inhaled corticosteroids in childhood asthma
TRANSCRIPT

Pediatr Drugs 2003; 5 (6): 351-361LEADING ARTICLE 1174-5878/03/0006-0351/$30.00/0
© Adis Data Information BV 2003. All rights reserved.
Inhaled Corticosteroids in Childhood AsthmaLong-Term Effects on Growth and Adrenocortical Function
Alessandro Salvatoni, Elena Piantanida, Luana Nosetti and Luigi Nespoli
Pediatric Clinic, University of Insubria, Varese, Italy
Inhaled corticosteroids (ICS) are the most potent of all the available inhaled treatments, and are effectiveAbstractmedications for long-term control of asthma. However, their use in children is limited by the risk of systemic
adverse effects. Although results reported in the literature on the adverse effects of ICS are conflicting and often
restricted to a small number of cases with a limited follow-up, most of them show an early decrease in growth
velocity without significant influence on final adult height. Partial adrenal suppression has also been demonstra-
ted in children treated with ICS for more than 2 months.
Only children with mild persistent, moderate, or severe asthma not controlled by non-corticosteroid drugs
should be treated with ICS for long periods. The dose of ICS must be individually adjusted to minimize the
possible adverse effects on growth, and all children with asthma receiving long-term treatment with ICS must be
regularly evaluated for growth impairment, which may necessitate dose reduction or drug replacement.
In recent years, a consensus has been achieved for controlling predict. The relationship of age at onset to prognosis is uncertain;
persistent asthma in childhood with the long-term treatment of most severely affected children have an onset of wheezing during
inhaled corticosteroids. Although the currently available inhaled the first year of life. These children may have growth retardation
corticosteroids should have minor systemic adverse effects, it is unrelated to corticosteroid treatment (although ultimate height
not yet well established whether long-term inhaled corticosteroid attainment is usually normal), chest deformity, and persistent
treatment could influence growth and adrenal function. In this abnormalities on pulmonary function testing.article we review the more recent papers on this topic. Manifestations of airway obstruction in asthma are a result of
bronchoconstriction, mucosal edema, cellular infiltration, and1. Asthma: Definition, Epidemiology
hypersecretion of mucus. These effects are a result of variousand Pathophysiology
allergic and nonspecific stimuli, including dust mites, pollens,
moulds, cockroach, cat or dog allergens, vegetable proteins, viralAsthma is defined as a ‘chronic, diffuse, inflammatory disorderinfections, cigarettes, air pollutants, cold air, exercise, etc.of the airways characterized by recurrent episodes of wheezing,
breathlessness, chest tightness, and coughing, associated with All these different stimuli can lead to the release of differentobstruction and hyperactivity of the airways to various stimuli, and types of mediators from local mucosal mast cells, i.e. histamine,a high degree of reversibility of the obstructive process’.[1] leukotrienes C4, D4 and E4, and platelet-activating factors that
Recent epidemiologic studies performed in the US and differ- initiate bronchoconstriction, edema, and immune response. The
ent European countries by the Centers for Disease Control and early immune response results in bronchoconstriction, is treatable
Prevention, document an increasing rate of asthma in the last 20 with β2-adrenoreceptor agonists, and may be preventable by mast
years.[2] Eighty to 90% of all cases of asthma are diagnosed by the cell-stabilizing agents (sodium cromoglycate or nedocromil). The
age of 6 years.[3] The course and severity of asthma are difficult to late inflammatory reaction, occurring 6–8 hours later, is character-

352 Salvatoni et al.
ized by eosinophilic and neutrophilic infiltration and airway 2.2 Pharmacodynamic and Pharmacokinetic Properties
hyper-responsiveness. This process can be treated and prevented
by corticosteroids, or prevented by sodium cromoglycate, Pharmacodynamic and pharmacokinetic properties of cortico-nedocromil or leukotriene inhibitors. Taking into account these steroids are largely dependent on their chemical and physicalconsiderations, treatment should be targeted to interrupt the pro- properties. They must have great receptor affinity, high anti-cess that leads to the activation of the immune system and prevents inflammatory action and, for the swallowed part of the drug, afunctional changes. rapid first-pass hepatic metabolism, to avoid high systemic bio-
Anti-inflammatory drugs are used for the long-term treatment availability.[7]
of mild persistent asthma. In particular, inhaled corticosteroidsOne of the most important aspects to be considered is their
(ICS) are the most potent of all the available inhaled treatments,lipophilic property. In fact, lipophilicity influences the rate of
and are consistently effective medications for long-term control ofabsorption in the lung. Fluticasone propionate and beclometha-
asthma (see table I).[4]
sone (the most lipophilic agents) have a distribution time of
several hours, while budesonide and flunisolide have a distribution2. Inhaled Corticosteroid (ICS) Therapytime of just several minutes. The latter also have a large volume of
The increased recognition of the important role of inflamma- distribution at steady-state. It has been postulated that lipophiliction in asthma, and the efficacy of corticosteroids in reducing agents can adhere better to the mucosa of the airways and prolonginflammation, has led to increased use of corticosteroids in the their topical action, reducing their systemic bioavailability andearly treatment of asthma. increasing their anti-inflammatory action.[8] Of course, because of
their lipophilicity and prolonged elimination half-life, lipophilic2.1 Mechanism of Action
agents may have increased systemic adverse effects, and for this
reason, the general approach is to use lower doses of the moreCorticosteroids have been shown to reduce airway hyper-re-lipophilic and more potent ICS.[9] Systemic bioavailability is thesponsiveness, improve lung function and asthma symptoms, andsum of inhaled drug absorbed across the airway mucosa and thereduce structural changes in the airways.[6] Corticosteroids act byswallowed part that escapes hepatic inactivation. A consistent partcontrolling the synthesis of several proteins. They act at specificof the portion of ICS deposited in the lung, ranging from 10–50%,receptors, localized in the cytoplasm of sensitive cells of variousis absorbed in the systemic circulation, the remaining 50–90%tissues, and form a corticosteroid-receptor complex. This complexbeing swallowed and absorbed at the gastrointestinal level. Thisthen undergoes modification and moves into the nucleus, where it
percentage may be greater in children because of the greaterbinds with chromatin and enhances specific gene transcription (see
proportion of drug swallowed, and is responsible for variablefigure 1).
Table I. Classifications of asthma severity and suggested treatment for long-term control[5]
Severity of asthma Symptoms Long-term control
Step 1: Mild intermittent Symptoms ≤2 times a week Not needed
Night-time symptoms ≤2 times a month
Step 2: Mild persistent Symptoms more than twice a week, but less than Sodium cromoglycate or nedocromil
once a day Either ICS (low dose) or montelukast (patients ≥6yrs
Night-time symptoms more than twice a month of age)
Step 3: Moderate persistent Daily, with exacerbations two or more times a week ICS (medium to high dose) + long-acting inhaled
Limited physical activity during exacerbations β2-agonists (for night-time control of symptoms)
Night-time symptoms more than once a week
Step 4: Severe persistent Continual, with limited physical activity ICS (high dose), and long-acting inhaled β2-agonists
Frequent and corticosteroid tablets (make repeated attempts to
maintain control with high dose ICS)
ICS = inhaled corticosteroids.
© Adis Data Information BV 2003. All rights reserved. Pediatr Drugs 2003; 5 (6)

Inhaled Corticosteroids: Growth and Adrenal Function 353
device used. This variation can be much smaller for the less potent
ICS, with higher oral and lower pulmonary availability. However,
it must be pointed out that in young children, independent of the
inhalation device, the proportion of the drug that is actually
inhaled is always smaller than in adolescents and adults. A further
factor influencing the proportion of the drug inhaled is obviously
the severity of the bronchial constriction.
2.3 Adverse Effects
When oral corticosteroids were first used in the treatment of
asthma in 1949–1950, long-term therapy resulted in adverse ef-
fects similar to those observed by Cushing in 1932. They could
suppress the hypothalamic-pituitary-adrenal (HPA) axis, and of
particular concern was the potential for growth retardation in those
children who received long-term corticosteroid therapy. It is worth
noting that, following this concern, the US FDA now requires
warning labels on the potential reduction in linear growth in
children treated with inhaled and intranasal corticosteroids.
ICS, a new class of drug with a rapid first-pass hepatic metabol-
ism, were introduced to avoid the adverse effects of long-term oral
corticosteroid treatment. They displayed more topical efficacy,
and were effective in the treatment of childhood asthma. However,
DNA
R
CS
CSRR
CS
hsp90
hsp9
0
mRNA
Protein
Fig. 1. Mechanism of action of corticosteroids. Binding of corticosteroids totheir receptor causes a dissociation of a phosphorylated protein of 90 kDain the citosol. This protein has been identified as a heat-shock protein(hsp90). It is presumed that the release of this protein plays an importantpart in the transformation of the receptor, enabling the hormone-receptorcomplex to proceed to its nuclear destination and interact with DNA. Hor-mone binding to the receptor induces dissociation of hsp90 from the recep-tor, causing a conformational (allosteric) change in the molecule whichallows DNA binding, gene activation, and mRNA transcription. The anti-inflammatory action of corticosteroids is mediated by down- or up-regula-tion of the synthesis of different proteins in different tissues. This is amultiform action, involving both inhibition of specific chemical mediators(enzymes, cytokines, adhesion proteins, regulation proteins) and modula-tion of the inflammation cell component. CS = corticosteroid; mRNA =messenger RNA; R = receptor.
systemic effects are also described for ICS, because of the system-
ically absorbed portion.[15] Thus, despite these remarkable bene-systemic effects resulting from differences in first-pass hepaticfits, there are also risks and adverse reactions,[9] which are dose-inactivation.dependent. Generally, a good therapeutic response in children can
There are many differences in bioavailability and lipophilicitybe achieved with beclomethasone dosages of 200–400 μg/day in a
among corticosteroids.[10] In the liver, fluticasone propionate istwice daily dosage regimen. However, sometimes children may
inactivated approximately 99%, budesonide 90%, and triamci-require higher dosages to better control severe symptoms. Adverse
nolone 80%, while beclomethasone dipropionate is not completely effects seem to be more likely with dosages of beclomethasoneinactivated in the hepatic first pass (60–70%), and an active ≥400 μg/day.[16]
metabolite is formed that has a similar potency.[11] Although the Different inhalation techniques (such as chambers, inhalers, orpotent ICS fluticasone propionate seems to have a superior tolera- spacers) can influence the portion of inhaled drug, and thusbility profile because of strong hepatic inactivation, the proportion systemic bioavailability. A further variable, which can influenceof drug absorbed from the lung can cause significant systemic the pulmonary and systemic bioavailability of ICS, is the gradualeffects. The potency, half-life, oral, and pulmonary availability, replacement of metered-dose inhalers containing chlorofluoro-and inhaled proportion by different devices of the most common carbons (CFC) with CFC-free preparations.[17]
ICS have been reported in table II. An ICS with a very low oral The studies on adverse effects of ICS on growth report conflict-availability and very high potency and pulmonary availability, ing results. Therefore, this is still an open point of discussion, alsosuch as fluticasone propionate, may have a wide variation in its considering that there is a tendency towards early and long-term
systemic availability, depending on the efficiency of the inhalation use of ICS in the treatment of asthma.
© Adis Data Information BV 2003. All rights reserved. Pediatr Drugs 2003; 5 (6)

354 Salvatoni et al.
3.2 Effects of Asthma on Growth
Before considering whether or not ICS affect growth, several
aspects must be considered. To begin with, children with asthma
have been reported to have shorter stature, smaller increase in
height for age (slower height velocity), and a different pattern of
growth, than children without asthma, irrespective of the use of
corticosteroids. The first studies showing the different growth
pattern in children with severe asthma were published approxi-
mately 50 years ago.[21] Several factors are probably responsible
for growth failure, i.e. chronic hypoxia, recurrent infections lead-
ing to under-nutrition and dystrophy, impaired lung function, and
probably also sleep disturbances and long-term stress. In children
with asthma, growth retardation is usually associated with delayed
sexual and skeletal maturation.
Tinan and Russell[22] showed that in children with asthma not
treated with corticosteroids, height is strictly related to lung func-
tion and the severity of the disease. However, in 1997 Silverstein
et al.[15] retrospectively studied a cohort of 153 patients with
asthma who had attained their adult height. The height of these
patients was not statistically different from that of non-asthmatic
people, suggesting that, overall, asthma does not have an impor-
tant effect on attained adult height.
This aspect is extremely important and more studies need to be
conducted because it can be a confounding factor when analyzing
the effect of ICS on final height.
Table II. Comparison of the pharmacodynamic and pharmacokinetic
properties of the four most common inhaled corticosteroids[12-14]
Corticosteroid Potencya Type of device Half-life Oral
(h) availability
(%)
Beclomethasone 0.4 MDI 6.3–7.4 30–40
dipropionate
MDI + spacer
Nebulizer
Flunisolide 1.8 MDI 1.5–2 6.7–20
MDI + spacer
Nebulizer
Budesonide 9.4 MDI 2.3 10–11
MDI + spacer
DPIb
Nebulizer
Fluticasone 18 MDI 14.4 <1
propionate MDI + spacer
DPIc
Nebulizer
a Binding affinity to corticosteroid receptors in vitro relative to
dexamethasone.
b Turbohaler® (the use of tradenames is for product identification
purposes only and does not imply endorsement).
c Diskhaler®.
DPI = dry powder inhaler; MDI = metered-dose inhaler.
3.3 How Corticosteroids Influence Growth3. Growth
There are several pathways through which corticosteroid ex-
cess influences growth.3.1 Normal GrowthFirstly, it seems that corticosteroids directly influence GH
secretion by an increased hypothalamic somatostatin secretion thatThe normal height velocity pattern is characterized by a dra-
inhibits pituitary GH secretion. Corticosteroids most likely act bymatic fall in the first 2 years of life from 25 to 6 cm/year, and a
down-regulating the GH receptor and reducing insulin-like growthfurther sudden rise during puberty called ‘peak height velocity’ factor 1 activity through a modulation of insulin-binding protein.(PHV). Prepubertal growth is influenced by thyroid hormones and In addition, corticosteroids also interfere with other hormones;
they inhibit new connective tissue synthesis and reduce productiongrowth hormone (GH). The pubertal PHV is under the control of
of adrenal androgens, which enhance the GH action during asexual hormones, mainly estrogens, which stimulate GH secretion,growth spurt at puberty.[18]
and is particularly susceptible to the systemic effects of ICS whichAlthough the different mechanisms by which corticosteroids
interfere with pubertal hormonal changes.[18,19] However, the latteraffect growth have been identified, it is difficult to perform a
point has not been generally accepted; in fact, Agertoft and Peder- complete and detailed study on the influence of ICS on growth.sen[20] showed that growth before puberty is more susceptible to ‘Normal growth’ is indeed the result of many different factors,
the action of ICS. such as genetic background, tempo of puberty, individual patterns
© Adis Data Information BV 2003. All rights reserved. Pediatr Drugs 2003; 5 (6)

Inhaled Corticosteroids: Growth and Adrenal Function 355
of puberty, etc. All these factors are confounding parameters the evening may influence the nocturnal secretory pattern of
which must be taken into account. growth hormone to a greater extent than a morning dose.[27]
Recent studies have demonstrated that, generally, ICS are wellFurthermore, children with severe asthma could have an im-
tolerated at the recommended conventional dosages (see table III),paired final height as a result of the combination of corticosteroid
although impaired growth velocity has been reported in sometherapy and asthma itself. We assume that children with mild
children receiving conventional dosages.[19,28] However, it isasthma have more patent airways than those with severe asthma;
sometimes necessary to use higher dosages of ICS, and there areconsequently drug deposition and absorption may be higher, with
several studies reporting that this is not completely risk-free.[29,30]subsequent higher systemic effects.
A recent meta-analysis[31] suggested that a moderate dosage ofThe effect on growth of recurrent oral administration of cortico-inhaled beclomethasone significantly decreases the linear growthsteroids, such as methylprednisolone, for uncontrolled asthma,velocity of children with mild to moderate asthma, as does fluti-must also be taken into account when we compare the efficacy andcasone propionate, although there are few studies on this drug.adverse effects of ICS. Finally, in relation to the placebo-control-These results are in contrast with those reported in a previousled trials, the fact that the children treated with placebo or non-meta-analysis.[32]
corticosteroid drugs have mild asthma in contrast to childrenDuring the past decade it has been shown that uninterruptedtreated with ICS who have, in most cases, moderate or severe
treatment with beclomethasone 400 μg/day can reduce growthasthma, must be considered as a possible bias. Thus, it is useful torates in prepubertal children.[28] It has also been demonstrated thatconsider the different aspects that may influence the effects of ICSbeclomethasone was statistically more effective in reducing air-on growth, and critically evaluate these parameters when decidingway hyper-responsiveness than either salmeterol or placebo; how-to use these drugs in the long-term management of asthma.ever, linear growth in children who received beclomethasone was
significantly less than in children treated with salmeterol or place-3.4 Long-Term Effects of ICS
bo.[28] Other studies have confirmed this reduction of approximate-
ly 1.5 cm/year in the growth of prepubertal children treated withConsidering the normal circadian rhythm of cortisol and GH beclomethasone 400 μg/day.[34,35] However, in a former study,[36]
secretion, with a peak secretion of growth hormone during the no statistically significant differences were found between beclo-night coincidental with the minimum of cortisol levels, it seems methasone and budesonide in the dosage range of 400–1000 μg/that the risk of adverse effects on growth occurs when exogenous day. In patients receiving either beclomethasone or budesonidecorticosteroids exceed the endogenous production of cortisol.[18]
400 μg/day, doubling the dose did not produce clinical benefits,Thus, it is quite obvious that the time of administration of ICS, as and a further increase in dose did not improve asthma control, butdemonstrated for oral corticosteroids, may influence the negative increased the risk of adverse effects.[36] The effects of dosages ofeffect on growth, with a single morning dose being best tolerat-
ed.[23-25]
Clinical experience has suggested that once daily administra-
tion in the morning is better than twice daily, because the possibili-
ty of growth suppression may increase with administration fre-
quency. Findings from a study using once daily intranasal budeso-
nide versus a twice daily regimen appear to support this
hypothesis.[26] Furthermore, results of a study that compared in-
haled budesonide 800μg once daily in the morning and 400μg
twice daily confirm that once daily morning administration of
budesonide reduces the risks of adverse effects on growth. This is
probably because of the interaction of ICS with the hormonal
circadian rhythm and GH suppression. Considering that the bio-
logic half-life of budesonide is approximately 2–4 hours, 400μg in
Table III. Inhaled corticosteroid dosages recommended by the American
Academy of Allergy, Asthma, and Immunology for long-term control of
asthma (reproduced from the American Academy of Allergy, Asthma, and
Immunology,[33] with permission)
Generic name (formulation) Dosage (μg/day)
Low Medium High
Beclomethasone dipropionate 84–336 336–672 >672
(MDI)
Budesonide (DPI) 200 200–400 >400
Flunisolide (MDI) 500–750 1000–1250 >1250
Fluticasone propionate (DPI) 100–200 200–500 >500
Fluticasone propionate (MDI) 88–176 176–440 >440
DPI = dry powder inhaler; MDI = metered-dose inhaler.
© Adis Data Information BV 2003. All rights reserved. Pediatr Drugs 2003; 5 (6)

356 Salvatoni et al.
ICS higher than 2000 μg/day are virtually unknown. In patients treatment. In particular, Doull et al.[34] noted a 1cm reduction in
whose asthma is not controlled with recommended dosages, strate- growth during 7 months of treatment with beclomethasone, with-
gies must be considered for increasing compliance and use of more out a significant catch-up growth during a washout period of 4
efficient inhalation techniques. months. In a second study, the same authors showed that the
reduction in growth velocity was limited to the first 18 weeks ofIn the last 20 years many studies have been published to try totreatment.[41] Unlike the above study, Tinkelman et al.[19] found noclarify whether ICS do actually affect growth, and if so, whether itdifference in growth velocity suppression in the first 6 months, andis a persistent or transient impairment (see table IV).between 6 and 12 months, in children treated with beclometha-A high volume of literature published during the past decadesone.has confirmed a dose-related inhibition of growth in short- and
Simons[28] showed that the majority of growth delay occursintermediate-term studies; however, long-term studies, defined aswithin the first 3 months of ICS therapy, with growth velocitystudies of treatment lasting >12 months, have shown no negativesimilar to that of the placebo group after this period. This meanseffects on final height.that if growth delay is confined to the first 3 months of therapy, theTwo important studies have been conducted on the long-termimplications for growth in long-term therapy are less significant.effects of ICS on linear growth.[20,39] The first one is the ChildhoodThe negative impact of ICS on growth velocity during the firstAsthma Management Program (CAMP) in which linear growthyear of treatment was also confirmed by a meta-analysis per-was examined in 1041 children aged between 5 and 12 years withformed by Sharek and Bergman,[31] who concluded that childrenmild to moderate asthma. Children were randomized to receivewith mild to moderate asthma using beclomethasone show abudesonide (200μg), nedocromil, or placebo twice daily for 4–6decreased linear growth velocity of about –1.51 cm/year. In addi-years (mean 4.3 years). The budesonide group demonstrated ation, the new molecule fluticasone propionate was analyzed and itsignificant decrease in growth velocity during the first year, with arevealed a modest statistically significant decrease in linearmean height increase during the whole study period of 1.1cm lessgrowth when compared with placebo (–0.43 cm/year).than that observed in the placebo group (22.7 versus 23.8cm; p =
In a recent 52-week study, Skoner et al.[30] showed a signifi-0.005). The difference in growth velocity between the two groups
cantly lower growth velocity in children with mild persistentdid not increase beyond the first year and, by the end of the study,
asthma treated with budesonide via nebulizer, compared withthe growth velocity was similar for all groups.[39] In the second
children receiving conventional non-corticosteroid treatment. Astudy, the mean difference between target height (calculated on the
similar difference was not observed in the other two groups ofbasis of parental height) and adult height attained in 211 children
children with more severe asthma treated with budesonide, ortreated with budesonide (average dosage 412 μg/day) for 9.2 years
receiving conventional treatment with corticosteroids. The au-was not different from that observed in 18 patients with asthma
thors’ interpretation of the results is that children with less severewho were not treated with ICS, and 51 healthy control individuals.
asthma ‘may have greater intrapulmonary deposition, and thusIn agreement with the former study, a growth reduction was
absorption, or be more sensitive to the effects of ICS’. However, itobserved during the first year of treatment, and the extent was
must be pointed out that all groups receiving treatment with ICSsignificantly related to age, with a more pronounced reduction in
had lower growth velocity than children treated without ICS;younger children.[20] Norjavara et al.[40] confirmed that long-term
therefore, we cannot see in this study any evidence that childrenICS treatment for asthma does not reduce adult height, by showing
with mild asthma are at greater risk of adverse effects.[30]that the introduction of ICS in Sweden has not changed the mean
difference in height between Swedish conscripts with and without Beyond these studies, a meta-analysis demonstrated that thereasthma. Moreover, in 1997 Silverstein et al.,[15] in a retrospective is a tendency, albeit small, for ICS to be associated with thestudy concerning a cohort of 153 patients with asthma who had impairment of final height in children with asthma.[32] However,attained their adult height, showed that patients with asthma who this effect was small and, therefore, it would not be confirmed byreceived corticosteroid treatment attained similar adult height to relatively few conflicting studies. Moreover, final growth impair-that of patients who had never been treated with corticosteroids. ment was limited to children also treated occasionally with sys-
Further studies that focused on shorter periods of treatment temic corticosteroids (methylprednisolone or prednisone), and the
confirm that ICS can impair growth velocity in the first year of reduction in linear growth during short-term ICS treatment was, in
© Adis Data Information BV 2003. All rights reserved. Pediatr Drugs 2003; 5 (6)

Inhaled C
orticosteroids: G
rowth and
Ad
renal Function357
© A
dis D
ata
Info
rma
tion
BV 2003. A
ll righ
ts rese
rved
.P
ed
iatr D
rug
s 2003; 5 (6)
Table IV. Summary of the main studies of adverse effects on growth of long-term inhaled corticosteroid treatment in children with asthma
No. of Mean age (range) Drug/dosage Study period (y) Conclusions Reference
patients [years]
52 9.6 (4–13) Budesonide 200 μg/day 1 No effects of budesonide on growth 37
195 11.9 (6–16) Beclomethasone 400 μg/day 1 Growth velocity suppression in children treated with 19
beclomethasone
216 6.2 (3–11) Budesonide 430–710 μg/day 3–6 No overall significant effect of budesonide vs run-in 38
without corticosteroids or control children
153 6.1 (± 4.8)a Unspecified 23 Use of corticosteroids in childhood: no effect on adult 15
height
241 9.3 (± 2.4)a Beclomethasone 400 μg/day 1 Beclomethasone group: linear growth was 1.44cm less 28
than children receiving salmeterol
67 10.5 (6–16) Beclomethasone 400 μg/day 1 Growth slower in beclomethasone group (–0.28 SD) 35
compared with salmeterol group (–0.03 SD) [p =
0.001]
268 8 (4.0–11.9) Fluticasone propionate 100–200 μg/ 1 Children treated with fluticasone propionate grew at 18
day rates similar to those in the placebo group
2355 (1–15) Unspecified 4 Children treated with high doses of inhaled 29
corticosteroids were shorter on average than the
reference population
325 Prepubescent Fluticasone propionate 100–200 μg/ 1 Children treated with fluticasone propionate had growth 10
day similar to the placebo group
211 8.7 (3–13) Budesonide 110–877 μg/day 9.2 Long-term treatment with budesonide did not influence 20
final adult height
1041 (5–12) Budesonide 400 μg/day 4–6 The mean height increase in children treated with 39
budesonide was 1.1cm less than in the placebo group
670 5 (0.5–8) Budesonide 500–2000 μg/day 1 Children with mild persistent asthma, treated with 30
budesonide 1 mg/day, compared with those in
conventional asthma therapy without inhaled
corticosteroids, had a decrease in growth rate of 0.8
cm/year
a Standard deviation.

358 Salvatoni et al.
most cases, counterbalanced by a catch-up growth in the long-term Static tests include measurement of cortisol levels in the morn-
period leading to normal final height. Finally, from this meta- ing, the circadian rhythm of cortisol, and free urine cortisol excre-analysis it emerged that there is no correlation between dose and tion. Dynamic tests measure the adrenal response after stimulus.growth retardation within the recommended doses (table III).[32]
The corticotrophin (ACTH) test (standard or low dose) evaluates
the adrenal reserve, while insulin and metyrapone tests evaluate4. Hypothalamic-Pituitary-Adrenal (HPA) Axis the integrity of the whole HPA axis, both the adrenal and pituitary
functions.[45-48]
The systemic activity of ICS is determined by several factors,
including corticosteroid receptor potency, receptor binding affini-4.2 HPA Axis and Corticosteroids
ty, plasma elimination half-life, lipophilicity, and systemic tissue
retention.In patients treated with oral corticosteroids, the subsequent useUse of ICS for long periods and at high doses may cause HPA
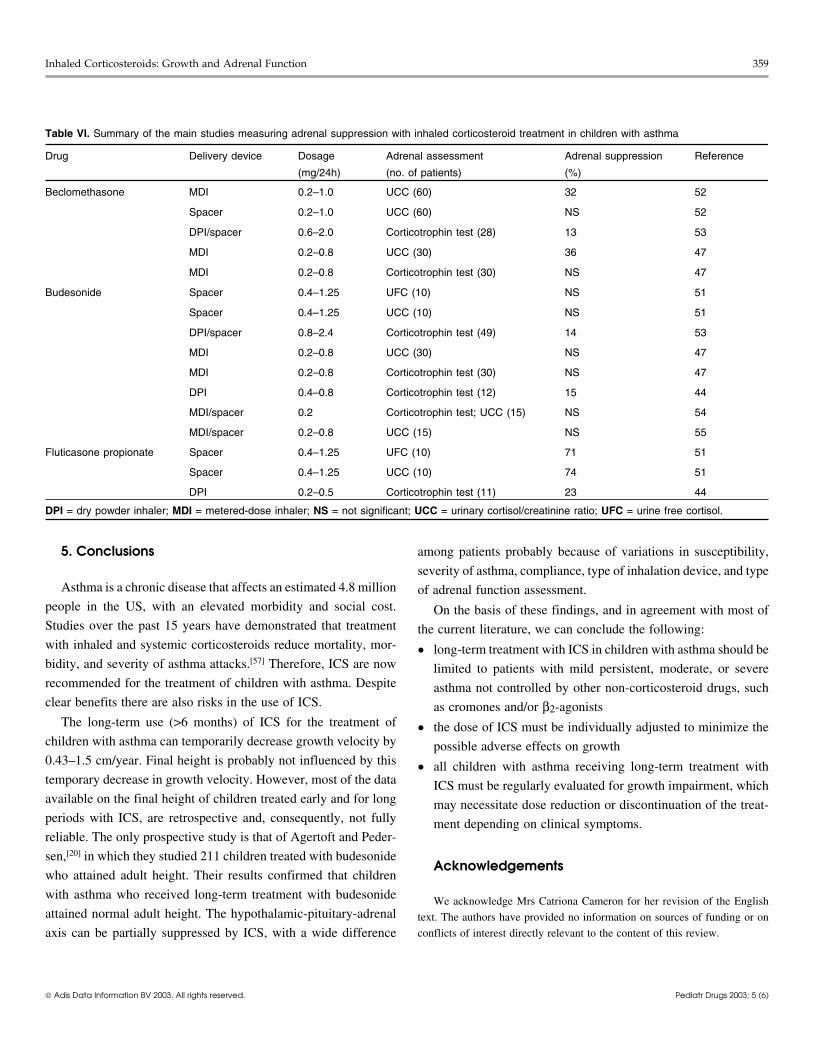
of ICS results in a slow recovery in HPA function, lasting, in someaxis suppression. This is a result of long-term negative feedbackcases, more than 3 years.[40,49] There are several studies showingexerted on corticotropin, and a subsequent reduction in adrenalvariable adrenal suppression in children treated with ICS (tablecortisol production. There are many conflicting results in theVI). According to these studies, fluticasone propionate (200–1250literature on the effects of ICS on the HPA axis; this is because ofμg/24h) always causes measurable suppression of overnightdifferent methods in the study of HPA function.12-hour urinary cortisol output or corticotrophin-stimulated plas-
ma cortisol,[50,51] while adrenal suppression by budesonide and4.1 Evaluation of HPA Axis Functionbeclomethasone is lower and inconsistent.
There are many standardized methods of evaluating the integri- The greater systemic activity of fluticasone propionate can bety of the HPA axis, both in a static and dynamic condition (see explained by its pharmacology. In fact it is generally accepted thattable V). fluticasone propionate is at least twice as potent as budesonide.
This is because fluticasone propionate has a higher lipophilicity
and a longer corticosteroid/receptor complex half-life than
budesonide.[54]
The absence of significant dose-related suppression of urinary
cortisol with budesonide has been demonstrated in two pediatric
studies, with dosages ranging from 200–800 μg/day.[47,55]
A recent study which used a more sensitive test for adrenal
suppression, the low-dose adrenocorticotrophin test, showed that
children with asthma treated with inhaled fluticasone propionate
or budesonide had a significantly lower mean stimulated concen-
tration of serum cortisol than patients treated with sodium cromog-
lycate.[44] In this study, the adrenal suppression was associated
with growth retardation only in patients treated with ICS for >6
months.
Although biochemical asymptomatic HPA axis suppression has
been shown during ICS treatment, severe hypoglycemia resulting
from adrenal insufficiency has only been reported in two pre-
school children receiving inhaled fluticasone propionate treatment
at a dosage of 780 μg/m2/day.[56]
Table V. Static and dynamic tests for the assessment of adrenal
function[42-44]
Test Reference values
Plasma cortisol level 0800h: 138–635 mmol/L
1600h: 83–413 mmol/L
2000h: ≤50% of 0800h
Urine free cortisol (24h urine Child: 5.5–74 mmol/24h
collection) Adolescent: 14–152 mmol/24h
Corticotrophin (ACTH) test Plasma cortisol increment of 200
(tetracosactide [cosyntropin] 250μg mmol/L, or a level of 500 mmol/L
IV, blood samples taken 30 and 60 at any time during the test
minutes after injection)
Low-dose corticotrophin (ACTH) test Plasma cortisol increment of 200
(tetracosactide 0.5 μg/1.73 m2 body mmol/L, or a level of 500 mmol/L
surface IV, blood samples taken 30 at any time during the test
and 60 minutes after injection)
Insulin-induced hypoglycemia (0.1 Cortisol ≥550 mmol/L (blood
U/kg regular insulin IV, blood glucose must fall to 1.9 mmol/L
glucose and plasma cortisol level during test)
measured 30 and 45 minutes after
injection)
© Adis Data Information BV 2003. All rights reserved. Pediatr Drugs 2003; 5 (6)
Inhaled Corticosteroids: Growth and Adrenal Function 359
Table VI. Summary of the main studies measuring adrenal suppression with inhaled corticosteroid treatment in children with asthma
Drug Delivery device Dosage Adrenal assessment Adrenal suppression Reference
(mg/24h) (no. of patients) (%)
Beclomethasone MDI 0.2–1.0 UCC (60) 32 52
Spacer 0.2–1.0 UCC (60) NS 52
DPI/spacer 0.6–2.0 Corticotrophin test (28) 13 53
MDI 0.2–0.8 UCC (30) 36 47
MDI 0.2–0.8 Corticotrophin test (30) NS 47
Budesonide Spacer 0.4–1.25 UFC (10) NS 51
Spacer 0.4–1.25 UCC (10) NS 51
DPI/spacer 0.8–2.4 Corticotrophin test (49) 14 53
MDI 0.2–0.8 UCC (30) NS 47
MDI 0.2–0.8 Corticotrophin test (30) NS 47
DPI 0.4–0.8 Corticotrophin test (12) 15 44
MDI/spacer 0.2 Corticotrophin test; UCC (15) NS 54
MDI/spacer 0.2–0.8 UCC (15) NS 55
Fluticasone propionate Spacer 0.4–1.25 UFC (10) 71 51
Spacer 0.4–1.25 UCC (10) 74 51
DPI 0.2–0.5 Corticotrophin test (11) 23 44
DPI = dry powder inhaler; MDI = metered-dose inhaler; NS = not significant; UCC = urinary cortisol/creatinine ratio; UFC = urine free cortisol.
5. Conclusions among patients probably because of variations in susceptibility,
severity of asthma, compliance, type of inhalation device, and typeAsthma is a chronic disease that affects an estimated 4.8 million of adrenal function assessment.
people in the US, with an elevated morbidity and social cost. On the basis of these findings, and in agreement with most ofStudies over the past 15 years have demonstrated that treatment the current literature, we can conclude the following:with inhaled and systemic corticosteroids reduce mortality, mor- • long-term treatment with ICS in children with asthma should bebidity, and severity of asthma attacks.[57] Therefore, ICS are now limited to patients with mild persistent, moderate, or severerecommended for the treatment of children with asthma. Despite asthma not controlled by other non-corticosteroid drugs, suchclear benefits there are also risks in the use of ICS. as cromones and/or β2-agonists
The long-term use (>6 months) of ICS for the treatment of • the dose of ICS must be individually adjusted to minimize thechildren with asthma can temporarily decrease growth velocity by possible adverse effects on growth0.43–1.5 cm/year. Final height is probably not influenced by this • all children with asthma receiving long-term treatment withtemporary decrease in growth velocity. However, most of the data ICS must be regularly evaluated for growth impairment, whichavailable on the final height of children treated early and for long may necessitate dose reduction or discontinuation of the treat-periods with ICS, are retrospective and, consequently, not fully ment depending on clinical symptoms.reliable. The only prospective study is that of Agertoft and Peder-
sen,[20] in which they studied 211 children treated with budesonideAcknowledgements
who attained adult height. Their results confirmed that children
with asthma who received long-term treatment with budesonide We acknowledge Mrs Catriona Cameron for her revision of the Englishattained normal adult height. The hypothalamic-pituitary-adrenal text. The authors have provided no information on sources of funding or on
conflicts of interest directly relevant to the content of this review.axis can be partially suppressed by ICS, with a wide difference
© Adis Data Information BV 2003. All rights reserved. Pediatr Drugs 2003; 5 (6)

360 Salvatoni et al.
26. Wolthers OD, Pedersen S. Knemometric assessment of systemic activity of onceReferencesdaily intranasal dry-powder budesonide in children. Allergy 1994; 49: 96-9
1. National Asthma Educational Program. Guidelines for the diagnosis and manage-27. Heuck C, Wolthers OD, Kollerup G, et al. Adverse effects of inhaled budesonidement of asthma. Bethesda (MD): US Department of Health and Human Ser-
on growth and collagen turn-over in children with asthma: a double-blindvices, 1998comparison of once-daily versus twice-daily administration. J Pediatr 1998;
2. Centers for Disease Control and Prevention. Surveillance for asthma: United133: 608-12
States, 1960-1995. MMWR CDC Surveill Summ 1998; 47 Suppl. 1: 1-2728. Simons FER. A comparison of beclomethasone, salmeterol, and placebo in chil-
3. Scott TW. Epidemiology and heterogeneity of asthma. Ann Allergy Asthmadren with asthma. Canadian Beclomethasone Dipropionate-Salmeterol
Immunol 2001; 87 Suppl. 1: 5-8Xinafoate Study Group. N Engl J Med 1997; 337: 1659-65
4. National Institutes of Health. Global strategy for asthma management and preven-29. McCowan C, Neville RG, Thomas GE, et al. Effects of asthma and its treatment ontion. Bethesda (MD): National Institutes of Health, 1995 Jan. NHLBI/WHO
growth: four year follow-up of cohort of children from general practices inworkshop report no. 95-3659Tayside, Scotland. BMJ 1998; 316: 668-72
5. National Education and Prevention Program. Guidelines for the diagnosis and30. Skoner DP, Szefler SJ, Welch M, et al. Longitudinal growth in infants and youngmanagement of asthma. Washington, DC: National Heart, Lung, and Blood
children treated with budesonide inhalation suspension for persistent asthma. JInstitute, Expert Panel Report 2, 1997 Jul. NIH Publication No. 97-4051Allergy Clin Immunol 2000; 105: 259-68
6. Van Essen-Zandvliet EE, Hughes MD, Waalkens HJ, et al. Effects of 22 months of31. Sharek PJ, Bergman DA. The effect of inhaled steroids on linear growth of childrentreatment with inhaled steroids and/or beta-2-agonist on lung function, airway
with asthma: a meta-analysis. Pediatrics 2000; 106 (1): E8responsiveness, and symptoms in children with asthma. Am Rev Respir Dis32. Allen DB, Mullen ML, Mullen B. A meta-analysis of the effect of oral and inhaled1992; 146: 547-54
corticosteroids on growth. J Allergy Clin Immunol 1994; 93 (6): 967-757. Hardman JG, Limbird LE, editors. Goodman and Gilman: the pharmacological33. American Academy of Allergy, Asthma and Immunology. Pediatric asthma –basis of therapeutics. 8th ed. New York: Pergamon Press, 1990
promoting best practice: guide for managing asthma in children. Milwaukee8. Johnson M. Pharmacodynamic and pharmacokinetics of inhaled glucocorticoster-(WI): The American Academy of Allergy Asthma and Immunology Inc, 1999oids. J Allergy Clin Immunol 1996; 97: 169-76
34. Doull IJ, Freezer NJ, Holgate ST. Growth of prepubertal children with mild asthma9. Skoner DP. Balancing safety and efficacy in pediatric asthma management. Pediat-treated with inhaled beclomethasone dipropionate. Am J Respir Crit Care Medrics 2002; 109: 381-921995; 151: 1715-910. Allen DB. Influence of inhaled steroids on growth: a paediatric endocrinologist’s
35. Verberne AA, Frost C, Roorda RJ, et al. One year treatment with salmeterolperspective. Acta Paediatr 1998; 87: 123-9compared with beclomethasone in children with asthma. The Dutch Paediatric11. Lipworth BJ, Jackson CM. Safety of inhaled and intranasal corticosteroids: lessonsAsthma Study Group. Am J Respir Crit Care Med 1997; 156: 688-95for the new millennium. Drug Saf 2000; 23: 11-33
36. Boe J, Bakke P, Rodolen T, et al. High-dose inhaled steroids in asthmatics:12. Colice GL. Comparing inhaled corticosteroids. Respir Care 2000; 45 (7): 846-53moderate efficacy gain and suppression of the hypothalamic-pituitary-adrenal13. Mager DE, Jusko WJ. Quantitative structure-pharmacokinetic/pharmacodynamic(HPA) axis. Eur Respir J 1994; 7: 2179-84relationships of corticosteroids in man. J Pharm Sci 2002; 91 (11): 2441-51
37. Ribeiro LB. Budesonide: safety and efficacy aspects of its long-term use in14. English AF, Neate MS, Quint DJ, et al. Biological activities of some corticoster-children. Pediatr Allergy Immunol 1993; 4: 73-8oids used in asthma [abstract]. Am J Respir Crit Care Med 1994; 149: A212
38. Agertoft L, Pedersen S. Effect of long-term treatment with an inhaled corticoster-15. Silverstein MD, Yunginger JW, Reed CE, et al. Attained adult height afteroid on growth and pulmonary function in asthmatic children. Respir Med 1994;childhood asthma: effect of glucocorticoid therapy. J Allergy Clin Immunol88: 373-811997; 99: 466-74
39. The Childhood Asthma Management Program Research Group. Long-term effects16. Anhoj J, Bisgaard AM, Bisgaard H. Systemic activity of inhaled steroids in 1- to 3-of budesonide or nedocromil in children with asthma. N Engl J Med 2000; 343:year-old children with asthma. Pediatrics 2002; 109 (3): E401054-6317. The transition to CFC-free inhalers: what pharmacists should know. Pharm J 1998;
40. Norjavara E, Gerhardsson de Vermer M, Lindmark B, et al. Reduced height in261: 316-7Swedish man with asthma at the age of conscription for military service. J18. Allen DB. Inhaled corticosteroid therapy for asthma in preschool children: growthPediatr 2000; 6: 25-9issues. Pediatrics 2002; 109: 373-80
41. Doull IJ, Campbell MJ, Holgate ST. Duration of growth suppressive effect of19. Tinkelman DG, Reed CE, Nelson HS, et al. Aerosol beclomethasone dipropionateregular inhaled corticosteroids. Arch Dis Child 1998; 78: 172-3compared with theophylline as primary treatment of chronic mild to moderately
42. Behrman RE, Kliegman RM, Jenson HB, editors. Nelson textbook of pediatrics.severe asthma in children. Pediatrics 1993; 92: 64-77Philadelphia (PA): WB Saunders Company, 200020. Agertoft L, Pedersen S. Effect of long-term treatment with inhaled budesonide on
43. Wilson JD, Foster DW, Kronenberg HM, et al., editors. Williams textbook ofadult height in children with asthma. N Engl J Med 2000; 343: 1064-9endocrinology. 9th ed. Philadelphia (PA): Saunders Company, 199821. Cohen MB, Abram LE. Growth pattern of allergic children. J Allergy 1948; 19:
44. Kannisto S, Korppi M, Remes K, et al. Adrenal suppression, evaluated by a low165dose adrenocorticotropin test, and growth in asthmatic children treated with22. Ninan TK, Russell G. Asthma, inhaled corticosteroids treatment and growth. Archinhaled steroids. J Clin Endocrinol Metab 2000; 85: 652-7Dis Child 1992; 67: 703-5
45. Hartzband PI, Van Herle AJ, Sorger L, et al. Assessment of hypothalamic pituitary23. Harter JG, Reddy JR, Thorn GW. Studies on an intermittent corticosteroids dosageadrenal axis dysfunction comparison of ACTH stimulation, insulin hypoglyce-regimen. N Engl J Med 1963; 269: 591-6mia and metyrapone. J Endocrinol Invest 1988; 11: 769-7624. Byron MA, Jackson J, Ansell BM. Effect of different corticosteroid regimens on
46. Stewart PM, Corrie J, Seckl JR, et al. A rational approach for assessing the HPAhypothalamic-pituitary-adrenal axis and growth in juvenile chronic arthritis. J Raxis. Lancet 1998; I: 1208-10Soc Med 1983; 76: 452-7
25. Reinberg A, Gervais P, Chaussade M, et al. Circadian changes in effectiveness of 47. Bisgaard H, Damkjaer M, Nielsen M, et al. Adrenal function in children withcorticosteroids in 8 patients with allergic asthma. J Allergy Clin Immunol 1983; bronchial asthma treated with beclomethasone dipropionate or budesonide. J71: 425-33 Allergy Clin Immunol 1988; 81: 1088-95
© Adis Data Information BV 2003. All rights reserved. Pediatr Drugs 2003; 5 (6)

Inhaled Corticosteroids: Growth and Adrenal Function 361
48. Broide J, Soferman R, Kivity S, et al. Low-dose adrenocorticotropin test reveals 54. Brown PH, Blundell G, Greening A, et al. Screening for HPA axis suppression inimpaired adrenal function in patients taking inhaled corticosteroids. J Clin asthmatics taking high dose inhaled glucocorticosteroids. Respir Med 1991; 85:Endocrinol Metab 1995; 80 (4): 1243-6 511-22
49. Barnes PJ, Pedersen S. Efficacy and safety of inhaled corticosteroids in asthma. 55. Wolthers OD, Pedersen S. Measures of systemic activity of inhaled corticosteroidsAm Rev Respir Dis 1993; 148: S1-17 in children: a comparison of urine cortisol excretion and knemometry. Respir
50. Volovitz B, Amir J, Malik H, et al. Growth and pituitary-adrenal function in Med 1995; 89: 347-9children with severe asthma treated with inhaled budesonide. N Engl J Med 56. Patel L, Wales JK, Kibirige MS, et al. Symptomatic adrenal insufficiency during1993; 329: 1703-8 inhaled corticosteroid treatment. Arch Dis Child 2001; 85: 330-4
51. Clark DJ, Lipworth BJ, Clark RA. Adrenal suppression with inhaled budesonide57. Suissa S, Ernst P, Benayoun S, et al. Low-dose inhaled corticosteroids and the
and fluticasone propionate given by large volume spacer to asthmatic children.prevention of death from asthma. N Engl J Med 2000; 343: 332-6
Thorax 1996; 51: 941-3
52. Goldberg S, Algur N, Levi M, et al. Adrenal suppression among asthmatic childrenreceiving chronic therapy with inhaled corticosteroids with and without spacer
Correspondence and offprints: Alessandro Salvatoni, Associate Professor,device. Ann Allergy Asthma Immunol 1996; 76 (3): 234-8
Clinica Pediatrica, Universita degli Studi dell’Insubria, Via Filippo del53. Ninan TK, Reid IW, Carter PE, et al. Effective high doses of inhaled corticoster-Ponte, 19, 21100 Varese, Italy.oids on adrenal function in children with severe persistent asthma. Thorax
1993; 48: 599-602 E-mail: [email protected]
© Adis Data Information BV 2003. All rights reserved. Pediatr Drugs 2003; 5 (6)