influence acute myocardial...
TRANSCRIPT

Influence of Acute Myocardial Depression
on Left Ventricular Stiffness
and Its Elastic and Viscous Components
GORDONH. TEMPLETON,KEENWILDENTHAL, JAMEST. WALRSON,andJERE H. MnrrcEL
From the Department of Physiology and the Pauline and Adolph WeinbergerLaboratory for Cardiopulmonary Research of the Department of InternalMedicine, University of Texas Health Science Center at Dallas, SouthwesternMedical School, Dallas, Texas 75235
A B S T R A C T The influence of acute myocardial de-pression on ventricular stiffness and on its elastic andviscous components was studied in 19 dogs. After theanimals were placed on cardiopulmonary bypass, stiff-ness was measured by sinusoidally injecting volumechanges of 0.5 ml (AV) at 22 Hz into paced, isovolu-mically contracting left ventricles and determining theamplitude (AP) of the sinusoidal pressure response.Stiffness was linearly related to pressure (P) through-out the cardiac cycle, so that AP/AV = aP + A, wherea and i are constants. Myocardial depression was in-duced in one of three different ways: by coronary arteryligation, by administration of propranolol (Inderal), orby administration of pentobarbital. All three interven-tions caused significant increases in the slope, a, of thestiffness-pressure relationship, while the intercept, A,remained unchanged. Release of the coronary occlusionor administration of acetylstrophanthidin partially re-versed depression and the change in a. Approximationof the mechanical nature of the left ventricle in termsof a linear second-order mechanical system permittedthe division of stiffness into its elastic and viscous com-ponents. Like total stiffness, both the elastic and theviscous components were linearly related to ventricularpressure. Elastic stiffness was not changed, but theslope of the line relating viscous stiffness to pressurewas significantly increased during ischemic depression,
Dr. Wildenthal holds a Research Career DevelopmentAward (HL 70125) from the National Heart and LungInstitute, and Dr. Willerson is an Established Investigatorof the American Heart Association, Inc.
Received for publication 6 November 1974 and in revisedform 9 April 1975.
indicating that a change in viscosity was primarily re-sponsible for the increase in total ventricular stiffness.
INTRODUCTIONMany interventions that alter left ventricular perform-ance have been tested for their simultaneous effects ondiastolic stiffness. Tests of alterations in systolic stiff-ness, on the other hand, have seldom been attempted,primarily because appropriate techniques have not beenavailable. For instance, the quick-release technique,widely used to measure mechanical properties in iso-lated papillary muscles, has not been extended to study-ing ventricular mechanical properties because of thetechnical difficulties involved. A new method for mea-suring ventricular stiffness has recently been devel-oped in our laboratory, and this technique provides ameans not only for measuring total ventricular stiffnessat multiple times throughout the cardiac cycle, but alsofor separating stiffness into its viscous and elasticcomponents.
It is well known that large changes in tension devel-opment can alter diastolic stiffness through a mecha-nism involving stress relaxation (1-5). Effects of largechanges in tension development on systolic stiffness,however, have not been defined. Accordingly, in thepresent study we have turned our attention toward de-termining whether and to what extent systolic stiffnessis altered during severe ventricular depression and re-duction in tension development.
METHODSA detailed description of the method used for measuringventricular stiffness has been presented previously, along
The Journal of Clinical Investigation Volume 56 August 1975- 278-285278

with theoretical consideration of the analysis and an evalua-tion of the technique (6-11). The present study utilizedsodium pentobarbital anesthesia (30 mg/kg) for 19 mongreldogs; next, a midline thoracotomy was performed and eachdog was placed on complete cardiopulmonary bypass. Theextracorporeal circuit consisted of an oxygenator, a heatexchanger, and a roller pump. Heart block was producedby ligation of the bundle of His in the atrial septum, andthe heart was subsequently paced at 120 beats/min by aGrass stimulator through electrodes sutured to the rightventricle (Grass Instrument Co., Quincy, Mass.). The leftventricle was made isovolumic by occlusion of the inflowand outflow tracts with Teflon buttons and insertion of adistensible balloon into the chamber through a stab incisionin the apex of the heart. Thebesian blood was not allowedto accumulate between the balloon and endocardium but wasdrained continuously through perforations in the mitral but-ton and around the stab incision.
The ventricular balloon was attached to a metal cannulathrough which the balloon was filled with 20-25 ml of salineuntil a diastolic pressure of between 1 and 5 mmHg wasobtained. A piston located at the external end of the can-nula was driven sinusoidally at 22 Hz to produce a peakvolume change in the ventricle of 0.5 ml. For this amplitudeand frequency, measurable sinusoidal pressure changes pro-duced in the ventricle during both diastole and systole weremeasured with a Konigsberg P21 pressure transducer insidethe balloon (Konigsberg Instruments, Inc., Pasadena,Calif.). The stiffness of the balloon was negligible, and theinherent time delay at 22 Hz between the peak of a pressurecycle and a volume cycle for the system without the heartwas zero for operating pressures below 90 mmHg and 60above 90 mm Hg. The amount of friction between theballoon and endocardium at a frequency of 22 Hz wasassumed to be negligible.
The pacing stimuli, left ventricular pressure with its sinu-soidal response, and the sinusoidal volume displacement, asrecorded by a differential transformer connected to the shaftof the piston, were recorded on analog tape during the ex-periments and later were processed on PDP-12 and PDP-10computers (Digital Equipment Corp., Cleveland, Ohio).The pacing stimulus, which was in synchronization with apreset number of volume cycles, was used to trigger thecomputer to begin digitizing the ventricular pressure andthe volumetric displacement wave forms at a sampling rateof 1,000/s. 16 successive pressure and volume wave formswere averaged to yield single pressure and volume waveforms to remove nonperiodic noise arising from equipmentvibration. Fourier series analysis was performed on theventricular pressure wave form. This analysis assumes thatthe pressure wave form consists of a finite number of sineand cosine waves, whose frequencies are multiples or har-monics of the fundamental frequency or heart rate. Bychoosing a perturbation frequency of 22 Hz, the pressureresponse to the volumetric forcing function is contained inharmonics higher than those harmonics contained in an un-perturbed ventricular pressure waveform. Consequently, byeliminating the lower-order harmonics (first to the eighth)that constitute the unperturbed ventricular pressure waveform for one cardiac cycle and resynthesizing the higher-order harmonics (above the eighth), a wave form that is afunction of the volumetric forcing function can be con-structed. The use of Fourier analysis to filter the sinusoidalpressure response from the perturbed pressure wave formgives essentially the same results as subtracting an unper-turbed pressure wave form from a perturbed one (9). Thepressure wave form obtained by Fourier analysis is sinus-
oidal, having a frequency of 22 Hz and a varying peakamplitude that increases in size during contraction and de-creases during relaxation. The peak amplitude (AP) ' foreach perturbation divided by the change in volume thatproduced it (AV) is defined as volume stiffness (AP/AV),and analysis of the entire contraction cycle yields 22 valuesfor volume stiffness at varying pressures. For each experi-mental condition, ventricular stiffness (AP/AV) was foundto be linearly related to ventricular pressure (P) through-out the cardiac cycle (r> 0.94, Fig. 1): AP/AV= aP + ,where a and p were the slope and intercept with the ordi-nate, respectively. From this expression, it is seen that theunits for the slope and intercept are (ml)-' and (mm Hg)/ml, respectively. Previous studies conducted in our labora-tory have shown that changes in ventricular volume, heartrate, norepinephrine (8), coronary blood flow (10), andserum osmolality (9) have not altered the linearity of therelationship between stiffness and pressure.
To divide stiffness into its elastic and viscous compo-nents, the response of the mechanical system, consisting ofthe piston, steel cannula, balloon, and left ventricle, wasassumed to be that of a linear second-order system. Justifi-cation for this assumption has been discussed in detail pre-viously (7, 11). In short, the assumption of system linearityis based on the experimental observation that the pressureresponse of the system to the sinusoidal volumetric forcingfunction is also sinusoidal. A second-order system is assumedsince it was observed experimentally that the peak of eachpressure cycle occurred before the peak of the nearest vol-ume cycle. This observation implies that the system has notonly a static or elastic response but a dynamic response dueto both viscosity and inertia.
Accordingly, the mechanical system, consisting of thepiston, connecting cannula, balloon, and left ventricle, isrepresented by this equation of motion:
1 d2P(t) 1 dP(t) 1 __ 1 d2V(t)K dt2 - dt m a dt2 (1)
where K is elastic stiffness, 77 is viscous damping, in is theequivalent mass, and a is a constant relating linear displace-ment to spherical volume changes. The sinusoidal forcingfunction, V(t), and the system pressure response for agiven ventricular pressure, P(t), are sinusoids and may beexpressed as follows:
V(t) = Vo cos wt,
P(t) = Po cos (wt + TI), (2)where Vo and Po are amplitudes of volume and pressure,ZZa is angular frequency, and * is the difference in timebetween the occurrence of the peak of a pressure cycle andthe peak of a volume cycle. By making ' positive, the pres-sure sinusoid leads the volume sinusoid in time as observedexperimentally. For a linear system in which pressure andvolume are the parameters, Eq. 1 demonstrates that thepressure of the elastic, viscous, and inertial elements areproportional to volume and its first and second derivativeswith time, respectively. For instance, by setting the firsttwo terms in the sum appearing in Eq. 1 at zero, Newton'ssecond law of motion is obtained.
'Abbreviations used in this paper: a, slope of stiffness-pressure relationship; A, intercept of stiffness-pressure re-lationship; LAD, left anterior descending; AP/AV, volumestiffness.
Myocardial Stiffness after Contractile Depression 279
Substituting Eq. 2 into 1 and solving for the conditionswhere the first and second derivatives of V(t) with respectto time are zero yield expressions for elastic and viscousstiffness, respectively, at any particular ventricular pressure.
A ~~amu; PoElastic stiffness = K = Vo mw2os '+ Poa (3)
Viscous stiffness-= = Vo sin (4)
These expressions are functions of the ventricular stiff-ness (Po/Vo) and the phase angle (I) both of which canbe measured from the recordings of sinusoidal volume vari-ation and the pressure response of the system obtained byFourier analysis.
In Eq. 1, the coefficients K, to, and m are constant. How-ever, Eq. 3 shows elastic stiffness or K to be dependentupon stiffness and the phase angle, both of which areobserved to vary directly with pressure during the cardiaccycle. Consequently, Eq. 1 applies only when stiffness andthe phase angle are constant, which in turn is true whenpressure is constant, as during diastole. To broaden thescope of the model to include systole as well as diastole,the dynamic response of the left ventricle is modeled piece-wise. That is, it is assumed that at a given developedpressure of the ventricle and a given active state of themuscle, the response to a single sinusoidal volume cycle isgiven by the equation of motion (Eq. 1) with constant co-efficients. Moreover, it is assumed that since the developedpressure and active state are changing relatively slowly withrespect to the period of each volume perturbation, eachpressure cycle can be analyzed as if it were one period of apure sinusoidal pressure response at that particular developedpressure and active state.
The chosen equation of motion (Eq. 1) contains mass.The value chosen for mass in the calculations was the sumof the fluid mass in the balloon and cannula plus the massof the left ventricle. This is an approximation of the trueeffective mass of the system. This use of an approximationwill not influence the report of relative changes in stiffness.However, it is assumed that mass does not significantlychange during ischemia, for this would influence the results.
Computer programs were developed to calculate the vis-cous and elastic stiffness from the stiffness and phase angledata measured from the digitized sinusoidal volume waveform and the sinusoidal pressure response obtained byFourier analysis. The peak values of each pressure andvolume sine wave were measured and the stiffness (AP/AV) calculated. The sampling theorem (12, 13) was pro-grammed to reconstruct both the volume and pressurewave forms to permit measurements within 10 of the timesof occurrence of the peaks of the pressure and volumecycles.
In the present study, isovolumic ventricles of five dogswere ventricularly paced at 120 beats/min and perfusedwith an aortic pressure of 75 mmHg. Control recordingson analog tape were made of the sinusoidal piston displace-ment, ventricular pressure, and the pacing stimulus. A re-versible ligature was placed around the proximal left an-terior descending coronary artery (LAD) immediately afterthe origin of the first septal branch. Placing the ligationat this position did not make the entire ventricle ischemic;instead we wanted a level of depression that gave a mea-surable developed pressure. This level of depression couldthen be described by a linear stiffness-pressure relation-ship, comparable with that for the control state. After liga-
tion of the proximal LAD coronary artery, recordings of thepreviously mentioned parameters were made after 2, 5, 10,15, and 20 min in four dogs and at 5-min intervals for 1 hin one dog. In two animals, removal of the LAD ligationwas accomplished without producing ventricular fibrillation.In these animals, recordings were made periodically for 10min after the release during stable ventricular pacing. Ina second group of 11 dogs, a large cardiodepressant doseof propranolol (Inderal, Ayerst Laboratories, New York)(8 mg/kg) was infused intravenously and recordings madebefore and after the drug was given. In a subset of thisgroup, five animals were given an initial dose of 1 mg/kgto investigate the influence of a beta-blocking dose of pro-pranolol (14) on ventricular stiffness at a time when onlyminimal direct ventricular depression occurred. In threeanimals, severely depressed by 8 mg/kg of propranolol,acetylstrophanthidin (0.44 mg/kg) was administered at atime of maximal ventricular depression. In three additionaldogs, the influence of depressant doses of sodium pentobarbi-tal (16 mg/kg/min until developed pressure was reducedby half or more) on stiffness was investigated. These ani-mals also received acetylstrophanthidin to test its influenceon stiffness again in the setting of myocardial depression.
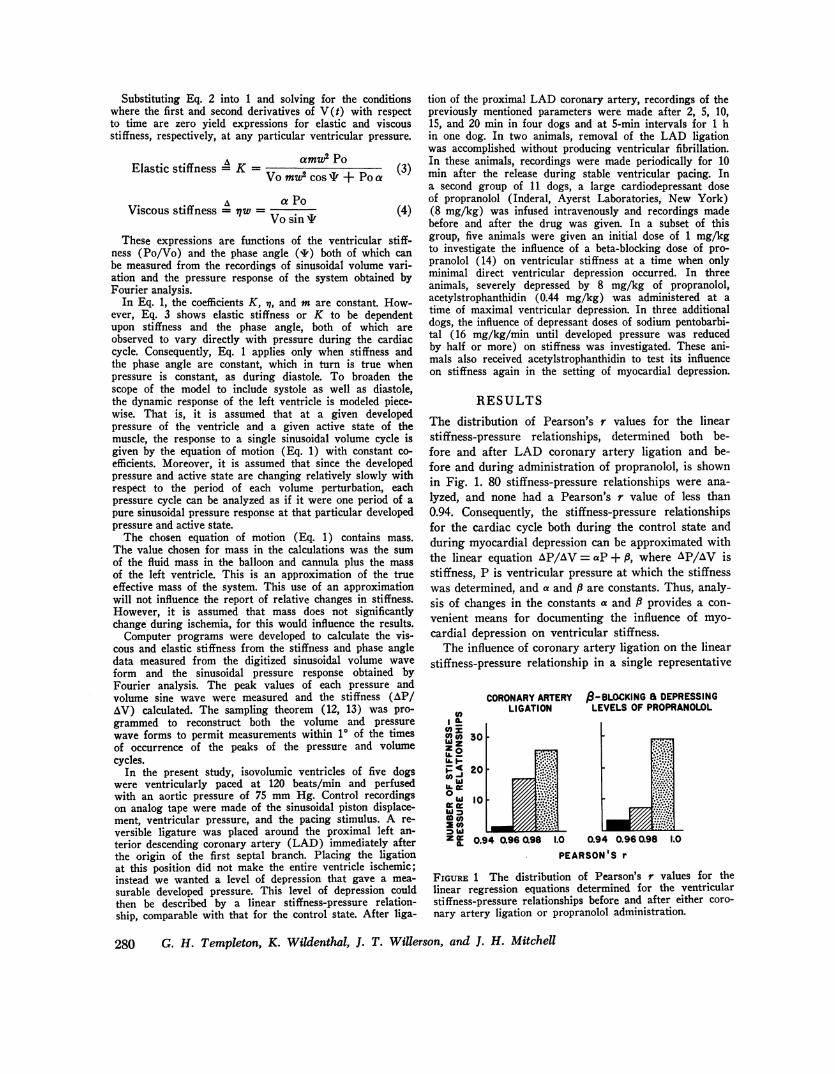
RESULTSThe distribution of Pearson's r values for the linearstiffness-pressure relationships, determined both be-fore and after LAD coronary artery ligation and be-fore and during administration of propranolol, is shownin Fig. 1. 80 stiffness-pressure relationships were ana-lyzed, and none had a Pearson's r value of less than0.94. Consequently, the stiffness-pressure relationshipsfor the cardiac cycle both during the control state andduring myocardial depression can be approximated withthe linear equation AP/AV = aP + A, where AP/AV isstiffness, P is ventricular pressure at which the stiffnesswas determined, and a and P are constants. Thus, analy-sis of changes in the constants a and P provides a con-venient means for documenting the influence of myo-cardial depression on ventricular stiffness.
The influence of coronary artery ligation on the linearstiffness-pressure relationship in a single representative
CORONARYARTERYLIGATION
a-BLOCKING a DEPRESSINGLEVELS OF PROPRANOLOL
t0( 30WZZo
20
0 0
z W 0.94 0.96 L98 1.0 0.94 0.960.98 1.0
PEARSON'S r
FIGURE 1 The distribution of Pearson's r values for thelinear regression equations determined for the ventricularstiffness-pressure relationships before and after either coro-nary artery ligation or propranolol administration.
280 G. H. Templeton, K. Wildenthal, J. T. Willerson, and J. H. Mitchell
20 min of coronaryartery ligation
AP/&V-0.075P+1.8 Ir 0.997 . Control
AP/AV - 0.058 P+1.7
r a 0.998
X3
8
6
4
2
0 10 20 30 40 50 60 70 80 90 100
20 min of coronaryartery ligation
P/AV 0.075 P+1.8 ,r 0.997
..10 min after release
of ligationAP/AV=0.061 P+1.8
t >8 r *0.9959
0 10 20 30 40 50 60 70 80
LEFT VENTRICULARPRESSURE(mmHg)
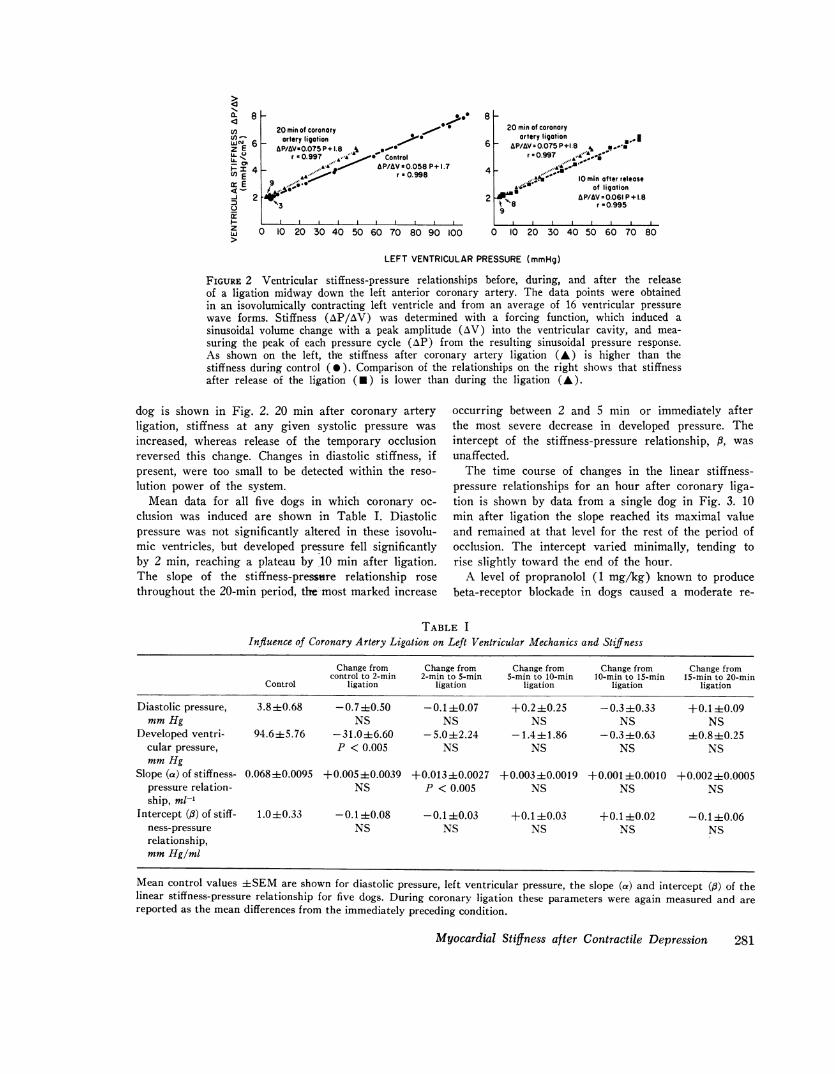
FIGURE 2 Ventricular stiffness-pressure relationships before, during, and after the releaseof a ligation midway down the left anterior coronary artery. The data points were obtainedin an isovolumically contracting left ventricle and from an average of 16 ventricular pressurewave forms. Stiffness (AP/AV) was determined with a forcing function, which induced asinusoidal volume change with a peak amplitude (AV) into the ventricular cavity, and mea-suring the peak of each pressure cycle (AvP) from the resulting sinusoidal pressure response.As shown on the left, the stiffness after coronary artery ligation (A) is higher than thestiffness during control ( 0 ). Comparison of the relationships on the right shows that stiffnessafter release of the ligation (U) is lower than during the ligation (A).
dog is shown in Fig. 2. 20 min after coronary arteryligation, stiffness at any given systolic pressure was
increased, whereas release of the temporary occlusionreversed this change. Changes in diastolic stiffness, ifpresent, were too small to be detected within the reso-
lution power of the system.Mean data for all five dogs in which coronary oc-
clusion was induced are shown in Table I. Diastolicpressure was not significantly altered in these isovolu-mic ventricles, but developed pressure fell significantlyby 2 min, reaching a plateau by 10 min after ligation.The slope of the stiffness-pressure relationship rose
throughout the 20-min period, the most marked increase
occurring between 2 and 5 min or immediately afterthe most severe decrease in developed pressure. Theintercept of the stiffness-pressure relationship, ,, was
unaffected.The time course of changes in the linear stiffness-
pressure relationships for an hour after coronary liga-tion is shown by data from a single dog in Fig. 3. 10min after ligation the slope reached its maximal valueand remained at that level for the rest of the period ofocclusion. The intercept varied minimally, tending torise slightly toward the end of the hour.
A level of propranolol (1 mg/kg) known to producebeta-receptor blockade in dogs caused a moderate re-
TABLE IInfluence of Coronary Artery Ligation on Left Ventricular Mechanics and Stiffness
Change from Change from Change from Change from Change fromcontrol to 2-min 2-min to 5-min 5-min to 10-min 10-min to 15-min 15-min to 20-min
Control ligation ligation ligation ligation ligation
Diastolic pressure, 3.8±0.68 -0.740.50 -0.1±40.07 +0.240.25 -0.340.33 +0.1I0.09mmHg NS NS NS NS NS
Developed ventri- 94.6 ±5.76 -31.0 ±6.60 -5.0±-2.24 -1.4±4-1.86 -0.3 ±0.63 ±0.8 ±0.25cular pressure, P < 0.005 NS NS NS NSmmHg
Slope (a) of stiffness- 0.068±0.0095 +0.005±0.0039 +0.013±0.0027 +0.003±0.0019 +0.001±0.0010 +0.002±0.0005pressure relation- NS P < 0.005 NS NS NSship, ml-'
Intercept (,B) of stiff- 1.0±0.33 -0.1 ±0.08 -0.1 ±0.03 +0.1±-0.03 +0.1±-0.02 -0.1±40.06ness-pressure NS NS NS NS NSrelationship,mmHg/ml
Mean control values ±-SEM are shown for diastolic pressure, left ventricular pressure, the slope (a) and intercept (0) of thelinear stiffness-pressure relationship for five dogs. During coronary ligation these parameters were again measured and arereported as the mean differences from the immediately preceding condition.
Myocardial Stiffness after Contractile Depression 281
a. 8U,(nwvE 6ILlLL>
- 2
I-j
zw
7lLAD OCCLUSION
35 min60min 10min
0 10 20 30 40 50 60 70 80 90 100 110
LEFT VENTRICULAR PRESSURE(mmHg)
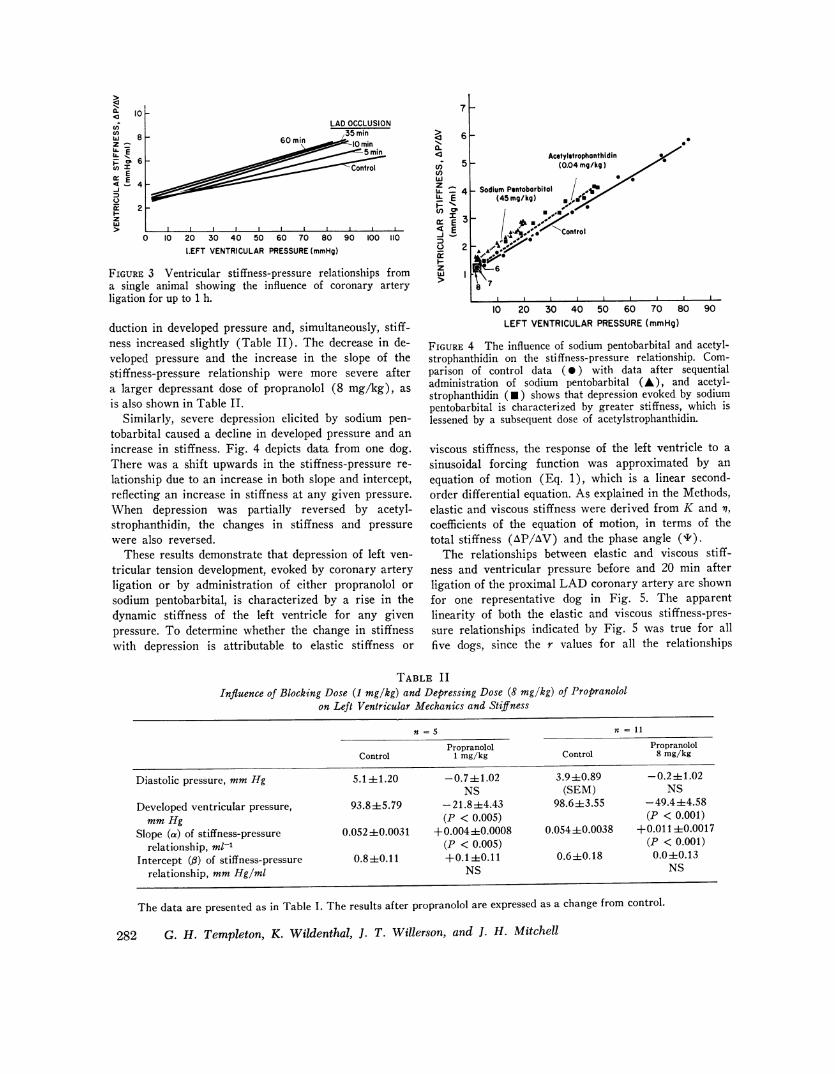
FIGURE 3 Ventricular stiffness-pressure relationships froma single animal showing the influence of coronary artery
ligation for up to 1 h.
duction in developed pressure and, simultaneously, stiff-ness increased slightly (Table II). The decrease in de-veloped pressure and the increase in the slope of thestiffness-pressure relationship were more severe aftera larger depressant dose of propranolol (8 mg/kg), as
is also shown in Table II.Similarly, severe depression elicited by sodium pen-
tobarbital caused a decline in developed pressure and an
increase in stiffness. Fig. 4 depicts data from one dog.There was a shift upwards in the stiffness-pressure re-
lationship due to an increase in both slope and intercept,reflecting an increase in stiffness at any given pressure.
When depression was partially reversed by acetyl-strophanthidin, the changes in stiffness and pressure
were also reversed.These results demonstrate that depression of left ven-
tricular tension development, evoked by coronary artery
ligation or by administration of either propranolol or
sodium pentobarbital, is characterized by a rise in thedynamic stiffness of the left ventricle for any givenpressure. To determine whether the change in stiffnesswith depression is attributable to elastic stiffness or
a.
c,; 5iv
c,)w
e -
I
en a
£ 3a:
_
U 2
i-zw I
Acetylstrophonthidin(0.04 mg/kg)
_ Sodium Pentoborbitol / a(45 mg/kg)
0*~~~~~
6
10 20 30 40 50 60 70 80 90LEFT VENTRICULARPRESSURE(mmHg)
FIGURE 4 The influence of sodium pentobarbital and acetyl-strophanthidin on the stiffness-pressure relationship. Com-parison of control data ( 0 ) with data after sequentialadministration of sodium pentobarbital (A), and acetyl-strophanthidin (U) shows that depression evoked by sodiumpentobarbital is characterized by greater stiffness, which islessened by a subsequent dose of acetylstrophanthidin.
viscous stiffness, the response of the left ventricle to a
sinusoidal forcing function was approximated by an
equation of motion (Eq. 1), which is a linear second-order differential equation. As explained in the Methods,elastic and viscous stiffness were derived from K and n,
coefficients of the equation of motion, in terms of thetotal stiffness (AP/AV) and the phase angle (').
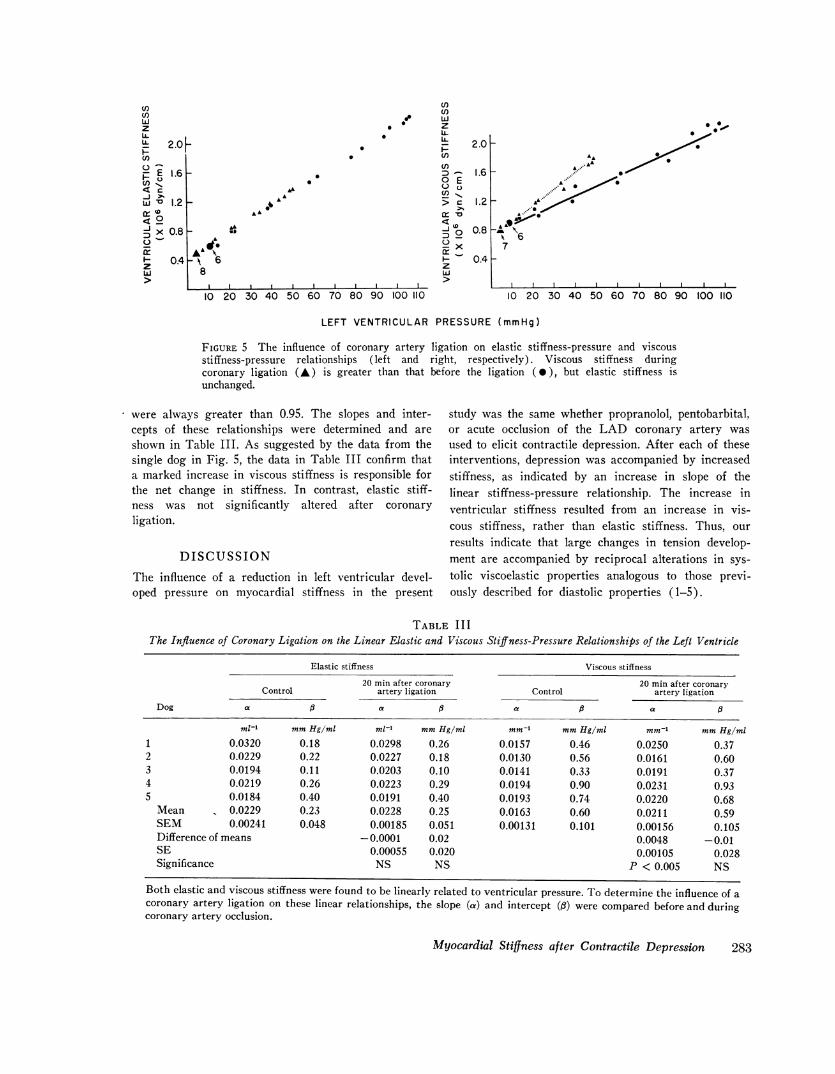
The relationships between elastic and viscous stiff-ness and ventricular pressure before and 20 min afterligation of the proximal LAD coronary artery are shownfor one representative dog in Fig. 5. The apparentlinearity of both the elastic and viscous stiffness-pres-sure relationships indicated by Fig. 5 was true for all
five dogs, since the r values for all the relationships
TABLE IIInfluence of Blocking Dose (1 mg/kg) and Depressing Dose (8 mg/kg) of Propranolol
on Left Ventricular Mechanics and Stiffness5
Propranolol PropranololControl 1 mg/kg Control 8 mg/kg
Diastolic pressure, mmHg 5.1±+ 1.20 -0.7-+ 1.02 3.9 +0.89 -0.2 i+1.02NS (SEM) NS
Developed ventricular pressure, 93.8+5.79 -21.8+4.43 98.6+3.55 -49.4+4.58
mmHg (P < 0.005) (P < 0.001)Slope (a) of stiffness-pressure 0.052 +0.0031 +0.004+0.0008 0.054i0.0038 +0.011 i0.0017
relationship, ml-' (P < 0.005) (P < 0.001)Intercept (fl) of stiffness-pressure 0.8+0.11 +0.1+-0.11 0.6+0.18 0.0+0.13
relationship, mmHg/ml NS NS
The data are presented as in Table I. The results after propranolol are expressed as a change from control.
282 G. H. Templeton, K. Wildenthal, J. T. Willerson, and J. H. Mitchell
L 10
U,U1)w 8Z ^
U.' EA: p 6
cE
<- 4
i 2z
LA6
8
to
. * zULi
- 2.0* e~~~~~~n
¾- 1.6AL
0
> c 1.2*s ~~~~~~~~~~~~~>1A, A r 10
el~~~~~~~~~-i 0.80~~ ~ ~ ~ ~ ~AL~~~~~~~~~~~d
:-x- 0.4z
LIII I I I >
10 20 30 40 50 60 70 80 90 100 110 10 20 30 40 50 60 70 80 90 100 110
LEFT VENTRICULAR PRESSURE(mmHg)
FIGURE 5 The influence of coronary artery ligation on elastic stiffness-pressure and viscousstiffness-pressure relationships (left and right, respectively). Viscous stiffness duringcoronary ligation (A) is greater than that before the ligation (0), but elastic stiffness isunchanged.
were always greater than 0.95. The slopes and inter-cepts of these relationships were determined and are
shown in Table III. As suggested by the data from thesingle dog in Fig. 5, the data in Table III confirm thata marked increase in viscous stiffness is responsible forthe net change in stiffness. In contrast, elastic stiff-ness was not significantly altered after coronaryligation.
DISCUSSION
The influence of a reduction in left ventricular devel-oped pressure on myocardial stiffness in the present
study was the same whether propranolol, pentobarbital,or acute occlusion of the LAD coronary artery was
used to elicit contractile depression. After each of theseinterventions, depression was accompanied by increasedstiffness, as indicated by an increase in slope of thelinear stiffness-pressure relationship. The increase inventricular stiffness resulted from an increase in vis-cous stiffness, rather than elastic stiffness. Thus, our
results indicate that large changes in tension develop-ment are accompanied by reciprocal alterations in sys-
tolic viscoelastic properties analogous to those previ-ously described for diastolic properties (1-5).
TABLE I I IThe Influence of Coronary Ligation on the Linear Elastic and Viscous Stiffness-Pressure Relationships of the Left Ventricle
Elastic stiffness Viscous stiffness
20 min after coronary 20 min after coronaryControl artery ligation Control artery ligation
Dog a a a 5 a 6
ml-' mmHg/ml ml-' mmHg/ml mm-' mmHg/ml mm-, mmHg/ml1 0.0320 0.18 0.0298 0.26 0.0157 0.46 0.0250 0.372 0.0229 0.22 0.0227 0.18 0.0130 0.56 0.0161 0.603 0.0194 0.11 0.0203 0.10 0.0141 0.33 0.0191 0.374 0.0219 0.26 0.0223 0.29 0.0194 0.90 0.0231 0.935 0.0184 0.40 0.0191 0.40 0.0193 0.74 0.0220 0.68
Mean 0.0229 0.23 0.0228 0.25 0.0163 0.60 0.0211 0.59SEM 0.00241 0.048 0.00185 0.051 0.00131 0.101 0.00156 0.105Difference of means -0.0001 0.02 0.0048 -0.01SE 0.00055 0.020 0.00105 0.028Significance NS NS P < 0.005 NS
Both elastic and viscous stiffness were found to be linearly related to ventricular pressure. To determine the influence of acoronary artery ligation on these linear relationships, the slope (ca) and intercept (fl) were compared before and duringcoronary artery occlusion.
Myocardial Stiffness after Contractile Depression 283
tnto
zULLL 2.0n
g E 1.6
it 1.2
X 0.8
< 04> LzwU

In interpreting these changes in myocardial stiffness,one must distinguish between the mechanical changesthat might accompany cardiac depression in a normallyejecting left ventricle with a sustained aortic pressurefrom an isovolumically contracting ventricle such aswas used in our study. In the latter, contractile depres-sion will result in a reduction of developed tension,whereas in the former it will lead to cardiac dilatationand, by the Laplace principle, an increase in tension.Because of this consideration it is important to empha-size that the present results concern the response toventricular depression with reduced tension; differentresults might be expected in hearts in which depressionis accompanied by cardiac dilatation with a net in-crease in tension.
It should also be noted that the stiffness changes weobserved were in response to very large alterations intension. We have previously shown that modest ino-tropic interventions, in which the velocity of shorteningincreased significantly but in which total tension devel-opment rose only slightly, were not accompanied bymeasurable alterations in net stiffness (8, 10). The ap-parent discrepancy between that study and the presentseems to us most likely to be due simply to major dif-ferences in the degree of alteration of tension. It alsoremains possible that depression of tension below nor-mal control levels in some way exerts a fundamentallydifferent effect on stiffness than does enhancement oftension development above normal, and that possibilityis currently being investigated.
The concept and importance of viscous stiffness ininfluencing traditional determinations of left ventriculardiastolic compliance or of systolic "series elasticity" asmeasured by quick-release experiments have been men-tioned in some previous reports (9, 11, 15-17), but re-main insufficiently defined. Viscous stiffness for cardiacmuscle had not been quantified before the present tech-nique was developed, and its relationship to other pa-rameters relating velocity and force remains unclear.However, a comparison between systolic viscous stiff-ness and the traditional force-velocity curve has beenmade in skeletal muscle studies. Using a sinusoidalforcing function, Buchthal and Rosenfalck (18, 19) ob-tained measurements of viscous stiffness in skeletalmuscle similar to those recorded in the present experi-ments for cardiac muscle. To compare systolic viscousstiffness to the force-velocity relationship, Buchthal de-rived an expression for viscous stiffness from Hill'smathematical expression of the force-velocity relation-ship. With typically observed values for the constantsof Hill's equation, a value of the derived viscous stiff-ness parameter was much less than the value of vis-cous stiffness measured by Buchthal's sinusoidal forc-ing technique. Buchthal deduced from this comparisonthat the contractile element in Hill's model contributed
to the viscous stiffness measured by the sinusoidalforcing technique but was not entirely responsible forthe measured viscous stiffness.
A similar comparison between viscous stiffness andthe force-velocity curve can be drawn for cardiac musclefor a better understanding of this new parameter interms of the more widely used one. Such a comparisoncan be made by realizing that viscous stiffness is, bydefinition, the ratio of change in force (AF) to changein velocity (AV). Then, this ratio (AF/AV) is thesame as the negative reciprocal of the slope of theforce-velocity curve. However, it should be emphasizedthat the techniques used in obtaining these two expres-sions of muscle viscosity are quite different, and con-sequently the data measured by them are not strictlycomparable. Since techniques are now available formeasuring viscous stiffness directly and since experi-ments such as those described in this report have estab-lished that myocardial viscous changes exert a majorinfluence during some interventions, it is to be hopedthat greater attention will be paid in the future to de-fining the nature and importance of the viscous stiffnessof the heart.
The increase in ventricular viscous stiffness by myo-cardial ischemia indicates that either the ability of themyocardium to generate a velocity at a given force hasbeen impaired or its ability to generate tension at agiven velocity has been improved. Whether this changein viscous stiffness indicates an impairment or an im-provement depends on whether the contractile apparatusis more dependent upon velocity or force; e.g., whetherthe contractile apparatus is a velocity generator or aforce generator. This distinction cannot be made atthe present time. All that is known from the represen-tation of Hill's contractile element with the force-veloc-ity curve is that force and velocity are interrelated; wedo not know which parameter is dependent on theother.
Due to technical difficulties, studies measuring theforce-velocity relationship have rarely been done inthe left ventricle. Some investigations have made sim-plifying assumptions to obtain in vivo force-velocityrelationship, and a few of these have investigated theinfluence of ischemia on in vivo force-velocity relation-ships. Mason, Spann, Zelis, and Amsterdam (20) ob-tained relationships comparable to force-velocity curvesfor patients by plotting dp/dt/p versus isovolumic pres-sure. The slope of their relationship was greater dur-ing control than failure. The reciprocal of the slope oftheir relationship thus increased with failure, indicatingan increase in viscous stiffness and agreeing with thechange in the direct measurements of viscous stiffnessduring ischemia seen in our results.
Finally, it would be interesting to be able to relatestudies such as ours to experiments using quick-re-
284 G. H. Templeton, K. Wildenthal, J. T. Willerson, and J. H. Mitchell

lease techniques. However, at the present, any com-parison between stiffness parameters measured by quick-release and sinusoidal techniques must be guarded.As pointed out previously (9, 11, 15-17), the quick-release does not measure a pure elastic response, eventhough the property it reflects has been termed the"series elastic element." Strict comparison between thetwo techniques can be assessed only after further ex-perimentation to see how both behave under differentexperimental interventions and to measure the viscouscomponent in the response to a quick release.
ACKNOWLEDGMENTSThis work was supported by grants from the AmericanHeart Association and the American Heart Association,Texas Affiliate, Inc., and Dallas County Chapter, and bygrants (HL 06296, HL 15522, and HL 17669), a contract(72-2947) from the National Heart and Lung Institute, andthe Harry S. Moss Heart Fund.
REFERENCES1. Bauereisen, E., R. Jacob, U. Kleinheisterkamp, U. Pei-
per, and K. H. Weigand. 1965. Enddiastolische Dehnbar-keit des linken Ventrikels in situ bei akuten Anderungendes arteriellen systemdrucks. Arch. Gestamte Physiol.Mens. Tiere (Pfluigers). 285: 335-348.
2. Sonnenblick, E. H., J. Ross, Jr., J. W. Covell, and E.Braunwald. 1966. Alterations in resting length-tensionrelations of cardiac muscle induced by changes in con-tractile force. Circulation Res. 19: 980-988.
3. Gilmore, J. P., H. E. Cingolani, R. R. Taylor, and R.H. McDonald, Jr. 1966. Physical factors and cardiacadaptation. Am. J. Physiol. 211: 1219-1226.
4. Wildenthal, K., C. B. Mullins, M. D. Harris, and J. H.Mitchell. 1969. Left ventricular end-diastolic distensibilityafter norepinephrine and propranolol. Am. J. Physiol.217: 812-818.
5. Leach, J. K., and F. J. Wall. 1972. Effect of inotropicagents on distensibility of the isolated cat heart. Proc.Soc. Exp. Biol. Med. 139: 310-314.
6. Templeton, G. H., J. H. Mitchell, R. R. Ecker, and G.Blomqvist. 1970. A method for measurement of dynamic
compliance of the left ventricle in dogs. J. Appi. Physiol.29: 742-745.
7. Templeton, G. H., and L. R. Nardizzi. 1974. Elastic andviscous stiffness of the canine left ventricle. J. APPi.Physiol. 36: 123-127.
8. Templeton, G. H., R. R. Ecker, and J. H. Mitchell.1972. Left ventricular stiffness during diastole and sys-tole: the influence of changes in volume and inotropicstate. Cardiovasc. Res. 6: 95-100.
9. Templeton, G. H., J. H. Mitchell, and K. Wildenthal.1972. Influence of hyperosmolality on left ventricularstiffness. Am. J. Physiol. 222: 1406-1411.
10. Templeton, G. H., K. Wildenthal, and J. H. Mitchell.1972. Influence of coronary blood flow on left ventricularcontractility and stiffness. Am. J. Physiol. 223: 1216-1220.
11. Templeton, G. H., K Wildenthal, J. T. Willerson, andW. C. Reardon. 1974. Influence of temperature on themechanical properties of cardiac muscle. Circ. Res. 34:624-634.
12. Schwartz, M. 1959. Information Transmission, Modula-tion and Noise: Unified Approach to CommunicationSystems. McGraw-Hill Book Company, New York.
13. Papoulis, A. 1965. Probability, Random Variables, andStochastic Processes. McGraw-Hill Book Company,New York.
14. Dollery, C. T., J. W. Paterson, and M. E. Conolly.1969. Clinical pharmacology of beta-receptor-blockingdrugs. Clin. Pharmacol. Ther. 10: 765-799.
15. Hill, A. V. 1950. The series elastic component of muscle.Proc. R. Soc. Lond. B. Biol. Sci. 137: 273-280.
16. Jewell, B. R., and D. R. Wilkie. 1958. An analysis ofthe mechanical components in frog's striated muscle. J.Physiol. (Lond.). 143: 515-540.
17. Wildenthal, K., C. L. Skelton, and H. N. Coleman, III.1969. Cardiac muscle mechanics in hyperosmotic solu-tions. Am. J. Physiol. 217: 302-306.
18. Buchthal, F., and P. Rosenfalck. 1957. Elastic proper-ties of striated muscle. Tissue Elasticity Pap. Conf.73-93.
19. Buchthal, F., and P. Rosenfalck. 1960. Dynamic elas-ticity in the initial phase of an isotonic twitch. ActaPhysiol. Scand. 49: 198-210.
20. Mason, D. T., J. F. Spann, Jr., R. Zelis, and E. A.Amsterdam. 1971. Comparison of the contractile stateof the normal, hypertrophied, and failing heart in man.In Cardiac Hypertrophy, N. R. Alpert, editor. AcademicPress, Inc., New York. 433-444.
Myocardial Stiffness after Contractile Depression 285