indiana cancer consortium...
TRANSCRIPT
annual reportINDIANA CANCER CONSORTIUM


1
Dear Colleagues,
In October 2001, a handful of organizations in Indiana formed under a
united mission to make a difference in cancer through a collaborative
process. Today, over 200 organizational and individual members support the
Indiana Cancer Consortium’s (ICC’s) mission to reduce the state’s cancer
burden through the implementation of a comprehensive plan that addresses
the entire cancer continuum – prevention, early detection, treatment, and
quality of life.
It is in this multi-sectored and diverse membership that the ICC finds a
unique strength in the fight against cancer. By uniting leaders across the
state, we collectively assess and approach Indiana’s disease challenges in
a way that no organization could undertake alone. Our members come
to the ICC meeting table ready to share expertise and resources; and in
return, they plan, contribute, and take advantage of a full range of free ICC
services — including professional trainings, educational publications, mini-
grants, and evidence-based guidance.
Together, Hoosiers have made great strides over the past several decades
in regard to cancer. However, while cancer rates have decreased, cancer
is still the second leading cause of death in Indiana. Approximately two in
five Indiana residents now living will eventually have cancer, suggesting that
every Hoosier has, or will have, a personal connection to cancer in some
way. As always, it is up to our members to help the ICC grow and make
more of an impact across Indiana.
As we look to the future, we hope you will continue to be our partner
in reducing the burden of cancer in Indiana. The ICC Steering Committee
remains committed to expanding the conversation of comprehensive
cancer control, and we sincerely thank you for your inspiring commitment,
ideas, and leadership.
Steve Tharp, M.D.Co-Chair, ICC
Sara EdgertonCo-Chair, ICC
insideABOUT ICC
INDIANA BURDEN UPDATE
PRIMARY PREVENTION
EARLY DETECTION
TREATMENT
QUALITY OF LIFE
DATA
ADVOCACY
SURVEY RESULTS
2013 PROJECTS
2
3
4
5
6
7
8
9
10
12
2
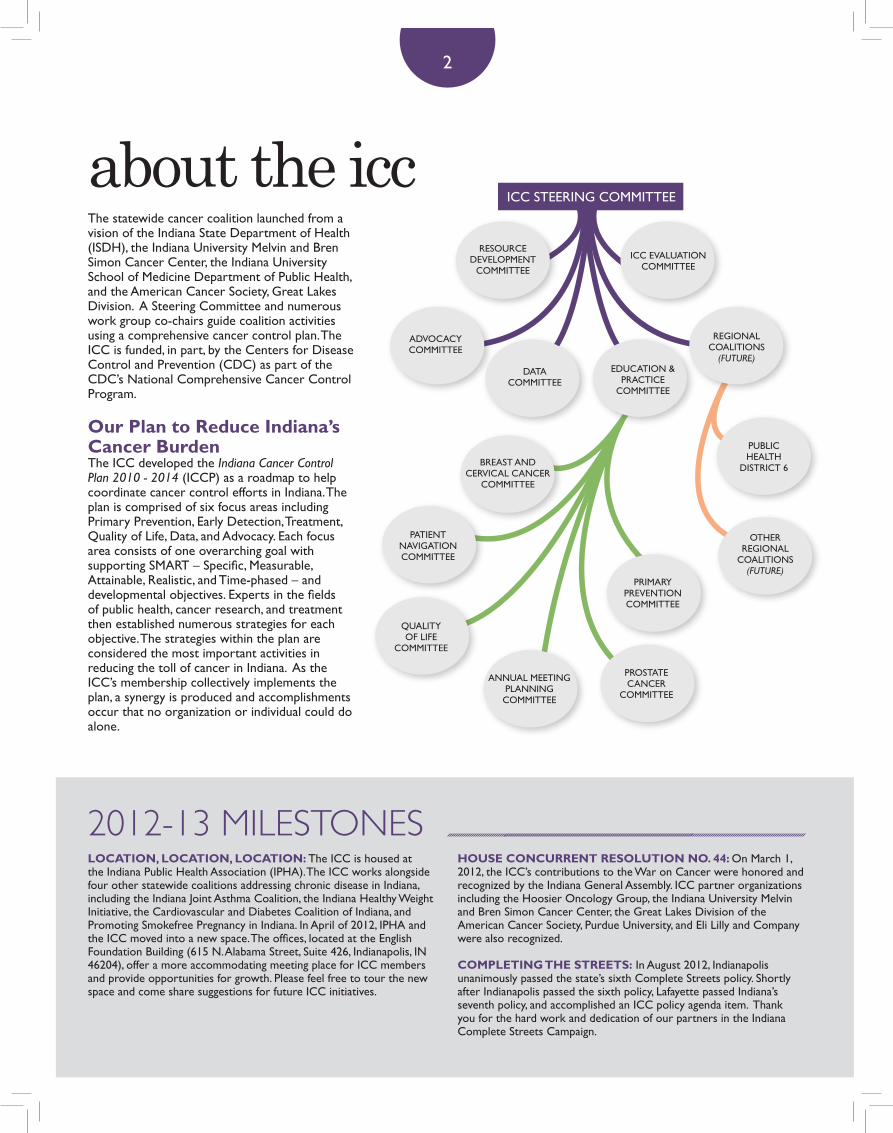
The statewide cancer coalition launched from a vision of the Indiana State Department of Health (ISDH), the Indiana University Melvin and Bren Simon Cancer Center, the Indiana University School of Medicine Department of Public Health, and the American Cancer Society, Great Lakes Division. A Steering Committee and numerous work group co-chairs guide coalition activities using a comprehensive cancer control plan. The ICC is funded, in part, by the Centers for Disease Control and Prevention (CDC) as part of the CDC’s National Comprehensive Cancer Control Program.
Our Plan to Reduce Indiana’s Cancer Burden The ICC developed the Indiana Cancer Control Plan 2010 - 2014 (ICCP) as a roadmap to help coordinate cancer control efforts in Indiana. The plan is comprised of six focus areas including Primary Prevention, Early Detection, Treatment, Quality of Life, Data, and Advocacy. Each focus area consists of one overarching goal with supporting SMART – Specific, Measurable, Attainable, Realistic, and Time-phased – and developmental objectives. Experts in the fields of public health, cancer research, and treatment then established numerous strategies for each objective. The strategies within the plan are considered the most important activities in reducing the toll of cancer in Indiana. As the ICC’s membership collectively implements the plan, a synergy is produced and accomplishments occur that no organization or individual could do alone.
LOCATION, LOCATION, LOCATION: The ICC is housed at the Indiana Public Health Association (IPHA). The ICC works alongside four other statewide coalitions addressing chronic disease in Indiana, including the Indiana Joint Asthma Coalition, the Indiana Healthy Weight Initiative, the Cardiovascular and Diabetes Coalition of Indiana, and Promoting Smokefree Pregnancy in Indiana. In April of 2012, IPHA and the ICC moved into a new space. The offices, located at the English Foundation Building (615 N. Alabama Street, Suite 426, Indianapolis, IN 46204), offer a more accommodating meeting place for ICC members and provide opportunities for growth. Please feel free to tour the new space and come share suggestions for future ICC initiatives.
HOUSE CONCURRENT RESOLUTION NO. 44: On March 1, 2012, the ICC’s contributions to the War on Cancer were honored and recognized by the Indiana General Assembly. ICC partner organizations including the Hoosier Oncology Group, the Indiana University Melvin and Bren Simon Cancer Center, the Great Lakes Division of the American Cancer Society, Purdue University, and Eli Lilly and Company were also recognized.
COMPLETING THE STREETS: In August 2012, Indianapolis unanimously passed the state’s sixth Complete Streets policy. Shortly after Indianapolis passed the sixth policy, Lafayette passed Indiana’s seventh policy, and accomplished an ICC policy agenda item. Thank you for the hard work and dedication of our partners in the Indiana Complete Streets Campaign.
about the icc
2012-13 MILESTONES
ICC STEERING COMMITTEE
RESOURCE DEVELOPMENT
COMMITTEE
PATIENT NAVIGATION COMMITTEE
PRIMARY PREVENTION COMMITTEE
QUALITYOF LIFE
COMMITTEE
ANNUAL MEETING PLANNINGCOMMITTEE
PUBLIC HEALTH
DISTRICT 6
OTHER REGIONAL
COALITIONS (FUTURE)
ICC EVALUATIONCOMMITTEE
ADVOCACYCOMMITTEE
DATACOMMITTEE
EDUCATION & PRACTICE
COMMITTEE
REGIONAL COALITIONS
(FUTURE)
BREAST AND CERVICAL CANCER
COMMITTEE
PROSTATECANCER
COMMITTEE

3
Cancer is the second leading cause of death in Indiana, claiming approximately 12,688 lives per year.1 Nearly 30 percent of new cancer cases are caused by tobacco use and another 43 percent exist because of lifestyle factors such as poor dietary habits, lack of exercise, not maintaining a healthy weight, occupational factors, and excessive alcohol intake. Nearly 65 percent of new cancer cases and 33 percent of cancer deaths could be prevented through lifestyle changes such as eliminated tobacco use, improving dietary habits, exercising regularly, maintaining a healthy weight, obtaining early detection cancer screening tests, and obtaining timely and appropriate treatment.
Indiana’s age-adjusted cancer incidence rate during 2005-2009 was 467.8 per 100,000 people. This was significantly lower than the national rate of 472.0 per 100,000 people. However, during the same
period, Indiana’s age-adjusted mortality (death) rate was nine percent higher than the national rate. This includes being 12 percent higher among Indiana males and eight percent higher among Indiana females. 2
The burden of specific cancer types among U.S. residents has changed over the years. For example, with the gradual decrease in smoking rates among Americans over the past several decades, lung cancer mortality rates have begun to decrease, especially among U.S. males. However, trends vary among the different cancer types. These statistics indicate that progress continues to be made in the early detection and treatment of certain cancers, and that the incidence and mortality of some cancers is declining. However, a significant cancer burden still exists among Indiana residents that requires continued, targeted cancer control efforts.
burden of cancer in Indiana
Due to Indiana’s high prevalence of smokers, lung cancer had the largest difference between Indiana and U.S. incidence and mortality rates, as the incidence rate among Indiana residents was 17 percent higher than the national average and the mortality rate was 22 percent higher.2
NATIONAL CANCER CONFERENCE: ICC members and staff attended the 2012 CDC National Cancer Conference in August. The event was held in Washington, D.C., with over 700 attendees who represented states, tribes, and districts across the nation. The ICC, the ISDH Cancer Control Section, and the Indiana Cancer Facts and Figures 2012 report were highlighted in a number of ways during the conference, including: featuring in the Stories of Success: Comprehensive Cancer Control in Action; earning a second place poster award in the Health Systems in a Changing Environment track; and presenting on GIS and cancer control by emphasizing the ICC local cancer control efforts.
NATIONAL SPOTLIGHT: The National Cancer Institute’s Research to Reality January cyber-seminar highlighted State Cancer Profiles. The ICC was invited to share Indiana’s experience in using State Cancer Profiles at the state and local levels. ICC leaders presented to 300 professionals around the nation and provided a practical example on how State Cancer Profiles can be applied to organizational planning and implementation efforts. The presentation highlighted the collaborative work of ICC partner organizations.
2012-13 MILESTONES (CONTINUED)

Individuals, organizations, and communities all contribute to primary prevention. Simply adopting specific lifestyle behaviors can significantly lower cancer risk. Healthy lifestyle behaviors include avoiding tobacco products and secondhand smoke, minimizing alcohol intake, following a balanced diet, exercising regularly, receiving recommended immunizations, and protecting against ultraviolet exposure. Other behaviors linked to cancer prevention include breastfeeding and practicing healthy sexual behavior. Empowering Hoosiers to adopt healthy lifestyles is a critical step toward cancer prevention.
What are we doing?Changing Health Behavior in Schools: The ICC Primary Prevention Action Team works to assist Indiana schools in implementing nutrition and physical activity interventions that will enable students to make healthy choices likely to carry over into adulthood, and ultimately aid in reducing the burden of cancer in Indiana. As a result, the action team provided a mini-grant opportunity to schools across the state to implement an evidence-based strategy to increase physical activity or healthy eating. The outcomes of this mini-grant opportunity address Primary Prevention Weight Management Objective 2. The committee awarded funding to the following schools: Crawfordsville Community Schools – School Garden; Frederick Douglass, Indianapolis Public Schools, School #19 – Indoor and Outdoor School Garden; and Wes-Del Community Schools – Limestone walking and jogging nature trail.
Thinking Local: The ICC established its first local cancer control coalition in 2011. The Public Health District Six Cancer Control Coalition includes 13 counties in East Central Indiana, seven of which have a higher smoking rate than the national average.3 Thus, the coalition works at the local level to implement evidence-based tobacco control policy, systems, and environmental change. Throughout 2012, the coalition contributed to an increase in the number of providers, employers, and organizations in the Quit Now Indiana Preferred Provider Network. Local cancer coalition members worked with health care providers and health care systems to implement the 2008 Clinical Practice Guideline for Treating Tobacco Use and Dependence. Decision-making bodies within communities have been educated on local comprehensive tobacco-free campus policies for hospitals, health care centers, mental health centers, clinics, and addiction treatment centers. Key successes for the District Six Coalition include increasing the monthly average Indiana Tobacco Quitline calls by 84 percent in three months.
4
primary preventionApproximately 300,000 deaths per year may be attributable to obesity.4 That is approximately 821 people per day – which is a Titanic full of people every 2.7 days.
In 2011, 65.6 percent of Indiana adults were considered either overweight or obese.3 This amounts to over 3 million Hoosier adults, which is equal to the population of the state of Iowa.
2012 PRIORITY OBJECTIVES
Weight Management, Objective 2: By 2014, decrease the percentage of high school students in Indiana who are obese from 14 percent to 13 percent as measured by the Youth Risk Behavior Surveillance – United States.
Tobacco Cessation, Objective 2: By 2014, increase the percentage of current smokers who attempt to quit from 50 percent to 65 percentas measured by the Adult Tobacco Survey.
Find a complete list of objectives at IndianaCancer.org.

Early detection is a strong predictor of cancer survival; in general, the earlier the cancer is detected, the better the prognosis. Often, regular screenings save lives by identifying cancers when they are most curable and treatment has the highest success rate. Cancers that can be detected through early screening include breast, colon, rectum, cervix, prostate, testis, oral cavity, and skin. Screening isn’t always without risk; it is important for Hoosiers to be informed decision-makers and talk to their primary health care providers about screening options.
What are we doing?Impacting the Nine-to-Five: In February of 2013, the ICC began inviting Hoosier employers to help reduce the state’s cancer burden by taking part in the ICC Employer Gold Standard Initiative. According to the 2006 Employer Health Benefits Survey, employers control health insurance for preventive care for 59 percent of working adults and their dependents.5 As such, the workplace has been identified as a key way to reach average-risk, age-
appropriate adults for screenings that lead to prevention and early detection for breast, cervical, and colorectal cancer. This innovative certification program addresses Early Detection Objectives 1, 2, and 4.
Addressing Health Disparities: To contribute to ICCP Early Detection Objectives 1, 4, and 5, the ICC Breast and Cervical Cancer Action Team is disseminating information related to breast and cervical cancer through lay health advisors. The action team has developed and implemented a Clinton County screening initiative, which uses promotoras (lay Hispanic community members who receive specialized training to provide basic health education in the community) to educate Hispanic women on the importance of yearly screenings and access to care. The group is interested in replicating the successful program in other counties of need.
Educating the Provider: In an attempt to expand the use of provider reminder systems for annual mammograms and clinical breast exams, the ICC Breast and Cervical
Cancer Action Team created an informational toolkit for all Indiana providers. The toolkit includes: an introduction to the ICC, its Breast and Cervical Cancer Action Team, and partner member agencies; a resource list on free or reduced cost mammogram and cervical cancer screening locations across the state; and a flowchart that offers providers potential paths to find free or low-cost screenings for patients in-need, utilizing ICC members such as the ISDH Breast and Cervical Cancer Program or Susan G. Komen for the Cure.
5
early detection
Improved access to health insurance will help increase early detection screening rates for cancer. In 2010, 13 percent of Indiana’s residents, approximately 855,000 people, lacked health insurance coverage.6
2012 PRIORITY OBJECTIVESObjective 1: By 2014, increase the percentage of women aged 40 and older who receive breast cancer screening within the last two years from 74 percent as mea-sured by the Indiana Behavioral Risk Factor Surveillance System.
Objective 2: By 2014, increase the percentage of adults aged 50 and older who receive risk based colorectal cancer screening (sigmoidoscopy or colonoscopy) and follow-up using accepted profes-sional guidelines from 59 percent to 67 percent as measured by the Indiana Behavioral Risk Factor Surveillance System.
Objective 4: By 2014, increase the percentage of women aged 21 and older who have had a Pap smear in the last three years from 77 percent as measured by the Indiana Behavioral Risk Factor Surveil-lance System.
Objective 5: (Developmental) By 2014, reduce barriers to screenings and diagnostic services for disparate populations.
Find a complete list of objectives at IndianaCancer.org.

Successful treatment involves a partnership between health care providers, patients, and family members or caregivers. Understanding treatment options is key to helping patients experience greater satisfaction with their care and treatment. When patients understand the nature and risks of their cancer diagnosis, and potential risks and benefits of treatment, they can make informed decisions that are consistent with their personal preferences and values.
What are we doing? Surveying the Navigators: The Indiana Patient Navigator Assessment was distributed by the ICC’s Patient Navigation Committee between November and December of 2012. Over 50 navigators from across the state completed the survey. It is the mission of this committee to connect, educate, and share best practices among patient navigators in Indiana, so that together, we can successfully reduce barriers and increase access to services specifically related to cancer. In 2013, the ICC Patient Navigation Committee aims to use the results of the 2012 assessment to begin building a substantial network of patient navigators and patient navigator programs to foster collaboration and education across the state.
Discussing the Hot Topics: The 2012 ICC Annual Meeting took place on April 27 at Joseph E. Walther Hall on the IUPUI campus. The meeting entitled “Hot Topics in Cancer Prevention and Control” was the highest attended ICC Annual Meeting to date. During the event, the ICC unveiled the Indiana Cancer Facts and Figures 2012 report along with our second infograph titled “The Impact of Cancer in Indiana.”
Additionally, the ICC distinguished a number of members:• ICC Outstanding Contributions to Cancer Control (Individual) – Robert Goulet, M.D.• ICC Outstanding Contributions to Cancer Control (Organization) – Little Red Door Cancer Agency• David Caldwell Survivorship Award – Gene Bednarek• Cancer Control Champions – Wendy Noe, Tanya Parrish, and Revienne Shedd-Steele
The event focused on Treatment Objective 2. Through presentations regarding breast and prostate cancer screening guideline revisions and HPV vaccination recommendations, experts from around the state educated ICC members about cancer early detection and treatment options, outcomes, and quality of life.
6
treatment
Mortality from all types of cancers decreased significantly from 2000 to 2009, going from a rate of 213 per 100,000 to 185.3 per 100,000 people.2
2012 PRIORITY OBJECTIVESObjective 1: (Developmental) By 2014, minimize barriers and increase access for cancer patients to receive evidence-based treatment services and appropriate follow-up in the state of Indiana.
Objective 2: (Developmental) By 2014, foster the statewide adoption of multidisciplinary, evidence-based care by physicians involved in the treat-ment of patients with cancer.
Find a complete list of objectives at IndianaCancer.org.

Quality of life issues cut across every aspect of the cancer continuum, from prevention through palliation. It is not something that can be measured by a standardized set of criteria; it is subjective and determined by the patient. The impact of quality of life issues range from moderate to severe, and can occur in the short or long term.
What are we doing? Treating the Treatment: During Prostate Cancer Awareness Month (September 2012), the ICC Prostate Cancer Committee hosted a seminar titled “Life with Prostate Cancer,” which addressed Quality of Life Objective 1 by disseminating information about effective methods of alleviating prostate cancer post-treatment symptomatology burdens. The seminar took place at Cancer Services of Northeastern Indiana in Fort Wayne, an ICC partner organization, and featured presentations from Donald Urban, M.D., from Parkview Physicians Group and Theodore Wagner, M.D., from Northeast Indiana Urology. Bill Seidel, prostate cancer survivor and Us Too member, gave audience members an intriguing survivor perspective. In all, Cancer Services of Northeastern Indiana and the ICC welcomed over 50 attendees including survivors and their loved
ones. Thank you to the many ICC partners that made this event a huge success.
Educating on Health Care Reform: To better educate patient navigators and other professionals in the cancer field about the health care and insurance burdens for cancer patients, the ICC Quality of Life Committee hosted “Cancer and the Law” on October 10, 2012 in Evansville. The event was led by Monica Bryant, Esq., a cancer rights attorney, speaker, author, and current chief operating officer for Navigating Cancer Survivorship. This free
educational seminar focused on helping patients navigate legal and financial concerns when coping with cancer, as well as specifically touching on health care reform topics for the health care worker.
7
quality of life
2012 PRIORITY OBJECTIVESObjective 1: (Developmental) By 2014, increase access to resources for cancer survivors.
Objective 2: (Developmental) By 2014, increase cancer survivors’ utilization of end of life care.
Find a complete list of objectives at IndianaCancer.org.
8
dataComprehensive and timely cancer data is critical to understanding cancer prevention and control. Incidence, mortality, and survival rates, as well as staging data, help identify cancer disparities and priorities – in short, without data, the ICC and the ICCP would lack focus and direction. In addition, Hoosiers need accurate, timely, and user-friendly data to make informed decisions regarding their health.
What are we doing? Distributing the Data: ICC leadership sees data dissemination and utilization as one of the most important duties of the ICC. Likewise, the ICC membership, as evaluated in the 2012 Membership Satisfaction Survey, regarded data and information related to cancer as one of the main resource strengths of the ICC, a success which could be attributed to the release of the Indiana Cancer Facts and Figures 2012 report. ICC staff and partners have distributed 250 print copies of the report and there have been 459 unique downloads from the ICC website.
Providing a Toolbox for the Health Professional: Toolkits addressing the cancer burden in Indiana are available on the ICC website at IndianaCancer.org. Current toolkits include a generalized cancer toolkit, as well as lung, breast, cervical, colorectal, and prostate cancers. Each toolkit contains information and statistics on cancer in Indiana, including who is at greatest risk, common signs and symptoms, early detection, prevention, and resources. The toolkits are designed to equip cancer control advocates and public health professionals with cancer datasheets, sample press releases, social media messages, and a list of external resources.
Visualizing the Data: The ICC uses infographics to convey complex cancer information and data in a quick and clear manner. Infographics, which are conceptualized by the ICC Data Committee and created by a talented graphic designer, have produced nearly 1,000 visits to the ICC website. Moreover, community advocates can use this tool to innovatively share data from the Indiana State Cancer Registry (ISCR) and the Behavioral Risk Factor Surveillance System. Current infographic subjects include Indiana’s cancer burden, smoke-free air, and complete streets.
Making the Cancer Registry Accessible: From September to November 2012, the ICC Data Committee proposed a number of enhancements to ISDH for the ISCR Statistics Report Generator. This generator serves as an important tool for local health professionals, allowing them to access up-to-date state cancer registry data and information.
Informing our Members: Data Objective 1 and 2 address ICC members awareness and use of cancer-related data and are monitored annually by the ICC Membership Satisfaction Survey. In the 2012 survey, 87 percent of respondents felt that the ICC had increased their awareness of relevant cancer data, which was up from the 74 percent recorded in 2010.
2012 PRIORITY OBJECTIVESObjective 1: By 2014, increase awareness of relevant data among ICC members.
Objective 2: By 2014, increase use of relevant data among ICC members.
Objective 4: By 2014, increase utilization of state cancer registry data among ICC members.
Objective 5: By 2014, increase utilization of Indiana Behavioral Risk Factor Surveillance System data among ICC members.
Objective 6: By 2014, increase the Indiana Behavioral Risk Factor Surveillance System sample size from 4,900 (2008) to a minimum of 6,000 per year.
Find a complete list of objectives at IndianaCancer.org.

9
advocacyAdvocacy efforts influence the way the public and policymakers at all levels think and act regarding a given issue. Anyone can be an advocate. It is important to inform and educate the public and policymakers in order to influence the laws, regulations, and rules that impact the experience of cancer from prevention through palliation.
What are we doing? Evidence-Based Change: Policy, system, and environmental changes make healthier choices a real, feasible option for every community member by looking at the laws, rules, and environments that impact our behavior. By changing laws and shaping physical landscapes, a big health impact can be made with less time and fewer resources. The ICC collaborates with many statewide partners to educate policymakers, workplaces, schools, hospitals, and communities on how to make the healthy choice the easy choice.
Collaborating on the Policy Agenda: In January 2011, the ICC Advocacy Committee adopted a policy agenda to prevent and control cancer in Indiana. The four policy priorities include: passing a
statewide comprehensive smoke-free air law; increasing the cigarette tax from 99.5 cents to $2 per pack; increasing the number of Complete Streets policies at the Metropolitan Planning Organization, county, or city levels from three to seven; and requiring school corporations to provide at least 30 minutes per day of the recommended 60 minutes per day of physical activity in elementary schools. In 2012, Indiana successfully implemented its seventh local Complete Streets policy, including a nationally recognized model policy in Indianapolis. This success highlights an exemplary application of collaboration in public health through the sharing of knowledge, resources, and data to pass policy.
Increasing our Reach: In 2012, the ICC increased newsletter distribution to include over 500 people. This effectively improved the ICC’s reach by 50 percent from 2010 to 2012 and completed ICCP Advocacy Objective 1. ICC members are encouraged to distribute information within their organizations and to help identify additional partners around the state with shared goals and objectives.
Member Satisfaction: ICC strives to boost members’ involvement in advocacy efforts targeted at reducing the cancer burden in Indiana. Through the ICC Membership Satisfaction Survey, Advocacy Objectives 2, 5, and 6 are measured and assessed. Of the 2012 survey respondents, 55 percent felt the ICC increased participation in legislative
advocacy (up from 34 percent in 2010); 76 percent felt the ICC increased member knowledge of cancer related disparities (up from 63 percent in 2010); and 65 percent felt the ICC strengthened public awareness of emerging cancer-related policy initiatives (up from 34 percent in 2010). Over the next two years, it is a priority of the ICC leadership to continue to increase the share of members who feel informed and empowered to advocate for laws, regulations, and policies that will reduce the cancer burden in Indiana.
Almost 40 percent of Hoosiers are covered by a Complete Street policy.7
2012 PRIORITY OBJECTIVESObjective 1: By 2014, increase the ICC communica-tions distribution by 50 percent from 336 to 504 as measured by the Indiana Comprehensive Cancer Control Pro-gram’s listserv database.
Objective 2: By 2014, increase ICC member participation in legislative advocacy, as measured by the ICC Membership Satisfaction Survey.
Objective 5: By 2014, increase ICC members’ knowledge of cancer-related disparities, as measured by the ICC Membership Satisfaction Survey.
Objective 6: By 2014, increase ICC communication with the general public to strengthen public awareness of emerging cancer-related policy initiatives, as measured by the ICC Satisfaction Survey.
Find a complete list of objectives at IndianaCancer.org.

10
survey results
Partner Organization SurveyThe purpose of the Partner Organization Survey is to assess the extent to which ICC partner organizations are addressing the goals, objectives, and strategies outlined in the ICCP. The survey is offered annually and was conducted most recently in May 2012. A total of 27 individuals completed the survey. Overall, the vast majority of respondents indicated that their agencies are working on the Primary Prevention goal (93%). The Early Detection goal and the Quality of Life goal are each being addressed by 70% of respondents. About two-thirds of respondents said their agencies are addressing the Treatment goal (67%) and the Advocacy goal (63%). Finally, just over one-half of respondents said that their agencies are addressing the Data goal (52%).
Below displays the number and percentage of respondents who indicated that their organizations are addressing a given goal area.
The ICC strives to gather and use member feedback to guide and strengthen our coalition. During 2012, we conducted two surveys of members and partners: the Partner Organization Survey (May 2012) and the ICC Membership Satisfaction Survey (December 2012).
Decrease cancer risk through lifestyle
behavioral interventions
frequency:
2593%
frequency:
1970%
frequency:
1867%
frequency:
1970%
frequency:
1452%
frequency:
1763%
Increase early detection and appropriate
screening for cancer
Promote informed decision making and
utilization of appropriate cancer treatment
Improve quality of life for cancer
patients, survivors, and their families
Increase the quantity, quality, &
availability of complete and timely cancer and
related data
Advocate for cancer-related policy
initiatives
In addition to the level of engagement in each goal area being high, the average levels of engagement among objectives within each goal area were also high. The goal area with the highest average level of engagement in all objectives was Early Detection, followed by Quality of Life. The goal areas with the lowest average engagement in all objectives (among survey participants) were Data, Advocacy, and the Primary Prevention subareas of Physical Activity, Immunizations, Breastfeeding, and Healthy Sexual Behavior. The results of the ICC’s survey on the extent to which partner organizations and other organizations have implemented interventions related to the ICCP indicate that partner organizations are actively engaged in implementing strategies in multiple goal areas. In fact, each goal area had engagement from at least one-half of the organizations that participated in the Partner Organization Survey. In addition to demonstrating engagement in multiple goal areas, partner organizations also reported engaging in multiple strategies within goal areas.

11
Membership Satisfaction SurveyIn December 2012, 62 members, partners, and collaborators completed the ICC Membership Satisfaction Survey. Of those who responded to the survey, most (89%) are members of the ICC. The purpose of this annual survey is to assess stakeholders’ degree of satisfaction with the structure, leadership, resources, communication, and impact of the ICC. Several questions have been asked repeatedly since 2004, while most have been added more recently. STRUCTURE AND LEADERSHIPRespondents were generally positive about the structure and leadership of the ICC. A majority of respondents agree with statements about ICC providing a “common ground”; that the ICC is making progress toward the goals and objectives outlined in the ICCP; that there is value in coordinating efforts with other members; that ICC leadership is knowledgeable; or that paid staff are efficient. Only a few of the survey items related to ICC Structure and Leadership were markedly different than previous years. The share of respondents who indicated that ICC is contributing to an enhanced quality of life for people impacted by cancer in Indiana increased, as did the share of those who believe that members assume responsibility for getting work done. In 2012, there were increases in the proportion of respondents who declined to indicate levels of agreement on several of the more specific items related to the staffing and operations of the ICC. RESOURCESRespondents were asked to indicate the degree to which they believe that the ICC has what it needs to be effective. The share of respondents who reported that the ICC has a high level of ability to bring people together increased in 2012. Likewise, the share of respondents who indicated that the ICC has sufficient
data and information related to cancer and those reporting sufficient legitimacy and credibility of ICC to work effectively also increased in 2012. The proportion of those who believe that the ICC has adequate connections to political decision-makers and government agencies has decreased. COMMUNICATIONE-mail blasts continue to be the preferred mode of communication for all topics and areas of information. Interest in use of the ICC Website as a tool to communicate with members appears to have declined since 2009. Interest in the use of Twitter and Facebook remains relatively low. ICC IMPACTFor all six objectives outlined in the ICCP included in the survey, the share of respondents who reported that they believe ICC has contributed in a positive way increased from 2010 to 2012. The share of members who reported that the ICC is increasing members’ awareness and knowledge of cancer-related data and participation in legislative advocacy was much higher in 2012 than in 2010. A higher share of respondents in 2012 also said that the ICC is increasing communication with the general public to strengthen public awareness of emerging cancer-related policy initiatives.

12
What we know, What we Don’t Know, What we Believe - The ICC invites members and other statewide partners to the 2013 Annual Meeting, where we will explore the reasoning behind today’s continuum of cancer care – the good, the bad, and the ugly. As Treatment Objective 2 states, it is the responsibility of the ICC to foster the statewide adoption of multidisciplinary, evidence-based care by physicians involved in treatment of patients with cancer. The message delivered to Indiana’s health care workforce in attendance will be clear: the future of effective cancer care is scientifically justifiable prevention, screening, treatment, and rehabilitation interventions.
Making an Informed Decision: The ICC will host a prostate cancer awareness summit that coincides with men’s health awareness week (June 10 to 16). The ICC Prostate Cancer Awareness Summit will cover many topics including an overview of prostate cancer, the risks and benefits of prostate cancer screening, the importance of informed decision making, and treatment options for men diagnosed with prostate cancer. The conference will primarily focus on informing health professionals, such as navigators, nurses, and health educators, on the current state of prostate cancer screenings, research, and treatment; however, the event will also appeal to men (and spouses) aged 40 to 65.
Addressing the Local Burden: The Cancer Control Section at ISDH, in partnership with the ICC, will fund an organization to address the disproportionate colorectal and lung cancer burden in Indiana’s Public Health District Nine. The grantee will host an informative session on local cancer control and coalition building as a first step to addressing this cancer disparity at the district level.
New Partnerships: Help us reduce Indiana’s cancer burden! Getting involved with the ICC is easy and free. Visit IndianaCancer.org/membership to become an ICC member and take part in one or more of the many committees.
get excited for 2013!
The ICC leadership sincerely thanks all of our volunteers for their contributions to the
many successes over the past year. Our membership donated more than 600 hours
of volunteer service from May 2012 to February 2013, and we could not be any
prouder of our collective accomplishments.

REFERENCES: 1 American Cancer Society. Cancer Facts and Figures 2012. Atlanta: American Cancer Society; 2012.2 U.S. Cancer Statistics Working Group. United States Cancer Statistics; 1999-2009 Incidence and Mortality Web-based Report. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; 2013. Accessed at wonder.cdc.gov on March 15, 2013. 3 Indiana Behavioral Risk Factors Surveillance System. Accessed at http://www.in.gov/isdh/25194.htm on April 1, 2013.4 U.S. Department of Health and Human Services. The Surgeon General’s call to action to prevent and decrease overweight and obesity. [Rockville, MD]: U.S. Department of Health and Human Services, Public Health Service, Office of the Surgeon General; [2001]. Available from: US GPO, Washington.5 2006 Employer Health Benefits Survey. Kaiser Foundation. [Online] Sept. 2006. Accessed at http://www.kff.org/insurance/7527/ on March 11, 2013. 6 Justis, Rachel. Health Insurance Coverage. InContext. [Online] Jan-Feb 2012. Accessed at http://www.incontext.indiana.edu/2012/jan-feb/article3.asp on March 13, 2013. 7 Department of Nutrition and Physical Activity. Indiana State Department of Health.
This publication was supported by cooperative agreement award U58DP003884 from the Centers for Disease Control and Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention.
Images: Jupiterimages; sxc.hu; Getty Images; Flickr.com

FACEBOOK.COM/ INDIANACANCER INDIANACANCER.ORG TWITTER.COM/
IN_CANCER