improving the diagnosis and management of opioid … constipation to optimize outcomes of patients...
TRANSCRIPT

1
Improving the Diagnosis and Management of Opioid-induced Constipation to Optimize Outcomes of Patients with Chronic Pain
Sponsored by Integrity Continuing Education, Inc.
Supported by an educational grant from Salix Pharmaceuticals, Inc.

2
Faculty Affiliation
Peter Pryzbylkowski, MDAttending Physician
Pain MedicineRelievus Pain ManagementHammonton, New Jersey

3
Faculty Disclosures
▪ Speakers Bureau: Astra Zeneca, Daiichi Sankyo

4
▪ Describe the prevalence of opioid-induced constipation (OIC) and its effect on patient health, quality of life (QOL), and adequacy of pain management
▪ Identify clinical barriers to accurate assessment and diagnosis of OIC
▪ Describe the recommended assessment of patients with OIC and indications for initiation of treatment
▪ Compare the relative efficacy and safety of currently available therapies for OIC
Learning Objectives

5
Everyday Burden of Chronic Pain Among Adults in the United States
Nahin, et al. J Pain. 2015;16(8):769–780.
2012 National Health Interview Survey
2.1%
4.5% 4.6%
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
A little pain A little to a lot of pain A lot of pain
Ad
ult
s re
po
rtin
g p
ain
o
ccu
rrin
g ev
ery
day
(%
)

6
Prescription Opioid Analgesic Use in the US
Dart RC, et al. NEJM. 2015;372:241-248.
Prescriptions Dispensed for Opioid Analgesics
No
. of
Pre
scri
pti
on
s D
isp
en
sed 67,000,000
61,000,000
54,000,000
48,000,000
42,000,000
0

7
Effects of Opioid Action
*Studies suggest 𝛿 and 𝜅 receptors may make a small but potentially clinically significant contribution ORL-1, opioid receptor-like-1, GI, gastrointestinal.
Rumman A, et al. Exp Rev Qual Life Canc Care. 2016;1(1):25-35.Kumar L, et al. Gastroenterol Res Pract. 2014;2014:141737.
Central(𝜇,𝛿,𝜅, & ORL-1
receptors)
Possible alteration of autonomic activity May reduce GI propulsion
Enteric(𝜇 receptors*)
Reduced bowel tone and contractility Prolonged transit time
Increased frequency and strength of circular muscle contractions
Increased nonpropulsive contractions and enhanced fluid absorption
Reduced longitudinal muscle propulsive contractions
Exacerbates trend to harder, drier stools
Increased anal sphincter tone and decreased reflex relaxation in response to rectal distension
Contributes to difficulty in rectal evacuation

8
Opioid-induced Bowel Dysfunction
Opioid-induced bowel dysfunction
Constipation NBSDelayed gastric
emptyingVomitingNausea GERD
GERD, gastroesophageal reflux disease; NBS, normal bowel sounds.

9
Frequency of Constipation with Oral Opioid Treatment
Note: Each symbol represents one study, and size of the symbol reflects the size of the trial, according to the scale at the right.RCTs, randomized control trials.Kalso, et al. Pain. 2004;112:372–380; Camilleri et al. Am J Gastroenterol 2011;106:835–842.
• Constipation is the most common GI complaint associated with opioid treatment
• Meta-analysis of 8 RCTs (N=1,114) found that 41% of patients suffered from OIC after 8 weeks of therapy
0 20 40 60 80 100Constipation (%) with placebo
100
80
60
40
20
0
Constipation (%) with opioid
400
200
0

10
Consequences of OIC
Early OIC
• Impaired QOL• Poor adherence• Medical complications
Later OIC
• Development of opioid-induced bowel dysfunction• Poor adherence or discontinuation
Long-term Implications
• Unnecessary or inadequate pain management• Increased surgical events, ED visits, and hospitalizations
ED, emergency department.Adapted from: Wick JY. 2016. Retrieved from http://www.pharmacytimes.com/publications/issue/2016/july2016/ opioids-and-constipation; Bell TJ, et al. Pain Med. 2009;10(1):35-42; Looström H, et al. Arch Oral Biol. 2011;56(4): 395-400; Pappagallo M.Am J Surg. 2001;182:11S-18S; Gupta S, et al. J Opioid Manag. 2015;11(4):325-338.

11
Patient-reported Impact of OIC on QOL
Patients Reporting Measure (%)
Rauck RL, et al. Pain Practice. 2016.
38
43
45
46
49
84
Impaired work performance
Limits ability to leave house
Limits social interaction
Limits sexual intimacy
Inability to perform daily activities
Impacts dietary choices

12
Patient-reported Impact of OIC on Mental Health
49
49
30
41
32
90
Embarrassment
Depression
Low-self esteem
Social isolation
Anger
Frustration/irritability
Patients Reporting Presence of Measure (%)
Rauck RL, et al. Pain Practice. 2016.

15
Constipation Is Associated with Increased Healthcare Utilization in Patients Undergoing Opioid Therapy
*Non-cancer patients receiving opioid therapy
Adapted from Olufade et al. Am Health Drug Benefits. 2017;10(2):79-86.
Healthcare utilization
(all-cause) Patients with
constipation, N (%)Patients w/o
constipation, N (%)P
value
Inpatient admission 785 (28.9) 368 (13.5) <.001
ED visits 1612 (59.4) 1279 (47.1) <.001
Outpatient office visits 2579 (95.0) 2476 (91.2) <.001
Other outpatient services 2634 (97.0) 2541 (93.6) <.001
Pharmacy claims 2716 (100.0) 2716 (100.0)

16
Constipation Is Associated with Increased Healthcare Costs in Patients Undergoing Opioid Therapy
*Non-cancer patients receiving opioid therapy
Adapted from Olufade et al. Am Health Drug Benefits. 2017;10(2):79-86.
$ (Mean, 95% CI)
Healthcare costs (all-cause)Patients with constipation
Patients w/o constipation
Pvalue
Inpatient admission46,817
(33,982-59,652)33,884
(27,999-39,769).186
ED visits703
(653-754)429
(395-464)<.001
Outpatient office visits843
(812-875)605
(584-626)<.001
Other outpatient services 8534
(7931-9136)4457
(4118-4796)<.001
Pharmacy claims 4622
(4343-4900)3627
(3377-3877)<.001
Total 28,234
(24,307-32,160)13,709
(12,618-14,801)<.001

17
Recognition and Diagnosis of OIC

18
▪ Duration of opioid treatment
▪ Older age
▪ Female sex
▪ Additional factors
– Higher education levels
– Concomitant aspirin use
– Nonsmoker status
▪ Incidence appears unaffected by the opioid route of
administration (oral or transdermal)
Risk Factors for OIC

19
Case Study #1: Identification and Diagnosis
▪ Jane, 50-year-old woman
▪ Chronic back pain due to an injury sustained in a vehicle accident 5 years ago
▪ History of mild depression
▪ Inadequate pain management despite NSAID therapy
▪ Initiated on opioid therapy 3 months ago
▪ Currently reports the following symptoms
– Straining
– Incomplete evacuation
– Hard dry stools every 3-4 days
NSAID, nonsteroidal anti-inflammatory drug.

20
▪ What type of assessment tools/measures would you apply in evaluating Jane?
▪ How would you determine whether Jane’s constipation is caused exclusively by her opioid treatment or reflects the impact of the treatment along with other constipating factors?
▪ What other conditions would you consider in the differential diagnosis?
Case Study #1: Discussion

21
A change when initiating opioid therapy from baseline bowel habits characterized by any of the following:
Definition of OIC
Reduced bowel
movement frequency
Development or worsening of straining to
pass bowel movements
Sense of incomplete
rectal evacuation
Harder stool consistency
Camilleri M, et al. Neurogastroenterol Motil. 2014;26(10):1386-1395.
22
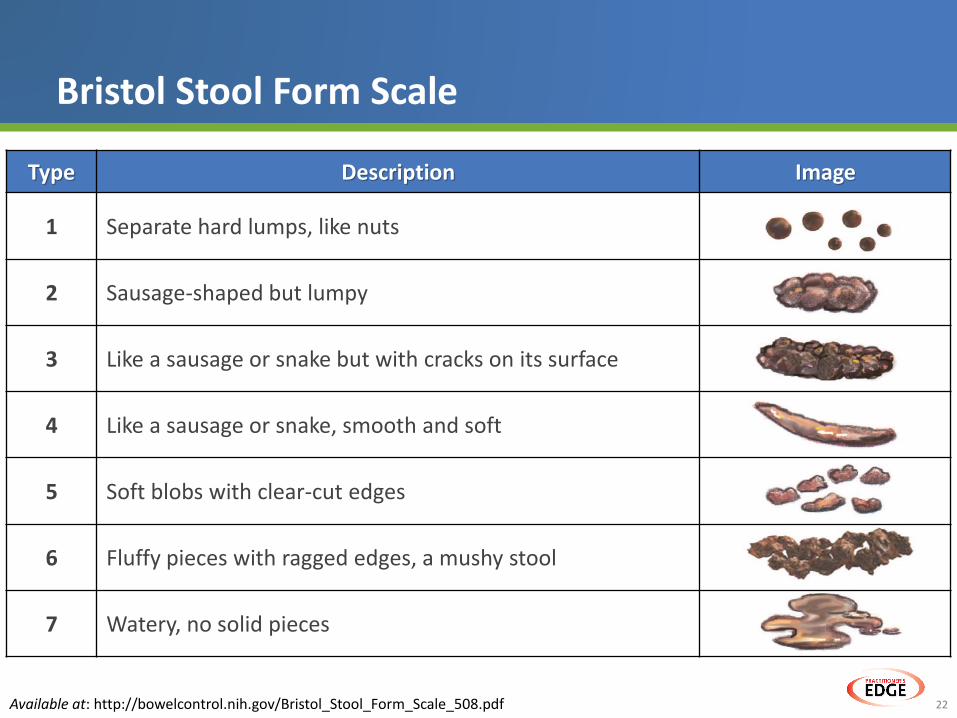
Bristol Stool Form Scale
Available at: http://bowelcontrol.nih.gov/Bristol_Stool_Form_Scale_508.pdf
Type Description Image
1 Separate hard lumps, like nuts
2 Sausage-shaped but lumpy
3 Like a sausage or snake but with cracks on its surface
4 Like a sausage or snake, smooth and soft
5 Soft blobs with clear-cut edges
6 Fluffy pieces with ragged edges, a mushy stool
7 Watery, no solid pieces

23
Assessment Tools and Outcome Measures
*Could theoretically be collected by an investigator as well as by the patient (eg, defecation frequency; †Reports coming directly from patients about how they feel or function in relation to a health condition and its therapy without interpretation by healthcare professionals or anyone else.;‡Patient-reported outcome measures that directly relate to the patient’s distress and the impact on their daily activities or QOL and are most obviously caused by OIC.
Neurogastroenterol Motil. 2014 October ; 26(10): 1386–1395.
Objective Measures*
• Bowel movement frequency/change in bowel movement frequency
• Time to laxation
• Laxation within 4 hours
• Gastrointestinal (or short bowel) transit time
• Bristol Stool Form scale
Patient-Reported Outcomes†
• Bowel Function Index
• Patient Assessment of Constipation –Symptoms
• Global Clinical Impression of Change
Patient-Reported Burden‡
• Constipation distress
• Patient Assessment of Constipation – QOL

25
Bowel Function Index (BFI)
Argoff CE, et al. Pain Medicine. 2015;16(12):2324-2337.
1. Ease of defecation (NAS) during the last 7 days according to patient assessment:
0 = easy / no difficulty100 = severe difficulty
2. Feeling of incomplete bowel evacuation (NAS) during the last 7 days according to patient assessment:
0 = not at all100 = very strong
3. Personal judgement of patient (NAS) regarding constipation during the last 7 days:
0 = not at all100 = very strong

26
Patient Assessment of Constipation Symptoms (PAC-SYM)
Slappendel R, et al. Eur J Pain. 2006;10(3):209-217.
Domain Item
Abdominal
• Discomfort in your stomach
• Pain in your stomach
• Bloating in your stomach
• Stomach cramps
Rectal
• Painful bowel movements
• Rectal burning during or after bowel movement
• Rectal bleeding or tearing during or after bowel movement
Stool
• Incomplete bowel movements, like you did not “finish”• Bowel movements that were too hard• Bowel movements that were too small• Straining or squeezing to try to pass a bowel movement• Feeling like you had to pass a bowel movement but could not
(“false alarm”)

27
Differential Diagnosis of Constipation
Category Cause
Functional Diet, motility disturbance, sedentary
StructuralAnorectal fissures, hemorrhoids, diverticulitis, mass lesions with obstruction
MetabolicDiabetes, hyperparathyroidism, hypercalcemia, hypokalemia, hypothyroidism, uremia, pregnancy
Neurogenic Stroke, MS, spinal cord injury, brain injury
Psychogenic Anxiety, depression, somatization
DrugsOpioids, anticholinergics, antidepressants, calcium channel blockers, psychotropics, diuretics, levodopa
MS, multiple sclerosis.Arce, et al. Am Fam Physician. 2002;65(11):2283-90.

28
Barriers to the Diagnosis of OIC
• Lack of disease awareness
• Failure to ask about constipation
• Screening based on Rome criteria may be inadequate
• Absence of universal diagnostic criteria
• Absence of a standard treatment protocol
• Reluctance to disclose symptoms to clinicians
Clinician-Related Barriers Patient-RelatedBarriers
Nelson, et al. Ther Adv Chronic Dis. 2016;7(2) :121-134.

29
Treatment of OIC

30
▪ Having established that Jane’s symptoms are primarily due to opioid therapy, what type of initial treatment would you recommend to address her symptoms of constipation?
▪ At what point would you initiate Jane on some form of prescription therapy?
Case Study #1: Discussion

31Webster LR. Pain Med. 2015;16 Suppl 1:S16-21.
Treatment Type Examples Comments
Stool softeners • Docusate
• Ease passage of stool
• May be prescribed in combination
with a laxative
Laxatives
Osmotic
agents
• Polyethylene glycol
solution
• Retain water in the gut• May be mixed with electrolytes to
avoid dehydration
Stimulants• Senna
• Bisacodyl• Increase intestinal motility
Bulk • Not recommended for OIC
Over-the-Counter Treatment Options

32
Criteria for Initiating Prescription Treatment of OIC
Argoff CE, et al. Pain Medicine. 2015;16(12):2324-2337.Ueberall et al. J Int Med Res. 2011;39(1):41-50.
Prescription treatments should be considered for patients with a BFI score ≥30 and inadequate response to first-line intervention
Re
lati
ve C
um
ula
tive
Fr
eq
ue
ncy
(%
)
0 10 20 30 40 50 60 70 80 90 100BFI Score
100
90
80
70
60
50
40
30
20
10
0
ReferencePopulation
OICPopulation
7.9%
28.8
95.0%

33
Prescription Treatments for OIC
*Indicated to accelerate time to upper and lower GI recovery following partial large or small bowel resection surgery with primary anastomosis
PGE1, prostaglandin E1; PEG, Polyethylene Glycol; BBB, blood-brain barrier.
Agent Mechanism of Action
Lubiprostone• Bicyclic fatty acid derived from PGE1• Increases fluid secretion in the GI tract
Naloxone/ oxycodone
• Naloxone is local (GI) µ-opioid antagonist• Differential bioavailability between naloxone and oxycodone
allows for central effects with diminished peripheral effects
Naloxegol• Polyethylene glycol derivative of naloxone• PEG moiety reduces ability to pass BBB
Methylnaltrexone• Quaternary N-methyl derivative of naltrexone• Decreased lipid solubility reduces ability to cross the BBB
Naldemedine• Naltrexone derivative• Additional side chain confers increased molecular weight and
polar surface area, reducing ability to cross the BBB
Alvimopan* • Competitively binds to GI tract mu-opioid receptors

34
Effect of Lubiprostone Treatment on SBM: 12-Week Response Rates
*P<.05; †Overall responders were defined as reporting at least a moderate response (≥1 SBM from baseline frequency) as well as a full response (≥3 SBMs/wk) for ≥9 of 12 wks.
BID, twice daily; SBM, spontaneous bowel movement.
Jamal MM, et al. Am J Gastroenterol 2015; 110:725-732.
Pe
rce
nta
ge o
f SB
MR
esp
on
der
s
0 2 4 6 8 10 12Treatment Week
70
60
50
40
30
20
10
0
Lubiprostone 24 µg BID
Placebo BID
Overall†
P=.030
27.1
18.9
**

35
Treatment with Lubiprostone Improves Symptoms of OIC
*Straining, for stool consistency; †stool consistency, for straining; ‡abdominal bloating, for abdominal discomfort; and §abdominal discomfort , for abdominal bloating.
Jamal MM, et al. Am J Gastroenterol 2015; 110:725–732.
Straining
Ove
rall
Me
an C
han
ge
fro
m B
ase
line
0
−0.5
−1.0
−1.5
−2.0
−2.5
Stool Consistency
ConstipationSeverity
AbdominalBloating
AbdominalDiscomfort
Placebo BID
Lubiprostone 24 µg BID
P=.004
P=.004*
P<.001
P<.001†
P=.010P=.155
P=.155‡
P=.063
P=.127§

36
Most Common Treatment-related AEs (>1%) with Lubiprostone
Spierings ELH, et al. Pain Pract. 2015;16:985-993.
Adverse Event (AE) Preferred TermLubiprostone 24 µg BID
(N = 439) n (%)
At least 1 treatment-related AE 108 (24.6)
Nausea 22 (5.0)
Diarrhea 20 (4.6)
Headache 7 (1.6)
Vomiting 6 (1.4)
Abdominal pain lower 5 (1.1)
Flatulence 5 (1.1)
Muscle spasms 5 (1.1)
Back pain 5 (1.1)
Anemia 5 (1.1)

37
Naloxone Treatment in Combination with Oxycodone (OXN)
*Paired t-test: OXN2001 P=.0002; OXN9001 P<.0001; and Total P<.0001.
Koopmans, et al. Curr Med Res Opin 2014; 30:2389-2396.
Combination treatment with a fixed 2:1 ratio of prolonged-release oxycodone/naloxone improved bowel function and reduced the use of laxatives in patients with OIC.
OXN2001• Patients with cancer-related
pain randomized to OXN PR for 4 weeks
OXN9001• Patients with non-cancer-
related pain randomized to OXN PR for 12 weeks.
Screening Start of End ofTreatment Point Treatment
Me
an B
FI S
core
100
90
80
70
60
50
40
30
20
10
0
OXN2001
OXN9001
Total
*

38
Safety of Naloxone and Oxycodone
Sandner-Kiesling A, et al. Int J Clin Prac. 2010;64(6):763-774.
Adverse EventOxycodone PR/Naloxone PR
(N=238) n (%)
Any AE 211 (81.8)
GI disorders 94 (36.4)
Constipation 40 (15.5)
Diarrhea 18 (7.0)
General disorders and administration site conditions 28 (10.9)
Infections and infestations 104 (40.3)
Musculoskeletal and connective tissue disorders 104 (40.3)
Arthralgia 23 (8.9)
Back pain 35 (13.6)
Osteoarthritis 16 (6.2)
Nervous system disorders 58 (22.5)
Headache 18 (7.0)
Psychiatric disorders 31 (12.0)
Respiratory, thoracic and mediastinal disorders 34 (13.2)
Skin and subcutaneous tissue disorders 41 (15.9)

39
Response to Treatment with Naloxegol
ITT, intention-to-treat.
Chey, et al. NEJM. 2014; 370:2387-2396.
29.4 29.3
40.8
34.9
44.439.7
0
10
20
30
40
50
Study 04 Study 05
Pat
ien
ts (
%)
Placebo Naloxegol, 12. 5 mg Naloxegol, 25 mg
Response Rates in the ITT Population
**
*
Relative Risk (95% CI) 1.38 (1.06-1.80) 1.51 (1.17-1.95) 1.19 (0.91-1.55) 1.35 (1.05-1.74)
P Value 0.02 0.001 0.20 0.02
No. Needed to Treat 8.8 6.7 17.8 9.7
N=214 N=213 N=214 N=232 N=232 N=232

40
Response to Naloxegol in Patients with an Inadequate Response to Laxatives
LIR, laxative inadequate response.
Chey, et al. NEJM. 2014; 370:2387-2396.
28.8 31.4
42.6 42.448.7 46.8
0
10
20
30
40
50
60
Study 04 Study 05
Pat
ien
ts (
%)
Placebo Naloxegol, 12. 5 mg Naloxegol, 25 mg
Response Rates in the LIR Population
** *
Relative Risk (95% CI) 1.48 (1.04-2.11) 1.69 (1.21-2.37) 1.35 (0.97-1.88) 1.49 (1.08-2.06)
P Value .03 .002 .07 .01
No. Needed to Treat 7.2 5.0 9.1 6.5
N=118 N=115 N=117 N=121 N=125 N=124

41
Safety of Treatment with Naloxegol
aPercentage data based on the number of patients in each treatment group and category; bOccurring during the treatment period; cOnly includes events that included permanent discontinuation of IP.IP, investigation product; LIR, laxative-inadequate responder.
Tack, et al. United Eur Gastroenterol J. 2015, Vol. 3(5) 471–480.
Any Event, n (%)b
Patients, n (%)a
Placebo(n = 238)
Naloxegol 12.5 mg(n = 237)
Naloxegol 25 mg(n = 241)
Any AE 119 (50.0) 120 (50.6) 152 (63.1)
Serious AE 13 (5.5) 7 (3.0) 8 (3.3)
AE leading to discontinuation of IPc 11 (4.6) 8 (3.4) 24 (10.0)
Death 0 0 0
Treatment-emergent AEs (≥3% in any treatment group)
Abdominal pain 13 (5.5) 18 (7.6) 38 (15.8)
Diarrhea 12 (5.0) 16 (6.8) 25 (10.4)
Fall 8 (3.4) 6 (2.5) 2 (0.8)
Nausea 7 (2.9) 15 (6.3) 20 (8.3)
Vomiting 5 (2.1) 6 (2.5) 9 (3.7)
Back pain 5 (2.1) 5 (2.1) 9 (3.7)
Headache 4 (1.7) 8 (3.4) 10 (4.1)
Flatulence 4 (1.7) 5 (2.1) 15 (6.2)
Upper abdominal pain 4 (1.7) 1 (0.4) 8 (3.3)
Hyperhidrosis 0 1 (0.4) 10 (4.1)

42
Efficacy of Methylnaltrexone
RFBM, rescue-free bowel movement; MNTX, methylnaltrexone; OLE, open-label extension.
Viscusi, et al. Reg Anesth Pain Med 2016;41: 93–98.
9.7
45.9
0
10
20
30
40
50
60
70
80
PlaceboTreatmentDuring RCT
(n=134)
MNTXTreatmentDuring OLE
(n=134)
Pat
ien
ts W
ith
RFB
M W
ith
in
4 H
ou
rs o
f D
ose
(%
)
9.0
34.5
0
10
20
30
40
50
60
70
80
PlaceboTreatmentDuring RCT
(n=134)
MNTXTreatmentDuring OLE
(n=134)
Infe
ctio
ns
Re
sult
ing
in R
FBM
Wit
hin
4 H
ou
rs o
f D
ose
(%
)

43
Efficacy of Oral Methylnaltrexone for OIC in Patients with Chronic Noncancer Pain
Dosing days resulting in RFBMs within 4hours of dosing (%) Responders during ≥ 9 of 12weeks (%)
*P<.05; **P = .03; †P = .005; ‡P = .02
Adapted from: Rauck et al. Pain Practice. 2017;17:820–828.
Do
sin
g d
ays
that
re
sult
ed
in R
FBM
sw
ith
in 4
h (
%)
0 1 2 3 4 5 6 7 8 9 10 11 12Time (wk)
35
30
25
20
15
10
* *
** *
* **
*
*** *
**
*
* *
*
Methylnaltrexone 150 mgMethylnaltrexone 450 mg
Methylnaltrexone 300 mgPlacebo
QD Period PRN Period
40.5
29.9
0
10
20
30
40
50
60
70
80
90
100
MNTX 450 mg(n = 200)
Placebo(n = 201)
Ove
rall
resp
on
de
rs (
%)
‡

44
Safety of Methylnaltrexone Treatment
▪ Meta-analysis of 7 studies found that patients treated with MNTX experienced the following:
▪ Incidence of MNTX-related serious AEs was 0.2%
RR 95% CI N I2
Abdominal pain 2.38 1.75-3.23 1,412 60%
Nausea 1.27 0.90-1.78 1,412 12%
Diarrhea 1.45 0.94-2.24 1,258 45%
RR, respiratory rate.
Siemens W, et al. Therapeutics and Clinical Risk Management. 2016;12:401-412.

45
Treatment with Naldemedine for OIC Is Associated with a Higher Response Rate vs Placebo
Hale et al. Lancet Gastroenterol Hepatol 2017;2:555–64.
COMPOSE-1
100
90
80
70
60
50
40
30
20
10
0
Pat
ien
ts (
%)
COMPOSE-2
47.6%n=273
52.5%n=276
34.6%n=272
33.6%n=274
Difference: 13.0% (4.8–21.3)
P=.0020
Difference: 18.9% (10.8–27.0)
P<.0001
Naldemedine
Placebo

46
Agent Mechanism of ActionClinical Phase
AxelopranPeripheral µ-opioid receptor antagonist
(PAMORA)
II
Alvimopan III
Linaclotide Guanylyl cyclase C receptor agonist II
TRV-130µ-opioid agonist (stabilizes G-protein receptor
conformations, prevents β-arrestin-2 activation)III
Prucalopride Selective, high-affinity 5HT4 receptor agonist III
Emerging Agents for OIC Treatment

47
The Impact of OIC on Long-term Pain Management

48
▪ John, 67-year-old man, presents for annual visit
▪ Initiated on opioid therapy for chronic pain associated with severe osteoarthritis beginning one year ago
▪ Symptoms of pain were improved during the first several months
▪ Patient reports the following over the past three months:
– Significantly diminished capacity for walking, stooping, and lifting/carrying objects
– Difficulty performing basic household chores
Case Study #2: Poor Adherence to Opioid Treatment

49
▪ What are the possible underlying reasons for the inadequacy of John’s level of pain control?
▪ What do you suspect is the most likely explanation?
Case Study #2: Discussion

50
Medication Nonadherence Among Patients Taking Opioid Medication
• 57% of patients reported having taken less opioid medication than prescribed or discontinuing medication due to side effects.
• Among these individuals, 90% reported OIC as the primary reason.
90.0
22.3
26.4
20.5
Constipation
Sedation
Nausea andvomiting
Other
Rauck RL, et al. Pain Practice. 2016.

51
OIC Interference with Pain Management
19.4
31.7
44.1
4.8
0
10
20
30
40
50
Pain adequatelymanaged
Pain mostlymanaged
Pain moderatelymanaged
Pain not at allmanaged
Pat
ien
ts R
ep
ort
ing
(%)
LoCasale RJ, et al. J Manag Care Spec Pharm. 2016;22(3):236-245.

52
Patient vs HCP Perceptions of OIC Interference with Pain Management
HCP, healthcare provider. LoCasale RJ, et al. J Manag Care Spec Pharm. 2016;22(3):236-245.
Comparison between patient and HCP responses revealed a discordance between their perceptions of how much OIC interfered with adequate pain management.
4.8 3.9
43.9 40.8
31.6 41.7
19.813.6
0
10
20
30
40
50
60
70
80
90
100
Baseline (n=415) Week 24 (n=103)
Pat
ien
ts (
%)
Complete interference Moderate interference
Little interference No interference
Patient Report: How Much Does Constipation Interfere with Ability to Control Pain
1.7 1.0
25.5 26.2
46.3 50.5
26.5 22.3
0
10
20
30
40
50
60
70
80
90
100
Baseline (n=415) Week 24 (n=103)
HC
Ps
(%)
Not at all managed Moderately managed
Mostly managed Adequately managed
HCP Report: How Much Does OIC Interfere with This Patient’s Adequate Pain Management

53
▪ Upon further questioning, John admits that he often reduces his dose of opioid medication due to the side effects he has been experiencing. He reports that he has been particularly bothered by bouts of constipation, which have increased in frequency since he first began taking opioids.
▪ What approach would you take to addressing John’s lack of adherence to his prescribed regimen?
Case Study #2: Discussion

54
Agreement of Patient- and HCP-Reported OIC Symptoms
LoCasale RJ, et al. J Manag Care Spec Pharm. 2016;22(3):236-245.
The proportion of HCPs who had observed or discussed each OIC symptom reported by patients as being of moderate or greater severity ranged from 1% to 41%.
1.3
4.1
6.0
7.3
9.2
11.3
13.5
14.3
15.8
20.6
27.0
28.5
37.0
40.7
0 5 10 15 20 25 30 35 40 45
Vomiting
GERD
Nausea
Rectal burning/bleeding or tearing duration or after BM
Headache or migraine
Feeling that had to pass but couldn't
Flatulence
Abdominal discomfort
BMs too small
Abdominal bloating
Painful BMs
Incomplete BMs
Straining/squeezing to try to pass
BMs too hard
OIC Symptoms HCP Has Observed or Discussed with Patient, n (%)
OIC
Sym
pto
ms
Re
po
rte
d a
s ≥
Mo
de
rate
by
Pat
ien
t n = 190
n = 173
n = 133
n = 126
n = 96
n = 74
n = 67
n = 63
n = 53
n = 43
n = 34
n = 28
n = 19
n = 6

55
Improving Adherence to Opioid Therapy
▪ A good patient-doctor relationship
▪ Defined treatment objectives
▪ Tools for disease prognosis
▪ Simple treatment regimens
▪ Identification of high risk for AEs or drug abuse
▪ AE management
▪ Monitoring treatment success
▪ Antidepressant management
▪ Community support
▪ Education for patients and caregivers
Graziottin, et al. Pain Practice. 201;574-581.

56
Physician-Patient Communication
Among those who felt uncomfortable talking about OIC with their HCP, reasons cited included“previously discussed in an earlier visit” (32%) and “I feel embarrassed” (68%).
71
90
49
80
29
10
51
20
Has your doctor discussed the side effectsof your pain medication when prescribing?
If yes, was OIC one of these?
Has your doctor discussed the subject ofOIC in follow up visits?
Do you feel comfortable talking about OICwith your HCP?
Yes No
Patients (%)
Rauck RL, et al. Pain Practice. 2016.

57
Assessing History of Constipation and Opioid Use: Asking the Right Questions
▪ Over the past 2 weeks, how many BMs were spontaneous?
▪ Ideally, how often would you like to have BMs?
▪ Since starting opioid medication, have you been experiencing constipation or worsening of current constipation?
▪ How long after did you begin experiencing constipation?
▪ In past 7 days, did you change how you used your opioid medication(s) so that you could have BMs?
LoCasale RJ, et al. J Manag Care Spec Pharm. 2016;22(3):236-245.

58
▪ OIC is a frequent side effect of opioid treatment that negatively impacts patient QOL and can lead to poor adherence and inadequate pain management
▪ If left untreated, OIC may lead to the development of severe bowel dysfunction, increased surgical events, ED visits, and hospitalizations
▪ In addition to nonpharmacologic treatments and OTC laxatives, prescription medications are available that have shown good efficacy for the improvement of OIC symptoms with minimal side effects
▪ Patients receiving opioids should be routinely assessed for signs of constipation and risk for poor opioid adherence with the overall goal of minimizing OIC impact while ensuring adequate pain control
Summary

59
Questions and Answers

60
Thank You!

61
Chronic Pain Among Adults in the US
Available at: http://www.gallup.com/poll/154169/chronic-pain-rates-shoot-until-americans-reach-late-50s.aspx

62
Impact of Persistence and Bothersomeness of Pain on Health Status and Disability
Health status Disability
Nahin, et al. J Pain. 2015;16(8):769–780.

63
Differential µ-opioid Receptor Tolerance in the GI Tract
Nelson, et al. Ther Adv Chronic Dis. 2016;7(2) :121-134.

64
Impact on Workplace Productivity
Survey QuestionHours
(mean ± SD)
How many hours did you miss from work because of problems associated with your constipation?
6.2 (13.9)
How many hours did you miss from work because of any other reason?
1.6 (5.3)
How many hours did you actually work? 36.3 (13.7)
Coyne KS, et al. Clinicoecon Outcomes Res. 2014;6:269-281.
65
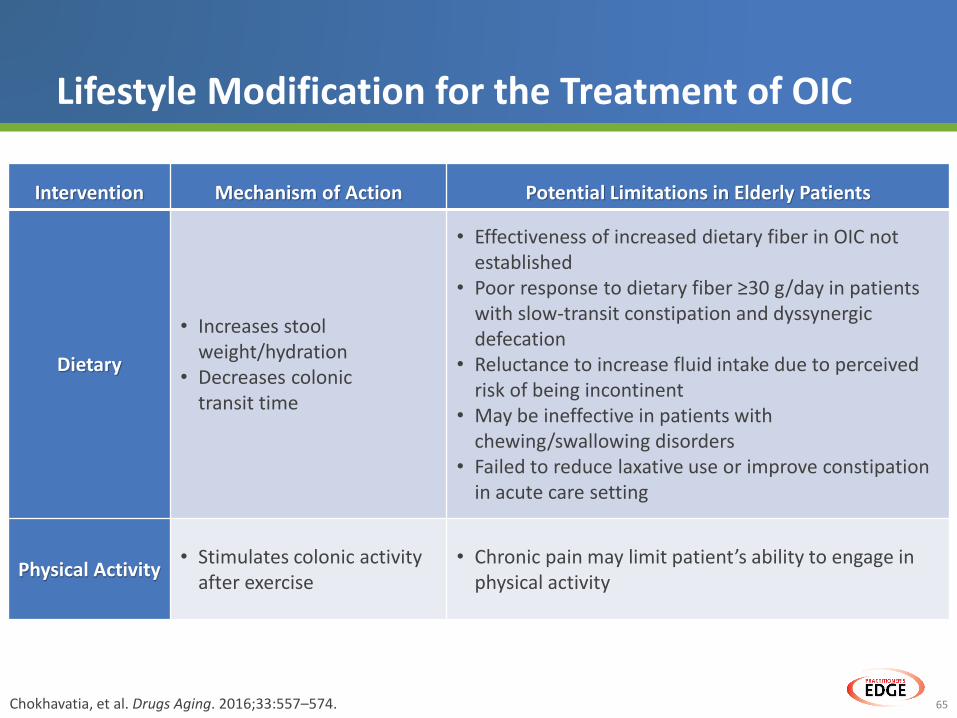
Lifestyle Modification for the Treatment of OIC
Chokhavatia, et al. Drugs Aging. 2016;33:557–574.
Intervention Mechanism of Action Potential Limitations in Elderly Patients
Dietary
• Increases stool weight/hydration
• Decreases colonic transit time
• Effectiveness of increased dietary fiber in OIC not established
• Poor response to dietary fiber ≥30 g/day in patients with slow-transit constipation and dyssynergic defecation
• Reluctance to increase fluid intake due to perceived risk of being incontinent
• May be ineffective in patients with chewing/swallowing disorders
• Failed to reduce laxative use or improve constipation in acute care setting
Physical Activity• Stimulates colonic activity
after exercise• Chronic pain may limit patient’s ability to engage in
physical activity

66
Effect of Naloxegol Treatment on Pain and Daily Opioid Use
Webster, et al. AAPM Annual Meeting Abstracts. 2016;219.