influence of exposure to microbes and polluents on the development of atopy and asthma prof. dr....
TRANSCRIPT

Influence of exposure to microbes and polluents on the
development ofatopy and asthma
Prof. dr. K.Desager
Department of Pediatrics
University of Antwerp
Dr C. Vael
Department of Microbiology
University of Antwerp

Hygiene hypothesis
Rising prevalence of atopic disorders in infants and children
‘Westernized life style’ Modified pattern of microbial
exposure in young children

Asthma phenotypes
Martinez 2002

Asthma Predictive Index< 3 yr and frequent episodes of wheeze
2 minor criteria:
allergic rhinitis
Wheeze without cold
eosinophilia
75% : active asthma at school age
1 major criterium
Parental asthma
atopic dermatitisofor
enand
Castro-Rodriguez AJRCCM 2000;162: 1403 -1406

Aim
to evaluate the bacterial flora of infants in relation to environmental pressure and to atopy

Materials and methods
Prospective cohort study: started 10/2002
• recruitment of 159 healthy neonates• cord blood polluents: Cd, Pb, DDE, PCB, dioxine• fecal sampling: 3w, 6m,12m n= 431• questionnaires: prenatal, 3w, every 6 mths till 3yr• clinical, eNO, SPT: 3 yr

Characteristic Number %
Metropolitan 102/158 65
Sex (male) 73/138 53
Mother dd astma ever 12/147 8
Father dd asthma ever 8/138 6
Skin Prick Test positive 15/116 13
Positive mAPI 18/111 16
0
5
10
15
20
25
30
wheeze

Regional differences
Characteristic metropolitan rural p
mAPI 29% 24% 0.67
SPT 18% 4% 0.045*
parental asthma 19% 4% 0.01*
antibiotics yr1 48% 55% 0.48
passive smoke 12% 21% 0.22
Outcome SPT OR 95% Confidence intervals
Parental asthma 4,1* 1,1 15,7
Passive smoke 1,9 0,3 11,6
Region (metropolitan vs rural) 4,0 0,8 20,1

eNO
• In 121 children eNO attempted.– technical difficulties: 14– refusal: 11 children– leakage or irregular breathing: 43 – acceptable measurements: 38 (min 2 and max 5
attempts)
• SPT: 15 positive SPT for at least one allergen– grass pollen: 6– house dust mite: 10– egg: 3– cow’s milk: 2

eNO - mAPI
• children with positive mAPI were differentiated from those with negative mAPI at eNO of 3.4 ppb
• sensitivity: 71% • specificity: 71%
mAPI
negative positive
eNO(ppb)
< 3.4 17 4
> 3.4 7 10
(p < 0.05 )

eNO - SPT
• cut-off value reflecting the best combination of sensitivity and specificity occurred at 4.9 ppb
• sensitivity: 80%• specificity: 88%
SPT
negative positive
eNO(ppb)
<4.9 29 1
>4.9 4 4
(p < 0.05 )

Wheeze 2 yrFamily history asthma or allergy
+
Birth weight +
Birth height +
Sex +
Pb cord blood +
DDE cord blood +
Antibiotics +
Effect Point Estimate
95% WaldConfidence Limits
Birth height 1,603 1,196 2,149
DDE (fat, LOG) 1,930 1,078 3,454
Number of days antibiotics 1,093 1,038 1,150
polluents

Sunyer Env Health Persp 2005; 113: 1787
DDE - wheeze

DDE - asthma
• causal pathway DDE and asthma?• Immune system: associated with changes in
– immune cells (Vine 2001)– immunoglobulins (Cooper et al. 2004; Vine 2001)– cytokines (Bilrha 2003; Daniel 2002)
• hormone-like activity of DDE: – interfere with mast cells in airways that express
estrogen/progesterone receptors, favoring the role of DDE in TH2 immune differentiation
– Direct effect on the airway through altering b2-adrenergic responsiveness and increasing the production of prostaglandins

conclusions
• Region: No difference mApi, less sensitisation in rural region due to less parental asthma
• eNo relationship with mAPI– Difficult to perform in 3 yr old– in agreement with data in older children, adults: atopy,
family history
• Prenatal exposure DDE related to wheeze 2 yrs– In agreement Sunyer

Factors modifying infant gut flora
1. Breastfeeding: because fecal pH? (3w)
Lactobacilli/Streptococci
Bifidobacteria
Bacteroides
2. Cesarian delivery: delayed colonization?
Bifidobacterium(1w)
Bacteroides (6m!)
Clostridium perfringens (1m)
(Harmsen H., J.Ped. Gastr.Nutr.,2000)
(Gronlund M., J.Ped.Gastr.Nutr.,1999)

Infant GI flora in allergy/atopy
3. Allergy/Atopy:
Lactobacillus (24m)
Bifidobacterium (1w,3m,12m,24m)
Bacteroides (12m,24m)
Enterococcus (1w,1m)
Clostridia (3m)
S. aureus (6m)
Yeasts (3m)
Early (<3m): Clostridium, Yeasts, Enterococcus, Bifidobacterium
Late (>3m): Lactobacillus,Bifidobacterium,Bacteroides,S. aureus
other species
(Bjorksten B.,Cl.Exp.All.,1999)
(Bjorksten B.,JACI,2001)
(Kalliomaki, JACI,2001)
(Ouwehand A.,JACI,2001)

Results: Breast feeding at age 3 weeks
Log CFU/g
0 1 2
enkel BV BV en FV FV
0,00
2,00
4,00
6,00
8,00
10,00 Bifidobacteria
Enterococcus
Clostridium
(p<0.01 Kruskal-Wallis)
Feeding Number(%)
BF 88 (57)
BF+FF 21 (14)
FF 45 (29)
BF: breast feeding
FF: formula feeding
BF BF+FF FF

Results: Breast feeding at age 6 months
,00 1,00 2,00
BV BV+FV FV
0,00
2,00
4,00
6,00
8,00
10,00 Stafylococcus
Bacteroides
LactobacillusFeeding Number (%)
BF 14 (10)
BF+FF 19 (13)
FF 109 (77)
Log CFU/g
(p<0.05 , * P = 0.08, Kruskal-Wallis)
*
BF: breast feedingFF: formula feeding
BF BF+FF FF

Results: wheezing at age 1 year
0 1
neen piepen 12m ja
0,00
2,00
4,00
6,00
8,00
10,00 Bacteroides 3w
Bacteroides 6m
Tot.Anaeroben 3w
Gr Neg aeroob 12m
(p < 0.05 Mann-Whitney U )
Log CFU/gWheezing
Nr of children (%)
Yes No
33 (21) 126
non-wheezers at 1 year wheezers
Tot. Anaerobes
3w
MCC
1 yr
Bacteroides
6m
Bacteroides
3w

,00 1,00
mAPI
0,00
2,00
4,00
6,00
8,00
10,00logBBE
logCAA
mAPI at age 3 years
Log CFU/g
(p < 0.05 Mann-Whitney U )
mAPI
Nr of children (%)
Yes No
33 (27) 88
Bacteroides 3w
Tot. Anaerobes 3w
Neg. Pos.

Bacteroides culture 3 wks - mAPI
mAPI
Bacteroides colonisation
Neg Pos
Neg 59 7
Pos 34 11
Specif.63%
Sens.
61%
pos. mAPI prevalence = 16%
(p < 0.05 Fisher exact)

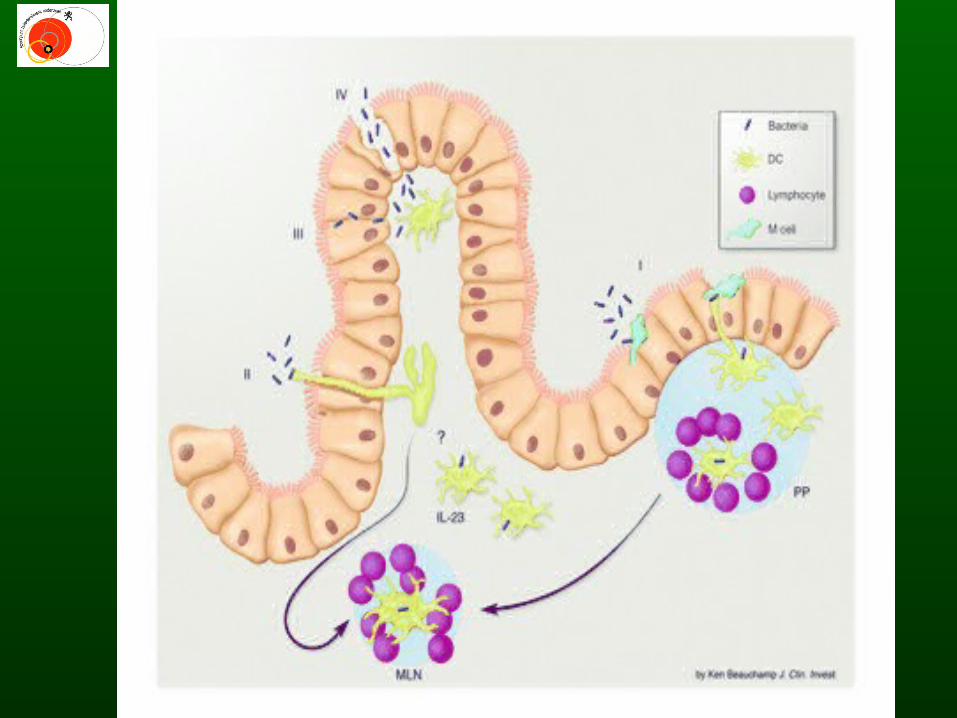
Toll-like receptors and intestinal microflora
Gr. pos bact. (Staf., PG) TLR 2 Th2Asthma
Bacteroides Lipoprotein *
Gr. neg. bact. (E. coli, LPS) TLR 4 Th1
(Agrawal S, J immunol., 2003)
* (Netea M. et al., Eur. J. Imm., 2004)

Copyright ©2002 BMJ Publishing Group Ltd.
Kirjavainen, P V et al. Gut 2002;51:51-55
Figure 1 Scattergram showing faecal concentrations of bacteroides and Escherichia coli versus serum total IgE concentration in each individual. Regression lines with 95% confidence intervals
(broken lines); Spearman's rho and p values are given for both slopes. HSG, highly sensitised group; SG, sensitised group.
2) 716 high school children:
If atopic disease
significantly higher Bacteroides vulgatus IgG titers
(Fukuda S et al., J.Adolesc. Health, 2004)
1)

Conclusions:
• Breastfeeding during the first year of life has an influence on the infant intestinal microflora.
• Changes in the intestinal flora in the first month of life are associated with wheezing at the age of 1 year and mAPI at the age of 3 years.
• Early postnatal intestinal colonization with Bacteroides fragilis is associated with a positive mAPI. Children with a positive mAPI have a 4 -10x higher risk of having subsequent asthma (age 6-13y).
Funded by the Flemish government within the project :
“Health and Environment, subdivision Asthma”.

Weisglas-Kuperus Tox lett 2004
Corrected breastfeeding, parity, education, smoking, fam history atopy, daycare
PCB’s: immunomodulating?

DDE - infections
• decreased response to viruses, bacteria?
• inconsistent results– moderate increase of acute infections during
first year of life (Dallaire et al. 2004)– not in 343 German school children (Karmaus
et al. 2003) – not in 207 Dutch infants (Weisglas-Kuperus et
al. 1995)

DDE – immunity, asthma
• changes in T-cell– mediated immune cytokines related with allergy (IL-4) (Bilrha 2003; Daniel 2002)
• similar effects: hexachlorobenzene (HCB) (Michielsen 1999) and polychlorinated biphenyls (PCBs) (Van Den Heuvel 2002)
• cross-sectional study school children Germany DDE related with increases in total IgE and asthma (Karmaus 2001, 2003)
• increase of asthma prevalence, mortality in adults was found among an older cohort of DDT sprayers (Beard 2003)
• prevalence of wheeze increased with a variety of pesticides among current applicators (Hoppin 2002)