improving the reconstruction of dental occlusion using a
TRANSCRIPT

Vol.:(0123456789)1 3
Journal of Ambient Intelligence and Humanized Computing https://doi.org/10.1007/s12652-021-03404-5
ORIGINAL RESEARCH
Improving the reconstruction of dental occlusion using a reconstructed‑based identical matrix point technique
Sukumaran Anil1,2 · Sajith Vellappally3 · Abdulaziz A. Al Kheraif3 · Darshan Devang Divakar3 · Wael Said4 · Azza S. Hassanein5
Received: 26 October 2020 / Accepted: 15 July 2021 © The Author(s) 2021
AbstractDigital dental models are widely used compared to dental impressions or plaster-dental models for occlusal analysis as well as fabrication of prosthodontic and orthodontic appliances. The digital dental model has been considered as one of the significant measures for the analysis of dental occlusion. However, the process requires more computation time with less accuracy during the re-establishment of dental occlusion. In this research, a modern method to re-establish dental occlusion has been designed using a Reconstructed-based Identical Matrix Point (RIMP) technique. The curvature of the dental regions has been reconstructed using distance mapping in order to minimize the computation time, and an iterative point match-ing approach is used for accurate re-establishment. Satisfactory restoration and occlusion tests have been analyzed using a dental experimental setup with high-quality digital camera images. Further, the high-quality camera images are converted to grayscale images for mathematical computation using MATLAB image processing toolbox. Besides, 70 images have been taken into consideration in which 30 planar view images has been utilized for experimental analysis. Indeed, based on the outcomes, the proposed RIMP outperforms overall accuracy of (91.50%) and efficiency of (87.50%) in comparison with conventional methods such as GLCM, PCR, Fuzzy C Means, OPOS, and OGS.
Keywords Dental occlusion · Camera images · Reconstruction · Grayscale images · Point classification
1 Introduction
Aesthetic and functional dental occlusion is the objective of orthodontic treatment. The tooth size, jaw relation, and teeth alignment are the important aspects of orthodontic manage-ment (Svedström-Oristo et al. 2001). Examination of the oral cavity, radiographic assessment, and evaluation of dental casts are performed to acquire the necessary data during the treatment planning (Rischen et al. 2013). However, the visual examination has limitations to properly visualize the palatal and lingual surface and the occlusion (Maspero et al. 2019).
Moreover, impression procedures can cause discomfort to the patient and require longer chair time (Yuzbasioglu et al. 2014). The plaster casts need physical storage space in addition to the financial and logistical burdens. Further-more, the visual inspection of dental plaster casts does not enable clinicians to examine, measure, or track orthodontic tooth movement and the surrounding bone’s root area (Li et al. 2018). The application of orthodontic force through the appliance shifts the teeth in incremental steps with
* Sukumaran Anil [email protected]
Sajith Vellappally [email protected]
Abdulaziz A. Al Kheraif [email protected]
Darshan Devang Divakar [email protected]
Wael Said [email protected]
Azza S. Hassanein [email protected]
1 Department of Dentistry, Oral Health Institute, Hamad Medical Corporation, P.O. Box 3050, Doha, Qatar
2 College of Dental Medicine, Qatar University, P.O. Box 2713, Doha, Qatar
3 Dental Health Department, Dental Biomaterials Research Chair, College of Applied Medical Sciences, King Saud University, P.O, Box 10219, Riyadh 11433, Saudi Arabia
4 Computer Science Department, Faculty of Computers and Information, Zagazig University, Zagazig 44511, Egypt
5 Biomedical Engineering Department, Faculty of Engineering, Helwan University, Cairo, Egypt

S. Anil et al.
1 3
successive activation of the appliance (Cunningham et al. 2000; Harrison 2011).
In several aspects of dental care, accuracy is a significant problem. To remove the hard dental tissue, an appropriately designed prosthesis is required to avoid the destruction of the existing structure (Aivatzidou et al. 2020; Perea-Lowery and Vallittu 2018). Fixed partial dentures and complete den-ture prostheses are particularly crucial if devices such as designed teeth or implants can be precisely adapted. There-fore, a highly precise reproduction is essential, particularly in dental impressions and laboratory setup (Malachias et al. 2005; Moreira et al. 2015).
Current validation techniques provide centralized linear measurements in all these areas through calipers or micro-scopes. Such methods are limited to a small number of meas-urement points and minimal data on 3D adjustments in the testing area (Chandak 2020). The modern forms of measur-ing include the optical or X-ray analysis of the whole object test area. It tests the entire region or volume and shows it on the computer screen as a 3D object (Erdelyi et al. 2020; Oprea et al. 2008; Shimada et al. 2020). Linear comparisons and overlaps between models with different scan times are feasible. With this outline, it is possible to measure the sur-face’s modifications at each scan point (Akyalcin et al. 2013; Wiranto et al. 2013).
The clinical examination and the assessment of teeth and fremitus mobility are the main methods used to rule-out of occlusal pathology (Fan and Caton 2018; Ribeiro-Dasilva et al. 2017). Many methods have been utilized to determine the occlusal properties, such as using images, and occlusal sonography (Agbaje et al. 2017).
However, conventional methods such as GLCM, PCR, Fuzzy C Means, OPOS, and OGS methods have been uti-lized to calculate occlusal properties shows less accuracy, less efficiency and more computational time. These chal-lenges have been resolved using RIMP which has been listed as follows:
• To design a modern method to re-establish dental occlu-sion using a Reconstructed-based Identical Matrix Point (RIMP) technique.
• To achieve less computation time and more accurate dur-ing the re-establishment
• To analyze satisfactory tests of restoration and occlu-sion at the lab scale, which outperforms conventional techniques.
The rest of the paper is organized as follows: Section 2 discusses the background survey and its limitations. Sec-tion 3 analysis the mathematical modeling for the Recon-structed-based Identical Matrix Point (RIMP) technique. Section 4 validates the results with simulation analysis. Section 5 concludes the research with perspective outcomes.
2 Literature survey
Veena et al. (2017) introduced two different dental anomaly detection algorithms. The work provides a new approach to the detection using hybridized negative trans-formations of dental caries. The texture classification is used for segmenting the objects based on the quality of texture instead of attributes. Grey level Co-occurrence Matrix (GLCM) is the texture of the panorama image. The results obtained from both techniques correlate to the orthopaedic radiologists’ diagnosis.
Kasai et al. (2016) present a system for estimating the dental plaque adhesion area using a commercial camera image for oral healthcare via management of the intraoral environment. They suggested an estimation procedure for the volume of dental plaque applied for Plaque Control Record (PCR) replacement. The relation between the PCR of the front teeth was examined using the suggested method. The test results indicate that the proposed method will estimate the PCRs on all teeth from the front tooth’s details.
Yeesarapat et al. (2014) develop an automatic dental fluorosis classification system using multi-prototypes derived from the fuzzy C-means clustering algorithm. The algorithms’ values are red, green, blue, hue, contrast, and strength canals. Dental fluorosis requirements are often specified for each class, depending on the number of pix-els. In contrast to findings with two experts, they find that the right pixel classification is about 92% on the data col-lection and about 90% on the blind dataset.
Deng et al. (2020) suggested a three-stage method for achieving the required dental final occlusion digitally and automatically by considering the most common One-Piece Orthognathic Surgery (OPOS). This approach consists of three stages: removal points and teeth from two upper and lower dental models, determination and precise align-ment of the upper and lower teeth with normal pressure between midline and canine Molar (M-C-M) according to these three clinical principles of regions, and without interrupting the established connection between M-C-Ms. The approach was quantitatively and qualitatively tested by 18 sets of dental models.
Seikaly et al. (2019) introduced the Alberta reconstruc-tive techniques to performing the jaw reconstruction and occlusion driven process. This process uses the free flap reconstructive protocols along with Alberta reconstruc-tive technique to examine the procedures for implementing jaw reconstruction. The created system is performed with a cohort study, and the system performs the jaw recon-struction with the effective, accurate, cost-effective and aesthetic process.
Seo et al. (2020) suggested a digital occlusion technique applied in unilateral cleft Orthognathic Surgery (OGS).

Improving the reconstruction of dental occlusion using a reconstructed-based identical matrix…
1 3
Single orthodontics and a single surgeon with 2-jaw OGS, utilizing three-dimensional surgical modelling, were used to study 30 successive patients diagnosed with unilateral cleft palate. According to this procedure, visual occlusions were established with the 30 patients’ images, and accord-ingly, quantitative (external group) data were gathered. The findings were matched for two groups. All material has been reviewed to optimize the procedure and identify the final guidelines.
However, many conventional methods such as GLCM, PCR, Fuzzy C Means, OPOS, OGS have been utilized to calculate occlusal properties for digital dental models. How-ever, conventional methods failed to focus on better accuracy and computational time with improved efficiency. This has been resolved in this research using a Reconstructed-based Identical Matrix Point (RIMP).
3 RIMP mathematical modeling and analysis
This paper developed a new approach called the Recon-structed-based Identical Matrix Point (RIMP) method, using the dentition’s symmetrical properties. Many simula-tors can hardly import the external intraoral scanning solid. The dental/stone casts used an intraoral scanner were used for virtual models. Intraoral images were generated on the virtual model using the geometry imaging method by plac-ing the appropriate characteristics points in two-dimensional and three-dimensional D models (with and without crowd-ing) and patients with relatively toothed teeth with intraoral images. Furthermore, RGB (red–green) colour information and a grab error can be retrieved. Image-to-geometry, allow-ing for mapping of colour information’s to 3D virtual den-tal models in 2D and 3D images. The proposed method is appropriate for all scanning systems. Colour models can be obtained from steel and artificial photographic models that allow colour information and beautiful smile matching. The initial missing teeth, which may entirely fulfil the patient’s anatomic specifications, are the most fitting for the partial strength, in which the initial teeth do not exist. Since the dental model is bilateral symmetric for most cases, sym-metrical teeth may be used to substitute the dental model with the original teeth. Therefore, it is possible to expect a customized dental reconstruction. Figure 1 displays the pro-posed solution flow diagram. In the initial step, the point matching algorithm and distance mapping process has been processed. For each tooth, the segmentation phase is done, and the partially edentulous position of the dental model is calculated by a pair of teeth to the right and left ends, which are a variation of the mirror transition, rotation, and transposition to decide the position of the implant accu-rately. Here, the high-quality camera images are converted
to grayscale images for mathematical computation using MATLAB image processing toolbox. Besides, the 3D rep-resentation model has been created and processed based on mathematical derivations for accurate tooth segmentation from grayscale images.
3.1 Point matching algorithm
Let (aj)M−1
p=1 and (bj)K−1q=1
be the 3D dental models of maxillary and mandibular feature points are observed from camera images based on grayscale conversion. Here p and q are the maxillary models of the teeth, and K and M are the mandibu-lar arches. In this case, the two series of points will be paired with a technique that contrasts points based on the tooth curves in line with MI’s dental models (Maximum Intercus-pation). The point match algorithm is based on an advanced function that utilizes weighted optimization of least squares model (Chen et al. 2013). The original alignment will con-sider a process of the energy feature, and a relationship between the two points ( aj) and ( bj) . The energy function is denoted as npq . It measures the rotation matrix R and the relationship, which will reduce a translation vector v.i, and j are vertex points and u, v is the translation vectors.
InitializetargetpointsM, p,K, q;
Begin
If (npq∕(aj − v − Rbj)2)
Matching(check) ∶
M−1∏
p=1
K−1∏
q=1
npq(
aj − v − Rbj)2
− �
M−1∏
p=1
K−1∏
q=1
npq (1)
Where∏(M−1)
(p=0)npq ≥ 1,∀p,
∏(M−1)
(q=0)npq ≥ 1,∀q, npq ∈ (0, 1),∀p, q
elseIf (npq(aj − v − Rbj)2)
Matching(check) ∶
M−1∏
p=1
K−1∏
q=1
npq(
aj − v − Rbj)2
− �
M−1∏
p=1
K−1∏
q=1
npq (2)
Where∏(M−1)
(p=0)npq ≤ 1,∀p,
∏(M−1)
(q=0)npq ≤ 1,∀p, npq ∈ (0, 1), ∀p, q
endif
endbegin
3.2 Algorithm.1. Point matching algorithm
� is the threshold that determines the objective and rejects outliers. Where
(
aj − v − Rbj)2
< 0, npq = 1 is preferred as npq = 0 , if all the other parameters are zeros in the pth and qth rows, for decreasing the objective function. The pair aj and bj are not viewed as generally identical outliers. In the point matching model, M denoted matrix and m denotes the number of iterations addresses the transition (R, m). It can be conveniently used to evaluate the other

S. Anil et al.
1 3
after either matrix or transformation is collected. Equa-tion (1)’s energy function is reduced to optimization with a weighted least square due to the accompanying matrix.
As shown in Eq. (2), the most challenging aspect of minimization is finding a successful correspondence matrix. To demonstrate the point match method, equali-ties of Eq. (2) and a square matrix set are considered. The correspondence matrix is a processing matrix with entries in columns 0 and 1 in line and columns. Suppose the cor-respondence matrix boundaries are reduced to positive real constant numbers. The correspondence matrix is doubly stochastic, with a combination of all positive continuous rows and columns.
(3)
M∏
p=0
npq ≤ 1, 0 ≤ p ≤ M − 1
K∏
q=0
npq ≤ 1, 0 ≤ q ≤ K − 1.
To eliminate the outliers, the disadvantages of inequali-ties must be recognized. The inequalities in (2) can be updated by adding positive slack values nMp and nKq and it is described in Eq. (3).
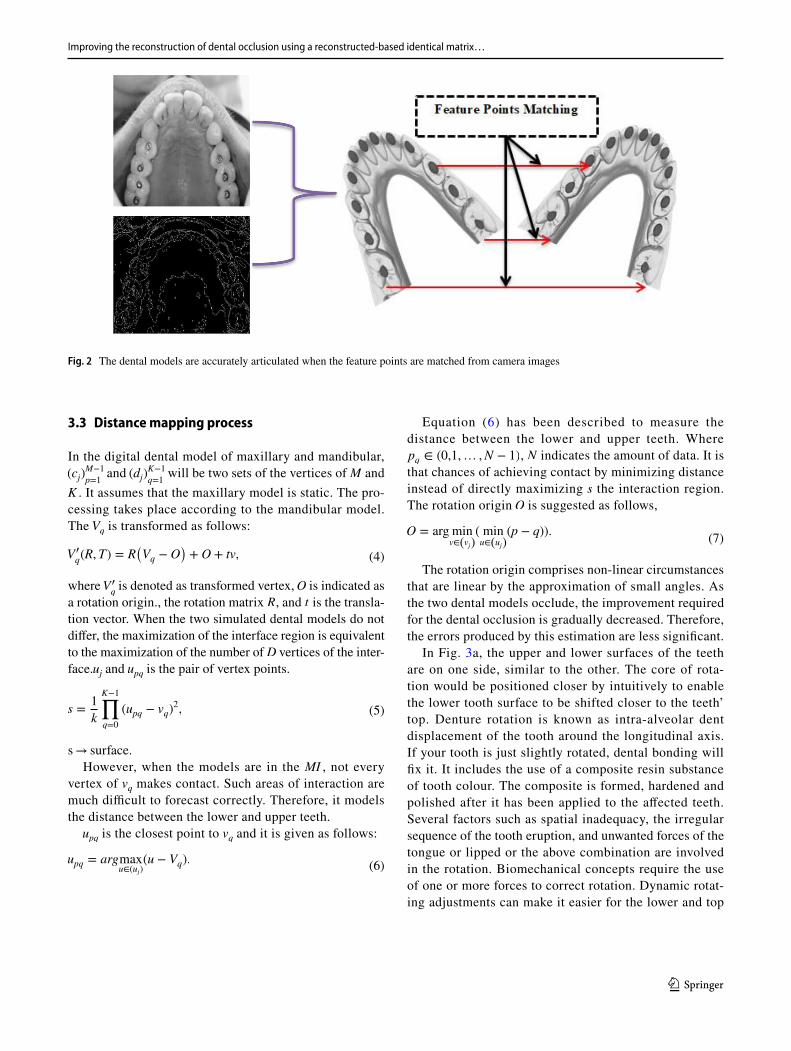
At the beginning of the Point matching algorithm, the mapping matrix is unknown and must be correctly deter-mined based on the dental occlusion criteria. Figure 2 indi-cates the correct situation when the point matching algo-rithm on such specific points is performed. The collection of features on the mandibular form’s arc matches the MI’s max-illary model (maximum Intercuspation). It may be achieved through estimation as the dental curves are very straight and symmetrically relative to the central incisal midline. The parameters can define the matrix even without the other parameters of the whole model being taken into considera-tion. They may be stopped during the initial configuration. To avoid the case, the occlusal planes of the teeth are taken into consideration.
Reconstructed Image
Input Image
Disarticulation of Maxillary
and Mandibular
Model
Create a Dental Model with
High Intercuspation
Point Matching Algorithm and Distance Mapping
Process
Tooth Segmentation
Dental Model Reconstruction and
Transformation Estimation using
RIMP
Par�ally Edentulous
Posi�on
Feature Points Matching
Fig. 1. Overall Architecture of the Proposed Framework
Improving the reconstruction of dental occlusion using a reconstructed-based identical matrix…
1 3
3.3 Distance mapping process
In the digital dental model of maxillary and mandibular, (cj)
M−1
p=1 and (dj)
K−1
q=1 will be two sets of the vertices of M and
K . It assumes that the maxillary model is static. The pro-cessing takes place according to the mandibular model. The Vq is transformed as follows:
where V ′q is denoted as transformed vertex, O is indicated as
a rotation origin., the rotation matrix R , and t is the transla-tion vector. When the two simulated dental models do not differ, the maximization of the interface region is equivalent to the maximization of the number of D vertices of the inter-face.uj and upq is the pair of vertex points.
s → surface.However, when the models are in the MI , not every
vertex of vq makes contact. Such areas of interaction are much difficult to forecast correctly. Therefore, it models the distance between the lower and upper teeth.
upq is the closest point to vq and it is given as follows:
(4)V �q(R, T) = R
(
Vq − O)
+ O + tv,
(5)s =1
k
K−1∏
q=0
(upq − vq)2,
(6)upq = argmaxu∈(uj)
(u − Vq).
Equation (6) has been described to measure the distance between the lower and upper teeth. Where pq ∈ (0,1,… ,N − 1) , N indicates the amount of data. It is that chances of achieving contact by minimizing distance instead of directly maximizing s the interaction region. The rotation origin O is suggested as follows,
The rotation origin comprises non-linear circumstances that are linear by the approximation of small angles. As the two dental models occlude, the improvement required for the dental occlusion is gradually decreased. Therefore, the errors produced by this estimation are less significant.
In Fig. 3a, the upper and lower surfaces of the teeth are on one side, similar to the other. The core of rota-tion would be positioned closer by intuitively to enable the lower tooth surface to be shifted closer to the teeth’ top. Denture rotation is known as intra-alveolar dent displacement of the tooth around the longitudinal axis. If your tooth is just slightly rotated, dental bonding will fix it. It includes the use of a composite resin substance of tooth colour. The composite is formed, hardened and polished after it has been applied to the affected teeth. Several factors such as spatial inadequacy, the irregular sequence of the tooth eruption, and unwanted forces of the tongue or lipped or the above combination are involved in the rotation. Biomechanical concepts require the use of one or more forces to correct rotation. Dynamic rotat-ing adjustments can make it easier for the lower and top
(7)O = arg minv∈(vj)
( minu∈(uj)
(p − q)).
Fig. 2 The dental models are accurately articulated when the feature points are matched from camera images

S. Anil et al.
1 3
Fig. 3 a Upper and lower teeth at the front teeth are similar to the back teeth. A constraint is a half-space. bThe edge cannot be transformed in the other half-space, such as the upper and lower teeth cannot be overlapped
Fig. 4 a Complete mandibular model. b Part of the mandibular model selected. c Base of triangular mesh. d Cloud Point as observed from MATLAB image processing toolbox

Improving the reconstruction of dental occlusion using a reconstructed-based identical matrix…
1 3
tooth surfaces to perfuse better as the tooth surfaces are different. The most significant move of automated den-tal occlusion is the application of collision constraints. It builds a 3D dental data collection collision avoidance system. Collision avoidance is known as restrictions and is implemented into the optimization system. Figure 3b indicates how a constraint is applied from camera images.
3.4 Data processing
The Digital Dental System is shown in Fig. 4. Figure 4a dis-plays a full, 3D laser surface scanner, a complete mandibular model with a right lateral incisor that has been synthetically missed. The aspect of the entire model used in the proposed approach shows in Fig. 4b. Figure 4c shows the triangular mesh region around the missing tooth. Figure 4d displays the point cloud of the model’s surface formed by the trian-gular mesh vertices. The findings have been retained in the form of stereolithography, which reveals a triangular mesh modelling system consisting of facets and vertices for the 3D framework of each dental model Fig. 4c. Every dimen-sion has a popular basic external vector. The recognized neighboring facets of each vertex are discussed. Across the surface, the vertices compensate for a cloud label Fig. 4d.
3.5 Dental segmentation
As shown in Fig. 5a, a partially edentulous teeth pattern will extract from the camera image grey value on each pixel from the reference surface representing the height of a specimen point on the tooth model. The black curve of Fig. 5b is a polynomial of the fourth order plated in the dental arch curve. The dental arch curve is followed by a set of candidates based on the dental arch’s edge. The dental arch named the cross-points from the spoke intersection. A direct spokes sequence is created by a point match algorithm (Fig. 5b). This raw sequence has been used to accurately segmentation both neighboring teeth by a spoke, and it is found accurately at the right-angle interstices. Missing or malocclusion of the teeth can be caused by many causes, including naturally weak bite, trauma, dental care including fillings, crowns, bridges and orthodontic treatment, without considering how the teeth connect properly, i.e. a healthy bite. The crowns, bridges and fillings that do not fit consist-ently up and down and about half of the patients treated with symptoms undergo orthodontic therapy. Therefore, it involves segmentation and processing throughout the tooth’s surface to be sliced, resampled, and smoothed to create a three-dimensional mesh. It is expected to be very sensitive
Fig. 5 Dental Image Segmentation a Image selection. b Raw Image. c Edentulous space. d Stretched Sequence

S. Anil et al.
1 3
to triangle count and mesh resolution with very low resolu-tions. Still, higher resolutions can be expected when surfaces and tooth sizes (e.g. predicted dental area) converge.
Nevertheless, the limit between the partially edentulate space has been analyzed when a whole dental model is pro-duced, and many spokes are correctly placed in the partially edentulate position. The two points articulated (Fig. 5c) are partially constant and numbered perpendicular to the curve from the beginning to end lines. Any teeth can miss a par-tially edentulous position as long as it continues.
Digital dental interface distance image in Fig. 5a. The sequence of raw spokes is shown in Fig. 5b. Many spokes are in part edentulous position by mistake, while others cor-rectly indicate each tooth. Figure 5c indicates the partially edentulous location of the two articulated spokes (red). Fig-ure 5d demonstrates the polished spokes sequence (blue and red), which separates the tooth correctly and the partially edentulous position.
Finally, the raw sequence is mixed with partly edentulous data to provide a refined expression sequence. It initially filters spokes, all of which are false, in a partially edentulous location. It separates the spokes from the beginning to the end of their arch lines. And the two spokes are connected to the sequence, and the arch lines connect the spokes. The polished spoke sequence is obtained (Fig. 5d), which cor-rectly differentiates the developing tooth from the partial edentulous position. The dental arches are the two arches of the teeth, one on each jaw, which form the dentition. The upper (magical) arches of the dental arches are consider-ably wider in humans and many other species than the lower (mandible or lower) arches such that the teeth on both the front and sides of the maxilla overlap slightly in the top of the maxilla in a normal condition (lower jaw). Hence, the masks’ approach and dentals when the mouth closes, known as occlusion, determine the occlusal relationship of opposite teeth and is maloccluded if facial or dental growth is incomplete.
3.6 Reconstruction‑based digital dental occlusion of the partially edentulous dentition using RIMP
The dental model’s reconstruction is explicitly planned to fill the edentulous gap of the symmetrical teeth on the other side of the jaw. Every point of the transformed surface is modi-fied in the same way. This information contributes to the process of reconstruction of the tooth model. The complete dentition dental model has to be computed.
Let Cq and Dp be the points of cloud for dental model. (Cq)1≤q≤U1
completely to the right or left of the dental model which is the coordinates of a 3D set of vertices and the (Dp)1≤p≤V1 on the other half, the dental model is the coordi-
nates of vertices. The cloud points ( Cq) is symmetric with ( Dp) in the potential ideal arrangement of completely mir-rored points. With this intense, rigid transformation � , it may compare the two types of R3
→ R3 performed on ( Dp).The first stage of rigid transformation consists of a mirror
transformation that is performed on ( Dp) as�1 ∶ R3→ R3 . The
transformation of a mirror is parameterized by a matrix of 3 × 3 reflection transformations M. ( Dp) Coordinates are indi-cated by(Zp)1≤p≤V1 . Here ZpistheimageofDp by the effect of transformation �1 , where U is the transformation matrix.
The second step is to introduce a transition of rotation and transmission �2 ∶ R3
→ R3 . (Zp)1≤p≤V1 is transformed to (̂Zp) . �2 parameterizes � , which is given as follows with 3 × 3 rota-tion matrix R and a three-translation vector t:
where � is the parameter for point registration, and p is the vertex point. Point registration is an optimal alignment between two set of points. Zp, � may be transformed to Cp . It demonstrates that one part of the Zp the dental model can be transformed into another part Cp with the rigid � transforma-tion. It refers to their subsets, T denotes the time. A crowded mouth with inadequate space to organize all teeth in one line often leads to traumatic occlusion or illness. Another impor-tant factor is the correct alignment of the upper and lower jaw; if it is not properly closed while chewing, several other oral disorders can occur later in life. The risks for periodon-tal disease increase significantly if the traumatic occlusion is not treated in good time. It is because the teeth are not straight or aligned. The biting pressure of other teeth makes them loose and ultimately sick. Orthognathic is the term used to define the consistency of the upper and lower align-ment of the jaw. This form of surgery aims not to straighten the teeth and correct the bone connection.
(C�u)1≤u≤U2 is a tooth in ( Cq),(D�
v)1≤v≤V2 is in ( Dp) and symmetrical tooth of ( D�
p).(D�v),Cp,Dq are denoted as dental
models and (C�u) is a symmetrical tooth. It can be described as
(8)(Zp) = 𝛿1∕
(
Dp,U)
; where(
Zp)
1>p>V1
(Zp) = 𝛿1(
Dp,U)
; where(
Zp)
1≤p≤V1
}
,
(9)�1(
Dp,U)
= UDp.
(10)(̂Zp) = �2(
Zp, �)
,
(10)𝛿2(
Zp, 𝜃)
= RZp + t, 𝜃 = (R, T) wherep > 0
𝛿2(
Zp, 𝜃)
= Rc − t, 𝜃 wherep < 0
}
,
(11)𝛿2(
Zp, 𝜃)
= Rc − t, 𝜃wherep < 0,

Improving the reconstruction of dental occlusion using a reconstructed-based identical matrix…
1 3
To the same rigid � transformation as shown in (5) and (6) by (U,R, t) variables and it has:
where Z�q ∈ (̂Zp) . Z′
q is a tooth in (̂Zp) . Where (Z�v)1≤v≤V2 is
the transition � of the tooth (Z�v) . It is a dental in (̂Zp) . In the
form of (̂Zp) matches ( Cq), (Z�v) and it matches ( C�
q).(̂Zp) is denoted as a symmetrical tooth.
The same applies to a different (C��1)1≤l≤U3 in ( Cq) tooth and
symmetrical tooth (X��g)1≤g≤V3 in ( Xq):
where (Z��g)1≤g≤V3 is the tooth ( Z��
g) parameterized by (U,R, t) a f t e r t r a n s f o r m a t i o n � . (C��
l) , (C��
l), (D��g), (D
��v), (Z
��g) is represented as a tooth.
According to (13) and (14), it is necessary to transform � from (U,R, t) , Z′
q to match C′q and D′′
g to C′′l using the same
transformation. If C′′l is missing, the partially edentulous space
requires to be filled with its symmetrical Z′′
g tooth and the rigid transformation with another pair of teeth C′
q and Z′q can
be estimated as long as it exists. It assumes that most patients’ teeth are symmetrical and can be controlled with the suggested approach.
3.7 Estimation transformation with partially edentulous positions
At this point, the transition is determined for a set of symmetri-cal teeth. In one dental model Hq(q = 1,…… ., L) , L indicates the position length and there can be many partially edentulous positions. On the one hand, all the partially edentulous posi-tions may be filled with the same transition from the previous topic with their symmetrical equivalents. However, it suggests estimating the transformation for any partially edentulous Hq the position with the teeth close to Hq to improve the exact-ness of the process. To illustrate the calculation, it proceeds to use the dental model seen in Fig. 3b. There is only one partly edentulous position in this case, which is not ambiguous by H.
First, it will evaluate the remaining teeth pair ( C�p) and
( D�q) . On the same side of H , a continuous object ( C�
p) with one or several teeth can be chosen, whether its symmetrical equivalent on the other side occurs. If ( C�
p) , and it will be perfect. The symmetric tooth on the left of the first premolar is designated as ( D�
q).
(12)(C�
u) ∈ Cp
(D�v) ∈ Dq.
(13)Z�q = URD�
v + t,
(14)
(C��l) ∈ Cq
(D��g) ∈ Dp
(Z��
g) = UR(D
��
v) + t
(
Z��g
)
∈ (̂Zp),
A ( D�v) mirror transition would be able to turn the sym-
metric ( U�v) tooth on the same side. The mirrored ( Z�
v) tooth can be measured as follows:
where U =
⎛
⎜
⎜
⎝
−1 0 0
0 1 0
0 0 1
⎞
⎟
⎟
⎠
The crown of (Z�v) and (D�
q) should be chosen; these are all 3D points identified respectively as design points and observation points. These three points are classified as the initial concept points. The RIMP contrasts two different types, but not the same, and their points are distributed randomly.
The curve angle is not a spending time separating the curve vertices that are difficult as the free curve, however group the points in the spectrum along the Z-coordinate and choose the upper vertices 1∕V for the teeth and 1∕V for the upper 1∕V lower vertices. The top 1∕V vertices (
Z′v
)
are chosen. Each set has different points. There is an approximation of their 3D coordinates. The � processing parameters can be tested using a RIMP. There are two main parts of a tooth – the crown and the root. The part of a tooth that can be seen in the mouth is the clinical curve, while by definition; the part that is not apparent is the clinical base. Due to its shape and form of hard tooth tissue covering the external surface, the crown and root are anatomically distinguishable. The permanent teeth are 32 teeth in each arch, and 16 in each arch. Eight teeth consist of two incisors, one canine, another two premo-lars, and three molars in each quadrant. These teeth are called numbers, 1 (centrally incised) to 8 (third molar or "Weisheit" tooth).
In (16), �pq is the regressive probability. C�p − �2 is the
squared Mahalanobis distance. The 3D coordinates for the transformed model points are defined as follows in the �2(�
�p, �
d) iteration step:
R and t can be given to initialize the identity matrix and zero vector. With the current Registration parameter �d the pos-terior �pq is evaluated in E-step. A reference point or outlier class can be allocated to every observed point.
In Eq. (18) Wq = p specifies that C′p matches x′p and
Wq =V2
V+1 specifies that C′
p is an outlier. The reflected (Z�v)
(15)(Z�v) = U(D�
q),
(16)�v+1 = argmin�1∕2
U2∕V∏
q=1
V2∕V∏
p=1
�vpq(C�
p − �2(��q�
d).
(17)�2(
��p, �d)
= Rc��p + tc,
(18)Wq = argmaxp
�dqp.
S. Anil et al.
1 3
tooth may be transformed into the (D�q) source tooth, as
seen in Fig. 6c, with the RIMP, and the recording param-eters � are obtained in conjunction with transformation � . The meshes are not entirely matched for two reasons. First, there are various types of corrections added to each tooth. Furthermore, the spokes that divide the dental model into segments with an interstice resistance angle in opposite directions differ in the left and right segmental limits of each mesh. Such considerations may explain why only the crowns are transformed.
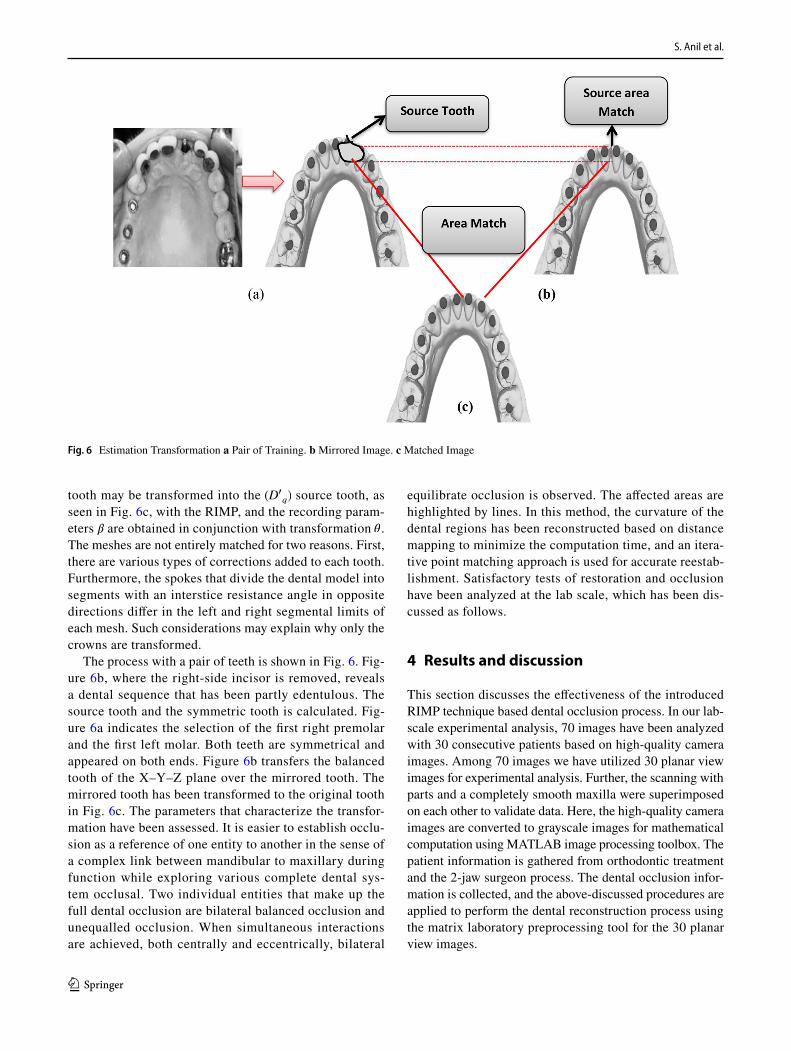
The process with a pair of teeth is shown in Fig. 6. Fig-ure 6b, where the right-side incisor is removed, reveals a dental sequence that has been partly edentulous. The source tooth and the symmetric tooth is calculated. Fig-ure 6a indicates the selection of the first right premolar and the first left molar. Both teeth are symmetrical and appeared on both ends. Figure 6b transfers the balanced tooth of the X–Y–Z plane over the mirrored tooth. The mirrored tooth has been transformed to the original tooth in Fig. 6c. The parameters that characterize the transfor-mation have been assessed. It is easier to establish occlu-sion as a reference of one entity to another in the sense of a complex link between mandibular to maxillary during function while exploring various complete dental sys-tem occlusal. Two individual entities that make up the full dental occlusion are bilateral balanced occlusion and unequalled occlusion. When simultaneous interactions are achieved, both centrally and eccentrically, bilateral
equilibrate occlusion is observed. The affected areas are highlighted by lines. In this method, the curvature of the dental regions has been reconstructed based on distance mapping to minimize the computation time, and an itera-tive point matching approach is used for accurate reestab-lishment. Satisfactory tests of restoration and occlusion have been analyzed at the lab scale, which has been dis-cussed as follows.
4 Results and discussion
This section discusses the effectiveness of the introduced RIMP technique based dental occlusion process. In our lab-scale experimental analysis, 70 images have been analyzed with 30 consecutive patients based on high-quality camera images. Among 70 images we have utilized 30 planar view images for experimental analysis. Further, the scanning with parts and a completely smooth maxilla were superimposed on each other to validate data. Here, the high-quality camera images are converted to grayscale images for mathematical computation using MATLAB image processing toolbox. The patient information is gathered from orthodontic treatment and the 2-jaw surgeon process. The dental occlusion infor-mation is collected, and the above-discussed procedures are applied to perform the dental reconstruction process using the matrix laboratory preprocessing tool for the 30 planar view images.
Fig. 6 Estimation Transformation a Pair of Training. b Mirrored Image. c Matched Image

Improving the reconstruction of dental occlusion using a reconstructed-based identical matrix…
1 3
4.1 Accuracy evaluation
In certain aspects of dental treatment, accuracy is a signifi-cant problem. The reconstruction of the dental hard tissue needs an accurate prosthesis to restore the existing structure. In particular, fixed partial teeth and full prosthesis are essen-tial if devices like teeth or implants can be modified accu-rately. The accuracy of a test is the capacity to reconstruct the teeth correctly. To measure the accuracy of a method, the proportion of true positive, and true negative in all the evaluated cases should be calculated. Based on the Eq. (19), if the False positive value is high it shows decreased level in the graphical structure. Further, If the True positive high it shows increased range in the graphical structure. This can be stated as in Eq. (19) (Alsiddiky et al. 2020):
This proposed Reconstructed-based Identical Matrix Point (RIMP) technique achieves better accuracy in the reconstructed dental model (83.51%) and partially edentu-lous dental model (91.50%) when compared to the other existing methods such as GLCM, PCR, Fuzzy C Means, OPOS, and OGS that mentioned in the literature survey section. Figure 7a shows the reconstructed dental model’s accuracy, and Fig. 7b shows the partially edentulous dental model’s accuracy.
4.2 Computational time evaluation
In the manual labelling step, time-consuming manual work is required. Furthermore, the standard dental model based
(19)Acccuracy =TruePositive + TrueNegative
TruePositive + TrueNegative + FalsePositive + FalseNegative.
on manually appointed characteristics, determined from a small number of dental shapes, is challenging to adapt to individuals’ morphology. This proposed Reconstructed-based Identical Matrix Point (RIMP) technique has less computational time in reconstructed dental (30 s) and partially edentulous dental models (19 s) than the other existing methods such as GLCM, PCR, Fuzzy C Means, OPOS, OGS. Figure 8a shows the computational time of the reconstructed dental model, and Fig. 8b shows the compu-tational time of the partially edentulous dental model. The two front teeth should be square rather than rectangular. Teeth should be higher than wide and should be rectangular. The two teeth (called lateral incisors) on both sides should be smaller and the width of the two front teeth roughly 80%. Small or ’peg-formed’ side incisors are a common concern.
The two sides should be half a millimetre higher than the two sides. The canine teeth shouldn’t be too sharp because people don’t like vampires! The dog’s teeth should be the same as the two front teeth.
4.3 Mean and standard deviation evaluation
The most accurate results of clinical alignment studies on the maxillary scale are the 1st right molar crypt (A), the 1st left molar tooth crypt (B), the 1st median tooth (C). The coordinates of this position are reported to demonstrate the simple truth. The coordinates of each symbol are contrasting until the models come back from some initial positions. Each of these models is reconstructed. It is described in Table 1
Fig. 7 a Accuracy of the reconstructed dental model, b Accuracy of the partially edentulous dental model

S. Anil et al.
1 3
Finally, this strategy has a specific ultimate objective. The preceding approaches are built to rework the tooth for chewing. The technique will measure the artificial tooth or repaired tooth crown in actual usage. However, the goal is to restore dental occlusion. No physical res-toration of missing teeth is possible in real surgery. The partially edentulous mandibula or maxilla is positioned without filling according to the occlusion plan to MI (Maximum Intercuspation) location. This approach is distinct from other approaches to dental occlusion. The previous methods of occlusion will only match the man-dible and the maxillary with full teeth. With the proposed approach, it will effectively match the partly edentulous dental model with MI. The correctness or efficacy of your dental occlusion depends on if your face is symmetrical or
asymmetrical and whether your facial bone structure has discrepancies or malformations that are the primary cause of your malocclusion. If tooth wear is absent, an excessive eruption could happen in patients due to a dent alveolar development and an increase in face height in turn. One should open the mouth between the edges of the lower and upper incisors. The full depth is measured. Dentists must justify the mandible deviation upon opening or shut-ting of the jaw while conducting an extraoral examination. The typical error of about 0:1 mm in the recently acquired tooth analysis can be compared to Table 2.
4.4 Efficiency evaluation
Some existing results relate to the excellent compatibility of the dental model reconstructed. The suggested RIMP would
Fig. 8 a Computational time of reconstructed dental model. b Computational time of partially edentulous dental model.
Table 1 Translational variations in the analysis of alignment with biological structures that are partially edentulous and corresponding reconstructed model
Marker Axis Reconstructed teeth Partially edentulous teeth
Mean (mm) Standard deviation
Mean(mm) Standard deviation
A X − 0.234 0.235 1.782 0.846Y − 0.256 0.263 1.672 0.673Z − 0.245 0.282 − 2.342 0.762
B X − 0.134 0.167 0.645 0.875Y − 0.145 0.178 0.428 1.987Z − 0.176 0.193 0.532 0.349
C X 0.054 0.183 − 0.234 0.241Y − 0.145 0.172 − 0.342 0.432Z 0.017 0.195 − 0.453 0.538
Table 2 Translation changes in the analysis by the original dental models, which are partially edentulous and accurately reconstructed
Marker Axis Reconstructed teeth Partially edentulous teeth
Mean (mm) Standard Devia-tion
Mean(mm) Standard deviation
A X − 0.0035 0.0038 0.2452 0.0034Y − 0.0048 0.0026 0.3523 0.0053Z − 0.0231 0.0087 0.5638 0.0027
B X − 0.0452 0.0051 0.9327 0.0072Y − 0.0342 0.0047 0.2455 0.0025Z − 0.0267 0.0038 0.6234 0.0043
C X − 0.0145 0.0023 0.3762 0.0032Y − 0.0137 0.0072 0.3421 0.0056Z − 0.0321 0.0082 0.4422 0.0078
Improving the reconstruction of dental occlusion using a reconstructed-based identical matrix…
1 3
substantially improve occlusion efficiency and implement the appropriate operating strategy for partially edentulous versions. This approach allows the maxillary and mandibular models to be expressed efficiently with greater efficiency. There is a small degree of variation is due to non region of interest (ROI) unwanted pixels in this method among the digitally articulated occlusion.
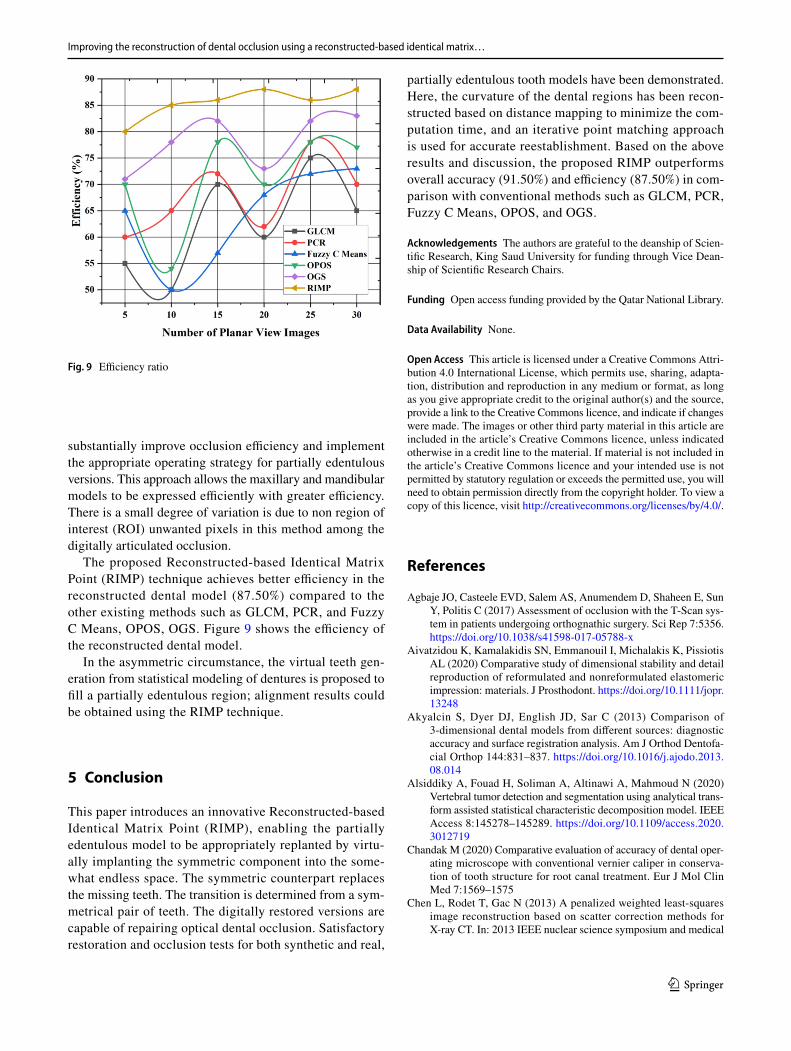
The proposed Reconstructed-based Identical Matrix Point (RIMP) technique achieves better efficiency in the reconstructed dental model (87.50%) compared to the other existing methods such as GLCM, PCR, and Fuzzy C Means, OPOS, OGS. Figure 9 shows the efficiency of the reconstructed dental model.
In the asymmetric circumstance, the virtual teeth gen-eration from statistical modeling of dentures is proposed to fill a partially edentulous region; alignment results could be obtained using the RIMP technique.
5 Conclusion
This paper introduces an innovative Reconstructed-based Identical Matrix Point (RIMP), enabling the partially edentulous model to be appropriately replanted by virtu-ally implanting the symmetric component into the some-what endless space. The symmetric counterpart replaces the missing teeth. The transition is determined from a sym-metrical pair of teeth. The digitally restored versions are capable of repairing optical dental occlusion. Satisfactory restoration and occlusion tests for both synthetic and real,
partially edentulous tooth models have been demonstrated. Here, the curvature of the dental regions has been recon-structed based on distance mapping to minimize the com-putation time, and an iterative point matching approach is used for accurate reestablishment. Based on the above results and discussion, the proposed RIMP outperforms overall accuracy (91.50%) and efficiency (87.50%) in com-parison with conventional methods such as GLCM, PCR, Fuzzy C Means, OPOS, and OGS.
Acknowledgements The authors are grateful to the deanship of Scien-tific Research, King Saud University for funding through Vice Dean-ship of Scientific Research Chairs.
Funding Open access funding provided by the Qatar National Library.
Data Availability None.
Open Access This article is licensed under a Creative Commons Attri-bution 4.0 International License, which permits use, sharing, adapta-tion, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http:// creat iveco mmons. org/ licen ses/ by/4. 0/.
References
Agbaje JO, Casteele EVD, Salem AS, Anumendem D, Shaheen E, Sun Y, Politis C (2017) Assessment of occlusion with the T-Scan sys-tem in patients undergoing orthognathic surgery. Sci Rep 7:5356. https:// doi. org/ 10. 1038/ s41598- 017- 05788-x
Aivatzidou K, Kamalakidis SN, Emmanouil I, Michalakis K, Pissiotis AL (2020) Comparative study of dimensional stability and detail reproduction of reformulated and nonreformulated elastomeric impression: materials. J Prosthodont. https:// doi. org/ 10. 1111/ jopr. 13248
Akyalcin S, Dyer DJ, English JD, Sar C (2013) Comparison of 3-dimensional dental models from different sources: diagnostic accuracy and surface registration analysis. Am J Orthod Dentofa-cial Orthop 144:831–837. https:// doi. org/ 10. 1016/j. ajodo. 2013. 08. 014
Alsiddiky A, Fouad H, Soliman A, Altinawi A, Mahmoud N (2020) Vertebral tumor detection and segmentation using analytical trans-form assisted statistical characteristic decomposition model. IEEE Access 8:145278–145289. https:// doi. org/ 10. 1109/ access. 2020. 30127 19
Chandak M (2020) Comparative evaluation of accuracy of dental oper-ating microscope with conventional vernier caliper in conserva-tion of tooth structure for root canal treatment. Eur J Mol Clin Med 7:1569–1575
Chen L, Rodet T, Gac N (2013) A penalized weighted least-squares image reconstruction based on scatter correction methods for X-ray CT. In: 2013 IEEE nuclear science symposium and medical
Fig. 9 Efficiency ratio

S. Anil et al.
1 3
imaging conference (2013 NSS/MIC), 27 Oct–2 Nov 2013, Seoul, South Korea, pp 1–3
Cunningham S, Horrocks E, Hunt N, Jones S, Moseley H, Noar J, Scully C (2000) ABC or oral health improving occlusion and oro-facial aesthetics: orthodontics. BMJ 321:288–290. https:// doi. org/ 10. 1136/ bmj. 321. 7256. 288
Deng H et al (2020) An automatic approach to establish clinically desired final dental occlusion for one-piece maxillary orthog-nathic surgery. Int J Comput Assist Radiol Surg 15:1763–1773. https:// doi. org/ 10. 1007/ s11548- 020- 02125-y
Erdelyi RA, Duma VF, Sinescu C, Dobre GM, Bradu A, Podoleanu A (2020) Dental diagnosis and treatment assessments: between X-rays radiography and optical coherence tomography. Materials (basel). https:// doi. org/ 10. 3390/ ma132 14825
Fan J, Caton JG (2018) Occlusal trauma and excessive occlusal forces: narrative review, case definitions, and diagnostic considerations. J Clin Periodontol 45:S199–S206. https:// doi. org/ 10. 1111/ jcpe. 12949
Harrison J (2011) Orthodontic Treatment. Vital 8:31–35. https:// doi. org/ 10. 1038/ vital 1329
Kasai M, Iijima Y, Takemura H, Mizoguchi H, Ohshima T, Satomi N (2016) Dental plaque assessment lifelogging system using com-mercial camera for oral healthcare. Annu Int Conf IEEE Eng Med Biol Soc 2016:2566–2569. https:// doi. org/ 10. 1109/ embc. 2016. 75912 54
Li Y, Jacox LA, Little SH, Ko CC (2018) Orthodontic tooth move-ment: the biology and clinical implications. Kaohsiung J Med Sci 34:207–214. https:// doi. org/ 10. 1016/j. kjms. 2018. 01. 007
Malachias A, Paranhos HDFO, Silva CHLd, Muglia VA, Moreto C (2005) Modified functional impression technique for complete dentures. Braz Dent J 16:135–139
Maspero C, Gaffuri F, Castro IO, Lanteri V, Ugolini A, Farronato M (2019) Correlation between dental vestibular-palatal inclina-tion and alveolar bone remodeling after orthodontic treatment: a CBCT analysis. Materials (basel) 12:4225. https:// doi. org/ 10. 3390/ ma122 44225
Moreira AH, Rodrigues NF, Pinho AC, Fonseca JC, Vilaça JL (2015) Accuracy comparison of implant impression techniques: a system-atic review. Clin Implant Dent Relat Res 17(Suppl 2):e751-764. https:// doi. org/ 10. 1111/ cid. 12310
Oprea S, Marinescu C, Lita I, Jurianu M, Visan DA, Cioc IB (2008) Image processing techniques used for dental x-ray image analysis. In: 2008 31st international spring seminar on electronics technol-ogy, 7–11 May 2008, pp 125–129. https:// doi. org/ 10. 1109/ ISSE. 2008. 52764 24
Perea-Lowery L, Vallittu PK (2018) Framework design and pontics of fiber-reinforced composite fixed dental prostheses—an over-view. J Prosthodont Res 62:281–286. https:// doi. org/ 10. 1016/j. jpor. 2018. 03. 005
Ribeiro-Dasilva MC, Nguyen J, Kiskaddon K, Dawson PE (2017) Introduction to occlusion. In: The dental reference manual. Springer, pp 147–160
Rischen RJ, Breuning KH, Bronkhorst EM, Kuijpers-Jagtman AM (2013) Records needed for orthodontic diagnosis and treatment planning: a systematic review. PLoS ONE 8:e74186–e74186. https:// doi. org/ 10. 1371/ journ al. pone. 00741 86
Seikaly H et al (2019) The alberta reconstructive technique: an occlu-sion-driven and digitally based jaw reconstruction. Laryngoscope 129:S1–S14. https:// doi. org/ 10. 1002/ lary. 28064
Seo HJ, Denadai R, Pai BC, Lo LJ (2020) Digital occlusion setup is quantitatively comparable with the conventional dental model approach: characteristics and guidelines for orthognathic surgery in patients with unilateral cleft lip and palate. Ann Plast Surg 85:171–179. https:// doi. org/ 10. 1097/ sap. 00000 00000 002079
Shimada Y et al (2020) 3D imaging of proximal caries in posterior teeth using optical coherence tomography. Sci Rep 10:15754. https:// doi. org/ 10. 1038/ s41598- 020- 72838-2
Svedström-Oristo AL, Pietilä T, Pietilä I, Alanen P, Varrela J (2001) Morphological, functional and aesthetic criteria of acceptable mature occlusion. Eur J Orthod 23(4):373–381. https:// doi. org/ 10. 1093/ ejo/ 23.4. 373
Veena DK, Jatti A, Joshi R, Deepu KS (2017) Characterization of dental pathologies using digital panoramic X-ray images based on texture analysis. Annu Int Conf IEEE Eng Med Biol Soc 2017:592–595. https:// doi. org/ 10. 1109/ embc. 2017. 80368 94
Wiranto MG, Engelbrecht WP, Tutein Nolthenius HE, van der Meer WJ, Ren Y (2013) Validity, reliability, and reproducibility of lin-ear measurements on digital models obtained from intraoral and cone-beam computed tomography scans of alginate impressions. Am J Orthod Dentofacial Orthop 143:140–147. https:// doi. org/ 10. 1016/j. ajodo. 2012. 06. 018
Yeesarapat U, Auephanwiriyakul S, Theera-Umpon N, Kongpun C (2014) Dental fluorosis classification using multi-prototypes from fuzzy C-means clustering. In: 2014 IEEE conference on compu-tational intelligence in bioinformatics and computational biology, 21–24 May 2014, pp 1–5. https:// doi. org/ 10. 1109/ CIBCB. 2014. 68455 34
Yuzbasioglu E, Kurt H, Turunc R, Bilir H (2014) Comparison of digital and conventional impression techniques: evaluation of patients’ perception, treatment comfort, effectiveness and clinical outcomes. BMC Oral Health 14:10–10. https:// doi. org/ 10. 1186/ 1472- 6831- 14- 10
Publisher’s Note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.