individualized medicine in ra (dr. ws chen)
Post on 21-Jul-2015
313 views
TRANSCRIPT
台北榮總 過敏免疫風濕科
陳瑋昇 主治醫師
Introduction (簡介)
Individualized Medicine in RA (21 May 2014)
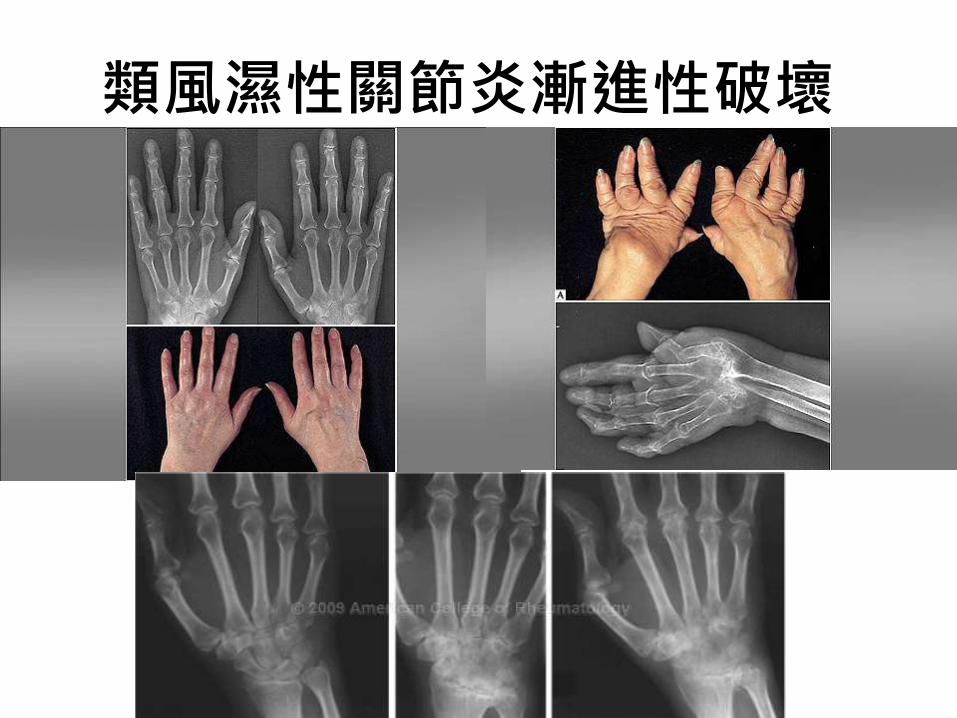
類風濕性關節炎漸進性破壞
嚴重度
(arb
itra
ry u
nit
s)
0
發病時間 (年)
5 10 15 20 25 30
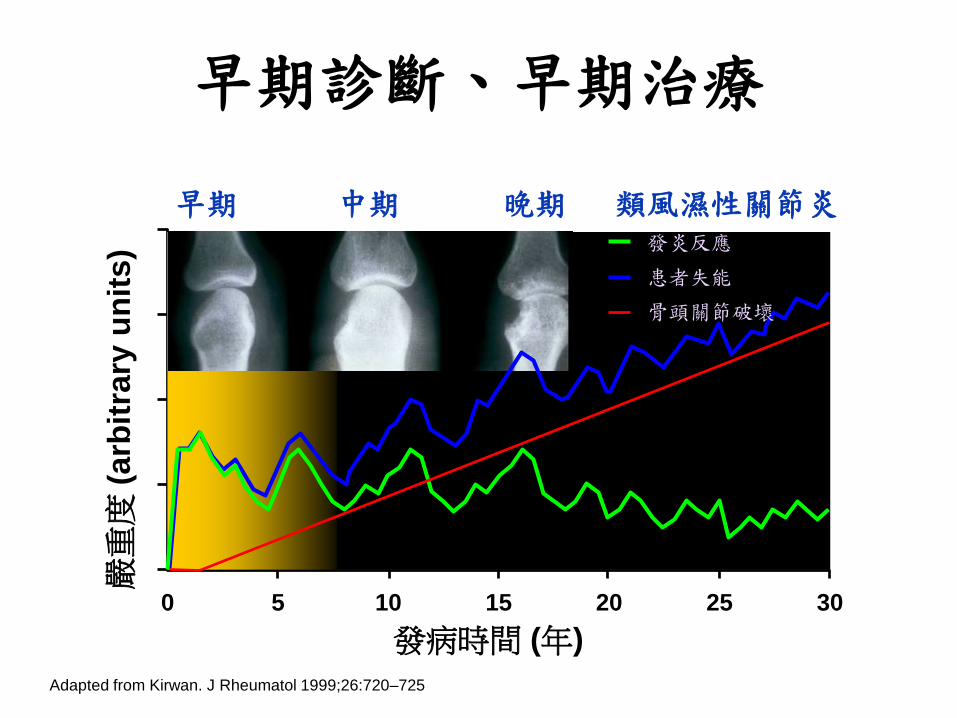
早期 中期 晚期 類風濕性關節炎
Adapted from Kirwan. J Rheumatol 1999;26:720–725
發炎反應
患者失能
骨頭關節破壞
早期診斷、早期治療
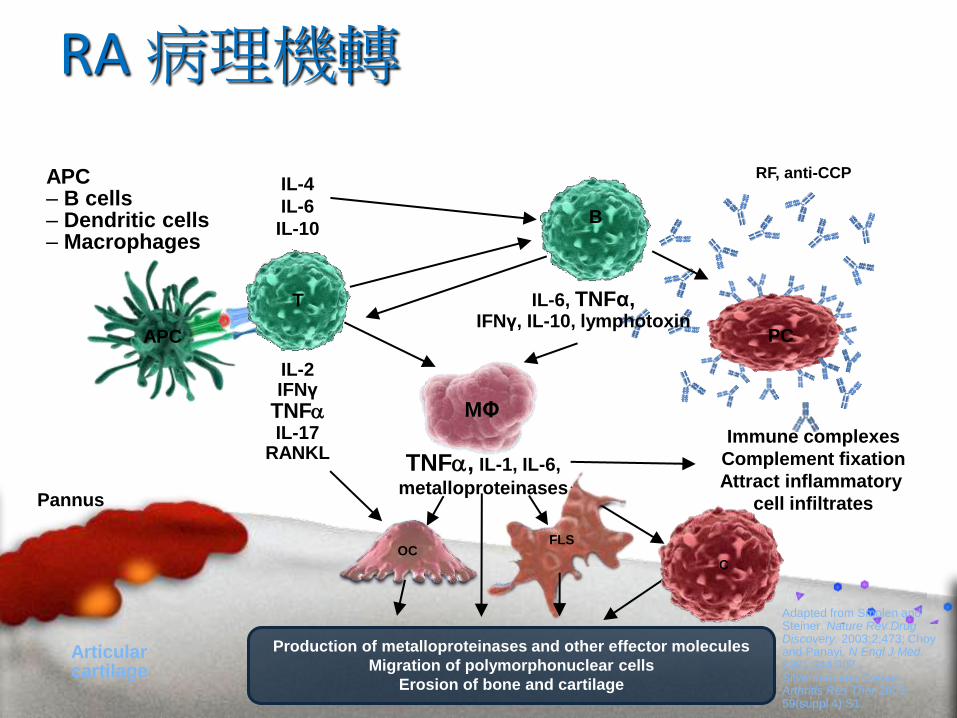
RA病理機轉
Immune complexes
Complement fixation
Attract inflammatory
cell infiltrates
IL-2IFNγ
TNFaIL-17
RANKL
Pannus
Articularcartilage
IL-4
IL-6
IL-10
IL-6, TNFα,IFNγ, IL-10, lymphotoxin
Adapted from Smolen and Steiner. Nature Rev Drug Discovery. 2003;2;473; Choy and Panayi. N Engl J Med.2001;344:907., Silverman and Carson. Arthritis Res Ther 2003; 59(suppl 4):S1.
APC– B cells– Dendritic cells– Macrophages
Production of metalloproteinases and other effector molecules
Migration of polymorphonuclear cells
Erosion of bone and cartilage
RF, anti-CCP
APC
TNFa, IL-1, IL-6,
metalloproteinases
T
B
C
FLSOC
PC
MΦ
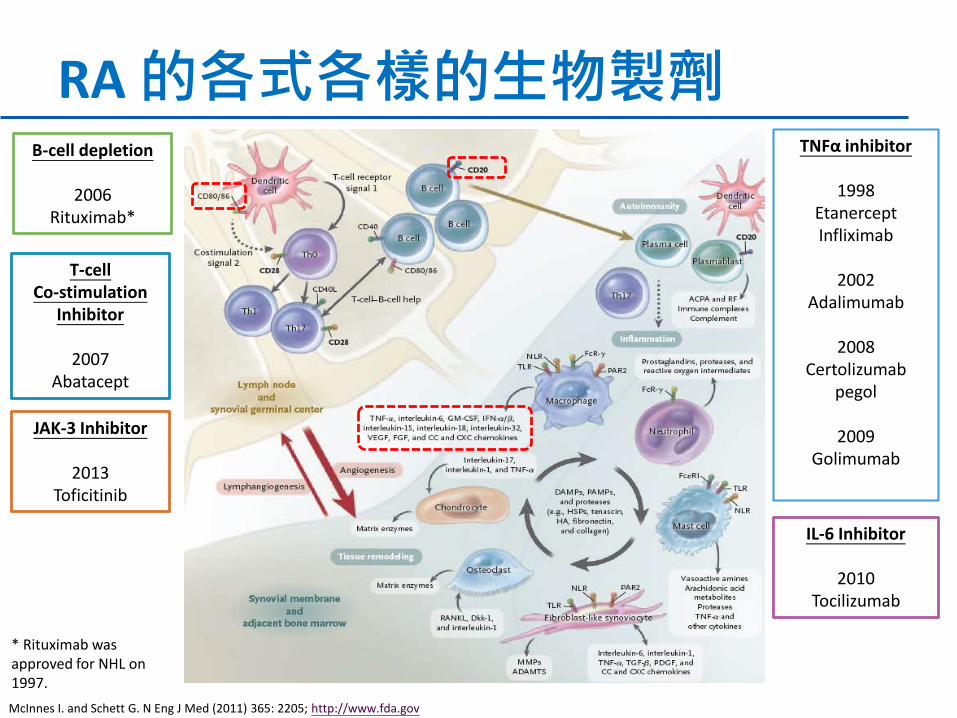
RA的各式各樣的生物製劑
McInnes I. and Schett G. N Eng J Med (2011) 365: 2205; http://www.fda.gov
TNFα inhibitor
1998 EtanerceptInfliximab
2002 Adalimumab
2008 Certolizumab
pegol
2009 Golimumab
B-cell depletion
2006 Rituximab*
IL-6 Inhibitor
2010 Tocilizumab
T-cell Co-stimulation
Inhibitor
2007 Abatacept
* Rituximab was approved for NHL on 1997.
JAK-3 Inhibitor
2013Toficitinib
Anti-CD20
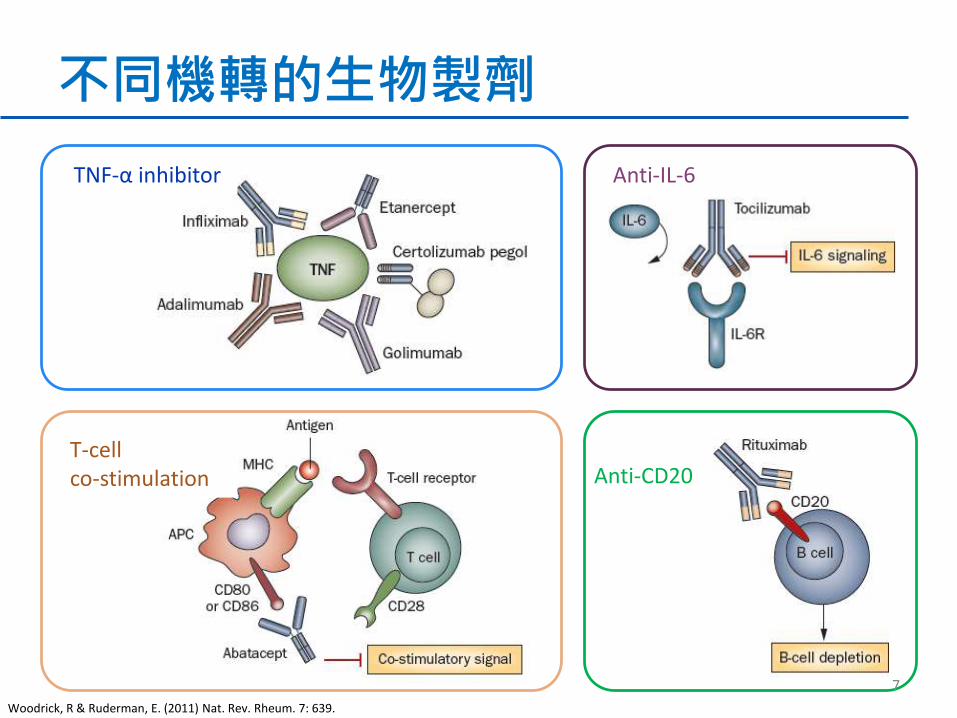
不同機轉的生物製劑
TNF-α inhibitor Anti-IL-6
T-cell co-stimulation
Woodrick, R & Ruderman, E. (2011) Nat. Rev. Rheum. 7: 639.
7

• 類風濕性關節炎的達標治療,其重點在於藉著訂定治療的目標以及發展治療的策略,希望能早期達到治療的目標,而且要繼續維持,以避免骨骼破壞和失能。
• 目前,許多國家都在推動類風濕性關節炎 T2T (Treat to Target) 的治療,在台灣稱為「達標治療」。
Smolen J. et al. Ann Rheum Dis (2010) 69: 631–637; 蔡嘉哲 et al. 中華民國風濕病醫學會 (2011)
Treat to Target (達標治療)
Individualized Medicine in RA (個人化醫療)
Individualized Medicine in RA (21 May 2014)

What is “Personalized Healthcare” ?
• Personalized medicine is a medical model that propose the customization of healthcare - with medical decisions, practices, and/or products being tailored to the individual patient.
Different therapies by different biomarker profiles
A group of patient with the same symptoms
Different Targeted Therapies
http://en.wikipedia.org/wiki/Personalized_medicine, retrieved on 24 March 2013; http://www.roche.com/about_roche/personalised_healthcare.htm, retrieved on 24 March 2013
Personalised/stratified medicine(個人化醫療)
• 現在有非常多種的生物製劑可以選擇
• 在這些治療裡面不同族群的病人有不同的治療效果與副作用
Clinical trials and real-life experience demonstrating significant interpatient
heterogeneity in efficacy as well as important adverse effects of these treatments
• 我們希望有最大的療效最少的副作用來達到減少關節的破壞傷害, 進一步希望能預測不同藥物的治療效果與副作用
In order to maximise their benefit:risk ratios and to minimise later joint
damage, predictors needed to define response and, ideally, adverse effects for each of these drugs
Isaacs J & Ferraccioli G. Ann Rheum Dis 2011;70:4–7.
Personalised/stratified medicine(個人化醫療)
• 有很多的研究對個人化醫療有興趣
Huge interest in this field of ‘personalised medicine
• 也就是讓治療量身訂做
Matching the treatment to the patient
• 減少疾病活性
Minimises periods of disease activity
• 保護關節維持功能
Protects joints, maintains function
• 減少副作用與共病
Should minimise adverse effects and comorbidity
• 降低治療的花費
Reduces costs of treatment
Isaacs J & Ferraccioli G. Ann Rheum Dis 2011;70:4–7.
Approaches to personalised/stratified medicine如何來做?
• 臨床徵候
Clinical features
• 血清學
Serology, proteomics
• 組織學
Histology
• 基因體學
Genomics
• 綜合以上各點
Combinations
Isaacs J & Ferraccioli G. Ann Rheum Dis 2011;70:4–7.
為什麼 RA 會是「個人化醫療」的目標?
• 疾病的診斷主要是以症狀為主。
• 在關節的滑膜腔內
– 有不同的白血球滲入(infiltration)和不同的細胞激素(cytokines)表現模式。
– 在基質細胞內也有不同的基因表現型式。
• 在周邊血液中
– 不同的自體免疫抗體可能會影響診斷結果(RF、Anti-CCP),這些自體免疫抗體的表可以視做不同的疾病起因。
– 不同的基因「簽章」(gene signatures)。
– 對不同的標靶治療有不同的反應。
RA 與其說是一種疾病,還不如說是「一些症狀的總和」
病人可能可以用不同的生物標記分成不同群組
Choy et al. Nat. Rev. Rheumatol. (2013) 9, 154–163; Tak, PP. Rheumatology (2012) 51: 600-609
Individualized Medicine in RA (21 May 2014)
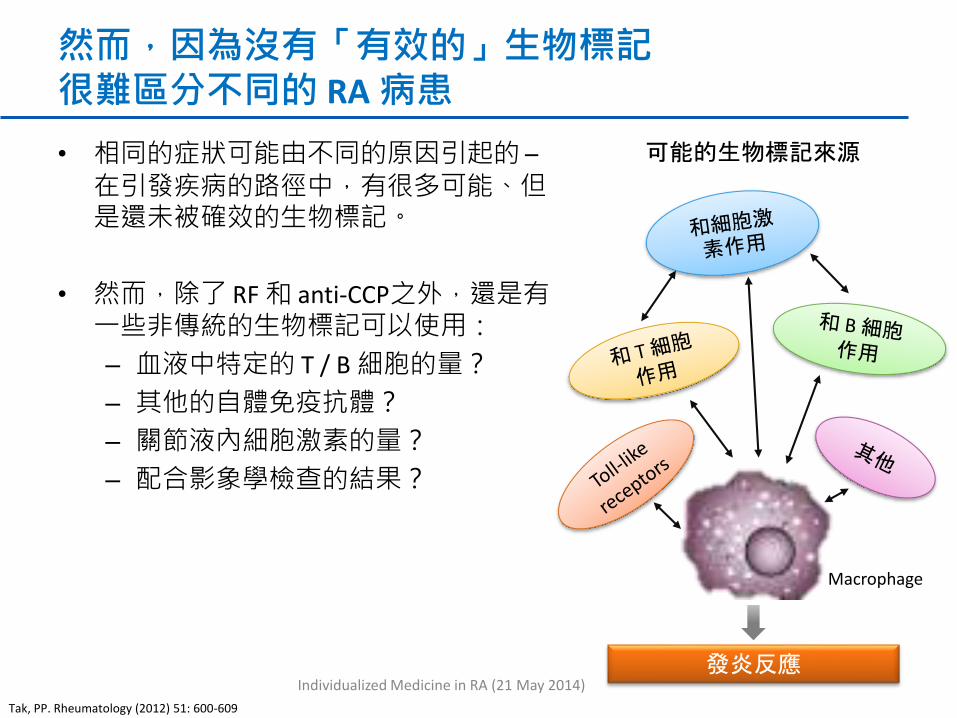
然而,因為沒有「有效的」生物標記很難區分不同的 RA 病患
• 相同的症狀可能由不同的原因引起的 –在引發疾病的路徑中,有很多可能、但是還未被確效的生物標記。
• 然而,除了 RF 和 anti-CCP之外,還是有一些非傳統的生物標記可以使用:
– 血液中特定的 T / B 細胞的量?
– 其他的自體免疫抗體?
– 關節液內細胞激素的量?
– 配合影象學檢查的結果?
Macrophage
可能的生物標記來源
發炎反應
Tak, PP. Rheumatology (2012) 51: 600-609
Individualized Medicine in RA (21 May 2014)
為什麼我們會想做 RA 的個人化(Individualized)醫療?
• 目前的 RA 治療方式大致都合手「ACR Rule」--也就是達到 ACR 20, 50, 70 的病患數達到 60%, 40%, 20%。
• 但是,我們要怎麼幫病患選擇「最合適」的藥物?
Risk A Comorbidity B Risk C
Drug A Drug B Drug C
Individualized Medicine in RA (21 May 2014)
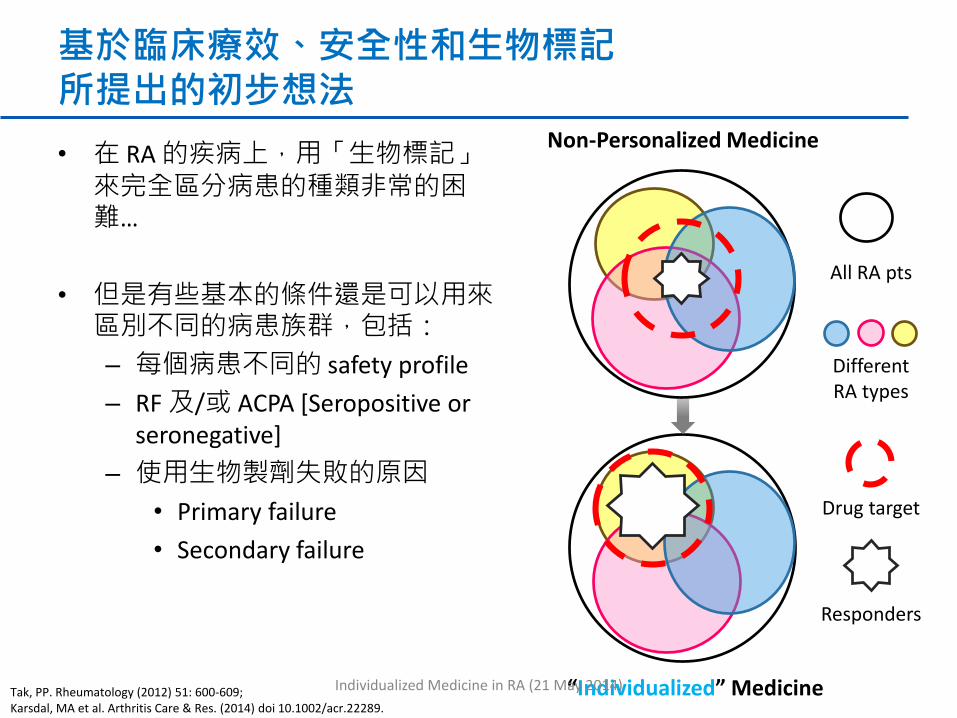
基於臨床療效、安全性和生物標記所提出的初步想法
• 在 RA 的疾病上,用「生物標記」來完全區分病患的種類非常的困難…
• 但是有些基本的條件還是可以用來區別不同的病患族群,包括:
– 每個病患不同的 safety profile
– RF 及/或 ACPA [Seropositive or seronegative]
– 使用生物製劑失敗的原因
• Primary failure
• Secondary failure
Non-Personalized Medicine
“Individualized” Medicine
Different RA types
All RA pts
Drug target
Responders
Tak, PP. Rheumatology (2012) 51: 600-609; Karsdal, MA et al. Arthritis Care & Res. (2014) doi 10.1002/acr.22289.
Individualized Medicine in RA (21 May 2014)

Date of preparation: April 2011, RXUKMABR00281m
那些病人對腫瘤壞死因子抑制劑效果好?
丹麥DANBIO registry: 對第一個TNFi 效果差的因素有:
– 年紀較大
– 併用類固醇者
– 關節功能較差者
義大利GISEA study 看哪需因素在第六個月容易達到緩解?
– 類風濕因子陰性
– 年齡小於53
– 男性
Isaacs J & Ferraccioli G. Ann Rheum Dis 2011;70:4–7.

Date of preparation: April 2011, RXUKMABR00281m
BSRBR/BRAGGSS: 血清陽性或陰性對TNFi 療效的差別
Predictor n (%)*Mean DAS score (SD)
AssociationBaseline Improvement
RF– 59 (11) 6.72 (1) 3.03 (1.7)p=0.02†
RF+ 462 (89) 6.59 (1) 2.43 (1.5)
ACPA– 96 (18) 6.61 (1) 2.90 (1.6)p=0.02†
ACPA+ 425 (82) 6.61 (1) 2.40 (1.5)
BRAGGSS = Biologics in Rheumatoid Arthritis Genetics and Genomics Study Syndicate
* Analyses performed in 521 patients for whom serum samples were available † Linear regression, adjusted for concurrent DMARD use,
sex and baseline HAQ and DAS28 score
Potter C, et al. Ann Rheum Dis 2009;68:69–74.
Date of preparation: April 2011, RXUKMABR00281m
29
75
14
44
0
10
20
30
40
50
60
70
80
Placebo + MTX Rituximab 2 x 1000 mg +
MTX
Placebo + MTX Rituximab 2 x 1000 mg +
MTX
Pa
tie
nts
(%
) (
Go
od
/Mo
d. E
UL
AR
re
sp
on
se
)
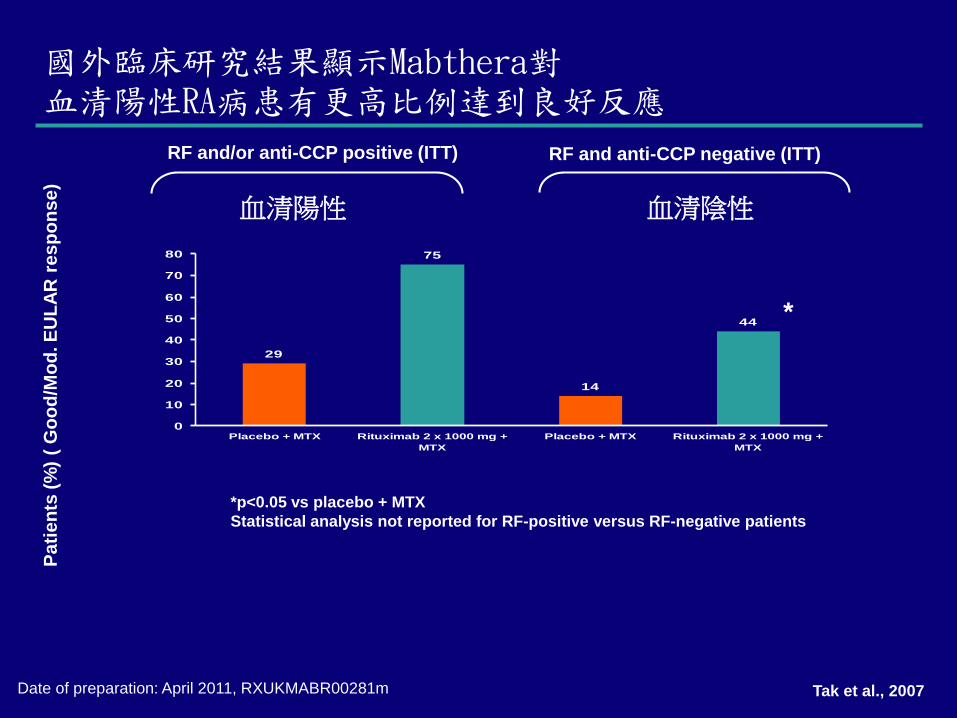
RF and/or anti-CCP positive (ITT) RF and anti-CCP negative (ITT)
*
國外臨床研究結果顯示Mabthera對血清陽性RA病患有更高比例達到良好反應
*p<0.05 vs placebo + MTX
Statistical analysis not reported for RF-positive versus RF-negative patients
Tak et al., 2007
血清陽性 血清陰性

Date of preparation: April 2011, RXUKMABR00281m
對第一種腫瘤壞死因子抑制劑(aTNF)治療失敗的RA患者,使用第二種aTNF 與 B 細胞療法(RTX)的比較
RA
疾病活動度
B細胞標靶療法(RTX)療效優於第二種腫瘤壞死因子抑制劑
Finckh et al. ARD 2010
Date of preparation: April 2011, RXUKMABR00281m
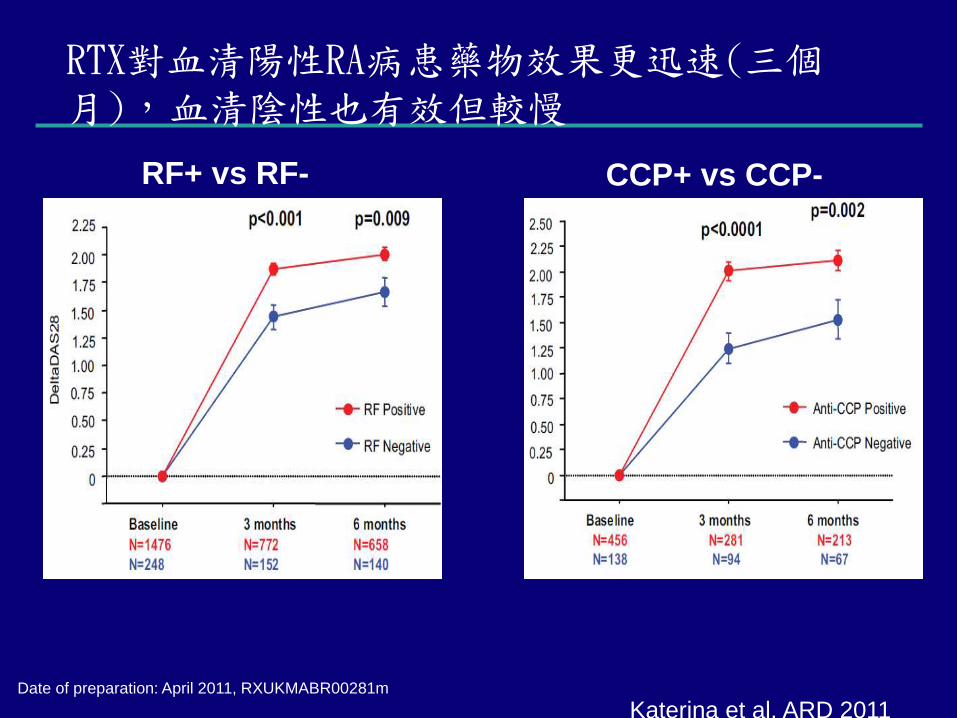
RTX對血清陽性RA病患藥物效果更迅速(三個月),血清陰性也有效但較慢
RF+ vs RF- CCP+ vs CCP-
Katerina et al. ARD 2011

Date of preparation: April 2011, RXUKMABR00281m
Dennis and colleagues have identified distinct pretreatment gene expression profiles in affected synovial tissue
specimens and a tissue type-related systemic protein pattern which are associated with a positive or negative
clinical outcome to monotherapy with adalumimab (anti-TNFα) and tocilizumab (anti-IL-6 receptor).
科學家發現滑膜組織或系統性蛋白可以跟TNFi
與anti-IL-6 的治療效果有關

• Cardiovascular disease• Other autoimmune
diseases
• Switch• Comparative
Effectiveness
RA 的個人化醫療(Individualized medicine)考量
• 除了一般的療效和安全性之外,也開始注重病患本身的危險因子及合併症。
RA 治療方式
危險因子
療效
合併症
安全性
• Latent TB Infection• Malignancy
• Infection • Other
complication
pSS, vasculitisCV Risk
TB, Hep B/CHerpes
• CV disease risk

A Proposed Treatment Algorithm For Individualized Medicine in RA
診斷RA安全性考量
1st腫瘤壞死因子抑制劑(TNFi) + 傳統抗風濕藥物 (±類固醇)
原發性TNFi療效不佳 次發性TNFi療效不佳(產生抗藥性)
有沒有惡性腫瘤
有沒有結核病史
Consider RTX**
RF+ and/or ACPA+
RF- and ACPA-RF+ and/or
ACPA+RF- and ACPA-
ABA, RTX, TOC ABA, TOC ABA, RTX, TOC or 2nd TNFi
ABA, TOC or 2nd TNFi
Adapted from Tak, PP. Rheumatology (2012) 51: 600-609.
Take Home Messages
Individualized Medicine in RA (21 May 2014)

Take Home Messages (結論)
• 類風濕關節炎的病友很多, 雖然症狀表現很相似, 但個別的病理機轉可能有所不同RA is a disease with the same symptoms but those may come from different
pathogenetic origins.
• 目前有很幾種生物製劑可以選擇, 希望能有更多預測因子讓我們能選擇針對個人更有效的治療Currently, several biologics are available for RA patients, however, there is a “ceiling”
(ACR rules) of their efficacy, which means, we may consider more factors to give patients’ better experiences in RA treatment.
• 個人化醫療很適合應用在類風溼性關節炎, 但仍需要更多的研究資料來提供更好的生物標記Concept of personalized medical may be suitable for RA, however, more studies in
biomarker researches is warranted.
Individualized Medicine in RA (21 May 2014)
Thank You.
Individualized Medicine in RA (21 May 2014)