information for women - sasksurgery.ca -...
TRANSCRIPT

Information for WomenAbout Incontinence & Vaginal Prolapse
Saskatchewan Pelvic Floor Pathway

ACKNOWLEDGEMENTS
This booklet was edited and compiled by the multidisciplinary Pelvic Floor Pathway Working Group of the Saskatchewan Ministry of Health,
with significant input from and oversight by gynecologists, urologists, family physicians, women’s health nurse practitioners and pelvic floor physical therapists from Saskatoon Health Region and Regina Qu’Appelle Health Region (RQHR) .
The contributions of everyone involved, especially patients who reviewed the contents in draft form, helped ensure this resource will serve the needs of patients.
The illustrations were created by RQHR Medical Media Services and are used with permission. Some photos used with permission from Dreamstime and iStockphoto.
See more information: www.health.gov.sk.ca/pelvic-floor

i
Introduction .........................................................................................................Page ii
Understanding the Problem ..........................................................................Pages 1-4
How the Bladder Works
Types of Incontinence
• Stressincontinence• UrgencyandUrgeIncontinence• Fecalincontinence
Vaginal Prolapse
Treatment Options .......................................................................................Pages 5-16
Self Management
• LifestyleChanges• BladderRetraining• PelvicFloorMuscleExercises
Pelvic Floor Physical Therapy
Medications for Urge Incontinence
Pessary
Surgery
• StressIncontinence• VaginalProlapse
Do I Want to Seek Treatment? ...........................................................................Page 17Thisworksheetmighthelpyoudecidewhetheryour symptomsarebothersomeenoughtoseektreatment.
Assessment and Diagnosis .............................................................................. Pages 18
Selecting a Treatment ................................................................................Pages 19-22
February 2013
TABLE OF CONTENTS

Urinaryincontinence(leakingurine)isacommonconditionthataffectsabout30%ofadultwomen.Sometimeswomenalsohaveotherproblemslikeabulgeorpressureinthevagina(prolapse).Thisbookletexplainswhatthesethingsare,whatcausesthem,andwhatcanbedonetohelp.
If you have any of these problems, this booklet is a good way to start learning more about them. Speak to a doctor or member of the Pelvic Floor Pathway Team to get a personal diagnosis or treatment.
INTRODUCTIONii

1
HOW THE BLADDER WORKS
Inyourbody,urineisstoredinanorgancalledthebladder.Yourbladderisrelaxedmostofthetime.Whenyouwanttourinate,yourbraintellsyourbladdertocontract,sendingtheurineout.
WHAT IS INCONTINENCE?
Urinaryincontinencemeansthatyouleakurinewhenyoudon’twantto.Aboutone-thirdofwomensometimesleakurine.Somewomenleakonlyalittle,andsomemayleakalot.Notallwomenfeelthatleakingisaseriousproblemforthem.
Therearetwomainreasonswhywomenleakurine:stress incontinenceandurge incontinence.
Stress incontinencemeansyouleakurinewhenyoucough,sneeze,exercise,bendoverorliftheavyobjects.Thisleakagehappensbecausetheseeventscauseanincreaseofphysicalpressureonyourbladder.
Withstressincontinence,theproblemisthatthemusclesandtissuesinyourpelvicfloorarenotstrongenoughtoresistexternalpressure.Whenextrapressureisplacedontheabdomenfromactivitieslikecoughing,laughing,jumpingorlifting,urineisforcedpastthemusclesthatkeeptheurethraclosed.Thiscanhappenwhenthemusclesinyourpelvicareaareweakenedbyhavingbabies,bychronicconstipationrequiringstraining,byobesity,orsimplybygettingolder.
PART I: UNDERSTANDING THE PROBLEM
If pressure from outside squeezes the urine out of the bladder, that is stress incontinence.
Urine
Bladder
Uretha Closed
Sphincter Muscles Squeezed Shut Sphincter Muscles Relaxed
Uretha Open
Coughingorsneezingincreasesthephysicalpressureonyourbladder.

2
Urge incontinenceiswhenyoufeelanurgentneedtopassurineandyouareunabletomakeittothetoiletintime.Yourbladderiscontractingwhenyoudon’twantitto!Youmayhavelittleornowarningthatthisisgoingtohappen,oryoumayhaveasuddenstrongneedtourinate.Theremaybetriggersthatcausethisurgency,suchashearingrunningwater,feelingchilled,arrivingatyourhousedoor,orstandingupfromachairorbed.Peoplewithurgeincontinencemayalsoneedtourinateoftenandgetupseveraltimesinthenight.Withurgeincontinence,theproblemisanoveractivebladdermuscle.
Manywomenhaveacombinationofstressandurgeincontinencecalledmixed incontinence.Itisgoodtoknowwhatkindofincontinenceyouhavebecausethecausesandtreatmentsaredifferent.
WHAT IS NORMAL?
Anaveragewomanurinatesupto7timesduringtheday(aboutevery2-3hours).Itisnormaltogetuponceinthenighttourinate,andtwiceasyougetolder.Normalbladdercapacityis300–600ml(250ml=1cup)
Normalfluidintakeisabout6-8cupsofwaterorotherdrinksperday.Drinkingmoreorlessthanthisamountcanmakeleakingworse.Drinksthathavecaffeine,liketea,coffeeandcolas,canalsomakeleakingworsebecausetheyirritatethebladder.
Fecal incontinencemeansanunwantedleakageofbowelcontents–gas,liquidorsolidstool.Somewomenhaveproblemswithbothfecalandurinaryincontinence.Thiscanbebecauseofpelvicfloormuscleweakness.
If your bladder suddenly contracts on its own, that is urgency; if urine leaks out, that is urge incontinence
PART I: UNDERSTANDING THE PROBLEM

3
WHAT IS VAGINAL PROLAPSE?
A vaginal prolapsecanhappenwhenthetissueandmusclesinsidethepelvisbecomeweak.Thisweaknessallowsthevagina,uterus,bowelorbladdertocomedown.Imagineasockturningitselfinsideout.
Themainsymptomofvaginalprolapseisabulgebetweenthelegsthatyoucanseeorfeel.Itmaygoinandoutofthevaginadependingonwhetheryouarestanding,sittingorlyingdown.Itfeelsbiggerwithactivitiesthatputpressureontheareasuchaslifting,coughing,strainingwithbowelmovements,andintheeveningafterbeinguprightallday.Prolapsemaystaythesamesizeforlongperiods
oritmaygetbiggerovertime.Forafew,thebulgebecomessmallerandlessnoticeable.
Prolapsehappensbecauseofweakness,damageorstretchingofthesupportstructuresatthebottomofthepelvisthatholdyourorgansin.Thesemusclesarecalledthe“pelvicfloor.”Althoughitcanoccurinanywoman,prolapseisoftencausedbyhavingbabies,increasingageandobesity.Otherfactorsthatmaystretchorweakenpelvictissuesincludeconstipation,chroniccoughorlong-termheavylifting.
Prolapsedoesnotusuallycausepainorconstipation,butitcanbeuncomfortableandmayaffectthebladder,bowelandsexualfunction.
Bladder
UrethraVagina
AnusRectum
Uterus
ddheenan©2012
Normal Anatomy
Pelvic Floor Muscles
Cervix
Uterus
Prolapsed Uterus
Pelvic FloorMuscles
Pelvic FloorMuscles
Normal Pelvic Anatomy
Illustrations courtesy Medical Media Services, Regina Qu’Appelle Health Region.
PART I: UNDERSTANDING THE PROBLEM
Anal Sphinter
Rectum
Rectocele
Prolapsed Bowel
Pelvic Floor Muscles

4
Prolapsed Bowel (rectocele): Whenthebowelcollapsesintothevaginafrombehind,stoolcangointhewrongdirectionwithstraining.Thiscancauseincompleteemptyingofthebowel.Somewomenmayneedtopushontheprolapsewiththeirfingersinthevaginatohelpemptythebowel.Changingthestoolconsistency,aimingforsoft,formedstoolandavoidingconstipation,pluslearningcorrectevacuationposturesandtechniquescanhelprelievesomeofthesesymptoms.
Prolapsed Bladder (cystocele): Whenthebladdercollapsesintothevagina,itcanmakeithardertoemptythebladdercompletelywhenyouurinate.Incompletebladderemptyingcancausebladderinfections.Somewomenwithbladderprolapsealsohaveurinaryincontinence.
PART I: UNDERSTANDING THE PROBLEM
Bladder
UrethraPelvic Floor
Muscles
Cystocele
Prolapsed Bladder
Pelvic Floor
MusclesAnal Sphinter
Rectum
Rectocele
Prolapsed Bowel
Pelvic Floor Muscles
Sexual function:Whenprolapseispresent,itisthewallsofthevaginathatcollapseinwardandcreateabulgebetweenthelegs.Somewomenfindthattheprolapsegetsinthewayofsexualintercourse.Thewomanorherpartnermayworryabouthurtingthewomanormakingtheprolapseworse,butthisisnot
thecase.Intercourseissafe,evenwhenprolapseispresent.Ifintercourseispainful,itmayberelatedotherfactors,suchasvaginaldrynessrelatedtomenopause.

5
SELF MANAGEMENT
A. LIFESTYLE CHANGES
With urge incontinence,theproblemisanoveractivebladdermuscle.Urgeincontinence can be improvedbyreducingthingsthatirritatethebladder.Thismayinvolvelifestylechangessuchasavoidingcaffeine(e.g.coffee,teaandcolas)andotherirritantssuchasalcohol,cigarettes,artificialsweeteners,spicyfoodsandcitrus.
Regulartoiletingevery2-3hoursmayalsohelpsomewomenwithurgeincontinencetopreventepisodesofleaking.
Stress and urge incontinence, and fecal incontinence, can be improved by changes like:
• Achievingahealthyweightbyeatinganutritiousdietandgettingregularexercise,
• Drinking6-8cupsoffluidperday,two-thirdsofwhichshouldbewater.
• Avoidingconstipation.
PART II: TREATMENT OPTIONS
Caffeine content of some common foods and drinks
Product Serving Size (unless
otherwise stated)
Milligrams of Caffeine
(approximate values)
oz ml
Coffee,filterdrip 8 237 179
Coffee,decaffeinated 8 237 3
Tea(leaforbag) 8 237 50
Green tea 8 237 30
Decaffeinatedtea 8 237 0
Colabeverage,regular 12 355 (1can)
36-46
Colabeverage,diet 12 355 39-50
Chocolatemilk 8 237 8
Candybar,milkchocolate
1 28g 7
Bakingchocolate,unsweetened
1 28g 25-58
Chocolatecake 2.8 80g 36
Chocolatepudding 5.1 145g 9
Source: Health Canada (www.hc-sc.gc.ca)

6
Fecal incontinence(leakingstool)canimprovewith:
• Dietarychangestoimprovestoolconsistency
• Pelvicfloormusclestrengthening
• Correcttoiletingtechniques
TheBristolStoolFormScale(shownhere)describesthedifferenttypesofstoolformorconsistency.Types1and2arehard,constipatedstoolwhichcanbedifficulttopass.Types3and4aresoft,formed,normalstoolwhichareeasytopass.Types5,6and7arelooseandverydifficulttocontrolespeciallyifthereisweaknessinthepelvicfloorandanalsphinctermuscles.ThedesiredstoolformisType3or4.
PART II: TREATMENT OPTIONS
BRISTOL STOOL FORM SCALE
Type 1 Separatehardlumpslikenuts(difficulttopass)
Type 2 Sausageshapedbutlumpy
Type 3 Likeasausagebutwithcracksonsurface
Type 4 Likeasausageorsnake,smoothandsoft
Type 5 Softblobswithclear-cutedges(passedeasily)
Type 6 Fluffypieceswithraggededges,amushystool
Type 7 Watery,nosolidpieces(entirelyliquid)

7
THE URGE CURVE
PART II: TREATMENT OPTIONS
B. BLADDER RETRAINING
Ifyouhaveurgency/urge incontinencetherearesomethingsthatyoucandoforyourselftocontroltheleaking.Forexample,youcanchangewhatyoueatanddrinktohelpreduceirritationofthebladder,asexplainedintheprevioussection.Youcanalsolearntocontrolthebladdermusclebetter.Thisiscalled“bladderretraining.”
Urge suppression and bladder retraining
Whenyourbladdermusclecontracts,theurgetourinateisstronganduncomfortable.Thecommonreactionistorushtothebathroomassoonaspossible.Butyoucanretrainyourbladdertowait,ifyouconsciouslytrytosuppresstheurge.
Thefeelingofurgencycomesinwaves.Itstarts,grows,peaksandfadesaway.Thiscantakeafewminutes.Whenyoufeeltheurgetourinate:
1. Stopwhatyouaredoingandbe still.
2. Sitdownandsqueezeyourpelvicfloormuscles.Thistechniqueisreferredtoas“freezeandsqueeze.”
3. Takeafewdeepbreathsandrelaxyourbodyandmind.
4. Distractyourmindbycountingbackwards,sayingthealphabet,recitingnurseryrhymesetc.
5. Whentheurgesubsides,calmlywalk to the toilet.
Ifyouhavecommontriggersforurgeincontinence(e.g.hearingrunningwaterorputtingyourkeyinthedoor),youcanusethistechniquetomanagetheurgeandbreakthehabit.Practicesqueezingthemusclesatthesametimeyouareconfrontedwiththetrigger.Withpractice,urgesuppressionbecomeseasierandmoresuccessful.
Selfcarecanstopyoufromleakingasoften,butitprobablywillnotstoptheleakingcompletely.Youmaystillwearpads,justincase.
USING INCONTINENCE PADS
Ifyouwearpadsallthetimeormostofthetime,youshoulduseabarriercreamtopreventirritation.
PEAKS
GROWS
squeeze
SUBSIDES
STOPS
walk to toilet
STARTS
be still waitdistract yourself

8 PART II: TREATMENT OPTIONS
C. PELVIC FLOOR MUSCLE EXERCISES
Strongpelvicfloormusclesgiveuscontroloverourbladderandbowel,andsupportourorgansinthepelvis.Strengtheningthepelvicfloormusclescanimprovestressandurgeincontinenceandpelvicorganprolapse.
What is the Pelvic Floor?
Thepelvicfloormusclesstretchlikeatrampolinefromthetailbone(coccyx)tothepubicbone(backtofront)andfromonesittingbonetotheother(sidetoside).Thesemusclesarenormallyfirmandthick.
Thebladder,uterusandbowellieontopofthepelvicfloormusclelayer.Thereare3openingsinthepelvicfloorlayerfortheurethra(thetubefromthebladder),thevagina,andtheanus(openingfromthebowel)topassthrough.Thepelvicfloormusclesnormallywrapfirmlyaroundtheseopeningstokeepthemclosed.Thereisalsoanextracircularmusclearoundtheanus(analsphincter)andtheurethra(urethralsphincter)tohelpwiththeclosure.
Whenthepelvicfloormusclesarecontracted,thepelvicorgansareliftedandthesphincterstighten,closingtheopeningsofthevagina,anusandurethra.
Pelvic Floor Exercises
Specialexercises,sometimescalledKegel exercises,helptostrengthenthemusclesofthepelvicfloor.Youcandotheseexercisesathomebyyourself.Manywomenfindthatcoachingfromaspeciallytrainedphysiotherapisthelpsthemtolearntheexercisesproperlyandgetthemofftoagoodstart.
Finding the right muscles:
Imaginethatyouaretryingtostopyoururinefloworaretryingtoholdbackgas.Youshouldfeelyourvaginaandyouranustighten.Liedownandinsertaclean,moistfingerintothevagina.Tightenthepelvicfloormuscles.Youshouldfeelasqueezearoundyourfinger.
Rectum
Vagina
Urethra
Pelvic Bones
Pelvic Floor MusclesPelvic Floor Muscles
Tailbone

9
Doing the exercises:
1. Startbydoingtheexerciseslyingdownwithyourkneesbent.
2. Squeezeyourpelvicfloormuscles.Holdfor5-10seconds.Relaxfor10seconds.Workyourwayuptorepeatingthisexercise5-10times.
3. Youmayonlybeabletoholdforafewsecondstostart.That’sokay.Startthereandworkyourwayup.
4. Repeattheseexercises2-3timesaday.
5. Challengeyourself!Dotheseexercisesinsittingorstandingpositions,whileyouwalk,sidesteporjump.Increasetherepetitionsanddecreasetheresttime.
Ifyouaredoingexercisesyourselfathome,herearesometips:
• Makesurethatyouareusingthepelvicfloormusclesonly,notthelegsorbuttocks.
• Avoidholdingyourbreathwhendoingtheseexercises.
• Usethepelvicfloorwhenyouneeditmost.Squeezebeforeyoucough,sneeze,laughor
liftsomethingheavy.Thisiscalled“theknack.”Squeezeifyoufeelastrongurgetoemptythebladderandfearlosingcontroloftheurgeadd(freezeandsqueeze).
Tips for remembering to sneak in a squeeze:
• Trytolinkyourpelvicfloorexerciseswithcertainactivities:morningandbedtime,watchingtelevision,waitingatredlights.
• Reddots:putstickersinplacestoremindyoutodoyourexercises.Forexample,putoneonthebathroommirror,rearviewmirror,bedsidetableort.v.
Keep it up
Dotheexercisesregularlyanddon’tgiveup!Itmaytakethreetosixmonthstoseefullresults.Youmaytestyourpelvicfloorstrengthonceamonthbytryingtostopyourflowofurine,butdo notdoyourexerciseswhileyouemptythebladder.Thatmightconfusethebladder.
PART II: TREATMENT OPTIONS

10 PART II: TREATMENT OPTIONS
PELVIC FLOOR PHYSICAL THERAPY Ifyouarehavingdifficultywiththeexercisesoryouarenotgettingtheresultsyouhadhopedfor,youmaybedoingtheexercisesincorrectly.Researchshowsthat50%ofwomencannotlearnpelvicfloormuscleexercisesfromhearingorreadinginstructions.Forthosewhoneedindividualcoachingandsupport,therearespecially trained physical therapistswhocanhelp.
Thetherapistwillperformaphysicalevaluation,includingavaginalexamination,toassessyourpelvicfloorfunctionandtailoranexerciseprogram
tomeetyourspecificneeds.Inadditiontoteachingyouhowtoisolateandcorrectlyperformyourpelvicfloormuscleexercisesinone-on-onesessions,thephysicaltherapistwillgiveyouacomprehensivehomeprogramofexercisesfor:
• Pelvicfloormusclestrengthening
• Abdominal(core)musclestrengthening
• Posturecorrection.
Thephysicaltherapistwillalsoteachyou:
• strategiesandtechniquestopreventurineleaksduetocoughing,laughing,sneezing,bending,liftingandmorevigorousactivities
• strategiesandtechniquestohelpyoucontrol/deferbladderurgency
• toiletingtechniquestohelpyoucompletelyemptyyourbladderifyouarehavingdifficultydoingsoandtohavebowelmovementswithoutstraining
Andwill
• Provideyouwithinformationandsupportforlifestylechangesthatwillhelpyoutoreduceincontinenceandsymptomsofprolapse.
Sixty(60)to75%ofwomenwhoparticipateinpelvicfloorphysicaltherapyprogramsaresatisfiedwiththeresults.
Therearenosideeffectsbutyoumustcontinuewiththeexercisesorlifestylechangesorsymptomswillreturn.
11
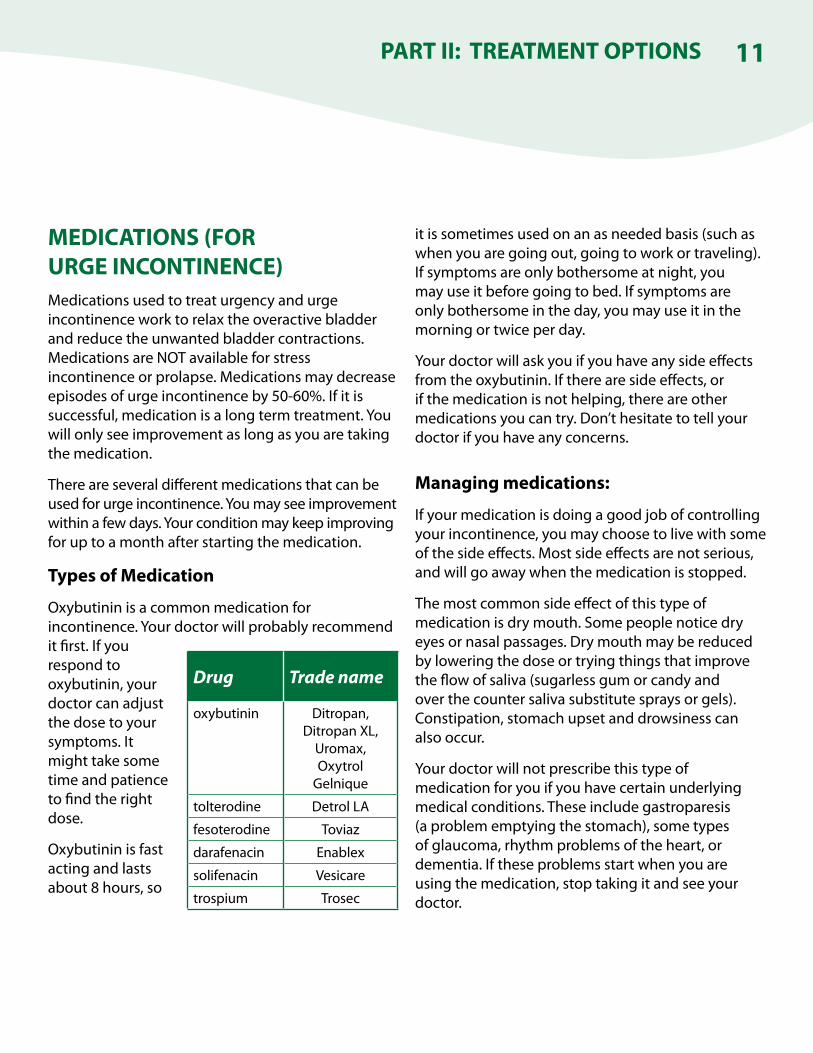
MEDICATIONS (FOR URGE INCONTINENCE)Medicationsusedtotreaturgencyandurgeincontinenceworktorelaxtheoveractivebladderandreducetheunwantedbladdercontractions.MedicationsareNOTavailableforstressincontinenceorprolapse.Medicationsmaydecreaseepisodesofurgeincontinenceby50-60%.Ifitissuccessful,medicationisalongtermtreatment.Youwillonlyseeimprovementaslongasyouaretakingthemedication.
Thereareseveraldifferentmedicationsthatcanbeusedforurgeincontinence.Youmayseeimprovementwithinafewdays.Yourconditionmaykeepimprovingforuptoamonthafterstartingthemedication.
Types of Medication
Oxybutininisacommonmedicationforincontinence.Yourdoctorwillprobablyrecommenditfirst.Ifyourespondtooxybutinin,yourdoctorcanadjustthedosetoyoursymptoms.Itmighttakesometimeandpatiencetofindtherightdose.
Oxybutininisfastactingandlastsabout8hours,so
itissometimesusedonanasneededbasis(suchaswhenyouaregoingout,goingtoworkortraveling).Ifsymptomsareonlybothersomeatnight,youmayuseitbeforegoingtobed.Ifsymptomsareonlybothersomeintheday,youmayuseitinthemorningortwiceperday.
Yourdoctorwillaskyouifyouhaveanysideeffectsfromtheoxybutinin.Iftherearesideeffects,orifthemedicationisnothelping,thereareothermedicationsyoucantry.Don’thesitatetotellyourdoctorifyouhaveanyconcerns.
Managing medications:
Ifyourmedicationisdoingagoodjobofcontrollingyourincontinence,youmaychoosetolivewithsomeofthesideeffects.Mostsideeffectsarenotserious,andwillgoawaywhenthemedicationisstopped.
Themostcommonsideeffectofthistypeofmedicationisdrymouth.Somepeoplenoticedryeyesornasalpassages.Drymouthmaybereducedbyloweringthedoseortryingthingsthatimprovetheflowofsaliva(sugarlessgumorcandyandoverthecountersalivasubstitutespraysorgels).Constipation,stomachupsetanddrowsinesscanalsooccur.
Yourdoctorwillnotprescribethistypeofmedicationforyouifyouhavecertainunderlyingmedicalconditions.Theseincludegastroparesis(aproblememptyingthestomach),sometypesofglaucoma,rhythmproblemsoftheheart,ordementia.Iftheseproblemsstartwhenyouareusingthemedication,stoptakingitandseeyourdoctor.
PART II: TREATMENT OPTIONS
Drug Trade name
oxybutinin Ditropan,DitropanXL,
Uromax,OxytrolGelnique
tolterodine DetrolLA
fesoterodine Toviaz
darafenacin Enablex
solifenacin Vesicare
trospium Trosec

12 PART II: TREATMENT OPTIONS
PESSARYApessaryisasiliconediscorringthatisspeciallyfitforyoubyadoctorornurse.Thepessaryisinsertedintothevagina(likeatampon)whereithelpstosupportthepelvicorgansandstopthemfromcomingdown(vaginal prolapse).
Apessarycanalsobeusedtotreatstress incontinence,becauseitputsgentlepressureontheurethra(tubethatdrainsthebladder)tohelpitstayclosed.Abouttwo-thirdsofwomenfindthatapessaryhelps.
Somewomentryapessarywhiletheywaitforstressincontinenceorprolapsesurgery,andothersuseapessarytoavoidsurgery.
Mostwomencanwearapessarysafelyforseveraldaysatatime.Pessariescanbeleftinformostactivitiesofdailylife,butshouldberemovedforsexualactivity.
Using a pessary
Youwillbefittedwithapessarythatistherightsizeandshape.Itmighttakeafewtriestofindapessarythatwillprovidesupportwithoutcausingdiscomfortorslippingout.Youwillbetaughttoinsertandremovethepessaryonyourown.Astringcanbeattachedtothepessarytoassistwithremoval.
Yourdoctormightprescribelowdoseestrogencreamtouseforkeepingyourvaginaltissuehealthy.
Youwillbeinstructedtoremoveyourpessaryonceortwiceweekly.Forexample,removeitovernightonMondayandThursdayeveryweek.Ifyouaremenopausalanddonotuseestrogen,removalofyourpessaryisrecommendedeverynight.
Ontheeveningswhenthepessaryisremoved,youmayuseyourestrogenandpreparethepessaryforinsertionthefollowingmorning.
Pessary care
Thepessaryiswashedwithmildsoap(avoidingperfumes)andrinsedwell.Afterdrying,anewstringmaybeattached,sothepessaryisreadytobere-insertedthefollowingmorning.Boilingorsterilizingthepessaryisnotnecessary.
Overtime,pessariesmaybecomediscoloured.Theyonlyrequirereplacementifcracksdeveloponthesurface.
Youwillbeaskedtoreturnforafollowupcheckafterusingapessaryfor2-4weeks.
Itmighttakeafewtriestofindapessarythatprovidessupportswithoutcausingdiscomfort.(PhotocourtesySuperiorMedicalLimited.)

13
Is there a risk to using a pessary?
Apessaryisverysafewhenusersfollowtheinstructionsforcareandmanagement.Themainriskofusingapessaryisthedevelopmentofaninfectionorerosion(ulcer)inthevaginawhichcanresultinbleedingorafoulsmellingdischarge.Youshouldseeyourdoctorifyoudevelopthesesymptoms.Arestfromusingthepessarymaybenecessary.
Becauseemergenciesmayoccurwhereawomanisnotabletospeakforherself,sheshouldletsomeoneclosetoherknowaboutherpessaryusesoitcanberemoved.
PART II: TREATMENT OPTIONS
Pessary

14
SURGERY FOR STRESS INCONTINENCESurgerywillcureorreducestressincontinencein8outof10women.However,manywomenhavebothstressandurgeincontinence.Evenifstressincontinencegoesaway,theymaycontinueleakingbecauseofurgeincontinence.Thisisnotafailureofthesurgery.
Medicaltechnologyisalwayschanging,andnewoperationsarefrequentlyintroduced.Rightnowthemostcommonformofstressincontinenceoperation is a vaginal tape(meshtapeplacedundertheurethratohelpkeepitclosed).Whendonealone,thisprocedureisusuallydaysurgery(cometohospitalandgohomethesameday).
Ifyouareinterestedinsurgery,youwillmeetwithasurgeontodiscussyourcondition.Thesurgeonwilldescribethesurgicaloptionsavailable,andthetypeofoperationhe/shethinksisbestforyou.
About Surgery
Surgerycanbedoneunderlocal,spinal,orgeneralanesthetic.Withlocalorspinalanestheticonlythenervesofyourpelvicareaarefrozen.Withgeneralanestheticyouaregivenmedicationtorelaxyourwholebodyandputyoutosleepduringsurgery.Yourquestionsaboutanestheticcanbeansweredatyourpre-admissionclinicvisitorbyyoursurgeon.
Risks of Surgery
Risksofanysurgeryincludeinfectionatthesurgicalsite,bleeding,damagetosurroundingstructuresandanesthetic-relatedrisks.
Surgeryforstressincontinencemaycausethestreamofurinetoslowdown.Thisisnotconsideredasignificantproblem.However,thereisasmallriskthatthesurgerywillactuallymakeitdifficultforawomantourinate.Thisproblemisusuallytemporary,andrequiresthewomentourinatebyinsertingacatheter(tube)intoherbladder.Iftheproblemdoesn’tgoawaysoon,asecondsurgerymightberequired,butthisisrare.
Inrarecases,surgeryforstressincontinencecancauseurgeincontinencetogetworse.
Operationsthatusemeshorotherartificialmaterialmayhaveproblemssuchasexposureofthemesh,pain,orinfection.Thismayrequireremovalofpartorallofthematerial.
Pre-admission clinic visit
Thisvisit,ifrequired,takesplacepriortoyoursurgerydate.Nursesreviewyourhistory,answerquestions,andperformnecessarytests.Youmaybetaughthowtoputacatheter(tube)insideyourbladder.Youmayalsoseeananesthetistorothermedicalspecialist.
PART II: TREATMENT OPTIONS

15
Ifyouareusingmedicationforurgeincontinenceyoumaybeaskedtostopthemedicationadayortwobeforeyoursurgery.Besuretoaskyoursurgeonaboutuseofbladdermedicationsaroundthetimeofyoursurgery.
Postoperative care
• Youmayhavepaininyourincisionsanywherefromafewdaystoafewweeks.
• Donothavevaginalintercoursefor1month.
• Donotliftmorethan10lbsorperformheavyworkfor1month.Timeoffworkdependsonyourtypeofworkandthetypeofsurgeryperformed.
• Youcannotdriveuntilyoucansafelygiveallyourattentiontotheroadwithoutpainorsedationfrommedications.Youwillneedaridehomefromthehospital.
Yourquestionscanbeansweredatyourpre-admissionclinicvisitorbyyoursurgeon.
Yourquestionscanbeansweredatyourpre-admissionclinicorbyyoursurgeon.
PART II: TREATMENT OPTIONS

16 PART II: TREATMENT OPTIONS
SURGERY FOR VAGINAL PROLAPSESurgerywillcureprolapseinabout7outof10womenwhochoosethistreatment.Onaverage,3outof10womenwhohavesurgerywillhaveasecondsurgeryforprolapseatsomepointinthefuture.
Thetypeofsurgeryyouneeddependsontheorgansthatneedtoberepaired.Inadditiontoliftingprolapsedorganssuchasthebladderorbowel,yoursurgeonmightrecommendremovingtheuterus(hysterectomy)orliftingthetopofthevagina(vaultsuspension).Surgeryforprolapsecanalsobecombinedwithsurgeryforstressincontinence.
Ifyouareinterestedinsurgery,youwillmeetwithasurgeontodiscussyourcondition.Thesurgeonwilltalktoyouaboutyourconditionandthetypeofoperationhe/shethinksisbestforyou.
About the Surgery
Prolapsesurgeryusuallyisdonethroughthevaginabutdependingontheanatomyofthepatientandthetrainingofthesurgeon,itmaybedonethroughtheabdomen.Afterprolapsesurgery,patientsaretypicallyinhospitalfor1-3days.Dependingontheoperationplanned,apatientmayoccasionallybescheduledasdaysurgery.
Risks of Surgery
Risksofanysurgeryincludeinfectionatthesurgicalsite,bleedinganddamagetosurroundingstructures(bladderandbowel).Thereisalsosmallriskofnerveinjuryrelatedtoyourpositionduringsurgery,bloodclotinthelegs/lung,medicalcomplications(suchaspneumoniaandcardiacproblems),andanesthetic-relatedrisks.
Thereisasmallriskthatprolapsesurgerywillmakeitdifficultforawomantourinate.Thisproblemisusuallytemporary,andrequiresthewomentourinatebyinsertingacatheter(tube)intoherbladder.Inrarecases,surgeryforprolapsecancauseonsetofurinaryincontinence.Anotherriskofprolapsesurgeryisshortorlongtermpainwithintercourse.
Pre-admission clinic visit
Thisvisit,ifrequired,takesplacepriortoyoursurgerydate.Nursesreviewyourhistory,answerquestions,andperformtests.Youmaybetaughthowtoputacatheter(tube)insideyourbladder.Youmayalsobeseenbyananesthetistorothermedicalspecialists.
Postoperative care
• Ifyouhaveacatheter,itmayberemovedinhospital,oryoumaycomebacktohaveyourcatheterremovedfollowingyourdischarge.
• Vaginaldischargeandirregularsmallamountofbleedingarecommonduringyourrecovery.
• Paintypicallylastsforafewweeks,butdependsonthesurgeryperformedandthepatient.
• Donothavevaginalintercourseuntilexaminedbyyoursurgeonatyourpostoperativevisit.
• Donottoliftmorethan10lbsorperformheavyworkfor6weeks.Timeoffworkdependsonyourtypeofworkandthetypeofsurgeryperformed.
• Youcannotdriveuntilyoucansafelygiveallyourattentiontotheroadwithoutpainorsedationfrommedications.Youwillneedaridehomefromthehospital.
Ifyouhavequestions,theycanbeansweredatyourpre-admissionclinicvisitorbyyoursurgeon.
17
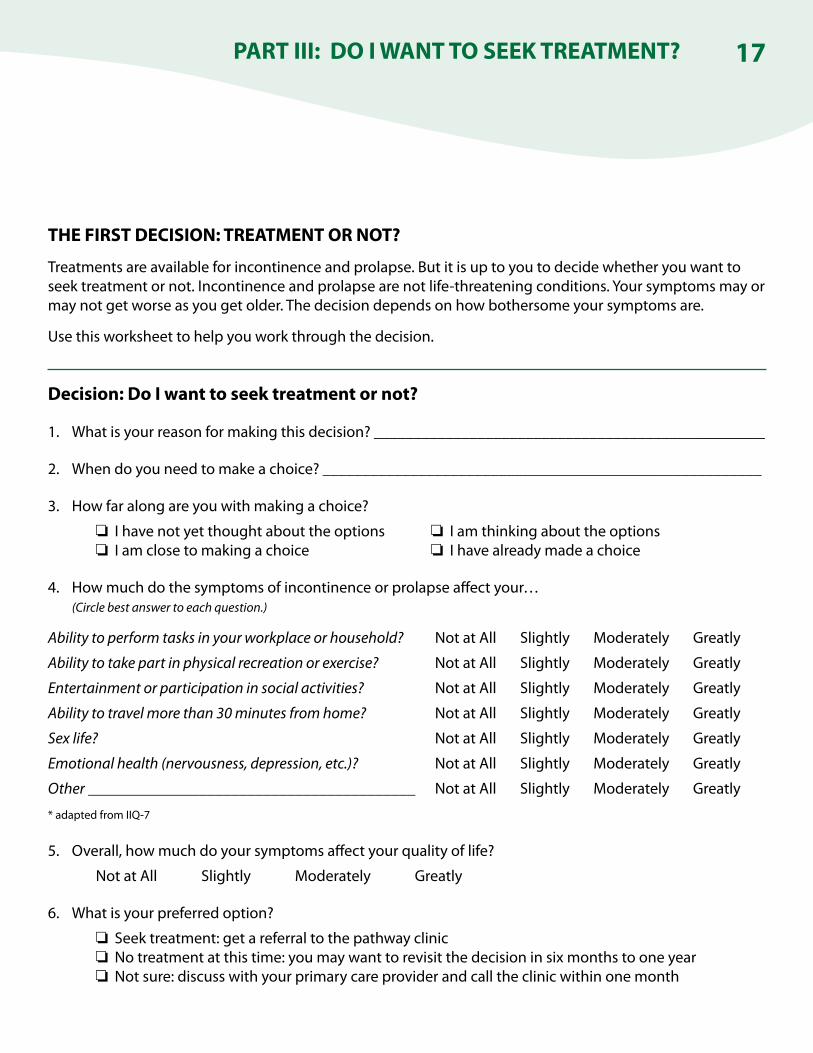
THE FIRST DECISION: TREATMENT OR NOT?
Treatmentsareavailableforincontinenceandprolapse.Butitisuptoyoutodecidewhetheryouwanttoseektreatmentornot.Incontinenceandprolapsearenotlife-threateningconditions.Yoursymptomsmayormaynotgetworseasyougetolder.Thedecisiondependsonhowbothersomeyoursymptomsare.
Usethisworksheettohelpyouworkthroughthedecision.
Decision: Do I want to seek treatment or not?
1. Whatisyourreasonformakingthisdecision?_________________________________________________
2. Whendoyouneedtomakeachoice?_______________________________________________________
3. Howfaralongareyouwithmakingachoice?
Ihavenotyetthoughtabouttheoptions Iamthinkingabouttheoptions Iamclosetomakingachoice Ihavealreadymadeachoice
4. Howmuchdothesymptomsofincontinenceorprolapseaffectyour… (Circle best answer to each question.)
Ability to perform tasks in your workplace or household? NotatAllSlightlyModeratelyGreatly
Ability to take part in physical recreation or exercise? NotatAllSlightlyModeratelyGreatly
Entertainment or participation in social activities? NotatAllSlightlyModeratelyGreatly
Ability to travel more than 30 minutes from home? NotatAllSlightlyModeratelyGreatly
Sex life? NotatAllSlightlyModeratelyGreatly
Emotional health (nervousness, depression, etc.)? NotatAllSlightlyModeratelyGreatly
Other_________________________________________ NotatAllSlightlyModeratelyGreatly
*adaptedfromIIQ-7
5. Overall,howmuchdoyoursymptomsaffectyourqualityoflife?
NotatAllSlightlyModeratelyGreatly
6. Whatisyourpreferredoption?
Seektreatment:getareferraltothepathwayclinic Notreatmentatthistime:youmaywanttorevisitthedecisioninsixmonthstooneyear Notsure:discusswithyourprimarycareproviderandcalltheclinicwithinonemonth
PART III: DO I WANT TO SEEK TREATMENT?
18
THE NEXT STEP
IfyoudecidetocontinueonthePathway,andseektreatmentforyourcondition,Step2isAssessment.AskyourdoctortoreferyoutoaPelvicFloorPathwayClinic(ifthishasnotalreadybeendone).YouwillneedtovisitaClinicinReginaorSaskatoon.
Beforeyourappointmentyouwillreceiveapackageofformsincluding:
amedicalhistoryform
athree-daybladderdiary(askingyoutorecordthetypeandamountoffluidyoudrink,thetimeandamountofurinevoided,andamountandnumberoftimesyouexperienceurineleakageoverathree-dayperiod)
questionnairesaboutyoursymptomsandhowtheyaffectyourqualityoflife
Your full cooperation is required in completing these forms and bringing them to your assessment appointment.
Atyourassessmentthehealthcareproviderwill:
Gooveryourformsandhistory
Discussyourproblemwithyou
Performatargetedphysicalexam including a pelvic examinationtoassessforprolapseandpelvicfloormusclestrength
Thehealthcareproviderwillhelpyoucomparetreatmentoptionsopentoyouandchoosefrom:
Pelvicfloorphysicaltherapy
Medication
Pessary
Surgery
Anytreatmentwillinvolvefurtherappointments,andsomewillrequiremoredetailedtestsandpelvicexaminations.Forsomeprograms,waittimesmayapply.
PART IV: ASSESSMENT & DIAGNOSIS

19
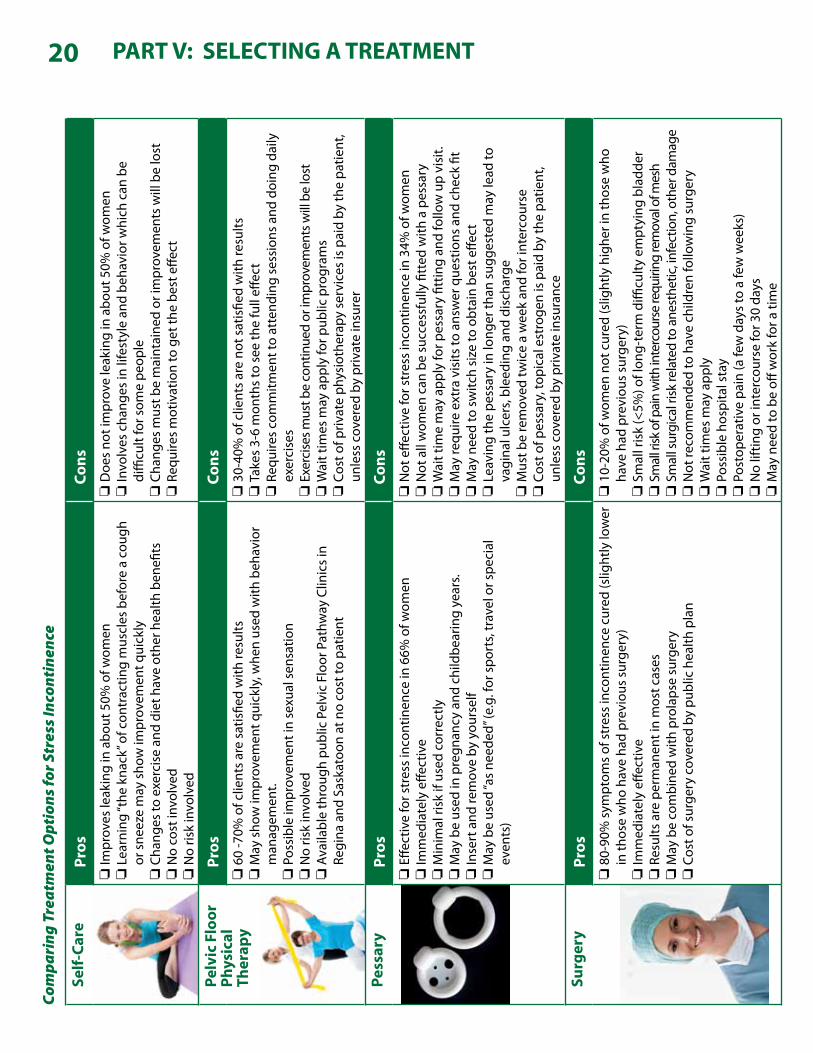
SELECTING A TREATMENT
Onceyouhaveacompleteassessmentandadetaileddiagnosis,youwillbereadymakeatreatmentchoice.Whetheryouareaffectedbyurgeincontinence,stressincontinence,vaginalprolapse,oracombinationofallthree,youwillfindthatthereareseveraltreatmentoptionsavailable.Yourhealthcareproviderwillhelptoexplainaboutyourconditionandthetreatmentoptions,butthedecisionabouttreatmentismadebyyou.
Itcanbehardtomakeachoicewhenthereareseveralgoodoptionsavailable.Itisagoodideatomakealistofallthetreatmentoptionsforyourcondition,andgatherinformationaboutthepositivesandnegativesofeachoption.Onthefollowingpages,youwillfindchartsthatsummarizetheprosandconsofeachtreatmentdiscussedinthisbooklet.Youmaywanttogetinformationfromothertrustedsources,too.Makealistofanyquestionsyouwanttoaskwhenyoumeetyourhealthcareprovider.
Onceyouhavereviewedalltheinformationabouttreatmentoptions,youmightbeabletoeliminatesomeoptions.Onthechartsprovided,youcancheckthe“pros”thatareveryimportanttoyou,orthe“cons”thatarenotacceptable.Thenyoucanmakeatentativedecisionaboutwhichtreatmentyouwanttotry.
WhenyouvisitthePelvicFloorPathwayClinic,ahealthcareproviderwillalsohelpyouthroughthestepsofthisdecision-makingprocessandletyouknowifyouroptionsarelimitedbyyourphysical
conditionand/oryourmedicalhistory.Explaintoyourhealthcareproviderwhichtreatmentyoutentativelyselected,andwhy.Yourhealthcareproviderwantsyoutomakeaninformedchoicethatisrightforyou.
Onceyouhaveselectedatreatment,pleasedoyourbesttofollowinstructionsandputeffortintoimprovingyourcondition.Butifthetreatmentyouselectdoesn’tseemtobehelping,youcanreturntothePelvicFloorPathwayClinicandbeginthedecisionmakingprocessagain.
PART V: SELECTING A TREATMENT
20 PART V: SELECTING A TREATMENTCo
mpa
ring
Tre
atm
ent O
ptio
ns fo
r Str
ess I
ncon
tine
nce
Self-
Care
Pros
Cons
Im
prov
esle
akinginabo
ut50%
ofw
omen
Lea
rning“the
kna
ck”o
fcon
trac
tingm
uscles
befor
eaco
ugh
orsne
ezem
aysho
wim
prov
emen
tquick
lyC
hang
esto
exe
rcisean
ddiet
hav
eot
herh
ealth
ben
efits
N
oco
stin
volved
N
oris
kinvo
lved
D
oesno
tim
prov
eleak
inginabo
ut50%
ofw
omen
In
volves
cha
nges
inlifestylean
dbe
havior
which
can
be
diffi
cultfo
rsom
epe
ople
C
hang
esm
ustb
em
aint
aine
dor
impr
ovem
entsw
illbelost
Req
uire
sm
otivationto
get
thebe
steffe
ct
Pelv
ic F
loor
Ph
ysic
al
Ther
apy
Pros
Cons
60-7
0%ofc
lient
saresa
tisfie
dwith
resu
ltsM
aysho
wim
prov
emen
tquick
ly,w
henus
edw
ithbeh
avior
man
agem
ent.
Pos
sibleim
prov
emen
tinse
xualsen
satio
nN
oris
kinvo
lved
A
vaila
bleth
roug
hpu
blicPelvicFloo
rPathw
ayClin
icsin
Regina
and
Sas
kato
onatn
oco
stto
patient
30-
40%ofc
lient
sareno
tsatisfie
dwith
resu
ltsTak
es3-6
mon
thsto
see
thefu
lleff
ect
Req
uire
sco
mm
itmen
ttoatte
ndingse
ssions
and
doing
daily
exer
cise
s
Exe
rcise
smus
tbeco
ntinue
dor
impr
ovem
entsw
illbelost
W
aitt
imes
may
app
lyfo
rpub
licpro
gram
sC
osto
fpriv
ateph
ysioth
erap
yse
rvices
ispaidby
thepa
tient
,un
lesscov
ered
bypr
ivateinsu
rer
Pess
ary
Pros
Cons
Effe
ctivefo
rstres
sinco
ntinen
cein
66%
ofw
omen
Im
med
iate
lyeffe
ctive
M
inim
alrisk
ifuse
dco
rrec
tlyM
aybeus
edin
pre
gnan
cyand
childbe
aringye
ars.
In
sertand
rem
oveby
you
rself
M
aybeus
ed“a
sne
eded
”(e.g.fo
rspo
rts,trav
elors
pecial
even
ts)
N
oteffe
ctivefo
rstres
sinco
ntinen
cein
34%
ofw
omen
N
otallwom
encan
besu
cces
sfullyfitted
with
apes
sary
W
aitt
imem
ayapp
lyfo
rpes
sary
fittingan
dfo
llowupvisit.
M
ayre
quire
extravisits
toans
wer
que
stions
and
che
ckfit
M
aynee
dto
switc
hsize
toobt
ainbe
steffe
ctLea
ving
thepe
ssar
yinlo
nger
than
sug
gested
may
lead
to
vagina
lulcer
s,blee
ding
and
disch
arge
M
ustb
ere
mov
edtw
iceawee
kan
dfo
rint
erco
urse
C
osto
fpes
sary,top
icalestro
genispaidby
thepa
tient
, un
lesscov
ered
bypr
ivateinsu
ranc
e
Surg
ery
Pros
Cons
80-
90%sym
ptom
sof
stres
sinco
ntinen
cecur
ed(s
light
lylo
wer
inth
osewho
hav
eha
dpr
evious
sur
gery
)Im
med
iate
lyeffe
ctive
Res
ultsare
per
man
entinm
ostc
ases
M
aybeco
mbine
dwith
pro
laps
esu
rger
yC
osto
fsur
gery
cov
ered
bypu
blichea
lthplan
10-
20%ofw
omen
not
cur
ed(s
light
lyhighe
rinth
osewho
ha
vehad
pre
viou
ssu
rger
y)Sm
allrisk(<
5%)o
flon
g-te
rmdiffi
culty
em
ptying
bladd
er
Smallrisk
ofp
ainwith
intercou
rserequ
iring
remov
alofm
esh
Sm
allsur
gica
lrisk
relatedto
ane
sthe
tic,in
fection,oth
erdam
age
N
otre
com
men
dedto
hav
ech
ildre
nfo
llowingsu
rger
yW
aitt
imes
may
app
lyPos
sibleho
spita
lstay
Pos
tope
rativ
epa
in(a
fewday
sto
afe
ww
eeks
)N
oliftin
gor
inte
rcou
rsefo
r30da
ysM
aynee
dto
beoff
wor
kfo
ratim
e

21PART V: SELECTING A TREATMENTCo
mpa
ring
Tre
atm
ent O
ptio
ns fo
r Urg
e In
cont
inen
ce
Self-
Care
Pros
Cons
Im
prov
esle
akinginabo
ut50%
ofw
omen
Elim
inatingca
ffeinesh
owseff
ectsafter
1-2
wee
ksFluidm
anag
emen
tand
toile
tingm
anag
emen
tmay
hav
eim
med
iate
effe
ctN
oco
stin
volved
N
oris
kinvo
lved
D
oesno
tim
prov
eleak
inginabo
ut50%
ofw
omen
In
volves
cha
nges
inlifestylean
dbe
havior
,which
can
be
diffi
cultfo
rsom
epe
ople
Pelv
ic F
loor
Ph
ysic
al
Ther
apy
Pros
Cons
60-7
0%ofc
lient
saresa
tisfie
dwith
resu
ltsM
aysho
wim
prov
emen
tquick
lyw
henus
edw
ithfr
eeze
and
sq
ueez
eM
aybeab
leto
disco
ntinue
urg
einco
ntinen
cem
edication
Pos
sibleim
prov
emen
tinse
xualsen
satio
nN
oris
kinvo
lved
A
vaila
bleth
roug
hpu
blicPelvicFloo
rClin
icsinReg
inaan
dSa
skatoo
natnoco
stto
patient
30-
40%ofc
lient
sareno
tsatisfie
dwith
resu
ltsTak
es3-6
mon
thsto
see
thefu
lleff
ect
Req
uire
sco
mm
itmen
ttoatte
ndingse
ssions
and
doing
daily
exer
cise
sExe
rcises
mus
tbem
aint
aine
dor
impr
ovem
entsw
illbelost
W
aitt
imes
may
app
lyfo
rpub
licpro
gram
sC
osto
fpriv
ateph
ysioth
erap
yse
rvices
ispaidby
thepa
tient
,un
lesscov
ered
bypr
ivateinsu
rer
Med
icat
ions
Pros
Cons
Im
prov
esle
akingin50-
60%ofw
omen
O
xybu
tininta
kes1-
2wee
ksto
see
fulleff
ect
O
ther
med
ications
take
abo
ut1m
onth
O
xybu
tininis
fastactingan
dca
nbe
use
don
anoc
casion
al
basi
sSideeff
ectsgoaw
ayw
henm
edicationissto
pped
D
oesno
tim
prov
eleak
ingin40-
50%ofw
omen
Sideeff
ectsin
clud
edr
ym
outh
,dry
eye
s,stom
achup
set,
cons
tipationan
dblur
redvision
N
otre
com
men
dedifpr
egna
ntort
ryingto
con
ceive
H
assleof
rem
embe
ringto
take
them
edicationre
gularly
N
eedto
talkto
doc
toro
rnur
sepractition
erfr
eque
ntlyunt
ilth
ebe
stm
edicationan
ddo
seis
det
erm
ined
Sym
ptom
sre
turn
ifyou
sto
pta
king
them
edication
C
osto
fmed
ications
ispaidby
thepa
tient
,unles
sco
vere
dby
pr
ivateinsu
rer

22 PART V: SELECTING A TREATMENTCo
mpa
ring
Tre
atm
ent O
ptio
ns fo
r Vag
inal
Pro
laps
e
Pelv
ic F
loor
Ph
ysic
al
Ther
apy
Pros
Cons
Som
eim
prov
emen
twhe
nm
ildpro
laps
eispre
sent
Im
prov
emen
tinblad
dera
ndbow
elem
ptying
with
toile
ting
tech
niqu
esPos
sibleim
prov
emen
tinse
xualsen
satio
nN
oris
kinvo
lved
A
vaila
bleth
roug
hpu
blicPelvicFloo
rPathw
ayClin
icsin
Regina
and
Sas
kato
onatn
oco
stto
patient
Signific
antim
prov
emen
tofp
rolaps
esy
mpt
omsisnot
ex
pected
Tak
es3-6
mon
thsto
see
thefu
lleff
ect
Req
uire
sco
mm
itmen
ttoatte
ndingse
ssions
and
doing
daily
exer
cise
sExe
rcises
mus
tbeco
ntinuo
usorim
prov
emen
tsm
aybelost
W
aitt
imes
may
app
lyfo
rpub
licpro
gram
sC
osto
fpriv
ateph
ysioth
erap
yse
rvices
ispaidby
thepa
tient
,un
lesscov
ered
bypr
ivateinsu
rer
Pess
ary
Pros
Cons
Im
med
iate
,com
fortab
lere
liefo
fvag
inalpre
ssur
efo
rmos
twom
enM
inim
alrisk
ifuse
dco
rrec
tlyM
aybeus
edin
pre
gnan
cyand
childbe
aringye
ars
In
sertand
rem
oveby
you
rself
M
aybeus
ed“a
sne
eded
”(e.g.spo
rts,trav
el,s
pecialeve
nts)
N
otallwom
encan
besu
cces
sfullyfitted
with
apes
sary
W
aitt
imem
ayapp
lyfo
rpes
sary
fittingan
dfo
llowupvisit.
M
ayre
quire
1or2
extravisits
toans
wer
que
stions
and
ch
eckfit
M
aynee
dto
switc
hsize
toobt
ainbe
steffe
ct.
Lea
ving
thepe
ssar
yinlo
nger
than
sug
gested
may
lead
to
vagina
lulcer
s,blee
ding
and
disch
arge
M
ustb
ere
mov
edtw
iceawee
kan
dfo
rint
erco
urse
C
osto
fpes
sary,top
icalestro
genispaidby
thepa
tient
,unles
sco
vere
dby
priv
ateinsu
rer
Surg
ery
Pros
Cons
70-
75%cha
nceof
long
term
impr
ovem
ent
Im
med
iate
lyeffe
ctive
M
aybeco
mbine
dwith
stres
sinco
ntinen
cesur
gery
C
osto
fsur
gery
cov
ered
bypu
blichea
lthplan
25-
30%cha
nceof
not
hav
inglong
term
suc
cess
Sm
allrisk(le
ssth
an5%)r
elated
toane
sthe
ticand
sur
gery
Sm
allriskof
painwith
inte
rcou
rsefrom
nar
rowingof
vag
ina
orte
nder
nessin
incision
sN
otre
com
men
dedto
hav
ech
ildre
nfo
llowingsu
rger
yW
aitt
imes
may
app
ly1-3
day
hos
pita
lstay
M
aygoho
mewith
acathe
ter
N
oliftin
gallowed
for6
wee
ksN
ointe
rcou
rseallowed
for6
wee
ks
N
eedto
beoff
wor
kfo
r6w
eeks


www.health.gov.sk.ca/pelvic-floor