infecção do trato urinário - spp · infecção do trato urinário helena pinto unidade de...
TRANSCRIPT
Infecção do trato urinário
Helena Pinto Unidade de Nefrologia pediátrica, Serviço de Pediatria
Centro Hospitalar S. João, E.P.E.- Porto
Curso de Inverno da SPP
Albufeira, Março 2012
Febrile Urinary Tract Infections in Children. Montini G, Tullus K, Hewitt I. N Engl J Med, July 2011; 365: 239-250. Long term antibiotics for preventing recurrent urinary tract infection in children (Review). Williams G, Craig JC. Cochrane Database Syst Rev, 2011; 16(3): CD001534. Urinary tract infection: Clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Subcommittee on Urinary Tract Infection (American Academy of Pediatrics). Pediatrics, Sept 2011, 128(3):595-609.
Bibliografia: a não perder...

• ...” are currently undergoing an intense debate...” (Saahed, 2011)
• ...”it remains one of the most- if not the most- controversial fields
in paediatric medicine”... (Tullus, 2011)
• ...”hotly debated”... (Prasad M, 2011)
• ...”this is a controversial subject”... (Coulthard M, 2007)
• ...”UTI is still so confusing”... (Tullus, 2011)
Infecção do trato urinário
Controvérsias:
• Diagnóstico:
- a quem colher urina
- método de colheita
- interpretação dos resultados
• Tratamento
• Seguimento
- estudo imagiológico subsequente
- profilaxia antibiótica
Epidemiologia:
• PNA mais frequente infecção bacteriana na criança com infecção
grave e/ou febre sem foco
• < 8 anos de idade: 8-11% das crianças do sexo feminino e 2-4% sexo masculino têm primeiro episódio de ITU febril
• ITUs não febris têm > prevalência após os 3 anos de idade e no sexo
feminino
• Febre maior probabilidade de envolvimento renal
(sensibilidade 53-84%, especificidade 44-92%) [1]

Epidemiologia:
• Disseminação ascendente ou hematogénea (+ freq < 12 semanas)
• Agentes etiopatogénicos:
Escherichia coli (60-92%)
Klebsiella spp
Enterobacter spp
Proteus mirabilis
Enterococcus spp
Pseudomonas aeruginosa
Staphylococcus coagulase negativo
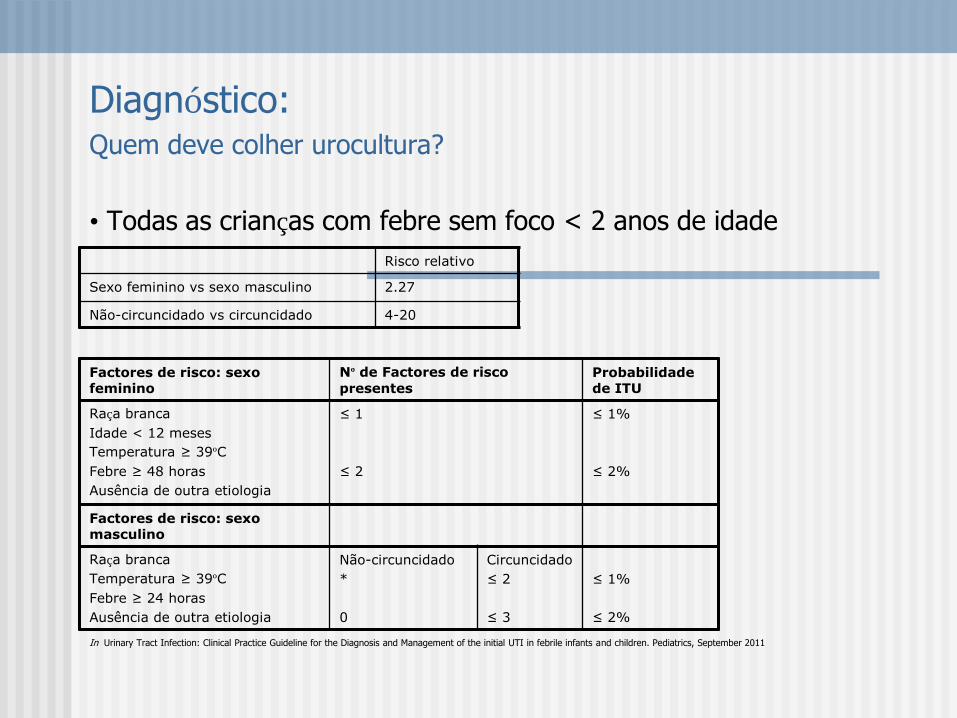
Diagnóstico: Quem deve colher urocultura?
• Todas as crianças com febre sem foco < 2 anos de idade
In Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the initial UTI in febrile infants and children. Pediatrics, September 2011
Risco relativo
Sexo feminino vs sexo masculino 2.27
Não-circuncidado vs circuncidado 4-20
Factores de risco: sexo feminino
Nº de Factores de risco
presentes Probabilidade de ITU
Raça branca
Idade < 12 meses
Temperatura ≥ 39ºC
Febre ≥ 48 horas
Ausência de outra etiologia
≤ 1
≤ 2
≤ 1%
≤ 2%
Factores de risco: sexo masculino
Raça branca
Temperatura ≥ 39ºC
Febre ≥ 24 horas
Ausência de outra etiologia
Não-circuncidado
*
0
Circuncidado
≤ 2
≤ 3
≤ 1%
≤ 2%
Diagnóstico: Quem deve colher urocultura?
• Sintomas urinários: disúria, polaquiúria, urgência, alteração das características macroscópicas da urina (hematúria, urina turva), incontinência urinária, dor abdominal
• Febre sem foco e antecedentes pessoais de ITU e/ou malformação nefro-urológica conhecida
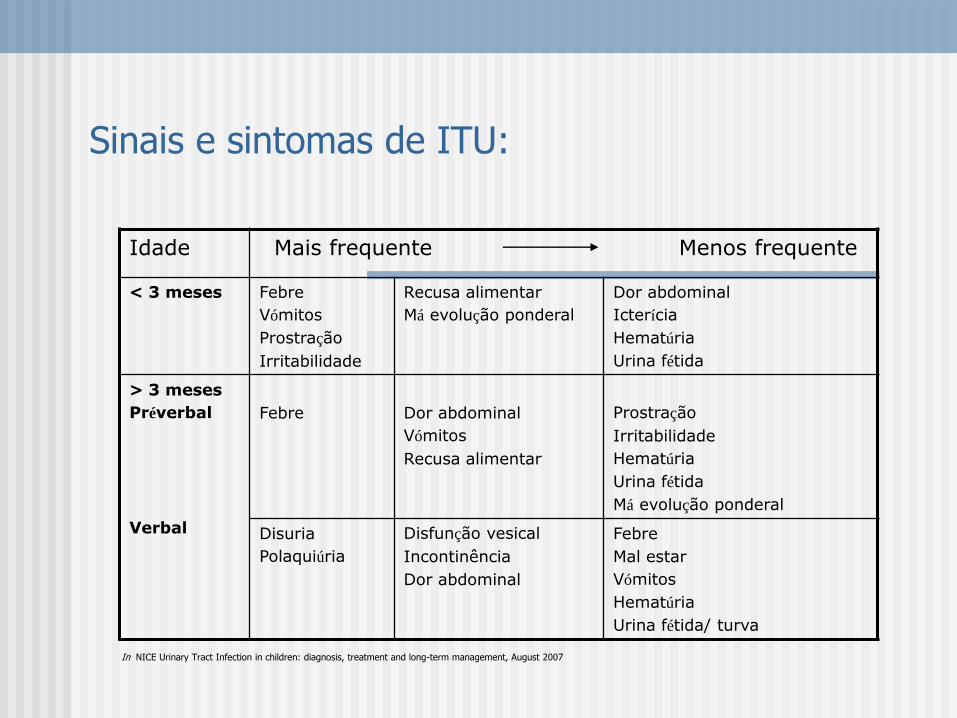
Sinais e sintomas de ITU:
Idade Mais frequente Menos frequente
< 3 meses Febre
Vómitos
Prostração
Irritabilidade
Recusa alimentar
Má evolução ponderal
Dor abdominal
Icterícia
Hematúria
Urina fétida
> 3 meses
Préverbal
Verbal
Febre
Dor abdominal
Vómitos
Recusa alimentar
Prostração
Irritabilidade
Hematúria
Urina fétida
Má evolução ponderal
Disuria
Polaquiúria
Disfunção vesical
Incontinência
Dor abdominal
Febre
Mal estar
Vómitos
Hematúria
Urina fétida/ turva
In NICE Urinary Tract Infection in children: diagnosis, treatment and long-term management, August 2007

Fatores de risco:
- ITU prévia
- Febre recorrente de etiologia desconhecida
- Diagnóstico prénatal de malformação nefrourológica
- História familiar de RVU ou doença renal
- Obstipação
- Disfunção vesical
- Lesão medular/ bexiga neurogénica
- Jacto urinário diminuído
- Má evolução ponderal
- Hipertensão arterial
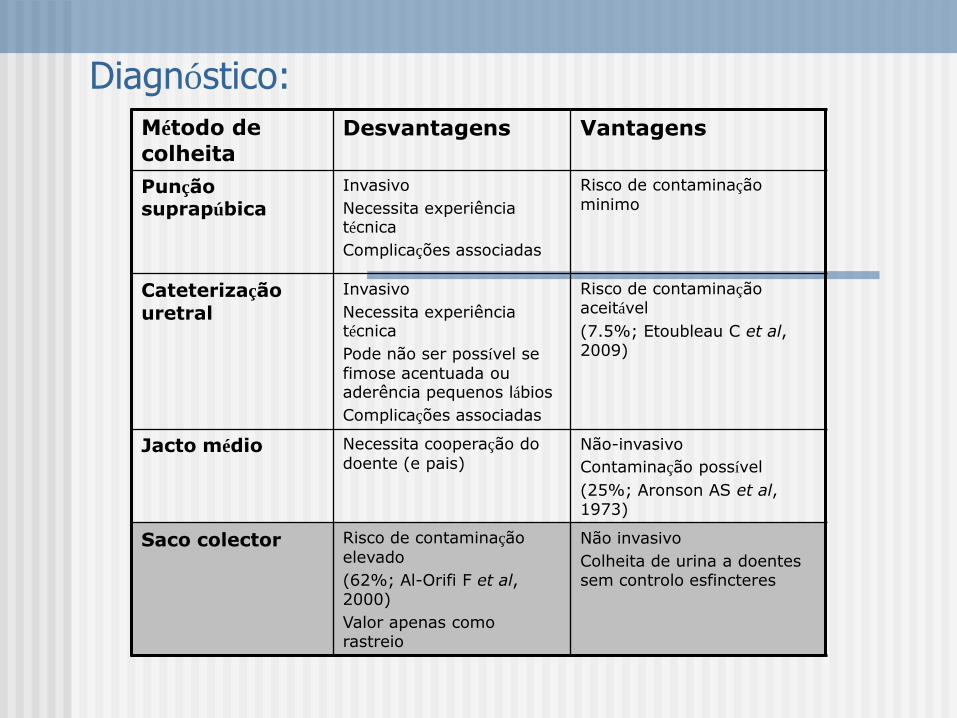
Diagnóstico:
Método de
colheita Desvantagens Vantagens
Punção suprapúbica
Invasivo
Necessita experiência técnica
Complicações associadas
Risco de contaminação
minimo
Cateterização
uretral
Invasivo
Necessita experiência técnica
Pode não ser possível se
fimose acentuada ou aderência pequenos lábios
Complicações associadas
Risco de contaminação aceitável
(7.5%; Etoubleau C et al, 2009)
Jacto médio Necessita cooperação do
doente (e pais) Não-invasivo
Contaminação possível
(25%; Aronson AS et al, 1973)
Saco colector Risco de contaminação
elevado
(62%; Al-Orifi F et al, 2000)
Valor apenas como rastreio
Não invasivo
Colheita de urina a doentes sem controlo esfincteres
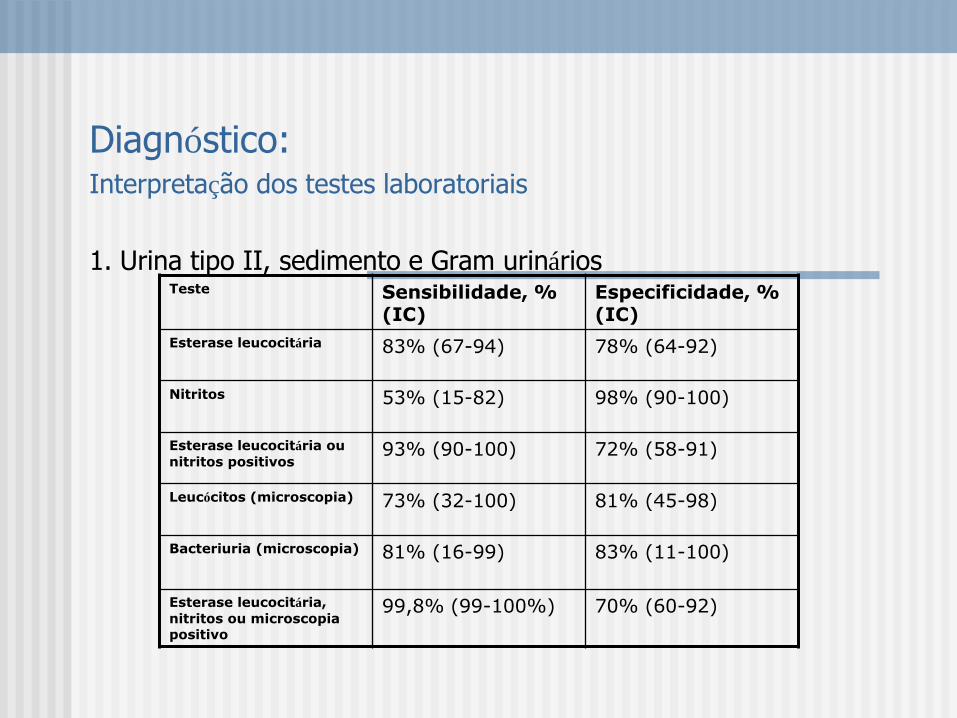
Diagnóstico: Interpretação dos testes laboratoriais
1. Urina tipo II, sedimento e Gram urinários
Teste Sensibilidade, % (IC)
Especificidade, % (IC)
Esterase leucocitária 83% (67-94) 78% (64-92)
Nitritos 53% (15-82) 98% (90-100)
Esterase leucocitária ou
nitritos positivos 93% (90-100) 72% (58-91)
Leucócitos (microscopia) 73% (32-100) 81% (45-98)
Bacteriuria (microscopia) 81% (16-99) 83% (11-100)
Esterase leucocitária,
nitritos ou microscopia positivo
99,8% (99-100%) 70% (60-92)

Diagnóstico: Interpretação dos testes laboratoriais
2. Urocultura
(resultado baseia-se na análise quantitativa das UFC/ml presentes no meio de
cultura)
Jacto médio: positiva se > 105 UFC/ml
Cateterização uretral: positiva se > 104 UFC/ml
Punção suprapúbica: positiva se qq crescimento bacteriano
Ed Kass (1957). Relation between pyelonephritis and bacterial counts in urine. NEJM, May 1957.
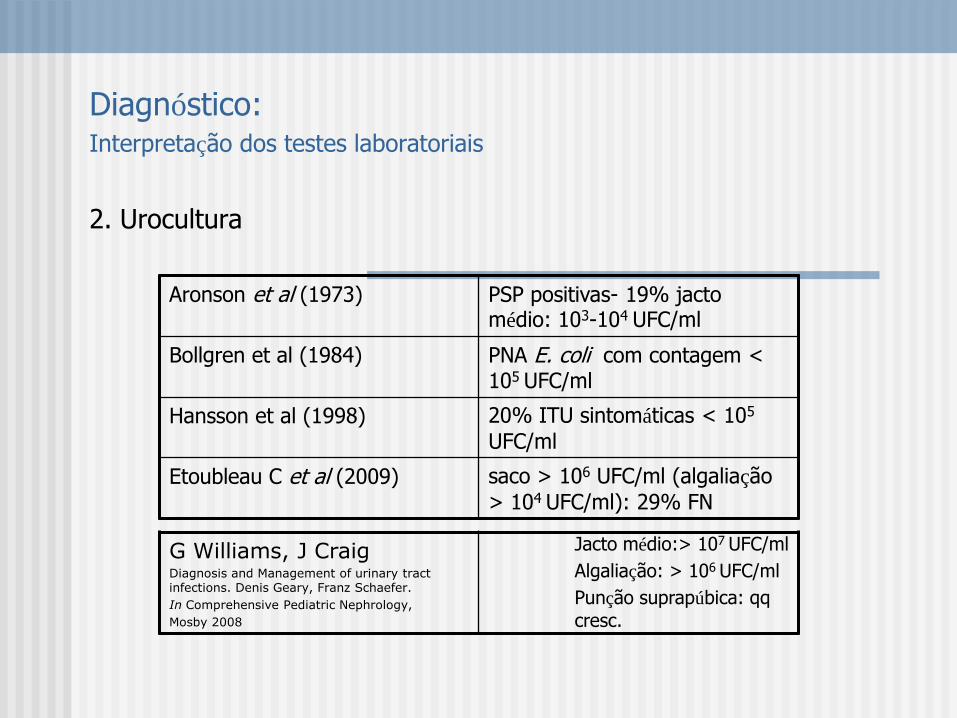
Diagnóstico: Interpretação dos testes laboratoriais
2. Urocultura
Aronson et al (1973) PSP positivas- 19% jacto médio: 103-104 UFC/ml
Bollgren et al (1984) PNA E. coli com contagem < 105 UFC/ml
Hansson et al (1998) 20% ITU sintomáticas < 105
UFC/ml
Etoubleau C et al (2009) saco > 106 UFC/ml (algaliação
> 104 UFC/ml): 29% FN
G Williams, J Craig Diagnosis and Management of urinary tract infections. Denis Geary, Franz Schaefer.
In Comprehensive Pediatric Nephrology,
Mosby 2008
Jacto médio:> 107 UFC/ml
Algaliação: > 106 UFC/ml
Punção suprapúbica: qq
cresc.

Diagnóstico: Interpretação dos testes laboratoriais
2. Sedimento urinário e urocultura
American Academy of Pediatrics Urinary Tract Infection: Clinical Practice Guideline for the diagnosis and management of the initial UTI in
febrile infant and children 2 to 24 months (September 2011)
Para estabelecer o diagnóstico de ITU é necessário quer a presença de piúria e/ou bacteriúria quer a presença de pelo menos 50 000 UFC/ml de um uropatogénio obtido por cateterismo vesical ou punção suprapúbica (nível evidência C)
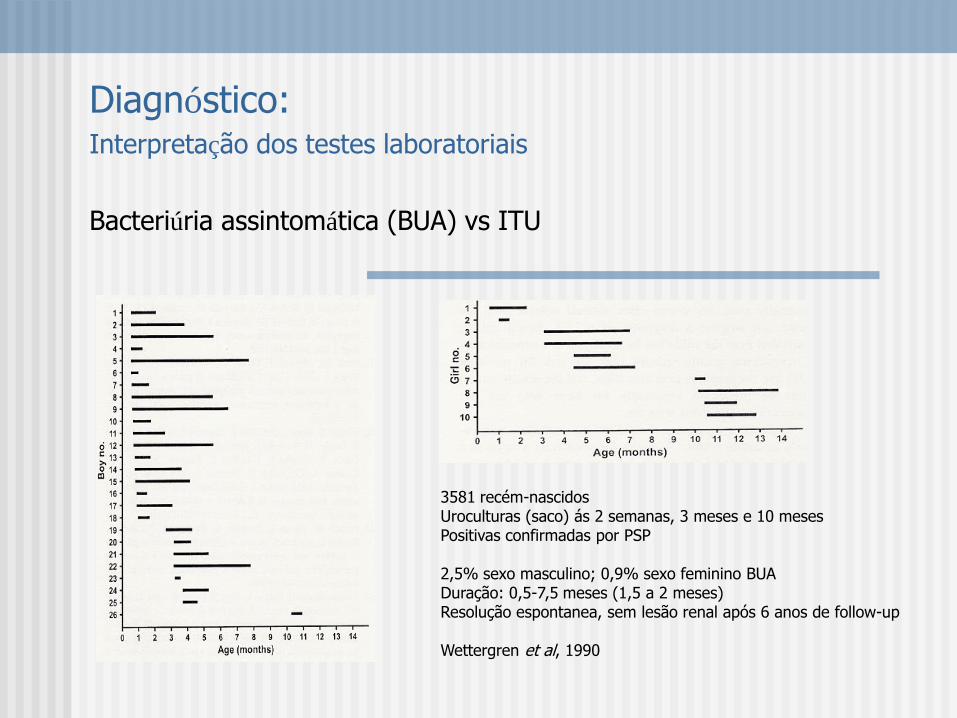
Diagnóstico: Interpretação dos testes laboratoriais
Bacteriúria assintomática (BUA) vs ITU
3581 recém-nascidos Uroculturas (saco) ás 2 semanas, 3 meses e 10 meses Positivas confirmadas por PSP 2,5% sexo masculino; 0,9% sexo feminino BUA Duração: 0,5-7,5 meses (1,5 a 2 meses) Resolução espontanea, sem lesão renal após 6 anos de follow-up Wettergren et al, 1990

Diagnóstico: Interpretação dos testes laboratoriais
Bacteriúria assintomática (BUA)
• 1:4 sexo masculino e 1:6 sexo feminino diagnosticados como ITU têm BUA
• Implicações na pratica clinica e investigação:
- tratamento e seguimento como ITU febril
- resultados investigacionais diluídos pela presença destes diagnósticos
falsos positivos

Bacteriúria assintomática (BUA)
• Implicações na investigação:
Brandstrom P et al, 2010 PSP; CV Antibiotic prophylaxis and endoscopic treatment decreased the infection rate.
Craig JC et al, 2009 PSP; CV Long-term, low-dose trimethoprim-sulfamethoxazole was associated with a decreased number of urinary tract infections in predisposed children.
Montini G et al, 2008 SC Prophylaxis does not reduce the rate of recurrent febrile urinary tract infections after the first episode
Pennesi M et al, 2008 SC Continuous antibiotic prophylaxis was ineffective in reducing the rate of pyelonephritis recurrence and the incidence of renal damage in children who were younger than 30 months and had vesicoureteral reflux grades II through IV.
Roussey-Kesler, 2008 SC These data suggest that antibiotic prophylaxis does not reduce the overall incidence of urinary tract infection in children with low grade vesicoureteral reflux. However, such a strategy may prevent further urinary tract infection in boys with grade III reflux.

Tratamento:
• Objectivos: erradicar o agente patogénico
controlar os sintomas
evitar o aparecimento de cicatrizes
• Critérios de internamento:
- idade < 3 meses
- 3-6 meses: marcadores inflamatórios elevados; impossibilidade de reavaliação em 48h
- aspecto séptico/sinais de sepsis
- vómitos/recusa alimentar significativa
- más condições sociais
- imunodeprimidos
- falência da terapêutica oral em ambulatório

Tratamento:
• Antibioterapia empírica:
Iniciar o mais precocemente possível
Baseada nos agentes mais frequentes e sua sensibilidade numa determinada região
Se PNA repetição por agentes atípicos: considerar os antibiogramas prévios
Período neonatal: ampicilina+ aminoglicosídeo ou
ampicilina+ cefalosporina de 3ª geração
1-3 meses: cefalosporina de 3ª geração
> 3 meses: amoxicilina+ acido clavulânico ou cefuroxima
Urocultura de controlo: se após 48-72h de início da antibioterapia não houver melhoria clínica (Oreskovic NM, 2007; Currie ML, 2003)

Tratamento:
• Diagnóstico e tratamento da disfunção vesical e/ou obstipação
• Diagnóstico e tratamento de malformação nefro-urológica associada
• Outros: derivados do arando; probióticos;...
“There is some evidence from two good quality RCTs that cranberry juice may decrease the number of symptomatic UTIs over a 12 month period in women.”
Cochrane Database Syst Rev. 2008 Jan 23;(1):CD001321
“Ongoing research reveals a promising capability to selectively target the gastrointestinal reservoirs of bacterias causing UTIs for elimination using probiotics.”
Storm DW et al. Novel management of urinary tract infections. Curr Opin Urol, 2011; 21(4): 328-33

Disfunção vesical:
• predispõe a ITUs repetição e lesão renal
(van Gool JD, 1992; Koff SA, 1998)
• diminui a probabilidade de resolução espontânea do refluxo
(Seruca H, 1989; Arant BS, 1992)
• associa-se a maior falência na correcção cirurgica de RVU
(Ditchfield MR, 1994; Merrick MV, 1995)

Disfunção vesical:
Tipos de disfunção:
Bexiga hiperactiva: contracção vesical anómala durante a fase de
enchimento. Sintomas: urgência; incontinência diurna; frequência urinária aumentada; manobras de retenção
Bexiga hipoactiva: micções muito pouco frequentes; manobras de
retenção; incontinência diurna; grandes volumes residuais vesicais
Micção disfuncional: incapacidade de relaxamento do esfincter uretral e/ou
pavimento pélvico durante a micção; associa-se com frequência a eliminação intestinal disfuncional: obstipação/encoprese
...
Tratamento: comportamental, farmacológico e controlo da obstipação

Seguimento:
• Orientação após 1º episódio para consulta de Nefrologia pediátrica:
- Urossepsis
- PNA associada a IRA
- Abcesso renal
- Infecção por agentes atípicos (não E. coli)
- Infecções recorrentes
- Alterações ecográficas: alteração da ecogenecidade do parênquima;
assimetria significativa do tamanho renal; malformação do sistema
excretor; suspeita de disfunção vesical

Seguimento:
ITU febril
Eco CUMS
DMSA
+
RVU
-
Normal
Sem necessidade de avaliação posterior
Avaliar a probabilidade de disfunção vesical
-
Tratamento médico e/ou cirurgico do RVU
+
ITUs recorrentes
DMSA
-
Normal +
CUMS
-
+
Adaptado de Prasad M, Cheng EY. Radiographic evaluation of children with febrile UTI: Bottom-up, Top-down or none of the above?. Advances in Urology, 2012.
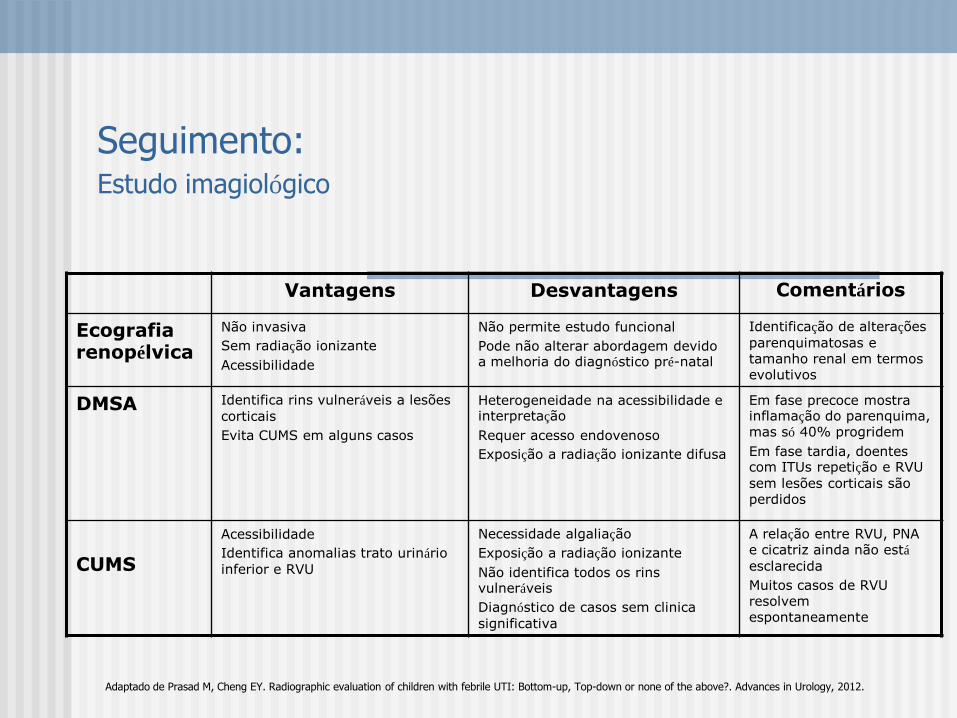
Seguimento: Estudo imagiológico
Vantagens Desvantagens Comentários
Ecografia renopélvica
Não invasiva
Sem radiação ionizante
Acessibilidade
Não permite estudo funcional
Pode não alterar abordagem devido a melhoria do diagnóstico pré-natal
Identificação de alterações
parenquimatosas e tamanho renal em termos evolutivos
DMSA Identifica rins vulneráveis a lesões
corticais
Evita CUMS em alguns casos
Heterogeneidade na acessibilidade e interpretação
Requer acesso endovenoso
Exposição a radiação ionizante difusa
Em fase precoce mostra inflamação do parenquima, mas só 40% progridem
Em fase tardia, doentes com ITUs repetição e RVU
sem lesões corticais são perdidos
CUMS
Acessibilidade
Identifica anomalias trato urinário
inferior e RVU
Necessidade algaliação
Exposição a radiação ionizante
Não identifica todos os rins vulneráveis
Diagnóstico de casos sem clinica
significativa
A relação entre RVU, PNA e cicatriz ainda não está
esclarecida
Muitos casos de RVU resolvem espontaneamente
Adaptado de Prasad M, Cheng EY. Radiographic evaluation of children with febrile UTI: Bottom-up, Top-down or none of the above?. Advances in Urology, 2012.
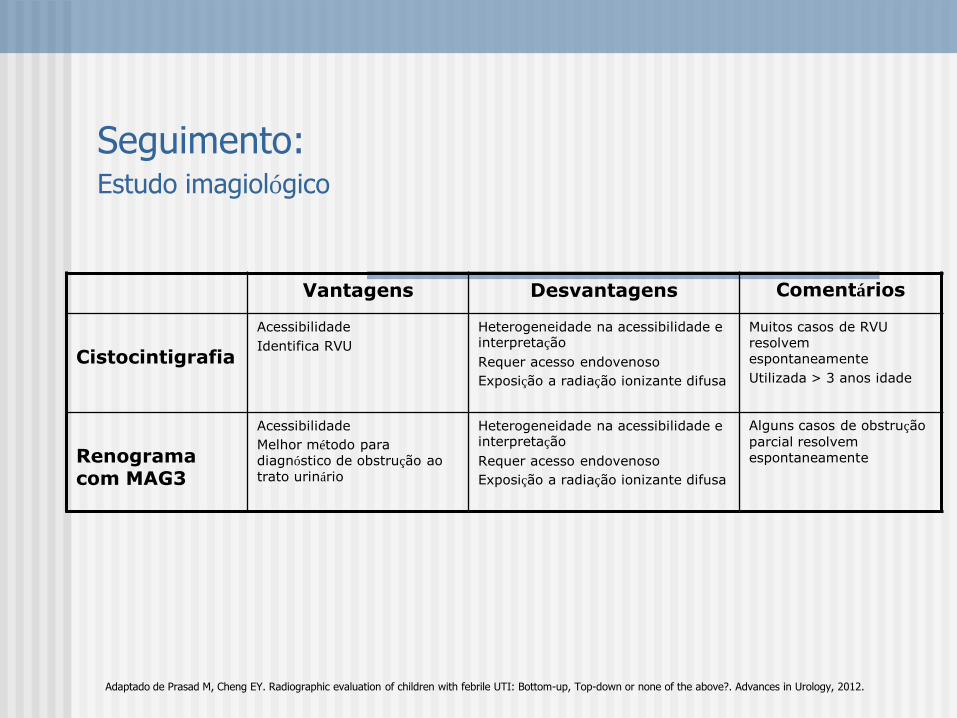
Seguimento: Estudo imagiológico
Vantagens Desvantagens Comentários
Cistocintigrafia
Acessibilidade
Identifica RVU
Heterogeneidade na acessibilidade e interpretação
Requer acesso endovenoso
Exposição a radiação ionizante difusa
Muitos casos de RVU resolvem espontaneamente
Utilizada > 3 anos idade
Renograma com MAG3
Acessibilidade
Melhor método para diagnóstico de obstrução ao trato urinário
Heterogeneidade na acessibilidade e interpretação
Requer acesso endovenoso
Exposição a radiação ionizante difusa
Alguns casos de obstrução
parcial resolvem espontaneamente
Adaptado de Prasad M, Cheng EY. Radiographic evaluation of children with febrile UTI: Bottom-up, Top-down or none of the above?. Advances in Urology, 2012.
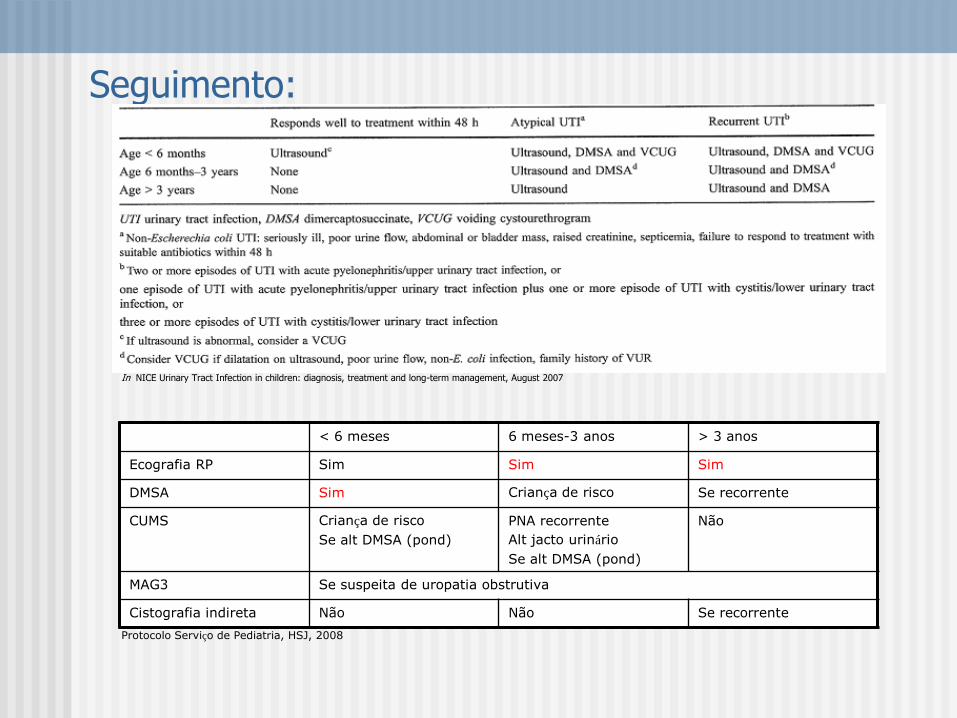
Seguimento:
In NICE Urinary Tract Infection in children: diagnosis, treatment and long-term management, August 2007
< 6 meses 6 meses-3 anos > 3 anos
Ecografia RP Sim Sim Sim
DMSA Sim Criança de risco Se recorrente
CUMS Criança de risco
Se alt DMSA (pond)
PNA recorrente
Alt jacto urinário
Se alt DMSA (pond)
Não
MAG3 Se suspeita de uropatia obstrutiva
Cistografia indireta Não Não Se recorrente
Protocolo Serviço de Pediatria, HSJ, 2008

Urinary tract infection in
children
Urinary tract infection in children:
diagnosis, treatment and long-term
management
In European Journal of Ped Surgery, June 2011
Experience with the NICE Guidelines for Imaging Studies in Children
with First Pyelonephritis.
Lytzen R, Thorun J, Cortes D
Department of Paediatrics, Hvidovre Hospital, Section of Endocrinology, Denmark.
Abstract
PURPOSE:
This retrospective study evaluates the applicability of a selective approach for imaging in children aged 0-15 years with a first
episode of pyelonephritis, based on the UTI guidelines of the
National Institute for Health and Clinical Excellence (NICE).
MATERIAL AND METHODS:
A total of 96 consecutive patients were included (age range: 0.1-14.9 years, median age: 0.7 years), treated for a first episode of
confirmed culture-positive pyelonephritis. At initial hospitalization
all patients underwent ultrasound examination of the kidneys and urinary tract (US) and technetium-99m mercaptoacetyltriglycine
scinti- and renography ( (99m)Tc MAG3). If vesicoureteral
reflux (VUR) was suspected, then prophylactic antimicrobial therapy was prescribed and the patients were referred to a surgeon for
further evaluation including voiding cystoureterography (VCU).
Patients with known urological anomalies including antenatally diagnosed anomalies were excluded. All patients were followed up
for a median of 5.2 years (3.5-8.6 years).
RESULTS:
Initially, US findings were abnormal in 29 (30%) patients and (99m)Tc MAG3 findings were abnormal in 20 (21%) cases. At follow-
up, prophylactic antimicrobial therapy was prescribed for 19
(20%), and VUR was diagnosed by VCU in 9 patients. Surgery was carried out in 7 (7%) patients, primarily for VUR. If the NICE
guidelines had been initially followed, 5 of our 9 patients with
VUR would not have been identified. VUR surgery was performed in 4 of these cases. Moreover, 9 cases with urological anomalies
subsequently prescribed prophylactic antimicrobial therapy
would have been missed.
CONCLUSION:
We do not recommend following the imaging strategies of the NICE guidelines for
children with a first episode of pyelonephritis. Our most important argument is that at
follow-up, after a minimum of 3.5 years, the initial diagnosis of VUR would have been
missed in 4 out of the 5 patients who underwent VUR surgery. © Georg Thieme Verlag KG Stuttgart · New York.

Seguimento: Profilaxia antibiótica
Quem deve fazer? • RVU grau III-V
• < 1ano RVU qq grau e 1PNA
• 6-12 meses após PNA (RVU)
• ITUs repetição e disfunção vesical
ou lesões corticais renais
Antibióticos:
Trimetoprim 1-2 mg/kg/dia
Nitrofurantoína 1 mg/kg/dia
TMP/SMZ 2 mg/kg/dia
Cefaclor 10-15 mg/kg/dia
In Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the initial UTI in febrile infants and children. Pediatrics, September 2011

American Academy of Pediatrics Clinical Practice Guideline
(Pediatrics, 128 (3); September 2011)
1. Se uma criança (2-24 meses) com febre sem foco vai iniciar atb, deverá colher sedimento urinário e urocultura por algaliação ou PSP antes de iniciar antibioterapia (nível de evidência A)
2. Se uma criança (2-24 meses) com febre sem foco não vai iniciar atb, o médico determina a probabilidade de ITU (nível de evidência A):
2a. Se a probabilidade é baixa pode manter apenas vigilância
2b. Se a probabilidade não é baixa, tem duas opções: colher de imediato por algaliação ou PSP ou colher sedimento urinário pelo método mais acessível e se alterações (leucócitos, nitritos ou bacteriuria), colher posteriormente por algaliação ou PSP. Se o sedimento é normal (sem leucocituria, nitrituria ou
bacteriuria) pode manter vigilancia sem atb reconhecendo no entanto que o sedimento urinário normal não exclui com certeza uma ITU

American Academy of Pediatrics Clinical Practice Guideline
(Pediatrics, 128 (3); September 2011)
3. Para estabelecer o diagnóstico de ITU é necessário quer a presença de piúria e/ou bacteriúria quer a presença de pelo menos 50 000 UFC/ml de um uropatogénio obtido por cateterismo vesical ou punção suprapúbica (nível de evidência C)
4. Quando iniciar o tratamento, o médico deve escolher a via de administração de acordo com as recomendações práticas. A via oral ou parentériaca são igualmente eficazes. Deve escolher o antibiótico de acordo com a sensibilidade local dos agentes uropatogénicos e ajusta-la posteriormente com o antibiograma (nivel de evidência A). O tratamento deve ter entre 7 e 14 dias (nível de evidência B)
5. Lactentes com ITUs febris devem efectuar ecografia renovesical (nível de evidência C)

American Academy of Pediatrics Clinical Practice Guideline
(Pediatrics, 128 (3); September 2011)
6. A CUMS não deve ser realizada de rotina após 1ª ITU febril. CUMS está indicada se a
ecografia revelar hidronefrose, lesões corticais ou outros achados que sugiram RVU de alto grau ou uropatia obstrutiva, bem como em outras circunstâncias clínicas complexas ou atípicas (nível de evidência B). A avaliação deve prosseguir
se houver ITUs febris recorrentes.
7. Após confirmação de ITU, os pais devem ser instruídos para procurarem avaliação médica (idealmente em 48 horas) numa futura intercorrência febril, de forma a uma nova ITU ser diagnosticada e tratada o mais precocemente possível (nível de
evidência C).
O que se está a planear?
Diagnóstico
• utilizar sempre o método de colheita mais apropriado
• desenvolver outros marcadores biológicos de infecção (MMP-9u, procalcitonina) e de RVU (procalcitonina, proteoma urinário- Drube et al, 2012)
• ITUs clinicas com crescimento bacteriano inferior ao esperado devem
ser incluidas nos estudos
• esclarecimento da relação RVU- lesão cortical (papel citoquinas-
dexametasona)
Seguimento
• novos métodos de imagem: cistourografia interactiva-RM;urografiaRM
• esclarecimento papel da atb profiláctica (vs antissépticos urinários)

Obrigada pela vossa atenção!

1. Febrile Urinary Tract Infections in Children. Montini G, Tullus K, Hewitt I. N Engl J Med, July 2011; 365: 239-250. 2. Long term antibiotics for preventing recurrent urinary tract infection in children (Review). Williams G, Craig JC. The Cochrane Collaboration, 2011. 3. Urinary tract infection: Clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Subcommittee on Urinary Tract Infection (American Academy of Pediatrics). Pediatrics, Sept 2011, 128(3):595-609. 4. Radiographic evaluation of children with febrile urinary tract infection: bottom-up, top-down, or none of the above? Prasad M, Cheng E. Adv Urology, 2012 (Epub ahead of print) 5. Difficulties in diagnosing urinary tract infections in small children. Tullus K. Pediatr Nephrol, 2011, 26: 1923-1926. 6. Complicaciones del cateterismo vesical realizado en un servicio de urgencias para obtener una muestra de orina. Vásquez S, Oñoro G et al. An Pediatr (Barc), 2011
7. The demographics and costs of inpatiente vesicoureteral reflux management in the USA. Spencer JD, Schwaderer A et al. Pediatr Nephrol, 2011; 10, (Epub ahead of print) 8. Urinary MMP-9/NGAL complex in children with acute cystitis. Hatipoglu S, Sevketoglu E et al. Pediatr Nephrol, 2011, 26(8): 1263-1268. 9. Novel management of urinary tract infections. Storm DW, Patel AS et al. Curr Opin Urol, 2011; 21(4): 328-333. 10. Vesicoureteral reflux: the RIVUR Study and the way forward. Greenfield S et al. J Urol, 2008, 179: 405-407. 11. Procalcitonin is a predictor for high-grade vesicoureteral reflux in children: meta-analysis of individual patient data. Leroy S, Romanello C et al. J Pediatr, 2011 (Epub ahead of print) 12. The Swedish reflux trial:Review of a randomized, controlled trial in children with dilating vesicoureteral reflux. Brandstrom P, Jodal U, et al. J Pediatr Urol, 2011 (Epub ahead of print) 13. Treatment and prophylaxis in pediatric urinary tract infection. Nickavar A, Sotoudeh K. Int J Prev Med, 2011; 2(1): 4-9. 14. Procalcitonin a key marker in children with urinary tract infection. Leroy S, Gervaix A. Adv Urol, 2011 (Epub ahead of print) 15. Comparaison de deux protocoles de prise en charge des infections urinaires fébriles de l’enfant. Blanchais T, Legrand A et al. Arch Pédiatrie, 2011; 18: 955-961.
16. Urinary proteome analysis to exclude severe vesicoureteral reflux. Drube J, Schiffer E et al. Pediatrics, 2012; 129(2): 356-363. 17. The role of dexamethasone on decreasing urinary cytokines in children with acute pyelonephritis. Sharifian M, Anvaripour N et al. Pediatr Nephrol, 2008; 23 (9): 1511-1516. 18. Early management and long-term outcomes in primary vesico-ureteric reflux. Coleman R. B J Urol Int, 2011; 108 (Suppl 2): 3-8.
Bibliografia: