in vitro-efficacy of oily calcium hydroxide suspension on ... osteora/02 in vitro-efficacy... ·...
TRANSCRIPT
Medizinische Fakultät Zahnmedizinische Kliniken Klinik für Parodontologie
Klinik für Parodontologie, Freiburgstrasse 7, CH-3010 Bern
Prof. Dr. Anton Sculean
Klinikdirektor
Freiburgstrasse 7 CH-3010 Bern
Tel.: +41 (0)31 632 25 89
Fax: +41 (0)31 632 49 15
www.zmk.unibe.ch
In vitro-efficacy of oily calcium hydroxide suspension on human
alveolar osteoblasts, periodontal ligament fibroblasts and
microorganisms
S. Eick, T. Strugar, S. Ruggiero, R. J. Miron, A. Sculean
Department of Periodontology, Dental School, University of Bern, Bern, Switzerland
Running title: OCHS and host cells and bacteria
Sigrun Eick, Department of Periodontology, Laboratory of Oral Microbiology, Dental
School, University of Bern, Freiburgstrasse 7, CH-3010 Bern, Switzerland
Tel.: +41 31 632 2542
Fax: +41 31 632 8608
e-mail: [email protected]
Key words: oily calcium hydroxide suspension, human alveolar osteoblasts,
periodontal ligament fibroblasts, periodontopathogens
Seite 2/27
Abstract
Background and Objective: Nowadays, several methods have been established for
the complete reconstruction of the periodontium for periodontitis treatment. Recently
an oily calcium hydroxide suspension has been introduced to favour the tissue
regeneration. The purpose of this in vitro study was to investigate the effect of an
oily calcium hydroxide suspension (OCHS) on attachment and proliferation of
osteoblasts and periodontal ligament fibroblasts as well as periodontopathogenic
bacteria.
Methods: Human alveolar osteoblasts (HAO) and periodontal ligament (PDL)
fibroblasts were cultured on OCHS. Adhesion and proliferation were counted up to 48
h and mineralization was assayed after 1 and 2 weeks. Furthermore antimicrobial
efficacy as well as the influence of infected PDL cells and OCHS on the HAO counts
were determined.
Results: More than a 2-fold increase in adherent HAO cells was observed at 4 h
following application of OCHS when compared to the control group. Proliferation of
HAO cells at 48 h was stimulated by moderate concentrations of OCHS, whereas a
high concentration of OCHS was inhibitory. Mineralization was observed only for
HAO cells treated with OCHS. For PDL fibroblasts, OCHS did not exert any positive
effect on attachment or proliferation. PDL fibroblasts infected with
periodontopathogens negatively influenced the proliferation of osteoblasts
independent of OCHS application.
Conclusions: The data suggest that OCHS promotes osteoblast attachment,
proliferation and mineralization in a concentration-dependent basis. OCHS does not

Seite 3/27
have any significant influence on attachment of PDL fibroblasts.
In addition periodontopathogens may negatively influence the
proliferation of osteoblasts.

Seite 4/27
Pathogenesis of periodontitis is thought to be a response of the host to microbial
plaque. A small group of predominantly gram-negative anaerobic or microaerophilic
bacteria within plaque is associated with initiation and progression of periodontitis.
Organisms strongly implicated as etiologic agents of periodontitis include
Aggregatibacter actinomycetemcomitans, Porphyromonas gingivalis, Tannerella
forsythia and Treponema denticola (1). Moreover, other species such as
Campylobacter rectus, Eubacterium nodatum, Fusobacterium nucleatum, Prevotella
intermedia, Parvimonas micra, Streptococcus constellatus support pathogenesis of
disease (1, 2). Bacteria interact with host cells resulting in expression of inflammatory
mediators which are capable of stimulating bone resorption and soft tissue
destruction via activation of matrix-metallo-proteases (3).
Resolution of inflammation and arresting disease progression is the minimal goal of
periodontal and periimplant treatment. Nowadays, the complete reconstruction of the
periodontium is the desired outcome. Several methods have previously been
introduced including guided tissue regeneration using non-resorbable and resorbable
membranes (4, 5). In combination with guided tissue regeneration or alone, several
compounds were proven to promote new bone formation. The application of enamel
matrix proteins to intrabony defects has been an established treatment regimen for
many years (6-8). Furthermore, bone grafts (9, 10) bone substitute materials (11, 12)
and growth factors (13-15) have also been successfully utilized.
Recently an oily calcium hydroxide containing paste (Osteora®, before
Osteoinductal®, DFS-Diamon GmbH Riedenburg, Germany) was introduced.
Calcium hydroxide (Ca(OH)2) which is a white odourless powder with a low solubility
in water has antibacterial properties by the release of highly reactive hydroxyl ions in

Seite 5/27
aqueous fluids which damages cytoplasmatic membranes,
proteins and DNA (16). In endodontic treatment it is used as a
pulp-capping agent (17), as a disinfectant during the root canal treatment (18) and for
apexification after pulp death (19). In the pulp, a superficial necrosis induced by the
high pH occurs with a mild inflammatory response and hard tissue formation in the
environment (20).
The calcium hydroxide containing paste uses as a carrier substance synthetically
produced porcine oleum pedum and vaselinum album. In several animal models,
studies of this oily calcium hydroxide suspension (OCHS) resulted in different
outcomes. In a guided tissue regeneration model in the calvaria of minipigs, OCHS
failed to exert osteoinductive properties (21). Application during the osteotomy phase
of distraction osteogenesis in a rabbit mandible increased regeneration and new
bone formation (22). In dogs, OCHS favoured periodontal regeneration when used
after access flap surgery of intrabony periodontal defects (23). In rats, it hampered
bone healing when applied with guided bone regeneration (24). Similarly, in a dog
model the healing process of endosseous implants was retarded after application of
OCHS (25).
In the few clinical studies, varying outcomes were also reported. OCHS improved
early wound healing after non-surgical therapy (26). In a study on access flap
surgery, higher pocket depths reductions and clinical attachment level gains were
found (27), whereas in a similar study OCHS failed to demonstrate any superior
outcome when compared with open flap surgery alone (28).
Despite the clinical use of OCHS, knowledge about the mode of action remains
limited. The purpose of the scheduled study was to determine the effect of OCHS on
Seite 6/27
osteoblasts and periodontal ligament fibroblasts cell behavior as
well as on periodontopathogenic bacteria.
Material and methods
Test substances
OCHS (Osteora®, DFS-DIAMON GmbH, Riedenburg, Germany) was used.
According to manufacturer’s information it is composed of 20% w/w Ca(OH)2, 40%
oleum pedum and 40% vaselinum album. Three different concentrations (1 U, 2 U, 3
U) were chosen. 1 U represents 2.5 mg of total material. As controls, calcium
hydroxide in aqueous solution (1.5 mg corresponding to 3 U of OCHS) and oleum
pedum substance (3 mg corresponding to 3 U of OCHS) were used. OCHS was also
tested at higher concentrations (50 mg, 100 mg) to determine a possible
antimicrobial effect.
Cells
Human alveolar osteoblasts (HAO) were obtained from three periodontally healthy
patients during surgery (extraction of teeth for orthodontic reasons). Following colla-
genase digestion, cells were plated in T-75 flasks containing cell cultivation medium
(DMEM, Invitrogen, Carlsbad, CA) supplemented with 10% of fetal bovine serum
(FBS, Invitrogen).
Human periodontal ligament (PDL) fibroblasts were collected from three periodontally
healthy patients during surgery (extraction of teeth for orthodontic reasons). PDL
cells were harvested from the middle third portion of tooth and placed in T-25 cell
Seite 7/27
culture flasks till cell confluency. The cultivation medium was
DMEM supplemented with 10% FBS.
Using the tissue for research purposes was approved by the Ethical commission of
the Canton Bern. All patients gave their consent.
Microorganisms
The following species have been tested for antimicrobial assays: F. nucleatum ATCC
25586, P. intermedia ATCC 25611, P. gingivalis (ATCC 33277 and three clinical iso-
lates), T. forsythia ATCC 43037, A. actinomycetemcomitans (Y4 and three clinical
isolates), C. rectus ATCC 33238, Eikenella corrodens ATCC 23834, E. nodatum
ATCC 33099, P. micra ATCC 33270, and Capnocytophaga gingivalis ATCC 33624.
All strains were precultivated 42 h before experiments. Modified tryptic soy agar (29)
was used as cultivation media.
A. actinomycetemcomitans Y4 as well as P. gingivalis ATCC 33277, T. forsythia
ATCC 43037 and T. denticola ATCC 35405 in combination were used in the experi-
ments which analyzed the effect of OCHS on microorganisms in interaction with host
cells.
Determination of effect of oily calcium hydroxide suspension on osteoblasts
Slides were placed into 24-well plates and covered with the test substances (1-3 U
OCHS, 1.5 mg Ca(OH)2 and 3 mg oleum pedum). Immediately thereafter, HAO cells
were added at a density of 10,000 cells / well and the wells were incubated at 37°C
with 5% CO2. Cells were fixed and stained for adhesion and proliferation experiments
at 2 h, 4 h, 24 and 48 h using DAPI staining. Cell differentiation was analyzed by

Seite 8/27
determination of alkaline phosphatase activity and
mineralization by using 2% alizarin red S staining 1 and 2
weeks after starting experiments. Each 10 fields of 1 mm2 were counted. A counting
grid was used and each field (50 µm × 50 µm) with positive staining was counted; the
mean was used as a single value for analysis.
Further, supernatants were collected at 24 h and 48 h and the levels of released
active TGF-β1 were determined by using ELISA-kits (R&D Systems Europa Ltd.,
Abingdon, UK) according to the manufacturer’s description. The detection level of the
kit was 50 pg/mL.
Determination of effect of oily calcium hydroxide suspension on PDL
fibroblasts
Similarly to HAO cells, effects on PDL fibroblasts were determined. Slides which
have been placed into 24-well plates were covered with the test substances. PDL
fibroblasts were added at a density of 10,000 cells / well. Cells were fixed and
stained for adhesion and for proliferation experiments at 2 h, 4 h, 24 h and 48 h using
DAPI staining as described for HAO cells.
Supernatants were collected 4, 24 and 48 h after starting the experiments. In the
supernatants, the levels of released active transforming growth factor (TGF)-β1 and
matrix metalloproteinase (MMP)-1 were determined by using ELISA-kits (R&D
Systems Europa Ltd.) according to the manufacturer’s description. The detection
level of the MMP-1 kit was 5 pg/mL.
Determination of antimicrobial efficacy of oily calcium hydroxide suspension

Seite 9/27
A modified agar diffusion method was used due to the
insolubility of OCHS. One hundred µl of bacterial suspension
(MacFarland 0.5) were spread on agar plates (Wilkins Chalgren agar supplemented
with 5% blood). Then, each two gaps were prepared using a cork borer (diameter 7
mm). After that, the gap was filled with 100 µL of agar followed by the test substance
(50 mg and 100 mg of OCHS). After incubation at 37°C in the anaerobic atmosphere
for 42 h, the inhibition zones were measured. To exclude a growth-promoting effect
of OCHS, suspensions of selected bacterial strains (P. gingivalis ATCC 33277, P.
gingivalis M5-1-2, A. actinomycetemcomitans Y4 and F. nucleatum ATCC 255866)
were added to 200 µL nutrient broth added with 50 mg of OCHS (20%w/v). Tubes
had been incubated for 24 h anaerobically. Immediately before removing 25 µl of
mixture, suspensions were mixed by vortexing and short centrifugation at 400 g. The
removed 25 µl were serially diluted and each 100 µl were plated on agar plates. The
numbers of viable bacteria were determined by counting the colony forming units
(cfu). All experiments were performed in duplicates.
Determination of the effect of oily calcium hydroxide suspension on
osteoblasts and PDL fibroblasts interaction with microorganisms
The concentration of 2 U (5 mg) OCHS was selected and placed on each well of a
24-well plate for experiments focusing on the interaction of host cells with bacterial
strains.
HAO cells and PDL fibroblasts respectively were seeded on the slides with and
without coverage of 2 U of OCHS. A. actinomycetemcomitans Y4 as well as the
combination of P. gingivalis ATCC 33277, T. forsythia ATCC 43037 and T. denticola

Seite 10/27
ATCC 35405 were added. The bacterial load was always 106
per well. The HAO cells and PDL fibroblasts respectively were
fixed and stained at 4 h.
Additionally HAO cells were exposed to supernatants of PDL fibroblasts on or without
OCHS and infected with bacteria. For that purpose, 2 U of OCHS were added to
each one well of a 24-well-plate. Then PDL fibroblasts were placed to that and
another plate without OCHS. In part PDL fibroblasts were infected with A.
actinomycetemcomitans Y4 and the combination of P. gingivalis ATCC 33277, T.
forsythia ATCC 43037 and T. denticola ATCC 35405 as described before. The cell
cultivation medium was DMEM without FBS. After 4 h incubation at 37°C,
supernatants were collected and sterile filtered. HAO cells were seeded on plates
and treated with the filtered supernatants of PDL cells mixed 1 : 1 with DMEM and
10% FBS. As made before, cells were fixed and stained for adhesion experiments at
4 h and for proliferation experiments at 48 h using DAPI staining.
Statistical analysis
Except for the antimicrobial assays at least six independent experiments were made
per group. Statistical analysis was made by using Student’s t-test for independent
samples and one way ANOVA test followed by Post Hoc LSD analysis.
Results
Effect of oily calcium hydroxide suspension on osteoblasts
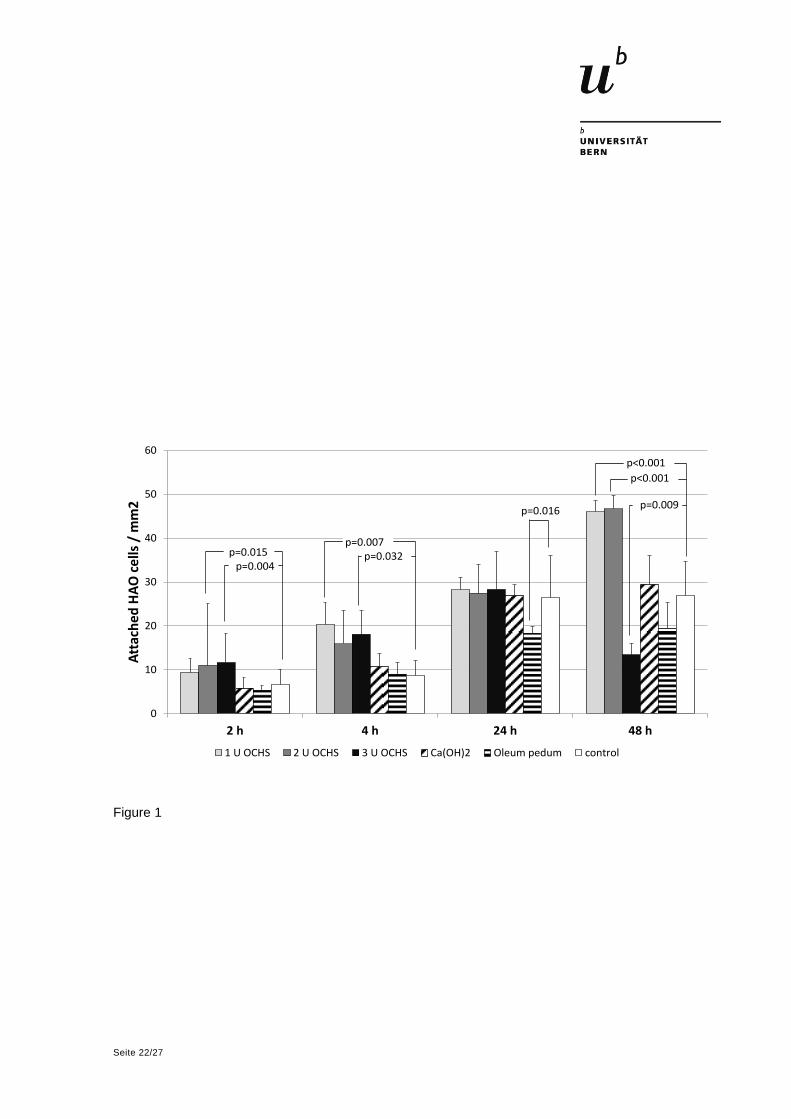
Addition of OCHS promoted the attachment of HAO cells. After 2 h, 11.00 ± 4.90
cells / mm2 adhered to a surface covered with 2 U of OCHS. Using 3 U the value was
Seite 11/27
11.67 ± 2.89 cells / mm2. These differences were significant in
comparison to the control, where 6.57 ± 3.55 HAO cells were
found per mm2 on the surface. After 4 h, 20.33 ± 14.13 HAO cells / mm2 were
counted after coverage with 1 U of OCHS and 18.11 ± 6.66 HAO cells / mm2 when 3
U of OCHS were used being significantly different from the controls (8.67 ± 3.50 HAO
cells / mm2). Stimulated proliferation was found 48 h after starting the experiments
and coverage with 1 U and 2 U of OCHS (1 U: 46.00 ± 13.11 HAO cells / mm2, 2 U:
46.67 ± 18.23 HAO cells / mm2 in comparison to control: 26.89 ± 7.25 HAO cells /
mm2). In contrast to the 1 U and 2 U of OCHS, the high concentration of 3 U
significantly inhibited the proliferation of HAO cells (13.44 ± 5.20 HAO cells / mm2).
An influence of the used Ca(OH)2 concentration was not registered. Coverage with
oleum pedum was followed by a decreased cell number 24 h after addition of the
cells. The results are presented in Figure 1.
Twenty-four hours after applying HAO cells to OCHS (all three used concentrations)
the amount of released TGF-β1 was significantly reduced, whereas after 48 h the
level of TGFβ-1 tended to increase in comparison to the control (Figure 2).
The differentiation and mineralization of the HAO cells was also analyzed. In all
experiments only HAO cells positively stained for alkaline phosphatase were found.
The mineralization was measured by counting the calcium noduli (stained area in %
of the whole area) 1 week and 2 weeks after beginning the experiments. To ensure
that only mineralization of cells was counted, OCHS with no cells was used as a
negative control. Without addition of OCHS, no mineralization was present on the
surface. When the surface was covered with OCHS, extracellular mineralization of
HAO was detectable after one week (5.57±1.97% stained area; Figure 3). The
quantity did not significantly change after two weeks (4.12±1.59%).

Seite 12/27
Effect of oily calcium hydroxide suspension on PDL fibroblasts
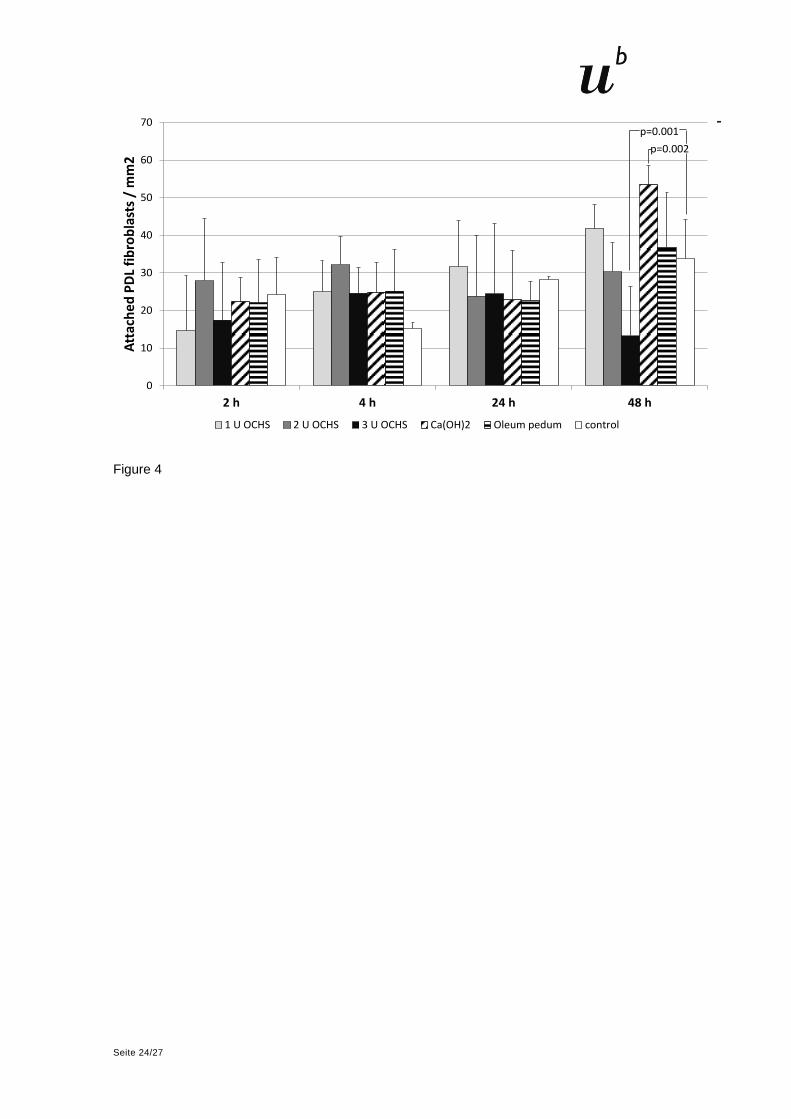
Addition of OCHS did not have any significant influence on attachment of PDL
fibroblasts. Reduced proliferation was found 48 h after starting the experiments and
coverage with 3 U of OCHS (13.22 ± 4.12 PDL fibroblasts / mm2) in comparison with
the controls (33.89 ± 17.48 PDL fibroblasts / mm2). In contrast, Ca(OH)2 stimulated
the proliferation of PDL fibroblasts (53.44 ± 15.22 PDL fibroblasts / mm2 compared to
control values at the 48 h time-point (Figure 4).
Four hours after applying PDL fibroblasts to 2 U of OCHS the amount of released
TGF-β1 was significantly increased, whereas after 48 h the level of TGFβ-1 was
reduced in comparison with the control (all three used concentrations of OCHS;
Figure 5). MMP-1 was not detectable 4 h after beginning the experiments. After 24 h,
all used concentrations of OCHS elevated significantly the levels of MMP-1 in the
supernatants. This effect was still visible after 48 h, but only for the two higher
concentrations of OCHS (Figure 5).
Antimicrobial efficacy of oily calcium hydroxide suspension
Experiments using modified agar diffusion technique did not reveal any inhibition
zone by OCHS in the two tested concentrations. Final experiments using selected
species underline that OCHS does not influence growth of periodontopathogens.
Neither growth-suppressing nor growth-promoting effects were visible; differences to
controls were always below 0.2 log10-stages (data not shown). It has to be noticed
that due to the insolubility of OCHS the tubes contained two layers, one of OCHS
Seite 13/27
and one of broth; thus only at the interface compounds released
from OCHS might interfere with bacteria.
Effect of oily calcium hydroxide suspension on osteoblasts and PDL
fibroblasts in interaction with microorganisms
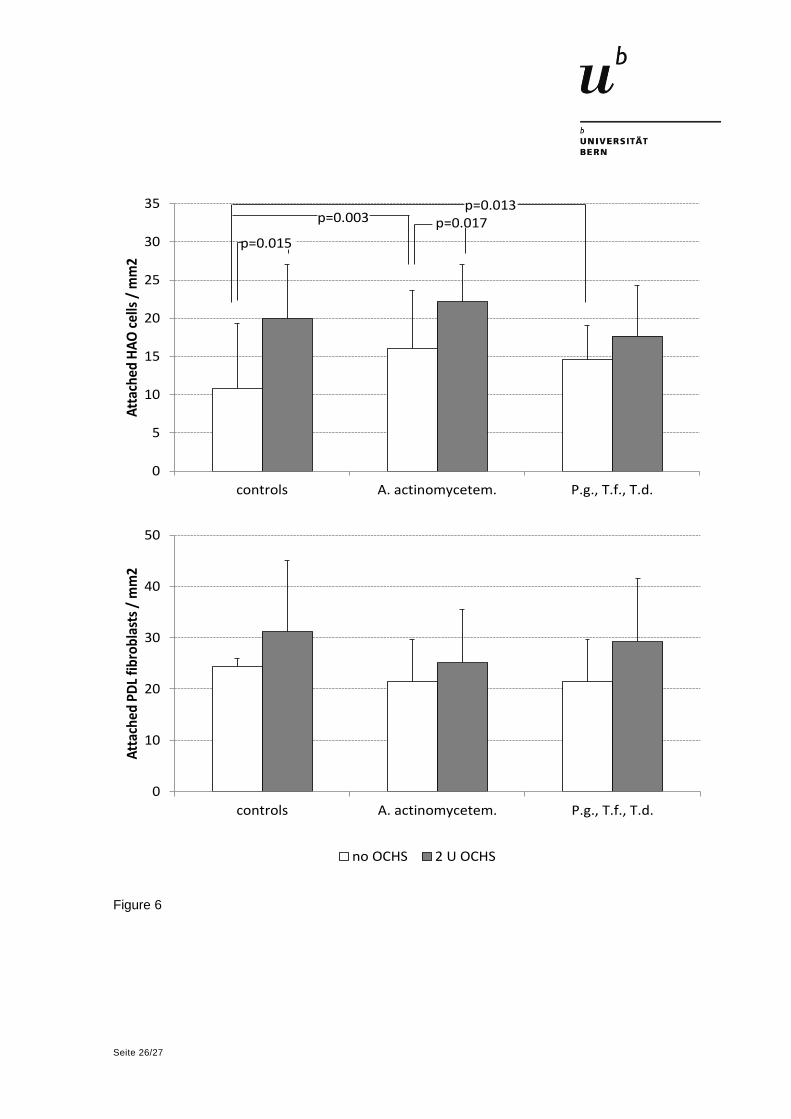
Surprisingly, the addition of bacteria enhanced the numbers of attached HAO cells
(A. actinomycetemcomitans Y4: 16.00 ± 4.44 HAO cells / mm2, P. gingivalis, T.
forsythia, T. denticola in mixture: 14.56 ± 4.07 HAO cells / mm2) being significantly
higher than the controls (10.87 ± 8.43 HAO cells / mm2). Otherwise, the addition of
bacteria did not significantly change the numbers of adhered HAO cells when the
slides were covered with 2 U of OCHS. If A. actinomycetemcomitans Y4 was present,
the difference of numbers of HAO cells with 2 U of OCHS (25.08 ± 10.04 HAO cells /
mm2) was still significant in comparison with those without OCHS (controls). Contact
with bacteria did not significantly influence the numbers of attached PDL fibroblasts
(Figure 6).
Most supernatants of PDL fibroblasts cultured on OCHS tended to promote
attachment and proliferation of HAO cells, the difference was significant for all tests
(p=0.015) and for A. actinomycetemcomitans at the 4 h time-point. Infection of PDL
fibroblasts with A. actinomycetemcomitans did not influence the numbers of attached
HAO cells. In contrast, the infection of PDL fibroblasts with the combination of P.
gingivalis, T. forsythia and T. denticola remarkably decreased the HAO cell counts at
the 48 h time-point (Figure 7).
Discussion

Seite 14/27
OCHS is an oily suspension which contains Ca(OH)2 as the
active constituent. Other components are synthetically produced
oleum pedum tauri as the carrier material which contains triglycerides including
oilacid, palmitin acid, hexadecen acid and vaselinum album.
Seeding of HAO cells on OCHS affected their attachment and proliferation. Our
results indicate concentration sensitivity. Low to moderate concentrations of OCHS
acted clearly stimulatory, whereas after application of the highest used concentration,
in part detrimental results were seen. To retard release of Ca(OH)2, OCHS contains a
high percentage of oleum pedum. The HAO counts were reduced after placement on
oleum pedum. Oleum pedum seems to counteract the stimulating activity of Ca(OH)2.
In an animal model using open Teflon capsules, OCHS inhibited bone formation and
an active resorption of OCHS was not observed (24). It can be suggested that the
missing degradable properties are certainly based on the oleum pedum. This seems
to be of more importance with increasing concentrations. This obvious sensitivity of
the used concentration might explain the reported different outcomes in animal and
clinical studies. According to our first results, a moderate concentration was chosen
for ongoing experiments. Using this concentration, mineralization was found 1 – 2
weeks after exposing osteoblasts to OCHS. Recently it was demonstrated that
Ca(OH)2 is able to stimulate mRNA expression of bone sialoprotein and Runx2 (30).
Runx2 is an essential transcription factor in osteoblast differentiation (31). Bone
sialoprotein is known to mediate cell attachment and promote bone formation and
mineralization (32).
OCHS did not exert any positive effect on attachment and proliferation of PDL
fibroblasts. Similarly to osteoblasts, the highest used concentration reduced
proliferation of PDL fibroblasts after 48 h. This was opposite to calcium hydroxide in

Seite 15/27
aqueous solution. Proliferation of PDL fibroblasts induced by
Ca(OH)2 was described recently; but in contrast to us, OCHS
also had a stimulatory effect on proliferation in that study (33).
TGF-β1which belongs to the TGF-β family is secreted in an inactive form; it is
activated by plasmin, thrombospondin, thrombin and MMPs (34, 35). TGF-β1 is a
multifunctional cytokine, it promotes biosynthesis of extracellular matrix in fibroblasts,
controls physiological processes during wound and bone healing and promotes
survival of myofibroblasts (34, 35). HAO cells released significantly less active TGF-
β1 after attachment when pretreated with OCHS, by trend this effect was weakened
48 h after the beginning of the experiments. Our first determination was at 4 h after
exposure to OCHS which may influence the results. In another study, 5 minutes after
treatment of bone surfaces with calcium hydroxide, bone cells secreted more TGF-
β1, but already after 15 min the levels of TGF-β1 returned to those without treatment
(36). In contrast, PDL fibroblasts released more TGF-β1 at the beginning, the effect
became opposite after 48 h in our study. MMP-1 was not detected initially. 24 h and
48 h after beginning, the levels of MMP-1 were increased when PDL fibroblasts were
cultured on CHOS. This was contradictory to the TGF-β1 levels and confirms findings
about reduced expression of MMP-1 in fibroblasts characterized by elevated TGF-β1
expression (37). MMP-1 is able to degrade fibrillar collagens and other matrix
molecules (38). The high initial amount of MMP-1 may support tissue remodeling.
Supernatants of PDL fibroblasts pretreated with OCHS promoted the attachment and
proliferation of HAO cells. This might be caused in part by the released calcium
hydroxide together with high amount of TGF-β1 in the environment of PDL fibroblasts
exposed to OCHS. Calcium hydroxide in aqueous solution was found to provide a
favorable environment for the anabolic effect of TGFβ1 on osteoblasts (39).
Seite 16/27
An antibacterial effect by OCHS even in extremely high
concentration was not found by using a modified agar diffusion
test. The result was confirmed by using liquid medium for selected species. Calcium
hydroxide is widely used in endodontic treatment. Also there, a limited antimicrobial
efficacy was described analyzing root canals after treatment in vivo (40, 41). Only
one other study reported the effect of OCHS on periodontopathogens. Two A.
actinomycetemcomitans strains were selected; OCHS did not exert an antibacterial
effect against the ATCC 43718 strain (serotype b) (42). This strain is the Y4 strain
which was included in our study. In our study also one clinical isolate belonged to
serotype c. In contrast to the results described before (42), we did not find any
antibacterial effect. Surprisingly, the addition of bacteria enhanced the number of
attached HAO cells. The cell cultivation medium contained serum. Serum may
provide receptors for attachment of bacteria and the bacteria themselves may serve
as a receptor for HAO cells. Coverage with OCHS neglected that effect. Interestingly,
even in the presence of A. actinomycetemcomitans OHCS stimulated the attachment
of HAO cells. Also infection of PDL fibroblasts with that species did not affect the
later attachment and proliferation of HAO cells independently if the PDL fibroblasts
were exposed to OCHS or not. A. actinomycetemcomitans stimulates the mRNA
expression of inflammatory cytokines differently, it induces mRNA expression of IL-6
and IL-8 but not of IL-1β (43), moreover capsular polysaccharide of A.
actinomycetemcomitans inhibits the release of interleukin (IL)-6 and IL-8 (44). On the
other hand capsular-like polysaccharide antigen of A. actinomycetemcomitans
induces apoptotic cell-death in osteoblastic cells (45).
Otherwise, P. gingivalis, T. forsythia and T. denticola in combination were selected.
These three species represent the so called “red complex”; they are highly

Seite 17/27
proteolytic, occur together in the late plaque and therefore in
closest contact with the adjacent tissue (46). Treatment of
osteoblasts with supernatants of infected PDL fibroblasts did not influence
attachment of HAO cells but it inhibited remarkably proliferation of HAO cells
independently if the PDL fibroblasts were exposed to OCHS or not. Sterile filtered
supernatants in the environment of infected PDL fibroblasts might contain secreted
virulence factors of bacteria. E.g., secreted proteases may influence proliferation of
HAO cells. Gingipains responsible for the majority of the proteolytic activity of P.
gingivalis (47), are able to destroy osteoprotegerin (48) and can inhibit proliferation of
osteoblasts by causing early G1 arrest in cell cycle (49). A T. forsythia protease has
been characterized recently (50), no data about a direct influence on osteoblasts are
available up to now. An outer membrane protein of T. denticola was shown to inhibit
osteoprotegerin expression (51). Further, periodontopathogens stimulate the release
of inflammatory cytokines from gingival fibroblasts which may affect proliferation of
osteoblasts. Viable P. gingivalis induce a strong mRNA expression of IL-1β, IL-6 etc.
(52). Thus, elimination of proteolytic pathogens is essential in treatment of
periodontitis. The missing antimicrobial activity of OCHS suggests the additional use
of an antimicrobial, such as chlorhexidine. In combination with a calcium hydroxide
paste 0.4% chlorhexidine did not affect osteoblastic cell biology in vivo (53).
Although, our in vitro studies did not consider the complexity in vivo, they may
explain in part the different outcomes observed in animal and clinical studies. In
conclusion, OCHS promotes attachment, proliferation of osteoblasts and
mineralization of their tissue. The effect seems to be concentration-dependent and
suggests an application of a moderate concentration. OCHS did not have significant

Seite 18/27
influence on attachment of PDL fibroblasts.
Periodontopathogens may negatively influence the proliferation
of osteoblasts.
Acknowledgement
We are grateful to Regula Hirschi and Marianne Weibel (Department of Periodontology, University of
Bern) for excellent assistance in performing in vitro assays. This study was funded by DFS-DIAMON
GmbH, Riedenburg, Germany. The authors declare that they have no conflicts of interest.
References
(1) Report C. Periodontal diseases: pathogenesis and microbial factors. Ann Periodontol 1996; 1: 926-932.
(2) Socransky SS, Haffajee AD, Cugini MA, Smith C, Kent RL, Jr. Microbial complexes in subgingival plaque. J Clin Periodontol 1998; 25: 134-144.
(3) Hernandez M, Dutzan N, Garcia-Sesnich J, et al. Host-pathogen interactions in progressive chronic periodontitis. J Dent Res 2011; 90: 1164-1170.
(4) Pretzl B, Kim TS, Holle R, Eickholz P. Long-term results of guided tissue regeneration therapy with non-resorbable and bioabsorbable barriers. IV. A case series of infrabony defects after 10 years. J Periodontol 2008; 79: 1491-1499.
(5) Silvestri M, Rasperini G, Milani S. 120 infrabony defects treated with regenerative therapy: long-term results. J Periodontol 2011; 82: 668-675.
(6) Siciliano VI, Andreuccetti G, Siciliano AI, Blasi A, Sculean A, Salvi GE. Clinical outcomes after treatment of non-contained intrabony defects with enamel matrix derivative or guided tissue regeneration: a 12-month randomized controlled clinical trial. J Periodontol 2011; 82: 62-71.
(7) Jepsen S, Heinz B, Jepsen K, et al. A randomized clinical trial comparing enamel matrix derivative and membrane treatment of buccal Class II furcation involvement in mandibular molars. Part I: Study design and results for primary outcomes. J Periodontol 2004; 75: 1150-1160.
(8) Sculean A, Kiss A, Miliauskaite A, Schwarz F, Arweiler NB, Hannig M. Ten-year results following treatment of intra-bony defects with enamel matrix proteins and guided tissue regeneration. J Clin Periodontol 2008; 35: 817-824.
(9) Sculean A, Stavropoulos A, Windisch P, Keglevich T, Karring T, Gera I. Healing of human intrabony defects following regenerative periodontal therapy with a bovine-derived xenograft and guided tissue regeneration. Clin Oral Investig 2004; 8: 70-74.
(10) Nygaard-Ostby P, Bakke V, Nesdal O, Susin C, Wikesjo UM. Periodontal healing following reconstructive surgery: effect of guided tissue regeneration using a bioresorbable barrier device when combined with autogenous bone grafting. A randomized-controlled trial 10-year follow-up. J Clin Periodontol 2010; 37: 366-373.
(11) Kumar PG, Kumar JA, Anumala N, Reddy KP, Avula H, Hussain SN. Volumetric analysis of intrabony defects in aggressive periodontitis patients following use of a novel composite alloplast: a pilot study. Quintessence Int 2011; 42: 375-384.
(12) Chawla K, Lamba AK, Faraz F, Tandon S. Evaluation of beta-tricalcium phosphate in human infrabony periodontal osseous defects: a clinical study. Quintessence Int 2011; 42: 291-300.
(13) Dori F, Kovacs V, Arweiler NB, et al. Effect of platelet-rich plasma on the healing of intrabony defects treated with an anorganic bovine bone mineral: a pilot study. J Periodontol 2009; 80: 1599-1605.
Seite 19/27
(14) Nevins M, Giannobile WV, McGuire MK, et al. Platelet-derived growth factor stimulates bone fill and rate of attachment level gain: results of a large multicenter randomized controlled trial. J Periodontol 2005; 76: 2205-2215.
(15) Kitamura M, Akamatsu M, Machigashira M, et al. FGF-2 stimulates periodontal regeneration: results of a multi-center randomized clinical trial. J Dent Res 2011; 90: 35-40.
(16) Mohammadi Z, Dummer PM. Properties and applications of calcium hydroxide in endodontics and dental traumatology. Int Endod J 2011; 44: 697-730.
(17) Willershausen B, Willershausen I, Ross A, Velikonja S, Kasaj A, Blettner M. Retrospective study on direct pulp capping with calcium hydroxide. Quintessence Int 2011; 42: 165-171.
(18) Palmer NO, Ahmed M, Grieveson B. An investigation of current endodontic practice and training needs in primary care in the north west of England. Br Dent J 2009; 206: E22; discussion 584-585.
(19) Chala S, Abouqal R, Rida S. Apexification of immature teeth with calcium hydroxide or mineral trioxide aggregate: systematic review and meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011; 112: e36-42.
(20) Higashi T, Okamoto H. Characteristics and effects of calcified degenerative zones on the formation of hard tissue barriers in amputated canine dental pulp. J Endod 1996; 22: 168-172.
(21) Busenlechner D, Tangl S, Mair B, et al. Simultaneous in vivo comparison of bone substitutes in a guided bone regeneration model. Biomaterials 2008; 29: 3195-3200.
(22) Polat HB, Yeler H, Gumus C, Bulut HE, Kucuk D. Effect of oil-based calcium hydroxide (Osteoinductal) on distraction osteogenesis in rabbit mandible. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009; 107: e30-36.
(23) Schwarz F, Stratul SI, Herten M, Beck B, Becker J, Sculean A. Effect of an oily calcium hydroxide suspension (Osteoinductal) on healing of intrabony periodontal defects. A pilot study in dogs. Clin Oral Investig 2006; 10: 29-34.
(24) Stavropoulos A, Geenen C, Nyengaard JR, Karring T, Sculean A. Oily calcium hydroxide suspension (Osteoinductal) used as an adjunct to guided bone regeneration: an experimental study in rats. Clin Oral Implants Res 2007; 18: 761-767.
(25) Kohal RJ, Hurzeler MB, Schneider SR, Riede UN, Caffesse RG. The effect of a calcium hydroxide paste on wound healing and osseointegration of dental implants. A pilot study in beagle dogs. Clin Oral Implants Res 1997; 8: 375-385.
(26) Kasaj A, Willershausen B, Berakdar M, Tekyatan H, Sculean A. Effect of an oily calcium hydroxide suspension on early wound healing after nonsurgical periodontal therapy. Clin Oral Investig 2006; 10: 72-76.
(27) Stratul SI, Schwarz F, Becker J, Willershausen B, Sculean A. Healing of intrabony defects following treatment with an oily calcium hydroxide suspension (Osteoinductal). A controlled clinical study. Clin Oral Investig 2006; 10: 55-60.
(28) Aparna S, Setty S, Thakur S. Oily calcium hydroxide suspension in the treatment of infrabony periodontal defects: a randomized controlled clinical trial. Quintessence Int 2011; 42: 835-842.
(29) Feres M, Haffajee AD, Allard K, Som S, Goodson JM, Socransky SS. Antibiotic resistance of subgingival species during and after antibiotic therapy. J Clin Periodontol 2002; 29: 724-735.
(30) Wang S, Sasaki Y, Ogata Y. Calcium hydroxide regulates bone sialoprotein gene transcription in human osteoblast-like Saos2 cells. J Oral Sci 2011; 53: 77-86.
(31) Franceschi RT, Ge C, Xiao G, Roca H, Jiang D. Transcriptional regulation of osteoblasts. Ann N Y Acad Sci 2007; 1116: 196-207.
(32) Ganss B, Kim RH, Sodek J. Bone sialoprotein. Crit Rev Oral Biol Med 1999; 10: 79-98. (33) Kasaj A, Willershausen B, Jewszyk N, Schmidt M. Effect of an oily calcium hydroxide
suspension (Osteoinductal) on human periodontal fibroblasts. An in vitro study. Eur J Med Res 2007; 12: 268-272.
(34) Patil AS, Sable RB, Kothari RM. An update on transforming growth factor-beta (TGF-beta): sources, types, functions and clinical applicability for cartilage/bone healing. J Cell Physiol 2011; 226: 3094-3103.
(35) Klass BR, Rolfe KJ, Grobbelaar AO. In vitro flexor tendon cell response to TGF-beta1: a gene expression study. J Hand Surg Am 2009; 34: 495-503.
(36) Smith EL, Colombo JS, Sloan AJ, Waddington RJ. TGF-beta1 exposure from bone surfaces by chemical treatment modalities. Eur Cell Mater 2011; 21: 193-201.
(37) Martelli-Junior H, Cotrim P, Graner E, Sauk JJ, Coletta RD. Effect of transforming growth factor-beta1, interleukin-6, and interferon-gamma on the expression of type I collagen, heat
Seite 20/27
shock protein 47, matrix metalloproteinase (MMP)-1 and MMP-2 by fibroblasts from normal gingiva and hereditary gingival fibromatosis. J Periodontol 2003; 74: 296-306.
(38) Pardo A, Selman M. MMP-1: the elder of the family. Int J Biochem Cell Biol 2005; 37: 283-288.
(39) Jaunberzins A, Gutmann JL, Witherspoon DE, Harper RP. TGF-beta 1 alone and in combination with calcium hydroxide is synergistic to TGF-beta 1 production by osteoblasts in vitro. Int Endod J 2000; 33: 421-426.
(40) de Souza CA, Teles RP, Souto R, Chaves MA, Colombo AP. Endodontic therapy associated with calcium hydroxide as an intracanal dressing: microbiologic evaluation by the checkerboard DNA-DNA hybridization technique. J Endod 2005; 31: 79-83.
(41) Sathorn C, Parashos P, Messer H. Antibacterial efficacy of calcium hydroxide intracanal dressing: a systematic review and meta-analysis. Int Endod J 2007; 40: 2-10.
(42) Kasaj A, Willershausen B, Junker R, et al. Influence of different biomaterials on the viability of Aggregatibacter actinomycetemcomitans. Arch Oral Biol 2011; 56: 917-923.
(43) Uchida Y, Shiba H, Komatsuzawa H, et al. Expression of IL-1 beta and IL-8 by human gingival epithelial cells in response to Actinobacillus actinomycetemcomitans. Cytokine 2001; 14: 152-161.
(44) Ohguchi Y, Ishihara Y, Ohguchi M, et al. Capsular polysaccharide from Actinobacillus actinomycetemcomitans inhibits IL-6 and IL-8 production in human gingival fibroblast. J Periodontal Res 2003; 38: 191-197.
(45) Yamamoto S, Mogi M, Kinpara K, et al. Anti-proliferative capsular-like polysaccharide antigen from Actinobacillus actinomycetemcomitans induces apoptotic cell death in mouse osteoblastic MC3T3-E1 cells. J Dent Res 1999; 78: 1230-1237.
(46) Holt SC, Ebersole JL. Porphyromonas gingivalis, Treponema denticola, and Tannerella forsythia: the "red complex", a prototype polybacterial pathogenic consortium in periodontitis. Periodontol 2000 2005; 38: 72-122.
(47) Potempa J, Pike R, Travis J. Titration and mapping of the active site of cysteine proteinases from Porphyromonas gingivalis (gingipains) using peptidyl chloromethanes. Biol Chem 1997; 378: 223-230.
(48) Yasuhara R, Miyamoto Y, Takami M, et al. Lysine-specific gingipain promotes lipopolysaccharide- and active-vitamin D3-induced osteoclast differentiation by degrading osteoprotegerin. Biochem J 2009; 419: 159-166.
(49) Kato T, Tsuda T, Inaba H, et al. Porphyromonas gingivalis gingipains cause G(1) arrest in osteoblastic/stromal cells. Oral Microbiol Immunol 2008; 23: 158-164.
(50) Karim AY, Kulczycka M, Kantyka T, et al. A novel matrix metalloprotease-like enzyme (karilysin) of the periodontal pathogen Tannerella forsythia ATCC 43037. Biol Chem 2010; 391: 105-117.
(51) Kim M, Jun HK, Choi BK, Cha JH, Yoo YJ. Td92, an outer membrane protein of Treponema denticola, induces osteoclastogenesis via prostaglandin E(2)-mediated RANKL/osteoprotegerin regulation. J Periodontal Res 2010; 45: 772-779.
(52) Scheres N, Laine ML, de Vries TJ, Everts V, van Winkelhoff AJ. Gingival and periodontal ligament fibroblasts differ in their inflammatory response to viable Porphyromonas gingivalis. J Periodontal Res 2010; 45: 262-270.
(53) da Silva RA, Leonardo MR, da Silva LA, de Castro LM, Rosa AL, de Oliveira PT. Effects of the association between a calcium hydroxide paste and 0.4% chlorhexidine on the development of the osteogenic phenotype in vitro. J Endod 2008; 34: 1485-1489.
Legends of figures
Fig. 1 - Attachment and proliferation of HAO cells (mean and SD) after coverage with
different amounts of oily calcium hydroxide suspension (OCHS) as well as Ca(OH)2
and oleum pedum

Seite 21/27
Fig. 2 - Released TGF-β1 (mean and SD) in the supernatants of
osteoblasts after coverage the surface with different amounts of
oily calcium hydroxide suspension (OCHS)
Fig. 3 - Cell mineralization stained with alizarin red one week after seeding HAO
cells. The mineralization is visible by the pink color (), left untreated HAO cells,
right HAO cells seeded on OCHS
Fig. 4 - Attachment and proliferation of PDL fibroblasts (mean and SD) after
coverage with different amounts of oily calcium hydroxide suspension (OCHS) as
well as Ca(OH)2 and oleum pedum
Fig. 5 - Released TGF-β1 and MMP-1 (mean and SD) in the supernatants of PDL
fibroblasts after coverage with different amounts of oily calcium hydroxide
suspension (OCHS)
Fig. 6 - Attachment of HAO and PDL fibroblasts cells (mean and SD) 4 h after
coverage with and without oily calcium hydroxide suspension (OCHS) and addition of
A. actinomycetemcomitans Y4 as well as the combination of P. gingivalis ATCC
33277, T. forsythia ATCC 43037, T. denticola ATCC 35405
Fig. 7 - Attachment and proliferation of HAO cells (mean and SD) 4 h and 48 h after
exposure to supernatants of PDL fibroblasts cultured 8 h on 2 U of oily calcium
hydroxide suspension (OCHS) and infected with addition of A.
actinomycetemcomitans Y4 as well as the combination of P. gingivalis ATCC 33277,
T. forsythia ATCC 43037, T. denticola ATCC 35405
Seite 22/27
0
10
20
30
40
50
60
2 h 4 h 24 h 48 h
Att
ach
ed H
AO
ce
lls /
mm
2
1 U OCHS 2 U OCHS 3 U OCHS Ca(OH)2 Oleum pedum control
p=0.015p=0.004
p=0.007p=0.032
p=0.016
p<0.001
p<0.001
p=0.009
Figure 1

Seite 23/27
p=0.024
p=0.013
p=0.016
Figure 2
Figure 3
Seite 24/27
0
10
20
30
40
50
60
70
2 h 4 h 24 h 48 h
Att
ach
edP
DL
fib
rob
last
s/
mm
2
1 U OCHS 2 U OCHS 3 U OCHS Ca(OH)2 Oleum pedum control
p=0.001
p=0.002
Figure 4

Seite 25/27
600
650
700
750
800
850
900
950
1000
4 h 24 h 48 h
pg/
mL
TGF-β
1
0
100
200
300
400
500
4 h 24 h 48 h
pg/
mL
MM
P-1
1 U OCHS 2 U OCHS 3 U OCHS control
p=0.047
p=0.002p=0.010
p=0.003
p=0.001
p=0.023
p<0.001p<0.001
p<0.001
Figure 5
Seite 26/27
0
10
20
30
40
50
controls A. actinomycetem. P.g., T.f., T.d.
Att
ache
d PD
L fi
bro
blas
ts /
mm
2
no OCHS 2 U OCHS
0
5
10
15
20
25
30
35
controls A. actinomycetem. P.g., T.f., T.d.
Att
ache
d H
AO
cel
ls /
mm
2
p=0.013p=0.003 p=0.017
p=0.015
Figure 6

Seite 27/27
0
5
10
15
20
25
30
35
control A. a. P.g. + T. f. + T. d. control A. a. P.g. + T. f. + T. d.
4 h 48 h
Att
ach
ed H
AO
cel
ls /
mm
2
p=0.013
p=0.001
p=0.001
Figure 7