in my own words ivf - fertility associates || home · in my own words ivf ... 3. embryology, ......
TRANSCRIPT
in mY oWn Words
ivF• Step-by-step through IVF
• Optimising success
• Risks and side effects
• Decisions to be made
• Managing your cycle
62 pathway to a child
ivF
pathway to a child 6564 pathway to a child
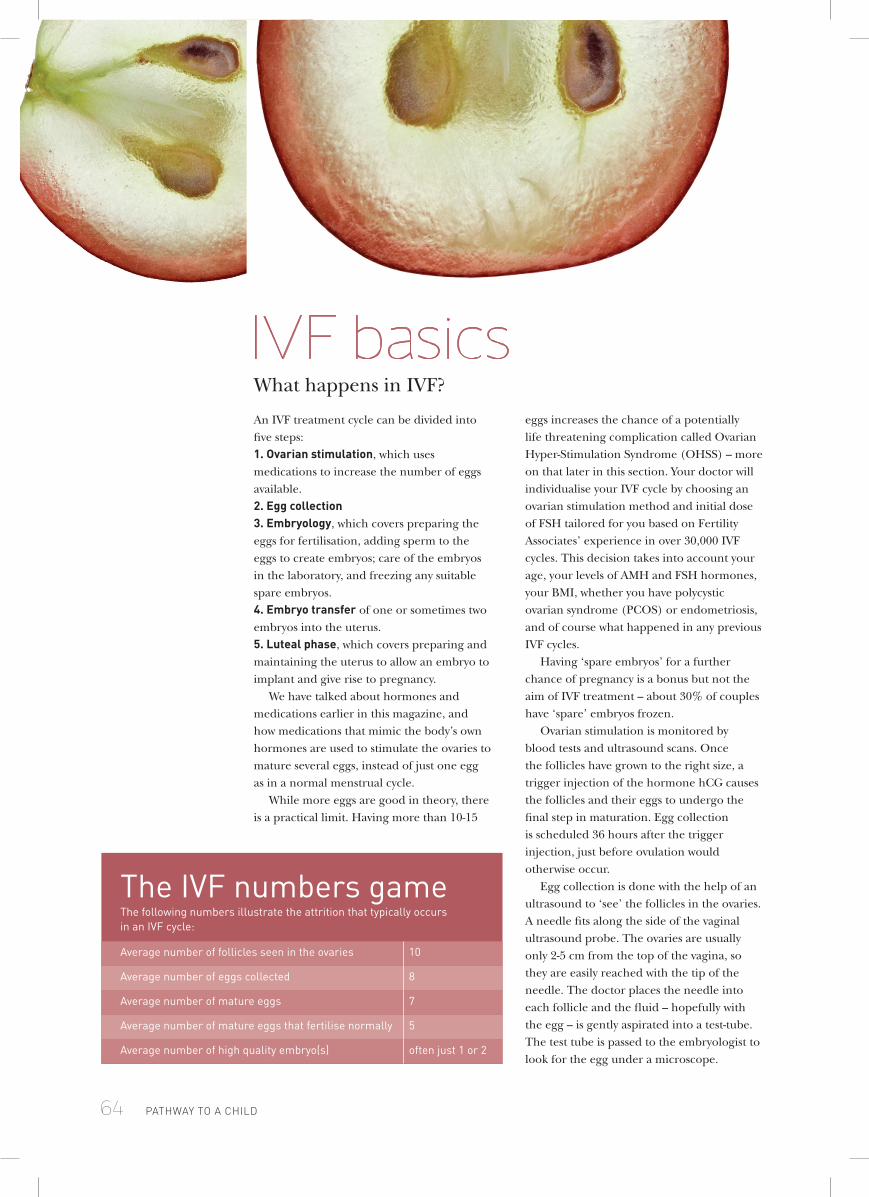
An IVF treatment cycle can be divided into five steps:1. ovarian stimulation, which uses medications to increase the number of eggs available. 2. egg collection3. embryology, which covers preparing the eggs for fertilisation, adding sperm to the eggs to create embryos; care of the embryos in the laboratory, and freezing any suitable spare embryos.4. embryo transfer of one or sometimes two embryos into the uterus.5. luteal phase, which covers preparing and maintaining the uterus to allow an embryo to implant and give rise to pregnancy.
We have talked about hormones and medications earlier in this magazine, and how medications that mimic the body’s own hormones are used to stimulate the ovaries to mature several eggs, instead of just one egg as in a normal menstrual cycle.
While more eggs are good in theory, there is a practical limit. Having more than 10-15
eggs increases the chance of a potentially life threatening complication called Ovarian Hyper-Stimulation Syndrome (OHSS) – more on that later in this section. Your doctor will individualise your IVF cycle by choosing an ovarian stimulation method and initial dose of FSH tailored for you based on Fertility Associates’ experience in over 30,000 IVF cycles. This decision takes into account your age, your levels of AMH and FSH hormones, your BMI, whether you have polycystic ovarian syndrome (PCOS) or endometriosis, and of course what happened in any previous IVF cycles.
Having ‘spare embryos’ for a further chance of pregnancy is a bonus but not the aim of IVF treatment – about 30% of couples have ‘spare’ embryos frozen.
Ovarian stimulation is monitored by blood tests and ultrasound scans. Once the follicles have grown to the right size, a trigger injection of the hormone hCG causes the follicles and their eggs to undergo the final step in maturation. Egg collection is scheduled 36 hours after the trigger injection, just before ovulation would otherwise occur.
Egg collection is done with the help of an ultrasound to ‘see’ the follicles in the ovaries. A needle fits along the side of the vaginal ultrasound probe. The ovaries are usually only 2-5 cm from the top of the vagina, so they are easily reached with the tip of the needle. The doctor places the needle into each follicle and the fluid – hopefully with the egg – is gently aspirated into a test-tube. The test tube is passed to the embryologist to look for the egg under a microscope.
ivF basicsWhat happens in IVF?
the iVF numbers gamethe following numbers illustrate the attrition that typically occurs in an iVF cycle:
average number of follicles seen in the ovaries 10
average number of eggs collected 8
average number of mature eggs 7
average number of mature eggs that fertilise normally 5
average number of high quality embryo(s) often just 1 or 2

ivF
pathway to a child 65
There are two ways of adding sperm to eggs. In conventional IVF, about 100,000 sperm are added to each egg. If there are few sperm or sperm quality is compromised, then a single sperm is injected into each egg in a technique known as ICSI. A recent variation of ISCI, called IMSI, uses ultra-high magnification to select each sperm.
Eighteen hours after adding sperm to eggs, an embryologist will check for signs of fertilisation. Embryos are checked again at 25 hours to look for early development, and then on day 3 and on day 5. Embryos are only observed when needed so that we can minimise the time they are out of the controlled environment of the incubator.
Embryos are usually transferred on day 3 or day 5, depending on your doctor’s management plan and the number of good quality embryos on day 3. Good quality ‘spare’ embryos are usually frozen on day 5 or 6. If for any reason it is not possible or advisable to do an embryo transfer, the embryos can be frozen for use later.
Most ovarian stimulation methods need extra progesterone supplied as vaginal pessaries to help prepare the uterus and to maintain the right environment for pregnancy to occur. This is called luteal support.
if you want to go into the details, we suggest you visit www.fertilityfacts.co.nz and read our Fertility Facts sheets on:
• ovarian Stimulation – which explains how each ovarian stimulation method works and the amount of variation in egg number that typically occurs between one iVF cycle and the next;
• ancillary treatments;
• Sperm microinjection (icSi);
• Freezing embryos.>
64 pathway to a child
iVF options• surgical sperm retrieval (ssr) Even when sperm are absent from the ejaculate, they can often be obtained from a fine needle biopsy of the testis.
we have a Fertility Facts sheet on Sperm microinjection (icSi) and Surgical Sperm Retrieval (SSR)
• iMsi or Picsi these are techniques to select the sperm to use for icSi, and may improve the chance of pregnancy or reduce the chance of miscarriage for some people. your doctor will discuss these techniques with you if they are an option.
we have fertility sheets on iMSi and picSi.
• in Vitro Maturation (iVM) in vitro maturation (iVM) is a variation of iVF with icSi that involves collection of immature eggs without using ovarian stimulation. iVM is an option for some women with polycystic ovaries who over-respond to ovarian stimulation medications. the pregnancy rate with iVM is about half that of conventional iVF.
we have a Fertility Facts sheet on iVM.
pathway to a child 67
>
66 pathway to a child
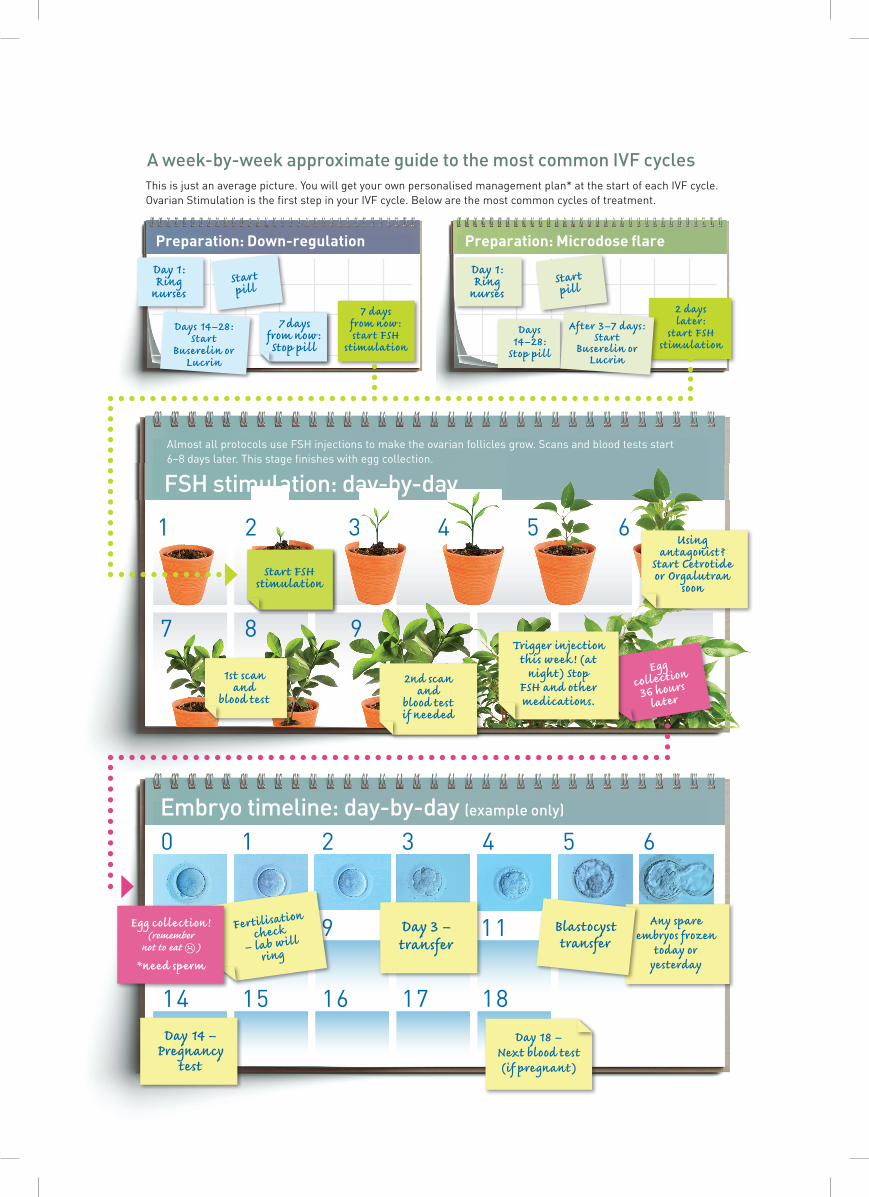
Embryo timeline: day-by-day (example only)
Preparation: Down-regulation Preparation: Microdose flare
a week-by-week approximate guide to the most common iVF cycles
3 65421
13121110987
1817161514
6543210
7 98
ivFthis is just an average picture. you will get your own personalised management plan* at the start of each iVF cycle.ovarian Stimulation is the first step in your iVF cycle. Below are the most common cycles of treatment.
1st scan and
blood test
2nd scan and
blood test if needed
Using antagonist?
Start Cetrotide or Orgalutran
soon
Egg collection !(remember
not to eat L)
*need sperm
Fertilisation check
– lab will ring
Day 3 – transfer
Any spare embryos frozen
today or yesterday
Blastocyst transfer
Day 14 –Pregnancy
test
Day 18 –Next blood test (if pregnant)
Trigger injection this week! (at
night) Stop FSH and other medications.
Day 1: Ring
nurses Start pill
Days 14–28:Start
Buserelin or Lucrin
7 days from now :Stop pill
7 days from now :start FSH
stimulation
Day 1: Ring
nurses Start pill
Days 14–28:
Stop pill
2 days later:
start FSH stimulation
After 3–7 days:Start
Buserelin or Lucrin
Egg collection
36 hours later
FSh stimulation: day-by-day
almost all protocols use FSh injections to make the ovarian follicles grow. Scans and blood tests start 6–8 days later. this stage finishes with egg collection.
Start FSH stimulation

pathway to a child 67
>
Problems and solutionsIVF treatment is a complex medical and scientific procedure so it is not surprising that unexpected things can sometimes happen even with the best knowledge in the world and lots of experience. If things do not go as well as expected, we will always discuss the options with you before any decision is made.• slow down regulation Sometimes down-regulation takes longer than expected – usually this just means delaying the start of the FSH injections by another 4-7 days. If a cyst develops it can usually be resolved by giving an injection of hCG. An alternative is to stop the cycle and to start again in 1-2 months time.• stopping treatment for under-stimulation If fewer follicles develop than expected the best option may be to stop treatment and start again using more medications. This happens in about 10% of cycles. If you have a poor response during a publicly funded cycle, we will make the decision on whether or not to stop and whether you can be offered another publicly funded cycle. • over-stimulation Having too many follicles increases the risk of Ovarian Hyper-stimulation Syndrome (OHSS). The solution depends on the degree of risk. It ranges from stopping the cycle, stopping FSH injections for a few days to cause some follicles to stop developing – which is called coasting, or freezing all the embryos to prevent pregnancy since pregnancy increases the risk of OHSS.• ovulation before egg collection This occurs in about in about 1 in 200 cycles.
• no or low fertilisation Unexpected low or no fertilisation can arise because of a sperm factor, an egg factor, or can just be unexplained. It seldom recurs and the pregnancy rate in subsequent ICSI cycles is normal.• infection of culture dishes Very occasionally culture media may become contaminated with bacteria from the semen or from the vagina during egg collection which leads to the embryos dying. There are various strategies to minimise the risk in subsequent cycles. • Delayed or abnormal embryo development Almost everyone has at least some embryos that stop developing normally by the time of embryo transfer. Occasionally all embryos stop developing before day 2 or 3 so that there are no embryos to transfer. When this happens it can be very difficult to advise what to do next – for some people the problem will recur in another cycle, while for others it is a ‘one-off’ phenomenon that probably arose by chance.
Risks and side effectsiVF treatment is a medical and surgical procedure which carries its share of side effects and risks. Side effects are common events that seldom pose a threat to health or life although they may be unpleasant and painful. Risks are uncommon events that can potentially have serious and permanent consequences.
the time course for iVF falls into three parts represented by the calendar on the opposite page. this is just an average picture – you’ll get a personalised management plan with your own key dates for starting medications and having tests at the beginning of each cycle. • the ovarian stimulation phase often starts with a month or so of preparation. the down-regulation and microdose flare protocols often use a contraceptive pill and then a GnRh agonist such as Buserelin or lucrin to do this. although this preparation means treatment takes a bit longer, it increases the reliability of the next step in most women. Some antagonist protocols skip the preparation step.• the fsH stimulation phase is very similar in almost all protocols. FSh injections make the follicles grow and it keeps them growing in preparation for egg collection.• with egg collection, the focus moves to the laboratory and embryology phase, with fertilisation, embryo culture, embryo transfer and freezing of any suitable spare embryos taking place over a 7-day period. at the same time, you start taking progesterone pessaries to support the lining of the uterus in what is known as the ‘luteal phase’ of the cycle.
>
66 pathway to a child
ivF
pathway to a child 6968 pathway to a child
common side effects• Mild post-menopausal-like symptoms, such as hot flushes, headaches, sore breasts, tiredness and occasionally nausea. these are caused by the rapid changes in hormone levels from taking the medications to stimulate the ovaries. • Mood swings, usually following the start of the FSh injections. Many women report being more tearful than usual. Mood swings are also caused by the rapid changes in hormone levels.• a sharp but fleeting pain when the egg collection needle punctures the ovaries at egg collection, and sometimes at other times during egg collection. this pain is due to movement of the ovaries.• a small amount of bleeding from the vagina after egg collection where the needle went through the vaginal wall. a small amount of brown blood loss for one or two days is common.• Sore ovaries for one or two days after egg collection.• Nausea and not remembering the procedure are common side effects of the sedative and narcotic medications used during egg collection. • Mild abdominal discomfort or bloating from the medications used to stimulate the ovaries, sometimes before but mainly after egg collection.• there is a small chance of bleeding from the cervix after embryo transfer, on the day of transfer or the next day. this is not believed to affect the chance of pregnancy.
Risks for the woman• respiratory depression the medications used for egg collection can reduce the amount of air you breathe and thus the oxygen in your blood. we monitor your oxygen level during and after egg collection with a pulse oximeter. if your oxygen level falls too low, the doctor will stop collecting eggs and give oxygen. Very rarely you may require emergency drugs. Brain damage and death are theoretically possible, but so rare that no figures are available for iVF.
• Pelvic infection after egg collection pelvic infection can occur when the egg collection needle carries bacteria from the vagina or the bowel into the abdomen, or transfers bacteria from a damaged Fallopian tube into the abdomen. infection occurs in about 1 in 500 cycles. the chance of infection can be reduced by giving antibiotics after egg collection if the needle punctures a damaged Fallopian tube, the bowel or an endometriotic cyst. • Vaginal bleeding after egg collection Vaginal bleeding of more than 100 ml (half a cup) occurs in about 1 in 100 egg collections, but usually settles quickly. • internal bleeding after egg collection puncture of a large blood vessel in the abdomen during egg collection occurs in about 1 in 1000 procedures. this would cause severe pain, and would usually occur before you went home. another symptom of internal bleeding can be shoulder-tip pain caused by blood irritating the diaphragm. • Vaso-vagal reaction there is a small chance of a vaso-vagal reaction at the time of embryo transfer. this is an involuntary reflex that causes the heart to slow, blood pressure to drop, and fainting. the embryo transfer is usually stopped and done at a later time. • uterine infection after embryo transfer Uterine infection after embryo transfer occurs in about 1 in 300 transfers. the symptoms are feeling sore or unwell, or a fever. infection usually settles with antibiotics. there have been cases of damage to the uterus or Fallopian tubes, but this is very rare. infection is likely to reduce the chance of pregnancy.• ectopic pregnancy when an embryo implants in a Fallopian tube, the cervix or the abdomen, it is called an ectopic pregnancy. Ectopic pregnancies can be dangerous because the placenta can burrow into a blood vessel and cause major internal bleeding. we can usually detect an ectopic pregnancy by the level of hcG in pregnancy tests and an early ultrasound scan, but not always. Symptoms include severe, localised abdominal pain.
ivF

pathway to a child 69
Pain is your body’s way of saying that something may be wrong. We need to know about any symptoms that might be concerning you. • Fever and abdominal pain are the symptoms of infection– contact the clinic, your doctor or GP the same day. • if you have more than a small amount of vaginal bleeding – contact the clinic, your doctor or GP immediately.• if you feel pain after egg collection or shoulder-tip pain the day of egg collection – contact the clinic, your doctor, or GP immediately. • if you feel sore, feverish or unwell anytime after embryo transfer, phone the clinic immediately.• localised abdominal pain when you are pregnant – contact the clinic, your doctor or GP immediately.
• ovarian Hyper-stimulation syndrome (oHss) ohSS is the most serious risk in iVF. a mild form occurs in up to 20% of women undergoing iVF, and the severe form in about 1–2% of women. if it is not treated, severe ohSS can cause blood clots, stroke and even death.
why it occurs in some people and not in others is unknown, but it only occurs after the ovaries have been stimulated and then exposed to hcG. it is more common in women who produce more follicles after iVF stimulation, and in women who have polycystic ovary Syndrome (pcoS). it seldom occurs until four days or more after the hcG trigger injection. it occurs more commonly in women who become pregnant. physiologically, it occurs when fluid moves from the blood into the abdomen or the lungs.
Mild and moderate cases are usually treated with observation and pain relief, but more severe cases always require admission to hospital. in hospital you may be given intravenous fluids or have fluid drained from the abdomen. if you are a New Zealand resident any hospitalisation as a consequence of iVF treatment is free, but if you are not a resident you will be personally responsible for costs of being admitted to hospital.
we take several active steps to reduce the chance of ohSS. we also help you detect the beginning of >
68 pathway to a child
ivF
ohSS by measuring your weight at embryo transfer and then asking you to measure it every two days.
if your weight increases by 2 kg or more it may be an early sign of ohSS – contact the clinic the same day.the following are possible symptoms of ohSS – if you have any of the these contact the clinic the same day:• increasing abdominal (tummy) pain;• abdominal bloating or swelling;• Nausea or vomiting;• decreased urine output;• Shortness of breath or difficulty breathing;• Severe headache.
Because ohSS only occurs with fertility treatment, the symptoms could be misinterpreted as appendicitis if you see a non-fertility doctor. if you see another doctor, please tell him or her that you have just had ovarian stimulation for iVF, and ask the doctor to contact the clinic. You may take paracetamol (Panadol) to relieve the pain.
• ovarian torsion in about 1 in 500 cycles an ovary becomes twisted around its blood supply which can cause severe and sudden pain and sometimes the loss of the ovary. it is more common in women who respond well to the iVF medications and who become pregnant. it is usually resolved by surgery to untwist the ovary.
Side effects and risks for men having Surgical Sperm Retrieval (SSR)about 5–10% of iVF procedures involve surgical sperm retrieval from the testes. Nausea and not remembering the procedure are the common side effects of the sedative and narcotic medications used during SSR. • respiratory depression the medications used for SSR can reduce the amount of air you breathe and thus the oxygen in your blood. we monitor your oxygen level during and after SSR collection with a pulse oximeter. if your oxygen level falls too low the doctor will stop and give oxygen. Very rarely you may require emergency medications. Brain damage and death are theoretically possible, but so rare that no figures are available for SSR.• Bleeding and infection Bleeding and infection

pathway to a child 71
are possible complications of SSR, although they are rare. it is not uncommon to feel discomfort for several days, and good scrotal support and panadol is advised.
• inflammation in the testes SSR is likely to cause inflammation in the testes that could reduce future sperm production. it can also damage blood vessels in the testes. Up to 80% of men having SSR will have inflammation or pooling of blood (haematoma) at the site of the biopsy. complete loss of blood supply and atrophy of the testes has been reported after a testicular biopsy. a repeated SSR procedure is more likely to be successful if it is done at least 6 months after the last procedure, suggesting SSR commonly causes temporary damage to the testes.
• if analgesic medications are used during biopsy they will affect your ability to drive safely, so you need to arrange transport home from the clinic. You can not drive or use machinery during the next 24 hours, and we advise that someone remains with you for six hours after the procedure.• if pain persists or recurs after SSR, contact the clinic immediately.
longer term risks and iVF• Pregnancy and child birth obstetric problems such as blood pressure, bleeding from the placenta (ante partum haemorrhage), low birth weight, and premature birth are higher in iVF pregnancies. the risks are higher for women over 40 years, and when using donor eggs, and not so high when using frozen embryos. you should take this into account when choosing a doctor or midwife for pregnancy care.• Multiple pregnancy having twins doubles or triples most birth-related risks to you and the babies. transferring one embryo at a time almost eliminates the risk of twins, but not quite, because the chance of identical twins is higher after iVF than from natural conceptions. around 2% of all births at Fertility associates after transfer of one iVF embryo are identical twins. identical twins carry a higher risk of complications for the children.
For some people there is a remote risk of
multiple pregnancy resulting from the fertilisation of an egg not retrieved during egg collection in addition to the embryo(s) transferred.
See our Fertility Facts on Risks of twins. www.fertilityfacts.co.nz
• cancer long-term follow up studies have failed to show any association between fertility treatment and ovarian or breast cancer. pregnancy provides some degree of protection against ovarian cancer. • sperm and embryo storage Frozen sperm and embryos are stored in thin plastic straws immersed in liquid nitrogen. cross-contamination of straws by viruses such as hepatitis or hiV is a theoretical risk although it has never been reported. as a precaution we store sperm for men positive to hepatitis B or c or to hiV in a separate bank.
there is a very small risk that a liquid nitrogen bank will fail, causing the sperm or embryos stored in it to perish. Bank failure has been reported occasionally around the world. we take reasonable precautions but cannot be held responsible for the loss of sperm or embryos from bank failure.• Wellbeing of iVf children the incidence of congenital abnormalities in children born after iVF or icSi is about a third higher than for children conceived naturally, which means a chance of around 4 per 100 births instead of 3 per 100 births. Nearly all follow up studies have found iVF children normal in their physical, mental and social development, but this is still a subject of ongoing research. there is some evidence of a slightly increased risk of childhood cancers. this translates to less than an extra 1 case of cancer per 1000 of iVF children.
there is a slightly higher rate of chromosomal abnormality in children from icSi, and male children may inherit their father’s infertility.
See our Fertility Facts on the wellbeing of iVF children, including after icSi. www.fertilityfacts.co.nz
ivF
70 pathway to a child
pathway to a child 71
decisions, decisions, decisions!You and your doctor will need to make several decisions about your IVF cycle before you start treatment. These are recorded in the doctor’s management plan, and those with an ethical aspect are also recorded in your consent form.• How many eggs to add sperm to? On average 75% of mature eggs fertilise normally in IVF and ICSI. Unless you have an ethical objection to discarding ‘poor quality’ embryos or to freezing ‘spare’ embryos, we recommend you request to add sperm to all eggs.• How many embryos to transfer? A woman’s body is designed to carry one baby at a time. As we mentioned before, twins are associated with 2–3 times more risk for both the mother and child for a broad range of adverse outcomes, from maternal death, still-birth to cerebral palsy.
Transfer of one embryo is now standard for women 40 years and younger, and strongly recommended for women 41 and older. Single embryo transfer is required for almost all publicly funded treatment.
The important facts to keep in mind are:• Up to and including the age of 40, the chance of twins with two embryos back is around 25–30%• Between the ages of 41 and 44, the chance of twins with two embryos is around 10-15%.• Even with one embryo back, 2% of pregnancies are identical twins, and even identical triplets have been reported.• With modern embryo freezing methods, 90-95% of embryos survive freezing and thawing.
When the embryo survives freezing and thawing, its chance of pregnancy is very similar to that of a fresh embryo. Our own work, and the work of others, shows the overall chance of having a child is the same whether you put two fresh embryos back, or one fresh and one thawed – BUT transferring one-by-one reduces twins from 25% to 2% and hence is much safer.• at what stage to transfer embryos?Embryos are usually transferred on day 3 or day 5 after egg collection. If there are several embryos of similar quality on day 3, then culturing to day 5 gives better information on which is the best embryo to transfer.
We recommend opting for a day 5 transfer but bringing it forward if one embryo stands out on day 3 or even on day 2.• embryo freezing Unless you have ethical objections, we recommend you request to freeze any good quality ‘spare’ embryos. We culture spare embryos to day 5 so that only embryos that have demonstrated their ability to keep developing are frozen.
ivF
70 pathway to a child
Transfer of one embryo is now standard for women 40 years and younger, and strongly recommended for women 41 and older.

pathway to a child 7372 pathway to a child
my husbaNd and I were first offered informa-tion about the fertility clinic approximately 2 years after a miscarriage. We had a lot of mixed emotions and even wondered why we were not so fortunate to be blessed with one child, especially when you hear about so many neglected children in the news.
We applied for public funding and were not eligible until 2010. My husband had a low sperm count and I had no problems at all, therefore we were accepted due to the fact that we had been trying for five years with no success. It seemed like a lifetime to wait. I know sometimes Māori can tend to feel uncomfortable with public funding, but I can assure you that at no stage at all were we made to feel uneasy or less eligible for treatment.
I was very happy to finally get the call from the fertility clinic to let me know that my IVF treatment was to start in June 2010. The procedure was very quick once started. The hormonal drugs did have a few side effects for me, but we were always well informed of what
we feel blessedTrying for a baby was an emotionally trying time for this couple, but they made it through with a little help.
to expect. It is a very emotional time and I found the best way for my husband and I to get through was to let my husband know how I was feeling. Although the female is the one who has to take all the drugs and cope with the side effects, I found my husband feeling helpless and wishing he could do more. Through my IVF cycle the Fertility clinic staff were very helpful and supplied plenty of information for what I was to expect next.
My husband and I managed to fertilise 8 eggs out of 12. We were informed of the condition of these embryos and were told that we had one that was growing nicely which was chosen to be transferred into the uterus. We were advised that the other embryos did not make it to blastocyst stage which did give me a slight feeling of emptiness. The clinic staff once again was very informative and advised us of the options we could take with these embryos.
The rest of the procedure was pretty straightforward and took a lot of patience. I found myself counting down the days just to hear ‘Yes, congratulations you are pregnant’, one of the happiest days of our lives.
The fertility clinic continued to be very supportive with regular monitoring of the pregnancy which made me feel a lot more confident about not having to face another miscarriage.
My personal view, being Māori, found that the fertility clinic staff were always warm and understanding which made us feel confident in all our decision making. I was very comfortable and asked a lot of ‘what if’ questions which were always answered with all possible outcomes.
My husband and I are very grateful to finally be blessed with our baby thanks to the help of all the staff at the fertility clinic.
“Regular monitoring of the pregnancy made me feel a lot more confident about not having to face another miscarriage.”
here you will find stories our patients have chosen to share with you about their experiences with fertility treatment, the impact on their lives and the different ways they coped with treatment. these stories are written by them and are unedited – they are in their own words...
in mY oWn Words
our Pathway...
ivF