increased renal and forearm vasoconstrictionin - heart
TRANSCRIPT

Br Heart Y 1993;70:247-25 1
Increased renal and forearm vasoconstriction inresponse to exercise after heart transplantation
Guy A Haywood, Peter J Counihan, James F Sneddon, Stephen H Jennison,Yaver Bashir, William J McKenna
AbstractObjective-To test the hypothesis thatthe loss of the inhibitory effect of thecardiac ventricular afferent fibres on thevasomotor centre would result inincreased vasoconstrictor drive to theforearm and renal vascular beds duringsupine exercise in heart transplantrecipients.Design-Comparison of regional haemo-dynamic response to exercise in hearttransplant recipients and two agematched control groups.Setting--Regional heart transplant unit.Patients and methods-Orthotopic hearttransplant recipients (n = 10), patientswith NYHA class II heart failure (n = 10),and normal controls (n = 10) underwentshort duration maximal supine bicycleexercise.Main outcome measureSimultaneousmeasurements were made of heart rate,systemic blood pressure, oxygen con-sumption (Vo2), -forearm blood flow, andrenal blood flow. Forearm blood flow wasmeasured by forearm plethysmographyand renal blood flow by continuous renalvein thermodilution.Results-The peak forearm vascularresistance was significantly greater in thetransplant group than in the controls(mean (SEM) 75 (18) v 40 (7) resistanceunits, p < 0.05). The percentage fall inrenal blood flow at peak exercise was sig-nificantly greater in heart transplantrecipients than in the controls (44% (4%)v 32% (4%), p < 0-05) as was the percent-age increase in renal vascular resistance(transplants: 116% (19%) v controls: 78%(17%), p < 0.05). Regional haemodynam-ics during exercise in the heart failuregroup were not significantly differentfrom those in the controls.Conclusions-These findings suggest thatsurgical division of the cardiac ventricu-lar afferent fibres results in increasedvasoconstrictor drive to the kidneys andnon-exercising muscle during exercise.This mechanism may contribute to per-sistent exercise limitation and renalimpairment after heart transplantation.
(Br HeartJr 1993;70:247-251)
During exercise in humans, blood flow isdiverted away from the kidneys and non-exer-cising muscle and towards exercising muscle
groups. This mechanism is controlled bythe complex interaction of local metabolicand neurohumoral factors, and the sympa-thetic efferent output arising from the vaso-motor centre directed to the individualvascular beds.3 In animals, non-myelinatedvagal afferent C fibres arising from ventricularmechanoreceptors in the heart have beenshown to exert an inhibitory influence on thevasomotor centre, modulating the level ofcentral efferent sympathetic outflow.4Animal studies suggest that the region of
the circulation most influenced by cardiacvagal afferent input to the vasomotor centre isthe renal vascular bed,56 but whether this isso in humans is not known.
There is also no information, except duringprolonged lower body negative pressure,7 onwhether changes in vascular resistance inmuscle reflect changes in the vascular tone ofinternal organs, such as the kidneys. Moststudies of cardiovascular reflexes in humanshave concentrated on muscle with either fore-arm plethysmography,8 or more recently,microneurographic recordings of peronealsympathetic nerve traffic9; whether resultsfrom these studies can be extrapolated toother regional circulations is unknown. Thisstudy tested the hypothesis that removal ofcardiac ventricular afferent nerves resultingfrom cardiac transplantation would removethe inhibitory influence of vagal afferent Cfibres on the vasomotor centre. This couldresult in enhanced vasoconstrictor responsesin the forearm and renal vascular beds duringdynamic leg exercise and the vasoconstrictionin the renal vascular bed would be similar tothat found in the forearm.
Patients and methodsSUBJECTSThe subjects who participated in the studywere: 10 symptom free patients, all men,2 5-9 months after orthotopic heart trans-plantation, 10 patients with grade II NewYork Heart Association heart failure (sevencardiomyopathies, two ischaemic heart dis-ease, and one valvar heart disease-aorticregurgitation), five men and five women, and10 controls composed of patients with normalelectrocardiograms and structurally normalhearts who were undergoing electrophysio-logical evaluation for detection of concealedaccessory pathways or who had been referredwith intermittent non-exertional chest painand had been shown to have normal exercisetests, normal coronary arteriography, andnormal coronary flow reserve (eight men and
St George's Hospital,LondonG A HaywoodP J Counihan;J F SneddonS H JennisonY BashirW J McKennaCorrespondence to:Dr Guy Haywood, WessexCardiothoracic Centre,Southampton GeneralHospital, Tremona Road,Southampton S09 4XY.Accepted for publication7 April 1993
247
on 2 January 2019 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.70.3.247 on 1 S
eptember 1993. D
ownloaded from

Haywood, Counihan, Sneddon, _Jennison, Bashir, McKenna
two women). All subjects gave fully informedwritten consent in a format approved by thehospital ethics committee. Patients with a
history of systemic hypertension, intrinsicrenal disease, or a serum creatinine greaterthan 160 ,umol/l were excluded. In the hearttransplant patients the study was performedimmediately before routine endomyocardialbiopsy. All biopsies were free of histologicalevidence of acute rejection.
Medications at the time of the studyHeart transplant patients were all maintainedon cyclosporin and azathioprine and two were
also receiving 10 mg of prednisolone daily.The heart failure group were all receivingsmall doses of a loop diuretic, also, three werereceiving an angiotensin converting enzyme
inhibitor. Control subjects were on no drugtreatment. Subjects received no medicationfor 24 hours before the study.
METHODSMeasurements were made after 20 minutes ofsupine rest and repeated in the last minute ofexercise. Heart rate was measured from an
instantaneous electrocardiographic monitor.Oxygen consumption (Vo2) and respiratoryquotient (RQ) were measured after 20 min-utes rest in the supine position and continu-ously throughout exercise by respiratory gasanalysis with a metabolic measurement cart(Sensor Medics Horizon MMC).'° Forearmblood flow was measured by forearm venous
occlusion plethysmography with a mercury insilastic temperature compensated straingauge."' 12 Left renal blood flow was measuredby continuous renal vein thermodilution.'3Heart rate (beats/min), Vo2 (ml/kg/min), RQ,forearm blood flow (ml 100 ml-'.min-'), andleft renal blood flow (ml/min) were measuredsimultaneously after 20 minutes of rest in thesupine position with the subjects' feetstrapped to the pedals of a supine exercisebicycle. A short duration maximal exerciseprotocol was used.'4 Work load was adjustedto result in a progressive rise in heart rateover the first seven minutes of exercise, afterwhich the workload was set to the maximumthat subjects could tolerate and they wereinstructed to pedal "flat out" to exhaustion.Resistance units for the forearm and kidneywere calculated by dividing the mean arterialblood pressure by the forearm blood flow inml/100nmlImin or the left renal blood flow inml/min. Renal oxygen delivery and consump-tion were calculated from the renal bloodflow, haemoglobin, and the arterial and renalvenous oxygen saturatibns from standardformulae.
STATISTICAL ANALYSISResults are presented as mean (SEM). Thedifferences between the controls and theheart failure and transplant groups were
analysed with the Mann-Whitney U test. TheSpearman correlation coefficient was calcu-lated for the percentage changes in forearmand renal vascular resistance in individualsubjects.
ResultsThere were no significant differences in theages of the three groups (controls 45 (5)years, transplant recipients 48 (2) years, heartfailure patients 42 (4) years). The restingheart rate was 89 (3) beats/min in the trans-plant group, significantly greater than that incontrols (74 (3), p < 0-01), but similar to thatin the heart failure group (83 (4) NS). Allpatients achieved their maximal exercisewithin 10 to 12 minutes from the start ofexercise. At maximal exercise controlsachieved a greater peak heart rate (149 (6)beats/min) than either the heart failurepatients (118 (4) p < 0-01) or the transplantpatients (1 16 (3) p < 0-01). There were no
significant differences in either resting or peakmean arterial blood pressures between thecontrols and the other two groups (resting:controls 99 (5), heart failure 106 (8), trans-plants 111 (5) mm Hg, peak: controls 123(6), heart failure 103 (5), transplants 126 (7).Table 1 shows exercise data for the threegroups. The Vo, max was 24 (2.4) ml/kg/minin controls, greater than in the heart failurepatients (16 (2 0) p < 0-01) and heart trans-plant recipients (16 (1I0), p < 0 01). The res-
piratory quotient achieved was 1-1 (0-02) inthe controls and 1.1 (0 02) in the transplantrecipients, indicating that they had exercisedto beyond the anaerobic threshold. Some ofthe patients with heart failure were symptomlimited before reaching a respiratory quotientgreater than 1-0 (0-9 (0-05)). The Vo, datawas unavailable from one patient in the trans-plant group because his beard prevented an
airtight seal between the mask and his face,and from two patients in the heart failuregroup who were unable to tolerate the facemask. Table 2 shows the changes in forearmblood flow in response to exercise and table 3shows the renal blood flow.
FOREARM BLOOD FLOWThe percentage fall in forearm blood flow atpeak exercise in heart transplant recipients(39% (10%)) was not significantly greaterthan in controls (32% (6%)) or in heart fail-ure patients (22% (7%)). The peak forearm
Table I Mean (SEM) systemic variables during exercise in controls, heart transplant recipients (TXpts), and patientswith heartfailure (CCF Pts)
Resting Peak heart Resting Peak Peakheart rate rate MABP MABP Vo2
Age (yr) (beatsmin) (beatsmin) (mm Hg) (mm Hg) (milkg/min) RQ
Controls (n = 10) 45 (5) 74 (3) 149 (6) 99 (5) 123 (6) 24 (2 4) 1-1 (0 02)TXPts(n= 10) 48(2) 89(3)* 116(3)* 111(5) 126(7) 16(1-0)* 1-1(0-02)CCF Pts (n = 10) 42 (4) 83 (4) 118 (4)* 106 (8) 103 (5) 16 (2 0)* 0-9 (0 05)
*p < 0-01 v controls. MABP, mean arterial blood pressure.
248
on 2 January 2019 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.70.3.247 on 1 S
eptember 1993. D
ownloaded from
Increased renal andforearm vasoconstriction in response to exercise after heart transplantation
Table 2 Changes in mean (SEM) forearm bloodflow (FBF) andforearm vascularresistance (FVR)
Resting Peak Fall Resting Peak IncreaseFBF FBF FBF FVR FVR FVR(mlllOOml/min) (ml/1OO ml/min) (%) (Res units) (Res units) (%)
Controls 5-3 (0-5) 3-5 (0-5) 32 (6) 21 (2) 40 (7) 97 (36)Tx Pts 4-3 (0-6) 2-2 (0-4) 39 (10) 32 (6) 75 (18)** 183 (54)CCF Pts 3-4 (0-4)** 2-6 (0-4) 22 (7) 40 (5) 48 (7) 34 (13)*
*p < 0-05 v controls (one tailed Mann Whitney U test); **p < 0-05 v controls (two tailed MannWhitney U test); Res units, resistance units; other abbreviations as for table 1.
Table 3 Changes in mean (SEM) renal bloodflow (RBF) and renal vascular resistance(RVR)
Resting Peak Resting Peakleft RBF left RBF Fall RBF RVR RVR Increase(ml/min) (mllmin) ($'q) (Res units) (Res units) RVR (%,)
ControlsTx PtsCCF Pts
456 (44) 316 (39) 32 (4) 0-24 (0 02) 0 43 (0-06) 78 (17)428 (78) 245 (56) 45 (5)** 0 35 (0 07) 0-72 (0-13)* 116 (19)*483 (64) 320 (58) 38 (5) 0-26 (0 03) 0 49 (0 13) 65 (24)
*p < 0-05 v controls (one tailed Mgn Whitney U test); **p < 0-05 v controls (two tailed MannWhitney U test); abbreviations as for tables 1 and 2.
vascular resistance was, however, significantlygreater in the transplant group than in con-trols (75 (18) v 40 (7) resistance units, p <0-05). The peak forearm vascular resistancein the heart failure group (48 (7) resistanceunits) showed no significant difference fromthe controls. Compared with controls,patients with heart failure had a lower per-centage increase in forearm vascular resis-tance (34 (13) v 97 (36) resistance units).
RENAL BLOOD FLOWThe percentage fall in renal blood flow atpeak exercise was significantly greater in hearttransplant recipients than in controls (44%(4%) v 32% (4%), p < 0-05) and the percent-age increase in renal vascular resistance wassignificantly greater (transplants: 1 16% (19%)v controls 78% (17%), p < 0 05). The heartfailure group was not significantlydifferent from controls in either percentagefall in renal blood flow (38% (5%)) or per-centage increase in renal vascular resistance(65% (24%)).
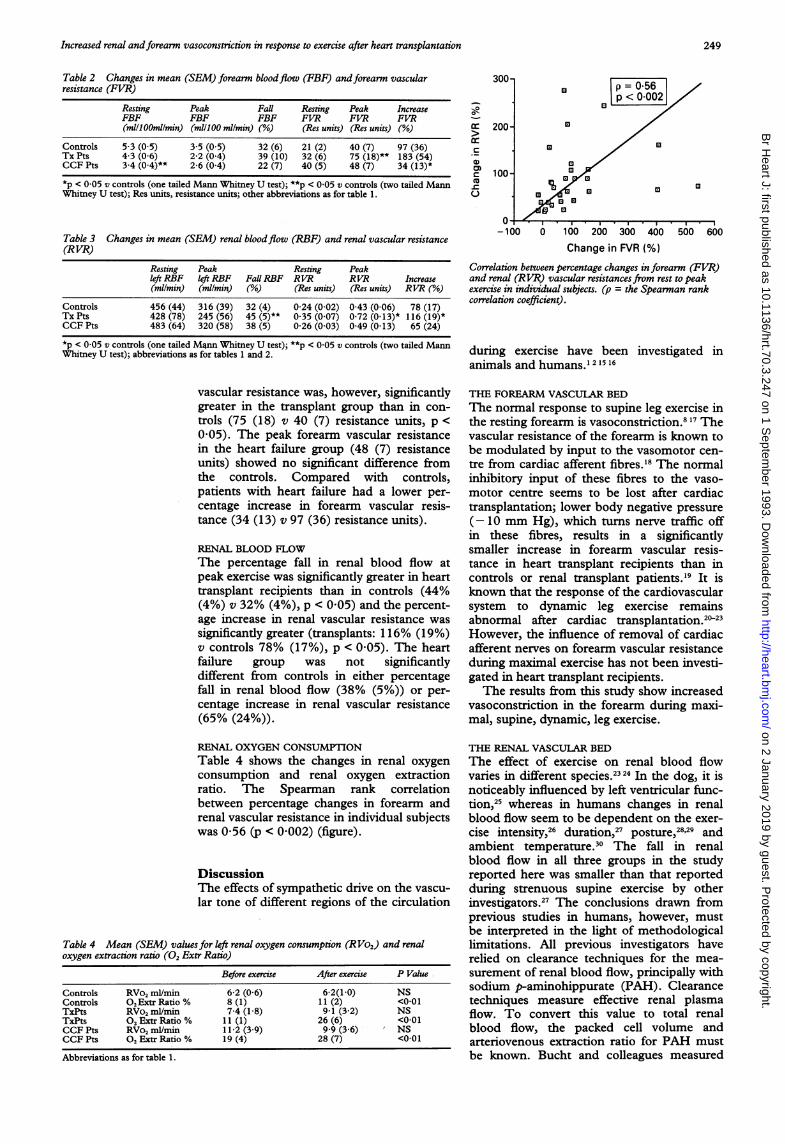
RENAL OXYGEN CONSUMPTIONTable 4 shows the changes in renal oxygenconsumption and renal oxygen extractionratio. The Spearman rank correlationbetween percentage changes in forearm andrenal vascular resistance in individual subjectswas 0-56 (p < 0 002) (figure).
DiscussionThe effects of sympathetic drive on the vascu-lar tone of different regions of the circulation
Table 4 Mean (SEM) values for left renal oxygen consumption (RVo,) and renaloxygen extraction ratio (0, Extr Ratio)
Before exercise After exercise P Value
Controls RVo, ml/min 6-2 (0-6) 6-2(1-0) NSControls O,Extr Ratio % 8 (1) 11(2) <0-01TxPts RVo, ml/min 7-4 (1-8) 9-1 (3 2) NSTxPts O, ExtrRatio % 11 (1) 26 (6) <0-01CCFPts RVo, ml/min 11-2 (3-9) 9-9 (3 6) NSCCF Pts 02 Extr Ratio % 19 (4) 28 (7) <0-01Abbreviations as for table 1.
300-
0*
G 200- E
c ~~00G) 0
m 00- X 0
u0
-100 0 100 200 300 400 500 600Change in FVR (%)
Correlation between percentage changes in forearm (FVR)and renal (RVR) vascular resistances from rest to peakexercise in individual subjects. (p = the Spearman rankcorrelation coefficient).
during exercise have been investigated inanimals and humans.' 21516
THE FOREARM VASCULAR BEDThe normal response to supine leg exercise inthe resting forearm is vasoconstriction.817 Thevascular resistance of the forearm is known tobe modulated by input to the vasomotor cen-tre from cardiac afferent fibres.'8 The normalinhibitory input of these fibres to the vaso-motor centre seems to be lost after cardiactransplantation; lower body negative pressure(-10 mm Hg), which turns nerve traffic offin these fibres, results in a significantlysmaller increase in forearm vascular resis-tance in heart transplant recipients than incontrols or renal transplant patients.'9 It isknown that the response of the cardiovascularsystem to dynamic leg exercise remainsabnormal after cardiac transplantation.2>2'However, the influence of removal of cardiacafferent nerves on forearm vascular resistanceduring maximal exercise has not been investi-gated in heart transplant recipients.The results from this study show increased
vasoconstriction in the forearm during maxi-mal, supine, dynamic, leg exercise.
THE RENAL VASCULAR BEDThe effect of exercise on renal blood flowvaries in different species.2324 In the dog, it isnoticeably influenced by left ventricular func-tion,25 whereas in humans changes in renalblood flow seem to be dependent on the exer-cise intensity,26 duration,27 posture,28'29 andambient temperature.30 The fall in renalblood flow in all three groups in the studyreported here was smaller than that reportedduring strenuous supine exercise by otherinvestigators.27 The conclusions drawn fromprevious studies in humans, however, mustbe interpreted in the light of methodologicallimitations. All previous investigators haverelied on clearance techniques for the mea-surement of renal blood flow, principally withsodium p-aminohippurate (PAH). Clearancetechniques measure effective renal plasmaflow. To convert this value to total renalblood flow, the packed cell volume andarteriovenous extraction ratio for PAH mustbe known. Bucht and colleagues measured
249
on 2 January 2019 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.70.3.247 on 1 S
eptember 1993. D
ownloaded from

Haywood, Counihan, Sneddon, Jennison, Bashir, McKYnna
the PAH extraction ratio at rest and duringmoderate exercise in three subjects and foundno significant change,29 but a fall in the PAHextraction fraction at maximal exercise, if notaccounted for in clearance calculations,would result in underestimation of renalblood flow. A further limitation of applyingclearance techniques to the study of exerciseis that they are unsuited to the measurementof rapidly changing haemodynamic states."In practice a steady state must be maintainedfor at least 15 minutes if the values for renalblood flow are to approach an acceptablelevel of accuracy. Most investigators havetherefore been forced to study long durationsub-maximal exercise. Because the continu-ous renal vein thermodilution techniqueallows direct measurement of renal bloodflow to be achieved over about 30 seconds,these methodological problems did not arise.By contrast the theoretical weaknesses of thecontinuous renal vein thermodilution tech-nique are that measurements are limited tothe blood flow in the left kidney rather thanin both kidneys. As there is no reason tobelieve that neural regulation of renal bloodflow affects the two kidneys differentially thisis unlikely to be of importance. The tech-nique has been extensively validated."3
In conclusion, the methodological differ-ences and the shorter duration of the exerciseprotocol used may explain the smallerdecreases in renal blood flow found in ;thisstudy compared with the findings of previousinvestigators. The results indicate that theincreased vasoconstriction in response toexercise found in the forearm is also presentin the renal vascular bed in patients who haveundergone heart transplantation.
RENAL OXYGEN CONSUMPTION IN RESPONSETO EXERCISEPatients with heart failure increase the per-centage of oxygen extracted from the bloodstream by the kidneys during exercise.'2 Thisis the first study to report oxygen extractionby the human kidney at maximal exercise andit would seem that the phenomenon found inpatients with heart failure at lower levels ofexercise, is also present in controls and hearttransplant recipients at peak exercise.
IS THE MECHANISM VENTRICULARDEAFFERENTATION?In interpreting the results from this study,care must be taken in assigning causal expla-nations to the increased reflex vasoconstric-tion found in the forearm and kidney duringleg exercise, as there are many differencesbetween controls and heart transplant recipi-ents other than cardiac denervation. Theresults seem, however, to parallel studies onthe effects of cardiac denervation in some ani-mal models. DiCarlo and Bishop found thatblockade of the cardiac vagal afferent fibresby intraperncardial procainamide injection,enhanced the vasoconstrictor response in therenal vascular bed during dynamic exercise inrabbits.24 Other explanations for the differ-ences found might be effects of the antirejec-
tion treatment on the response of the efferentsympathetic nervous system to exercise, or achronic effect of cardiothoracic surgery otherthan cardiac denervation. There is some evi-dence that cyclosporin increases sympatheticnerve traffic and calf vascular resistance in theresting state," however, this influence shouldhave been present both at rest and at peakexercise and does not therefore explain thegreater percentage increase in vasoconstric-tion in response to exercise. In the forearmvascular bed the altered forearm vascularreflexes in response to lower body negativepressure seen after cardiac transplantation arenot present in renal transplant patients onsimilar treatment'9; the differences noted aretherefore unlikely to be due to immunosup-pressive treatment.
It also seems unlikely that the differencesin regional haemodynamic responses to exer-cise result from the limited functional capac-ity of the cardiovascular system in hearttransplant recipients. The heart failure groupreached a similar Vo2 to the transplant recipi-ents; although there was a trend towardsincreased renal vascular resistance, there wasno significant difference in the peak forearmvascular resistance or the percentage fall inrenal blood flow from that shown by the nor-mal controls. It is also possible that decreasedafferent input from arterial baroreceptors tothe vasomotor centre might have resulted inincreased sympathetic drive during exercise inthe transplant recipients. Artificial increase ofblood pressure by a noradrenaline bolus dur-ing static exercise in cats is known to reduceefferent sympathetic drive to the kidneys.This was thought to be due to stimulation ofthe arterial baroreflex. Although the peakblood pressures were similar in the controland transplanted groups, the increase inblood pressure from rest to peak exercise incontrols was not significantly greater than intransplant recipients (24 (7) v 15 (5) mm Hg,NS). The mean blood pressure change incontrols was, however, significantly greaterthan in the patients with heart failure (24 (7)v - 3 (7) mm Hg, p < 0-05) and yet therewas no significant increase in renal or forearmvasoconstriction in the heart failure groupcompared with controls. It therefore seemsunlikely that the principle cause of theincreased vasoconstrictor drive seen in thetransplant recipients was a lower level ofstimulation- of the arterial baroreflex.
UNIFORMTY OF REGIONAL VASCULARREFLEXESThis is the first report in humans of simulta-neous measurement of the effects of exerciseon the regional circulations of both a limbmuscle bed and an internal organ. The meanpercentage changes in forearm and renalblood flows are similar in the controls andheart transplant patients (controls: fall inforearm blood flow 32% (6%), fall in renalblood flow 32% (4%); and transplants: fall inforearm blood flow 39% (10%), fall in renalblood flow 44% (4%); however, there is somedisparity between the responses in the two
250
on 2 January 2019 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.70.3.247 on 1 S
eptember 1993. D
ownloaded from

Increased renal andforearm vasoconstriction in response to exercise after heart transplantation
regions in the heart failure group (fall in fore-arm blood flow 22% (7%), fall in renal bloodflow 38% (5%). Whether this reflects adifferential effect of activated neurohumoralmechanisms on the two regions is speculative.Despite this there is a moderate correlation(p = 0-56, p < 0 002) between the changes inforearm and renal vascular resistance whenthe values for individual subjects ._are plottedfor all patients in the study. Overall, theresults suggest that short term changes in vas-cular tone in the limb muscle beds inresponse to sympathetically mediated cardio-vascular reflexes, are broadly'similar to "thosein the kidneys.
PATHOPHYSIOLOGICAL SIGNIFICANCEThe functional capacity of the circulationremains limited after heart transplantationdespite normal resting ventricular ejectionfractions.2022 35 The limitation of maximaloxygen consumption is thought to reflect lim-itation of the increase in cardiac output inresponse to- exercise. Whereas this failure tomount a normal increase in cardiac outputmay be primarily explained by a blunted heartrate response during exercise, it is also possi-ble that abnormally raised systemic vascularresistance resulting from increased vasocon-striction in non-exercising regions is a con-tributing factor. Evidence exists for 'gradualsympathetic efferent reinnervation of thetransplanted heart36; vagal afferent reinnerva-tion of the transplanted heart has not beenfound. Changes in exercise haemodynamicsarising from the division of vagal afferentfibres may therefore be permanent. Renalimpairment is one of the largest problems inthe management of patients after heart trans-plantation. The most important cause ofrenal dysfunction in these patients is almostcertainly the renal toxicity of cyclosporin.Part of the mechanism of cyclosporin inducedrenal toxicity is thought to be renal vasocon-striction. It is possible that the removal ofthe main cardiovascular reflex acting to mod-erate sympathetic vasoconstrictor drive to thekidney,56 is a contributing factor' in thosepatients who develop renal impairment afterheart transplantation.Guy A Haywood, James F Sneddon, and Yaver Bashir weresupported by British Heart Foundation -Junior ResearchFellowships. Peter J Counihan was supported by a SquibbCardiovascular Research Fellowship. Presented in part at theyoung research workers competition, British Cardiac SocietyMeeting, Harrogate, May 1992.
1 Wade OL, Bishop JM. Cardiac output and regional bloodflow. Oxford: Blackwell, 1962.
2 Rowell L. Redistribution of blood flow during exercise. In:Shepherd J, Abboud F, Geiger S, eds. Han4book ofphys-iology (American Physiological Society). The cardiovascularsystem. The penrheral . circuklion, part 2. Baltimore:Waverly Press, 1983:1004-9.
3 Abboud F, Thames M. Interaction of cardiovascularreflexes in circulatory control. In: Shepherd J, AbboudF, Geiger S, eds. Handbook of physiology (AmericanPhysiological Society). The cardiovascular system. Theperipheral circulation, part 2. Baltimore: Waverley Press,1983:706-7.
4 Mancia G, Donald D, Shepherd J. Inhibition of adrener-gic outflow to peripheral blood vessels by vagal afferentsfrom the cardiopulmonary region in the dog. Circ Res1973;33:713-21.
5 Thames M, Abboud F. Interaction of somatic and cardio-pulmonary receptors in control of renal circulation. AmJ Physiol 1979;237:H560-5.
-6 Thames M, Miller B, Abboud F. Baroreflex regulation of
renal nerve activity during volume expansion. Am JPhysiol 1982;243:H810-4.
7 Hirsch A, Levenson D, Cutler S, Dzau V, Creager M.Regional vascular responses to prolonged lower bodynegative pressure in normal subjects. Am Y Physiol1989;257:H219-25.
8 Bevegard B, Shepherd J. Reaction in man of resistanceand capacitance vessels in forearm and hand to legexercise. JAppl Physiol 1966;21:123-32.
9 Rea R, Eckberg D. Carotid baroreceptor-muscle sympa-thetic relation in humans. Am Y Physiol 1987;253:R929-34.
10 Jones N. Evaluation of a microprocessor controlled exer-cise testing system. YAppl Physiol 1984;57:1312-8.
11 Greenfield A, Whitney R, Mowbray J. Methods for theinvestigation of peripheral blood flow. British MedicalBulletin 1963;19:101-9.
12 Whitney R. Measurement of volume changes in humanlimbs. JPhysiol 1953;121:1-27.
13 Haywood G, Stewart J, Counihan P, Sneddon J, Tighe D,McKen'na W. Validation -of bedside measurements ofabsolute human renal blood flow by a continuous ther-modilution technique.'Crit Care Med 1992;20:659-64.
14 Counih;anP, Frenneaux--M, Webb D, McKenna W.Abnormal vascular responses to supine exercise inhypertrophic cardiomyopathy. Circulation 1991;84:686-96.
15 Bevegard'B, Shepherd J. Regulation of the circulationdiuring exercise in man. Physiol Rev 1967;47:178-213.
16 Rowell L. Huian car'diovascular adjustments to exerciseand thermal stress. Physiol Rev 1974,54:75-159.
17 Blair D, Glover W, Roddie I. Vasomotor responses in thehuman arm during leg exercise. Circ Res 1961;9:264-74.
18 Walker J, Abboud F, Mark A, Thames M. Interaction ofcardiopulmonary and somatic reflexes in humans. y ClinInvest 1980;65:1491-7.
19 Mohanty P, Thames M, Arrowood J, Sowers J,McNamara C, Szentpetery S. Impairment of cardiopul-monary baroreflex after cardiac transplantation inhumans. Circulation 1987;75:914-21.
20 Pope S, Stinson E, Daughters G, Schroeder J, Ingels N,Alderman E. Exercise response of the denervated heartin long-term cardiac transplant recipients. Am. Cardiol1980;46:213-8.
21 Banner N, Uloyd M, Hamilton R, Innes J, Guz A, YacoubM. Cardiopulmonary response to dynamic exercise afterheart and combined heart-lung transplantation. BrHearty. 1989;61:215-23.
22 Stevenson L, Sietsema K, Tillisch J, et al. Exercise capac-ity for survivors of cardiac transplantation or sustainedmedical therapy for stable heart failure. Circulation1990;81:78-85.
23 Manohar M. Blood flow to the respiratory and limb mus-cles and to abdominal organs during maximal exertionin ponies. Y Physiol(Lond) 1986;377:25-35.
24 Dicarlo S, Bishop V. Regional vascular resistance duringexercise: role of cardiac afferents and exercise training.Am YPhysiol 1990;258:H842-7.
25 Higgins C, Vatner S, Frauiliu D, Braunwald E. Effects ofexperimentally produced heart failure on the peripheralvascular response to severe exercise in conscious dogs.Circ Res 1972;31:186-94.
26 Merrill A, Cargill W. The effect of exercise on the renalplasma flow and filtration rare of normal and cardiacsubjects. Y7 Clin Invest 1948;27:272-7.
27 Grimby G. Renal clearances at rest and during prolongedsupine exercise at different loads. Y7 Appl Physiol1965;20:1294-8.
28 Werko L, Bucht H, Josephson B. The renal extraction ofpara-aniinohippuric acid and oxygen in man duringpostural changes of the circulation. Scand Y Clin LabInvest 1949;1:321-7.
29 Bucht H, Ek, J, Eliasch H, Holngren A, Josephson B,Werko L. The effect of exercise in the recumbent posi-tion on the renal circulation and sodium excretion innormal individuals. Acta Physiol Scand 1953:28:95-100.
30 Radigan L, Robinson S. Effects of environmental heatstress and exercise on renal blood flow and filtrationrate. YAppl Physiol 1949;2: 185-91.
31 Selkurt E. The renal circulation. In: Hamilton W,Dow P, ed. Handbook of physiology (American Physo-.lgical Society). Baltimore: Waverley Press, 1975:1483.
32 Bishop J, Wade 0, Donald K. Changes in jugular andrenal arteriovenous oxygen content difference duringexercise in heart disease. Clin Sci 1958;17:611-9.
33 Scherrer U, Rollins J, Tindall R, Morgan B, Victor R.Does cyclosporine stimulate sympathetic outflow inhumans. Circulation 1989;80(suppl 2):11-89.
34 Matsukawa K, Mitchell J, Wall P, Wilson L. The effect ofstatic exercise on renal sympathetic nerve activity in
_conscious cats. y Physiol (Lond) 1991;434:453-67.35 Pflugfelder P, Purves P, McKenzie F, Kostuk W. Cardiac
dynamics during supine exercise in cyclosporine-treatedorthopic heart transplant recipients: assessment byradionuclide angiography. I Am Coil Cardiol 1987;10:336-41.
36 Wilson R, Christensen B, Olivari M, Simon A, White C,Laxson D. Evidence for structural sympathetic reinner-vation after orthotopic cardiac transplantation inhumans. Circulation 1991;83:1210-20.
37 McNally P, Walls J, Feehally J. The effect of nifedipine onrenal function in normotensive cyclosporin-A-treatedrenal allograft recipients. Nephrol Dial Transplant1990;5:962-8.
251
on 2 January 2019 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.70.3.247 on 1 S
eptember 1993. D
ownloaded from