in the spotlight emergency nutrition...enu emergency nutrition update nutriset has recently released...
TRANSCRIPT

1
Emergency Nutrition in Large Scale EmergenciesIn this edition: • Latest highlights on recent research in emergency nutrition
• Updates on changes to Nutriset F75 and F100 formula calculation
• Key successes and challenges of undertaking emergency nutrition in large scale emergencies both globally and for World Vision
• Bringing hope in Pakistan – one mother’s experience of how CMAM is changing lives
and as always, lots more important pieces to keep you updated on developments in emergency nutrition, within World Vision and beyond.
ENUEMERGENCY NUTRITION UPDATE
Nutriset has recently released updated guidelines on how to calculate F75 and F100, used for severely malnourished children in inpatient care. Nutriset’s F75 and F100 therapeutic milks come in sachets of 410g and 456g and are mixed using the following calculation: 1 sachet + 2 litres of boiled/potable water = 2.4 litres of therapeutic milk.
In 2004, in response to requests for assistance in calculating and mixing smaller amounts of milk, Nutriset began including a red scoop with its therapeutic milks along with instructions on how much water should be added per scoop of powder. Since then, these instructions have been reviewed, and the following revised guidelines should now be used for smaller quantities of therapeutic milk using Nutriset’s red scoops (red scoops specifically provided by Nutriset and containing Nutriset’s log on the handle):
F100: 1 level Nutriset red scoop with 14 ml of water
F75: 1 level Nutriset red scoop with 18 ml of water
Nutrisets red scoops are included in all procurements for Nutriset therapeutic milk. In order to assist the above process, Nutriset is currently in the process of developing smaller-size sachets.
World Vision note – To date World Vision’s knowledge of the use of the Nutriset red scoop in field settings is limited. If you have experiences using the Nutriset red scoop please email [email protected] and let us know. We are particularly keen to understand what the key advantages and challenges you have faced procuring, measuring, mixing and delivering F75 and F100.
........................................................OCTOBER–DECEMBER 2010 ISSUE 8
TOOLS, GUIDELINES & RECOMMENDATIONS
The Latest Scoop!
Child in Haiti Photo by Jon Warren Nov 2010
In the Spotlight

2
Large scale emergencies continue to take place around the world, ranging from rapid onset such as most recently in Haiti and Pakistan, to slower onset such as in Niger. In most of these situations, food and related nutritional concerns are a major concern.
Over time the ability of the UN and NGO’s to respond to nutrition in emergencies has improved. There has been greater coordination through mechanisms such as the UN Nutrition Cluster, as well as developments in capacity building, emergency preparedness, monitoring and surveillance. While acknowledging the advances, responses in emergencies, particularly in large scale emergencies, continue to face challenges including reaching affected populations, obtaining accurate rapid assessment data, prioritising needs, having sufficient capacity including technical, logistical and monetary, and monitoring and evaluating responses.
Cluster ExperienceA recent review of the Country and Global Level Coordination experience in Haiti following the earthquake in January 2010 highlights some of the key challenges and opportunities for emergency nutrition1.
Context – In January 2010 an earthquake in Haiti measuring 7.0 on the Richter scale, damaged large parts of the country including the capital Port-au-Prince. By mid February it was estimated that 217,000 people had been killed, 300,000
wounded and 3 million affected. Prior to the emergency, stunting was estimated to be 29%, exclusive breastfeeding 41%, and global acute malnutrition 5%. As part of the UN Cluster System for coordination in emergencies, the Nutrition Cluster led by UNICEF was activated within one week of the eathquake striking. Representatives from the UN, government and NGOs, including World Vision, were active participants.
Highlights
• Regular meetings enabled sharing of information between UN, Government and NGO’s, which assisted in identifying needs and avoiding overlaps.
• Rapid agreement and dissemination of a Haiti Specific UN interagency joint statement on IFE to all operational agencies
• Rapid development and dissemination of a UNICEF/WHO technical note on infant feeding in the context of HIV and Haiti.
• Rapid provision of demographic breakdown provided by The Centre for Disease Control assisted in identifying needs and making programming decisions.
• Successful implementation of a range of activities within the first month, including a website where all relevant information was accessible (www.oneresponse.org.nutrition), mapping of resources and gaps, a draft response strategy, and the start-up of various programmes.
Challenges• UN capacity – The Global Nutrition
Cluster was running at one third of capacity at the time the disaster occurred, in part due to lack of funding. UNICEF indentified an internal lack of surge capacity. While a disaster response roster had been drafted prior to the disaster, there was still significant need to draw on capacity from other countries, which left gaps in some countries losing key staff.
• Implementing partner capacity – There was an indentified lack of implementing partners for programming, particularly in the area of severe malnutrition. Finding sufficient health staff was also difficult as many had been injured or died.
• Language - Locating French or Creole speaking nutrition experts was particularly challenging
• Conflicts between needs and mandates – For example the Nutrition Cluster identified that there was a need for nutritional support to the elderly; however this conflicted with UNICEF’s mandate to work with children only. As such the Cluster had to advocate to other groups who could respond.
• Intercepting unsolicited formula – There were many groups who requested and accepted unsolicited infant formula in breach of the International Code on Marketing of Breast Milk Substitutes. Tracking and addressing this proved very time consuming
ENU SPOTLIGHT
Nutrition in Large Scale Emergencies
........................................................
1. Information for the ENU submission piece has largely been drawn from the following articles:
• Dolan, C & Ververs, M. (2010, September). The Haiti Earthquake Country and Global Cluster Coordination Experiences and Lessons Learnt. Field Exchange, Issue 29, p2-7
• Nutrition Cluster Coordination Team and UNICEF Haiti. (2010, September). UNICEF’s perspective on cluster coordination and programme response in Haiti 2010. Field Exchange, Issue 29, p7-8.
Submitted by Kaitrin Both,Emergency Nutrition Advisor World Vision
Australia and World Vision International

3
........................................................
World Vision’s ExperienceWorld Vision experience and capacity in nutrition has continued to grow from national office to global, particularly over the past few years. It’s interesting to note that many of the successes and challenges faced by the UN Cluster System and Nutrition Cluster System are not dissimilar to WV’s own experience. Most recent responses have highlighted that while WV has been able to achieve a lot there remain areas for strengthening.
Highlights and Challenges Some of the key challenges WV has faced in recent times and is working hard to address include:
• Ensuring a qualified Emergency Nutritionist is deployed at the onset of an emergency for Nutrition & Health strategy and proposal development.
• Ensuring adequate monitoring & evaluation systems are included in programme designs from the beginning.
• Ensuring a nutritionally adequate food ration for the beneficiaries
One challenge in particular has been repeatedly raised in recent responses; staff capacity. WV has made excellent progress in scaling up nutrition staffing capacity in the past few years. We have seen the establishment of the WV Global Health Centre including an Emergency Health Director; the formation of the WV Nutrition Centre of Expertise including one Emergency Nutritionist Advisor position, and the addition of a Health and Nutrition Specialist on the WV Global Rapid Response Team. In addition, Nutritionists have been employed in the various Regions and one CMAM Advisor has been hired for the Africa region. Their roles have included assisting National Offices and building capacity of staff in areas such as CMAM and IFE. Despite this overall increased National Office capacity, the timely availability of staff for deployment in an emergency has remained a challenge due to staffing workloads and
flexibility to leave ongoing work to rapidly respond.
A newly advertised position, the Emergency Nutrition Specialist, will strengthen the capacity of WVI to respond in a timely manner to nutritional needs during humanitarian crises. This position will serve 50% of their time as part of the GRRT, for deployment, to large-scale emergency anywhere in the world where WV responds directly. Their remaining 50% will be based within WV Canada’s Nutrition and Health team. Hiring is currently taking place for this position.
As emergencies continue to arise, WV seeks to continuously to reflect on and improve its ability to prepare and respond to emergencies through nutrition. If you have suggestions on ways we can do this, be sure to share these ideas with your Regional Nutrition Advisor.
A special thank-you to Sarah Carr and Claire Beck for their contribution to this piece.
Haiti Photo by Jon Warren Nov 2010
4
NEWS FROM THE FIELD........................................................
Country
S. S
udan
Ken
ya
Eth
iopi
a
Som
alia
Zim
babw
e
Nig
er
ED
RC
WD
RC
Zam
bia
Mau
rita
nia
Sier
ra L
eone
Project areas / ADP’s covered
Tonj Sth, Tonj Nth & Gogrial West
10 13 1 2 18 2 6 2 5 2
Project status(O = ongoing)
Up to end of 2011
Up to end of 2011
O
Somaliland closed. Puntland opened.
O in Lupane & Rushinga
OO in Masisi & Rwanguba
O
Phased out. Waiting for funds
O O
Foodsecurity situation
Poor - receiving food aid
Very poor – need food aid
Very poor – need food aid
Poor – receiving food aid
Poor – receiving food aid in some areas
Poor – receiving food aid
Poor – receiving food aid mainly due to conflict
Poor – receiving food aid mainly due to conflict
Poor – receiving food aid
Poor Poor
General security
Poor - cattle rustling and clan violence
Poor - cattle rustling
Generally good
Very poor – clan wars in Somalia
Good Moderate to good
Poor - sporadic rebel attacks
Good – but can change rapidly due to rebels activities
Generally good Good Good
Access to population
Poor due to rains Moderate Good
Poor due to insecurity
Good Good Poor Good
Good except during rains
Good Good
Total number of sites
OTP=31 SFP=31
OTP= 66 SFP= 83
OTP=61 SFP=N/A
OTP=39 SFP=33
OTP=11 SFP=11
OTP=47 SFP=52
OTP=17 SFP=0
OTP=21 SFP=0
OTP=16 SFP=16
OTP= 22 SFP= 0
Numberadmitted since programme setup
OTP&SC =3096 SFP= 9686
OTP= 4333 SFP= 312734
OTP= 6812 SFP= N/A
OTP= 1216 SFP= 10838
OTP= 385 SPF= NA
OTP= 2877 SFP= 7622
OTP= 1808 SFP= 6467
OTP= 1649 SFP= 0
OTP= 524 SFP= 969
OTP= NA SFP= 479
OTP= 7
Number trained in CMAM
CV=265 MOH=10 WV=44
CV=330 MOH=53 WV=82
CV=560MOH= 173 WV= 14
CV=1692 MOH=11 WV=95
CV= 210 MOH=23 WV=4
CV= 1329 MOH= 282 WV=16
CV=333 MOH=14 WV=6
CV= 89 MOH=53 WV=11
CV=795 MOH=36 WV=12
DU DU
Recovered 85% >80% 85% 82%* 70% 77.4% 90% 97% 85%
Deaths in programme <3% <3% <3% <3% <3% 3.9% <3% <3% <3%
Default 14% <15% 1.7% 9% 24% 13% 6% 2% 6%
Coverage 67.1% in Tonj Sth
63% in Turkana
67% in Durame
42.7% in Burkahaba >50% <44% in
Maradi 76% 53% in Lwambo
53% Sinazonwe & 67% Musele
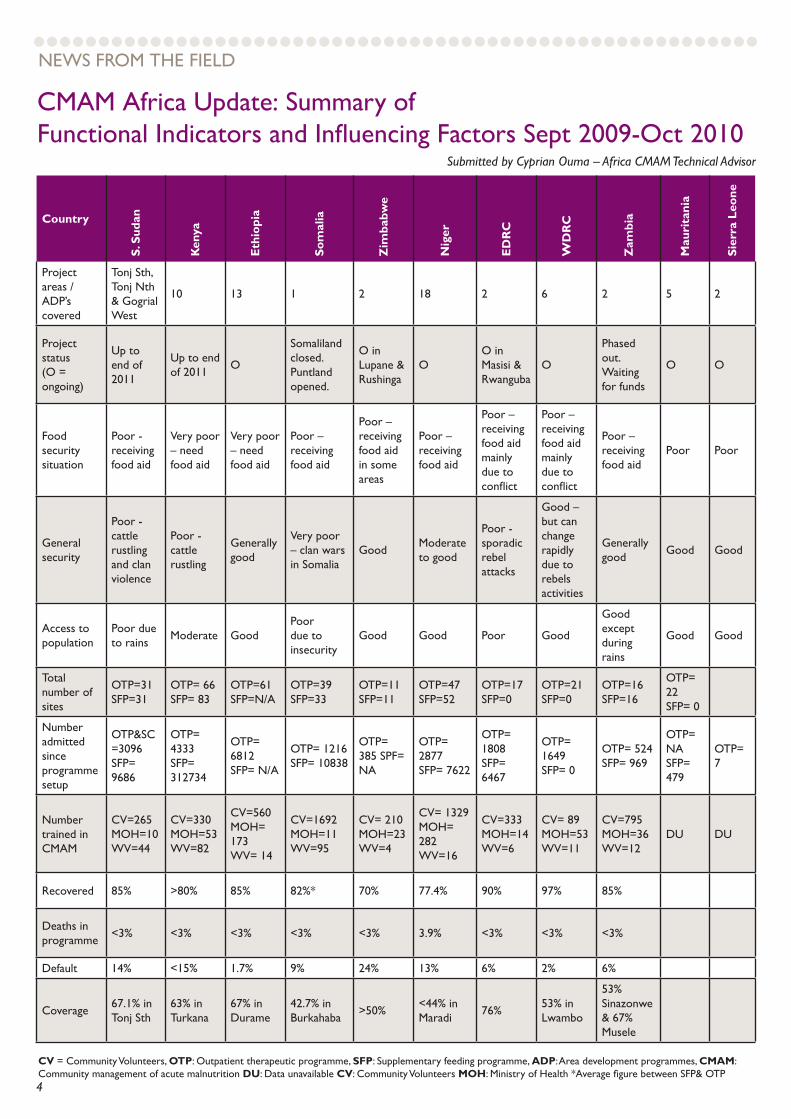
CMAM Africa Update: Summary ofFunctional Indicators and Influencing Factors Sept 2009-Oct 2010
Submitted by Cyprian Ouma – Africa CMAM Technical Advisor
CV = Community Volunteers, OTP: Outpatient therapeutic programme, SFP: Supplementary feeding programme, ADP: Area development programmes, CMAM: Community management of acute malnutrition DU: Data unavailable CV: Community Volunteers MOH: Ministry of Health *Average figure between SFP& OTP

5
Photos by WV Pakistan, Oct 2010
........................................................
A Success Story from Pakistan
Submitted by Dr Sarfaraz Ali Khawaja, Health & Nutrition Coordinator, Sukkur, Pakistan
On October 6, Bindiya, a 16 month old baby girl living in a small village in Khair Pur Sindh district arrived at one of WV’s Nutrition Centres.Bindiya’s mother told WV Pakistan (WVP) staff that she was worried for her baby’s health. She reported that she had felt helpless to be able to do anything for her child, however when she found out about the WV Nutrition Programme through WVP’s Health Promoters (HP) in her community, it was a ray of hope, and on the advice of the WVP HPs she came to the WV Nutrition Centre.
Suffering from malnutrition due to unavailability of food and poor child feeding practices, Bindiya’s weight was recorded as 5.4kg, height 71cm and MUAC 10.5cm. After a further check-up, Bindiya was registered into the Outpatient Therapeutic Programme (OTP) where she received Plumpynut, and her mother received a ration card and was briefly oriented on how to give her child Plumpynut.
On October 13, Bindiya was scheduled to return to the Centre for a follow-up visit but she didn’t come. WV HPs visited her area to find out the reason. They located Bindiya and her mother and identified that Bindiya had eaten only some of the Plumpynut she received from the Centre; the rest was remaining as her mother had not given it to her.
While visiting, WV HP staff did a routine examination measuring Bindiya’s weight (5.6kg) and MUAC (11.3cm). Though Bindiya had not eaten all the packets given, she had eaten some resulting in her MUAC increasing and her weight also increasing slightly. Seeing this improvement, Bindiya’s mother became more motivated to give the Plumpynut and while visiting, WV HP staff stayed to ensure she managed to get her child to eat the required amount of Plumpynut.
On October 19, the mother came in with a big smile on her face. When she arrived, the mother looked mentally relaxed and was praying for the success of the programme. She had noticed a huge improvement in Bindiya’s health and behaviour. Bindiya now enthusiastically ate the Plumpynut, and now weighed 6.4kg with a MUAC of 12.2cm. Her mother told the staff her husband also noticed a very big improvement and encouraged her to return to the Centre for follow-up.
This is just one of the stories of how CMAM programming in Pakistan is contributing to health and happiness of the most needy.
........................................................
Standardised Training Package on SMART Methodology is Released by ACF CanadaAction Against Hunger (ACF) Canada, with the support of the Inter-Agency Standing Committee (IASC) of the Global Nutrition Cluster has recently released the English version of the SMART Methodology Standardised Training Package (STP).
The Standardised Training Package (STP) aims to provide organisations and individuals with a useful reference resource when thinking about training others in SMART. The STP has incorporated the recent (Version 2) methodological advancements and also
contains easy-to-follow presentations, simple exercises, trainer’s tips, videos as well as helpful assessment tools to complement the training experience. It is recommended that in order to be the most effective, a mixture of classroom
TOOLS, GUIDELINES & RECOMMENDATIONS
(Standardised - Continued On Page 6)

6
........................................................
Chaparro CM, Dewey KG. Use of lipid-based nutrient supplements (LNS) to improve the nutrient adequacy of general food distribution rations for vulnerable sub-groups in emergency settings, Maternal Child Nutrition. 2010 Jan; 6 Suppl 1:1-69.
It was proposed that current food interventions in emergency settings may be insufficient to meet the high nutrient
needs of infants, young children, and pregnant and lactating women (PLW), and that adding lipid-based nutrient supplements (LNS) to general food distribution (GFD) programmes and supplementary feeding programmes could fill nutrient gaps in the diets of these most vulnerable groups.
RUTF containing 10% Less Milk Is Less Effective Than One with 25% Milk in the Treatment of SAM
Eleanor Oakley, Jason Reinking, Heidi Sandige, Indi Trehan, Gregg Kennedy, Kenneth Malta, and Mark Mammary. A Ready-To-Use Therapeutic Food Containing 10% Milk Is Less Effective Than One with 25% Milk in the Treatment of Severely Malnourished Children J. Nut. 2010; 140 2248-2252
Standard therapy for severe acute malnutrition (SAM) is home-based therapy with ready-to-use therapeutic food (RUTF) containing 25% milk. In an effort to lower the cost of RUTF and increase availability, some have suggested that a portion of milk be replaced with soy. This trial was designed to determine whether treating children with SAM with 10% milk RUTF containing soy would result in a similar recovery rate compared with the 25% milk RUTF. A randomized, double-blind, controlled, clinical, quasi-effectiveness trial of isoenergetic amounts of 2 locally produced RUTF to treat SAM in Malawi among children aged 6–59 months was conducted. A total of 1874 children were enrolled. Children were assessed every fortnight and participated in the study until they clinically recovered or received 8 weeks of treatment. The primary outcome was recovery (weight-for-height Z score > −2 and no oedema). Secondary outcomes
were rates of weight and height gain. Survival analysis was used to compare the recovery rates.
Findings were that recovery among children receiving 25% milk RUTF was greater than children receiving 10% milk RUTF, 64% compared with 57% after 4 wk, and 84% compared with 81% after 8 wk (P < 0.001). Children receiving 25% milk RUTF also had higher rates of
weight and height gain compared with children receiving 10% milk RUTF. The study concluded that treating children with SAM with 10% milk RUTF is less effective compared with treatment with the standard 25% milk RUTF. These findings also emphasize that clinical evidence should be examined before recommending any changes to the formulation of RUTF.
Submitted by Crispin Baderha WVDRC DM&E & Claire Beck WV GRRT Health & Nutrition Specialist
RESEARCH & GLOBAL PARTICIPATION
Enrichment using ‘one-size-fits-all’ product could fill nutrient gaps in emergency food packages
(Enrichment - Continued On Page 7)
....................................activities, field activities and mentoring should be undertaken as part of the training process.
World Vision note - The STP provides an excellent clear and simple training package but assumes participants have some survey knowledge. If the STP is to be used foradvanced Training of Trainers (TOTs), further detailed training may be required.
For more information on the STP, including activation of a username and password for the STP material, go to www.smartmethodology.org. A French version of the STP is due to be released shortly.
(Standardised - Continued From Page 5)

7
WV Emergency Nutrition Staff Updates
For questions or contributions to the WV ENU, please contact the WV Nutrition Centre of Expertise [email protected]
NCOE is hosted by WVCanada.
Global Health & Nutrition
Nutrition Centre of Expertise
Filling The Role Full TimeThe Nutrition Centre of Expertise (NCoE) currently has 1 full time position dedicated to Emergency Nutrition (Technical Specialist, Emergency Nutrition). For the past few years, Colleen Emary and Sarah Carr have largely been sharing this role. Since our last edition, Colleen Emary has departed for her one-year maternity leave and Sarah Carr is currently filling the role full time.
MEET AND GREET
Sisay Sinamo
Next ENUIf you have any suggestions, stories or reports
which you think would be helpful for ENU readers, please email to [email protected] by Tuesday
21st March 2011. Our theme topic for Jan-Mar 2011 will be WV’s CMAM Database.
Years with WV – 9 years - Oct 2001 - April 2008 World Vision Ethiopia, May 2008 - Dec 2009 Africa Regional Office and Jan 2010 – now East Africa Region
Current position – Nutrition Advisor
Current work location – East Africa Region, Nutrition Learning Centre, based in Ethiopia
Main work responsibilities/activities• Providing technical support and
coordination of developmental and emergency nutrition in the East Africa Region.
• Working with the Global Team to define standards, document and share best practices and lessons
• Building staff nutrition technical skills and expertise in the region to conduct assessment (such as LQAS, SMART) and implement project models (such as CMAM, PD Hearth and nutrition component of the 7-11)
• Establishing linkages and networking with partners and institutes working on nutrition, conducting research and sharing World Vision work through publication and engage with and contribute to the nutrition working
group and health and nutrition Community of Practice.
• Supporting NOs in strategy development, resource mobilization and project/programme implementation
Best part of your job / working in emergency nutrition – Conducting assessments and response plans, helping develop staff skills, and being on site to support implementation of emergency nutrition activities
Most challenging part of your job? – Resource mobilization - especially working to meet the emergency nutrition resource needs of projects/national offices
When you’re not working? –Spending time with my family and volunteering at church.
..................
The authors describe the process used for identifying an optimal formulation of LNS for infants and young children and pregnant and lactating women (PLW) in emergency settings and to enhance the nutritional quality of food aid. Related issues discussed include: bioavailability of nutrients and toxicity concerns; chemical forms of fortificants; stability and shelf-life; production, packaging and distribution of LNS in the context of emergencies, and cost implications of the addition of LNS to current GFD rations.
Analyses confirmed that the typical GFD ration currently provided in emergency settings does not meet the nutritional needs of infants, young children, and PLW. Nutrient shortfalls included calcium, iron, zinc, B vitamins, vitamins D, E, and K, and fat and essential fatty acids. The authors designed a ‘one-size-fits-all’ LNS formula to meet these needs, using one ‘dose’ (20 g, or 4 teaspoons/day) for infants and young children and two ‘doses’ (40 g, or 8 teaspoons/day) for PLW. Addition of LNS to the GFD ration would increase costs. However, depending on the contribution of food costs to total programme costs, the overall increase in costs may be manageable, especially if improved nutrition of vulnerable groups prevents severe malnutrition and other adverse health consequences.
(Enrichment - Continued From Page 6)
..................