improving dignity for older people in hospital - kcl.ac.uk · pdf file• non-participatory...
TRANSCRIPT
Improving Dignity for
Older People in HospitalChristine Norton PhD MA RN
Florence Nightingale Professor of Nursing
Imperial Healthcare & King’s College London
Team: Marcelle Tauber-Gilmore, Sue Procter, Corina
Naughton, Zainab Zahran, Gulen Addis + students
Aim of the study
To improve the delivery of dignity in the care
to older adults during acute hospital
admission through a staff led intervention
Research Questions
1) Can a supported dignity programme impact on
the quality of interaction between staff and
older patients and improve patient experience?
2) Can improvement be sustained once support
is withdrawn?
Background
• Dignity a particular issue in acute care
(Francis and others)
• Pace of modern hospitals is challenging to
dignity and person centred care
• We obtained 2 year funding from Burdett
Trust for Nursing
• 3 phases:
– Systematic review
– Interviews, survey and observations
– Dignity intervention
Dignity definitionThe Steering Group’s agreed definition of dignity:
“Dignity is concerned with how people feel, think and behave in relation to the worth or value of themselves and others.
Dignity in care means the kind of care, which supports and promotes, and does not undermine or erode, a person’s self-respect regardless of any difference.
[Patient] 'Being treated like I was somebody'.”
Incorporated:
-The Royal College of Nursing's dignity definition (2008) and
-Social Care Institute for Excellence (SCIE) Dignity in Care Research Overview Guide using Policy Research Institute on Ageing and Ethnicity (PRIAE) and Help the Aged, (2001)
-Opinions of the Steering Group (2014)
Review and interviews• Systematic review: interventions for dignity
in acute care: none!! (Lots of descriptions
and recommendations but never tested).
Plus no outcome measures tested.
(Zahran et al, J Clin Nursing 2016)
• Views of older people and staff about
dignity. Agreed about what dignity is. Care
inconsistent and continence a challenge.
Staffing levels and organisational culture
central. Lack of training. (Tauber et al, J
Clin Nursing 2017).
• “maybe its more recognisable when its not
there” (doctor)
• “he [nurse] spoke, he held me, he cuddled
me, and encouraged me to scream it out, to
let it out. And I did. And the panic passed”.
(Patient 6)
• “when you are in hospital you forget about
privacy, you’re here as a patient” (Patient 1)
• “I asked for a bed pan because I was so
exhausted. A girl (HCA) came in, turned off
the buzzer and said: we are doing handover,
no-one can help you now” (Patient 5)
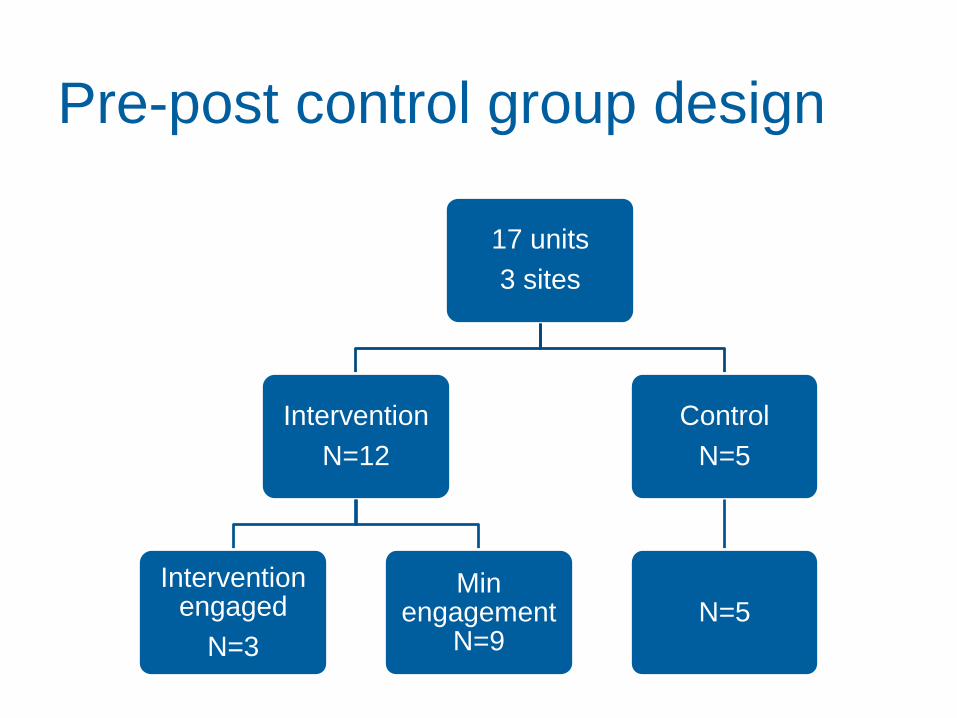
Pre-post control group design
17 units
3 sites
Intervention
N=12
Intervention engaged
N=3
Min engagement
N=9
Control
N=5
N=5
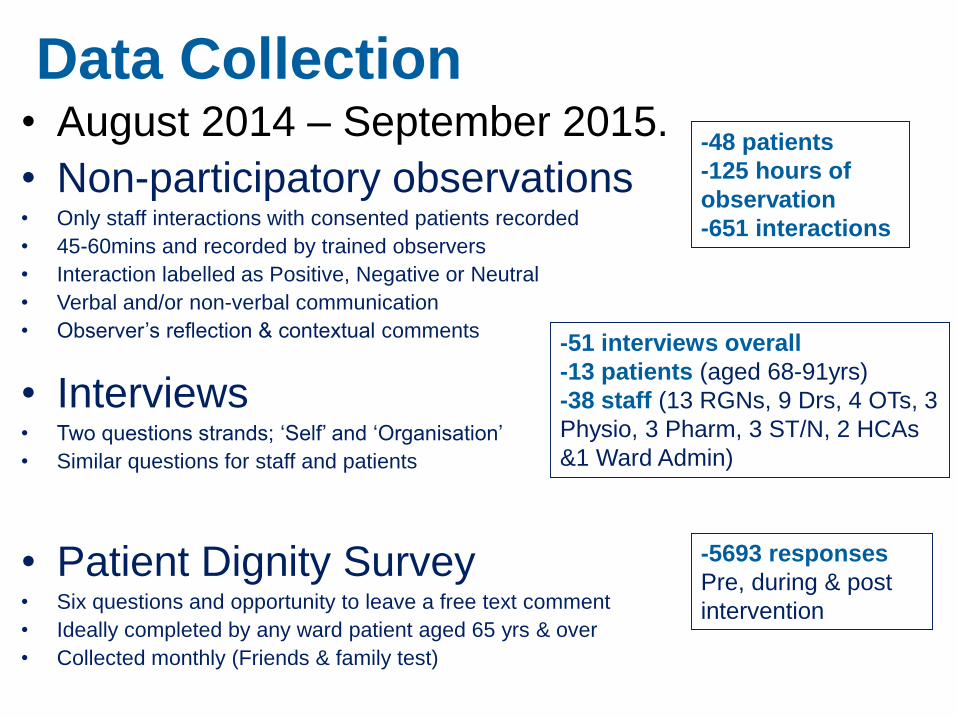
Data Collection• August 2014 – September 2015.
• Non-participatory observations• Only staff interactions with consented patients recorded
• 45-60mins and recorded by trained observers
• Interaction labelled as Positive, Negative or Neutral
• Verbal and/or non-verbal communication
• Observer’s reflection & contextual comments
• Interviews• Two questions strands; ‘Self’ and ‘Organisation’
• Similar questions for staff and patients
• Patient Dignity Survey• Six questions and opportunity to leave a free text comment
• Ideally completed by any ward patient aged 65 yrs & over
• Collected monthly (Friends & family test)
-48 patients
-125 hours of
observation
-651 interactions
-51 interviews overall
-13 patients (aged 68-91yrs)
-38 staff (13 RGNs, 9 Drs, 4 OTs, 3
Physio, 3 Pharm, 3 ST/N, 2 HCAs
&1 Ward Admin)
-5693 responses
Pre, during & post
intervention
Time
:
Interaction
Description:
Between: Code: Verbal/N
on-
Verbal:
Length of
Interaction
Reflections
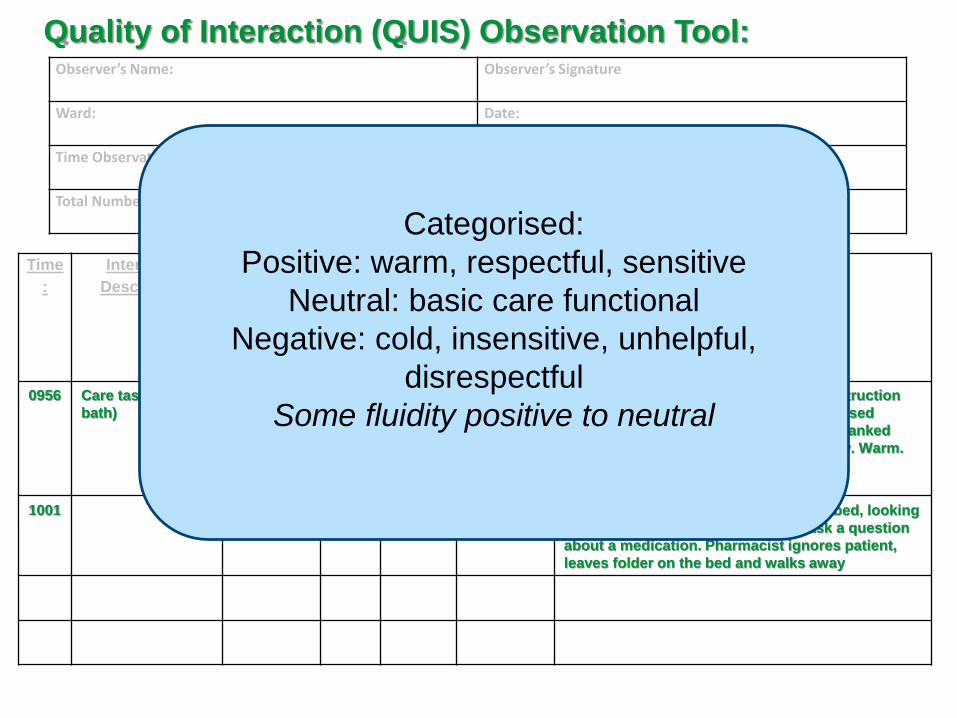
0956 Care task (bed
bath)
Nurse
& Patient
+ V Long Behind curtain. Lovely explanation & instruction
from nurse, encouragement pt. Pt expressed
preference for shave, nurse agreed. Pt thanked
nurses, acknowledged by nurse. Friendly. Warm.
Social conversation
1001 Pharmacist
& Patient
- NV Brief Pharmacist stood at the end of patient bed, looking
at bed side folder. Patient trying to ask a question
about a medication. Pharmacist ignores patient,
leaves folder on the bed and walks away
Observer’s Name: Observer’s Signature
Ward: Date:
Time Observation Period Started: Time Observation Period Finished:
Total Number of Interactions: Positive: Neutral: Negative:
Quality of Interaction (QUIS) Observation Tool:
Categorised:
Positive: warm, respectful, sensitive
Neutral: basic care functional
Negative: cold, insensitive, unhelpful,
disrespectful
Some fluidity positive to neutral
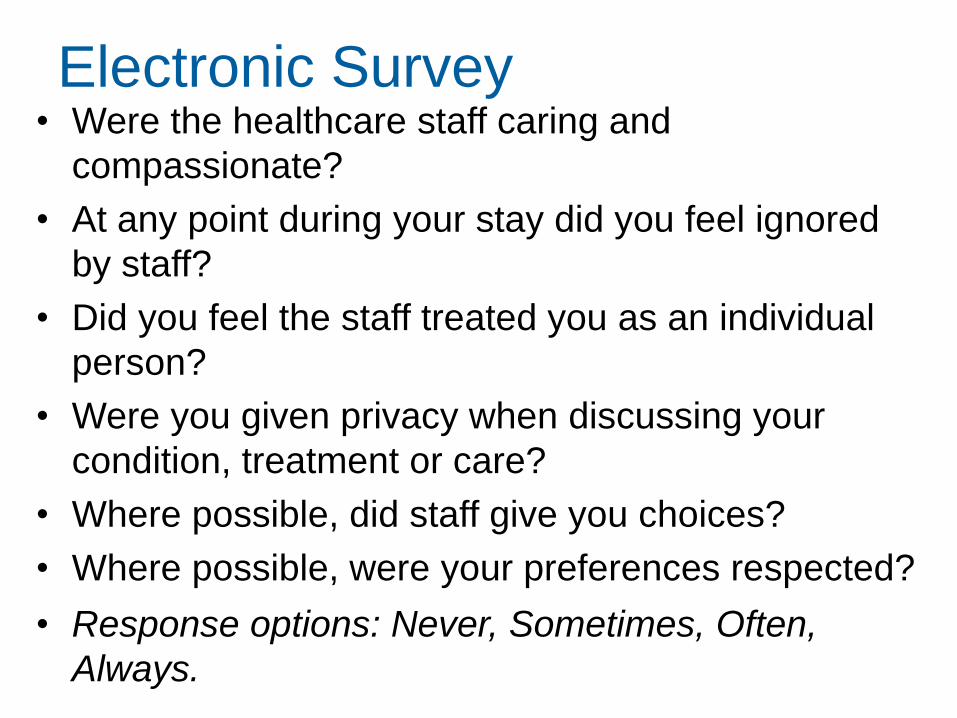
Electronic Survey• Were the healthcare staff caring and
compassionate?
• At any point during your stay did you feel ignored
by staff?
• Did you feel the staff treated you as an individual
person?
• Were you given privacy when discussing your
condition, treatment or care?
• Where possible, did staff give you choices?
• Where possible, were your preferences respected?
• Response options: Never, Sometimes, Often,
Always.
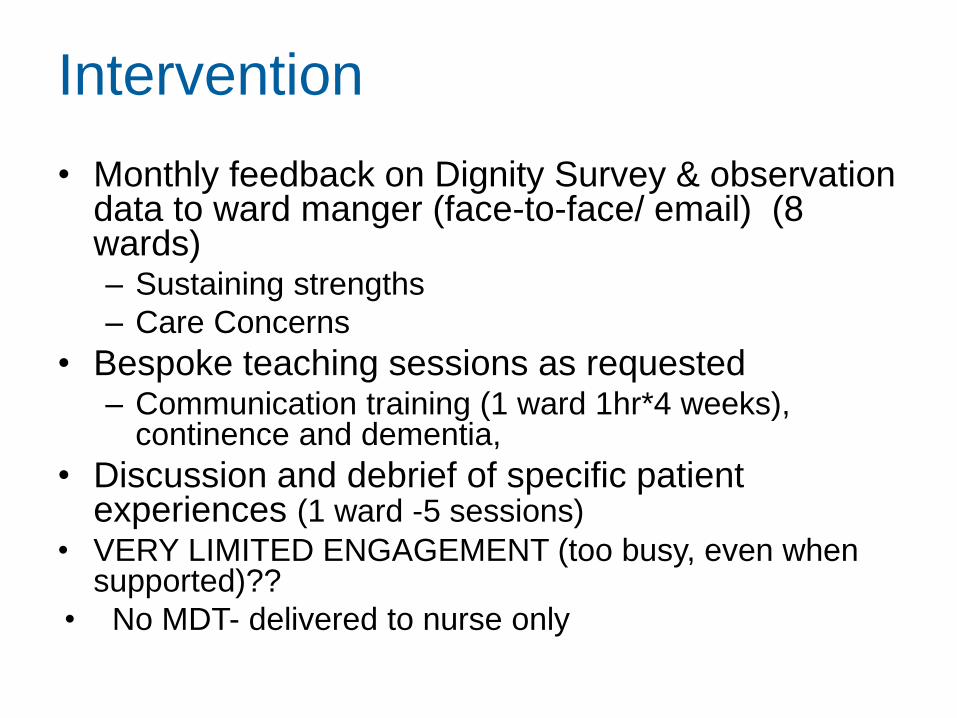
Intervention
• Monthly feedback on Dignity Survey & observation data to ward manger (face-to-face/ email) (8 wards)– Sustaining strengths
– Care Concerns
• Bespoke teaching sessions as requested– Communication training (1 ward 1hr*4 weeks),
continence and dementia,
• Discussion and debrief of specific patient experiences (1 ward -5 sessions)
• VERY LIMITED ENGAGEMENT (too busy, even when supported)??
• No MDT- delivered to nurse only
Bespoke dignity feedback by
ward
• Staff Reaction to feedback:
• Shock, dismay
• More doom and gloom
• But
• Can try harder
• Did not realise that is how we came
across
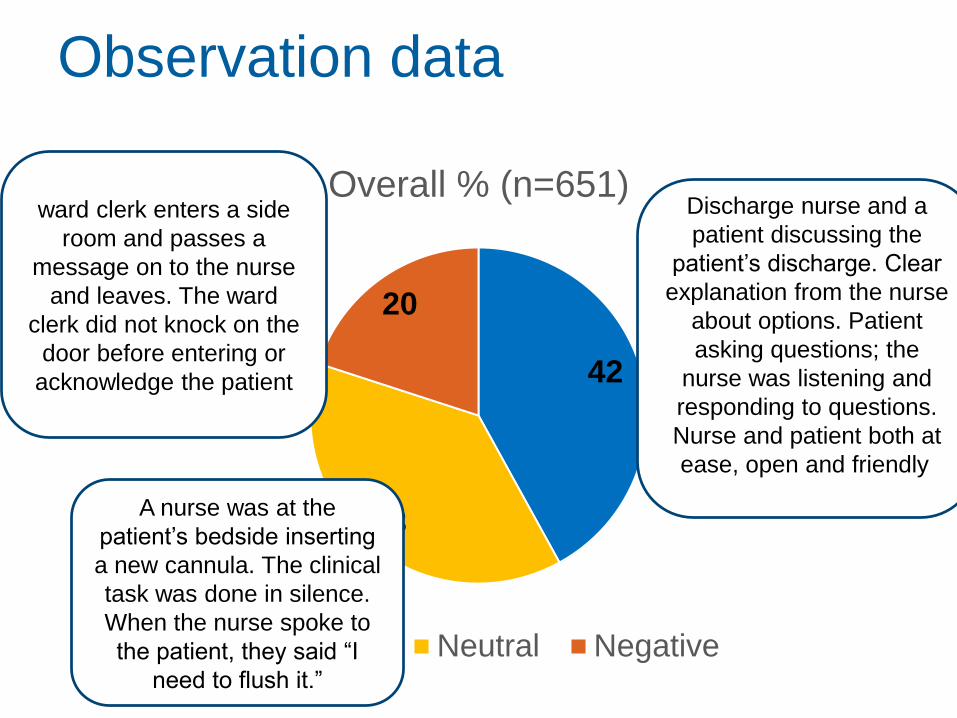
Observation data
42
38
20
Overall % (n=651)
Positive Neutral Negative
A nurse was at the
patient’s bedside inserting
a new cannula. The clinical
task was done in silence.
When the nurse spoke to
the patient, they said “I
need to flush it.”
Discharge nurse and a
patient discussing the
patient’s discharge. Clear
explanation from the nurse
about options. Patient
asking questions; the
nurse was listening and
responding to questions.
Nurse and patient both at
ease, open and friendly.
ward clerk enters a side
room and passes a
message on to the nurse
and leaves. The ward
clerk did not knock on the
door before entering or
acknowledge the patient
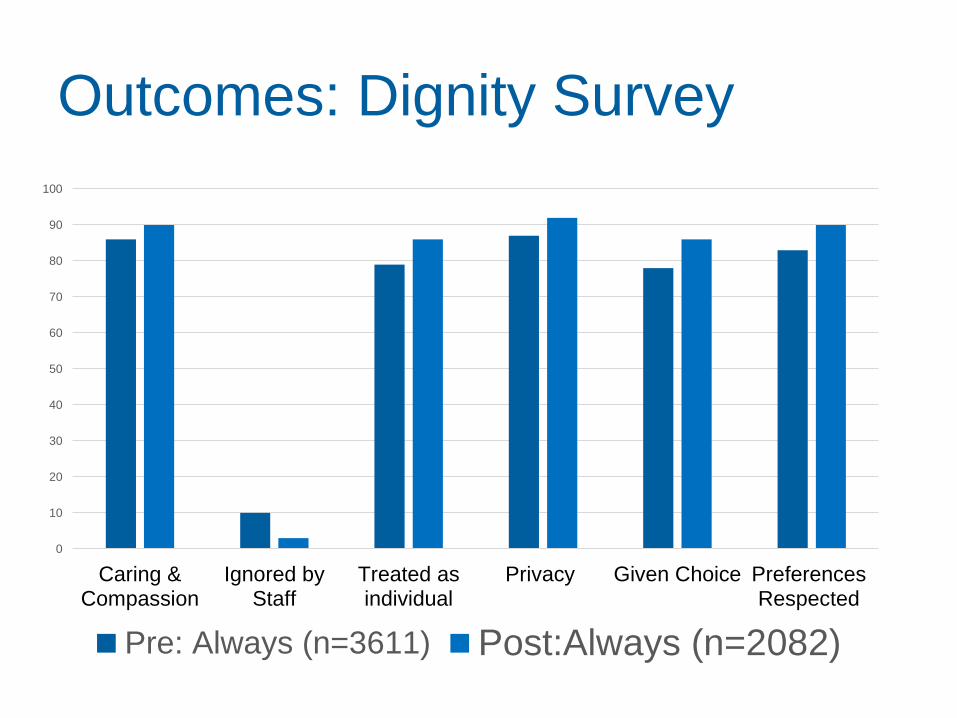
Outcomes: Dignity Survey
0
10
20
30
40
50
60
70
80
90
100
Caring &Compassion
Ignored byStaff
Treated asindividual
Privacy Given Choice PreferencesRespected
Pre: Always (n=3611) Post:Always (n=2082)
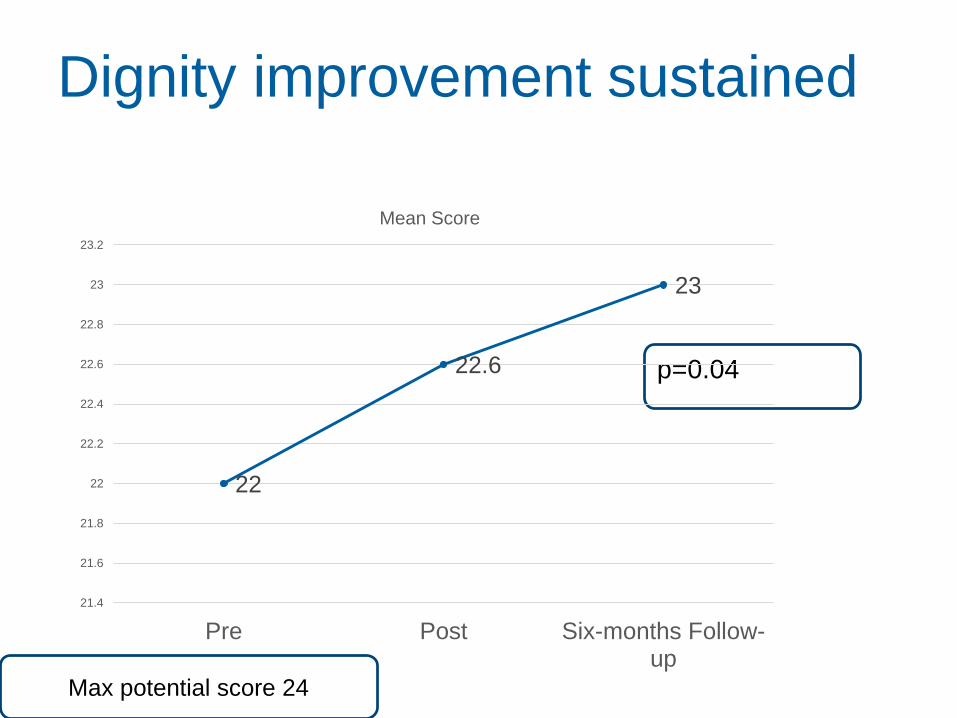
Dignity improvement sustained
p=0.04
22
22.6
23
21.4
21.6
21.8
22
22.2
22.4
22.6
22.8
23
23.2
Pre Post Six-months Follow-up
Mean Score
Max potential score 24
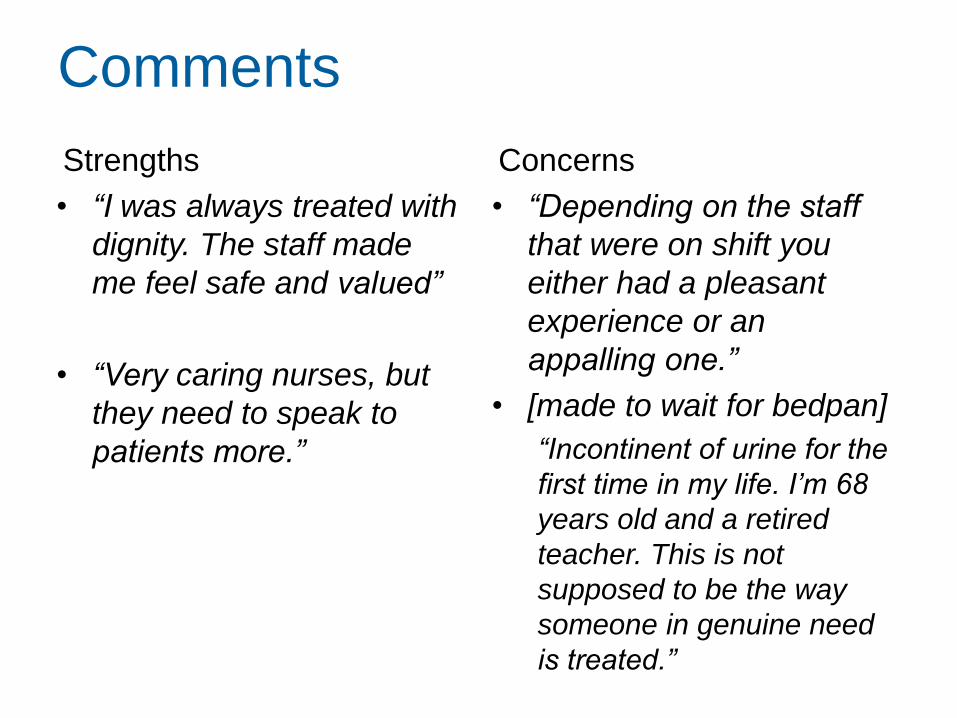
Comments
Strengths
• “I was always treated with
dignity. The staff made
me feel safe and valued”
• “Very caring nurses, but
they need to speak to
patients more.”
Concerns
• “Depending on the staff
that were on shift you
either had a pleasant
experience or an
appalling one.”
• [made to wait for bedpan]
“Incontinent of urine for the
first time in my life. I’m 68
years old and a retired
teacher. This is not
supposed to be the way
someone in genuine need
is treated.”
Trust feedback event
• Dramatised: entrenched poor behaviour, stealth and
robotic care- based on observation data
i) Role-modelling and leadership
i) Support (from individual line manager,
senior management or the organisation)
i) Culture (locally and organisationally)
i) Education, training and development
i) Communication
Learning & Next Steps
• Monthly dignity survey & observation feedback
valuable but time consuming to sustain
– Potential for quarterly
• Wards had limited capacity to actively engage in
quality improvement interventions
– Specific project e.g. continence more traction
• Trust developed leadership programme for different
nursing bands
• Film illustrating impact poor quality interactions
(10mins)- reflection tool to aid the revalidation
process
Dignity in acute care
• Very difficult to implement interventions
• Feasible to influence by simple feedback?
• Students really enjoyed observations
• Simple scores (high) maybe hide actual
experiences?
• Dedicated strategies- MDT
– Training? Actors really engaged staff
• Time & staffing
• Talk & Listen –’whole team’
• Continence