in traditional societies, death was part of everyday life
TRANSCRIPT

1
Marjo Outila, Marjaana Seppänen, Pilvikki Lantela, Pekka Vasari
Bringing dying back home? – Northern Finns’ end-of-life preparations, concerns and
care preferences and Finnish care policy’s emphasis on care at home1
Abstract
In recent years, Finnish care policy has emphasised that older people should remain at home
for as long as possible. Since the final stages of life and death will theoretically happen more
often in the home, it is important to identify people’s experiences and needs regarding end-of-
life care and dying. The aim of this article is to provide knowledge on these questions from the
perspective of the Northern Finnish people (N=294). Statistical analysis was used with data
gathered from a survey of a random sample. People’s wishes for their end-of-life place and
carers and their end-of-life plans and concerns, are analysed as part of a social and cultural
construction of dying and end-of-life care. The results show that people do have end-of-life
concerns and that they consider end-of-life planning important but that few preparations are
actually made. In many instances, home is regarded as the best place for end-of-life care and
dying, but care institutions are also regarded positively. Reliance on professional care is very
strong, even though people hope to receive care from family members as well. The results are
discussed in the light of Finnish care policy and end-of-life culture.
Keywords: advance care planning, end-of-life care, dying
Introduction
In traditional societies, death was part of everyday life. People prepared for it in the midst of
their everyday lives and died in the places where they had spent their lives (Elias 1985).
However, as societies started to modernize and the service sector began to grow, the last stages
of life were transferred from homes to institutions such as hospitals and care homes. Death
became isolated from everyday life and medicalized (Miettinen 2006).
1 This study is part of a comparative end-of-life care research initiated by Sapporo City University (Kazuyo
Sooudi and Midori Mimaya) and Hokkaido University (Reiko Takeu and Azusa Shikanai) and carried out by the
aforementioned together with the University of Lapland. Supplementary questions were added to the Finnish
questionnaire (e.g. concerning end-of-life preparations) by the Finnish research team (Marjaana Seppänen,
Marjo Outila, Eeva Rossi, Heli Valokivi, Satu Peteri). The analysis of the data was conducted as part of ‘A well-
functioning home care to Lapland - Diverse forms of support to living at home’ project funded by the Finnish
Ministry of Social Affairs and Health. At an early phase of the analysis, help was received from statistics teacher
Marianne Silen (University of Lapland).

2
In recent decades, the orientation of care for older people has changed from institutionalised
care to care given at home. To enable people to live at home for as long as possible is currently
the organizing principle of services in Finland. This became particularly clear in 2013 with a
new ‘Act on Supporting the Functional Capacity of the Older Population and on Social and
Health Services for Older Persons’ (980/2012). From the beginning of 2015, the law was
changed to promote a larger proportion of older adults residing in private homes. As an
outcome of these reforms, it can be anticipated that the final stages of life will more often be
spent at home—and due to the reduction in child mortality and improvements in medical care,
death is most likely to be encountered after a long life in which illness has been part of life
(Luptak 2004; Lloyd 2010).
Dying has mostly been approached as a medical and nursing issue, both in professional practice
and in research (Brown and Walter 2014). As part of this tradition, death has been studied from
the perspectives of the psychological processes experienced (e.g. Kübler-Ross 1969) and the
care needed. The care of older persons has been examined from the perspective of both
caregivers and care receivers in both informal and formal care contexts (e.g. Genet et al. 2011).
As having older people in poor physical health and dying at home becomes a more regular part
of the everyday life of families and home care services, the significance of the subject becomes
greater. Providing information about psychosocial and cultural issues in the context of end-of-
life care and death is a rare but important and growing research area (Donovan et al. 2011; Carr
2012; Bullock 2011; Ko et al. 2013). The understanding of death is culturally bound (Leishman
2009a), and the structures of society and the organization of responsibilities and practices
relating to care define how the last stages of life and death are encountered (Gomes et al. 2011).
Especially important are those practices that relate to the social and health services (Luptak
2004).
Theoretical point of view, research questions, data and method
The aim of this study was to provide knowledge about the end-of-life wishes, concerns, and
preparations of the people of northern Finland as part of their socio-cultural construction of
death and end-of-life care. We analysed our findings in the light of current thinking that
Western culture is in a place where old age, especially the fourth age in which care and end-
of-life issues are central, is culturally rejected and pushed away from normal social life (Higgs
and Gillerad 2015; Elias 1985).
Elias (1985) suggests that we have been distanced from the aging process and from dying. He
writes about the ‘repression’ of death, as one aspect of a more comprehensive movement in
civilisations in which death is pushed more and more behind the scenes of everyday social life.
Many people have difficulty in identifying with aging and death. For the dying, this means
isolation and those close to the dying person often have difficulty in facing the prospect of
death. Death and dying are spoken of less openly and less frequently. Elias writes that people
are forced back onto their own resources, and into their own individual powers of invention, in
dealing with, for example, emotions relating to dying. There are insufficient common
expressions or standardized forms of behaviour to make it easy for people to confront
emotionally challenging situations like dying. (Elias 1985.) Included in the socio-cultural
constructions of old age and dying are perceptions of how we should act in relation to our own
death; how we should prepare for it, and how we wish for or can rely on the help and care of
others when our own death is near. Death as a social construction means that it is defined using
words, concepts and ways of thinking that are available in the individual’s culture; included

3
are ideas of change through time and the differences, for example, between individuals and
social groups (Leishman 2009b; Kastenbaum 1998).
Our research questions are:
• What kind of end-of-life preparations, concerns and care preferences do people have?
• What can be said about the social exclusion of dying when thinking about people’s end-
of-life preparations, concerns and care preferences, and what implications may this
have for care policy and practices?
Our research data consisted of responses from 294 people to a postal survey with a random
sample. The aim of the survey was to gather information related to end-of-life care and dying.2
The survey was sent to 1000 adults older than 20 years living in two cities in northern Finland,
and the data was collected in December 2015. The selection of Rovaniemi and Sodankylä as
the research areas was based on a Japanese-Finnish comparative study design: in both
countries, two northern urban regions that are surrounded by a sparsely populated area were
selected for study. The response rate was 29%. (See Table 2 for detailed information.)
Demographic variables in the survey were age, gender, household size, education, annual
income, self-reported financial security and self-reported health. Probably due to the theme of
the survey, over half of the respondents were 63 years of age or older. As compared to the
general population of the area, respondents were more likely to be older, women, less likely to
be living alone, and having a low income (19 999 euros or less, per household, per year).
The aim of the study was to form an overview of the respondents’ thoughts and opinions;
therefore the data were analysed by using descriptive statistics. The differences among
variables were analysed by bivariate cross-tabulation, and the significance of differences
between groups was evaluated using a chi-square test. Reported p-values were exact (2-sided).
Most research in the area of advanced care planning and end-of-life care is qualitative, using
focus groups and interviews for gathering data (e.g. Bito 2007; Ko and Bergman 2012; Piers
et al. 2013). This study contributes to the literature by using mainly quantitative methods and
targeting a wider age range. Unlike many other studies, this survey did not target the older
generations only, but all adult residents (20 years or older, with a mean of 62 years), and
information was collected randomly rather than recruiting people from clinics or senior centres
(versus Malcomson and Bisbee 2007; Lynn, Curtis and Lagerwey 2016; Brinkman-
Stoppelenburg, Rietjens and van der Heide 2014).
At the end of the survey, respondents were asked to share their thoughts and experiences of
home care, end-of-life care and dying. Eighty-three (28%) shared their thoughts on these topics.
Extracts from these data are used in this article to reveal respondents’ thoughts and feelings.
2 There were 46 questions in the questionnaire, one of which was an open question. Examples of questions:
Have you experienced someone close to you dying? Does thinking about the end-of-life worry you? If it does,
what kind of worries do you have? Where would you like to spend the final stages of your life? From whom
would you like to receive care at the end of life?

4
Ethical issues
The questionnaire and research plan were approved by the University of Lapland research
ethics committee.
Results
End-of-life concerns
‘More than death, I fear ending up in a breathing machine, or the like, lying and withering
with the pain.’
Death causes worries and fears in people’s lives, although the causes of their concerns may
change over time (Elias 1985). In our study, more than half of the respondents had some kind
of end-of-life concerns (Table 1). Respondents were most worried about the family that would
be left behind. The possibility of pain, illnesses and suffering at the end-of-life also caused
concerns. The qualitative study of Fleming et al. (2016) echoes these themes: the participants
were not worried about death itself, but about the dying process and its impact on the persons
who would be left behind. As in our study, the respondents hoped to die quickly and peacefully.
Table 1 Respondents’ end-of-life concerns Thinking of
end-of-life
causes concerns
%
Concern
about death
itself
%
Concern over
family
%
Financial
concerns
%
Regret over
unfinished
things
%
Other
concerns
%
% of all
respondents
57 22.4 37.1 16.7 9.9 10.9
Female
Male
58.2
55.4
p:0.633
ꭓ2(1)=0.237
25.1
19
p:0.256
ꭓ2(1)=1.526
38
35.5
p:0.713
ꭓ2(1)=0.186
14.6
19
p:0.339
ꭓ2(1)=0.993
8.8
11.6
p:0.552
ꭓ2(1)=0.620
11.1
9.9
p:0.848
ꭓ2(1)= 0.106
<63 yrs
≥63 yrs
61.2
53.1
p:0.189
ꭓ2(1)=1.916
23.1
22.5
p:1.000
ꭓ2(1)=0.014
45.4
30.6
p:0,011*
ꭓ2(1)=6.685
13.1
19.4
p:0.157
ꭓ2(1)=2.060
13.8
5.6
p:0,024*
ꭓ2(1)=5.741
9.2
11.9
p:0.568
ꭓ2(1)=0.525
Household
1 person
2 persons 3-6 persons
45.8
56.3 73
p:0,004**
ꭓ2(2)=10.879
20.5
22.9 25
p:0.825
ꭓ2(2)=0.430
19.3
36.8 59.4
p:<0.001***
ꭓ2(2)=24.990
15.7
13.2 23.4
p:0.176
ꭓ2(2)=3.453
7.2
6.9 18.8
p:0,020*
ꭓ2(2)=7.866
10.8
11.1 9.4
p:0.938
ꭓ2(1)=0.145
Financially Secure
Insecure
52
75.4
p:0.001**
ꭓ2(1)=11.494
20
25.7
p:0.398
ꭓ2(1)=1.004
34
47.1
p:0.062
ꭓ2(1)=3.825
9.5
35.7
p:<0.001***
ꭓ2(1)=26.122
8
17.1
p:0,040*
ꭓ2(1)=4.663
9
12.9
p:0.488
ꭓ2(1)=0.857
Annual
income per
household -19 999
20-69 999
50.6
61.8
19
24.7
24.1
45.6
22.8
15.8
8.9
10.8
13.9
10.1

5
70 000- 59.5 p:0.255
ꭓ2(2)=2.719
23.8 p:0.638
ꭓ2(2)=0.988
33.3 p:0,004**
ꭓ2(2)=10.781
7.1 p:0.086
ꭓ2(2)=4.990
11.9 p:0.891
ꭓ2(2)=0.325
11.9 p:0.704
ꭓ2(2)=0.757
*p<0.05
** p<0.01
*** p<0.001
Concerns about family left behind and regret about unfinished issues are less common among
older than younger adults. Younger respondents (under 63, and henceforth referred to as
younger adults) are generally more worried than the older adults (63 or older, and henceforth
referred as older adults), although the difference is not statistically significant.3 Most existing
research suggests that concerns lessen as people age. Fear of death or death anxiety is less
common among older adults than among younger adults (Cicirelli 2006; Chopik 2017; Fortner
and Neimeyer 1999; Russac et al. 2007).
Our study did not confirm the connection between health problems and end-of-life concerns,
which was contrary to other studies that have stressed that poor health and mental health
problems are related to end-of-life concerns (Fortner and Neimeyer 1999; Hofer et al. 2017;
Krause and Hayward 2015). One possible explanation for this is the low number of respondents
who reported ill health.
Social support and being married can buffer fear of death (Chopik 2017; Hofer et al. 2017;
Azeem and Naz 2015), but in our data, there was no significant difference regarding fear of
death and dying between those who lived alone and those who lived with a partner or family
members. However, respondents from bigger households were generally more worried than
those living alone. Age mediated this result: 82.8% of people living in 3–6 person households
were under 63. Unsurprisingly, respondents from bigger households were also more worried
about family members than those living alone, and they had more regrets over unfinished
issues. Additionally, our research suggests that financial insecurity has an impact on people’s
end-of-life concerns. People who reported themselves to be financially insecure had more
concerns generally, both financial and regrets about unfinished issues. There was no difference
in end-of-life concerns between the women and men in our study. Previous studies show
contradictory results regarding the effect of gender on death anxiety (French, Greenauer and
Mello 2017; Azeem and Naz 2015; Hofer et al. 2017; Fortner and Neimeyer 1999; Neimeyer
et al. 2011; Russac et al. 2007).
Surprisingly, our study pointed out a negative connection between end-of-life concerns and
preparations. One fourth of those with end-of-life concerns and 34% of those without concerns
had made end-of-life preparations. These results were only tentative (p: 0.118), and a similar
connection between concerns and the completion of an advance directive was not found. Do
concerns limit people’s ability or willingness to prepare?
End-of-life preparations
‘I have made a living will. They are not going to keep me alive by force with tubes and with
heavy pain medication.’
3The age groups were divided (<63 yrs and ≥63 yrs) based on the fact that 63 is a common retirement
age in Finland.
6
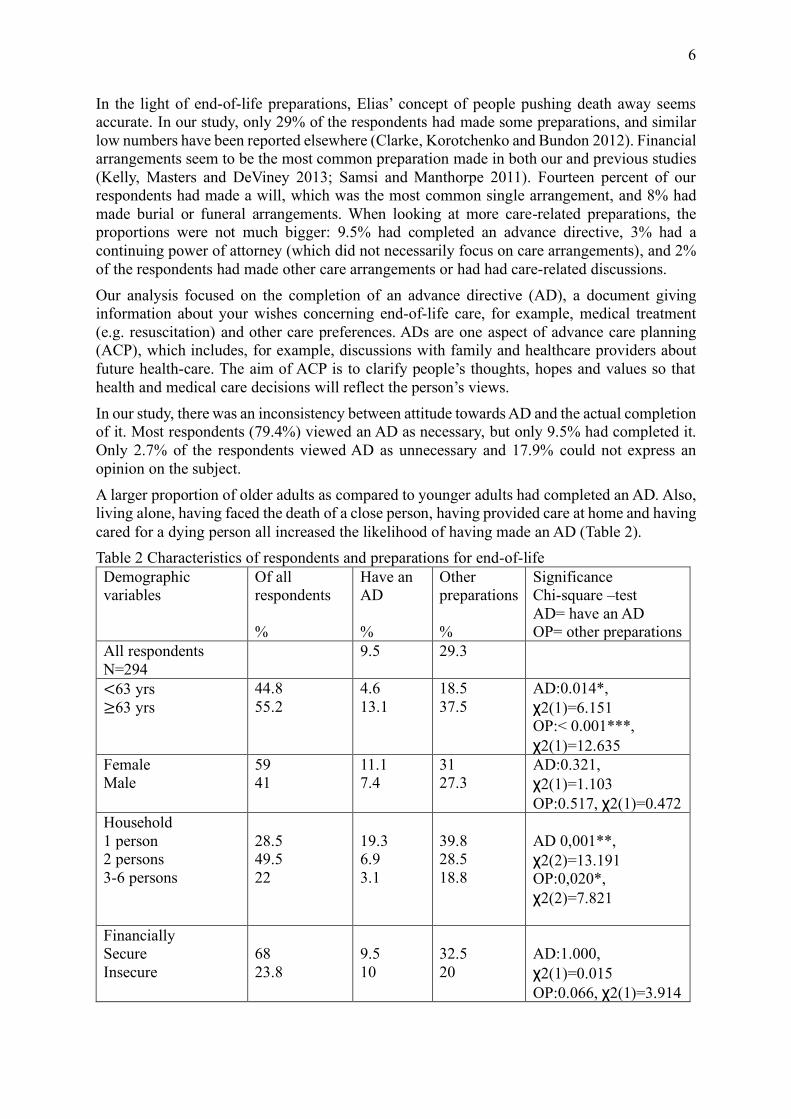
In the light of end-of-life preparations, Elias’ concept of people pushing death away seems
accurate. In our study, only 29% of the respondents had made some preparations, and similar
low numbers have been reported elsewhere (Clarke, Korotchenko and Bundon 2012). Financial
arrangements seem to be the most common preparation made in both our and previous studies
(Kelly, Masters and DeViney 2013; Samsi and Manthorpe 2011). Fourteen percent of our
respondents had made a will, which was the most common single arrangement, and 8% had
made burial or funeral arrangements. When looking at more care-related preparations, the
proportions were not much bigger: 9.5% had completed an advance directive, 3% had a
continuing power of attorney (which did not necessarily focus on care arrangements), and 2%
of the respondents had made other care arrangements or had had care-related discussions.
Our analysis focused on the completion of an advance directive (AD), a document giving
information about your wishes concerning end-of-life care, for example, medical treatment
(e.g. resuscitation) and other care preferences. ADs are one aspect of advance care planning
(ACP), which includes, for example, discussions with family and healthcare providers about
future health-care. The aim of ACP is to clarify people’s thoughts, hopes and values so that
health and medical care decisions will reflect the person’s views.
In our study, there was an inconsistency between attitude towards AD and the actual completion
of it. Most respondents (79.4%) viewed an AD as necessary, but only 9.5% had completed it.
Only 2.7% of the respondents viewed AD as unnecessary and 17.9% could not express an
opinion on the subject.
A larger proportion of older adults as compared to younger adults had completed an AD. Also,
living alone, having faced the death of a close person, having provided care at home and having
cared for a dying person all increased the likelihood of having made an AD (Table 2).
Table 2 Characteristics of respondents and preparations for end-of-life
Demographic
variables
Of all
respondents
%
Have an
AD
%
Other
preparations
%
Significance
Chi-square –test
AD= have an AD
OP= other preparations
All respondents
N=294
9.5
29.3
<63 yrs
≥63 yrs
44.8
55.2
4.6
13.1
18.5
37.5
AD:0.014*,
ꭓ2(1)=6.151
OP:< 0.001***,
ꭓ2(1)=12.635
Female
Male
59
41
11.1
7.4
31
27.3
AD:0.321,
ꭓ2(1)=1.103
OP:0.517, ꭓ2(1)=0.472
Household
1 person
2 persons
3-6 persons
28.5
49.5
22
19.3
6.9
3.1
39.8
28.5
18.8
AD 0,001**,
ꭓ2(2)=13.191
OP:0,020*,
ꭓ2(2)=7.821
Financially
Secure
Insecure
68
23.8
9.5
10
32.5
20
AD:1.000,
ꭓ2(1)=0.015
OP:0.066, ꭓ2(1)=3.914

7
Annual income per
household
-19 999
20 000-69 999
70 000-
28.3
56.6
15.1
10.1
11.4
-
26.6
32.3
21.4
AD:0.074,
ꭓ2(2)=5.181
OP:0.340, ꭓ2(2)=2.217
Education
Basic
Vocational/secondary
Higher/university
25.8
36.6
37.6
10.8
10.5
7.4
32.4
19
36.1
AD:0.691,
ꭓ2(2)=0.819
OP:0,018*,
ꭓ2(2)=8.139
Self-rated health
Good
Bad
82.1
17.9
7.6
14.3
28
32.7
AD:0.160,
ꭓ2(1)=2.280
OP:0.602, ꭓ2(1)=0.425
Experience of death
of a loved one
Experience
No experience
Child
Sibling
Spouse
Friend
92.9
7.1
5.8 (17)
22.1 (65)
14.3 (42)
18.4 (54)
9.5
9.5
17.6 (3)
16.9 (11)
19 (8)
16.7 (9)
30
19
47.1 (8)
36.9 (24)
42.9 (18)
29.6 (16)
AD:1.000,
ꭓ2(1)=0,000
OP:0.332, ꭓ2(1)=1.138
AD:0.386,
ꭓ2(1)=1.382
OP:0.106, ꭓ2(1)=2.765
AD:0.030*,
ꭓ2(1)=5.302
OP:0.164, ꭓ2(1)=2.373
AD:0.041*,
ꭓ2(1)=5.158
OP:0.044*,
ꭓ2(1)=4.383
AD:0.069,
ꭓ2(1)=3.917
OP:1.000, ꭓ2(1)=0.005
Experience in
providing care at
home
Experience
No experience
45.2
54.8
13.5
6.2
30.8
28
AD:0,045*,
ꭓ2(1)=4.532
OP:0.608, ꭓ2(1)=0.291
Providing care for a
dying person
Experience
No experience
Professional
experience
Informal experience
34.8
65.2
11.5
20.2
15
6.4
18.2
13.8
35
26.2
24.2
39.7
AD:0.021*,
ꭓ2(1)=5.632
OP:0.135, ꭓ2(1)=2.436
Numbers in brackets in the second column refer to the number of persons.
*p<0.05
** p<0.01
*** p<0.001

8
End-of-life issues may seem somewhat redundant for younger people in a society where death
is far from everyday life. One of the respondents wrote: ‘At the age of 27 it is difficult to think
about the end of life period’. When people get older, the probability of facing the death of a
family member or a friend increases, thus the probability of facing end-of-life care issues
increases as well. As a result of this, it is more likely that people will come to think about their
own end-of-life and perhaps make some arrangements for that. Our study reinforces the results
of earlier studies on the effect of age: older adults’ ACP exceeds the arrangements of younger
adults. The statistical significance is stronger in other arrangements than in AD. Usually, ACP
increases with age, but there are exceptions (Ke et al. 2017; Kelly, Masters and DeViney 2013;
Lynn, Curtis and Lagerwey 2016; Shapiro 2015).
In the light of our study, living alone affects ACP. People who live in one-person households,
especially older people, have more often made an AD and other end-of-life arrangements. This
result parallels that of other studies. People who live alone with no relatives have a tendency
to plan more than others. They may have no one who is eligible to act as their surrogates so
they feel the need to plan ahead for themselves. (Samsi and Manthorpe 2011; Carr and
Khodyakov 2007; Piers et al. 2011.)
Our analysis points in the direction that experiencing the loss of spouse, friend, child or sibling
increases the likelihood of making an AD. Also, experience in providing care at home or for a
dying person, especially in a professional setting, increases the likelihood of making an AD. It
seems that close encounters with death prompt people to plan their own end-of-life. More
research is needed to confirm these results, but according to existing research, facing the death
of a close person increases the likelihood of making an AD (Carr and Khodyakov 2007; Piers
et al. 2011; Kelly, Masters and DeViney 2013).
Prior studies have pointed out that people’s health, education (contra Khosla, Curl and
Washington 2016) and socioeconomic status also affect ACP. People with a poorer health status
(Ke et al. 2017; Ko, Lee and Hong 2016; Lovell and Yates 2014), recent hospitalizations (Carr
and Khodyakov 2007; Ke et al. 2017), or living in a care institution (Lynn, Curtis and Lagerwey
2016) are more likely to complete ADs. Analysis of our data indicated similar results, but
because of the small proportion of people in our study who reported having trouble with their
health, the analysis is only tentative. Contrary to other findings, our study did not affirm the
impact of female gender (Ke et al. 2017; Lynn, Curtis and Lagerwey 2016), higher income
level (Lynn, Curtis and Lagerwey 2016; Shapiro 2015; Khosla, Curl and Washington 2016) or
higher educational level (Kelly, Masters and DeViney 2013; Lynn, Curtis and Lagerwey 2016)
on greater engagement with ACP. Higher education seems to have some effect on other
arrangements, but not on AD. However, economic security had some effect on making
arrangements other than completing an AD. Those who felt financially secure had more often
made end-of-life arrangements than those who felt financially insecure, although the difference
was not statistically significant.4
Despite the generally positive attitude towards AD (Table 2), advance care planning is still
quite rare (see also Ko and Berkman 2012). Prior research has found several reasons for this
that seem to be in line with Elias’ (1985) concepts involving the absence and subsequent
rejection of death and old age in everyday life. ACP is seen as unpleasant and hostile (Jeong,
4 According to previous studies (e.g. Bullock 2011; Ko and Berkman 2012) religion and cultural or ethnic
background also impact ACP. Our survey did not cover those aspects.

9
Higgins and McMillan 2011), fearsome or upsetting (Malcomson and Bisbee 2009), a thing
that has not even come into one’s mind, a thing for which the time has not yet come (Simon et
al. 2015), something that does not need to be done or else is ineffective (Brinkman-
Stoppelenburg, Rietjens and van der Heide 2014; Ke et al. 2017).
There is research evidence that questions the effectiveness of ADs (Shapiro 2015) but there is
also evidence for the positive effects of ACP, even though not actualized as planned (Sudore
and Fried 2010). It has been said that ACP leads to a different level of appreciation of one’s
personal entity and transcendence (Jeong, Higgins and McMillan 2011), while also giving
doctors an increased level of knowledge regarding their patients’ wishes. Existing research
suggests that people usually need support in order to make an ACP (Simon, Porterfield and
Raffin 2015; Malcomson and Bisbee 2009; Lovell and Yates 2014). It seems that some older
people are ready to discuss end-of-life issues and make end-of-life plans but that the
opportunities to do so are lacking (Malcomson and Bisbee 2009; Ko, Lee and Hong 2016;
Sharp et al. 2013). In order for the support to be effective, it must consist of information with
concerted action, or interactive and informative interventions (Jeong, Higgins and McMillan
2011; Ko, Lee and Hong 2016; Freytag and Rauscher 2017).
In our study, the overall proportion of people that had made end-of-life preparations (Table 2)
seemed small compared to the concerns that people reported (Table 1). People do have end-of-
life concerns, they feel the need to plan their care, but few preparations are made.
Preferences for place of end-of life care
‘If I were in my right mind and could move about relatively well, I would absolutely live at
home the final stage. But if I had dementia, were paralyzed, all drugged up, or otherwise a so-
called “difficult” case, there’s no way I would like to be in home care – the family would
probably suffer too.’
Some of the most central issues in end-of-life care are wishes regarding end-of-life place and
carers. More than half of the respondents in our study preferred to spend their end-of-life period
at home (Table 3). Prior research shows that home is usually the place where people prefer to
receive end-of-life care (Choi et al. 2010) and die (Beccaro et al. 2006; Choi et al. 2010). The
proportion of people choosing home over an institution varies, but commonly it is well over 50
percent (Hunt, Shlomo and Addington-Hall 2014a; Hunt, Shlomo and Addington-Hall 2014b;
Gott et al. 2004; Hoare et al. 2015; Gomes et al. 2013).
Table 3 Respondents’ preferences for place at the end-of-life
Home % Hospital % Care home
%
Hospice % Significance
%
All 57 4 24.2 14.8
Female
Male
53.5
61.2
4.4
3.4
22.6
26.7
19.5
8.6
p:0.083
ꭓ2(3)=6.643
<63 yrs
≥63 yrs
73.2
44
-
7.3
17.1
30
9.8
18.7
p:<0.001***
ꭓ2(3)=27.417
Household
1 person
44
6.7
29.3
20
p:0.004**

10
2 persons
3-6 persons
53.7
77.8
4.4
-
25
17.5
16.9
4.8 ꭓ2(6)=19.207
Self-reported health
Good
Bad
62.6
40.8
3.3
6.1
19.4
36.7
14.7
16.3
p:0.024*
ꭓ2(3)=9.347
Annual income per
household
-19 999
20-69 999
70 000-
48.6
58.4
75.6
7.1
2.6
2.4
30
24
7.3
14.3
14.9
14.6
p:0.059
ꭓ2(6)=12.051
Education
Basic
Vocational/secondary
Higher/university
41.8
61.4
63.1
7.5
4
1.9
40.3
16.8
20.4
10.4
17.8
14.6
p:0.005**
ꭓ2(6)=18.404
*p<0.05
** p<0.01
*** p<0.001
In our study, the biggest difference in place preference was between the age groups. Older
adults preferred an institution more often than younger adults. Prior research has shown diverse
results for the effect of age. Sometimes, older age groups prefer home as the place of death
more than younger people (Gomes and Higginson 2008; Sanjo et al. 2007), but sometimes it is
the other way around (Foreman et al. 2006). Previous research also points out that the preferred
place for end-of-life care might differ from the preferred place for dying. Even though people
may not prefer to have care at home, they may prefer to die at home (Aoun and Skett 2013).
Another significant variable was household size: people living alone preferred an institution
over home more often than people living with others (see also Iecovich, Carmel and Bachner
2009). Aoun and Skett’s study (2013) with terminally-ill people who lived alone reveals that
home may not always be the preferred location for end-of-life care or death. It may be that
people who live alone prefer care institutions because they do not think it will possible to rely
on professional care at home to the extent that living at home would be possible in the absence
of a spouse, children or other informal caregivers. In accordance with Aoun and Skett’s
research (2013), health also affected respondents’ preferences: less than half of the respondents
who reported ill health chose home for their end-of-life place. Of the healthy respondents, over
sixty percent chose home. Some expressed firmly their desire to stay in an institution if the
circumstances were rough: ‘If I get a memory sickness, I, at least, hope to get to a place where
there is around-the-clock surveillance. In the final stage of cancer, [I would choose] terminal
care in a hospital or in hospice if there is one.’
Cross-tabulation of age, size of household and preferred end-of-life place confirmed that age
is a stronger predictor of preference for an institution than household size: among all the
household categories, over half of the older adults preferred institutions. Among younger
adults, it was the other way around: regardless of the household size, over half preferred home.
Educational background and economic situation are, to some extent, also connected with
preference: a larger percentage of respondents with a lower annual income and lower education
preferred an institution over the home. The difference was significant only for educational
background. It is to be noted that 81.9% of the respondents with basic education only were
older adults. Self-reported financial security did not affect preferences. In our study, there were

11
no differences between genders, in contrast to, for example, the studies of Choi et al. (2010)
and Foreman et al. (2006) in which men preferred end-of-life care and dying at home more
often than women did.
The issues that respondents raised in their responses dealt with the challenges of living at home,
such as loneliness and lack of safety, but also the possibility of making one’s own choices in
one’s own home. In spite of the general desire to spend the end-of-life at home, being at home
raised mixed thoughts and feelings. Over 80% of the respondents would, to some extent, be
happy if their family took care of them. At the same time, over 60% felt that they would be a
burden on their families.
A theme frequently commented on in the responses was the state of professional care. People
were worried that the resources for home care were insufficient and that there was a lack of
psychosocial support and pain relief. Comments on the care received in hospitals, care homes
and hospices were twofold: on one hand, people were very pleased, for example, with the care
their family members had received, but on the other hand, they were very critical of the way
that people were treated and left alone. It is worth noting that the perception of providing care
at home was related to the wish to remain at home until the end of life. A bigger proportion
(76.8%) of those who wanted to remain at home had a good picture of home care than those
people who wished to spend their end-of-life in a care institution (60.9%) (p:0.005,
ꭓ2(1)=7.952).
Researchers have pointed out the inconsistency between the wish to die at home and the actual
number of deaths occurring in institutions (Hunt, Shlomo and Addington-Hall 2014a; Bell,
Somogyi-Zalud and Masaki 2009). The percentage of people dying in institutional settings is
still high in Finland (according to Aaltonen [2015], 85.5% died in institutions in 2008) and in
Europe, but there does seem to be a decreasing trend towards choosing a hospital death in
Western societies (Houttekier et al. 2011; Gomes, Calanzani and Higginson 2011; Flory et al.
2004). However, despite the growing trend towards the support of home care, the relatively
large proportion of people still preferring formal care in an institutional setting should not be
dismissed.
People have different preferences for their end-of-life place, thus the heterogeneity of
individual wishes should be acknowledged. Existing research stresses that there is a general
lack of knowledge regarding people’s preferences. This confirms Elias’ (1985) notion of the
exclusion of death and end-of-life issues: end-of-life and dying are difficult topics to discuss.
This causes problems in achieving a good quality ACP, for people’s well-being and for the
actualization of their preferences (Badrakalimuthu and Barclay 2014; Raz, Shalev and Amit
2011; Hunt, Shlomo and Addington-Hall 2014a). Therefore, the starting point for a good ACP
should be an awareness of the person’s wishes and the way that they feel about care, for
example the sharing of care responsibilities between family members.
Preferences for end-of-life carers
‘What scares me most in aging is that I don’t have any children. Who will truly attend to my
interests when I am dependent on others’ help?’
In addition to end-of-life place preferences, respondents were asked about their carer
preferences. The carers most preferred were health care professionals; the next most preferred
carers were spouse and children (Table 4).

12
Table 4 Respondents’ preferences for end-of life carers
Demographic
variables
Health care
professionals
%
Spouse
%
Daughter
%
Son
%
Friend
%
All
respondents
77.6 54.8 38.1 35.4 9.9
Female
Male
78.9
75.2
p:0.480
ꭓ2(1)=0.567
48.5
63.6
p:0,012*
ꭓ2(1)=6.521
40.4
34.7
p:0.392
ꭓ2(1)=0.957
39.2
29.8
p:0.107
ꭓ2(1)=2.759
14
4.1
p:0.005**
ꭓ2(1)=7.768
<63 yrs
≥63 yrs
80.8
75.6
p:0.321
ꭓ2(1)=1.104
63.8
48.1
p:0,009**
ꭓ2(1)=7.167
39.2
36.9
p:0.716
ꭓ2(1)=0.169
36.9
33.8
p:0.621
ꭓ2(1)=0.317
16.2
4.4
p:0.001**
ꭓ2(1)=11.408
Household
1 person
2 persons
3-6 persons
72.3
78.5
84.4
p:0.210
ꭓ2(2)=3.113
21.7
66
70.3
p:<0.001***
ꭓ2(2)=50.093
36.1
34
50
p:0.082
ꭓ2(2)=4.988
36.1
27.8
51.6
p:0.004**
ꭓ2(2)=10.990
10.8
6.3
17.2
p:0.054
ꭓ2(2)=6.007
Annual
income per
household
-19 999
20 - 69 999
70 000-
68.4
80.4
85.7
p:0.044*
ꭓ2(2)=6.208
38
62
71.4
p:<0.001***
ꭓ2(2)=16.812
32.9
38.6
38.1
p:0.699
ꭓ2(2)=0.763
26.6
38
35.7
p:0.208
ꭓ2(2)=3.066
10.1
10.1
11.9
p:0.962
ꭓ2(2)=0.121
*p<0.05
** p<0.01
*** p<0.001
The responses reflect a strong reliance on professional care and a mindset in which the roles of
family members and formal caregivers are clearly separated: ‘I think that I would feel safer in
the care of professionals who have familiarized themselves with palliative care, in a home-like
environment; loved ones and family members by my side as friends, not as my carers.’ It seems
that people expect society to take care of its members: ‘Society cannot expect family or friends
to accept taking care of the end-of-life care. They have their own life.’ Even though the majority
of the respondents preferred to have health care professionals as their carers, there was also
distrust towards them. For example one of the respondents wrote: ‘The alternative [to staying
at home] is the current lying drugged up and abandoned in a hospital ward or lying in your own
waste in a commercial elderly home.’
Despite the preference for professional care, over half also preferred a spouse and about one-
third a child as a caregiver. Men, more often than women, wished to receive care from their
spouse. This was an exception to our otherwise fairly gender neutral results. In addition to a
bigger proportion of males, younger adults, people living in bigger households and people with
a higher income wished for their spouse to be their caregiver.

13
The preferences and comments of respondents can be interpreted as part of the
institutionalization and medicalization of end-of-life care: dying in hospitals and care homes
in the care of health care professionals is familiar. This is accompanied by individualization
and an emphasis on individuals’ independence: receiving care from family members is not an
obvious preference (Elias 1985).
Discussion
Kastenbaum (1995) (cited in Cicirelli 2006, p.39) refers to the death system of each culture,
meaning the people, places, objects, symbols and times that are related to death and dying. In
the light of this study, the Finnish death system is strongly linked to health care professionals
and formal institutions. There is a strong reliance on formal care, and death is hidden away in
institutions such as hospitals and care homes. On the other hand, death-related issues are
connected to the closest family members. People worry about and to some extent hope for care
from their family members, but there is lack of discussion in families involving planning for
end-of-life care and dying. Preparing for the end-of-life is viewed as an appropriate thing in
itself, but in reality few make tangible preparations, despite their concerns related to death and
end-of-life care. These results reflect Elias’ (1985) notion of ageing and dying being pushed
behind the social scene and away from everyday life, with an absence of readily used
expressions and practices that would help people deal with end-of-life issues.
Changes in the political governance of end-of-life care are about to introduce change into the
system for dealing with death in Finland. What kind of cultural change will they bring? Will
they take into account the fears and concerns that people have towards dying and end-of-life
care? Will they support people in vulnerable situations who have different concerns, poor health
or financial struggles, all of which can make facing death harder, and who feel more need for
support than the average person?
The implications of our study are two-fold for care policy: First, the concerns that people have
in relation to end-of-life suggest that there is a need for support in completing ACPs. People
feel the need to plan but the lack of readily accessible practices to complete an ACP leads to
the situation where for many people it is left undone. The suggestion that there should be
increased ACP planning is supported by existing research which provides evidence for its
usefulness. ACP planning increases the probability of making people’s end-of-life preferences
known and respected (although this is not always possible), and the ACP has the potential to
increase the well-being of people who engage with it (Hunt, Shlomo and Addington-Hall
2014a).
From the perspective of social and health care development, it should be noted that the support
people have in their end-of-life planning comes, most frequently, from lawyers and financial
planners (Simon, Porterfield and Raffin 2015; Malcomson and Bisbee 2009). However, people
have other concerns in addition to financial ones, and for these it may be that social and health
care professionals are the natural source of support. The development of Western societies has
led to a situation where people face death relatively alone, and in places where they are unable
to avoid the experience (Elias 1985). The need for support may continue to grow if the direction
of social development continues as it is. In Finland, there are signs of change: for example,
there is a growing interest in integrating ACP into older adults’ care services.

14
Our second suggestion relates to the fairly large consensus that home is the best place to live,
to receive care and to die (see e.g. Sepperd, Wee and Strauss 2011; Jeppson-Grassman and
Whitaker 2007). Our analysis suggests that there is a need to investigate more closely the risks
of pushing this idea further. Even though many people want to spend their end-of-life at home,
according to our study, this wish is not entirely evident. In some life situations, people clearly
prefer institutional settings for their end-of-life care, while those people who do wish to stay at
home as long as possible still have a strong need for and reliance on formal care. These results
suggest that people’s preferences may differ significantly from political care guidelines that are
increasingly stressing informal care (Heikkinen 2017). The risks of isolation, loneliness,
insecurity and excessive pressure on families must be noted.
References
Aaltonen, M. (2015) Patterns of care in the last two years of life. Care transitions and places
of death of old people. Acta Electronica Universitatis Tamperensis 1588. Tampere: Tampere
University Press.
Aoun, S.M., & Skett, K. (2013) A longitudinal study of end-of-life preferences or terminally-
ill people who live alone. Health and Social Care in the Community, 21, 530–535 (2013).
doi:10.1111/hsc.12039.
Azeem, F., & Naz, M.A. (2015) Resilience, death anxiety, and depression among
institutionalized and noninstitutionalized elderly. Pakistan Journal of Psychological Research,
30(1), 111–130.
Badrakalimuthu, V., & Barclay, S. (2014) Do people with dementia die at their preferred
location of death? A systematic literature review and narrative synthesis. Age and Ageing, 43,
13–19 (2014). doi:10.1093/ageing/aft151.
Beccaro, M., Costantini, M., Rossi P. G., Miccinesi G., Grimaldi M., Bruzzi, P. (2006) Actual
and preferred place of death of cancer patients. Results from the Italian survey of the dying of
cancer (ISDOC). Journal of Epidemiology and Community Health, 60, 412–416 (2006).
doi:10.1136/jech.2005.043646.
Bell, C.L., Somogyi-Zalud, E., Masaki, K.H. (2009). Methodological review: measured and
reported congruence between preferred and actual place of death. Palliative Medicine, 23, 482–
490 (2009). doi:10.1177/0269216309106318.
Bito, S., Matsumura, S., Singer, M.K., et al. (2007). Acculturation and end-of-life decision
making: comparison of Japanese and Japanese-American focus groups. Bioethics, 21, 251–
262 (2007). doi:10.1111/j.1467-8519.2007.00551.x
Brinkman-Stoppelenburg, A., Rietjens, J.A., Van Der Heide, A. (2014). The effects of advance
care planning on end-of-life care: A systematic review. Palliative Medicine, 28, 1000–1025
(2014). doi:10.1177/0269216314526272.
Brown, L., & Walter, T. (2014). Towards a social model of end-of-life care. British Journal of
Social Work, 44, 2375–2390 (2014). doi:10.1093/bjsw/bct087.

15
Bullock, K. (2011). The influence of culture on end-of-life decision making. Journal of Social
Work in End-of-Life & Palliative Care, 7, 83–98 (2011). doi:10.1080/15524256.2011.548048.
Carr, D., & Khodyakov, D. (2007). End-of-life health care planning among young-old adults:
An assessment of psychosocial influences. The Journals of Gerontology Series B:
Psychological Sciences and Social Sciences, 62, S135–S141 (2007).
doi:10.1093/geronb/62.2.S135.
Carr, D. (2012). Racial and ethnic differences in advance care planning: identifying subgroup
patterns and obstacles. Journal of Aging and Health, 24, 923–947 (2012).
doi: 10.1177/0898264312449185.
Choi, J., Miyashita, M., Hirai, K., Sato, K., Morita, T., Tsuneto, S., Shima, Y. (2010).
Preference of place for end-of-life cancer care and death among bereaved Japanese families
who experienced home hospice care and death of a loved one. Supportive Care in Cancer, 18,
1445–1453 (2010). doi:10.1007/s00520-009-0767-3.
Chopik, W.J. (2017). Death across the lifespan: Age differences in death-related thoughts and
anxiety. Death studies 41, 69–77 (2017). doi:10.1080/07481187.2016.1206997.
Cicirelli, V.G. (2006). Older adult’s views on death. New York: Springer.
Clarke, L.H., Korotchenko, A., Bundon, A. (2012). 'The calendar is just about up': older adults
with multiple chronic conditions reflect on death and dying. Ageing and Society, 32, 1399–
1417 (2012). doi:10.1017/S0144686X11001061.
Donovan, R., Williams, A., Stajduhar, K., Brazil, K., Marshall, D. (2011). The influence of
culture on home-based family caregiving at end-of-life: A case study of Dutch reformed family
care givers in Ontario, Canada. Social Science & Medicine, 72, 338–346 (2011).
doi:10.1016/j.socscimed.2010.10.010.
Elias, N. (1985) The loneliness of dying (trans: Jephcott E.) New York: Blackwell.
Fleming, J., Farquhar, M., Cambridge City over-75s Cohort (CC75C) study
collaboration, Brayne, C., Barclay S. (2016). Death and the Oldest Old: Attitudes and
Preferences for End-of-Life Care - Qualitative Research within a Population-based Cohort
Study. PLoS One. doi: 10.1371/journal.pone.0150686.
Flory, J., Yinong, Y.X., Gurol, I., Levinsky, N., Ash, A., Emanuel, E. (2004). Place of death:
U.S. trends since 1980. Health Affairs, 23(3), 194–200.
Foreman, L.M., Hunt, R.W., Luke, C.G., Roder, D.M. (2006). Factors predictive of preferred
place of death in the general population of South Australia. Palliative Medicine, 20, 447–453
(2006). doi:https://doi.org/10.1191/0269216306pm1149oa.
16
Fortner, B.V., & Neimeyer, R. (1999). Death anxiety in older adults: a quantitative review.
Death Studies, 23, 387–411 (1999). doi:10.1080/074811899200920.
French, C., Greenauer, N., & Mello, C. (2017). A multifactorial approach to predicting death
anxiety: assessing the role of religiosity, susceptibility to mortality cues, and individual
differences. Journal of social work in end-of-life & palliative care, 13(2-3), 151–172.
doi:10.1080/15524256.2017.1331181.
Freytag, J., & Rauscher, E.A. (2017). The importance of intergenerational communication in
advance care planning: generational relationships among perceptions and beliefs. Journal of
Health Communication, 22, 488–496 (2017). doi:10.1080/10810730.2017.1311971.
Genet, N., Boerma, W.G.W., Kringos, D.S., Bouman, A., Francke, A.L, Fagerström C. et al.
(2011). Home care in Europe: a systematic literature review. BMC Health Service Research.
30,11, 207. doi:10.1186/1472-6963-11-207.
Gomes, B., & Higginson, I.J. (2008). Where people die (1974-2030): past trends, future
projections and implications for care. Palliative Medicine, 22, 33–41 (2008).
doi:10.1177/0269216307084606.
Gomes, B., Calanzani, N., Higginson, I.J. (2011). Reversal of the British trends in place of
death: time series analysis 2004-2010. Palliative Medicine, 26, 102–107 (2011).
doi:10.1177/0269216311432329.
Gomes, B., Calanzani, N., Gysels, M., Hall, S., Higginson, I.J. (2013). Heterogeneity and
changes in preferences for dying at home: a systematic review. BMC Palliative Care,
doi:10.1186/1472-684X-12-7.
Gott, M., Seymour, J., Bellamy, G., Clark, D., Ahmedzai, S. (2004). Older people's views about
home as a place of care at the end of life. Palliative Medicine, 18, 460–467 (2004).
doi:10.1191/0269216304pm889oa.
Heikkinen, A. (2017). Kuoleman kohtaamisen paikka. Master’s thesis. Social work.
Rovaniemi: University of Lapland.
Higgs P. & Gilleard C. (2015) Rethinking Old Age. Theorising the Fourth Age. London:
Palgrave Macmillan.
Hoare, S., Morris, S.Z., Kelly, M.P., Kuhn, I., Barclay, S. (2015). Do patients want to die at
home? A systematic review of the UK literature, focused on missing preferences for place of
death. Plos one. doi: 10.1371/journal.pone.0142723.
Hofer, J., Busch, H., Šolcová, I.P., Tavel, P. (2017). Relationship between subjectively
evaluated health and fear of death among elderly in three cultural contexts. International
Journal of Aging & Human Development, 84, 343–365 (2017).
doi:10.1177/0091415016685331.
Houttekier, D., Cohen, J., Surkyn, J., Deliens, L. (2011). Study of recent and future trends in
place of death in Belgium using death certificate data: a shift from hospitals to care homes.
BMC Public Health. doi:10.1186/1471-2458-11-228.

17
Hunt, K.J., Shlomo, N., Addington-Hall, J. (2014a). End-of-life care and achieving preferences
for place of death in England: Results of a population-based survey using the VOICES-SF
questionnaire. Palliative Medicine, 28, 412–421 (2014). doi:10.1177/0269216313512012.
Hunt, K.J., Shlomo, N., Addington-Hall, J. (2014b). End-of-life care and preferences for
place of death among the oldest old: Results of a population-based survey using
VOICES-Short Form. Journal of Palliative Medicine, 17, 176–182 (2014).
doi:10.1089/jpm.2013.0385
Iecovich, E., Carmel, S., Bachner, Y.G. (2009). Where they want to die: correlates of elderly
persons' preferences for death site. Social Work in Public Health, 24, 527–542 (2009).
doi:10.1080/19371910802679341.
Jeong, S.Y., Higgins, I., McMillan, M. (2011). Experiences with advance care planning: older
people and family members’ perspective. International Journal of Older People Nursing, 6(3),
176–186.
Jeppson-Grassman, E. & Whitaker, A. (2007). End of life and dimensions of civil society: The
Church of Sweden in a new geography of death. Mortality, 12, 261–280 (2007).
doi:10.1080/13576270701430635.
Kastenbaum, R.J. (1998). Death, Society, and Human Experience. New York: Routledge.
Ke, L.-S., Huang, X., Hu, W.-Y., O’Connor, M., Lee, S. (2017). Experiences and perspectives
of older people regarding advance care planning: A meta-synthesis of qualitative studies.
Palliative Medicine, 31, 394–405 (2017). doi:10.1177/0269216316663507.
Kelly, C.M., Masters, J.L., DeViney, S. (2013). End-of-life planning activities: an integrated
process. Death Studies, 37, 529–551 (2013). doi:10.1080/07481187.2011.653081
Khosla, N., Curl, A.L., Washington, K.T. (2016). Trends in engagement in advance care
planning behaviors and the role of socioeconomic status. The American Journal of Hospice
and Palliative Care. 33, 651–657 (2016). doi: 10.1177/1049909115581818.
Ko, E. & Berkman, C.S. (2012). Advance directives among Korean American older adults:
knowledge, attitudes, and behavior. Journal of Gerontological Social Work 55, 484–502
(2012). doi: 10.1080/01634372.2012.667523.
Ko, E., Cho, S., Perez, R.L., Yeo, Y., Palomino, H. (2013). Good and bad death: Exploring the
perspectives of older Mexican Americans. Journal of Gerontological Social Work, 56, 6–25
(2013). doi:10.1080/01634372.2012.715619.
Ko, E., Lee, J., Hong, Y. (2016). Willingness to complete advance directives among low-
income older adults living in the USA. Health & Social Care in the Community, 24, 708–716
(2016). doi:10.1111/hsc.12248.
Krause, N. & Hayward, D.R. (2015). Acts of Contrition, Forgiveness by God, and Death
Anxiety Among Older Mexican Americans. The International Journal for the Psychology of
Religion, 25, 57–73 (2015). doi:10.1080/10508619.2013.857256.

18
Kübler-Ross, E. (1969). On Death and Dying. New York: Macmillan.
Leishman, J.L. (2009a). Introduction. In J.L. Leishman (Ed.), Perspectives on Death and Dying
(pp. 1–13). Keswick: M&K Publishing.
Leishman, J.L. (2009b). Death, social change and lifestyle in UK. In J.L. Leishman (Ed.),
Perspectives on Death and Dying (pp. 65–79). Keswick: M&K Publishing.
Lloyd, L. (2010). End-of-Life Issues. In D. Dannefer & C. Phillipson (Ed.), The SAGE
Handbook of Social Gerontology (pp. 618-629). London: Sage.
Lovell, A. & Yates, P. (2014). Advance Care Planning in palliative care: a systematic literature
review of the contextual factors influencing its uptake 2008-2012. Palliative Medicine, 28,
1026–1035 (2014). doi:10.1177/0269216314531313.
Luptak, M. (2004). Social work and end-of-life care for older people: A historical perspective.
Health & Social Work, 29(1), 7–15.
Lynn, T., Curtis, A., Lagerway, M.D. (2016). Association between attitude toward death and
completion of advance directives. OMEGA—Journal of Death and Dying, 74, 193–211 (2016).
doi:10.1177/0030222815598418.
Malcomson, H. & Bisbee, S. (2009). Perspectives of healthy elders on advance care planning.
Journal of American Academy Nurse Practitioners, 21, 18–23 (2009). doi:10.1111/j.1745-
7599.2008.00369.x.
Miettinen, S. (2006). Eron aika. Tyttärien kertomuksia ikääntyneen vanhemman kuolemasta.
Yhteiskuntapolitiikan laitoksen tutkimuksia 4. Helsinki: Yliopistopaino.
Neimeyer, R.A., Currier, J.M., Coleman, R., Tomer, A., Samuel, E. (2011). Confronting
suffering and death at the end of life: The impact of religiosity, psychosocial factors, and life
regret among hospice patients. Death Studies, 35, 777–800 (2011).
doi:10.1080/07481187.2011.583200
Piers, R.D., Van Eechoud, I.J., Van Camp, S., Grypdonck, M., Deveugele, M., Verbeke, N.C.
et al. (2011). Advance care planning in terminally ill and frail older persons. Patient Education
and Counselling, 90, 323–329 (2011). doi:10.1016/j.pec.2011.07.008.
Raz, M., Shalev, C., Amit, S. (2011). Dying of 'old age' in Israel. The European Legacy, 16,
363–375 (2011). doi:10.1080/10848770.2011.575599
Russac, R.J., Gatliff, C., Reece, M., Spottswood, D. (2007). Death anxiety across the adult
years: An examination of age and gender effects. Death Studies, 31, 549–561.
doi:10.1080/07481180701356936
Samsi, K. & Manthorpe, J. (2011). “I live for today”: a qualitative study investigating older
people’s attitudes to advance planning. Health and Social Care in the Community, 19, 52–59
(2011). doi:10.1111/j.1365-2524.2010.00948.x.

19
Sanjo, M., Miyashita, M., Morita, T., Hirai, K., Kawa, M., Akechi, T., et al. (2007).
Preferences regarding end-of-life cancer care and associations with good-death concepts: a
population-based survey in Japan. Annals of Oncology, 18, 1539–1547 (2007).
doi:10.1093/annonc/mdm199.
Sepperd, S., Wee, B., Strauss, S.E. (2011). Hospital at home: home-based end of life care. The
Cochrane Database of Systematic Reviews. doi:10.1002/14651858.CD009231.
Shapiro, S.P. (2015). Do Advance directives direct? Journal of Health Politics, Policy and
Law, 40, 487–530 (2015). doi:10.1215/03616878-2888424.
Sharp, T., Moran, E., Kuhn, I., Barclay, S. (2013). Do the elderly have a voice? Advance care
planning discussions with frail and older individuals: a systematic literature review and
narrative synthesis. The British Journal of General Practice, 63, e657–e668 (2013).
doi:10.3399/bjgp13X673667.
Simon, J., Porterfield, P., Bouchal, S.R. (2015). ‘Not yet’ and ‘Just ask’: barriers and
facilitators to advance care planning—a qualitative descriptive study of the perspectives of
seriously ill, older patients and their families. BMJ Supportive & Palliative Care 5, 54–62
(2015). doi:10.1136/bmjspcare-2013-000487.
Sudore, R.L., & Fried, T.R. (2010). Redefining the “planning” in advance care planning:
Preparing for end-of-life decision making. Annals of Internal Medicine, 153, 256–261 (2010).
doi:10.7326/0003-4819-153-4-201008170-00008.