innovative radiotherapy techniques time-driven … radiotherapy techniques time-driven...
TRANSCRIPT
© 2010 Universitair Ziekenhuis Gent
Innovative Radiotherapy Techniques
Time-Driven Activity-Based Costing
Yolande Lievens, MD, PhD
Radiation Oncology
University Hospital Gent
UNAMEC – November 5th 2014
the aim of radiotherapy:
improve local control, survival and quality of life
technologic advances:
equitoxic dose escalation vs. reduced side effects
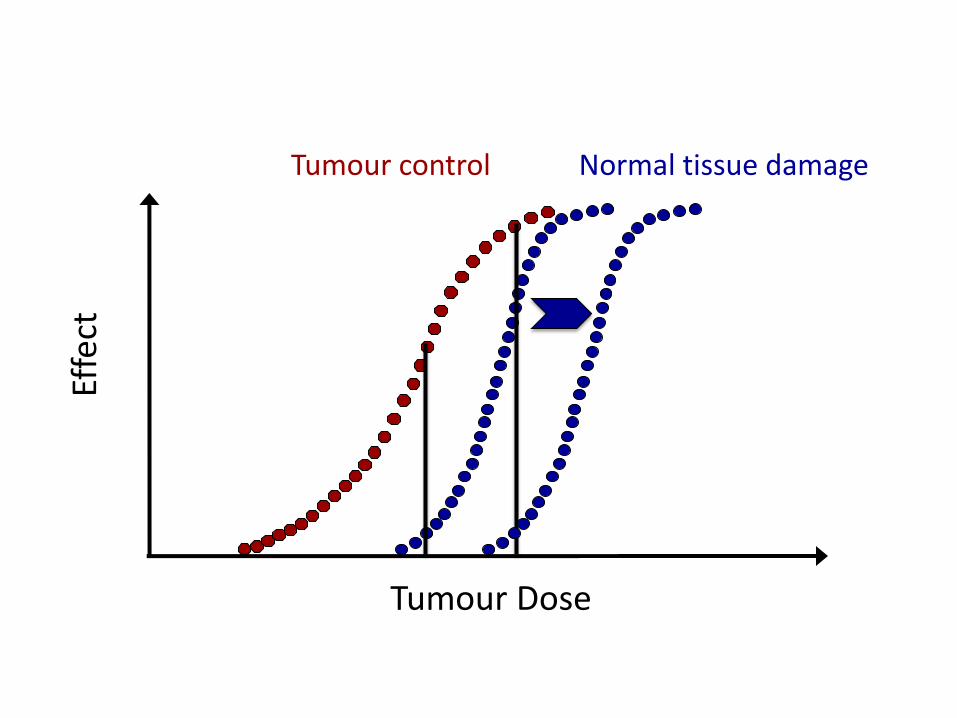
Tumour control
Effe
ct
Tumour Dose
Normal tissue damage

Dose escalation Increase the tumour dose
for the same dose to the healthy tissues
Decrease toxicity (ALARA) Reduce the dose to the healthy tissues
for the same tumour dose

2D RT 60Gy/2Gy
3D-CRT 66-70Gy/2Gy
IMRT >70Gy/2Gy
SBRT 60Gy/20Gy

Fang et al. IJROBP 2006 Lagerwaard et al. IJROBP 2008

Liao et al. IJROBP, 2009
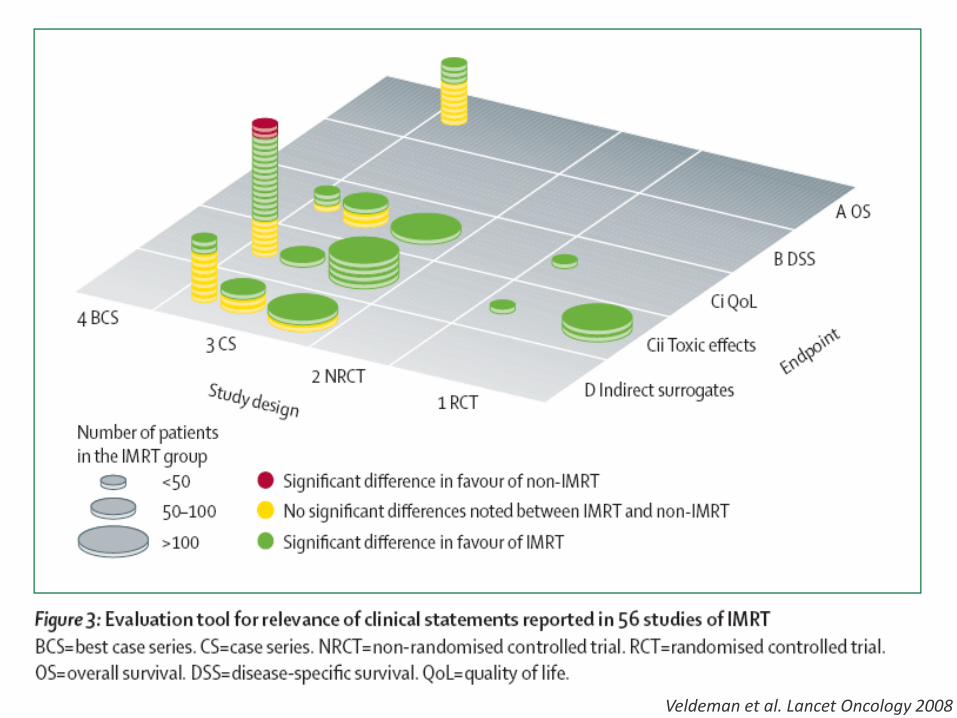
Veldeman et al. Lancet Oncology 2008

It’s always too early to evaluate a technology, until, suddenly, it’s too late!
Buxton’s Law

development RCT unethical? Widespread use still avoidable?
Effectiveness?
exte
nt
clin
ical
use
t premarket emerging diffusing established obsolete
Perform
ance &
safety
Co
st calculatio
n?
CEA
- BIA
investment
Fin
anci
ng
in silico studies Phase I-II
in selected centres
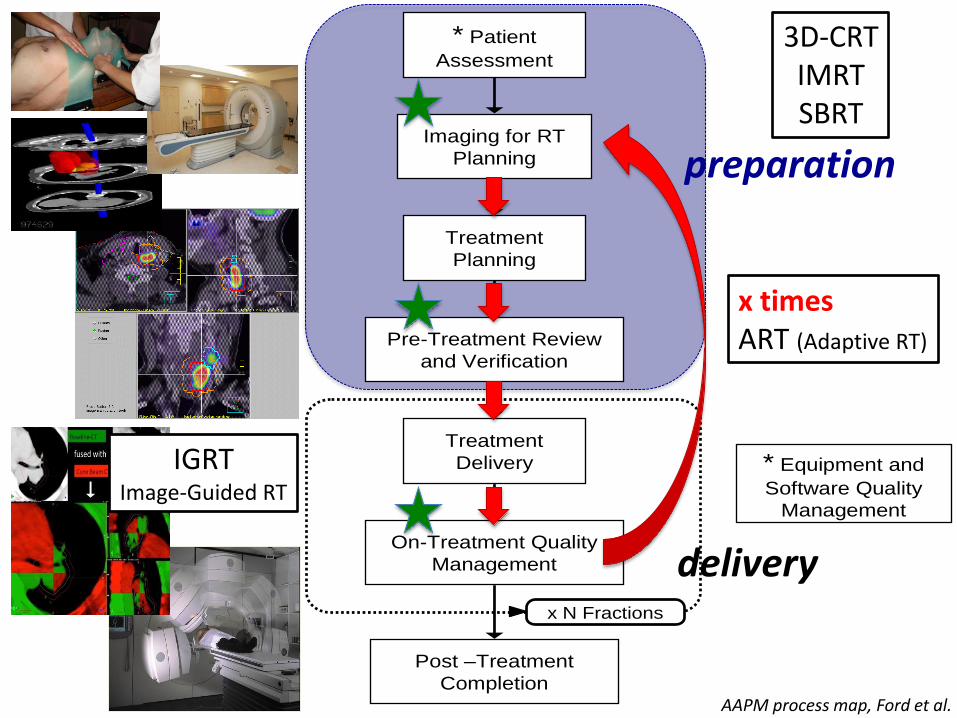
* Patient
Assessment
Imaging for RT
Planning
Treatment
Planning
Pre-Treatment Review
and Verification
Treatment
Delivery
Post –Treatment
Completion
On-Treatment Quality
Management
* Equipment and
Software Quality
Management
x N Fractions
AAPM process map, Ford et al.
x times ART (Adaptive RT)
preparation
3D-CRT IMRT SBRT
delivery
IGRT Image-Guided RT

more complex treatments
more time
more resources capital investments
sophisticated equipment
buildings
human resources treatment
maintenance
more costly
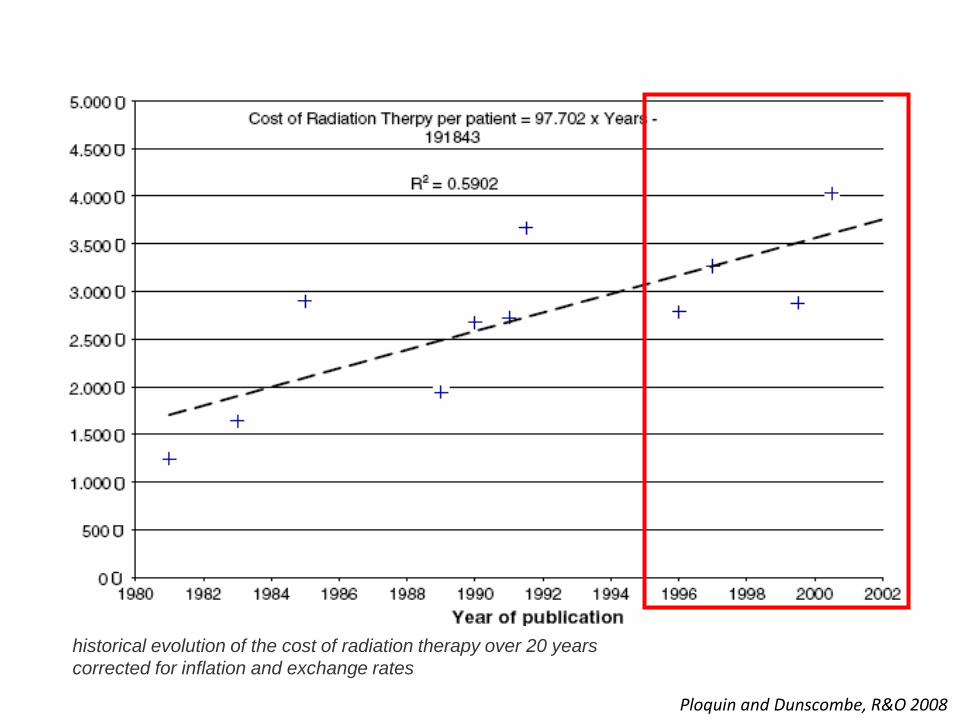
Ploquin and Dunscombe, R&O 2008
historical evolution of the cost of radiation therapy over 20 years
corrected for inflation and exchange rates

what we want for our patients
what society wants for all patients
maximise health within a given budget minimise cost per life year gained
early availability of new and promising treatments
high-tech, high cost, high reimbursements (?)
« The difference between the reimbursement in the United States and most European health care systems
has been proposed as a contributing factor in explaining the slower introduction of IMRT in European centres.
Although favourable reimbursement may ensure
cost-effectiveness from a departmental perspective, it clearly does not guarantee cost-effectiveness
from the society or the health service point of view. »
Bentzen IJROBP 2004

ideally reimbursement should
cover the costs adapt to technology evolution endorse quality account for effectiveness
Belgian radiotherapy reimbursement
no correlation to costs lags behind on technology evolution does not support quality is not related to effectiveness

Hulstaert et al, Rapport 198 KCE 2013

reimbursement for SBRT ?
what is
the (level 1) evidence?
the cost?
the value for money?
the budgetary impact?

coverage with evidence development
Innovative radiotherapy techniques
Define the indications
Define the costs to be covered
Define the evidence generation
Evidence generation and follow-up
In close collaboration with the radiotherapy departments
NIHDI
KCE
CR
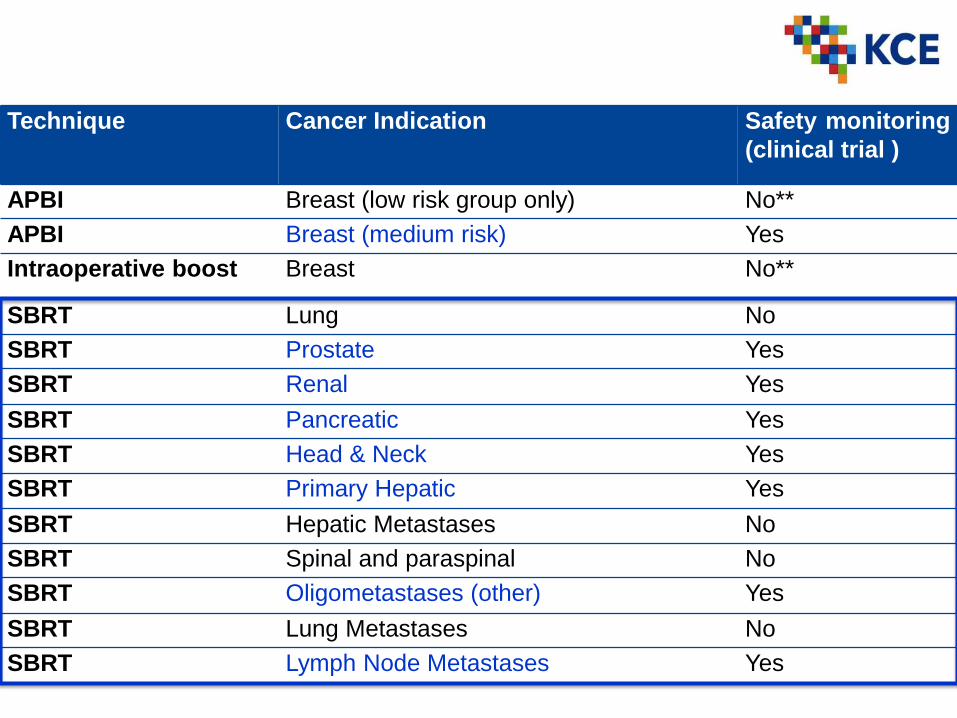
Technique Cancer Indication Safety monitoring
(clinical trial )
APBI Breast (low risk group only) No**
APBI Breast (medium risk) Yes
Intraoperative boost Breast No**
SBRT Lung No
SBRT Prostate Yes
SBRT Renal Yes
SBRT Pancreatic Yes
SBRT Head & Neck Yes
SBRT Primary Hepatic Yes
SBRT Hepatic Metastases No
SBRT Spinal and paraspinal No
SBRT Oligometastases (other) Yes
SBRT Lung Metastases No
SBRT Lymph Node Metastases Yes

Kaplan and Porter, Harvard Business Review 2011

microcosting
gross costing

time and motion studies
detailed resource use analysis
bottom up
sensitivity & precision
complexity & cost
total budget allocated
to specific services
top down
simplicity & low cost
lack of sensitivity
microcosting
gross costing

bottom up
top down

treatments
radiotherapy resources
personnel equipment buildings overhead
“1st stage cost drivers” “resource drivers”
e.g. time percentages
“2nd stage cost drivers” “activity drivers”
number of activities… time
direct allocation
indirect allocation using cost drivers
resource costs
cost-objects
activities
time-driven Activity-Based Costing
consumables

activities consume resources to produce products

Lievens et al. IJROBP, 2003 Van de Werf et al. R&O, 2012

Out of scope
Treatment cost
DIRECTINDIRECT
Personnel MaterialEquipment
RT patient related activities RT support act.
Intake consultation
Medical review
…
APBI -brachytherapy
SBRT – lung –5 fractions
…
Overhead
OtherEquipment
Maint. & QA
Material
Time driven
Activity consumption Per fraction
Non-RT, care
activities
Non- care activities
RT patient related
RT support
Mark-up % on
treatment cost
80% fraction
20% patient
56.6%
Hulstaert et al, Report 198 KCE 2013

0
2000
4000
6000
8000
10000
12000
14000
16000
3 4-6 7-10
Co
st
(€)
N of fractions
Free breathing - center A
Free breathing - center B
Free breathing - center C
Free breathing - center D
Free breathing - center E
Free breathing - center F
Gating - center G
Gating - center H
Tracking - center I
Tracking or Free breathing - center J
Hulstaert et al, Report 198 KCE 2013
average cost SBRT: 6,221€

Hulstaert et al, Report 198 KCE 2013
4-year provisional financing of SBRT
prospective evaluation
real-life setting
Which departments?
Which indications?
Which technology?
What standards of care?
What outcome?
What budget?

Hulstaert et al, Report 198 KCE 2013
7 304
5 116 5 134
6 378 6 400
7 289 7 522
8 418 8 519 8 701
9 561
-
1 000
2 000
3 000
4 000
5 000
6 000
7 000
8 000
9 000
10 000
Average A B C D E F G H I J
Co
st
per t
reatm
en
t (€)
Prostate IMRT 33-40 fractions

Hulstaert et al, Report 198 KCE 2013
-
500
1 000
1 500
2 000
2 500
3 000
3 500
4 000
4 500
A B C D E F G H I J
Eq
uip
me
nt
+ p
ers
on
ne
l c
os
t p
er
tre
atm
en
t (€
)
Average cost per process step for all external radiotherapy treatments
First patient contact Simulation Delineation Planning
Treatment delivery End of treatment Adaptative RT

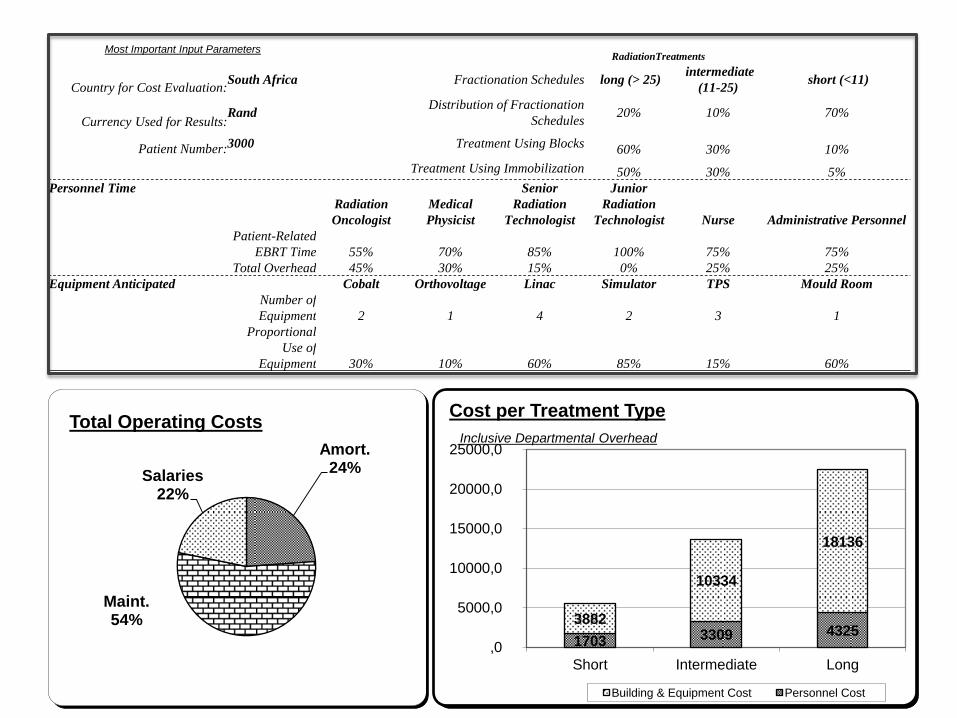
Most Important Input Parameters RadiationTreatments
Country for Cost Evaluation: South Africa Fractionation Schedules long (> 25)
intermediate
(11-25) short (<11)
Currency Used for Results: Rand
Distribution of Fractionation
Schedules 20% 10% 70%
Patient Number: 3000 Treatment Using Blocks 60% 30% 10%
Treatment Using Immobilization 50% 30% 5%
Personnel Time
Radiation
Oncologist
Medical
Physicist
Senior
Radiation
Technologist
Junior
Radiation
Technologist Nurse Administrative Personnel
Patient-Related
EBRT Time 55% 70% 85% 100% 75% 75%
Total Overhead 45% 30% 15% 0% 25% 25%
Equipment Anticipated Cobalt Orthovoltage Linac Simulator TPS Mould Room
Number of
Equipment 2 1 4 2 3 1
Proportional
Use of
Equipment 30% 10% 60% 85% 15% 60%
Amort. 24%
Maint. 54%
Salaries 22%
Total Operating Costs
1703 3309 4325 3882
10334
18136
,0
5000,0
10000,0
15000,0
20000,0
25000,0
Short Intermediate Long
Cost per Treatment Type
Inclusive Departmental Overhead
Building & Equipment Cost Personnel Cost

Most Important Input Parameters RadiationTreatments
Country for Cost Evaluation: South Africa Fractionation Schedules long (> 25)
intermediate
(11-25) short (<11)
Currency Used for Results: Rand
Distribution of Fractionation
Schedules 20% 10% 70%
Patient Number: 3000 Treatment Using Blocks 60% 30% 10%
Treatment Using Immobilization 50% 30% 5%
Personnel Time
Radiation
Oncologist
Medical
Physicist
Senior
Radiation
Technologist
Junior
Radiation
Technologist Nurse Administrative Personnel
Patient-Related
EBRT Time 55% 70% 85% 100% 75% 75%
Total Overhead 45% 30% 15% 0% 25% 25%
Equipment Anticipated Cobalt Orthovoltage Linac Simulator TPS Mould Room
Number of
Equipment 2 1 4 2 3 1
Proportional
Use of
Equipment 30% 10% 60% 85% 15% 60%
94% 89%
67%
98%
83% 93%
51% 62%
57%
98%
63% 70%
0%
20%
40%
60%
80%
100%
120%
Radiation Oncologist Medical Physicist Senior RadiationTechnologist
Junior RadiationTechnologist
Nurse AdministrativePersonnel
Personnel Utilization Total Time EBRT Time Only

AVAILABILITY equipment & staffing
guidelines reimbursement
NEEDS translation CCORE utilisation
to Europan countries
ACTIVITY-BASED COSTING at the national level
in European countries
ECONOMIC EVALUATION at the national level
in European countries HERO-project
National Societies
National Societies
CCORE
National Societies
CCORE
IAEA National Societies
ESTRO Clinical
Committee

a wider scope, the (near) future • Breast reconstruction techniques after mastectomy: description and costing of the medical subcomponents (HTA Study 2014-25)
• New Generation Sequencing panel tests in oncology
• Cost of medical imaging techniques (MRI/CT/… )
• …
adapt (part) of the nomenclature review hospital financing based on actual costs

Take-home messages Rapid evolution of radiotherapy, reimbursement inadequate Need for correct cost data, for reliable effectiveness data Coverage with evidence development TD-ABC used in several radiotherapy settings TD-ABC is a possible model to support market access of innovative medical technologies in Belgium

Thank you for your attention !
Thanks to
the Belgian Health Care Knowledge Centre Frank Hulstaert & Caroline Obyn Anne-Sophie Mertens & Dries Van Halewyck
the Belgian Cancer Registry and the RIZIV-INAMI
Jan Verstraete & Evelyn van de Werf Barbara Vanderstraeten
the IAEA Vic Levin, Branislav Jeremic, Eduardo Zubizerrato
the ESTRO-HEROes Cai Grau, Noémie Defourny, Peter Dunscombe & Chiara Gasparotto