortality in Insulin-treated vs on–Insulin-treated AMI Patients
Kosiborod M, et al. JAMA. 2009;301(15):1556-1564.
Hypoglycemia
No hypoglycemia
P=.92P<.001
Mo
rta
lity
, %
10.4
18.4
9.2 10.2
0
10
20
No Insulin Treatment Insulin Treatment
Hypoglycemia was a predictor of
higher mortality in patients nottreated with insulin, but not
in patients treated with insulin
Hazard Ratio for Death According to the
Occurrence of Hypoglycemia on 1 Day or
More Than 1 Day and Receipt or Nonreceipt of
Insulin Therapy at the Time of the First Hypoglycemic
Episode.
The NICE-SUGAR Study Investigators. N Engl J Med 2012;367:1108-1118
2015 Inpatient Glucose Goals
Organization ICU Non-ICU Pre-prandial Non-ICU Maximum
AACE/ACE 140-180 mg/dl <140 mg/dl 180 mg/dl
ADA 140-180 mg/dl <140 mg/dl 180 mg/dl
ACP 140-200 mg/dl Avoid <140 mg/dl
Endocrine Society <140 mg/dl 180 mg/dl
Society of Critical
Care Medicine100-150 mg/dl
UCSF 100-160 mg/dl 100-180 mg/dl
Blood Glucose Levels During Isulin Treatment
Days of Therapy
Blo
od g
luco
se (
mg/d
L)
100
120
140
160
180
200
220
240
A dm it 1 2 3 4 5 6 7 8 9 10
SSRI
Lantus + glulisine
Mean Blood Glucose Levels During Insulin Therapy
* p<0.01
¶ p<0.05
¶
* * *¶ ¶ ¶
Day 3: P=0.06
Umpierrez GE Et al. Diabetes Care. 2007;30:2181–2186.
How to Obtain “Tight” Control
�Bedside glucose monitoring
� IV insulin drips
�Diabetes Flow sheets
�Discourage the use of traditional
Sliding Scale insulin
INSULIN
SLIDING
SCALE

8/5/2015
6
INSULIN
SLIDING
SCALE
Roller Coaster Effect of Insulin Sliding Scale
Mr. And Mrs. XXXXX are admitted
for “Giants” fever.
Mr. XXXXX has Type 2 diabetes and
takes a total of 75 Units insulin per
day (2 shots). Glucoses at home are
“poorly controlled.”
Mrs. XXXXX also has Type 2 diabetes
but she has good control taking about
25 units of Lispro premeal and 40
Units glargine at night.
Fingerstick qid with regular insulin SQ
coverage:
FSBG Action
< 50 1 amp D50 iv and call HO
51-80 give juice and repeat in 0.5-1 hr
81-150 no coverage
151-200 2U regular insulin SQ
201-250 4U regular insulin SQ
251-300 6U regular insulin SQ
301-350 8U regular insulin SQ
351-400 10U regular insulin SQ
>400 12U regular insulin SQ, call HO
INSULIN
SLIDING
SCALE

8/5/2015
7
Jane Jeffrie Seley
DNP, MPH, GNP, BC-ADM, CDE, CDTC
Diabetes Nurse PractitionerInpatient Glycemic Control TeamNew York Presbyterian Hospital Weill Cornell Medical College New York, New York
Disclosures
Presenter: Jane Jeffrie Seley
Attended Advisory Board Meeting:
-Novo Nordisk March 2015
-Bayer Diabetes Care April 2015
-Sanofi Diabetes April 2015
Improving Insulin Safety
Creating and Implementing
Comprehensive Insulin Order Sets
Why Computerized Order Sets?
• Reduces insulin dosing errors: Auto-calculates safe dose
• Simplifies & promotes weight based dosing: Auto-populates weight into dosing algorithm
• Reduces insulin TYPE errors: basal, prandial and correction insulins are separated40
Why Computerized Order Sets (Cont.)? • Reduces clinical inertia: Takes fear out of
dosing insulin by automating process
• Reduces omission of doses and improper timing of BGM & insulin: e.g. RN gets
medication due reminder, Prescriber & RN get reminder of need for basal insulin for Type 1
patients
41
Secret to Success With Comprehensive
Pre-Selected Matters
Secret to Success: Pre-Checked Orders
8/5/2015
8
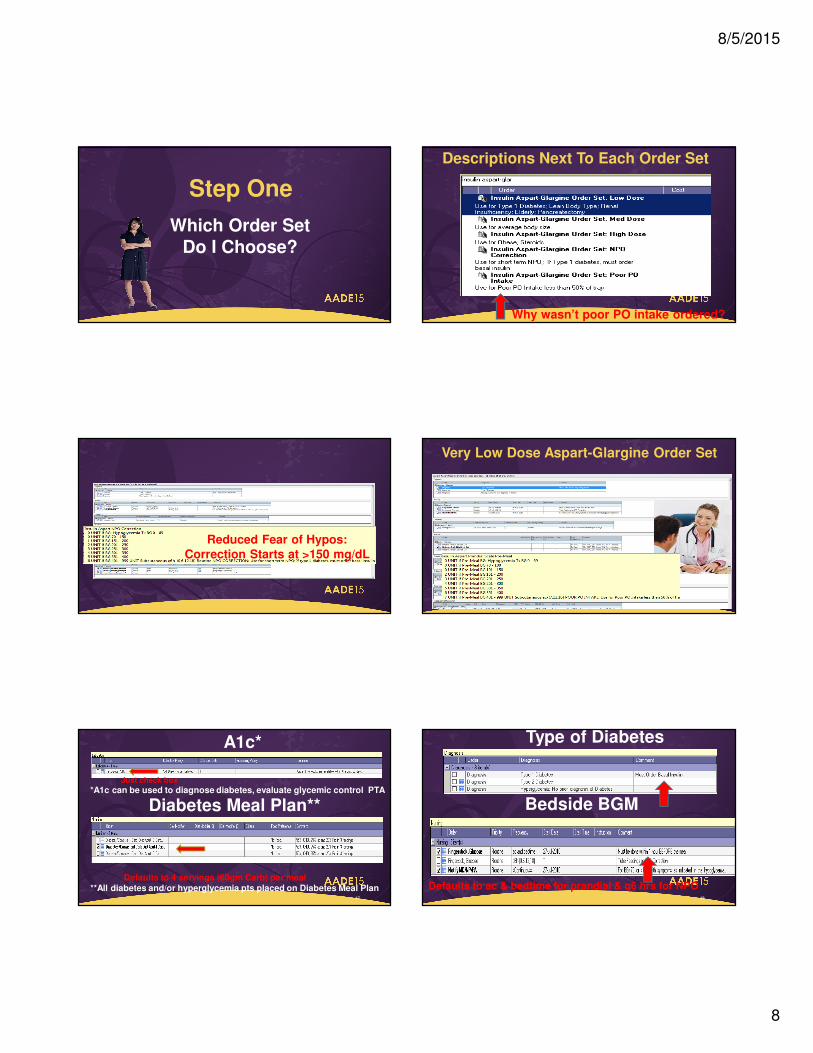
Step One
Which Order Set
Do I Choose?
Descriptions Next To Each Order Set
Why wasn’t poor PO intake ordered?
NPO Aspart Only Order Set
for short-term NPOReduced Fear of Hypos:
Correction Starts at >150 mg/dL
Very Low Dose Aspart-Glargine Order Set
Diabetes Meal Plan**
47
Defaults to 4 servings (60gm Carb) per meal**All diabetes and/or hyperglycemia pts placed on Diabetes Meal Plan
A1c*
*A1c can be used to diagnose diabetes, evaluate glycemic control PTAJust check box
Type of Diabetes
48
Bedside BGM
Defaults to ac & bedtime for prandial & q6 hrs for NPO

8/5/2015
9
49
NPO: no auto-basal for type 2
Very Low Dose .10 u/kg
Low Dose .15 u/kg
Med Dose .20 u/kg
High Dose .30 u/kg
Hypoglycemia Treatment
50
Diabetes Education
Diabetes Survival Skills
Pt Education: Focus on Survival Skills
Diabetes Teaching Resources
Consistent Carbohydrate Menu
Lists Serving Sizes & Grams! ! ! ! ! ! ! ! ! ! !
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
Graham Crackers (3 crackers) . . . . . . . . .
Plain Rice Cake (1 cake) . . . . . . . . . . . . . . . . . .
Pudding:
Vanilla (½ cup) . . . . . . . . . . . . . . . . . . . . . .. . . . .
Chocolate (½ cup) . . . . . . . . . . . . . . . . . . . . . .
Rice Pudding (½ cup) . . . . . . . . . . . . . .
Ice Cream:
Vanilla (½ cup) . . . . . . . . . . . . . . . . . . .. . . . . . .
Chocolate (½ cup) . . . . . . . . . . . . . . . .. . . . . . .
Jello/Gelatin:
Sugar Free Strawberry (~½ cup)………………..
Beverages
Skim, 2% or whole milk (8 oz). . . ……... .
Lactose Free milk (8 oz) . . . . . . . . . . . . . . . . . . .
Vanilla Soy milk (8 oz) . . . . . . . . . . . . . . . . . . . . .
Regular or Decaf Coffee/Tea (8 oz). . . . . . . . . . . . .
Diet Ginger Ale (8 oz) . . . . . . . . . . . . . . . .
!
!Condiments/Salad Dressing:
Smart Balance Butter Spread (1 tsp).. . . . . . . . .
Peanut Butter (1½ Tbsp) .. . . . . . . . . . . . . . . .. . . . .
Sugar Free Jelly (1 Tbsp) . . . . . . . . . . . . .
Sugar Free Syrup (2 Tbsp) . . . . . . . . . . . . . . . . . . . .
Lemon Juice (1 packet) . . . . . . . . . . . . . . .
Ketchup (1 Tbsp) . . . . . . . . . . . . . . . . . . . . .
Fat-Free Mayo (1 Tbsp) . . . . . . . . . . . . . . . ..
Mustard (1 packet) . . . . . . . . . . . . . . . . . . . .
Fat-Free Italian (1 Tbsp) . . . . . . . . . . . . . . . . . .. . . .
Creamy French (1 Tbsp) . . . . . . . . . . . . . . . . .. . .
.
!
Sample!Food!Label!!!
!Step 3!
Carbohydrate Grams
Carbohydrate Servings
5 – 10 ½
11 – 19 1
20 – 24 1 ½
25 – 34 2
35 – 44 2 ½
45 – 49 3
50 – 55 3 ½
56 – 64 4
17
7
22
24
24
27
32
2
11
13
18
0
0
0
4
6
3
0
2
1
0
1
2
1
½
1½
1½
1½
2
2
0
1
1
1
0
0
0
0
½
0
0
0
0
0
0
0
Step!1!
Step!2!

8/5/2015
10
Teaching Patients to Use Insulin Pen Diabetes Education
Documentation
Diabetes Champions
• Meets Monthly (1 hr)
& Annually (8 hr)
• Email reminders sent to
all RNs, NPs, RDs
• Created TEAM WEB
with educational
resources for pts &
professionals
Developing & Implementing
Glycemic Control Guidelines
Adult Inpatient
Glycemic
Management
Guideline
Pocket Card
Page 1
Insulin Titration Algorithm
60
WHICH INSULIN NEEDS ADJUSTMENT:
If AM fasting BG is
too high or low:Adjust Glargine
If pre-lunch, pre-dinner or
bedtime is too high or low:Adjust Aspart
HOW TO ADJUST:
If BG is less than 50:
If BG is less than 70:
Deduct 50%
Deduct 20%
If BG is 70-100: Deduct 10%
If BG is 180-250:
If BG is >250:
Add 10%
Add 20%

8/5/2015
11
Inpatient Guideline Pocket Card (P2) Inpatient Guideline Pocket Card (P3)
Inpatient Guideline
Pocket Card (P4)
Data VISPattern Management Tool
Online Mandatory Education
by Discipline:Dietitians
NursesPharmacists
Prescribers (NPs, PAs)
References• American Diabetes Association (2015). Standards of Medical Care In Diabetes-
2015. Diabetes Care: 38(1):1-86.
• Draznin, B., Gilden, J., et al (2013). Pathways to quality inpatient management of
hyperglycemia and diabetes: A call to action. Diabetes Care; 36(7):1807-14.
• Flory, J.H., Aleman, J.O., Furst, J., & Seley, J.J. (2014). Basal Insulin Use in the
Non-Critical Care Setting: Is Fasting Hypoglycemia Inevitable or Preventable? J.
Diabetes Sci. Technology, J Diabetes Sci Technol; 8(2):427-428.
• Rodriguez, A., Magee, M. et al (2014). Best Practices for Interdisciplinary Care
Management by Hospital Glycemic Teams: Results of a Society of Hospital Medicine Survey Among 19 US Hospitals. Diabetes Spectrum; 27(3), 197-205.
• Rushakoff, R., et al (2014). Using a Mentoring Approach to implement an Inpatient
Glycemic Control Program in Unites States Hospitals. Healthcare; 2 (2014). Pp 205-
210.

8/5/2015
12
References (Cont.)
• Ryan, D., Swift, C., (2014). The Mealtime Challenge: Nutrition and Glycemic
Control In the Hospital. Diabetes Spectrum; 27 (3). Pp 163-168.
• Mendez, C. Umpierrez, G.E. (2014). Pharmacotherapy for hyperglycemia in
Noncritically Ill Hospitalized Patients. Diabetes Spectrum; 27 (3). Pp 180-188.
• Seley, J.J. (2015, In Press). Diabetes Care in the Inpatient Setting, in Complete
Nurse's Guide to Diabetes Care (3rd ed.), Childs, B.P., Cypress, M., & Spollett, G. (Eds): American Diabetes Association, Alexandria, VA.
• Umpierrez GE, Hellman R et al (2012). Management of hyperglycemia in
hospitalized patients in non-critical care setting: an endocrine society clinical
practice guideline. Endocrine Society. J Clin Enddocrinol Metab. Jan;97(1):16-
38.
UCSF Inpatient Diabetes
• Infrastructure
– 1989: Bedside Glucose Monitoring
– 1990: IV insulin order set
– Mid 1990s SQ Insulin Order sets
– 1999: intranet education
– 2004: Mandatory use of New insulin order sets
– 2004: New mandatory nursing (online) and Physician
education (online and small group case based)
– 2012: Inpatient EMR for orders (EPIC)
Insulin Order Forms• Adult
– DKA– Adult SQ Insulin – Patient
eating
– Adult SQ Insulin – NPO, TPN, Tube Feeding
– IV insulin – ICU protocol– IV insulin – Med-Surgical Unit
protocol
– Adult Insulin pump• Patient waver form
– Adult SQ insulin algorithm for NPO patients**
– CV Surgery Specific orders• PREO-OP Pathway**
• OB-GYN
– SQ Insulin – Patient eating
– IV Insulin form - delivery
– Pump Form• Pump waiver form
• Pediatrics
– SQ Insulin – Patient eating
– Pump Form• Pump waiver
– DKA
– IV insulin
Therapeutic Inertia
• Glucoses Better
• Low rate of hypoglycemia
• Nevertheless, our audits continued to show inappropriate initial insulin orders and therapeutic inertia for both attending staff and housestaff, with required insulin order changes not being made on a daily basis.
Therapeutic Inertia
• Physician Education
• Daily High Glucose Report– Nurse to check in on patients with very high glucoses
• Diabetes team for patients with high glucoses– Physician
– Nurse
– Pharmacist
• Diabetes Team for All Patients– Physician
– Nurse
– Pharmacist
General Resident Education
• residents may gain confidence about their knowledge and feel more at ease with
inpatient glucose management, but significant improvements in management
have generally not occurred.
8/5/2015
13
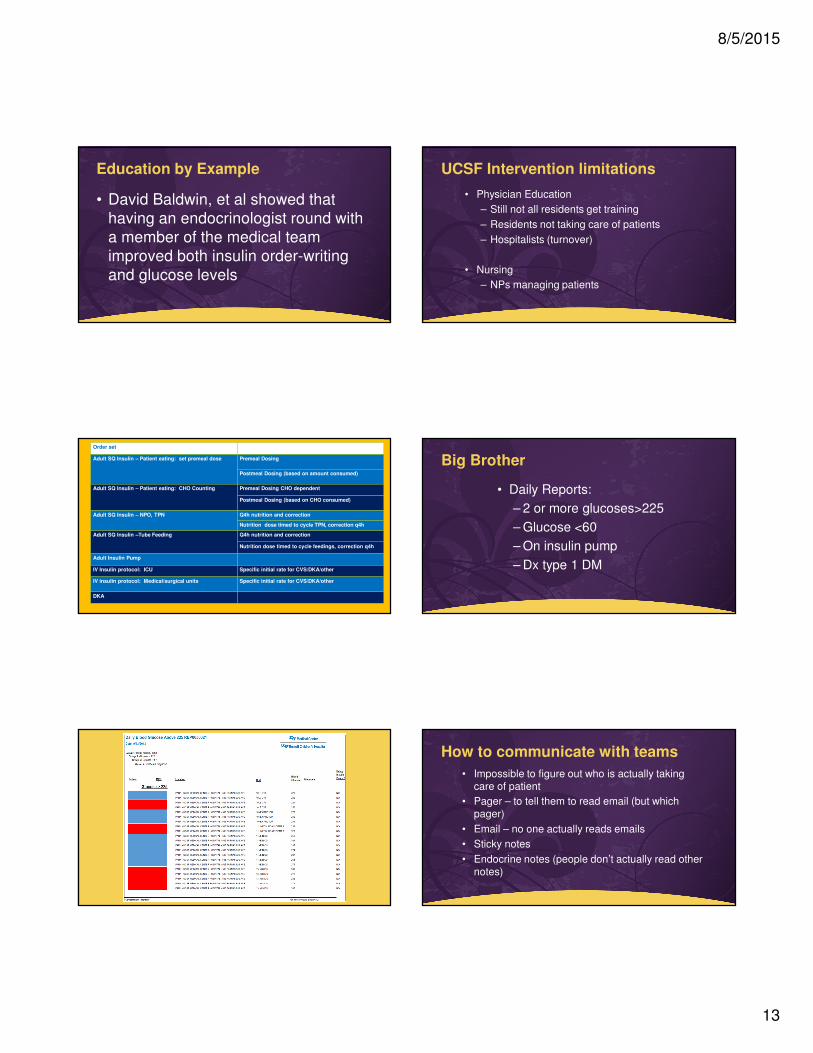
Education by Example
• David Baldwin, et al showed that
having an endocrinologist round with
a member of the medical team
improved both insulin order-writing
and glucose levels
UCSF Intervention limitations
• Physician Education
– Still not all residents get training
– Residents not taking care of patients
– Hospitalists (turnover)
• Nursing
– NPs managing patients
Order set
Adult SQ Insulin – Patient eating: set premeal dose Premeal Dosing
Postmeal Dosing (based on amount consumed)
Adult SQ Insulin – Patient eating: CHO Counting Premeal Dosing CHO dependent
Postmeal Dosing (based on CHO consumed)
Adult SQ Insulin – NPO, TPN Q4h nutrition and correction
Nutrition dose timed to cycle TPN, correction q4h
Adult SQ Insulin –Tube Feeding Q4h nutrition and correction
Nutrition dose timed to cycle feedings, correction q4h
Adult Insulin Pump
IV Insulin protocol: ICU Specific initial rate for CVS/DKA/other
IV insulin protocol: Medical/surgical units Specific initial rate for CVS/DKA/other
DKA
Big Brother
• Daily Reports:
– 2 or more glucoses>225
– Glucose <60
– On insulin pump
– Dx type 1 DM
How to communicate with teams
• Impossible to figure out who is actually taking care of patient
• Pager – to tell them to read email (but which pager)
• Email – no one actually reads emails
• Sticky notes
• Endocrine notes (people don’t actually read other notes)

8/5/2015
14
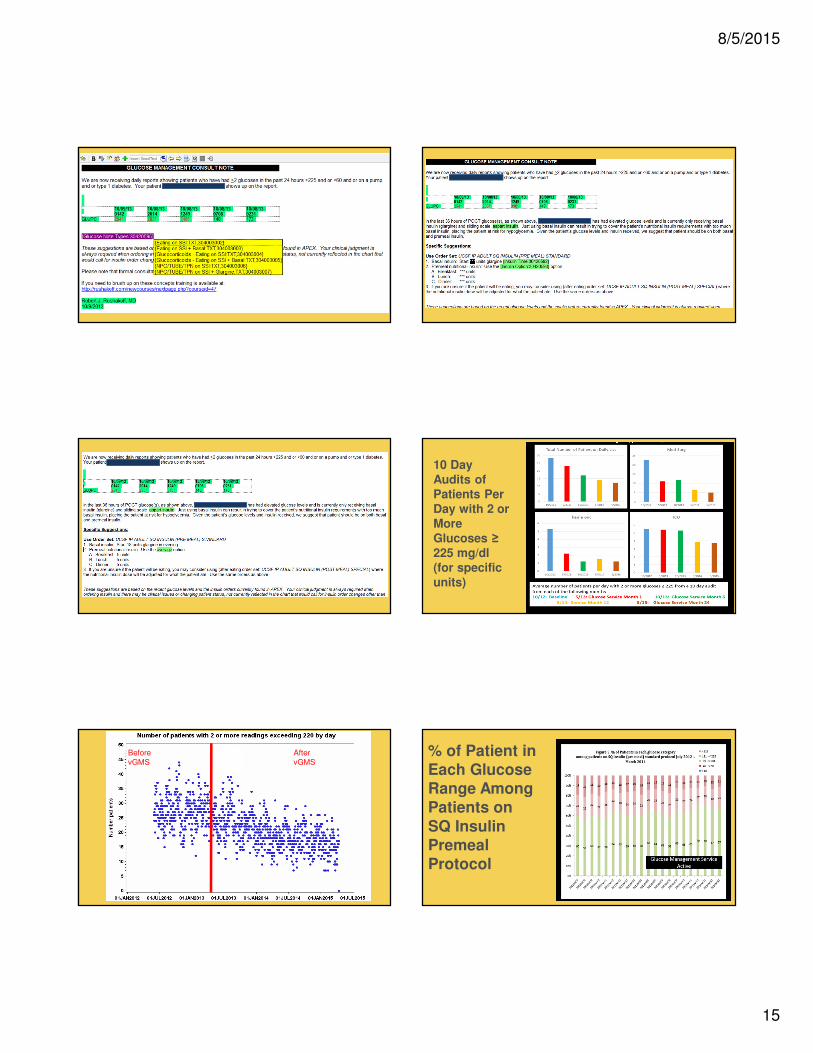
Inpatient Hyperglycemia
The virtual Inpatient Glucose Management Service
8/5/2015
15
10 Day
Audits of
Patients Per
Day with 2 or
More
Glucoses ≥
225 mg/dl
(for specific
units)
Before
vGMS
After
vGMS% of Patient in
Each Glucose
Range Among
Patients on
SQ Insulin
Premeal
Protocol
8/5/2015
16
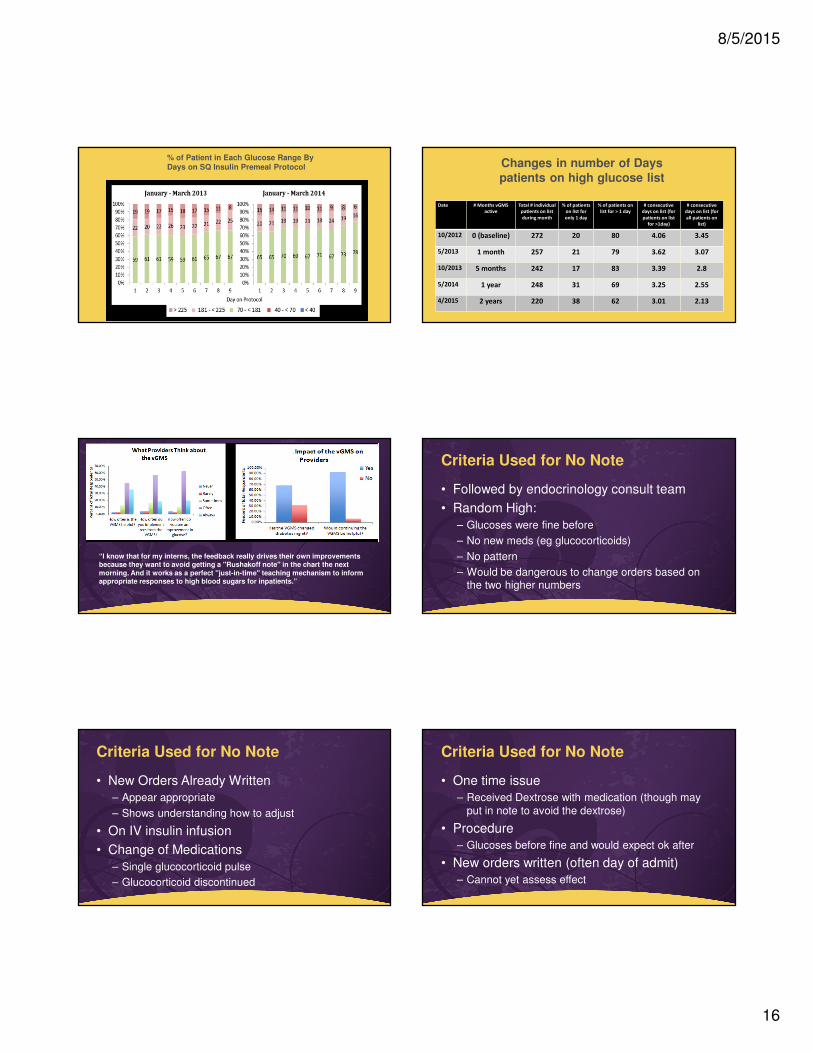
% of Patient in Each Glucose Range By
Days on SQ Insulin Premeal Protocol
Date # Months vGMS
active
Total # individual
patients on list
during month
% of patients
on list for
only 1 day
% of patients on
list for > 1 day
# consecutive
days on list (for
patients on list
for >1day)
# consecutive
days on list (for
all patients on
list)
10/2012 0 (baseline) 272 20 80 4.06 3.45
5/2013 1 month 257 21 79 3.62 3.07
10/2013 5 months 242 17 83 3.39 2.8
5/2014 1 year 248 31 69 3.25 2.55
4/2015 2 years 220 38 62 3.01 2.13
Changes in number of Days
patients on high glucose list
“I know that for my interns, the feedback really drives their own improvements because they want to avoid getting a "Rushakoff note" in the chart the next
morning. And it works as a perfect "just-in-time" teaching mechanism to inform appropriate responses to high blood sugars for inpatients.”
Criteria Used for No Note
• Followed by endocrinology consult team
• Random High:
– Glucoses were fine before
– No new meds (eg glucocorticoids)
– No pattern
– Would be dangerous to change orders based on the two higher numbers
Criteria Used for No Note
• New Orders Already Written
– Appear appropriate
– Shows understanding how to adjust
• On IV insulin infusion
• Change of Medications
– Single glucocorticoid pulse
– Glucocorticoid discontinued
Criteria Used for No Note
• One time issue
– Received Dextrose with medication (though may
put in note to avoid the dextrose)
• Procedure
– Glucoses before fine and would expect ok after
• New orders written (often day of admit)
– Cannot yet assess effect

8/5/2015
17
The numbers
• Number of vGMS notes in past 2 years:
3400
• Time to complete task:
30-45 minutes
• Change in number of Formal Endocrinology Consults:
none
• Physicians– Robert Rushakoff
– Umesh Masharani
– Melissa Weinberg
– Sarah Kim
– Aaron Neinstein
– Bonnie Kimmel
– Saleh Adi
– Stephen Gitelman
– Jan Hirsch
– Kathryn Rouine-
Rapp
– David Robinowitz
– Michael Hwa
– Heather Nye
– Steve Pantilat
• Pharmacists– Heidemarie
Windham
– Lisa Kroon
– Kethen So
– Thomas Bookwalter
– Anna Seto
– Yali Brennan
• Administration– Rosanne
Rappazini
– Jennifer Pacholuk
– Joy Pao
– Janice Hull
� Nurses� Mary Sullivan
� Pauline Chin
� Marlene Bedrich
� Craig Johnson
� Molly Killion
� Jeanne Buchanan
� Noraliza Salazar
� Lynn Dow
� Byanqa Robinson
� Dietary� Marian Devereaux
� Ami Bhow
PEOPLE CHANGING INPATIENT DM MANAGEMENT AT UCSF
Community Hospital Training
Annenberg Project
Rushakoff RJ, Sullivan MM, Seley JJ, Sadhu A, O'Malley CW, Manchester C, Peterson E, Rogers KM. Using a Mentoring Approach to Implement an Inpatient Glycemic Control Program in United States
Hospitals. Health Care: The Journal of Delivery Science and Innovation Volume 2, Issue 3, September
2014, Pages 205–210
Physicians
• Robert J. Rushakoff, MDDirector Inpatient Diabetes, UCSF
• Cheryl W. O’Malley, MDProgram Director, Internal Medicine Banner Good Samaritan
Medical, Phoenix, Arizona
• Kendall M. Rogers, MDChief, Hospital Medicine University of New Mexico Health Sciences Center
Albuquerque, New Mexico
• Archana Sadhu, MD Director, Inpatient Diabetes Program, The Methodist Hospital System Houston,
Texas
Diabetes Educators
• Carol Manchester, MSN, ACNS, BC-ADM, CDEUniversity of Minnesota Medical Center, Minneapolis, Minnesota
• Jane Jeffrie Seley, DNP, MPH, BC-ADM, CDENew York Presbyterian/Weill Cornell Medical Center
• Mary M. Sullivan, RN, DNP, ANP-BC, CDEUniversity of California, San Francisco
• Eric D. Peterson, EdM, FACMEAnnenberg Center for Health Sciences at Eisenhower
8/5/2015
18
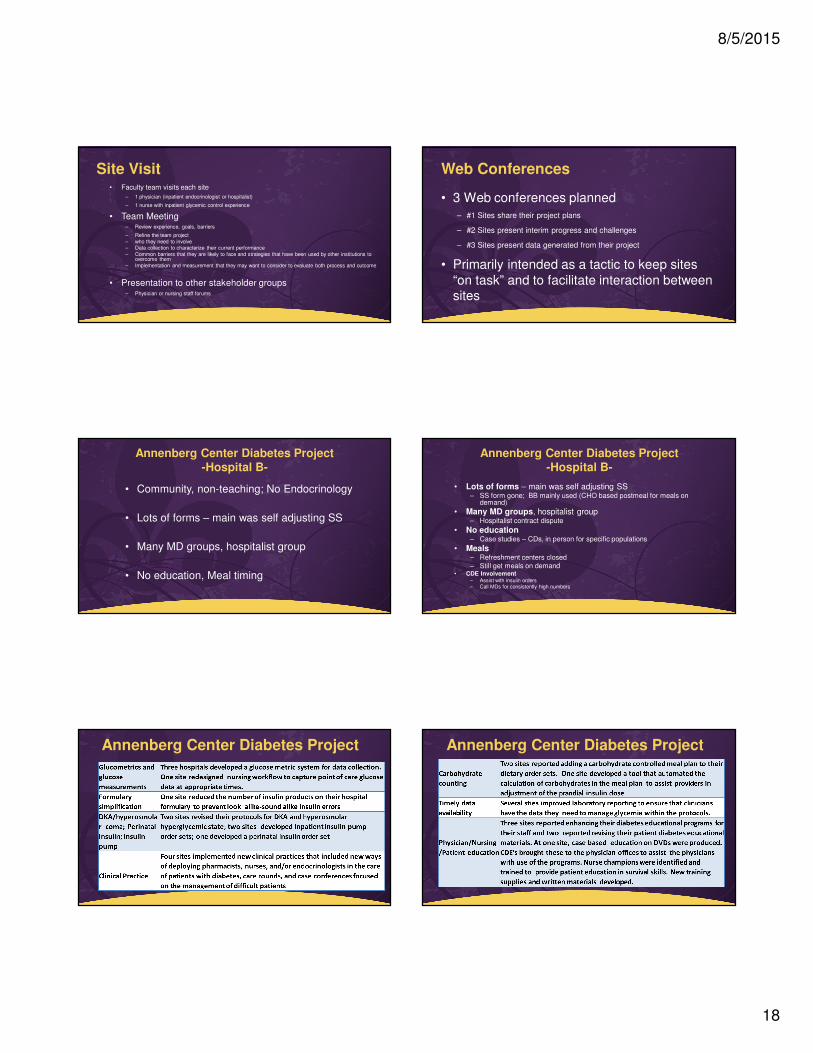
Site Visit• Faculty team visits each site
– 1 physician (inpatient endocrinologist or hospitalist)
– 1 nurse with inpatient glycemic control experience
• Team Meeting– Review experience, goals, barriers
– Refine the team project
– who they need to involve– Data collection to characterize their current performance
– Common barriers that they are likely to face and strategies that have been used by other institutions to overcome them
– Implementation and measurement that they may want to consider to evaluate both process and outcome
• Presentation to other stakeholder groups– Physician or nursing staff forums
Web Conferences
• 3 Web conferences planned
– #1 Sites share their project plans
– #2 Sites present interim progress and challenges
– #3 Sites present data generated from their project
• Primarily intended as a tactic to keep sites
“on task” and to facilitate interaction between sites
Annenberg Center Diabetes Project-Hospital B-
• Community, non-teaching; No Endocrinology
• Lots of forms – main was self adjusting SS
• Many MD groups, hospitalist group
• No education, Meal timing
Annenberg Center Diabetes Project-Hospital B-
• Lots of forms – main was self adjusting SS– SS form gone; BB mainly used (CHO based postmeal for meals on
demand)
• Many MD groups, hospitalist group– Hospitalist contract dispute
• No education– Case studies – CDs, in person for specific populations
• Meals– Refreshment centers closed
– Still get meals on demand• CDE Involvement
– Assist with insulin orders– Call MDs for consistently high numbers
Annenberg Center Diabetes Project Annenberg Center Diabetes Project

8/5/2015
19