improving chronic disease management - british … · improving chronic disease management: a...
TRANSCRIPT
Improving Chronic Mana
A Compelling Business Case for
Report from the Diabe
Email: Debora
Disease gement:
Diabetes
tes Working Group
Ph
hShera@Date: S
Prepared by: Sierra Systems Deborah Shera
one: 250.385.1535 Fax: 250.385.4761 SierraSystems.com eptember 23, 2002
Acknowledgements
The BC Diabetes Business Plan was funded by a public-private partnership of the BC Ministries of Health Planning and Health Services, and Novartis Pharmaceuticals Canada.
While this report was prepared by Sierra Systems, it is important to recognize all the partners who without their involvement, this document could not have been produced. We want to thank our partners, the members of the Diabetes Working Group, Novartis, and the BC Ministries of Health. Special acknowledgements to Howard Platt and the Utilization Management Branch, Valerie Tregillus, Director of Strategic Initiatives, Robert Fisk and the Population Health Surveillance and Epidemiology Branch, Paul Lam, Information Management Branch, and Angela Micco, Chronic Disease Management Project Officer, BC Ministries of Health.
Chronic Disease Management: Page i Improved Management of Diabetes Report from the Diabetes Working Group
TABLE OF CONTENTS
Executive Summary ............................................................................................................ 1
Background ................................................................................................................... 1 Scope of the Problem .................................................................................................... 2 Primary Prevention........................................................................................................ 4 Potential for the Management of Diabetes .................................................................... 4 What Is Being Proposed? .............................................................................................. 6 Business Case................................................................................................................ 7 The Diabetes Initiative .................................................................................................. 8 Next Steps ..................................................................................................................... 8
1. Introduction ................................................................................................................. 11
1.1. Background ........................................................................................................ 11 1.2. Getting Started.................................................................................................... 12 1.3. Next Steps .......................................................................................................... 12 1.4. Scope, Objectives and Approach ....................................................................... 13
2. Diabetes – The Challenge ........................................................................................... 15
2.1. Chronic Disease – The Issue .............................................................................. 15 2.2. Diabetes – What is it?......................................................................................... 15 2.3. The Burden of Diabetes in Canada .................................................................... 16
2.3.1. Population Profile .............................................................................................16 2.3.2. The Unequal Burden.........................................................................................16 2.3.3. The Potential Consequences .............................................................................17 2.3.4. Impact on Resources .........................................................................................19 2.3.5. Some Context....................................................................................................20 2.3.6. The Future.........................................................................................................20
2.4. Scope of the Problem for British Columbia ....................................................... 21 2.4.1. Diabetes in British Columbia............................................................................21 2.4.2. The Costs ..........................................................................................................23
2.5. Issues Specific to Diabetes in Children and Youth ............................................ 24 2.5.1. The Scope of the Problem in BC – Increasing Numbers of Children...............25
3. Primary Prevention...................................................................................................... 27
3.1. Type 2 Diabetes Can Be Prevented or Delayed – The Evidence Base .............. 27
Page ii
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
3.1.1. Reversing the Trend..........................................................................................28 3.2. Translating Evidence into Action....................................................................... 29
4. The Potential for Management of Diabetes................................................................. 31
4.1. The Need ............................................................................................................ 31 4.2. System Design.................................................................................................... 32 4.3. The Challenge .................................................................................................... 32 4.4. Key Features of Chronic Disease Management ................................................. 33
4.4.1. The Importance of Self-Management Techniques............................................34 4.5. Chronic Disease Management and Diabetes ...................................................... 35
4.5.1. Good Management Can Delay or Minimize Sequealae....................................36 4.5.2. Good Management Saves Resources ................................................................37
4.6. The Potential for Management of Children with Diabetes ................................ 41 4.7. The Current Management of Diabetes in BC..................................................... 42
4.7.1. A Benchmark for Comparison ..........................................................................43 4.7.2. Interdisciplinary Team-Based Care ..................................................................44 4.7.3. Initial and Ongoing Education and Support......................................................45 4.7.4. Clinical Care .....................................................................................................45 4.7.5. Depression Management...................................................................................48 4.7.6. Patient Self-Report from Limited Trial Survey ................................................48 4.7.7. What Can Be Concluded?.................................................................................48
5. The Proposed Diabetes Initiative ................................................................................ 51
5.1. An Evaluation of the Chronic Care Model......................................................... 51 5.1.1. Quality Improvement Process...........................................................................53
5.2. Core Features of the Initiative............................................................................ 53 5.2.1. Patient Components – Effective Self Management Supports and
Education ..........................................................................................................54 5.2.2. Physicians and Health Care Provider Components – Effective,
Prepared, Interdisciplinary Team......................................................................56 5.2.3. Effective Decision Support - Population Level Components ...........................57 5.2.4. Effective Decision Support – Provider and Patient Level ................................57 5.2.5. Clinical Information Supports...........................................................................58
5.3. Project Evaluation, Performance Measurement and Outcome Analyses ........... 59 5.4. Spread and Sustainability ................................................................................... 59
6. The Business Case....................................................................................................... 61
6.1. The Challenges of a Business Case in Health Care ........................................... 61
Chronic Disease Management: Page iii Improved Management of Diabetes Report from the Diabetes Working Group
6.1.1. Time Horizon and Complexity .........................................................................61 6.1.2. The Question of Audience ................................................................................62 6.1.3. Sustainability and Spread..................................................................................63 6.1.4. Extrapolation of Findings from Other Jurisdictions .........................................63
6.2. Outcome Objectives for Implementation of Optimal Diabetes Management in BC............................................................................................. 63
6.3. The Financial Analysis....................................................................................... 64 6.3.1. Assumptions......................................................................................................66
6.4. Risk Analysis...................................................................................................... 69 6.4.1. Scope Risk: High ..............................................................................................70 6.4.2. Service Delivery Model Risk: High..................................................................70 6.4.3. Benefits Risk: High...........................................................................................71 6.4.4. Implementation Model Risk: Medium..............................................................71 6.4.5. Cost Risk: Medium ...........................................................................................71 6.4.6. Other Risks: Low..............................................................................................72
6.5. Feasibility Analysis ............................................................................................ 72
7. The Diabetes Initiative ................................................................................................ 73
7.1. Chronic Care Model ........................................................................................... 73 7.2. The Provincial Collaborative ............................................................................. 73
7.2.1. Governance and Operations..............................................................................73 7.2.2. Marketing and Communication ........................................................................75
7.3. Local Implementation #1: VIHA, South Island ................................................. 75 7.4. Next Steps .......................................................................................................... 76 7.5. How Can You Become Involved?...................................................................... 77
Appendices APPENDIX A. DIABETES WORKING GROUP MEMBERS APPENDIX B. NHS DIABETES FRAMEWORK APPENDIX C. BC DIABETES CARE GUIDELINES APPENDIX D. BC DIABETES GUIDELINES’ PERFORMANCE OUTCOMES - LEVELS OF
CLINICAL TESTING BY BC HEALTH SERVICE DELIVERY AREA, 2000/01 APPENDIX E. REFERENCES

Chronic Disease Management: Page 1 Improved Management of Diabetes Report from the Diabetes Working Group
EEEXXXEEECCCUUUTTTIIIVVVEEE SSSUUUMMMMMMAAARRRYYY
“Today in the United States chronic disease is the major cause of disability, is the main reason why people seek health care, and consumes 70% of healthcare spending. With acute disease, the treatment aims at return to normal. With chronic disease, the patient’s life is irreversibly changed. Neither the disease nor its consequences are static. They interact to create illness patterns requiring continuous and complex management.” (Holman and Lorig, 2000)
Diabetes is diagnosed in approximately 19,000 British Columbians every year. In 2000/01, there were approximately 175,000 people in British Columbia diagnosed with diabetes and there were many more that were undiagnosed. Contrary to popular belief, diabetes is both progressive and life threatening with potentially devastating consequences for health. However there is a great deal that can be done to prevent the complications of diabetes and improve outcomes for people.
For the past several years, health professionals and managers within British Columbia have recognized a need for improved coordination in the management of chronic disease. Today, providers and decision-makers acknowledge multiple challenges to effective chronic disease management. Challenges include: the under-coordination of health services, limited incentives and training for health care professionals, poor diagnostic methods, limited disease management protocols, lack of patient involvement in managing disease, and stove-piped funding mechanisms. These realities underpin recent efforts to change existing structures and practices in order to advance professional practice in chronic disease management, and improve health outcomes for people living with chronic illness. Most recently, the focus in British Columbia has been on the management of diabetes.
The document provides the evidence that the BC health system, in its current design, is challenged to effectively manage chronic disease both now and in the future. Economic and quality of care arguments are presented to support the proposition that this situation cannot be ignored. There is a need to move to redesign key aspects of the primary health care delivery system now, to find new ways of working together in partnership with key stakeholders, and to utilize process cycles that are evaluated and build upon each other. A system of care must be developed that assists patients and practitioners in achieving the goals of chronic disease management.
Background
In the spring of 2002, the Diabetes Working Group was established comprising of representatives of the BC Ministry of Health Services, Vancouver Coastal Health Authority, Canadian Diabetes Association, Vancouver Island Health Authority, Provincial Health Services Authority, British Columbia Medical Association and Novartis. The Group was formed to develop a business case in support of a provincial diabetes initiative in British Columbia. This Diabetes Initiative fits within a broader provincial context of the four provincial health strategies: Provincial Prevention

Page 2
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
and Wellness Strategy; Primary Health Care Renewal Strategy; Chronic Disease Management Strategy; and Diabetes Prevention and Management: A BC Framework for Action.
The Diabetes Working Group determined that the Chronic Care Model (CCM), developed by the Group Health Cooperative in Puget Sound (Seattle, Washington), and the Institute for Health Improvement, would form the conceptual basis for the business plan. As well, the plan would incorporate key elements of the Expert Patient Model currently being implemented within the National Health Service in the United Kingdom. This business plan builds upon the diabetes business case developed for the previous Vancouver/Richmond Health Board, 2002 as well as the BC Business Case for Congestive Heart Failure, 2002.
The scope of the Diabetes Business Plan is to describe the business case for implementing a provincial Diabetes Initiative for all individuals with diabetes; i.e. children and adults with Type One or Type Two diabetes, as well as a plan for a staged implementation in British Columbia. It is important to note that although all elements of a complete framework of prevention, promotion and management of chronic disease and diabetes are important, the Diabetes Working Group has chosen in this proposal to focus on the elements of disease management and amelioration of avoidable complications and consequences.
Using the Diabetes Working Group to direct the project, provide input and access to Ministry data, as well as obtain input and feedback from key experts, Sierra Systems has been able to draft a business plan for wider review and feedback.
Scope of the Problem
Diabetes mellitus is a group of metabolic diseases characterized by hyperglycemia, resulting from defects in insulin secretion and/or insulin action. Without insulin, glucose cannot be sufficiently absorbed from the bloodstream into the cells of the body. There are two distinct forms of diabetes: Type 1, or insulin dependent diabetes, which is an auto-immune disease; and Type 2, or non-insulin dependent diabetes, which is associated with insulin resistance. Diabetes is a chronic and progressive disease that impacts upon almost every aspect of life. It can result in premature death, ill health and disability, yet these consequences can often be prevented, or delayed, by high-quality care.
In Canada, the number of people, (aged 12 years and over) with both diagnosed and undiagnosed diabetes, was estimated by Health Canada to be 1.2 million to 1.4 million or 4.9 % to 5.8% of the population. (Diabetes in Canada, 1999) Nine out of 10 people with diabetes have Type 2 diabetes, traditionally a condition affecting mainly older people. However, burgeoning obesity is associated with an alarming increase in the incidence in the younger population.
Diabetes does not affect everyone in Canadian society equally. Significant inequalities exist in the risk of developing diabetes particularly for First Nations people as well as in access to health services and the quality of those services, and in health outcomes, particularly with regard to Type 2 diabetes. Diabetes is now being called the disease of the elderly and the poor.

Chronic Disease Management: Page 3 Improved Management of Diabetes Report from the Diabetes Working Group
Health Canada projections into the year 2016 show an exponential increase in the number of deaths due to diabetes of 12,000 annually. Ten years ago, using projections from US figures, the economic burden of diabetes to Canada was estimated by Health Canada to be as high as $9 US billion annually. (Diabetes in Canada, 1999)
In British Columbia, diabetes is diagnosed in approximately 19,000 British Columbians every year. The incidence of diabetes in British Columbia continued to increase over the past decade, due to the increase in obesity and inactivity as well as the aging population. Diabetes was diagnosed in 175,000 British Columbians in 2000/01. (MOH, 2002) By 2010, the prevalence is expected to grow to 325,000 (7.1%) an increase of 90%. (Diabetes in British Columbia Systhesis Report, 2000) It is estimated that the prevalence today is closer to 4.9% of the BC population. This estimate of people with diabetes in BC represents only those on the diabetes registry who are residents of BC with MSP coverage. It does not include those who are undiagnosed, without medical coverage, in the armed forces or on reserve First Nations people. The number would be much higher if it could be ascertained how large this undiagnosed and non MSP group was.
Diabetes is a disease that causes additional health complications and conditions. The table below shows the comparison that people with diabetes have a greater risk for other diseases and their complications than the total population in BC for 2000/01.
Table 1
Care Provided in 2000/01 People with Diabetes Entire Province
Number of People 175,000 4,055,000 Surgery for disorders of the retina 3,907 6,516 Toes, feet or lower limbs amputated 390 703 Surgery for cataracts 5,311 27,358 Coronary artery bypass surgery 775 2,390 Coronary angioplasties 1,122 4,370 Dialysis for any reason 1,075 2,727
The cost of diabetes care in BC is staggering. For 2000/01, an estimated $761,400,000 was expended on hospital, physician, renal and pharmaceutical care and services. This is 16.6% of the overall health budget for only 4.9% of the population. (MOH, 2002)
If the health care system does not manage the disease of diabetes appropriately and does not address their issues, then the frightening potential is for these figures, with their associated costs, to at least double by the year 2010.
While this business case focuses on improved management strategies for diabetes in adults, this does not reduce the importance and need for improved prevention and management strategies for children and youth in BC. As with adults, the number of children with both Type 1 and Type 2 diabetes is growing at a rapid rate world-wide. Type 1 usually diagnosed in children is increasing at 3% per year. For Type 2 diabetes with the escalating increase in obesity, a known risk factor for Type 2 diabetes, there has been an alarming increase in the incidence in the younger
Page 4
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
population. Type 2 affects special groups of children – 1-2% of children of First Nations, Hispanic or black origin, and up to 4% of adolescent girls – and has devastating consequences of early-onset complications, such as heart-attacks, strokes, blindness and amputations in 30-year-olds. (American Diabetes Association, 1999)
Primary Prevention
The business case and financial analysis focus on the prevention and management of diabetes complications and disabilities. The limited scope of the analysis does not in any way minimize either the importance, or the need for, an investment in primary prevention.
The findings of recent clinical trials have concluded that the risk of developing Type 2 diabetes among people with impaired glucose tolerance or impaired fasting glucose can be reduced dramatically simply through diet and exercise. It should be noted that while targeting at-risk individuals is important in reversing the trend towards increased incidence of diabetes, projections indicate that individuals at medium or low risk for diabetes will actually comprise the greatest number of new cases of Type 2 diabetes over the next few years.
Ultimately, a population-based approach aimed at changing the social, policy, and environmental norms that create conditions of risk for the entire population, in combination with the high-risk approach, is considered the best avenue for achieving the greatest impact. This population-based approach is being used in the Ministry of Health Planning’s Prevention and Wellness Strategy focusing on chronic disease primary prevention including diabetes. (MOHP Service Plan, 2002)
Potential for the Management of Diabetes
As is the case with chronic disease generally, diabetes can be managed with most of its complications avoided or minimized. Although there is no cure for diabetes, close monitoring of blood sugar levels, blood pressure, and ongoing interaction with a health care professional can help individuals stave off the insidious effects of the disease, improve quality of life and, as a result, reduce associated healthcare costs.
Two of the most comprehensive studies in this field are:
• A ten-year longitudinal study by the US National Institute of Diabetes and Digestive and Kidney Diseases which found that patients who were able to monitor and control blood sugar levels were also able to slow the onset of eye, kidney and nerve diseases resulting from diabetes. The Diabetes Control and Complications Trial (DCCT, 1993), and
• United Kingdom Prospective Diabetes Study (UKPDS) which established that the appropriate care and management of diabetes can reduce or delay complications and control associated health care costs while improving the quality of life for those individuals living with diabetes (UKPDS, 1998).
Chronic Disease Management: Page 5 Improved Management of Diabetes Report from the Diabetes Working Group
Both the DCCT and the UKPDS highlight the fact that intensive control and management in diabetes must not be limited to glycemic control. The prevention of the complications of diabetes is also strongly associated with the management of hypertension and hyperlipidemia. Their results conclusively demonstrate the benefit of intensive management strategies in both types of diabetes. While these findings are replicated in many other smaller studies, these two represent the most comprehensive studies of their nature.
A number of studies are also presented which demonstrate significant cost and resource savings to the health care system through effective management. The results of the cost savings in studies of Wagner (2001) and Rubin (1998) form the basis of the business case.
National and international studies have demonstrated that most diabetes patients receive insufficient education on how to manage their disease and up to 70% have questions that remain unanswered. This translates into a patient profile where most patients must be self monitoring, left primarily to take their own medications, measure blood sugar levels, make major lifestyle changes, and alert the physician to changes in their health if they are to avoid the debilitating effects of this disease. (Wagner, 2001)
Comparing current practices within BC with best practices as defined by the approved BC Guidelines suggest that current management of diabetes is less than optimal. People with diabetes, are not receiving the levels of clinical testing indicated in these evidence-based guidelines. The data shows some BC physicians are following the testing guideline, so clearly these are achievable. It is reasonable to conclude that if the signs of complications are not being identified through screening/monitoring then they cannot, in the main, be appropriately managed.
Studies from other jurisdictions suggest that in reality approximately 50% of people with diabetes are likely not even diagnosed. The consequences of failing to effectively manage diabetes will be significant. There must inevitably be many more cases of hypertension, stroke, heart disease, blindness, end stage renal failure, peripheral neuropathy and lower limb amputations, and premature death as the incidence and prevalence of diabetes increase. Many of these complications and premature deaths would be prevented by well-organized care. The economic impact on the health care system will be compounded by the cost to society of the increased disability consequent upon this failure to manage a common, well understood problem.
In addition to the economic burden of not acting, there is an ethical issue raised by ignoring the human suffering generated by diabetes, its complications, and premature deaths. The ethical issue is particularly powerful in the current situation where the technology and knowledge is relatively inexpensive and easily available to solve a huge, and increasing, health care problem.
In summary:
• Diabetes is rapidly becoming an epidemic and in fact already is amongst many population groups
• There are inadequate data to identify the population
• There are significant concerns that care is variable
Page 6
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
• There is poor coordination between providers and services across the region
• There are an absence of systems to evaluate outcomes for individual clients/patients and the total population
• Diabetes is not optimally managed in BC
• Evidence from other jurisdictions clearly demonstrates improvements can be made to the system of care
• The economic consequences of doing nothing are staggering
To do nothing is highly questionable from a social, population health and ethical perspective.
What Is Being Proposed?
The lack of a common performance improvement framework is not unique to diabetes and has been a barrier to quality improvement efforts in chronic disease generally. Poor performance and failure to adhere to evidence-based guidelines are the inevitable result of the current BC health system design. The challenge of diabetes must be met through identifying and addressing the underlying systemic issues in a multifaceted and coordinated manner.
The BC Diabetes Initiative proposes to evaluate the usefulness of one model, the Institute for Health Care Innovation (IHI), Chronic Care Model (CCM), to effecting appropriate system redesign in BC. A framework, as opposed to detailed implementation plan, is presented and key principles and core attributes are described for the provincial diabetes initiative. It is recognized that local needs and capacity will shape individual project details however, share a common set of principles and core attributes. A global program budget is developed based upon these core attributes.
The cost side of the business case equation was developed using the CCM as a framework. The budget serves as a financial template and it is not intended that individual line items be prescriptive for community based projects. Provincial level budget items will remain constant but local costs may vary depending upon requirements and existing capacity.
The following characteristics have been found to be effective in optimal management of chronic disease and will be incorporated in the project:
• Proactive rather than reactive approaches to care plan for care rather than provide services on demand
• Support to clients for self-management and better outcomes with informed, activated client; includes coordinating such support with the community at large.
• Delivery system redesign to meet the needs of clients who require more time, a broader array of resources and closer follow-up: includes the necessary services and supplies for chronic disease management.
Chronic Disease Management: Page 7 Improved Management of Diabetes Report from the Diabetes Working Group
• Decision-support for a prepared, proactive team including provider training and decision support through guidelines and other tools: includes access to specialist consultation.
• Recognition and rewards for the behavioural change that is required of both clients and health care providers.
• Information systems that support population-based care for outcome determination and provider reminders and feedback for proactive rather than reactive care.
• High-level support by senior MOH and health authority executives.
This project represents only the first phase of a broad initiative to improve the management of chronic disease across the province. The evaluation will inform the development of public policy and ongoing quality improvement processes. The objective is for effective chronic disease management to ‘spread’.
Business Case
This plan begins the process of developing a valid business case for system change designed to improve the management of chronic disease generally, and diabetes specifically, within BC. It is timely and appropriate that this form of cost justification become a normal course of practice within the Canadian health care industry.
The complexity of healthcare makes the development of valid cost/benefit analyses at best, challenging. Prior to developing the economic rationale it is important to note some of these challenges and caveats, and to be clear on the assumptions upon which many of the estimates and projections are made.
The financial review includes a detailed quantitative analysis of the costs and benefits over a 4year period, including a Net Present Value analysis to determine the financial feasibility of the BC Diabetes Initiative, including all assumptions made. It must be stressed that the financial analysis is provided for PLANNING PURPOSES ONLY and should not be construed to constitute the actual costs and benefits that will be incurred. Two important benefits – reduction in incidence resulting from primary prevention and improvements in quality of life resulting from improved care – are not considered for the purposes of this financial analysis.
The nature of the high and medium risks support the conclusion that a lot more study and refinement is required before a provincial implementation of the Diabetes Initiative can be considered. The scope of the service, the service delivery and implementation models for the initiative, as well as and the associated costs and benefits need to be more clearly understood.
Conclusion: based on the findings of the financial analysis of a diabetes initiative with a pay back of 33 months and the risk analysis to move the BC Diabetes Initiative from theory to reality at this time requires a staged implementation approach, starting with a local implementation.

Page 8
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
The Diabetes Initiative
The underpinning of the Diabetes Initiative will be the “Chronic Care Model”. The model is population-based, data driven and creates practical, supportive, evidence-based interactions between an informed activated client and a prepared proactive practice team
The Diabetes Initiative will evaluate the Expanded Chronic Care Model as an organizational approach to caring for people with diabetes in a BC primary health care setting. The Diabetes Working Group concluded from the risk analysis that it would be prudent to implement this initiative in a staged manner. Phase One will be undertaken in partnership with the Vancouver Island Health Authority. While the first stage of this broad initiative will be within VIHA, this does not limit other health authorities from becoming involved. Findings from this phase will inform and shape further phases to include the rest of VIHA and other health authorities. VIHA is committed to sharing the learning from their implementation.
The details of Phase One have yet to be determined but include the participants, timing, budget, partners, governance and operations, marketing and communications.
Next Steps
This document has summarized the issue and management of chronic disease and diabetes in BC, Canada and elsewhere in the world. The literature reveals that the numbers of people with chronic diseases are rapidly increasing and diabetes is becoming an epidemic. While many of the consequences of diabetes can be avoided the current BC primary care system does not support optimal management. At the same time the current costs of managing the health care for diabetes in BC are staggering. There are demonstrated successes in better management of chronic diseases including diabetes, both in health outcomes for individuals with diabetes and cost savings for the health care system.
It is clear that there is an economic case to proceed with a diabetes initiative with a pay back of 33 months. The economic and care consequences of failing not to manage diabetes are overwhelming and will quickly exceed the capacity of the BC health care system to sustain. Failure to utilize the current concepts of evidence-based management of diabetes would be morally and ethically irresponsible.
The Diabetes Working Group is recommending the initiation of the BC Diabetes Initiative. This project provides an opportunity for a first step in the required health care system redesign. The most feasible option for this first step that will mitigate the risks is a local implementation, in the Greater Victoria area, southern part of the Vancouver Island Health Authority. This local implementation will refine the delivery model for the chronic disease management and in particular diabetes for a Canadian setting, as well as reconfirm the costs and benefits associated with the business case.
Chronic Disease Management: Page 9 Improved Management of Diabetes Report from the Diabetes Working Group
While VIHA is one of the early implementers of Phase One of the Diabetes Initiative, this does not limit other health authorities from becoming involved. The recent direction on primary health care from the Federal and Provincial governments and the infusion of the Primary Health Care Transition fund, may provide opportunities for Health Authorities to implement a Diabetes Initiative utilizing the Chronic Care Model and linking with their other primary health care strategies. The table at the end of Section 7 has been developed to help generate ideas from other groups who would like to participate in this broad-based collaborative. The collaborative is eager to work with health authorities and providers in improving diabetes care in this province.
The advancement of this project rests on a series of next steps that include the following:
• Approval of the Diabetes Business Plan and announcement to implement the BC Diabetes Initiative
• Formalization of partnerships and funding
• Establishment of a governance structure
• Development and implementation of a detailed work plan
• Start of Initiative
Chronic Disease Management: Page 11 Improved Management of Diabetes Report from the Diabetes Working Group
111... IIINNNTTTRRROOODDDUUUCCCTTTIIIOOONNN
1.1. Background
For the past several years, health professionals and managers within British Columbia have recognized a need for improved coordination in the management of chronic disease. Today, providers and decision-makers acknowledge multiple challenges to effective chronic disease management. Challenges include: the under-coordination of health services, limited incentives and training for health care professionals, poor diagnostic methods, limited disease management protocols, lack of patient involvement in managing disease, and stove-piped funding mechanisms. These realities underpin recent efforts to change existing structures and practices in order to advance professional practice in chronic disease management, and improve health outcomes for people living with chronic illness. Most recently, the focus in British Columbia has been on the management of diabetes.
In the spring of 2002, the Diabetes Working Group was established to develop a business case in support of a provincial diabetes initiative in British Columbia (see Appendix A for Working Group members). The Diabetes Initiative fits within a broader provincial context as illustrated by the following four provincial health strategies:
• Provincial Prevention and Wellness Strategy led by Population Health and Wellness, Ministry of Health Planning focuses on five priorities for the primary prevention of chronic diseases such as Type 2 diabetes. These priorities are increasing physical activity and healthy eating and decreasing tobacco use and alcohol and substance misuse. (MOHP Service Plan, 2002)
• Primary Care Renewal Strategy focuses on new ways to deliver primary health care to British Columbians to increase access; place emphasis on health promotion, disease and injury prevention, and management of chronic diseases including diabetes; establish interdisciplinary teams; and facilitate coordination and integration of all health services. Supported in part by the Primary Health Care Transition Fund.
• Chronic Disease Management Strategy focuses on three key ways to improve chronic diseases in BC: initiate a staged implementation of Chronic Disease Management (CDM); develop products and initiatives to support and measure improvements in CDM care; and pursue technological innovations for increased access to health information and services.
• Diabetes Prevention and Management: A BC Framework for Action – this plan represents the culmination of a provincial planning process that was initiated in 1999/2000, involving substantial research and consultation. This strategy was informed by previous work undertaken by the BC Diabetes Reference group as well as the Canadian Diabetes Strategy.
Page 12
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
1.2. Getting Started
On March 27, 2002, a Strategic Workshop on Chronic Disease Management (CDM) was hosted by the Health Association of BC, with the support of the Ministry of Health Services, and in partnership with the BC Medical Association and Registered Nurses Association of BC. Participants identified the need for a planned, supported and funded CDM approach for BC. Additionally, in 2001, a BC based physician survey identified diabetes as the priority candidate for a CDM initiative.
As a result of these two key stakeholder consultations, the Ministries of Health, as one part of their Chronic Disease Management Strategy, determined the need for a business plan for diabetes management. The Diabetes Working Group was formed comprising representatives of the BC Ministry of Health Services, Vancouver Coastal Health Authority, Vancouver Island Health Authority, Provincial Health Services Authority, British Columbia Medical Association, Canadian Diabetes Association, and Novartis. The first meeting of this group was in April, 2002.
The Diabetes Working Group determined that the Chronic Care Model (CCM), developed by the Group Health Cooperative in Puget Sound and the Institute for Health Improvement, would form the conceptual basis for the business plan. As well, the plan would incorporate key elements of the Expert Patient Model currently being implemented within the National Health Service in the United Kingdom. These models are discussed in greater detail in later sections of the paper.
This plan builds upon two business cases, the Integrated Diabetes Care: An Application of the Chronic Care Model, February 2002 developed for the previous Vancouver/Richmond Health Board and the BC Congestive Heart Failure Collaborative Report, Business Plan for Congestive Heart Failure Initiative, April, 2002 developed by the BC Ministries of Health.
Subsequent to the first meeting of the Diabetes Working Group there was a round of data collection which consisted of (a) interviews with members of the collaborative, (b) a review of the published, peer-review literature to update what existed in the VRHB document, as well as inclusion of information on diabetes in children and health promotion and prevention.
1.3. Next Steps
Much of the developmental work of the Diabetes Working Group is now complete, and the members of the working group are ready to move forward. Advancement of the Diabetes Initiative for British Columbia rests on a series of next steps that include the following:
• Approval of the Diabetes Business Plan with announcement of the implementation of Phase One of the Initiative
• Formalization of partnerships and funding
• Establishment of a governance structure
• Development and implementation of a detailed work plan
Chronic Disease Management: Page 13 Improved Management of Diabetes Report from the Diabetes Working Group
1.4. Scope, Objectives and Approach
The scope of the Diabetes business plan is:
• Diabetes – Diabetes mellitus is a group of metabolic diseases characterized by hyperglycemia, resulting from defects in insulin secretion and/or insulin action.
• Business Plan – describe the business case for implementing a provincial Diabetes Initiative for all individuals with diabetes; i.e. children and adults with Type One or Type Two diabetes, as well as a plan for a staged implementation in British Columbia.
• British Columbia – the province of British Columbia in Canada
The primary objective of the business plan is to determine if a business case exists for a Diabetes Initiative in British Columbia – in other words is this initiative worthy of investment.
Using the Diabetes Working Group to direct the project, provide input and access to Ministry data, as well as obtain input and feedback from key experts, Sierra Systems has been able to draft a business plan for wider review and feedback.
In support of the primary objective this business plan will:
• Describe how the Diabetes Initiative fits with, and supports progress towards, the broader priorities and strategic framework of the Ministries of Health;
• Describe the significant impact the rapid increase in prevalence of diabetes will have on the provincial health system;
• Present evidence that proven clinical and management techniques currently exist which can assist in meeting these challenges and indeed avert what many describe as a potential epidemic;
• Evaluate the current capacity of the system to manage these present and future challenges;
• Describe the current status of evidence-based management of chronic disease and diabetes within BC;
• Define the social, health and economic consequences of failure to effectively manage diabetes; and finally
• Present the outline, resource requirements, and business rationale for the Diabetes Initiative to redesign the BC system in support of effective management of diabetes within a primary health care system that provides excellent, comprehensive and integrated care
It is important to note that although all elements of a complete framework of prevention and management of chronic disease and diabetes are important, the Diabetes Initiative has chosen in this business plan to primarily focus on the elements of disease management and amelioration of avoidable complications and consequences.
Page 14
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
The Diabetes Initiative will only be successful if it can create strong partnerships and find new ways of working together. A broad based partnership involving all key stakeholders will be required to support this initiative.
Chronic Disease Management: Page 15 Improved Management of Diabetes Report from the Diabetes Working Group
222... DDDIIIAAABBBEEETTTEEESSS ––– TTTHHHEEE CCCHHHAAALLLLLLEEENNNGGGEEE
To set the context for the business plan, an overview of diabetes, the projected increase and the potential consequences both to patients and the health care system within our province are provided.
2.1. Chronic Disease – The Issue
“Today in the United States chronic disease is the major cause of disability, is the main reason why people seek health care, and consumes 70% of healthcare spending. With acute disease, the treatment aims at return to normal. With chronic disease, the patient’s life is irreversibly changed. Neither the disease nor its consequences are static. They interact to create illness patterns requiring continuous and complex management.” (Holman and Lorig, 2000)
The number of persons with chronic illness is growing at an astonishing prevalence rate due in part, to the aging of the population, lifestyle habits, such as increased incidence of inactivity and obesity, and the greater longevity of persons with many chronic conditions. As one example, the rate of diabetes in the UK is predicted to double by 2010. (UKPDS, 1998)
The proportion of people with long-term medical conditions is rising in BC as in the UK and US, with as many as 800,000 people living with either diabetes or some form of cardiovascular disease, about one in five. (MOH, 2000/01)
The challenges presented by this growth rate are compounded by the reality and complexities of frequent co-morbidity. One nationally representative study in the US identified that 25% of the population had one or more of 5 chronic conditions. The existence of co-morbidity was the most frequent in those patients with diabetes and ischemic heart disease - 55.5 % and 60.8 % respectively. (Druss, 2001)
2.2. Diabetes – What is it?
Diabetes mellitus is a group of metabolic diseases characterized by hyperglycemia, resulting from defects in insulin secretion and/or insulin action. Insulin, a hormone secreted from beta cells in the pancreas, assists with the conversion of glucose into energy. Without insulin, glucose cannot be sufficiently absorbed from the bloodstream into the cells of the body. There are two distinct forms of diabetes: Type 1, or insulin dependent diabetes, which is an auto-immune disease; and Type 2, or non-insulin dependent diabetes, which is associated with insulin resistance. Diabetes is a chronic and progressive disease that impacts upon almost every aspect of life. It can result in premature death, ill health and disability, yet these consequences can often be prevented, or delayed, by high-quality care.
Page 16
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
Nine out of ten people with diabetes have Type 2, traditionally a condition affecting mainly older people. However, burgeoning obesity is associated with an alarming increase in the incidence in the younger population. The high price of diabetes, both in terms of morbidity and financial burden upon society, make a preventative and management strategy highly desirable. (Scottish Diabetes Framework, 2001)
As is the case with chronic disease generally, diabetes can be managed and most of its complications avoided or minimized. Although there is no cure for diabetes, close monitoring of blood sugar levels, blood pressure, and ongoing interaction with a health care professional can help individuals stave off the insidious effects of the disease, improve quality of life and, as a result, reduce associated healthcare costs. (Diabetes in Canada, 1999)
2.3. The Burden of Diabetes in Canada
2.3.1. Population Profile
The number of Canadian residents, (aged 12 years and over) with both diagnosed and undiagnosed diabetes, was estimated by Health Canada to be 1.2 million to 1.4 million in 1996/97 or 4.9% to 5.8% of the population. (Diabetes in Canada, 1999)
• There are an estimated 60,000 new cases of diabetes diagnosed annually.
• Among Aboriginal peoples, age-standardized diabetes prevalence rates are reported to be triple those found in the general population. Furthermore, for every case diagnosed, one remains undiagnosed. In this population diabetes is becoming an epidemic. Of concern is the projected 20% increase over the next 25 years. (BC Strategy for Diabetes Prevention and Management, 2000)
• Diabetes is ranked as the seventh leading cause of death in Canada, with 5,447 deaths reported in 1996, while it is estimated that deaths attributable to diabetes are under reported by a factor of five. (Diabetes in Canada, 1999)
2.3.2. The Unequal Burden
Diabetes does not affect everyone in society equally. Significant inequalities exist in the risk of developing diabetes, in access to health services and the quality of those services, and in health outcomes, particularly with regard to Type 2 diabetes. Diabetes is now being called the disease of the elderly and the poor.
• People of South Asian, African, African-Caribbean, Hispanic and Middle Eastern descent have a higher than average risk of Type 2 diabetes, as do less affluent people. Socially excluded communities, including prisoners, refugees and asylum seekers, and people with learning disabilities or mental health problems, may receive poorer quality care. Risk may accumulate if an individual belongs to more than one of these groups. (NHS, 2001)
Chronic Disease Management: Page 17 Improved Management of Diabetes Report from the Diabetes Working Group
• The age-standardized prevalence of diabetes among aboriginal people in Canada, with the exception of Inuit people, is at least three times that of the general population. Recent population-based epidemiological surveys in Canada have revealed age-adjusted prevalence rates of 19% to 26%, which are among the highest reported rates in the world. (Meltzer et al, 1998)
• The prevalence of diabetes rises steeply with age: one in 20 people over the age of 65 in the UK has diabetes and in people over the age of 85 years this rises to one in five. The diagnosis of diabetes may be delayed in older people, with symptoms being wrongly attributed to aging. (Department of Health, UK, 2001)
• The frequency of diabetes in England is higher in men than women. However, women with diabetes are at relatively greater risk of dying than men. This may be because gender compounds other aspects of inequality. (Department of Health, UK, 2001)
• Among primary care patients with type 2 diabetes, inadequate health literacy is independently associated with worse glycemic control and higher rates of retinopathy. Inadequate health literacy may contribute to the disproportionate burden of diabetes-related problems among disadvantaged populations. (Schillinger, 2002)
2.3.3. The Potential Consequences
Prolonged exposure to raised blood glucose levels damages tissues throughout the body by damaging the small blood vessels. While initial changes are reversible, over time, prolonged raised blood glucose levels can lead to irreversible damage including:
• Cardiovascular disease
− Approximately 21% of people with diabetes have heart disease or are suffering the effects of stroke. This compares with 4% of the population without diabetes.
− In the 35-64 age group people with diabetes are six times more likely to have heart disease or stroke than are people without diabetes. (Diabetes in Canada, 1999)
• Damage to the eyes, which can lead to visual impairment and blindness
− Cataracts are twice as common in people with diabetes and occur 10 years earlier than in people who do not have diabetes. (NHS, 2001)
− Diabetes is the sole or contributing cause of blindness in about 86% of the eyes of people with Type 1 diabetes, and in 33% of people with Type 2 diabetes.
− Proliferative retinopathy occurs in 23% of patients with Type 1 diabetes, 14% of people with Type 2 diabetes on insulin and 3% of people with Type 2 diabetes not taking insulin. (Diabetes in Canada, 1999).
• Damage to the kidney, which can lead to progressive renal failure
− The proportion of people with newly diagnosed kidney failure that also have diabetes increased from 16% in 1981 to 28% in 1996. As of December 1996, there were 3,340 people with diabetes who were receiving treatment for end stage renal disease, or kidney failure. (Canadian Organ Replacement Register, Annual Report, 1998)
Page 18
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
− There is a growth of 10% -15% in Canada per year of chronic kidney disease and the major causal factor is attributed to diabetes.(Chronic Kidney Disease, BC Strategy, 2002)
• Damage to the nerves which can lead to loss of sensation in the feet
− Diabetes is the leading cause of non-traumatic limb amputation. In 2001/02 there were 390 people with diabetes who had lower limb amputations. (MOH 2001/02)
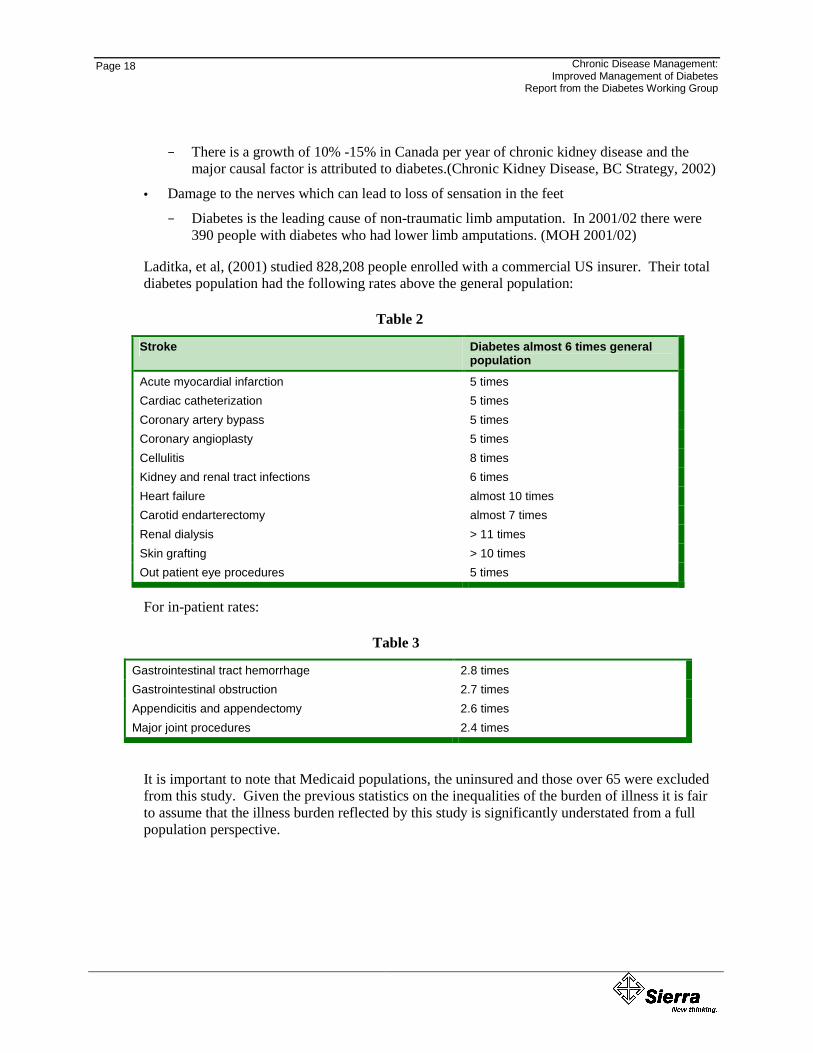
Laditka, et al, (2001) studied 828,208 people enrolled with a commercial US insurer. Their total diabetes population had the following rates above the general population:
Table 2
Stroke Diabetes almost 6 times general population
Acute myocardial infarction 5 times Cardiac catheterization 5 times Coronary artery bypass 5 times Coronary angioplasty 5 times Cellulitis 8 times Kidney and renal tract infections 6 times Heart failure almost 10 times Carotid endarterectomy almost 7 times Renal dialysis > 11 times Skin grafting > 10 times Out patient eye procedures 5 times
For in-patient rates:
Table 3
Gastrointestinal tract hemorrhage 2.8 times Gastrointestinal obstruction 2.7 times Appendicitis and appendectomy 2.6 times Major joint procedures 2.4 times
It is important to note that Medicaid populations, the uninsured and those over 65 were excluded from this study. Given the previous statistics on the inequalities of the burden of illness it is fair to assume that the illness burden reflected by this study is significantly understated from a full population perspective.
Chronic Disease Management: Page 19 Improved Management of Diabetes Report from the Diabetes Working Group
2.3.4. Impact on Resources
A review of studies across several jurisdictions demonstrates that health care for people with diabetes costs in the range of 2-3 times more than that for the non-diabetes population of the same age.
A British study found that Type 2 diabetes alone is a major drain on resources, as people with Type 2 diabetes are 2 to 3 times more likely to be admitted to hospital than their demographic peers, and they stay in hospital on average, four times as long. (UK Department of Health, 2002)
US studies indicate that people with diabetes are hospitalized more frequently than those without the disease, and use physician services at a higher rate than non-diabetes individuals. (Laditka et al, 2001)
Table 4
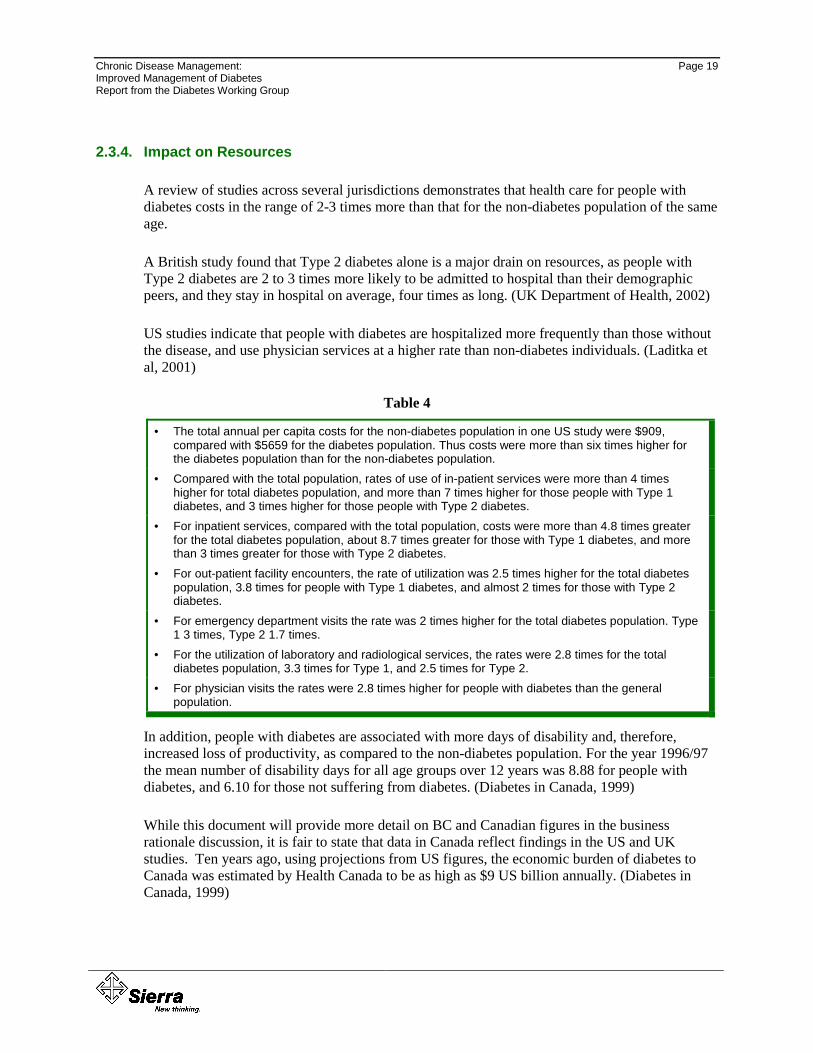
• The total annual per capita costs for the non-diabetes population in one US study were $909, compared with $5659 for the diabetes population. Thus costs were more than six times higher for the diabetes population than for the non-diabetes population.
• Compared with the total population, rates of use of in-patient services were more than 4 times higher for total diabetes population, and more than 7 times higher for those people with Type 1 diabetes, and 3 times higher for those people with Type 2 diabetes.
• For inpatient services, compared with the total population, costs were more than 4.8 times greater for the total diabetes population, about 8.7 times greater for those with Type 1 diabetes, and more than 3 times greater for those with Type 2 diabetes.
• For out-patient facility encounters, the rate of utilization was 2.5 times higher for the total diabetes population, 3.8 times for people with Type 1 diabetes, and almost 2 times for those with Type 2 diabetes.
• For emergency department visits the rate was 2 times higher for the total diabetes population. Type 1 3 times, Type 2 1.7 times.
• For the utilization of laboratory and radiological services, the rates were 2.8 times for the total diabetes population, 3.3 times for Type 1, and 2.5 times for Type 2.
• For physician visits the rates were 2.8 times higher for people with diabetes than the general population.
In addition, people with diabetes are associated with more days of disability and, therefore, increased loss of productivity, as compared to the non-diabetes population. For the year 1996/97 the mean number of disability days for all age groups over 12 years was 8.88 for people with diabetes, and 6.10 for those not suffering from diabetes. (Diabetes in Canada, 1999)
While this document will provide more detail on BC and Canadian figures in the business rationale discussion, it is fair to state that data in Canada reflect findings in the US and UK studies. Ten years ago, using projections from US figures, the economic burden of diabetes to Canada was estimated by Health Canada to be as high as $9 US billion annually. (Diabetes in Canada, 1999)
Page 20
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
2.3.5. Some Context
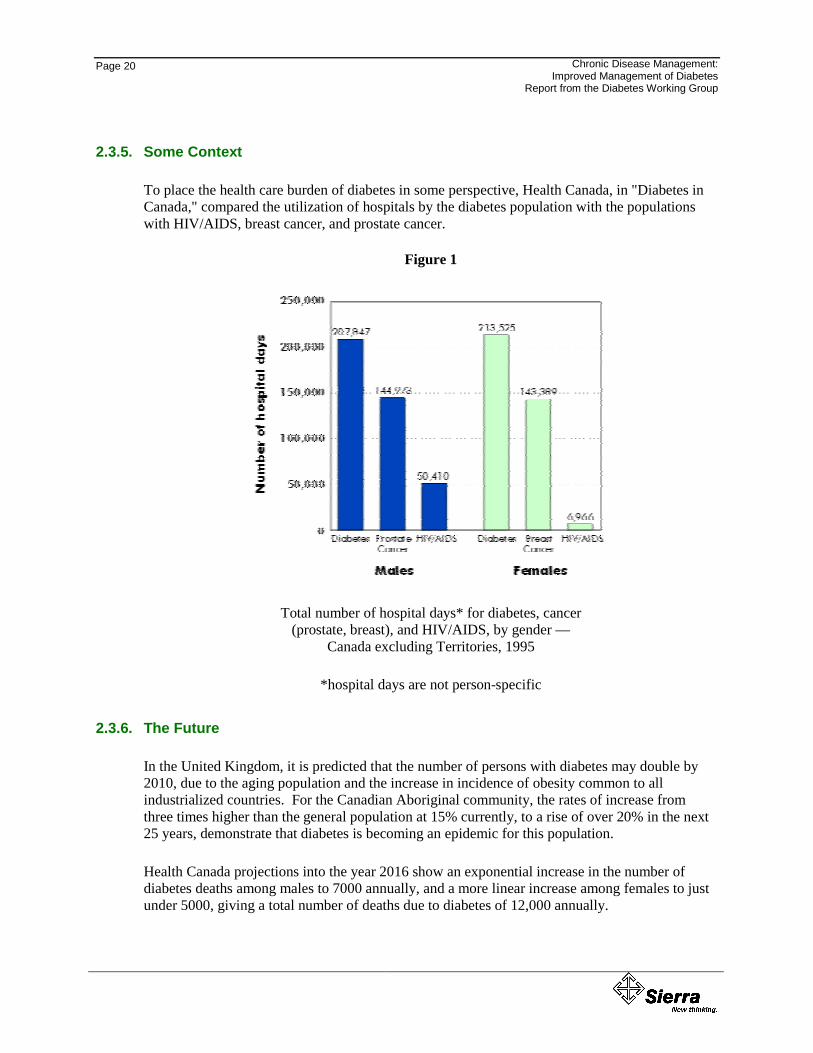
To place the health care burden of diabetes in some perspective, Health Canada, in "Diabetes in Canada," compared the utilization of hospitals by the diabetes population with the populations with HIV/AIDS, breast cancer, and prostate cancer.
Figure 1
Total number of hospital days* for diabetes, cancer (prostate, breast), and HIV/AIDS, by gender —
Canada excluding Territories, 1995
*hospital days are not person-specific
2.3.6. The Future
In the United Kingdom, it is predicted that the number of persons with diabetes may double by 2010, due to the aging population and the increase in incidence of obesity common to all industrialized countries. For the Canadian Aboriginal community, the rates of increase from three times higher than the general population at 15% currently, to a rise of over 20% in the next 25 years, demonstrate that diabetes is becoming an epidemic for this population.
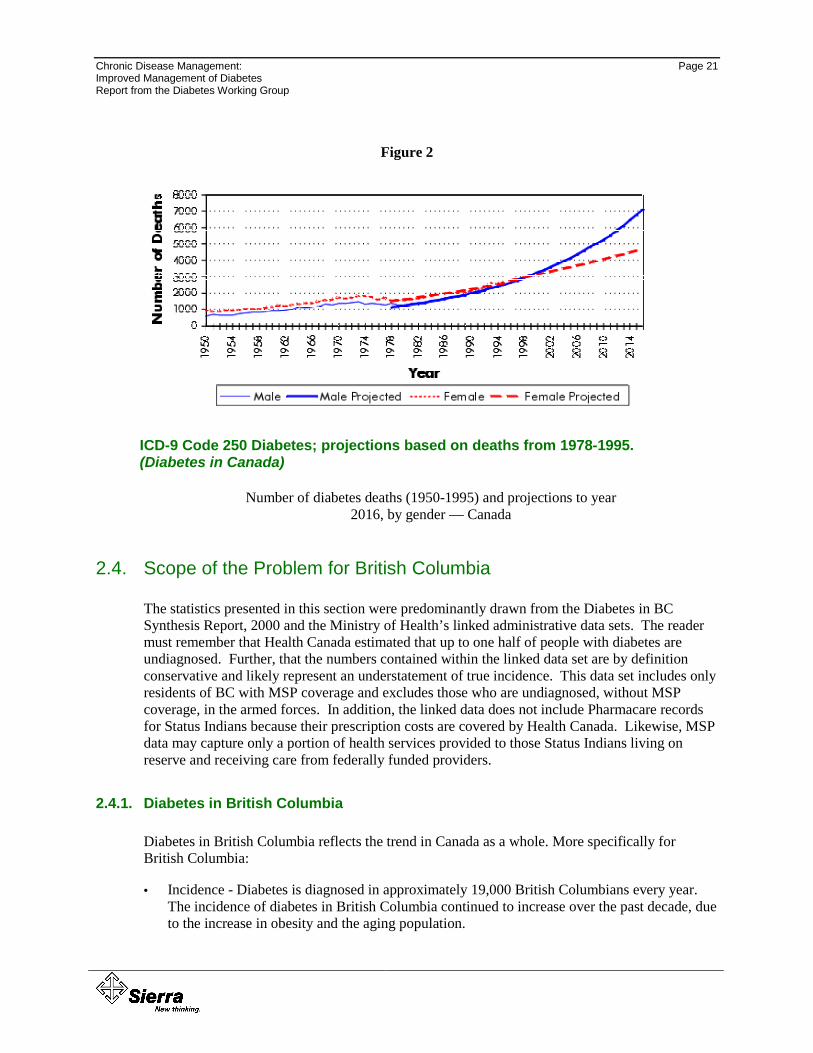
Health Canada projections into the year 2016 show an exponential increase in the number of diabetes deaths among males to 7000 annually, and a more linear increase among females to just under 5000, giving a total number of deaths due to diabetes of 12,000 annually.
Chronic Disease Management: Page 21 Improved Management of Diabetes Report from the Diabetes Working Group
Figure 2
ICD-9 Code 250 Diabetes; projections based on deaths from 1978-1995. (Diabetes in Canada)
Number of diabetes deaths (1950-1995) and projections to year 2016, by gender — Canada
2.4. Scope of the Problem for British Columbia
The statistics presented in this section were predominantly drawn from the Diabetes in BC Synthesis Report, 2000 and the Ministry of Health’s linked administrative data sets. The reader must remember that Health Canada estimated that up to one half of people with diabetes are undiagnosed. Further, that the numbers contained within the linked data set are by definition conservative and likely represent an understatement of true incidence. This data set includes only residents of BC with MSP coverage and excludes those who are undiagnosed, without MSP coverage, in the armed forces. In addition, the linked data does not include Pharmacare records for Status Indians because their prescription costs are covered by Health Canada. Likewise, MSP data may capture only a portion of health services provided to those Status Indians living on reserve and receiving care from federally funded providers.
2.4.1. Diabetes in British Columbia
Diabetes in British Columbia reflects the trend in Canada as a whole. More specifically for British Columbia:
• Incidence - Diabetes is diagnosed in approximately 19,000 British Columbians every year. The incidence of diabetes in British Columbia continued to increase over the past decade, due to the increase in obesity and the aging population.
Page 22
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
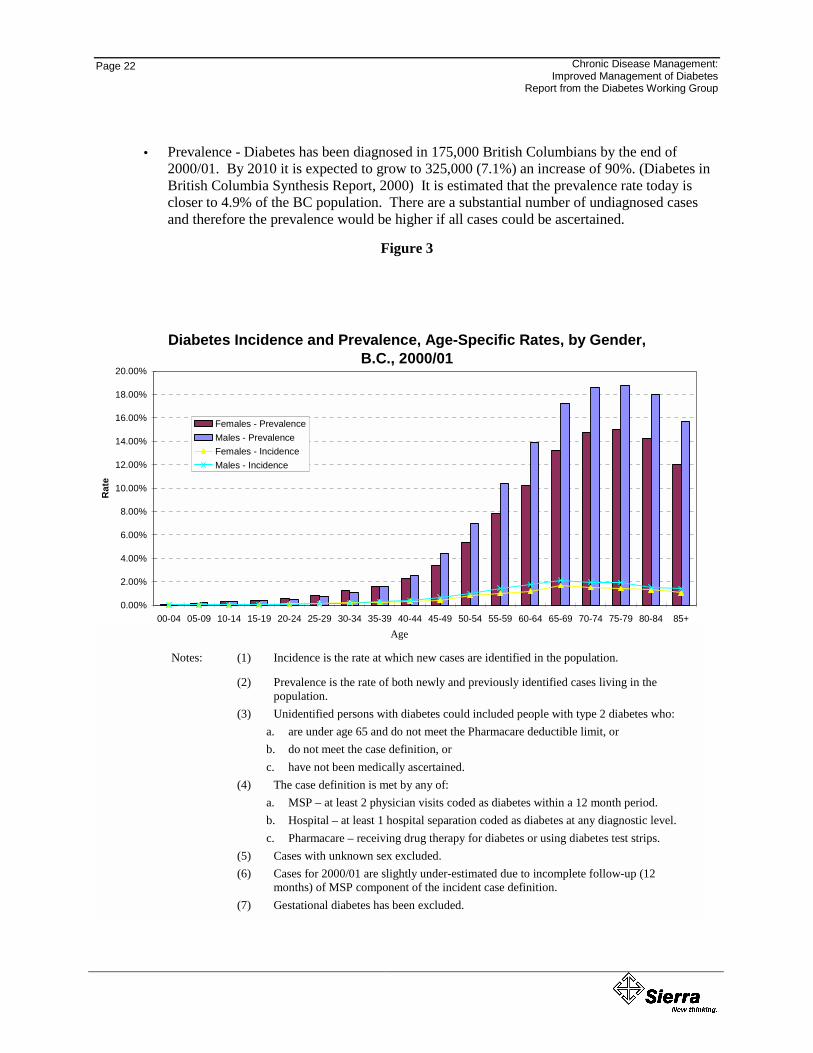
• Prevalence - Diabetes has been diagnosed in 175,000 British Columbians by the end of 2000/01. By 2010 it is expected to grow to 325,000 (7.1%) an increase of 90%. (Diabetes in British Columbia Synthesis Report, 2000) It is estimated that the prevalence rate today is closer to 4.9% of the BC population. There are a substantial number of undiagnosed cases and therefore the prevalence would be higher if all cases could be ascertained.
Figure 3
Diabetes Incidence and Prevalence, Age-Specific Rates, by Gender, B.C., 2000/01
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
14.00%
16.00%
18.00%
20.00%
00-04 05-09 10-14 15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85+Age
Rat
e
Females - PrevalenceMales - PrevalenceFemales - IncidenceMales - Incidence
Notes: (1) Incidence is the rate at which new cases are identified in the population. (2) Prevalence is the rate of both newly and previously identified cases living in the population. (3) Unidentified persons with diabetes could include people with type II diabetes who: (a) are under the Pharmacare deductible limit, or (b) do not meet the case definition, or (c) have not been medically ascertained. (4) The case definition is met by any of: (a) MSP - at least 2 physician visits coded as diabetes within a 12-month period. (b) Hospital - at least 1 hospital separation coded as diabetes at any diagnostic level. (c) Pharmacare - receiving drug therapy for diabetes or using diabetes test strips. (5) Cases with unknown sex excluded. (6) Cases for 2000/01 are slightly under-estimated due to incomplete follow-up (12 months) of MSP component of the incident case difinition.
Age
Notes: (1) Incidence is the rate at which new cases are identified in the population.
(2) Prevalence is the rate of both newly and previously identified cases living in the population.
(3) Unidentified persons with diabetes could included people with type 2 diabetes who: a. are under age 65 and do not meet the Pharmacare deductible limit, or b. do not meet the case definition, or c. have not been medically ascertained.
(4) The case definition is met by any of: a. MSP – at least 2 physician visits coded as diabetes within a 12 month period. b. Hospital – at least 1 hospital separation coded as diabetes at any diagnostic level. c. Pharmacare – receiving drug therapy for diabetes or using diabetes test strips.
(5) Cases with unknown sex excluded. (6) Cases for 2000/01 are slightly under-estimated due to incomplete follow-up (12
months) of MSP component of the incident case definition. (7) Gestational diabetes has been excluded.
Chronic Disease Management: Page 23 Improved Management of Diabetes Report from the Diabetes Working Group
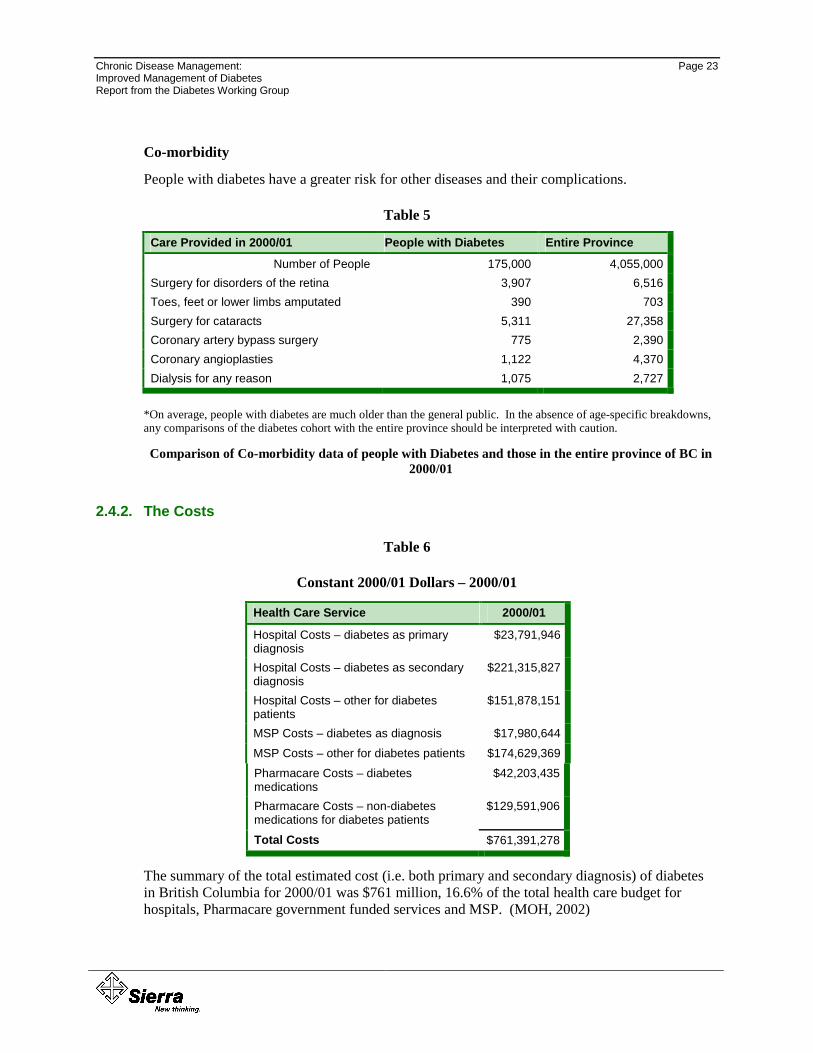
Co-morbidity
People with diabetes have a greater risk for other diseases and their complications.
Table 5
Care Provided in 2000/01 People with Diabetes Entire Province
Number of People 175,000 4,055,000 Surgery for disorders of the retina 3,907 6,516 Toes, feet or lower limbs amputated 390 703 Surgery for cataracts 5,311 27,358 Coronary artery bypass surgery 775 2,390 Coronary angioplasties 1,122 4,370 Dialysis for any reason 1,075 2,727
*On average, people with diabetes are much older than the general public. In the absence of age-specific breakdowns, any comparisons of the diabetes cohort with the entire province should be interpreted with caution.
Comparison of Co-morbidity data of people with Diabetes and those in the entire province of BC in 2000/01
2.4.2. The Costs
Table 6
Constant 2000/01 Dollars – 2000/01
Health Care Service 2000/01
Hospital Costs – diabetes as primary diagnosis
$23,791,946
Hospital Costs – diabetes as secondary diagnosis
$221,315,827
Hospital Costs – other for diabetes patients
$151,878,151
MSP Costs – diabetes as diagnosis $17,980,644 MSP Costs – other for diabetes patients $174,629,369 Pharmacare Costs – diabetes medications
$42,203,435
Pharmacare Costs – non-diabetes medications for diabetes patients
$129,591,906
Total Costs $761,391,278
The summary of the total estimated cost (i.e. both primary and secondary diagnosis) of diabetes in British Columbia for 2000/01 was $761 million, 16.6% of the total health care budget for hospitals, Pharmacare government funded services and MSP. (MOH, 2002)
Page 24
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
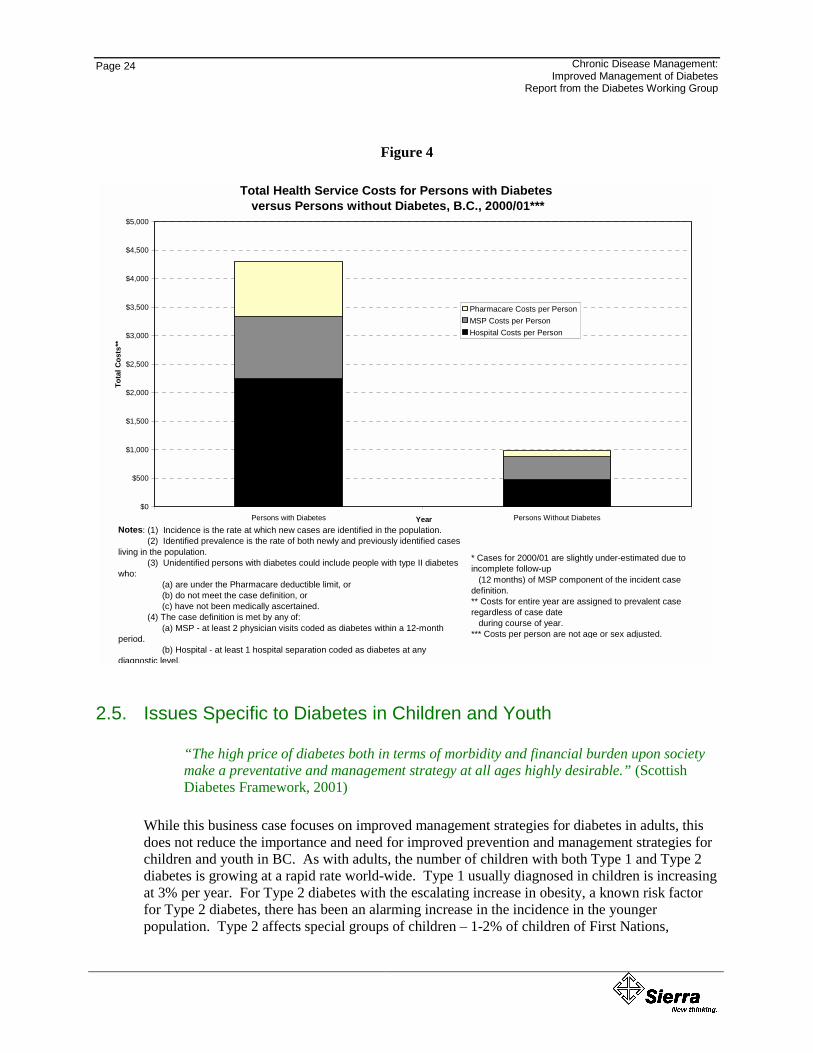
Figure 4
$0
$500
$1,000
$1,500
$2,000
$2,500
$3,000
$3,500
$4,000
$4,500
$5,000
Persons with Diabetes Persons Without DiabetesYear
Tota
l Cos
ts**
Pharmacare Costs per PersonMSP Costs per PersonHospital Costs per Person
Total Health Service Costs for Persons with Diabetes versus Persons without Diabetes, B.C., 2000/01***
Notes: (1) Incidence is the rate at which new cases are identified in the population. (2) Identified prevalence is the rate of both newly and previously identified cases living in the population. (3) Unidentified persons with diabetes could include people with type II diabetes who: (a) are under the Pharmacare deductible limit, or (b) do not meet the case definition, or (c) have not been medically ascertained. (4) The case definition is met by any of: (a) MSP - at least 2 physician visits coded as diabetes within a 12-month period. (b) Hospital - at least 1 hospital separation coded as diabetes at any diagnostic level.
* Cases for 2000/01 are slightly under-estimated due to incomplete follow-up (12 months) of MSP component of the incident case definition.** Costs for entire year are assigned to prevalent case regardless of case date during course of year.*** Costs per person are not age or sex adjusted.
2.5. Issues Specific to Diabetes in Children and Youth
“The high price of diabetes both in terms of morbidity and financial burden upon society make a preventative and management strategy at all ages highly desirable.” (Scottish Diabetes Framework, 2001)
While this business case focuses on improved management strategies for diabetes in adults, this does not reduce the importance and need for improved prevention and management strategies for children and youth in BC. As with adults, the number of children with both Type 1 and Type 2 diabetes is growing at a rapid rate world-wide. Type 1 usually diagnosed in children is increasing at 3% per year. For Type 2 diabetes with the escalating increase in obesity, a known risk factor for Type 2 diabetes, there has been an alarming increase in the incidence in the younger population. Type 2 affects special groups of children – 1-2% of children of First Nations,

Chronic Disease Management: Page 25 Improved Management of Diabetes Report from the Diabetes Working Group
Hispanic or black origin, and up to 4% of adolescent girls – and has devastating consequences of early-onset complications, such as heart-attacks, strokes, blindness and amputations in 30-year-olds. (American Diabetes Association, 1999)
Clearly diabetes is a significant health issue in children and youth. There is further work to be undertaken including a need to address strategies that are outside of this business plan.
2.5.1. The Scope of the Problem in BC – Increasing Numbers of Children
Table 7
• In 2000/01 there were 2635 diabetes patients up to and including 19 years of age in BC. (MOH, 2001)
• In 1999, 950 patients were seen in the BC Children’s Diabetes Clinic – an increase of 300 patients over the past 6 years
• In 1999, there were 136 newly diagnosed cases in the BC Children’s Diabetes Day Care program – almost double the number of cases 6 years ago
• Increasing numbers of children and teens with Type 2 diabetes are being referred, particularly in the non-white immigrant and First Nations populations
• There has been a disturbing two-fold increase in the incidence of Type 1 diabetes in toddlers with diabetes: manipulation of diet and insulin therapy is more difficult in younger children who rapidly progress through developmental stages and need to grow.
• There has been an increase in the incidence of children with other disorders who develop diabetes – Cystic Fibrosis, Oncology.
• About 7% of diabetes children also have Celiac Disease, an immune-mediated inflammation of the small intestine caused by gluten in grains, which requires complicated diet management
(BC Children’s Hospital)
Chronic Disease Management: Page 27 Improved Management of Diabetes Report from the Diabetes Working Group
333... PPPRRRIIIMMMAAARRRYYY PPPRRREEEVVVEEENNNTTTIIIOOONNN
This document presents the business case and financial analysis for the prevention and management of diabetes complications and disabilities. The limited scope of the analysis does not in any way minimize either the importance, or the need for, an investment in primary prevention.
Type 2 diabetes comprises approximately 90% of all cases of diabetes in British Columbia. Over the next 10 years, the prevalence of Type 2 diabetes is expected to increase dramatically; mainly as a result of the aging of the population. Moreover, the incidence of obesity, a known risk factor for Type 2 diabetes, is steadily increasing among both children and adults. The trend towards increased incidence of Type 2 diabetes appears, however, to be reversible. Unfortunately, there is no strong evidence from the literature on successful prevention strategies for Type 1 diabetes.
Given the above and the evidence from previous sections, the focus and efforts towards primary prevention strategies cannot be understated. It is significant that this year, Population Health and Wellness, Ministry of Health Planning is working with partners, including health authorities, to develop a prevention and wellness strategy focusing on four strategic priorities for the primary prevention of chronic diseases such as Type 2 diabetes. These priorities are increasing physical activity and healthy eating and decreasing tobacco use and alcohol and substance misuse. The prevention and wellness strategy will reflect collaborative action and integrated approaches to address these common modifiable risk factors. The strategy will also include an injury prevention component.
It is important in this document to provide a brief review of some recent findings of the success and challenges of primary prevention before moving to the prevention and management of those people with diabetes.
3.1. Type 2 Diabetes Can Be Prevented or Delayed – The Evidence Base
The findings of recent clinical trials have concluded that the risk of developing Type 2 diabetes among people with impaired glucose tolerance or impaired fasting glucose can be reduced dramatically simply through diet and exercise.
The Diabetes Prevention Program, a major clinical trial sponsored by the National Institutes of Health (NIH), found that in comparison to a control group, study participants who walked or participated in moderate exercise for 150 minutes a week, and lost 5-7 percent of their body weight reduced their risk of developing Type 2 diabetes by 58 percent. Importantly, the study also found that this type of lifestyle intervention successfully reduced the risk of developing Type 2 diabetes among high risk groups, namely individuals age 60 and older, women with a history of gestational diabetes, and people with a first-degree relative with Type 2 diabetes. (Diabetes Research Group, 2002)

Page 28
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
The study also found that the risk of developing Type 2 diabetes was reduced by 31 percent among participants whose sole intervention was the drug metformin. This finding did not, however, apply for older participants.
International studies have similarly shown that Type 2 diabetes can be prevented through lifestyle changes. For example, the findings of a Finnish randomized clinical trial reported in the New England Journal of Medicine indicated that the risk of developing diabetes was reduced by 58 percent among participants who were randomly assigned to an intervention group that received counseling aimed at reducing weight, and increasing physical activity. (Tuomilehto et al, 2001) Moreover, studies conducted in both China (Pan et al, 1997) and in Sweden (Eriksson et al, 1991) reported substantial reductions in the incidence of Type 2 diabetes among high-risk participants who improved their diet and activity levels.
3.1.1. Reversing the Trend
The prevalence of diabetes within BC is projected to increase in a manner similar to many other jurisdictions. The following figure illustrates the potential for management through lifestyle modification programs.
Figure 5
Diabetes Prevalence Projections, Cases, B.C., 1995/96 to 2012/13
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
1995
/96
1996
/97
1997
/98
1998
/99
1999
/00
2000
/01
2001
/02
2002
/03
003/
04
004/
05
005/
06
006/
07
007/
08
008/
09
009/
10
010/
11
011/
12
012/
13
Prev
alen
t Cas
es*
Projected Rate No Reduction IncidenceRate 25% Reduction Incidence By Lifestyle Modification Program**Rate 50% Reduction Incidence By Lifestyle Modification Program***
* Prevalence is the rate of all cases occurring in the population, both new and existing1995/96 to 2000/01, applied to the future population projections from BC STATS.**Assumes that approximately half of the lifestyle modification benefit was achieved (2years, and sustained thereafter, as per Diabetes Prevention Program Research Groupor Metformin", NEJM, Vol. 346, No. 6, Feb. 7, 2002: 393-.***Assumes that approximately the full lifestyle benefit was achieved (50% deuction in
Actual Prevalence
Lifestyle Modification Program Beginning 2003/04
* Prevalence is the rate of all cases occurring in the populapreliminary extrapolation of data for the period 1995/96 toSTATS. ** Assumes that approximately half of the lifestyle modifthroughout the province, implemented over 5 years, and su Group. * Reduction in the incidence of Type 2 diabetes wFeb. 7, 2002:393 *** Assumes that approximately the full lifestyle benefit w
2 2 2 2 2 2 2 2 2 2
Year cases. Projection based on a preliminary extrapolation of data for the period
5% reduction in incidence) throughout the province, implemented over 5 , "Reductiion in the Incidence of Type 2 Diabetes with Lifestyle Intervention
incidence).
Year tion, both new and existing cases. Projection based on a 2000/01, applied to the future population projections from BC
ication benefit was achieved (25% reduction in incidence) stained thereafter, as per Diabetes Prevention Program Researchith Lifestyle Intervention or Metformin, NEJM, Vol. 346, No. 6,
as achieved (50% reduction in incidence)
Chronic Disease Management: Page 29 Improved Management of Diabetes Report from the Diabetes Working Group
3.2. Translating Evidence into Action
A convincing evidence base exists to support the implementation of interventions that affect the lifestyle of individuals at risk for Type 2 diabetes. Reversing the trend toward increased incidence of Type 2 diabetes through implementation of interventions aimed at reducing sedentary lifestyle and obesity could serve to contain costs. Similarly, the economic benefit of reducing the prevalence of diabetes, and thus health service utilization, is obvious. Nonetheless, historically, preventive efforts have often been underutilized.
Several reasons for this underutilization have been identified. Specifically, prevention tends to be subtle and therefore often under funded; there is a tendency to focus on crisis; it often takes several years for the benefits of prevention to emerge; and well-resourced, carefully planned, and strategically marketed products that are not conducive to health promotion often overwhelm prevention efforts.
Prevention efforts are more likely to be successful if individual and environmental components are targeted. At the individual level, social marketing, prevention programs and services, and public policies can both raise public awareness of the issues that affect their health as well as predispose them to, and support them in, influencing these factors. Moreover, prevention initiatives will more likely be successful in an environment where implementation involves multiple partners in multiple settings such as health care facilities, workplaces, schools, local communities, municipalities and cities; where people are at the center of decisions and actions, and have access to education and information, programs, and an environment that helps them develop skills needed to enable health lifestyle choices.
In 2002, the American Diabetes Association and the National Institutes of Diabetes and Digestive and Kidney Disease have concluded that diabetes prevention meets most of the conditions used to decide whether program initiation to prevent a disease is justified, namely:
• The disease imposes a significant burden on the affected population;
• The progression of the disease can be measured because its early development and natural history are well understood, and
• A safe, acceptable, and predictive test to detect the disease state exists.
The evidence base indicates that safe, reliable and effective methods to prevent or delay disease onset exist. A caution – the effort to find individuals who are at high risk for the disease and the cost of the intervention should be cost effective, has not yet been empirically established. Whereas it has been argued that screening for diabetes during routine encounters with the health care system is the most cost-effective way of identifying individuals at risk for diabetes, studies have not been published regarding the cost effectiveness of screening for impaired glucose tolerance or impaired fasting glucose. (Engelgua, et al, 1988)
However, the American Diabetes Association, the National Institutes of Diabetes and Digestive and Kidney Disease have argued that active case finding is a justifiable activity because the
Page 30
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
complications of diabetes bear a large burden, and the evidence clearly shows that diabetes can be delayed or even prevented.
Furthermore, the lifestyle intervention that was shown to delay or prevent diabetes onset (i.e., weight loss and exercise) has also been shown to have the additional benefits of improving cardiovascular health and quality of life. (NIH, 1998 and NIH Consensus Development Panel on Physician Activity and Cardiovascular Health, 1996) Based on current evidence, the American Diabetes Association has recommended that screening to detect people with impaired glucose tolerance or impaired fasting glucose during health care office visits should be considered for individuals 45 years and older, and strongly recommended in those over 45 years and overweight (BMI> 25 kg/m2). Screening for individuals younger than 45 years should be considered if they are overweight and have another risk factor for diabetes (e.g., first-degree relative with diabetes, etc). (American Diabetes Association, the National Institutes of Diabetes and Digestive and Kidney Disease, 2002)
It should be noted that while targeting at-risk individuals is important in reversing the trend towards increased incidence of diabetes, projections indicate that individuals at medium or low risk for diabetes will actually comprise the greatest number of new cases of Type 2 diabetes over the next few years. Ultimately, a population-based approach aimed at changing the social, policy, and environmental norms that create conditions of risk for the entire population, in combination with the high-risk approach, is considered the best avenue for achieving the greatest impact.
Diabetes is one of the most costly and burdensome chronic diseases. Projections indicate that the prevalence of this disease is on the increase, mainly as a result of BC’s aging population. A case can be made that interventions that successfully sustain weight reduction and/or maintain healthy weight through physical activity and healthy eating should be part of diabetes strategies. Again, this is why the Prevention and Wellness Strategy focusing on chronic disease primary prevention including diabetes is so important for BC. (MOHP Service Plan, 2002)
Chronic Disease Management: Page 31 Improved Management of Diabetes Report from the Diabetes Working Group
444... TTTHHHEEE PPPOOOTTTEEENNNTTTIIIAAALLL FFFOOORRR MMMAAANNNAAAGGGEEEMMMEEENNNTTT OOOFFF DDDIIIAAABBBEEETTTEEESSS
In all developed nations, the management of people with chronic disease consumes a large portion of health care expenditures. For example, in the United States today chronic disease is the major cause of disability, is the main reason people seek health care and consumes 70% of health care spending. (Holman et al, 2000). The Institute of the Future in describing the ‘juggernaut of chronic illness’ predicts that by 2010 some 120 million Americans, about 40% of the total population, will be living with a chronic illness and 40% of these will have at least two chronic conditions. The Institute estimates that the direct medical costs of chronic conditions in the US will total $600 billion per year by 2010 and goes on to say that if we try to extend today’s approach to chronic care, which is ‘fragmented, system-centric and non-empowering’, the system will collapse. (Mettler, 2000) Yet despite these predictions chronic disease is often poorly treated and ineffectively prevented.
The burden of chronic disease not only impacts the health care system in terms of increased service utilization and cost; it also has profound impacts on people’s lives. People living with chronic disease face limitations in their daily activities, some find it difficult to maintain work and social activities, and others are unable to live independently.
4.1. The Need
Regardless of age at onset, whether their aetiology is known, or whether their manifestations are primarily physical or psychosocial, essentially all chronic conditions present a common set of challenges to the sufferers and their families – dealing with symptoms, disability, emotional impacts, complex medication regimes, difficult lifestyle adjustments, and obtaining helpful medical care. Many chronically ill persons wrestle with the physical, psychological and social demands of their illness without much help from a primary health care system that is neither organized, nor explicitly funded, to provide these supports. (Wagner, 2001)
A recent Cochrane Collaboration Review concluded that successful approaches to the management of a chronic disease are most often multifaceted, and include one or more of the following:
• Provider oriented components such as continuing education or physician feedback;
• Organizational changes in personnel or the management of visits and follow up;
• Information systems changes, and
• Patient oriented interventions of an educational or supportive nature.
Combinations of various forms of provider education, computerized tracking and reminder systems, and organized approaches to follow up achieved the greatest success in improving process indicators. However, even complex interventions that were targeted solely at providers did not impact actual outcome unless also accompanied by interventions directed at patients.
Page 32
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
4.2. System Design
While acute medicine recognized cure as the objective and measure of success, a different model is required to manage chronic disease. In the management of chronic disease we need to shift from an exclusive focus on the disease process itself, to a broader focus on the person with the disease. While ‘cure’ remains unquestionably an appropriate goal, other goals are also important – goals such as restoring functional capacity; relieving suffering; preventing associated illness and depression as examples.
“current health care policy, finance, information and management structures lock in place a delivery model that defies the logic of chronic illness” (Bringewatt, 2001)
Throughout this document deficits in the current management of chronic disease will be underscored. These deficits are the inevitable consequence of the current system design as opposed to being attributable to the performance of any group(s) of providers. While medical science and technology have evolved to the extent that many of these chronic conditions can be well managed, the current health care system and incentive structures create the unfortunate circumstance where many of those with these conditions are receiving less than ideal, evidence-based, care.
In Canada the healthcare system was established and funded to respond rapidly and efficiently to acute illness and injury. It has continued to maintain this acute care orientation and, as a result, is lagging behind demographic trends. Recent surveys suggest that fewer than half of US patients with hypertension, depression, diabetes and asthma are receiving appropriate treatment. (Wagner, 2001) The evidence suggests that this situation is mirrored in Canada.
“by virtue of the nature of illness with which it deals and the characteristics of the clients it serves, good chronic care is intrinsically much more difficult to achieve than is most acute care” (Vladeck, 2001)
Ideal chronic care requires coordinated, proactive, interdisciplinary teams, using best practice guidelines to support a patient well prepared to act as the overall manager of their own care. The result of the failure of the Canadian system to keep pace with the changing demographics is unnecessary complications with associated unnecessary acute care admissions and costs. This, combined with the demographic projected escalation in prevalence create a scenario that is not financially sustainable and can and should be prevented.
“What is urgently required is system redesign, alignment of structures, processes and incentives to support proactive, continuous, coordinated chronic care.” (Wagner, 2001)
4.3. The Challenge
Vladeck (2001) identifies the following systemic obstacles to optimal chronic disease care:
Chronic Disease Management: Page 33 Improved Management of Diabetes Report from the Diabetes Working Group
• The challenge of changing established practice patterns and styles of the wide range of providers involved in the management of chronic disease;
• Organizational design and performance - since new ways of delivering chronic care must be developed within a health care delivery system still largely oriented and preoccupied with acute, short term illness, and
• The above eventually intersect with the third category – public policy which impedes organizational reform in the health care delivery systems in a number of subtle ways.
4.4. Key Features of Chronic Disease Management
Approaches to chronic disease management include some combination of initiatives - treatment and prevention - to build capacity at both the patient and physician level. In a special edition of the British Medical Journal on chronic disease management (February, 2000), essential ingredients of chronic disease management were set forth. They include the following:
• Support for patients in the management of their disease;
• Explicit delegation of tasks for primary care physicians;
• Optimization of drug management;
• Intensive and systematic patient follow-up;
• Use of interdisciplinary teams to deliver care;
• Application of performance measurement tools to track quality of care and evaluate effectiveness of interventions;
• Effective organization of care and services to achieve health outcomes and lower costs, and
• Research on innovative methods to support people with chronic illness.
A notable chronic disease management initiative is Improving Chronic Illness, a national program of the Robert Wood Johnson (RWJ) Foundation in the United States. This program led to the development of the Chronic Care Model that integrates the available literature about promising strategies for chronic disease management. (Wagner et al, 1996) The Chronic Care Model identifies the essential elements of a system that encourages high-quality chronic disease management which includes: the community; the health system; self-management support; delivery system design; decision support and clinical information systems.
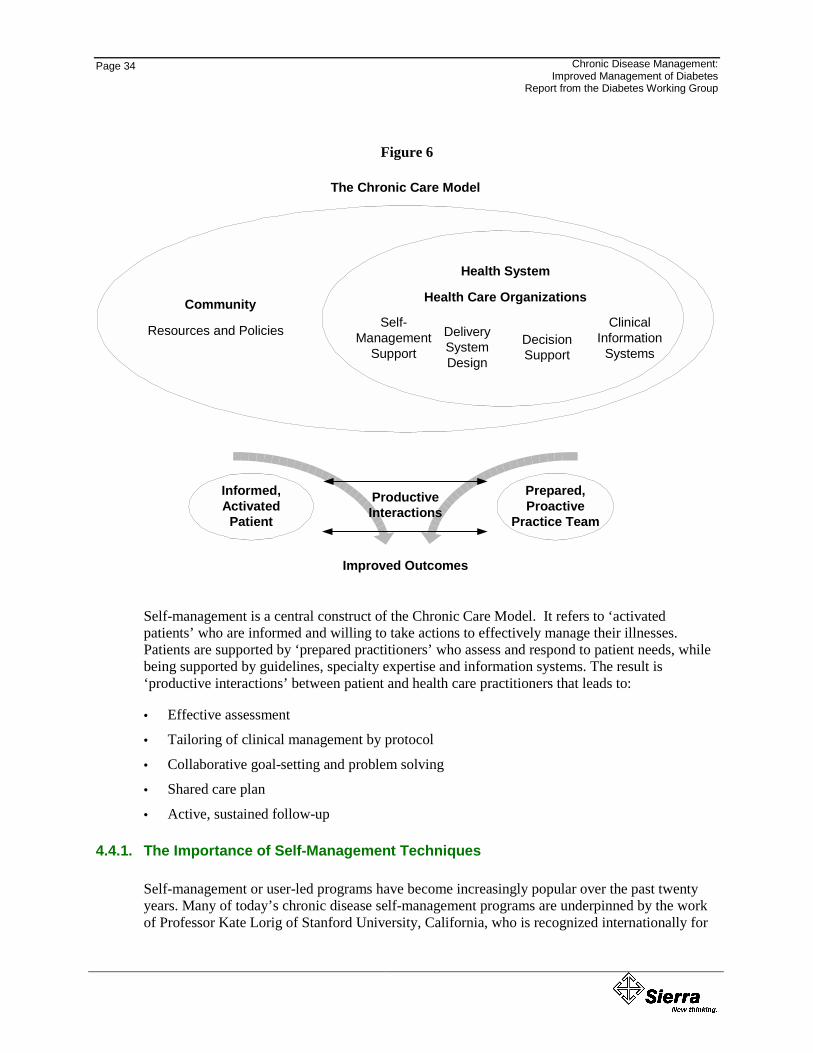
Page 34
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
Figure 6
Informed,Activated
Patient
Prepared,Proactive
Practice Team
ProductiveInteractions
Improved Outcomes
Community
Resources and Policies
Health Care Organizations
Health System
Self-Management
SupportDeliverySystemDesign
DecisionSupport
ClinicalInformation
Systems
The Chronic Care Model
Self-management is a central construct of the Chronic Care Model. It refers to ‘activated patients’ who are informed and willing to take actions to effectively manage their illnesses. Patients are supported by ‘prepared practitioners’ who assess and respond to patient needs, while being supported by guidelines, specialty expertise and information systems. The result is ‘productive interactions’ between patient and health care practitioners that leads to:
• Effective assessment
• Tailoring of clinical management by protocol
• Collaborative goal-setting and problem solving
• Shared care plan
• Active, sustained follow-up
4.4.1. The Importance of Self-Management Techniques
Self-management or user-led programs have become increasingly popular over the past twenty years. Many of today’s chronic disease self-management programs are underpinned by the work of Professor Kate Lorig of Stanford University, California, who is recognized internationally for
Chronic Disease Management: Page 35 Improved Management of Diabetes Report from the Diabetes Working Group
her work in this field. Locally, Dr. Patrick McGowan of the University of Victoria, British Columbia has conducted research in the self-management of arthritis and published several articles associated with the benefits of self-management models.
Self-management programs recognize that people with chronic illness need to deal not only with their disability but also with pain, stigma and stress on a daily basis. The programs develop coping skills and typically cover topics such as cognitive symptom management, exercise, nutrition, problem solving and communication with health professionals. Additionally, teams of trained volunteers, who themselves have a chronic condition, often lead self-management programs. By providing patients with information and developing knowledge of their illness, self-management programs encourage patients to work in partnership with health care providers. Patients feel more capable of dealing with the many challenges they face and thereby, gain greater control over their disease and their lives.
Effective self-management is more than providing information or telling patients what to do. It requires giving patients a central role in determining their care, one that fosters a sense of responsibility for their own health. Under a chronic disease self-management approach, patients and health care providers work together to define problems, set priorities, establish goals, create treatment plans and solve problems along the way.
One exemplar initiative has been developed and implemented in the United Kingdom. It is described in a recently released document entitled, The Expert Patient: A New Approach to Chronic Disease Management for the 21st Century. (UK Department of Health, 2001) The Expert Patient program is designed to reduce the severity of symptoms and improve the confidence, resourcefulness and self-efficacy of patients so that they are empowered to assume responsibility for the management of their disease. An underlying assumption of this initiative is that “the knowledge and experience held by the patient has for too long been an ‘untapped resource, and that today’s patients with chronic diseases need not be ‘mere recipients of care’.” Rather, they should become key decision-makers in the treatment and management of their disease.
4.5. Chronic Disease Management and Diabetes
As is the case with chronic disease generally, diabetes can be managed and most of its complications avoided or minimized. Although there is no cure for diabetes, close monitoring of blood sugar levels, blood pressure, and ongoing interaction with a health care professional can help individuals stave off the insidious effects of the disease, improve quality of life and, as a result, reduce associated healthcare costs.
It is recognized that the cost/benefit analyses in health care are fraught with methodological and other related challenges. However, this plan must base its arguments and assumptions on the literature as it exists today. Most of the relevant evidence in chronic disease comes from other jurisdictions, with their associated systemic and cultural differences. The review is limited to literature from the US, UK, and the minimal available from Canadian jurisdictions as they are the most similar to the Canadian system while recognizing that there are key differences.
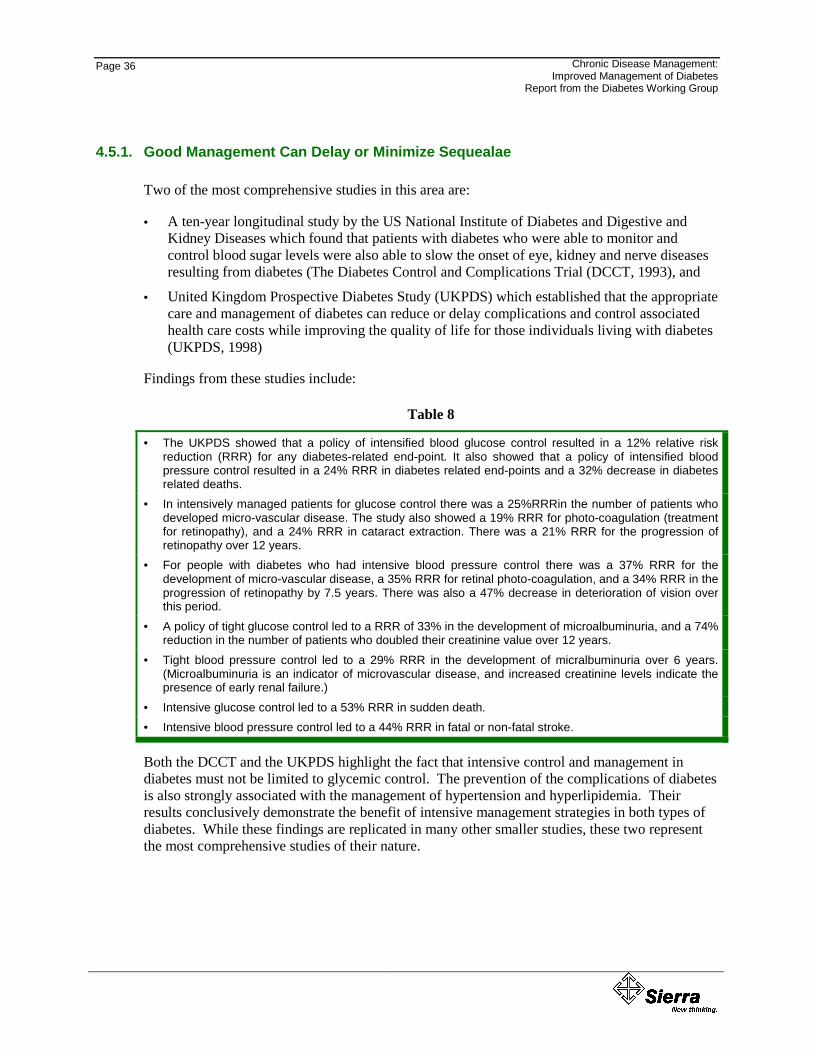
Page 36
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
4.5.1. Good Management Can Delay or Minimize Sequealae
Two of the most comprehensive studies in this area are:
• A ten-year longitudinal study by the US National Institute of Diabetes and Digestive and Kidney Diseases which found that patients with diabetes who were able to monitor and control blood sugar levels were also able to slow the onset of eye, kidney and nerve diseases resulting from diabetes (The Diabetes Control and Complications Trial (DCCT, 1993), and
• United Kingdom Prospective Diabetes Study (UKPDS) which established that the appropriate care and management of diabetes can reduce or delay complications and control associated health care costs while improving the quality of life for those individuals living with diabetes (UKPDS, 1998)
Findings from these studies include:
Table 8
• The UKPDS showed that a policy of intensified blood glucose control resulted in a 12% relative risk reduction (RRR) for any diabetes-related end-point. It also showed that a policy of intensified blood pressure control resulted in a 24% RRR in diabetes related end-points and a 32% decrease in diabetes related deaths.
• In intensively managed patients for glucose control there was a 25%RRRin the number of patients who developed micro-vascular disease. The study also showed a 19% RRR for photo-coagulation (treatment for retinopathy), and a 24% RRR in cataract extraction. There was a 21% RRR for the progression of retinopathy over 12 years.
• For people with diabetes who had intensive blood pressure control there was a 37% RRR for the development of micro-vascular disease, a 35% RRR for retinal photo-coagulation, and a 34% RRR in the progression of retinopathy by 7.5 years. There was also a 47% decrease in deterioration of vision over this period.
• A policy of tight glucose control led to a RRR of 33% in the development of microalbuminuria, and a 74% reduction in the number of patients who doubled their creatinine value over 12 years.
• Tight blood pressure control led to a 29% RRR in the development of micralbuminuria over 6 years. (Microalbuminuria is an indicator of microvascular disease, and increased creatinine levels indicate the presence of early renal failure.)
• Intensive glucose control led to a 53% RRR in sudden death. • Intensive blood pressure control led to a 44% RRR in fatal or non-fatal stroke.
Both the DCCT and the UKPDS highlight the fact that intensive control and management in diabetes must not be limited to glycemic control. The prevention of the complications of diabetes is also strongly associated with the management of hypertension and hyperlipidemia. Their results conclusively demonstrate the benefit of intensive management strategies in both types of diabetes. While these findings are replicated in many other smaller studies, these two represent the most comprehensive studies of their nature.
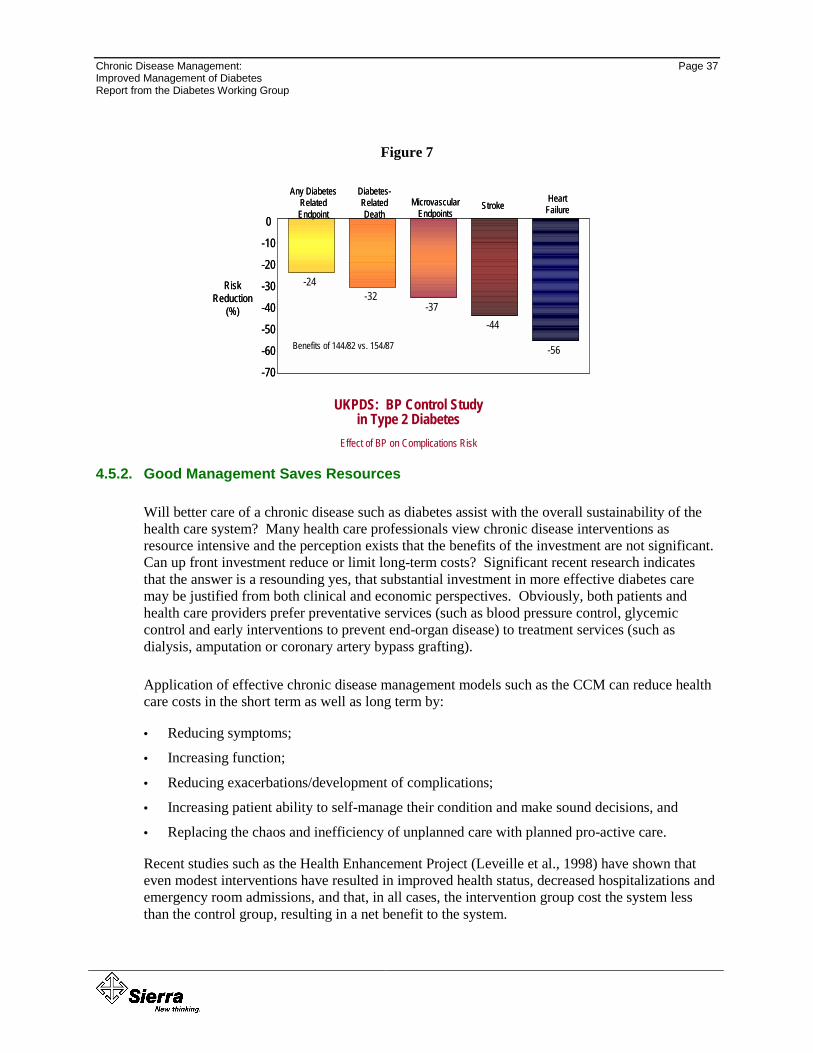
Chronic Disease Management: Page 37 Improved Management of Diabetes Report from the Diabetes Working Group
Figure 7
4.5.2. Good Management Saves Resources
Will better care of a chronic disease such as diabetes assist with the overall sustainability of the health care system? Many health care professionals view chronic disease interventions as resource intensive and the perception exists that the benefits of the investment are not significant. Can up front investment reduce or limit long-term costs? Significant recent research indicates that the answer is a resounding yes, that substantial investment in more effective diabetes care may be justified from both clinical and economic perspectives. Obviously, both patients and health care providers prefer preventative services (such as blood pressure control, glycemic control and early interventions to prevent end-organ disease) to treatment services (such as dialysis, amputation or coronary artery bypass grafting).
Application of effective chronic disease management models such as the CCM can reduce health care costs in the short term as well as long term by:
• Reducing symptoms;
• Increasing function;
• Reducing exacerbations/development of complications;
• Increasing patient ability to self-manage their condition and make sound decisions, and
• Replacing the chaos and inefficiency of unplanned care with planned pro-active care.
Recent studies such as the Health Enhancement Project (Leveille et al., 1998) have shown that even modest interventions have resulted in improved health status, decreased hospitalizations and emergency room admissions, and that, in all cases, the intervention group cost the system less than the control group, resulting in a net benefit to the system.
UKPDS: BP Control Study in Type 2 Diabetes
Effect of BP on Complications Risk
0
-10
-20
-30
-40
-50
-60
-70
-24-32
-37-44
-56Benefits of 144/82 vs. 154/87
Risk Reduction
(%)
Any Diabetes Related Endpoint
Diabetes-Related Death
MicrovascularEndpoints
StrokeHeart
Failure0
-10
-20
-30
-40
-50
-60
-70
-24-32
-37-44
-56Benefits of 144/82 vs. 154/87
Risk Reduction
(%)
Any Diabetes Related Endpoint
Diabetes-Related Death
MicrovascularEndpoints
StrokeHeart
Failure
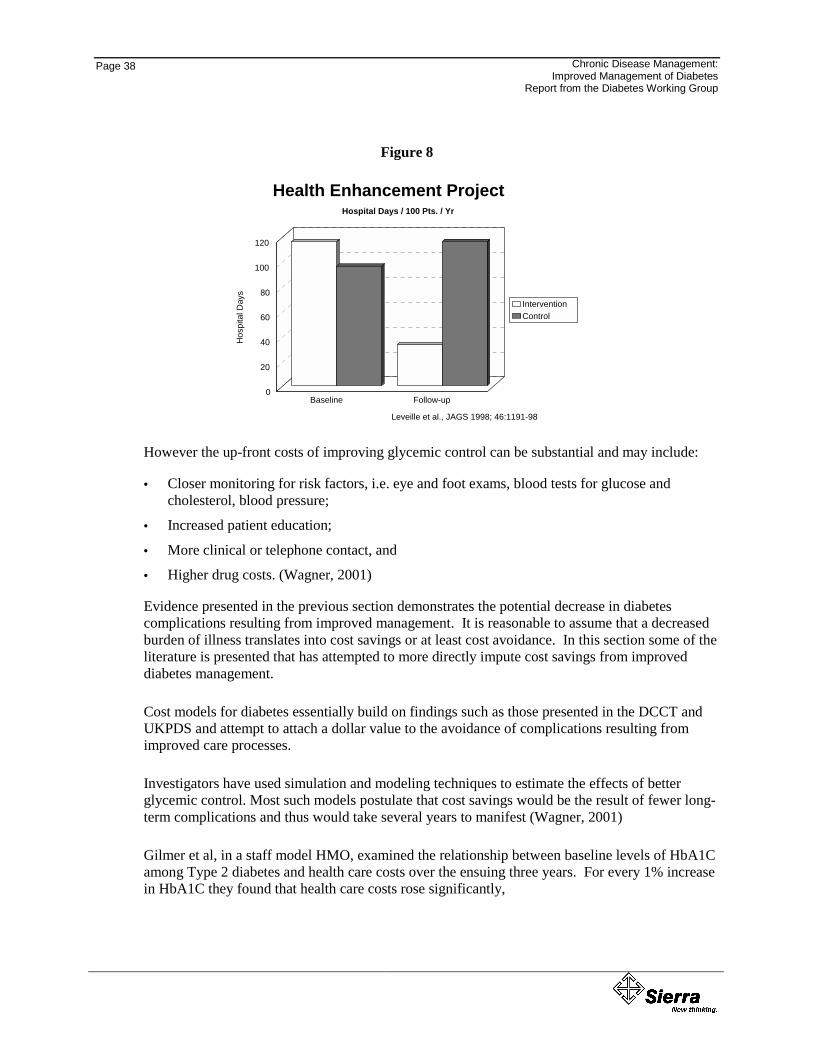
Page 38
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
Figure 8
Health Enhancement ProjectHospital Days / 100 Pts. / Yr
Leveille et al., JAGS 1998; 46:1191-98
Baseline Follow-up0
20
40
60
80
100
120H
ospi
tal D
ays
InterventionControl
However the up-front costs of improving glycemic control can be substantial and may include:
• Closer monitoring for risk factors, i.e. eye and foot exams, blood tests for glucose and cholesterol, blood pressure;
• Increased patient education;
• More clinical or telephone contact, and
• Higher drug costs. (Wagner, 2001)
Evidence presented in the previous section demonstrates the potential decrease in diabetes complications resulting from improved management. It is reasonable to assume that a decreased burden of illness translates into cost savings or at least cost avoidance. In this section some of the literature is presented that has attempted to more directly impute cost savings from improved diabetes management.
Cost models for diabetes essentially build on findings such as those presented in the DCCT and UKPDS and attempt to attach a dollar value to the avoidance of complications resulting from improved care processes.
Investigators have used simulation and modeling techniques to estimate the effects of better glycemic control. Most such models postulate that cost savings would be the result of fewer long-term complications and thus would take several years to manifest (Wagner, 2001)
Gilmer et al, in a staff model HMO, examined the relationship between baseline levels of HbA1C among Type 2 diabetes and health care costs over the ensuing three years. For every 1% increase in HbA1C they found that health care costs rose significantly,
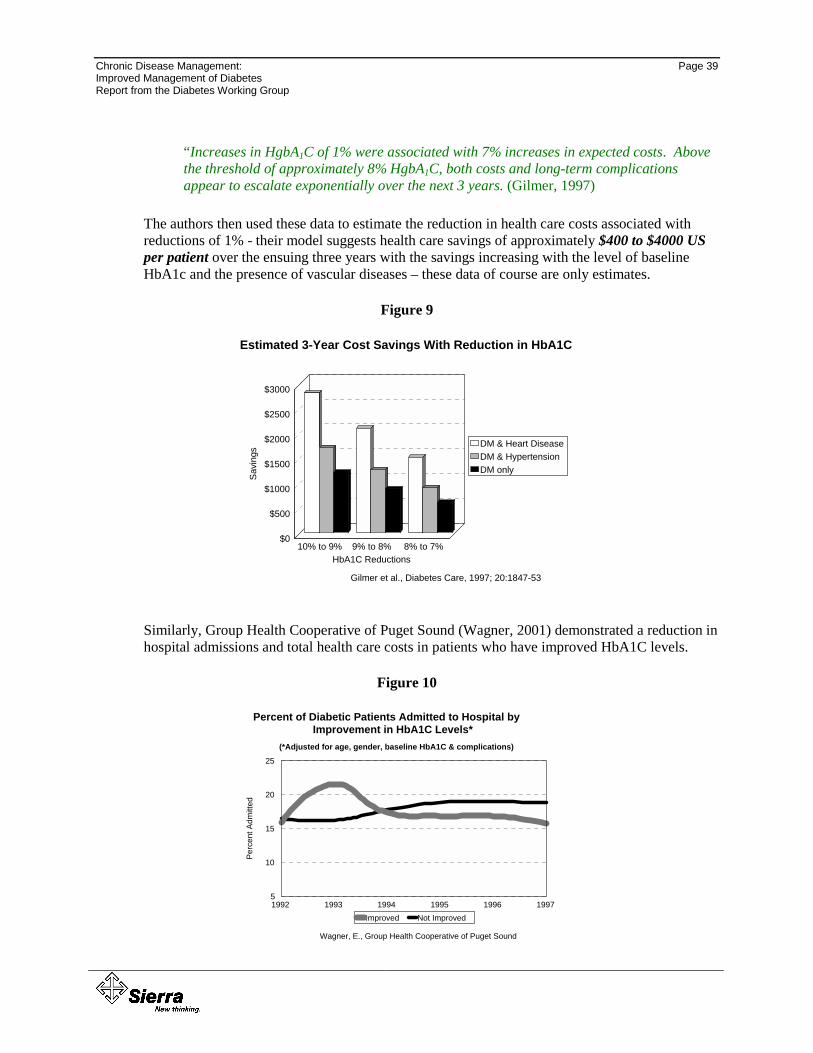
Chronic Disease Management: Page 39 Improved Management of Diabetes Report from the Diabetes Working Group
“Increases in HgbA1C of 1% were associated with 7% increases in expected costs. Above the threshold of approximately 8% HgbA1C, both costs and long-term complications appear to escalate exponentially over the next 3 years. (Gilmer, 1997)
The authors then used these data to estimate the reduction in health care costs associated with reductions of 1% - their model suggests health care savings of approximately $400 to $4000 US per patient over the ensuing three years with the savings increasing with the level of baseline HbA1c and the presence of vascular diseases – these data of course are only estimates.
Figure 9
Estimated 3-Year Cost Savings With Reduction in HbA1C
Gilmer et al., Diabetes Care, 1997; 20:1847-53
10% to 9% 9% to 8% 8% to 7%HbA1C Reductions
$0
$500
$1000
$1500
$2000
$2500
$3000
Savi
ngs DM & Heart Disease
DM & HypertensionDM only
Similarly, Group Health Cooperative of Puget Sound (Wagner, 2001) demonstrated a reduction in hospital admissions and total health care costs in patients who have improved HbA1C levels.
Figure 10
Percent of Diabetic Patients Admitted to Hospital by Improvement in HbA1C Levels*
(*Adjusted for age, gender, baseline HbA1C & complications)
Wagner, E., Group Health Cooperative of Puget Sound
1992 1993 1994 1995 1996 19975
10
15
20
25
Perc
ent A
dmit t
ed
Improved Not Improved
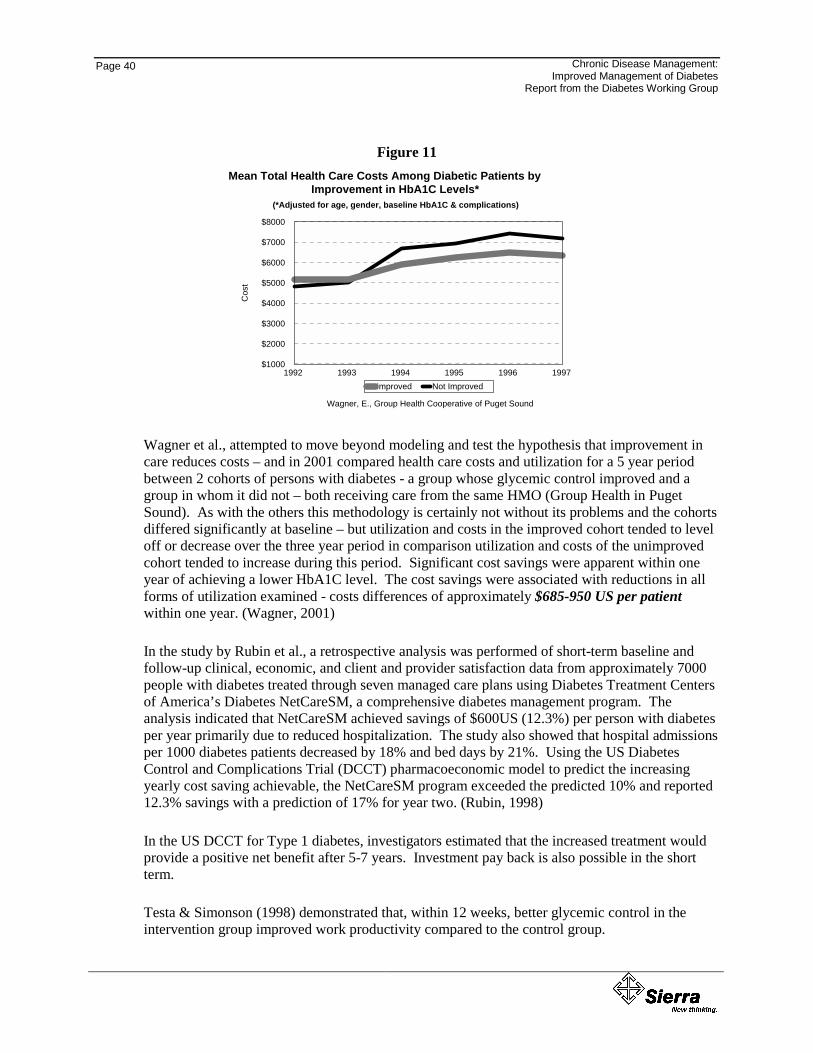
Page 40
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
Figure 11 Mean Total Health Care Costs Among Diabetic Patients by
Improvement in HbA1C Levels*
Wagner, E., Group Health Cooperative of Puget Sound
1992 1993 1994 1995 1996 1997$1000
$2000
$3000
$4000
$5000
$6000
$7000
$8000
Cos
t
Improved Not Improved
(*Adjusted for age, gender, baseline HbA1C & complications)
Wagner et al., attempted to move beyond modeling and test the hypothesis that improvement in care reduces costs – and in 2001 compared health care costs and utilization for a 5 year period between 2 cohorts of persons with diabetes - a group whose glycemic control improved and a group in whom it did not – both receiving care from the same HMO (Group Health in Puget Sound). As with the others this methodology is certainly not without its problems and the cohorts differed significantly at baseline – but utilization and costs in the improved cohort tended to level off or decrease over the three year period in comparison utilization and costs of the unimproved cohort tended to increase during this period. Significant cost savings were apparent within one year of achieving a lower HbA1C level. The cost savings were associated with reductions in all forms of utilization examined - costs differences of approximately $685-950 US per patient within one year. (Wagner, 2001)
In the study by Rubin et al., a retrospective analysis was performed of short-term baseline and follow-up clinical, economic, and client and provider satisfaction data from approximately 7000 people with diabetes treated through seven managed care plans using Diabetes Treatment Centers of America’s Diabetes NetCareSM, a comprehensive diabetes management program. The analysis indicated that NetCareSM achieved savings of $600US (12.3%) per person with diabetes per year primarily due to reduced hospitalization. The study also showed that hospital admissions per 1000 diabetes patients decreased by 18% and bed days by 21%. Using the US Diabetes Control and Complications Trial (DCCT) pharmacoeconomic model to predict the increasing yearly cost saving achievable, the NetCareSM program exceeded the predicted 10% and reported 12.3% savings with a prediction of 17% for year two. (Rubin, 1998)
In the US DCCT for Type 1 diabetes, investigators estimated that the increased treatment would provide a positive net benefit after 5-7 years. Investment pay back is also possible in the short term.
Testa & Simonson (1998) demonstrated that, within 12 weeks, better glycemic control in the intervention group improved work productivity compared to the control group.
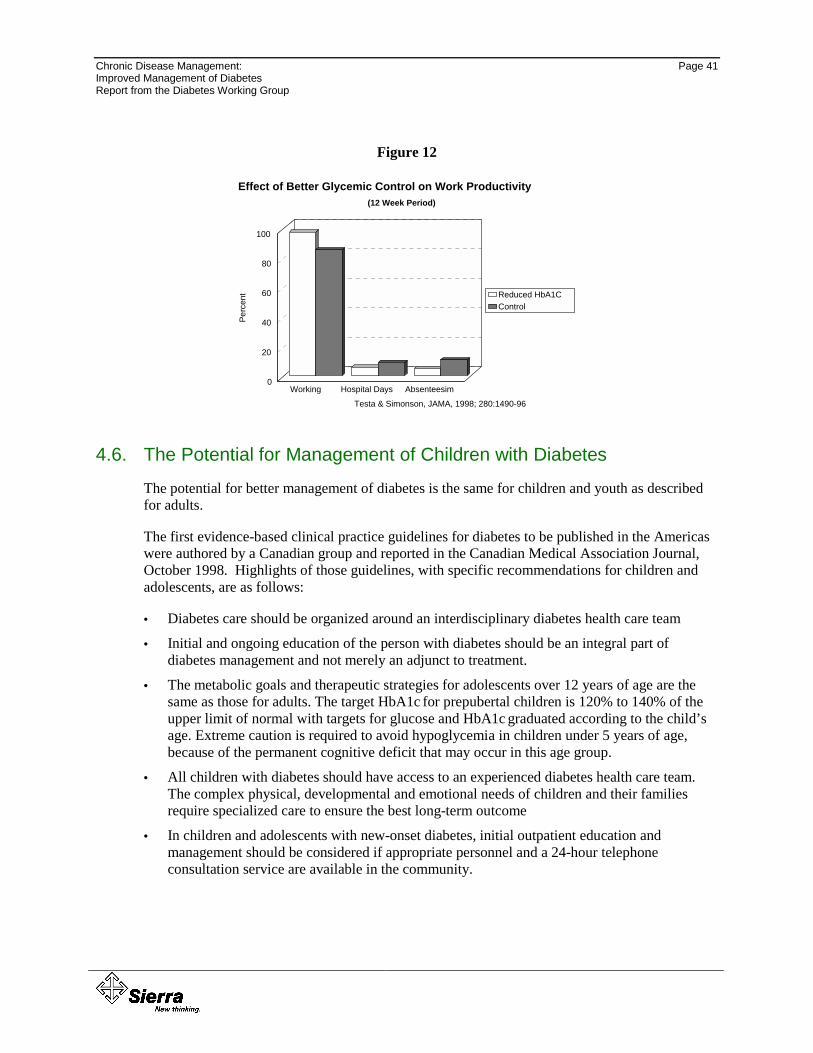
Chronic Disease Management: Page 41 Improved Management of Diabetes Report from the Diabetes Working Group
Figure 12
Effect of Better Glycemic Control on Work Productivity(12 Week Period)
Testa & Simonson, JAMA, 1998; 280:1490-96
Working Hospital Days Absenteesim0
20
40
60
80
100Pe
rcen
t Reduced HbA1CControl
4.6. The Potential for Management of Children with Diabetes
The potential for better management of diabetes is the same for children and youth as described for adults.
The first evidence-based clinical practice guidelines for diabetes to be published in the Americas were authored by a Canadian group and reported in the Canadian Medical Association Journal, October 1998. Highlights of those guidelines, with specific recommendations for children and adolescents, are as follows:
• Diabetes care should be organized around an interdisciplinary diabetes health care team
• Initial and ongoing education of the person with diabetes should be an integral part of diabetes management and not merely an adjunct to treatment.
• The metabolic goals and therapeutic strategies for adolescents over 12 years of age are the same as those for adults. The target HbA1c for prepubertal children is 120% to 140% of the upper limit of normal with targets for glucose and HbA1c graduated according to the child’s age. Extreme caution is required to avoid hypoglycemia in children under 5 years of age, because of the permanent cognitive deficit that may occur in this age group.
• All children with diabetes should have access to an experienced diabetes health care team. The complex physical, developmental and emotional needs of children and their families require specialized care to ensure the best long-term outcome
• In children and adolescents with new-onset diabetes, initial outpatient education and management should be considered if appropriate personnel and a 24-hour telephone consultation service are available in the community.
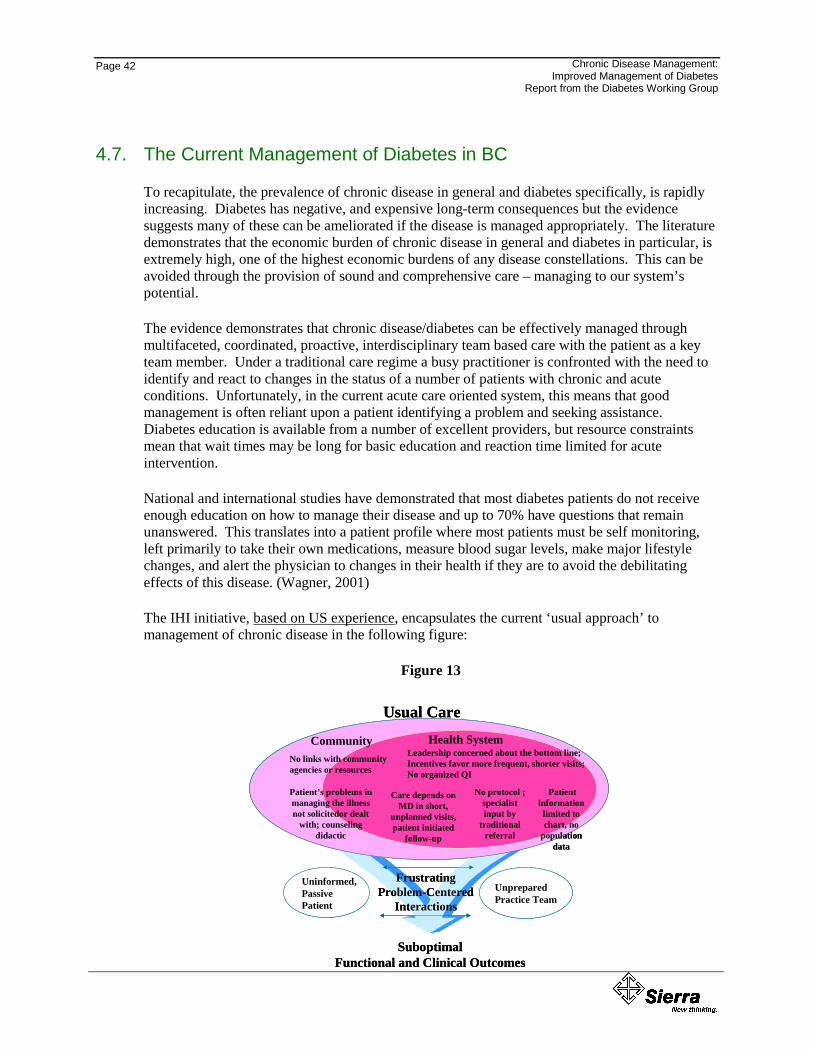
Page 42
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
4.7. The Current Management of Diabetes in BC
To recapitulate, the prevalence of chronic disease in general and diabetes specifically, is rapidly increasing. Diabetes has negative, and expensive long-term consequences but the evidence suggests many of these can be ameliorated if the disease is managed appropriately. The literature demonstrates that the economic burden of chronic disease in general and diabetes in particular, is extremely high, one of the highest economic burdens of any disease constellations. This can be avoided through the provision of sound and comprehensive care – managing to our system’s potential.
The evidence demonstrates that chronic disease/diabetes can be effectively managed through multifaceted, coordinated, proactive, interdisciplinary team based care with the patient as a key team member. Under a traditional care regime a busy practitioner is confronted with the need to identify and react to changes in the status of a number of patients with chronic and acute conditions. Unfortunately, in the current acute care oriented system, this means that good management is often reliant upon a patient identifying a problem and seeking assistance. Diabetes education is available from a number of excellent providers, but resource constraints mean that wait times may be long for basic education and reaction time limited for acute intervention.
National and international studies have demonstrated that most diabetes patients do not receive enough education on how to manage their disease and up to 70% have questions that remain unanswered. This translates into a patient profile where most patients must be self monitoring, left primarily to take their own medications, measure blood sugar levels, make major lifestyle changes, and alert the physician to changes in their health if they are to avoid the debilitating effects of this disease. (Wagner, 2001)
The IHI initiative, based on US experience, encapsulates the current ‘usual approach’ to management of chronic disease in the following figure:
Figure 13
Uninformed,PassivePatient
FrustratingProblem-Centered
InteractionsUnpreparedPractice Team
SuboptimalFunctional and Clinical Outcomes
Care depends on MD in short,
unplanned visits, patient initiated
follow-up
No protocol ; specialist input by
traditional referral
Patient information
limited to chart, no
population data
Patient’s problems in managing the illness not solicitedor dealt
with; counseling didactic
Health SystemNo links with communityagencies or resources
Community Leadership concerned about the bottom line;Incentives favor more frequent, shorter visits;No organized QI
Usual Care
Uninformed,PassivePatient
FrustratingProblem-Centered
InteractionsUnpreparedPractice Team
SuboptimalFunctional and Clinical Outcomes
Care depends on MD in short,
unplanned visits, patient initiated
follow-up
No protocol ; specialist input by
traditional referral
Patient information
limited to chart, no
population data
Patient’s problems in managing the illness not solicitedor dealt
with; counseling didactic
Health SystemNo links with communityagencies or resources
Community Leadership concerned about the bottom line;Incentives favor more frequent, shorter visits;No organized QI
Usual Care
Chronic Disease Management: Page 43 Improved Management of Diabetes Report from the Diabetes Working Group
Even though based on US experience, some aspects of the ‘current approach’ can also be extrapolated to the BC context. As the diagram denotes, usual care has been found to have many limitations for chronic disease management, including:
• Short, episodic visits;
• Focus on symptoms and diagnosis, not prevention;
• Limited attention to client and caregiver skills in caring for condition;
• Inadequate use of effective interventions and continued use of ineffective ones, and
• Treatment plans limited to presenting issue.
Chronic disease is one of the most significant challenges facing the health care system of tomorrow – the rise in prevalence in diabetes amongst many of our populations is going to reach near epidemic proportions in the near future. The evidence clearly demonstrates that chronic disease and diabetes cause a significant economic burden not only on society in general, but also on an already taxed health care system directly. The evidence also demonstrates that most of this can be avoided if chronic disease was managed appropriately – the question for BC is – how well are we managing? Are we minimizing the health and economic burden now and for the future?
4.7.1. A Benchmark for Comparison
The diagnosis and management of diabetes has been the subject of much examination. Clinical protocols for the diagnosis and management of people with diabetes have been developed and circulated widely. These protocols provide advice on how to care for diabetes patients by providing disease related education to the patients themselves, involving the patients in care planning, and involving an interdisciplinary team in care. In addition protocols exist for testing to assess control of blood glucose and to detect early complications.
In BC, the Guidelines and Protocols Advisory Committee developed Diabetes Care Guidelines in June 2002. See Appendix C - BC Diabetes Care Guidelines. These were subsequently approved by the BCMA and adopted by the Medical Services Commission. The objective of these guidelines is to assist primary care physicians meet the complex needs of persons with diabetes. They focus not on the treatment of diabetes, but on the approaches and systems that should be in place to improve the likelihood that appropriate, evidence-based care is provided.
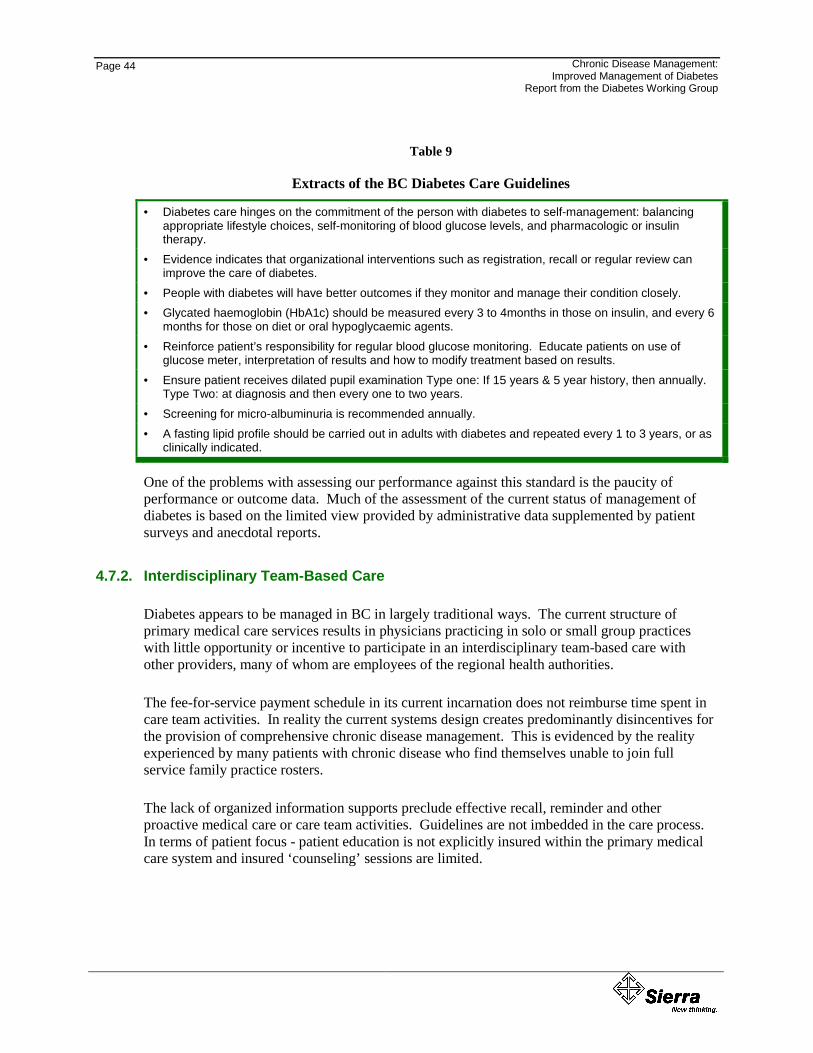
Page 44
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
Table 9
Extracts of the BC Diabetes Care Guidelines
• Diabetes care hinges on the commitment of the person with diabetes to self-management: balancing appropriate lifestyle choices, self-monitoring of blood glucose levels, and pharmacologic or insulin therapy.
• Evidence indicates that organizational interventions such as registration, recall or regular review can improve the care of diabetes.
• People with diabetes will have better outcomes if they monitor and manage their condition closely. • Glycated haemoglobin (HbA1c) should be measured every 3 to 4months in those on insulin, and every 6
months for those on diet or oral hypoglycaemic agents. • Reinforce patient’s responsibility for regular blood glucose monitoring. Educate patients on use of
glucose meter, interpretation of results and how to modify treatment based on results. • Ensure patient receives dilated pupil examination Type one: If 15 years & 5 year history, then annually.
Type Two: at diagnosis and then every one to two years. • Screening for micro-albuminuria is recommended annually. • A fasting lipid profile should be carried out in adults with diabetes and repeated every 1 to 3 years, or as
clinically indicated.
One of the problems with assessing our performance against this standard is the paucity of performance or outcome data. Much of the assessment of the current status of management of diabetes is based on the limited view provided by administrative data supplemented by patient surveys and anecdotal reports.
4.7.2. Interdisciplinary Team-Based Care
Diabetes appears to be managed in BC in largely traditional ways. The current structure of primary medical care services results in physicians practicing in solo or small group practices with little opportunity or incentive to participate in an interdisciplinary team-based care with other providers, many of whom are employees of the regional health authorities.
The fee-for-service payment schedule in its current incarnation does not reimburse time spent in care team activities. In reality the current systems design creates predominantly disincentives for the provision of comprehensive chronic disease management. This is evidenced by the reality experienced by many patients with chronic disease who find themselves unable to join full service family practice rosters.
The lack of organized information supports preclude effective recall, reminder and other proactive medical care or care team activities. Guidelines are not imbedded in the care process. In terms of patient focus - patient education is not explicitly insured within the primary medical care system and insured ‘counseling’ sessions are limited.
Chronic Disease Management: Page 45 Improved Management of Diabetes Report from the Diabetes Working Group
4.7.3. Initial and Ongoing Education and Support
“Diabetes is a 24 hour, every day of the year condition and people with diabetes need the knowledge, confidence and support to manage their own diabetes. People with diabetes should be able to access high quality information, treatment and care, particularly during the initial management. After diagnosis people with diabetes should be supported to stay healthy and so minimize the incidence of complications. All people with diabetes should be offered advice about reducing the risk of their long term complications and receive regular surveillance of risk factors. When risk factors are detected people with diabetes should be supported in controlling these risks and at an early stage offered effective treatment to retard the progression of complications” (Scottish Diabetes Framework, 2001)
The literature demonstrates that effective and comprehensive, life long self-management education and support is one of the keys to successful management of chronic disease/diabetes. Within BC, patient education is essentially limited to centres, frequently within acute care settings, held primarily during working hours, and based predominantly in the English language and western culture. Given the incidence of diabetes in the Aboriginal and ethnic populations this is certainly problematic. Waiting lists for this education are often lengthy.
In some health authorities in BC, there are attempts to offer ongoing education programs for people with diabetes. Although there are some interdisciplinary teams working with people with diabetes, organizational structure and resource limitations mean there is often minimal ongoing, proactive, organized follow-up.
Access to self-management program as described in the best practices and evidence-based literature is extremely limited.
4.7.4. Clinical Care
Unfortunately the only data available are resident in administrative data sets. As mentioned, the population of diabetes patients that the MOH linked data set at the Ministry of Health identified has some caveats and is probably a conservative estimate of the actual population of diabetes patients. However, MSP billing data for people previously diagnosed as suffering from diabetes give some indications on whether or not the CDA and BC Guideline recommendations are being met for the population of identified diabetes patients.
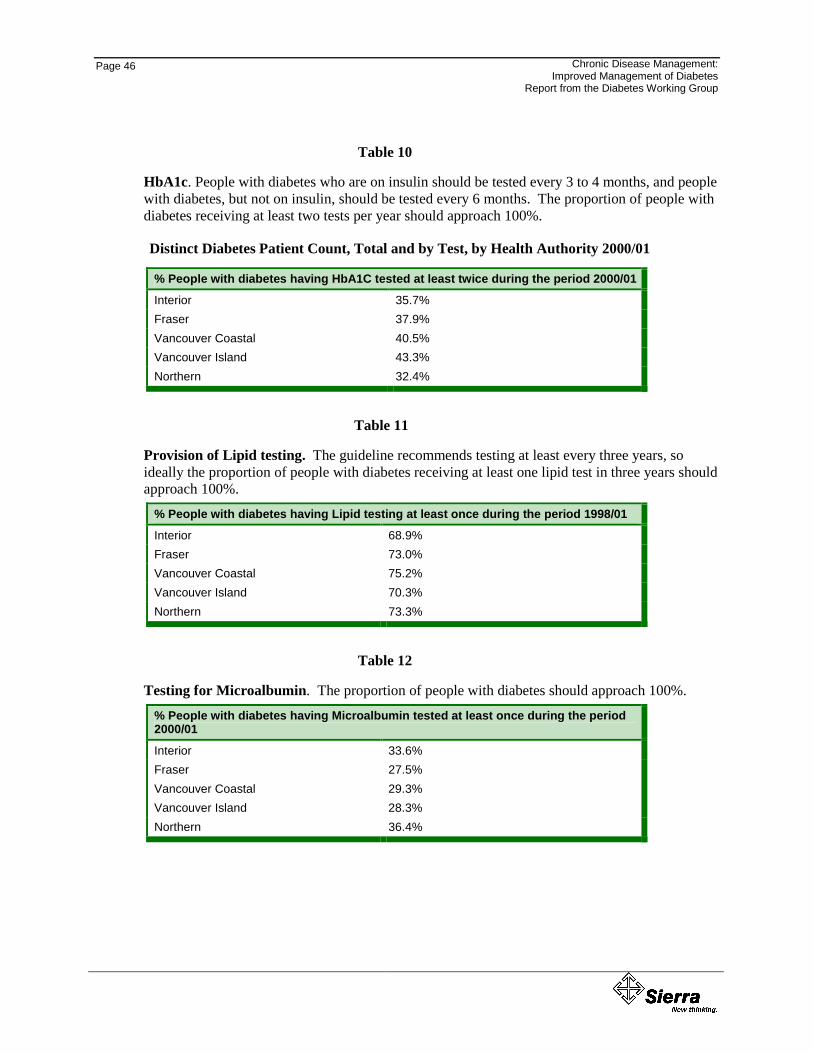
Page 46
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
Table 10
HbA1c. People with diabetes who are on insulin should be tested every 3 to 4 months, and people with diabetes, but not on insulin, should be tested every 6 months. The proportion of people with diabetes receiving at least two tests per year should approach 100%.
Distinct Diabetes Patient Count, Total and by Test, by Health Authority 2000/01
% People with diabetes having HbA1C tested at least twice during the period 2000/01
Interior 35.7% Fraser 37.9% Vancouver Coastal 40.5% Vancouver Island 43.3% Northern 32.4%
Table 11
Provision of Lipid testing. The guideline recommends testing at least every three years, so ideally the proportion of people with diabetes receiving at least one lipid test in three years should approach 100%.
% People with diabetes having Lipid testing at least once during the period 1998/01
Interior 68.9% Fraser 73.0% Vancouver Coastal 75.2% Vancouver Island 70.3% Northern 73.3%
Table 12
Testing for Microalbumin. The proportion of people with diabetes should approach 100%.
% People with diabetes having Microalbumin tested at least once during the period 2000/01
Interior 33.6% Fraser 27.5% Vancouver Coastal 29.3% Vancouver Island 28.3% Northern 36.4%
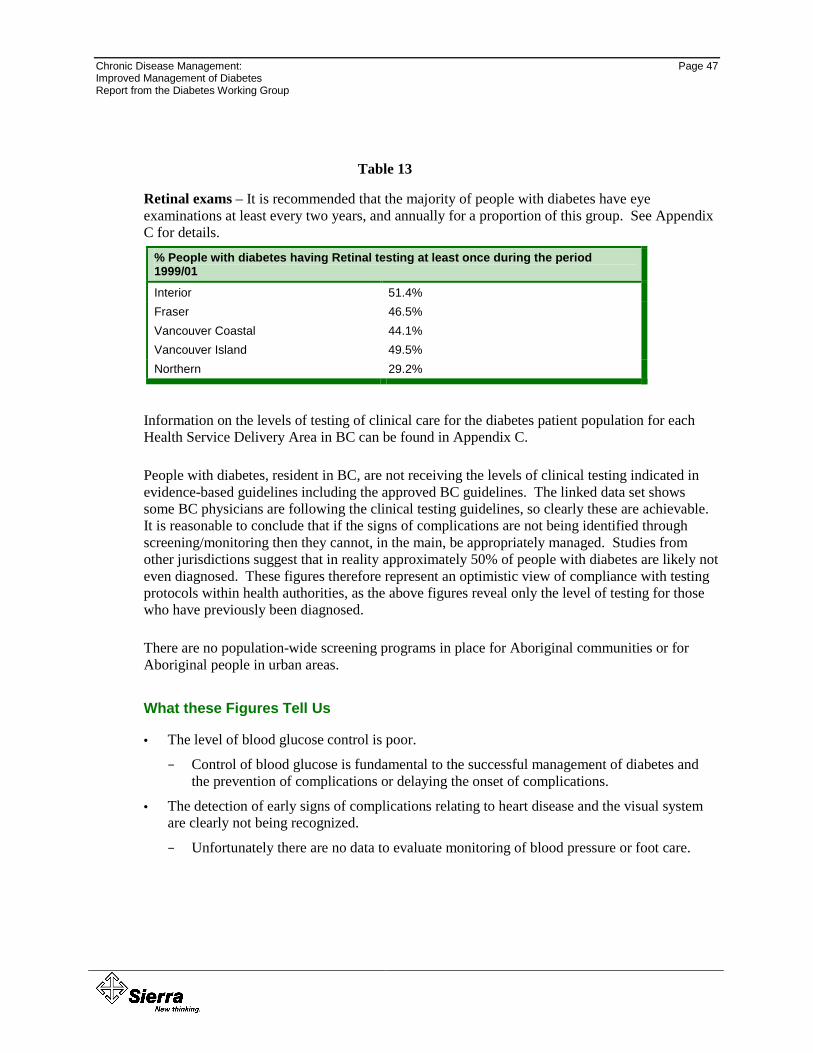
Chronic Disease Management: Page 47 Improved Management of Diabetes Report from the Diabetes Working Group
Table 13
Retinal exams – It is recommended that the majority of people with diabetes have eye examinations at least every two years, and annually for a proportion of this group. See Appendix C for details.
% People with diabetes having Retinal testing at least once during the period 1999/01
Interior 51.4% Fraser 46.5% Vancouver Coastal 44.1% Vancouver Island 49.5% Northern 29.2%
Information on the levels of testing of clinical care for the diabetes patient population for each Health Service Delivery Area in BC can be found in Appendix C.
People with diabetes, resident in BC, are not receiving the levels of clinical testing indicated in evidence-based guidelines including the approved BC guidelines. The linked data set shows some BC physicians are following the clinical testing guidelines, so clearly these are achievable. It is reasonable to conclude that if the signs of complications are not being identified through screening/monitoring then they cannot, in the main, be appropriately managed. Studies from other jurisdictions suggest that in reality approximately 50% of people with diabetes are likely not even diagnosed. These figures therefore represent an optimistic view of compliance with testing protocols within health authorities, as the above figures reveal only the level of testing for those who have previously been diagnosed.
There are no population-wide screening programs in place for Aboriginal communities or for Aboriginal people in urban areas.
What these Figures Tell Us
• The level of blood glucose control is poor.
− Control of blood glucose is fundamental to the successful management of diabetes and the prevention of complications or delaying the onset of complications.
• The detection of early signs of complications relating to heart disease and the visual system are clearly not being recognized.
− Unfortunately there are no data to evaluate monitoring of blood pressure or foot care.
Page 48
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
4.7.5. Depression Management
Up to one in five people with diabetes suffer from depressive disorders and the risk of clinical depression is even higher amongst those with co-morbidity and complications. Depression can have a damaging impact on effectiveness of self-management.
While there are no data to assess how depression is currently addressed within the diabetes patient population, depression generally is not effectively managed within the system. As there are no comprehensive programs to support individuals living with chronic disease, it is reasonable to assume that support for depression within this population is variable, and dependent upon the experience, expertise and time availability of the family physician. It is important to note that the current f-f-s schedule limits GP ‘counseling’ to four, 20 minute sessions per patient, per year.
In a recent patient survey, almost half the respondents were not checked for depression. When the number who did not know if they had been checked for depression were added, the number increased to 64% of respondents. (Richmond Survey Draft Document, 2002)
4.7.6. Patient Self-Report from Limited Trial Survey
A limited test-trial survey was undertaken in 2002 involving clients within the former Capital Health Region and Richmond Health Service Delivery Area. In the patient self-report from the Richmond survey of 115 respondents, respondents reported being tested once yearly for the following - 71% for HbA1c, 83% for blood pressure, 50% for blood cholesterol, 40% for microalbumin, 23% for feet, 32% for eyes and 2% for depression.
Similar results were found in the Capital Health Region survey. Overall, the surveys found that “good diabetes care is predicated on having open lines of communication between physicians and patients, and having an integrated “diabetes team” available to provide care and support”. (Richmond Survey, Draft Document, 2002) The respondents expressed a strong desire to manage their diabetes appropriately.
4.7.7. What Can Be Concluded?
In short, it appears the current system for diabetes management within British Columbia reflects the ‘usual care’ diagram presented in Section 5.6. Anecdotes from both Victoria and Vancouver further suggest that patients with chronic diseases, once diagnosed, have difficulty finding a full service primary care physician who will enroll them on their patient roster. Increasingly they are left to the vagaries of walk in care.
The figures indicate that appropriate clinical management of people with diabetes is not being achieved in British Columbia.
“every system is perfectly designed to achieve the results it achieves” (Berwick, 1998)
Chronic Disease Management: Page 49 Improved Management of Diabetes Report from the Diabetes Working Group
The consequences of failing to effectively manage diabetes will be significant. There must inevitably be many more cases of hypertension, stroke, heart disease, blindness, end stage renal failure, peripheral neuropathy and lower limb amputations, and premature death as the incidence and prevalence of diabetes increases. Many of these complications and premature deaths could be prevented by well-organized care.
The economic impact on the health care system will be compounded by the cost to society of the increased disability consequent upon this failure to manage a common, well understood condition.
In addition to the economic burden of not acting, there is an ethical issue raised by ignoring the human suffering generated by diabetes, its complications, and premature deaths. The ethical issue is particularly powerful in the current situation where the technology and knowledge is relatively inexpensive and easily available to solve a huge, and increasing, health care problem. In summary:
• Diabetes is rapidly becoming an epidemic and in fact already is amongst many of our population groups.
• There are inadequate data to identify the population.
• There are significant concerns that care is variable.
• There is poor coordination between providers and services across the region.
• There are an absence of systems to evaluate outcomes for individual clients/patients and the total population.
• Diabetes is not optimally managed in BC.
• Evidence from other jurisdictions clearly demonstrates that improvements can be made to the system of care.
• The economic consequences of doing nothing are staggering.
To do nothing is highly questionable from a social, population health, economic and ethical perspectives.
Chronic Disease Management: Page 51 Improved Management of Diabetes Report from the Diabetes Working Group
555... TTTHHHEEE PPPRRROOOPPPOOOSSSEEEDDD DDDIIIAAABBBEEETTTEEESSS IIINNNIIITTTIIIAAATTTIIIVVVEEE
The lack of a common performance improvement framework is not unique to diabetes and has been a barrier to quality improvement efforts in chronic disease generally. Poor performance and failure to adhere to evidence based guidelines are the inevitable result of the current system design. The challenge of diabetes must be met through identifying and addressing the underlying systemic issues in a multifaceted and coordinated manner.
‘all models are wrong, some are useful’ (W. Edwards Demming)
In this section a framework is presented for the provincial diabetes initiative. Key principles and attributes are described. A global program budget is developed based upon these core attributes. A framework, as opposed to detailed implementation plan, is presented as it is recognized that local needs and capacity will shape individual project details. All projects will, however, share a common set of principles and core attributes.
The cost side of the business case equation in Section 6 was developed using the CCM as a framework. The budget serves as a financial template and it is not intended that individual line items be prescriptive for community based projects. Provincial level budget items will remain constant but local costs may vary depending upon requirements and existing capacity.
5.1. An Evaluation of the Chronic Care Model
As described in Section 4, the CCM embraces the principles suggested by the Cochrane review of evidence. The CCM model is an organizational approach to caring for people with chronic disease in a primary care setting. The model is population-based, data driven and creates practical, supportive, evidence based interactions between an informed activated client and a prepared proactive practice team. It is significant that the World Health Organization recently adopted the CCM as the model for management of chronic diseases.
Supporting a ‘productive interaction’ between a patient and practice team is very difficult in traditional primary care and the research suggests that better outcomes, compliance and satisfaction will accrue from redesigning delivery systems to meet the needs of chronically ill patients. The CCM identifies the essential elements of a system that encourages high-quality chronic disease management. These cluster in: the community, the health system, self-management support, delivery system design, decision support, and clinical information systems
The BC Diabetes Initiative will be based on an ‘expanded’ chronic care model.
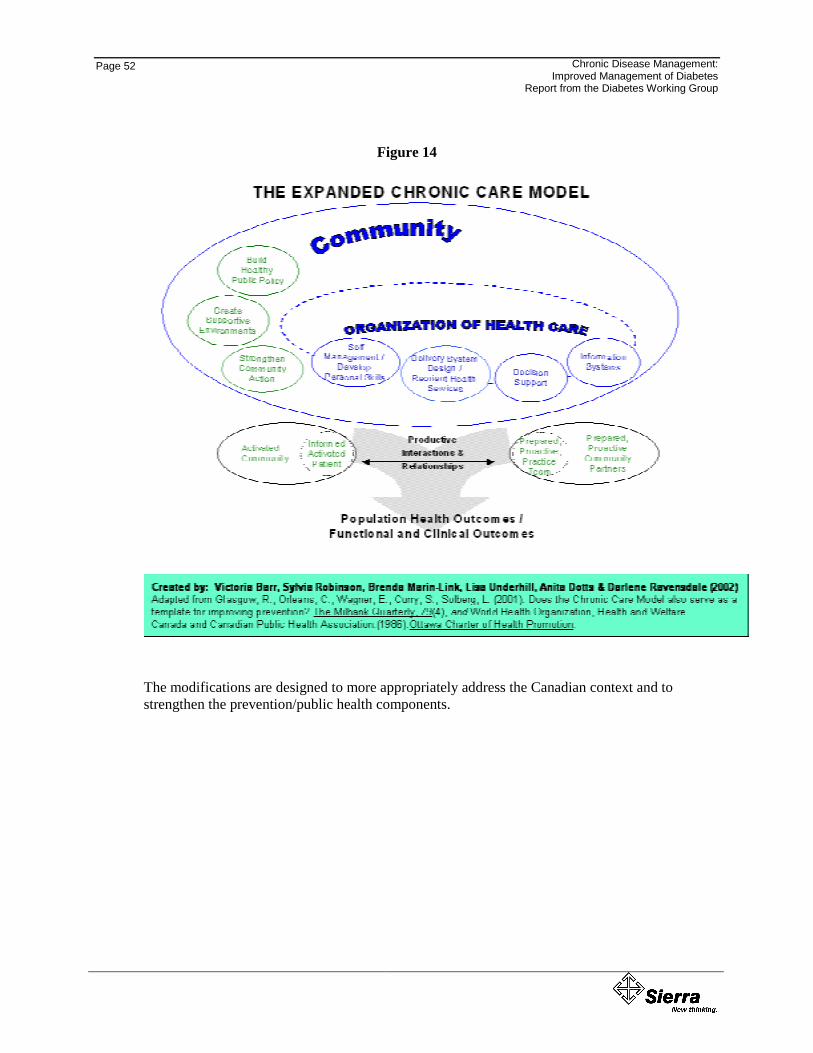
Page 52
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
Figure 14
The modifications are designed to more appropriately address the Canadian context and to strengthen the prevention/public health components.
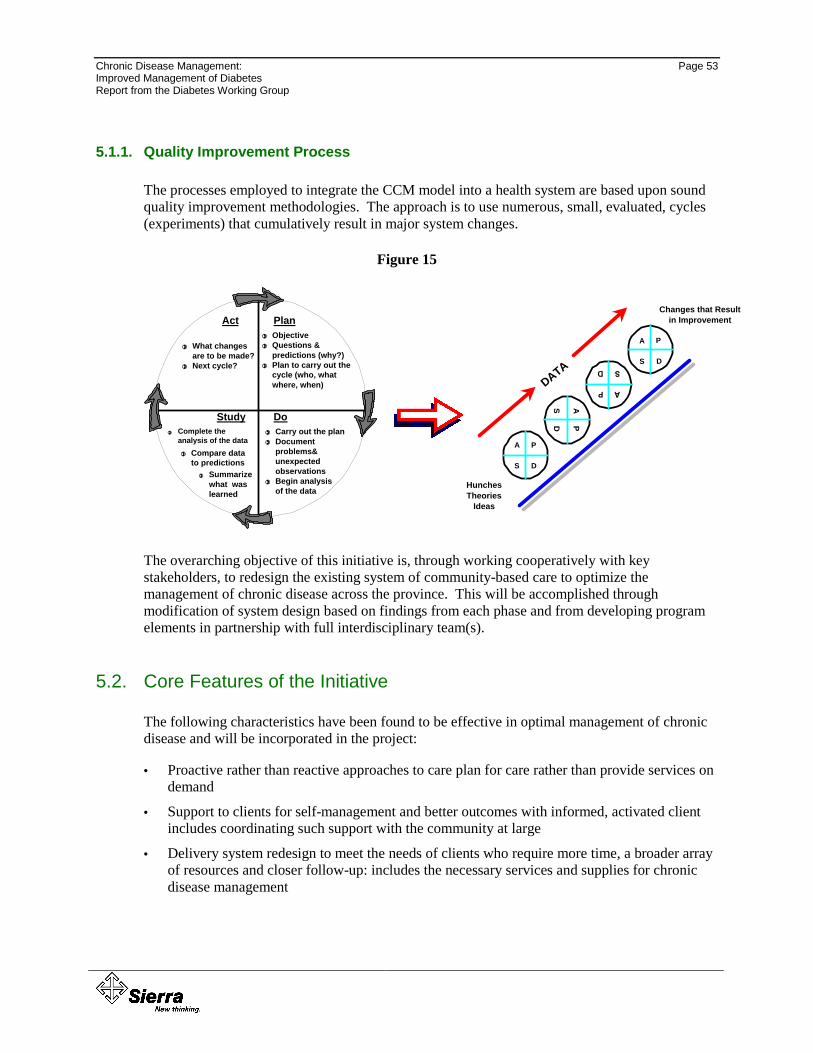
Chronic Disease Management: Page 53 Improved Management of Diabetes Report from the Diabetes Working Group
5.1.1. Quality Improvement Process
The processes employed to integrate the CCM model into a health system are based upon sound quality improvement methodologies. The approach is to use numerous, small, evaluated, cycles (experiments) that cumulatively result in major system changes.
Figure 15 PD
AS
P
D
A
S
P
D
A
S
HunchesTheories
Ideas
Changes that Result in Improvement
DATA
Act Plan
Study Do
ObjectiveQuestions & predictions (why?)Plan to carry out the cycle (who, what where, when)
!!!!
!!!!
!!!!
Carry out the planDocument problems& unexpected observationsBegin analysis of the data
!!!!
!!!!
!!!!
Complete the analysis of the data
!!!!
Compare data to predictions
!!!!
Summarize what was learned
!!!!
What changes are to be made?Next cycle?
!!!!
!!!!
The overarching objective of this initiative is, through working cooperatively with key stakeholders, to redesign the existing system of community-based care to optimize the management of chronic disease across the province. This will be accomplished through modification of system design based on findings from each phase and from developing program elements in partnership with full interdisciplinary team(s).
5.2. Core Features of the Initiative
The following characteristics have been found to be effective in optimal management of chronic disease and will be incorporated in the project:
• Proactive rather than reactive approaches to care plan for care rather than provide services on demand
• Support to clients for self-management and better outcomes with informed, activated client includes coordinating such support with the community at large
• Delivery system redesign to meet the needs of clients who require more time, a broader array of resources and closer follow-up: includes the necessary services and supplies for chronic disease management
Page 54
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
• Decision-support for a prepared, proactive interdisciplinary team including provider training and decision support through guidelines and other tools; includes access to specialist consultation
• Recognition and rewards for the behavioural change that is required of both clients and health care providers
• Information systems that support population-based care for outcome determination and provider reminders and feedback for proactive rather than reactive care
• High-level support by senior MOH and health authority executives
• Connecting patients and providers to community resources
For the purposes of Phase One, and in recognition of constrained resources, every effort will be made to build on work and resources already developed both within BC, and from other jurisdictions. Prior to implementation, all guidelines, best practice materials, flowsheets, decision support tools, etc. will receive approval from the appropriate provincial/regional care/clinical committees.
5.2.1. Patient Components – Effective Self Management Supports and Education
To build patient capacity in diabetes management and to facilitate patient self-management, the following elements are required.
Patient Surveys
Patient surveys are an effective way of incorporating patients’ perspectives into diabetes management. The BC survey consists of questions related to diagnosis, treatment, coping strategies, needs and challenges.
Patient Recall and Follow-up
Institute a patient recall system where the Provincial Diabetes Registry will be searched for patients who have not received follow-up care in the recommended period of time and generate alerts to notify these patients and/or their care teams immediately. The Diabetes Initiative would institute mechanisms for effective patient follow-up, such as group visits or home-based interventions, telephone follow-up and follow-up clinics.
Patient Education Resources
Effective patient education resources will help patients deal with their illness on a day-to-day basis and focus on the self-monitoring of symptoms. Patient education resources will take the form of:
• High quality printed materials;
Chronic Disease Management: Page 55 Improved Management of Diabetes Report from the Diabetes Working Group
• Interactive Internet or web-based instruction, and
• Telehealth initiatives.
Effective teaching on chronic disease must be grounded in theories of human behaviour and principles of learning and motivation. Patient self-management involves the conscious use of strategies to manipulate situations and thereby reduce the impact of disease on daily life. The patient learns what strategies work (or do not) through the process of experimentation. Patient education should not be a matter of simply providing information about the disease, but should allow patients to develop the capacity to observe themselves, make sensible judgments, feel confident, and strive for desirable outcomes.
Care Plans for Patients
An essential tool for patient self-management is the care plan, developed in partnership between the patient and health care provider team.
Care plans provide the following:
• Identify specific problems
• Establish realistic objectives
• Set targets (expected levels of change with time lines)
• Develop strategies to achieve objectives
• Address foreseeable obstacles and challenges
• Seek written commitment to see the plan through
Care plans need to be developed in the context of patient preferences and readiness, and need to flow from best practices for diabetes management (as embedded in clinical practice guidelines and standards of care).
Self-Efficacy Training
Some time-tested models of self-efficacy training exist and could be modified to local needs and circumstances. Typically, self-efficacy programs are run by people who themselves have a chronic condition. They cover topics such as the following:
• Pain control
• Use of medications
• Behaviour and lifestyle change
• Methods to adjust to social and workplace dislocations
• Strategies to cope with emotional reactions
• Methods to interpret changes in the disease and its consequences
Page 56
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
• Use of medical and community resources
Self-efficacy enables participants to learn from each other and has enabled participants to experience reduced symptoms, improved physical activity and significantly less need for medical treatment.
By encompassing a variety of theoretical and intellectual foundations, the Diabetes Initiative is interdisciplinary in nature and relevant to a variety of professions and disciplines.
5.2.2. Physicians and Health Care Provider Components – Effective, Prepared, Interdisciplinary Team
To build physician and health care provider capacity in diabetes management and to close the gap between current practice and best practice in the management of diabetes, the following components are required.
Shared Care
Identify and implement physician reimbursement and incentive mechanisms to encourage shared care between specialists and general practitioners. Services such as patient assessment and care planning, self-management training and support, and active follow-up must be adequately reimbursed if they are to become part of routine patient care.
Shared care initiatives will include:
• Telephone consultations where specialist salaries are compensated for time spent conducting telephone consultations with general practitioners in communities around the province, and
• Physician training such as diabetes management seminars, “train the trainer” initiatives and quarterly teleconference series.
These kinds of programs build capacity province-wide and encourage the consistent application of standards of care.
Community Networks
Encourage community-based agencies, community health care providers, and existing community networks to work toward improved diabetes management, including social supports, healthy public policies, and healthy lifestyle (risk reduction) programs. Encourage patient advocacy groups to continue to play their critical role in ensuring that all persons afflicted with diabetes have access to appropriate care. Establish a centralized Diabetes Resource Centre that will house relevant materials and resources for distribution to community groups and other interested parties.
Chronic Disease Management: Page 57 Improved Management of Diabetes Report from the Diabetes Working Group
5.2.3. Effective Decision Support - Population Level Components
In order to determine the scope and extent of diabetes in BC and to monitor, track and report on key indicators for diabetes, as well as evaluate the success of our interventions the following elements are required.
Diabetes Patient Registries (Provincial/Health Authorities)
Using data from the BC Medical Service Plan, as well as hospital and pharmaceutical data the Diabetes Patient Registries will track people with clinical evidence of diabetes, as well as people at high risk of diabetes. The health authority registries would be capable of identifying patients with modifiable risk factors for diabetes, including smoking, physical activity, blood pressure serum cholesterol and plasma glucose. A provincial Diabetes Registry would have the capability to be searched for patients who have not received follow-up care in the recommended period of time. Registry data will support outcome evaluation of the Diabetes Initiative.
Performance Measurement
Identify the key indicators to measure the performance of the Diabetes Initiative. Once baseline measures are obtained set targets for improvement in diabetes (e.g. reduce the hospitalization rate by an identified percentage.) Collect data over time to populate the indicators and produce an annual report using a report card format to facilitate easy reading and comparability of outcomes from one year to another.
5.2.4. Effective Decision Support – Provider and Patient Level
A care team requires supports to be effective and prepared. One key foundation is effective decision support.
Practice Guidelines Development and Use
Practice guidelines are an essential component of any chronic disease management strategy. They will include some combination of the following:
• Patient assessment
• Methods and indications for relevant clinical investigations
• Therapy, treatment and medication
• Indications for referral
• Local arrangements for referral to specialists and diabetes clinics
• Methods to involve patients
• Arrangements for patient education and family support
Page 58
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
• Arrangements for follow-up and review
A Canadian review showed that variables that affect the adoption of guidelines include: the quality of the guidelines; characteristics of the health professional; characteristics of the practice setting; and, incentives and regulations. This study also ranked the effectiveness of various adoption mechanisms. Lowest ranking went to traditional continuing medication education and mailings. Information targeted to specific providers and delivered by peers or opinion leaders ranked moderately effective. Reminder systems, academic detailing and multiple interventions are ranked most effective. (Lorig, 1999)
BC Diabetes Care practice guidelines were completed in June 2002. The guidelines were developed under the guidance of the Guidelines and Protocols Advisory Committee (GPAC), established by the Medical Services Commission to oversee and coordinate guideline development and implementation in BC. The practice guidelines approved by BCMA will be reviewed every two years or sooner, as new and relevant information becomes available. (Appendix C) This initiative will work closely with the MSC and GPAC to enhance physician adoption of these guidelines.
Standards of Care
Clinical practice guidelines will be translated into various evidence-based tools and templates to support practice decisions and include clinical pathways and management algorithms. Technology can be used to support physician assessment tools, care templates, algorithms, etc, and provide clinical cuing systems to increase conformance to standards of care. Standards of care will also be made available to patients as a way to increase their understanding of best practices in the management of their illness.
5.2.5. Clinical Information Supports
Clinical information supports are essential for appropriate, integrated and proactive management of diabetes. This will be a challenge in the current structure where the information on patients currently resides in paper-based charts in physician offices and diabetes centres. The Initiative will start simply and build upon its success. Initiatives will include:
• In partnership with key stakeholders, the Ministry will continue refining the capacity to track the overall population through de-identified administrative linked data sets;
• Development of a consent based project access database registry and process that includes clinically useful, integrated and timely information for the full care team;
• A system that provides reminders and feedback for providers and patients, that identifies subgroups for proactive care, and facilitates individual patient care planning;
• Coordination with the development both of a provincial diabetes registry as well as the regionally based community system and registry components, and
• The capacity to track performance over time through access to a provincial web based functionality.
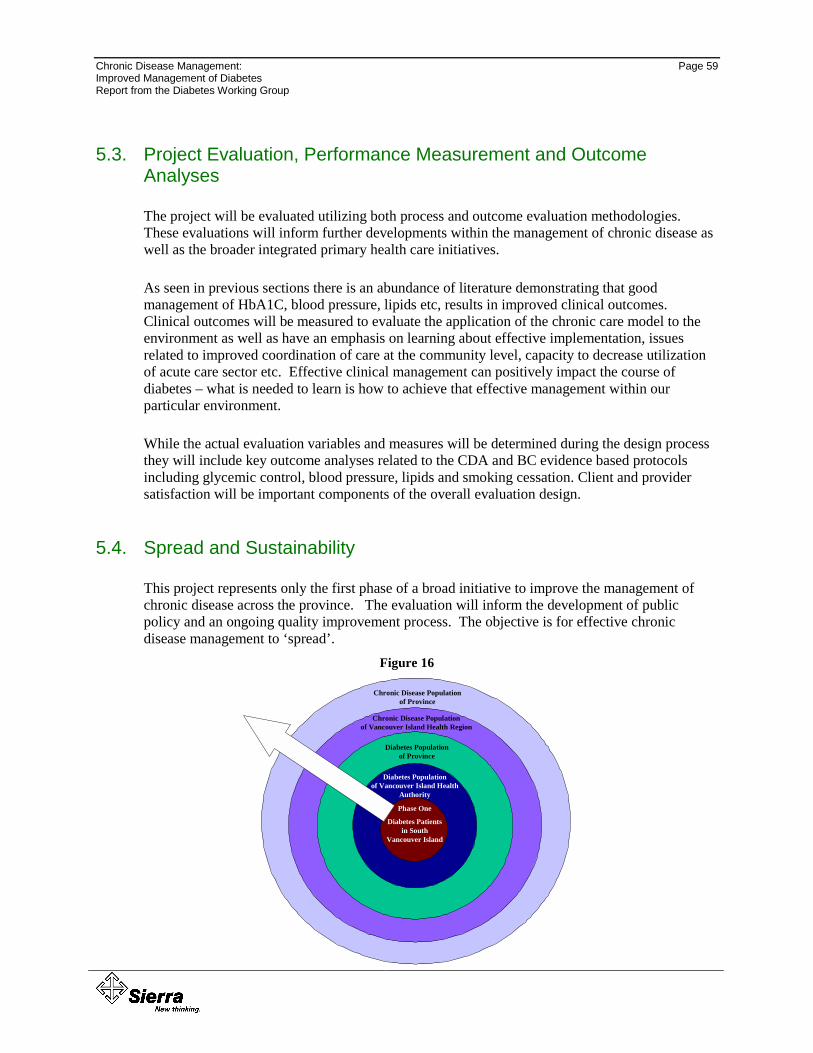
Chronic Disease Management: Page 59 Improved Management of Diabetes Report from the Diabetes Working Group
5.3. Project Evaluation, Performance Measurement and Outcome Analyses
The project will be evaluated utilizing both process and outcome evaluation methodologies. These evaluations will inform further developments within the management of chronic disease as well as the broader integrated primary health care initiatives.
As seen in previous sections there is an abundance of literature demonstrating that good management of HbA1C, blood pressure, lipids etc, results in improved clinical outcomes. Clinical outcomes will be measured to evaluate the application of the chronic care model to the environment as well as have an emphasis on learning about effective implementation, issues related to improved coordination of care at the community level, capacity to decrease utilization of acute care sector etc. Effective clinical management can positively impact the course of diabetes – what is needed to learn is how to achieve that effective management within our particular environment.
While the actual evaluation variables and measures will be determined during the design process they will include key outcome analyses related to the CDA and BC evidence based protocols including glycemic control, blood pressure, lipids and smoking cessation. Client and provider satisfaction will be important components of the overall evaluation design.
5.4. Spread and Sustainability
This project represents only the first phase of a broad initiative to improve the management of chronic disease across the province. The evaluation will inform the development of public policy and an ongoing quality improvement process. The objective is for effective chronic disease management to ‘spread’.
Figure 16
Diabetes Population of Province
Diabetes Population of Vancouver Island Health
Authority
Phase One
Diabetes Patients in South
Vancouver Island
Chronic Disease Population of Province
Chronic Disease Population of Vancouver Island Health Region
Page 60
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
Spread in the context of this project can be defined as the formal development of a process to encourage other people, health services, physicians to adopt the changes that are promoted both for the management of diabetes across the region as well as all chronic disease. A range of strategies will be developed to ensure spread, including:
• Public Policy
• Presentations
• Partnerships
• Newsletters, insertions in relevant newsletters
• Communication and marketing strategies
• Reports at conferences
• Presentations to other physicians and provider groups
• CME, presentations at rounds
Chronic Disease Management: Page 61 Improved Management of Diabetes Report from the Diabetes Working Group
666... TTTHHHEEE BBBUUUSSSIIINNNEEESSSSSS CCCAAASSSEEE
6.1. The Challenges of a Business Case in Health Care
The business case analysis has four components:
• A description of the proposed investment;
• A financial analysis of the proposed investment;
• A risk analysis of the proposed investment; and
• A feasibility analysis of what should be done next.
This plan begins the process of developing a valid business case for system change designed to improve the management of chronic disease generally, and diabetes specifically, within BC. It is timely and appropriate that this form of cost justification become a normal course of practice within the Canadian health care industry.
The complexity of healthcare makes the development of valid cost/benefit analyses at best, challenging. Prior to developing the economic rationale it is important to note some of these challenges and caveats, and to be clear on the assumptions upon which many of our estimates and projections are made.
As Wagner (2001) has said, there are some logical assumptions one can make as to how improved systems of chronic illness care reduce costs, including through:
• reducing symptoms;
• increasing function;
• reducing exacerbations;
• increasing patient ability to manage their condition and make sound decisions, and
• reducing unnecessary utilization associated with unplanned care.
But, in answer to the question – does better chronic illness care improve the financial situation of the system? – the answer is, it depends, on such things as the system perspective, the reimbursement model under which the physicians operate and the chronic condition of concern e.g., depression vs. diabetes.
6.1.1. Time Horizon and Complexity
One of the challenges faced when undertaking a cost/benefit analysis of interventions within the area of chronic disease is that any return on investment cannot be immediately measured. If the complications of diabetes are successfully avoided, evidence will accumulate over a time span of
Page 62
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
over two years. Benefits are measured in outcomes achieved through dollars spent on care for persons with chronic conditions as their condition evolves over years, not days, and across multiple care settings. It is also measured in improved quality of life, higher levels of consumer satisfaction, improved productivity, and decreased or delayed disability.
Cost savings, or more accurately cost avoidance, may not accrue within the funding envelope that makes the initial investment. For example within the BC system investment in diabetes will occur in primary and community care, in more time spent by the primary health care team, potentially in drug management and in patient education and support, yet the cost benefit accrues years later in avoidance of dialysis, surgery and admissions to acute and long term care.
6.1.2. The Question of Audience
Quality improvements in health care have different, intersecting and often competing financial implications for the parties involved. These can vary greatly depending upon the overall funding envelope and organizational structure. For example, there are differing incentives for level of treatment between the payment modalities of f-f-s and capitation/prepaid modalities.
Within BC the traditional ‘swings and round about’ assumption underlying the current G.P. payment schedule is becoming rapidly less sustainable as the rosters of full service family physicians contain increasingly higher proportions of chronic and complex patients. Providing good diabetes patient care is not as economically rewarding in f-f-s primary medical care as is the provision of light, episodic, walk in patient traffic. This is evidenced in the growing crisis in chronic care where many patients with these conditions cannot join a ‘traditional’ family practice.
Many of the fundamental tenets of good chronic disease management, such as support for patient self-management, use of alternate providers, group visits, team conferences, patient recall, telephone support etc., are either not insured, or from the physician perspective, not economically viable. Indeed, at present there are few provider rewards that connect monetary reward to quality. It would be difficult, if not impossible, to create a business argument for exceptional chronic disease management for an audience of f-f-s family physicians.
“It will take an investment in community-based services, in community health, family practice, information systems, patient education, appropriate drug regimes, and health promotion and prevention to improve chronic care. The economic benefits will accrue in acute and long-term care. As you will see from the evidence referenced in the following sections chronic care has made a business case in entities with ‘industrial strength’ – those integrated systems of care where financial, market and clinical incentives - mostly to be found in the US health insurance industry - align.” (Vladeck, 2001)
This discussion is addressed to the leadership of the Medical Services Commission, MOH and Health Authorities specifically, and the overall funded health system more generally. It does not attempt to make an isolated cost benefit argument for individual physicians, for the Pharmacare program, or other separate funding envelopes. It also assumes that both the regional and
Chronic Disease Management: Page 63 Improved Management of Diabetes Report from the Diabetes Working Group
provincial levels of health governance will be influenced by broader economic arguments relating to increased productivity and tax dollars and decreased disability/sick time.
6.1.3. Sustainability and Spread
The cost/benefit ratio of chronic care is completely dependent upon the range of population that is eventually positively impacted and the degree/size of negative consequences avoided. If this project will only improve the care of the patients it initially addresses in Phase One then there is not a good economic rationale for proceeding. If, however, it supports the spread of appropriate care so that all individuals with chronic disease receive optimal care then the argument becomes compelling and the project must proceed.
Much of what will be trialed and instituted in this project are common systems changes that, as application is expanded, will improve process and outcomes across all chronic conditions (e.g. self management programs, group visits, elements of case management etc.) While the business rationale is limited to diabetes, in reality the proposal needs to be considered within the broader perspective of all chronic disease, across the full provincial population, both now and over the near term as prevalence rates exponentially increase.
A search of the literature failed to provide many details of cost savings from programs representing excellent management. The reason for this is that good chronic disease management programs are not common in the world, and are almost unknown in Canada. Tight control of the diabetes patient state will not reduce the costs of managing the population with diabetes to an equivalence of the cost of providing health care to the population without diabetes, but it will ameliorate the costs and the burden of illness and disability. It is safe to assume that failure to utilize the current concepts of evidence based management of diabetes will result in an ever increasing burden on the acute and long term care resources of BC.
6.1.4. Extrapolation of Findings from Other Jurisdictions
The lack of studies within the Canadian context means that this business case must rely on research from other jurisdictions. While limiting the research to the UK and US settings, and attempting to project only from those studies believed to be valid and as close to mirroring the BC context as possible, it is true that these assumptions can be challenged and may bring bias to the financial analyses. At this time, the basis of the analyses is believed to be on the most appropriate research findings available: the reader must remain aware of the potential bias resulting from these assumptions.
6.2. Outcome Objectives for Implementation of Optimal Diabetes Management in BC
If the experience from other jurisdictions (UKPD, 1998) and assuming a total diabetes patient population of 175,000 for BC is assumed, the following long term outcome objectives could be
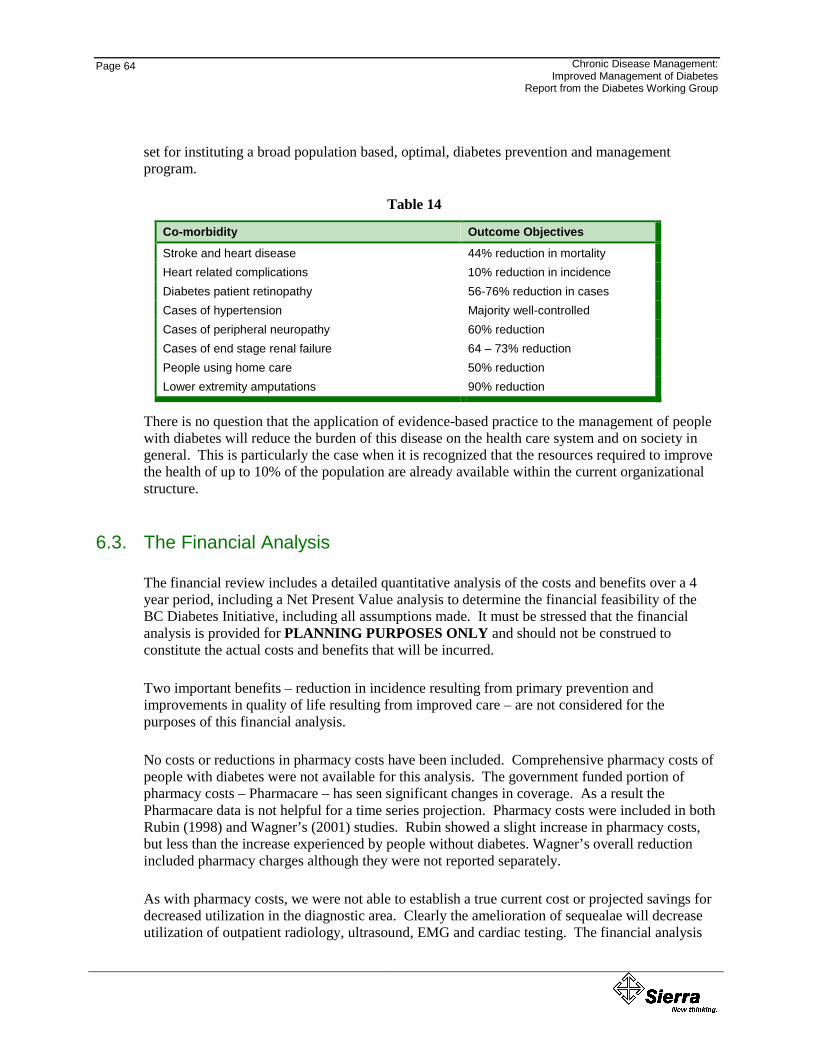
Page 64
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
set for instituting a broad population based, optimal, diabetes prevention and management program.
Table 14
Co-morbidity Outcome Objectives
Stroke and heart disease 44% reduction in mortality Heart related complications 10% reduction in incidence Diabetes patient retinopathy 56-76% reduction in cases Cases of hypertension Majority well-controlled Cases of peripheral neuropathy 60% reduction Cases of end stage renal failure 64 – 73% reduction People using home care 50% reduction Lower extremity amputations 90% reduction
There is no question that the application of evidence-based practice to the management of people with diabetes will reduce the burden of this disease on the health care system and on society in general. This is particularly the case when it is recognized that the resources required to improve the health of up to 10% of the population are already available within the current organizational structure.
6.3. The Financial Analysis
The financial review includes a detailed quantitative analysis of the costs and benefits over a 4 year period, including a Net Present Value analysis to determine the financial feasibility of the BC Diabetes Initiative, including all assumptions made. It must be stressed that the financial analysis is provided for PLANNING PURPOSES ONLY and should not be construed to constitute the actual costs and benefits that will be incurred.
Two important benefits – reduction in incidence resulting from primary prevention and improvements in quality of life resulting from improved care – are not considered for the purposes of this financial analysis.
No costs or reductions in pharmacy costs have been included. Comprehensive pharmacy costs of people with diabetes were not available for this analysis. The government funded portion of pharmacy costs – Pharmacare – has seen significant changes in coverage. As a result the Pharmacare data is not helpful for a time series projection. Pharmacy costs were included in both Rubin (1998) and Wagner’s (2001) studies. Rubin showed a slight increase in pharmacy costs, but less than the increase experienced by people without diabetes. Wagner’s overall reduction included pharmacy charges although they were not reported separately.
As with pharmacy costs, we were not able to establish a true current cost or projected savings for decreased utilization in the diagnostic area. Clearly the amelioration of sequealae will decrease utilization of outpatient radiology, ultrasound, EMG and cardiac testing. The financial analysis
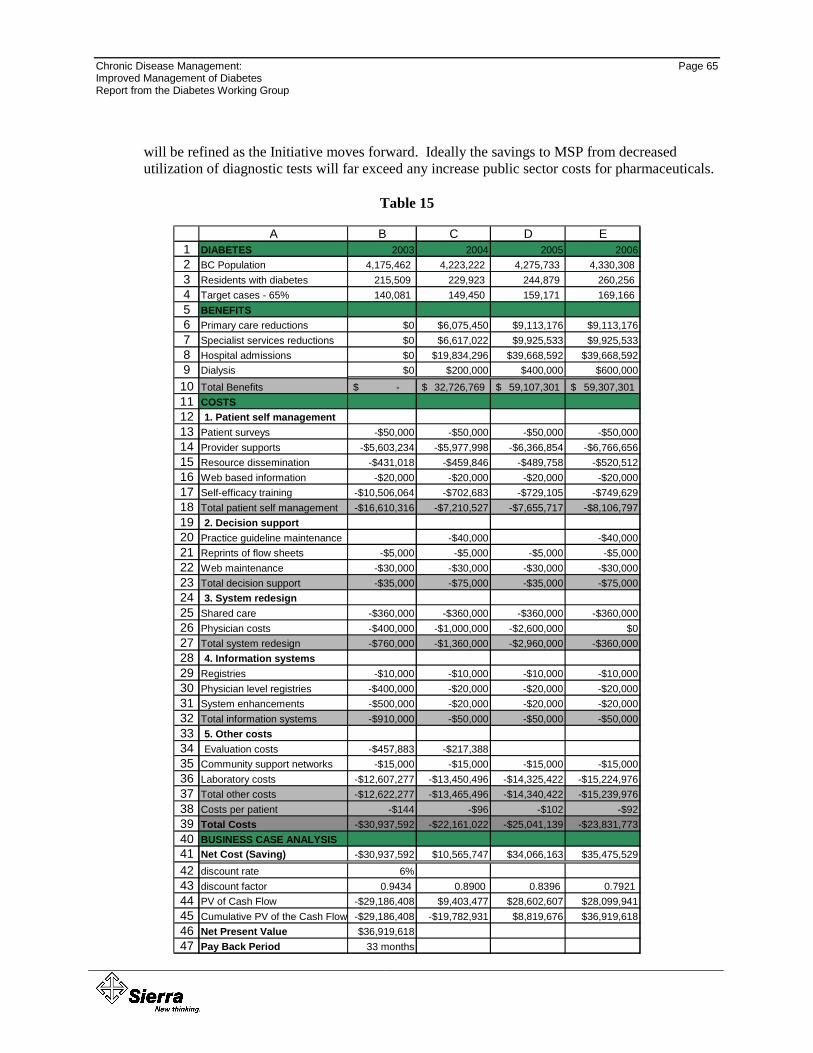
Chronic Disease Management: Page 65 Improved Management of Diabetes Report from the Diabetes Working Group
will be refined as the Initiative moves forward. Ideally the savings to MSP from decreased utilization of diagnostic tests will far exceed any increase public sector costs for pharmaceuticals.
Table 15
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647
A B C D EDIABETES 2003 2004 2005 2006BC Population 4,175,462 4,223,222 4,275,733 4,330,308 Residents with diabetes 215,509 229,923 244,879 260,256 Target cases - 65% 140,081 149,450 159,171 169,166 BENEFITSPrimary care reductions $0 $6,075,450 $9,113,176 $9,113,176Specialist services reductions $0 $6,617,022 $9,925,533 $9,925,533Hospital admissions $0 $19,834,296 $39,668,592 $39,668,592Dialysis $0 $200,000 $400,000 $600,000Total Benefits -$ 32,726,769$ 59,107,301$ 59,307,301$ COSTS 1. Patient self management
Patient surveys -$50,000 -$50,000 -$50,000 -$50,000Provider supports -$5,603,234 -$5,977,998 -$6,366,854 -$6,766,656Resource dissemination -$431,018 -$459,846 -$489,758 -$520,512Web based information -$20,000 -$20,000 -$20,000 -$20,000Self-efficacy training -$10,506,064 -$702,683 -$729,105 -$749,629Total patient self management -$16,610,316 -$7,210,527 -$7,655,717 -$8,106,7972. Decision support
Practice guideline maintenance -$40,000 -$40,000Reprints of flow sheets -$5,000 -$5,000 -$5,000 -$5,000Web maintenance -$30,000 -$30,000 -$30,000 -$30,000Total decision support -$35,000 -$75,000 -$35,000 -$75,0003. System redesign
Shared care -$360,000 -$360,000 -$360,000 -$360,000Physician costs -$400,000 -$1,000,000 -$2,600,000 $0Total system redesign -$760,000 -$1,360,000 -$2,960,000 -$360,0004. Information systems
Registries -$10,000 -$10,000 -$10,000 -$10,000Physician level registries -$400,000 -$20,000 -$20,000 -$20,000System enhancements -$500,000 -$20,000 -$20,000 -$20,000Total information systems -$910,000 -$50,000 -$50,000 -$50,0005. Other costsEvaluation costs -$457,883 -$217,388
Community support networks -$15,000 -$15,000 -$15,000 -$15,000Laboratory costs -$12,607,277 -$13,450,496 -$14,325,422 -$15,224,976Total other costs -$12,622,277 -$13,465,496 -$14,340,422 -$15,239,976Costs per patient -$144 -$96 -$102 -$92Total Costs -$30,937,592 -$22,161,022 -$25,041,139 -$23,831,773BUSINESS CASE ANALYSISNet Cost (Saving) -$30,937,592 $10,565,747 $34,066,163 $35,475,529discount rate 6%discount factor 0.9434 0.8900 0.8396 0.7921PV of Cash Flow -$29,186,408 $9,403,477 $28,602,607 $28,099,941Cumulative PV of the Cash Flow -$29,186,408 -$19,782,931 $8,819,676 $36,919,618Net Present Value $36,919,618Pay Back Period 33 months
Page 66
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
6.3.1. Assumptions
Line 1: Timeframe – the financial analysis was conducted over a 4 year period assuming a start date of 2003.
Line 2: BC Population – total population estimates for 2003 –2006 from BC Stats.
Line 3: BC Population with Diabetes – the estimated number of our population with diabetes – projected prevalence based on observed prevalence in 2000/01 of 4.3% growing to a prevalence of 6.29% in 2007/08. The projections take into account aging of the population.
Line 4: BC Diabetes Management Target Cases – the estimated number of British Columbians with diabetes who we estimate are receiving less than optimal care – assumption based on amalgamation of research from other jurisdictions and the findings from the BC administrative data set. The estimate of the target group is 65% of all those people with diabetes.
Line 5: Benefits – the anticipated financial benefits derived from implementing the Diabetes Management Initiative.
Line 6: Primary Care Reductions – the benefit associated with a 0% change in year 1, 10% decrease in year 2, and 15% reduction in subsequent years for primary care services that can be anticipated from a diabetes management program. In 2000/01 for BC, the total cost of MSP fee-for-service primary care for Diabetes was $54,635,345. A compensation increase of 11.2% occurred in 2002. Reductions have been calculated based on the 2000/01 expenditure inflated to 2002 fee levels. Wagner’s (2001) work showed an overall reduction in costs of about 16% ($685 to $950 on a base of $5,000) attributable mainly to primary care and specialty services. Wagner’s actual savings in this area were much higher as he found little change in hospital costs. Estimated reductions accrue from reduced visits from averted complications.
Line 7: Specialist Services Reductions– the benefit associated with a 0% in year 1, 10% decrease in year 2, and 15% reduction in subsequent years. In 2000/01 for BC, the total cost of MSP fee-for-service specialist services (excluding diagnostics and laboratory) for people with diabetes was $59,505,595. A compensation increase of 11.2% occurred in 2002. Reductions have been calculated based on the 2000/01 expenditure inflated to 2002 fee levels. Estimated reductions accrue from reduced visits from averted complications.
Line 8: Hospital Admission Reductions – the benefit associated with a 0% change in year 1, 5% decrease in year 2, and 10% decrease in subsequent years anticipated from a diabetes management program. In 2000/01 for BC, the total cost of hospitalization for diabetes was $396,985,924, or an average of $2,247 per person. About 30% of all people with diabetes had at least one hospital admission during the year. Rubin (1998) showed a reduction in hospital costs of 26% (and very little saving in primary or specialist care) while Wagner (2001) showed little saving in hospital costs (but an overall reduction of 16%). Estimates of hospital cost reductions result in overall costs reductions that are less than either Rubin or Wagner but which are apportioned more evenly across the domains.
Line 9: Reduction in Utilization of Dialysis – the benefit associated with a 0% reduction in year 1, a reduction of 5 patients in year 2, 10 patients in year 3 and 15 patients in year 4. Renal dialysis is estimated to cost $40,000 per person per year.
Line 10: Total Benefits – the sum of the benefits derived from reductions in physician services, hospital admissions and dialysis
Chronic Disease Management: Page 67 Improved Management of Diabetes Report from the Diabetes Working Group
Line 11: Costs – the anticipated financial costs associated with implementing the Diabetes Management Initiative on a provincial basis.
Line 13: Patient Surveys –cost of a part time FTE, development costs with disease organizations (focus group testing), postage and telephone support.
Line 14: Provider supports – additional costs to support interdisciplinary team care. Estimate based on a cost of $40 per individual for each of the target population.
Line 15: Resource dissemination – estimated at $2 per person for all people with diabetes.
Line 16: Web based information – costs of researching, writing, vetting and updating the original materials.
Line 17: Self-efficacy training – estimated at $75 per person in the target group in year 1, and $75 per additional person in the target group in subsequent years.
Line 18: Total – Patient Self Management Costs
Line 20: Practice guidelines – the BC guidelines have been produced and distributed. Estimated costs of periodic review and update are shown.
Line 21: Reprints – estimated costs of printing and mailing out decision support documents such as the patient flow sheet.
Line 22: Web maintenance – estimated costs of maintaining the chronic disease management web site element relevant to diabetes care. (estimate provided by the Ministry of Health Services)
Line 23: Total – Decision Support
Line 25: Shared Care – estimated cost of establishing appropriate processes and mechanisms for enhancing specialist/GP support in the management of diabetes. Costs based on $6,000 per month X 5 regions
Line 26: Transitional Physician Costs – transitional costs of redesigning the system to an integrated chronic care model from the provider perspective. Items could include physician training and support, assistance with office redesign, meeting costs etc. Recognizing that the responsibility for funding the provision of medical services falls under the mandate of the Medical Services Commission (MSC) this line is purposefully vague. It is assumed that the costs for this item could accrue to the MSC either through the $10 million available for primary care renewal or from health transition monies. These strategies will be developed with physicians and their associations. The amount is based on $1,000 per 4,000 physicians spread over three years. We will work closely with the GP Services Committee and allocations from the $10 million fund may be available for this purpose.
Line 27: Total – System Redesign
Lines 29: Registries – Ministry of Health estimate of the cost of maintaining the provincial diabetes registry.
Line 30: Physician level registries – Ministry of Health estimate of the costs of making available to physicians, through secure web based access, the element of provincial registry applicable to individual physicians.
Page 68
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
Line 31: System enhancements – Ministry of Health estimate of the costs of system enhancements to make available to patients, through secure web access, their individual information such as date of last HbA1c.
Line 32: Total – Information Systems
Line 34: Evaluation – estimated costs of supporting evaluation of quality improvement cycles is 5% in the first two years (3% Year One, and 2% Year 2)
Line 35: Community support networks – $15,000 per year to support meeting and related costs
Line 36: Laboratory costs – adherence to the new diabetes guideline is anticipated to increase laboratory costs by about $100 per year for target cases.
Line 37: Total - Other Costs
Line 38: Cost per Diabetes Patient – the total costs divided by the number of BC residents with diabetes.
Line 39: Total Costs
Line 40: Business Case Analysis – the Net Present Value Analysis to determine if the business case exists for the Diabetes Initiative.
Line 41: Net Cost of Saving – the net (cost) or saving is determined by subtracting the total costs from the total benefits.
Line 42: Discount Rate – the discount rate is assumed to be 6% - the interest rate of a competing investment.
Line 43: Discount Factor – the discount factor is 1/(1+r)n where r is the discount rate and n is the period in years.
Line 44: The Present Value of the Cast Flow – is the discount rate multiplied by the net (cost)/saving for each period.
Line 45: The Cumulative Present Value of the Cash Flow – is the total sum of cash flow present values from period 1 to period 5 (i.e. 2002 – 2006)
Line 46: The Net Present Value – the value of the investment expressed in current dollars.
Line 47: The Payback Period – is the time required for the cumulative present value of the cash flow to yield a positive value – the period of time it takes for the accrued benefits to offset the costs.
Note – Pharmaceutical Costs/Diagnostic Savings Pharmacy Costs – No costs or reductions in pharmacy costs have been included. Comprehensive pharmacy costs of people with diabetes were not available for this analysis. The government funded portion of pharmacy costs – Pharmacare – has seen significant changes in coverage. As a result the Pharmacare data is not helpful for a time series projection. Pharmacy costs were included in both Rubin (1998) and Wagner’s (2001) studies. Rubin showed a slight increase in pharmacy costs, but less than the increase experienced by people without diabetes. Wagner’s overall reduction included pharmacy charges although they were not reported separately.
Diagnostic Savings – As with pharmacy costs, we were not able to establish a true current cost or projected savings for decreased utilization in the diagnostic area. Clearly the amelioration of
Chronic Disease Management: Page 69 Improved Management of Diabetes Report from the Diabetes Working Group
sequealae will decrease utilization of outpatient radiology, ultrasound, EMG and cardiac testing. The financial analysis will be refined as the Diabetes Initiative moves forward. Ideally the savings to MSP from decreased utilization of diagnostic tests will far exceed any increase public sector costs for pharmaceuticals.
The financial analysis as outlined demonstrates a payback within 33 months. This is a short payback period and strongly suggests that the Diabetes Initiative based on the assumptions outlined is worthy of investment.
This analysis is based on costs and benefits that are derived from a Diabetes Initiative that has the following characteristics:
• The Initiative is directed at all BC residents with diabetes although certain elements will be directed towards the target cases.
• The benefits indicated are based on the studies of Wagner (2001) and Rubin (1998)
• The Diabetes Initiative would have population, provider and patient levels of action
A Diabetes Management Collaborative consisting of key stakeholders would be put in place to evaluate the Initiative and provide advice back to the key stakeholder groups.
6.4. Risk Analysis
The identification of the types and magnitude of risks associated with implementing the Diabetes Initiative in British Columbia include the following:
Table 16
Type of Risk Level of Risk
Scope Risk High Service Delivery Model Risk High Benefits Risk High Implementation Model Risk Medium Cost Risk Medium Quality of Care Risk Low Professional Practice Risk Low Management and Operation Risk Low Technology Risk Low
For the high and medium risk items the following analysis applies and must be taken into consideration when considering what implementation options are feasible for the Diabetes Initiative in British Columbia.
Page 70
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
6.4.1. Scope Risk: High
• Some success has been achieved in the United States using new chronic disease management models, directed at diabetes. These implementations have had a tightly managed scope – for example, at the Group Health Cooperative of Puget Sound (Seattle Washington) where the chronic disease management approach has been used, there are proven paybacks. The chronic disease management approach has yet to be used in Canada and is not being proposed “as is” for implementation in British Columbia. The Chronic Care Model that is proposed has yet to be tested and proven for diabetes.
• The risk in the Canadian setting is to want to expand the scope “to be all things to all people” –disease management, self care, health promotion and prevention, health information line, providers network and so on. This tendency is caused by the Canadian health care setting being broader in scope and less confined by a controlled (i.e., insurance/HMO) service delivery model than the US.
• This risk can be reduced if the initial scope of the Diabetes Initiative is confined to what has been successful in other jurisdictions and project management methodologies are incorporated in the implementation.
6.4.2. Service Delivery Model Risk: High
• Chronic Disease Management in the US and the NHS has been associated with the development and evolution of managed care organizations. It has been very successfully implemented within that service delivery model.
• There has not been the same level of implementation and success with the chronic disease management model in Canada – especially as it relates to diabetes.
• Successful implementation in other jurisdictions occurred within ‘single organizations’ that is all core elements of initiative are governed or funded by one organization. Within the BC context we are dealing with a mix of regionalized (acute and community services) and central (pharmacare and MSP) programs.
• The implementation of chronic disease management (i.e., diabetes) concurrent to primary care renewal initiatives runs the risk of having it being seen as tool to move the managed care agenda forward. Chronic disease management (i.e., diabetes) could then become a focal point in the debate about whether managed care is preferable. As a result support for chronic disease management (i.e., diabetes), especially among provider groups may be influenced by broader reform agendae.
• This risk can be reduced if chronic disease management (i.e., diabetes) is presented and accepted by stakeholders as a tool that can benefit the health system in both a non-managed care and in a managed care environment. Further, this risk can be reduced if chronic disease management (i.e., diabetes) is successfully demonstrated in a non-managed care environment.
Chronic Disease Management: Page 71 Improved Management of Diabetes Report from the Diabetes Working Group
6.4.3. Benefits Risk: High
• The implementation of chronic disease management (i.e., diabetes) in the United States and the NHS in managed care delivery systems has shown reductions in GP visits, specialist visits, emergency department visits, hospitalizations and dialysis.
• The implementation in Canada of chronic disease management (i.e., diabetes) is new. The evidence that the benefits obtained in the United States/NHS can be duplicated in Canada does not yet exist.
• While some of the incremental costs of this program accrue to the province, many accrue at the health authority level. The investment is to be made in community services yet the benefits predominantly occur within secondary care, both provider and facility. The challenge will be to transfer the savings (cost avoidance as opposed to true savings) to support the community based initiative on an ongoing basis to ensure program sustainability. This is always difficult when public attention is traditionally focused on waiting lists and emergency room utilization.
• The risk of not being able to realize the benefits (through cost reduction or cost avoidance) is that chronic disease management (i.e., diabetes) simply becomes an incremental cost to the health system.
To reduce this risk the Government of British Columbia through the BC Ministries Health and health authorities could implement a cost avoidance strategy that would reduce a planned future expenditure(s) (e.g. planned budget increase) by the amount(s) required to realize the benefit. This approach is contingent upon clearly knowing the extent of benefits that can be achieved in a Canadian setting.
6.4.4. Implementation Model Risk: Medium
• Chronic disease management has yet to be offered to large populations within Canada. The level of readiness and willingness to participate by key providers (i.e. physicians and nurses) and diabetes patients has yet to be determined.
• Unless previously proven chronic disease management models for diabetes are implemented in British Columbia then there is no basis on which to assume that the implementation model to be used will be successful.
• To reduce this risk a staged approach to implementation needs to be considered, whereby the selected implementation model can be tested and refined in a limited setting before it is rolled out at a regional or provincial level.
6.4.5. Cost Risk: Medium
• The primary cost drivers in a Diabetes Initiative are the cost of laboratory testing as well as information systems supports and patient supports for self management. To manage these costs it is critical that each cost factor is carefully managed.
Page 72
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
• This risk can be reduced by only implementing a full scale Diabetes Initiative after it has been fully tested and the demand and cost implications of providing this type of service can be better understood.
6.4.6. Other Risks: Low
There is a clear business case to proceed with payback on investment within 33 months. There are some project risks which need to be managed. The risks associated with quality of care, the role and scope of professional practice, the ability of health organizations to manage and operate the service, as well as the technology required to support the service is considered low.
6.5. Feasibility Analysis
The next step is the determination of what is feasible with a Diabetes Initiative – what can be realistically started in British Columbia within the next 12 months.
Three implementation options are obvious:
1. Local Implementation – within controlled environment in a small geography within a regional health authority.
2. Regional Implementation – within a single regional health authority.
3. Provincial Implementation – within all regional health authorities in the province.
The nature of the high and medium risks support the conclusion that a lot more study and refinement is required before a provincial implementation of the Diabetes Management Initiative can be considered. The scope of the service, the service delivery and implementation models for the initiative, as well as and the associated costs and benefits need to be more clearly understood.
Conclusion: based on the findings of the financial analysis and the risk analysis to move the Diabetes Management Initiative from theory to reality at this time requires a staged implementation approach, starting with a local implementation. Risks will be mitigated through adoption of strong project management methodologies.
Chronic Disease Management: Page 73 Improved Management of Diabetes Report from the Diabetes Working Group
777... TTTHHHEEE DDDIIIAAABBBEEETTTEEESSS IIINNNIIITTTIIIAAATTTIIIVVVEEE
7.1. Chronic Care Model
The underpinning of the Diabetes Initiative will be the “Chronic Care Model” (described in Section 5). The model is population-based, data driven and creates practical, supportive, evidence based interactions between an informed activated client and a prepared proactive practice team. This Initiative will evaluate the Expanded Chronic Care Model (Section 5) as an organizational approach to caring for people with diabetes in a BC primary health care setting. The Diabetes Working Group concluded from the risk analysis that it would be prudent to implement this initiative in a staged manner. The first local implementation will take place in the Vancouver Island Health Authority. While the first stage of this broad initiative will be within VIHA, other health authorities should become involved. Findings from local implementation will inform and shape future phases. VIHA is committed to sharing the learning from their implementation.
7.2. The Provincial Collaborative
7.2.1. Governance and Operations
The broad Diabetes Initiative, by the nature of the players, will be a Collaborative. The Collaborative will be created at a provincial level with participation from the key partners. The role of the Collaborative will be to support the provision of the 3 levels of action - population, provider and patient by providing:
• strategic guidance
• expert advice
• operational coordination
• marketing and communication
• funding support
• evaluation services
• the accountability for the delivery of the diabetes services will lie with the various partners depending upon the level of action.
The Population level of action documents the extent of diabetes in British Columbia, identifies diabetes indicators, monitors performance, and establishes a Provincial Diabetes Registry. This will lead to effective information management and regular and thorough reporting of progress related to the management of diabetes in this province. The key partners include:
Page 74
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
• BC Ministries of Health - data collection, data management, indicator development, Diabetes registry, data analysis and reporting
• Health Authorities - data collection, data management, indicator development, Diabetes registry, data analysis and reporting
The Provider level of action develops and implements clinical practice guidelines for diabetes management, implements methods to adopt and reinforce practice guidelines, devises standards of care and associated tools, institutes mechanisms for patient follow-up and recall, facilitates shared care and engages community-based agencies in initiatives to improve diabetes management.
The key partners include:
• BC Ministries of Health/Medical Services Commission - clinical guidelines development and review (with GPAC), standards of care coordination, and physician reimbursement mechanisms (including the Medical Services Commission)
• Health Authorities - diabetes specialists, clinic expertise / resources, patient follow-up and recall and community networks
• BCMA - practice guidelines, GP Services Committee, Primary Care Transition Fund Steering Committee
• Physicians - physician support, shared care
• Canadian Diabetes Association - community networks, resource message development and Diabetes resource centre
• Novartis – is working with the Ministry of Health Services to ensure private sector contribution to implementation of this initiative.
The Patient level of action develops and implements a patient survey, identifies and develops (as needed) patient education resources and tools, introduces care plans, and institutes a self-efficacy training program. The key partners include:
• BC Ministries of Health - patient survey and patient education resources and tools
• Health Authorities - patient education resources and tools, patient care plan and a self-efficacy training program
• Physicians - to be determined
• Canadian Diabetes Association - patient education resources and tools and a self-efficacy training program
• Novartis - is working with the Ministry of Health Services to ensure private sector contribution to implementation of this initiative.
Experience has also shown that several important themes reoccur through the different stages of a public-private initiative, such as the Diabetes Initiative. These include the importance of free and open communications between partners, a commitment to fair process, acceptance of organizational change, and a need for accountability procedures. It is important, therefore, for
Chronic Disease Management: Page 75 Improved Management of Diabetes Report from the Diabetes Working Group
partners to establish principles that will guide the public-private arrangement and to develop a road map to direct and inform the process.
7.2.2. Marketing and Communication
The success of the Diabetes Initiative will depend on awareness of the services offered by a number of different stakeholders - patients, providers (physicians, nurses), regional health authority management, Ministries of Health management, and other organizations involved in Diabetes. The Diabetes Initiative will be responsible for managing the provincial level marketing and communication.
Marketing and communication strategies will need to:
• create awareness and encourage diabetes patients to use the services
• promote ongoing dialogue and endorsement/support from key stakeholders such as physicians
Marketing and communication strategies will include:
• creating an identity or image for the Diabetes Initiative (also known as “branding”) that is easily identifiable
• designating a Diabetes Initiative spokesperson and conducting a high-visibility media event to announce the program publicly
• promoting the services to the public, health care professionals, health authorities, government, to create awareness and acceptance of the Initiative. Internet, and printed media (e.g. magazines, newsletters, etc) will be employed
• conducting stakeholder (e.g. physicians, patients) information sessions and distributing stakeholder information packages
• public and community relations, via community networks
7.3. Local Implementation #1: VIHA, South Island
The Vancouver Island Health Authority has prepared an implementation plan as a companion document to the Provincial Business Case. The VIHA Implementation Plan has two purposes.
• It is a working document for VIHA to guide chronic disease quality improvement efforts during a new phase of development which we refer to as "Implementing Improved Diabetes Management: Local Implementation #1".
• It can also be used by others as one example of translating the provincial-level economic arguments into regional actions. The Implementation Plan focuses on the VIHA, South Island Health Service Delivery Area (HSDA) which includes Greater Victoria and the surrounding municipalities.

Page 76
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
The South Island HSDA has an established quality improvement group called the Diabetes Outcome Improvement Team (DO IT). The Implementation Plan includes the regional initiatives that are listed in the table shown in Section 7.5. (This table shows the relationship of the provincial, regional, and provider-level projects costed in the business case analysis.) In addition, DO IT has capitalized on the experience of several years of local quality improvement efforts to include additional regional PDSA (plan, do, study, act) cycles. These additions, which do not necessarily have provincial counterparts, are examples of how local innovation to meet local needs are necessary and complement provincially-coordinated efforts. VIHA has also used the Expanded Chronic Care Model as an organizing framework for the Implementation Plan. The Plan reflects the full-breadth of the model including health promotion and disease prevention, as well as chronic disease management. To access the VIHA, South Island Diabetes Implementation Plan, see http://www.caphealth.org/mho/diabetes/. The work described in the VIHA Plan is underway, and is expected that the Plan will be in active use and adapted as the work progresses in all areas of the Model.
7.4. Next Steps
This document has summarized the issue and management of chronic disease and diabetes in BC, Canada and elsewhere in the world. The literature reveals that the numbers of people with chronic diseases are rapidly increasing and diabetes is becoming an epidemic. While many of the consequences of diabetes can be avoided the current BC primary care system does not support optimal management. At the same time the current costs of managing the health care for diabetes in BC is staggering. There are demonstrated successes in better management of chronic diseases including diabetes, both in health outcomes for individuals with diabetes and cost savings for the health care system.
It is clear that there is an economic case to proceed with a Diabetes Initiative with a pay back of 33 months. The economic and care consequences of the failure not manage diabetes are overwhelming and will exceed the capacity of the BC health care system. Failure to utilize the current concepts of evidence-based management of diabetes would be irresponsible.
The Diabetes Working Group is recommending proceeding with the BC Diabetes Initiative. To mitigate risk, the initiative will proceed with a local implementation within VIHA. This local implementation will refine the delivery model for chronic disease management, and in particular diabetes, for the Canadian context as well as reconfirm the costs and benefits associated with the business case. While VIHA is one of the early implementers, this does not preclude the participation of other health authorities or partners. The recent directions on primary health care from the Federal and Provincial governments and the infusion of the Primary Health Care Transition Fund, may provide opportunities for all Health Authorities to implement a Diabetes Initiative utilizing the Chronic Care Model closely linked with their other primary health care strategies.
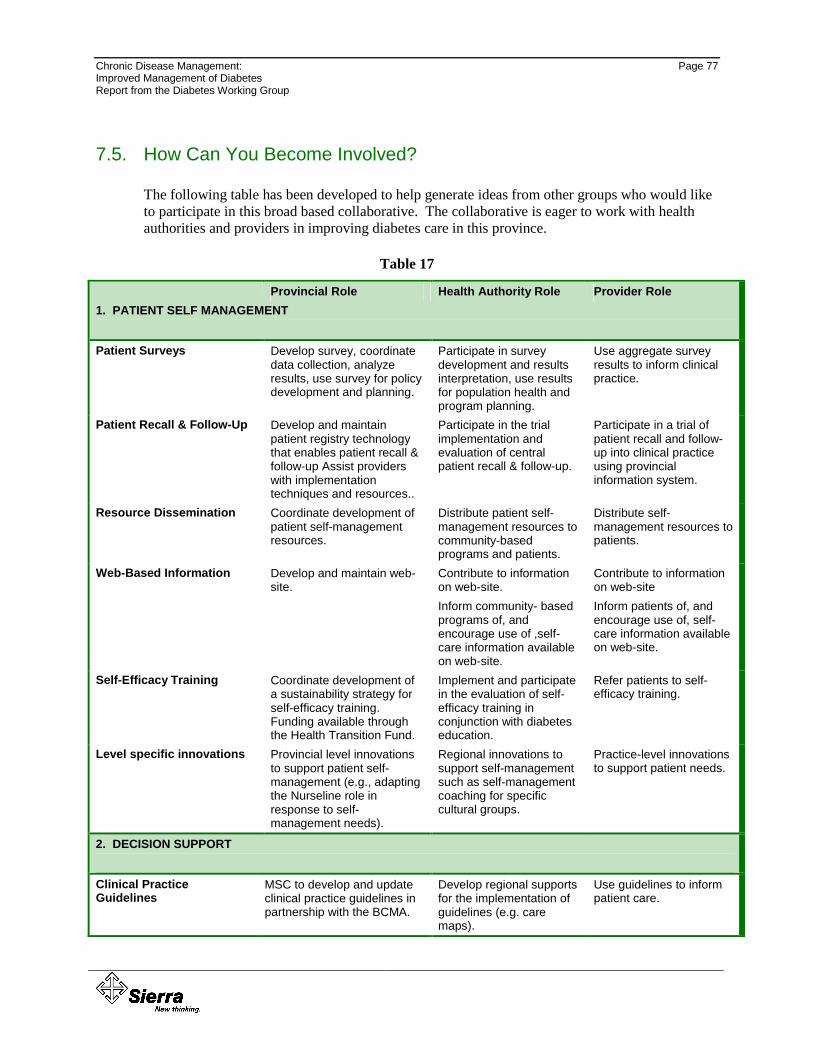
Chronic Disease Management: Page 77 Improved Management of Diabetes Report from the Diabetes Working Group
7.5. How Can You Become Involved?
The following table has been developed to help generate ideas from other groups who would like to participate in this broad based collaborative. The collaborative is eager to work with health authorities and providers in improving diabetes care in this province.
Table 17
Provincial Role Health Authority Role Provider Role 1. PATIENT SELF MANAGEMENT Patient Surveys Develop survey, coordinate
data collection, analyze results, use survey for policy development and planning.
Participate in survey development and results interpretation, use results for population health and program planning.
Use aggregate survey results to inform clinical practice.
Patient Recall & Follow-Up
Develop and maintain patient registry technology that enables patient recall & follow-up Assist providers with implementation techniques and resources..
Participate in the trial implementation and evaluation of central patient recall & follow-up.
Participate in a trial of patient recall and follow-up into clinical practice using provincial information system.
Resource Dissemination
Coordinate development of patient self-management resources.
Distribute patient self- management resources to community-based programs and patients.
Distribute self-management resources to patients.
Web-Based Information
Develop and maintain web-site.
Contribute to information on web-site. Inform community- based programs of, and encourage use of ,self-care information available on web-site.
Contribute to information on web-site Inform patients of, and encourage use of, self-care information available on web-site.
Self-Efficacy Training
Coordinate development of a sustainability strategy for self-efficacy training. Funding available through the Health Transition Fund.
Implement and participate in the evaluation of self-efficacy training in conjunction with diabetes education.
Refer patients to self-efficacy training.
Level specific innovations Provincial level innovations to support patient self-management (e.g., adapting the Nurseline role in response to self-management needs).
Regional innovations to support self-management such as self-management coaching for specific cultural groups.
Practice-level innovations to support patient needs.
2. DECISION SUPPORT Clinical Practice Guidelines
MSC to develop and update clinical practice guidelines in partnership with the BCMA.
Develop regional supports for the implementation of guidelines (e.g. care maps).
Use guidelines to inform patient care.
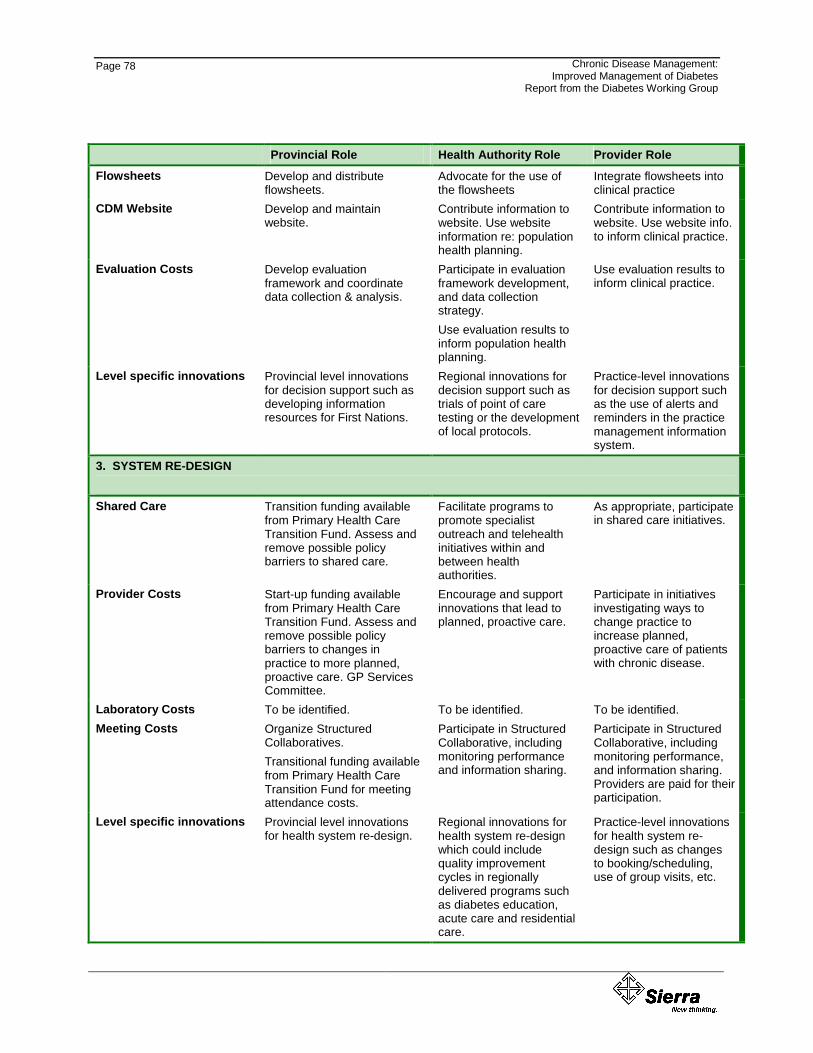
Page 78
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
Provincial Role Health Authority Role Provider Role Flowsheets Develop and distribute
flowsheets. Advocate for the use of the flowsheets
Integrate flowsheets into clinical practice
CDM Website Develop and maintain website.
Contribute information to website. Use website information re: population health planning.
Contribute information to website. Use website info. to inform clinical practice.
Evaluation Costs Develop evaluation framework and coordinate data collection & analysis.
Participate in evaluation framework development, and data collection strategy. Use evaluation results to inform population health planning.
Use evaluation results to inform clinical practice.
Level specific innovations Provincial level innovations for decision support such as developing information resources for First Nations.
Regional innovations for decision support such as trials of point of care testing or the development of local protocols.
Practice-level innovations for decision support such as the use of alerts and reminders in the practice management information system.
3. SYSTEM RE-DESIGN
Shared Care Transition funding available from Primary Health Care Transition Fund. Assess and remove possible policy barriers to shared care.
Facilitate programs to promote specialist outreach and telehealth initiatives within and between health authorities.
As appropriate, participate in shared care initiatives.
Provider Costs Start-up funding available from Primary Health Care Transition Fund. Assess and remove possible policy barriers to changes in practice to more planned, proactive care. GP Services Committee.
Encourage and support innovations that lead to planned, proactive care.
Participate in initiatives investigating ways to change practice to increase planned, proactive care of patients with chronic disease.
Laboratory Costs To be identified. To be identified. To be identified. Meeting Costs Organize Structured
Collaboratives. Transitional funding available from Primary Health Care Transition Fund for meeting attendance costs.
Participate in Structured Collaborative, including monitoring performance and information sharing.
Participate in Structured Collaborative, including monitoring performance, and information sharing. Providers are paid for their participation.
Level specific innovations Provincial level innovations for health system re-design.
Regional innovations for health system re-design which could include quality improvement cycles in regionally delivered programs such as diabetes education, acute care and residential care.
Practice-level innovations for health system re-design such as changes to booking/scheduling, use of group visits, etc.
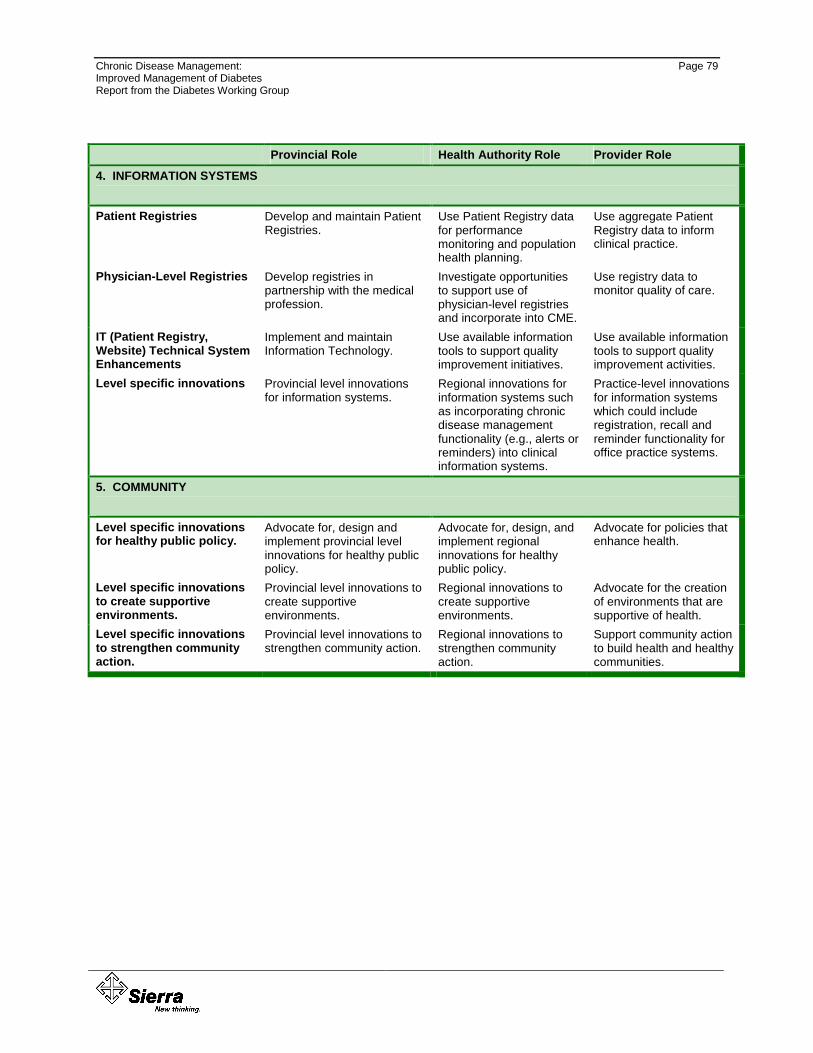
Chronic Disease Management: Page 79 Improved Management of Diabetes Report from the Diabetes Working Group
Provincial Role Health Authority Role Provider Role 4. INFORMATION SYSTEMS
Patient Registries Develop and maintain Patient Registries.
Use Patient Registry data for performance monitoring and population health planning.
Use aggregate Patient Registry data to inform clinical practice.
Physician-Level Registries Develop registries in partnership with the medical profession.
Investigate opportunities to support use of physician-level registries and incorporate into CME.
Use registry data to monitor quality of care.
IT (Patient Registry, Website) Technical System Enhancements
Implement and maintain Information Technology.
Use available information tools to support quality improvement initiatives.
Use available information tools to support quality improvement activities.
Level specific innovations Provincial level innovations for information systems.
Regional innovations for information systems such as incorporating chronic disease management functionality (e.g., alerts or reminders) into clinical information systems.
Practice-level innovations for information systems which could include registration, recall and reminder functionality for office practice systems.
5. COMMUNITY
Level specific innovations for healthy public policy.
Advocate for, design and implement provincial level innovations for healthy public policy.
Advocate for, design, and implement regional innovations for healthy public policy.
Advocate for policies that enhance health.
Level specific innovations to create supportive environments.
Provincial level innovations to create supportive environments.
Regional innovations to create supportive environments.
Advocate for the creation of environments that are supportive of health.
Level specific innovations to strengthen community action.
Provincial level innovations to strengthen community action.
Regional innovations to strengthen community action.
Support community action to build health and healthy communities.
Chronic Disease Management Appendix A-1 Improved Management of Diabetes Report from the Diabetes Working Group
Appendix A. Diabetes Working Group Members
Cathy Adair, Executive Director, Pacific Area, Canadian Diabetes Association
Mehmood Alibhai, Novartis
Dr. Marshall Dahl, BC Medical Association Representative
Dr. Daniel Metzger, Endocrinology and Diabetes Unit, BC Children’s Hospital
Dr. Howard Platt, Director, Utilization Management Branch, BC Ministry of Health Services
Sylvia Robinson, Manager, Chronic Disease Initiatives, Vancouver Island Health Authority
Deborah Shera, Partner, Sierra Systems
Barb Stackhouse, Director, Community Health Services, Vancouver Coastal Health Authority
Alice Taft, Area Director and Site Administrator, Primary and Community Hospital Care, Vancouver Island Health Authority
Valerie Tregillus, Director of Strategic Initiatives, BC Ministry of Health Services
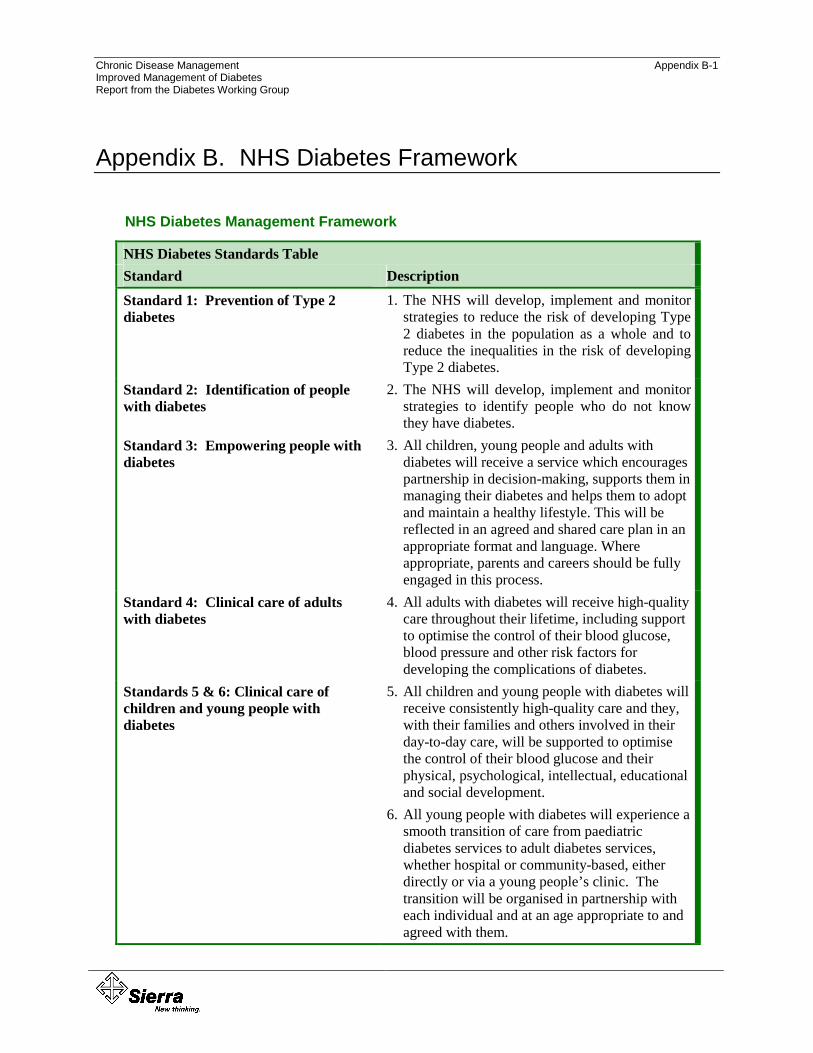
Chronic Disease Management Appendix B-1 Improved Management of Diabetes Report from the Diabetes Working Group
Appendix B. NHS Diabetes Framework
NHS Diabetes Management Framework
NHS Diabetes Standards Table Standard Description Standard 1: Prevention of Type 2 diabetes
1. The NHS will develop, implement and monitor strategies to reduce the risk of developing Type 2 diabetes in the population as a whole and to reduce the inequalities in the risk of developing Type 2 diabetes.
Standard 2: Identification of people with diabetes
2. The NHS will develop, implement and monitor strategies to identify people who do not know they have diabetes.
Standard 3: Empowering people with diabetes
3. All children, young people and adults with diabetes will receive a service which encourages partnership in decision-making, supports them in managing their diabetes and helps them to adopt and maintain a healthy lifestyle. This will be reflected in an agreed and shared care plan in an appropriate format and language. Where appropriate, parents and careers should be fully engaged in this process.
Standard 4: Clinical care of adults with diabetes
4. All adults with diabetes will receive high-quality care throughout their lifetime, including support to optimise the control of their blood glucose, blood pressure and other risk factors for developing the complications of diabetes.
Standards 5 & 6: Clinical care of children and young people with diabetes
5. All children and young people with diabetes will receive consistently high-quality care and they, with their families and others involved in their day-to-day care, will be supported to optimise the control of their blood glucose and their physical, psychological, intellectual, educational and social development.
6. All young people with diabetes will experience a smooth transition of care from paediatric diabetes services to adult diabetes services, whether hospital or community-based, either directly or via a young people’s clinic. The transition will be organised in partnership with each individual and at an age appropriate to and agreed with them.

Appendix E-2
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
NHS Diabetes Standards Table Standard Description Standard 7: Management of diabetes emergencies
7. The NHS will develop, implement and monitor agreed protocols for rapid and effective treatment of diabetes emergencies by appropriately trained health care professionals. Protocols will include the management of acute complications and procedures to minimise the risk of recurrence.
Standard 8: Care of people with diabetes during admission to hospital
8. All children, young people and adults with diabetes admitted to hospital, for whatever reason, will receive effective care of their diabetes. Wherever possible, they will continue to be involved in decisions concerning the management of their diabetes.
Standard 9: Diabetes and pregnancy 9. The NHS will develop, implement and monitor policies that seek to empower and support women with pre-existing diabetes and those who develop diabetes during pregnancy to optimise the outcomes of their pregnancy.
Standards 10, 11 & 12: Detection and management of long-term complications
10. All young people and adults with diabetes will receive regular surveillance for the long-term complications of diabetes.
11. The NHS will develop, implement and monitor agreed protocols and systems of care to ensure that all people who develop long-term complications of diabetes receive timely, appropriate and effective investigation and treatment to reduce their risk of disability and premature death.
12. All people with diabetes requiring multi-agency support will receive integrated health and social care.
Chronic Disease Management Appendix C-1 Improved Management of Diabetes Report from the Diabetes Working Group
Appendix C. BC Diabetes Care Guidelines
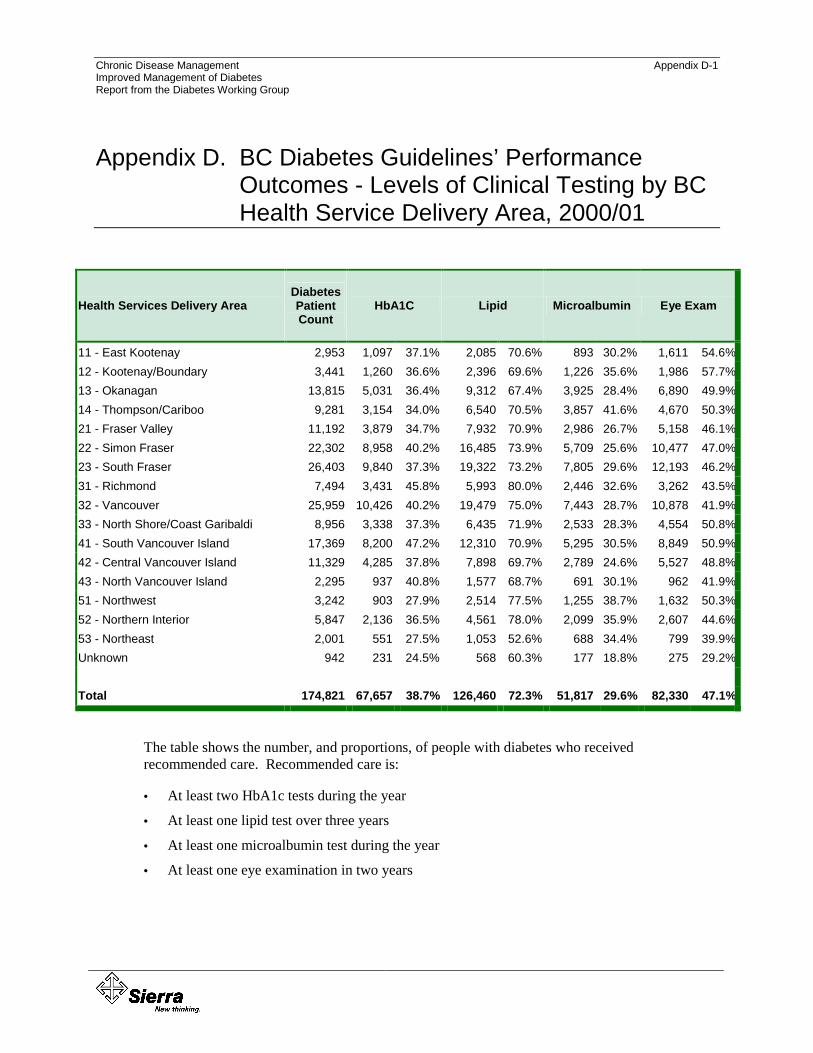
Chronic Disease Management Appendix D-1 Improved Management of Diabetes Report from the Diabetes Working Group
Appendix D. BC Diabetes Guidelines’ Performance Outcomes - Levels of Clinical Testing by BC Health Service Delivery Area, 2000/01
Health Services Delivery Area Diabetes Patient Count
HbA1C Lipid Microalbumin Eye Exam
11 - East Kootenay 2,953 1,097 37.1% 2,085 70.6% 893 30.2% 1,611 54.6%12 - Kootenay/Boundary 3,441 1,260 36.6% 2,396 69.6% 1,226 35.6% 1,986 57.7%13 - Okanagan 13,815 5,031 36.4% 9,312 67.4% 3,925 28.4% 6,890 49.9%14 - Thompson/Cariboo 9,281 3,154 34.0% 6,540 70.5% 3,857 41.6% 4,670 50.3%21 - Fraser Valley 11,192 3,879 34.7% 7,932 70.9% 2,986 26.7% 5,158 46.1%22 - Simon Fraser 22,302 8,958 40.2% 16,485 73.9% 5,709 25.6% 10,477 47.0%23 - South Fraser 26,403 9,840 37.3% 19,322 73.2% 7,805 29.6% 12,193 46.2%31 - Richmond 7,494 3,431 45.8% 5,993 80.0% 2,446 32.6% 3,262 43.5%32 - Vancouver 25,959 10,426 40.2% 19,479 75.0% 7,443 28.7% 10,878 41.9%33 - North Shore/Coast Garibaldi 8,956 3,338 37.3% 6,435 71.9% 2,533 28.3% 4,554 50.8%41 - South Vancouver Island 17,369 8,200 47.2% 12,310 70.9% 5,295 30.5% 8,849 50.9%42 - Central Vancouver Island 11,329 4,285 37.8% 7,898 69.7% 2,789 24.6% 5,527 48.8%43 - North Vancouver Island 2,295 937 40.8% 1,577 68.7% 691 30.1% 962 41.9%51 - Northwest 3,242 903 27.9% 2,514 77.5% 1,255 38.7% 1,632 50.3%52 - Northern Interior 5,847 2,136 36.5% 4,561 78.0% 2,099 35.9% 2,607 44.6%53 - Northeast 2,001 551 27.5% 1,053 52.6% 688 34.4% 799 39.9%Unknown 942 231 24.5% 568 60.3% 177 18.8% 275 29.2% Total 174,821 67,657 38.7% 126,460 72.3% 51,817 29.6% 82,330 47.1%
The table shows the number, and proportions, of people with diabetes who received recommended care. Recommended care is:
• At least two HbA1c tests during the year
• At least one lipid test over three years
• At least one microalbumin test during the year
• At least one eye examination in two years
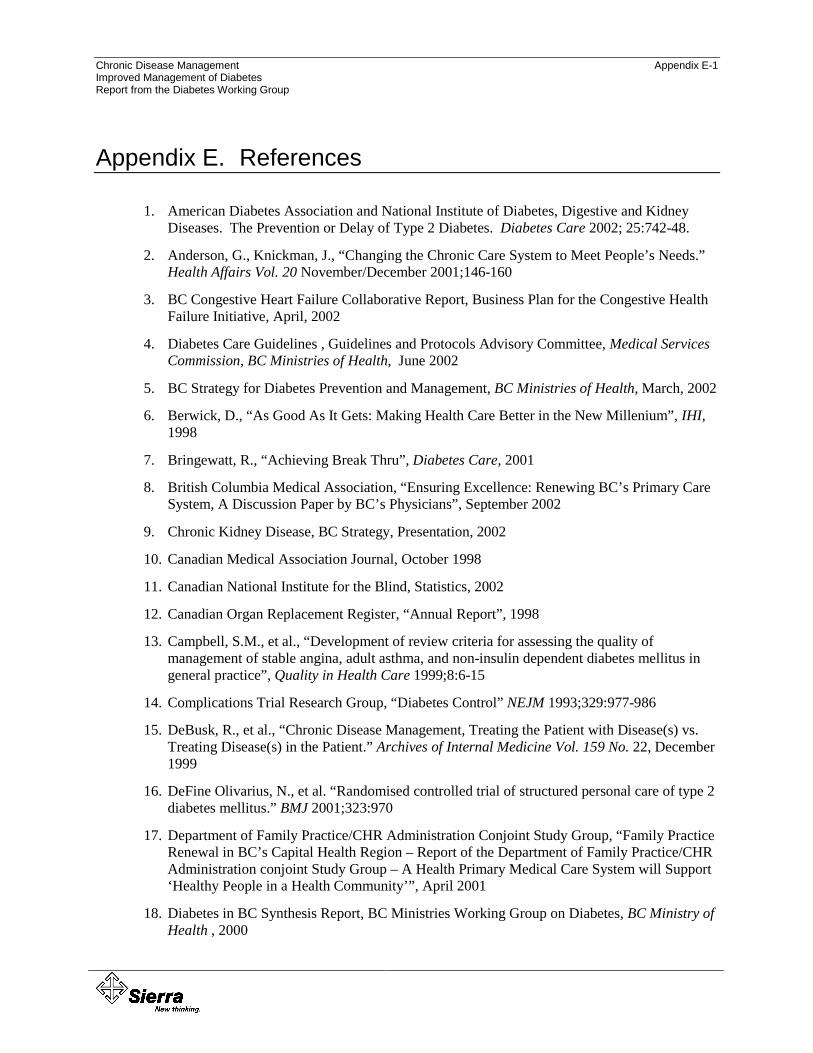
Chronic Disease Management Appendix E-1 Improved Management of Diabetes Report from the Diabetes Working Group
Appendix E. References
1. American Diabetes Association and National Institute of Diabetes, Digestive and Kidney Diseases. The Prevention or Delay of Type 2 Diabetes. Diabetes Care 2002; 25:742-48.
2. Anderson, G., Knickman, J., “Changing the Chronic Care System to Meet People’s Needs.” Health Affairs Vol. 20 November/December 2001;146-160
3. BC Congestive Heart Failure Collaborative Report, Business Plan for the Congestive Health Failure Initiative, April, 2002
4. Diabetes Care Guidelines , Guidelines and Protocols Advisory Committee, Medical Services Commission, BC Ministries of Health, June 2002
5. BC Strategy for Diabetes Prevention and Management, BC Ministries of Health, March, 2002
6. Berwick, D., “As Good As It Gets: Making Health Care Better in the New Millenium”, IHI, 1998
7. Bringewatt, R., “Achieving Break Thru”, Diabetes Care, 2001
8. British Columbia Medical Association, “Ensuring Excellence: Renewing BC’s Primary Care System, A Discussion Paper by BC’s Physicians”, September 2002
9. Chronic Kidney Disease, BC Strategy, Presentation, 2002
10. Canadian Medical Association Journal, October 1998
11. Canadian National Institute for the Blind, Statistics, 2002
12. Canadian Organ Replacement Register, “Annual Report”, 1998
13. Campbell, S.M., et al., “Development of review criteria for assessing the quality of management of stable angina, adult asthma, and non-insulin dependent diabetes mellitus in general practice”, Quality in Health Care 1999;8:6-15
14. Complications Trial Research Group, “Diabetes Control” NEJM 1993;329:977-986
15. DeBusk, R., et al., “Chronic Disease Management, Treating the Patient with Disease(s) vs. Treating Disease(s) in the Patient.” Archives of Internal Medicine Vol. 159 No. 22, December 1999
16. DeFine Olivarius, N., et al. “Randomised controlled trial of structured personal care of type 2 diabetes mellitus.” BMJ 2001;323:970
17. Department of Family Practice/CHR Administration Conjoint Study Group, “Family Practice Renewal in BC’s Capital Health Region – Report of the Department of Family Practice/CHR Administration conjoint Study Group – A Health Primary Medical Care System will Support ‘Healthy People in a Health Community’”, April 2001
18. Diabetes in BC Synthesis Report, BC Ministries Working Group on Diabetes, BC Ministry of Health , 2000
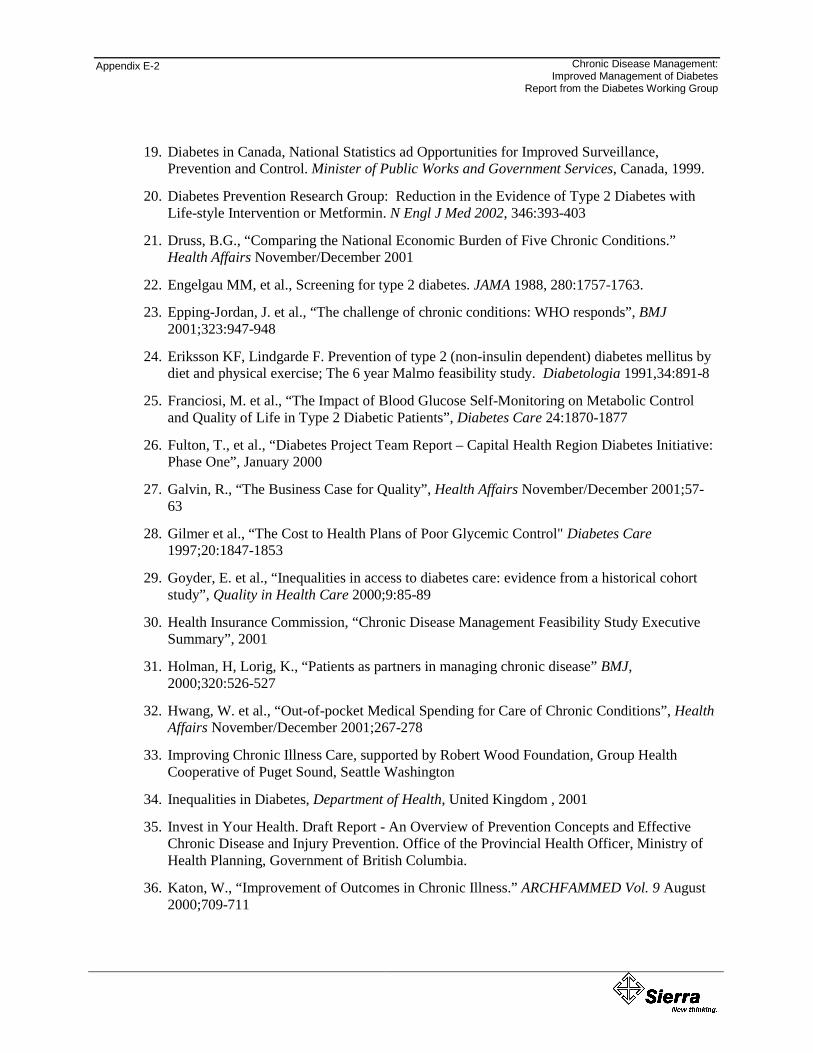
Appendix E-2
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
19. Diabetes in Canada, National Statistics ad Opportunities for Improved Surveillance, Prevention and Control. Minister of Public Works and Government Services, Canada, 1999.
20. Diabetes Prevention Research Group: Reduction in the Evidence of Type 2 Diabetes with Life-style Intervention or Metformin. N Engl J Med 2002, 346:393-403
21. Druss, B.G., “Comparing the National Economic Burden of Five Chronic Conditions.” Health Affairs November/December 2001
22. Engelgau MM, et al., Screening for type 2 diabetes. JAMA 1988, 280:1757-1763.
23. Epping-Jordan, J. et al., “The challenge of chronic conditions: WHO responds”, BMJ 2001;323:947-948
24. Eriksson KF, Lindgarde F. Prevention of type 2 (non-insulin dependent) diabetes mellitus by diet and physical exercise; The 6 year Malmo feasibility study. Diabetologia 1991,34:891-8
25. Franciosi, M. et al., “The Impact of Blood Glucose Self-Monitoring on Metabolic Control and Quality of Life in Type 2 Diabetic Patients”, Diabetes Care 24:1870-1877
26. Fulton, T., et al., “Diabetes Project Team Report – Capital Health Region Diabetes Initiative: Phase One”, January 2000
27. Galvin, R., “The Business Case for Quality”, Health Affairs November/December 2001;57-63
28. Gilmer et al., “The Cost to Health Plans of Poor Glycemic Control" Diabetes Care 1997;20:1847-1853
29. Goyder, E. et al., “Inequalities in access to diabetes care: evidence from a historical cohort study”, Quality in Health Care 2000;9:85-89
30. Health Insurance Commission, “Chronic Disease Management Feasibility Study Executive Summary”, 2001
31. Holman, H, Lorig, K., “Patients as partners in managing chronic disease” BMJ, 2000;320:526-527
32. Hwang, W. et al., “Out-of-pocket Medical Spending for Care of Chronic Conditions”, Health Affairs November/December 2001;267-278
33. Improving Chronic Illness Care, supported by Robert Wood Foundation, Group Health Cooperative of Puget Sound, Seattle Washington
34. Inequalities in Diabetes, Department of Health, United Kingdom , 2001
35. Invest in Your Health. Draft Report - An Overview of Prevention Concepts and Effective Chronic Disease and Injury Prevention. Office of the Provincial Health Officer, Ministry of Health Planning, Government of British Columbia.
36. Katon, W., “Improvement of Outcomes in Chronic Illness.” ARCHFAMMED Vol. 9 August 2000;709-711

Chronic Disease Management Appendix E-3 Improved Management of Diabetes Report from the Diabetes Working Group
37. Diabetes in Canada – National Opportunities for Improved Surveillance, Prevention and Control” Laboratory Centre for Disease Control. Health Canada 1999
38. Laditka, S.B., et al., “Health Care Use of Individuals with Diabetes in an Employer-based Insurance Population”, Arch Intern Med May 2001;161:1301-1308
39. Leveille et al , Health Enhancement Project 1998 JAGS 1998;46:1191-98
40. Litzelman, DK et al., “Reduction of lower extremity clinical abnormalities in patients with non-insulin-dependent diabetes mellitus. A randomized, controlled trial.”, NCBI 2001
41. Lorig KR, et al., “Evidence suggesting that a Chronic Disease Self-Management Program can improve health status while reducing hospitalization: A Randomized Trial.” Medical Care 1999; 37(1):5-14.
42. Maberley, D., “Diabetes and Diabetic Retinopathy in Canadian Aboriginal Peoples: a Literature Review”, 2001
43. Meltzer, S., “1998 clinical practice guidelines for the management of diabetes in Canada”, Supplement to CMAJ 1998;159(8 Suppl)
44. Melville, A., Richardson, R., “Complications of diabetes: screening for retinopathy and management of foot ulcers”, Quality in Health Care 2000;9:137-141
45. Mettler, M. ‘That patient is not diabetes case #115491. She’s me’. Robert Wood Johnson Foundation, October, 2000.
46. Glasgow, R., et al., “Does the Chronic Care Model also serve as a template for improving prevention?”, The Milbank Quarterly, 79(4), and World Health Organization, Health and Welfare Canada and Canadian Public Health Association, (1986), Ottawa Charter of Health Promotion
47. Mirkin, R. et al., “The Care Management Institute’s Integrated Diabetes Care Program: A Collaborative Approach to Improving Patient Care and Outcomes”, National Institute for Health Care Management Forum, 2001
48. National Institutes of Health: Clinical guidelines on the identification, evaluation and treatment of overweight and obesity in adults; the evidence report. Obes Res 1998; 6 (Suppl. 2): 51S-209S.
49. National Health Performance Framework Report, National Health Performance Committee, ,Canadian Diabetes Association, August 2001
50. NIH Consensus Development Panel on Physician Activity and Cardiovascular Health: Physical activity and cardiovascular health. JAMA 1996; 276:241-246.
51. NHS Department of Health, “Modern Standards and Service Models – National Service Framework for Diabetes: Standards”, United Kingdom, 2001
52. Ni, H. et al., “Managed Care and Outcomes of Hospitalization Among Elderly Patients with Congestive Heart Failure”, Archives of Internal Medicine June 1998;Vol.158 No. 11
Appendix E-4
Chronic Disease Management: Improved Management of Diabetes
Report from the Diabetes Working Group
53. Pan XR, et al.,Effects of diet and exercise in prevention NIDDM in people with impaired glucose tolerance: The Da Qing IGT and Diabetes Study. Diabetes Care 1997;20:537-44
54. Pierce, M., “Improving care for people with diabetes”, Quality in Health Care 2000;9:82
55. Renders, C. et al., “Long-Term Effectiveness of a Quality Improvement Program for Patients with Type 2 Diabetes in General Practice”, Diabetes Care Vol. 23, No. 8., August 2001:1365-1370
56. Rubin et al., “Clinical and Economic Impact of Implementing a Comprehensive Diabetes Management Program in Managed Care:, Journal of Clinical Endocrinology and Metabolism, Vol. 83, No. 8, 1998: 2635-2642
57. Sadur, C.N., “Diabetes management in a health maintenance organization. Efficacy of care management using cluster visits”, Diabetes Care 1999;22:2011-2017
58. Schillinger, D. et al., “Association of Health Literacy with Diabetes Outcomes”, 2002:288, 475-482
59. Scottish Diabetes Framework Working Group, “Scottish Diabetes Framework Consultation Paper”, NHS, United Kingdom, July 2001
60. Sturm, R., Roan Gresenz, C., “Relations of income inequality and family income to chronic medical conditions and mental health disorders: national survey”, BMJ 2002;324:1-5
61. Tan et al., “Prevalence of Diabetes and Ethnic Differences in Cardiovascular Risk Factors”, Diabetes Care, 1999, 22:241-247
62. Testa, M., Simonson, D., “Health Economic Benefits and Quality of Life During Improved Glycemic Control in Patients with Type 2 Diabetes Mellitus” JAMA 1998;280
63. Tuomilehto J, Lindstrom MS, Eriksson J, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med 2001; 3441:343-50.
64. UK Department of Health, “The Expert Patient: A New approach to Chronic Disease Management for the 21st Century”, 2001
65. UKPDS, “Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38”, BMJ 1998;317:703-713
66. UKPDS, “Efficacy of atenolol and captopril in reducing risk of macrovascular and microvascular complicationsin type2 diabetes: UKPDS 39”, BMJ 1998;317:713-720
67. UKPDS, “Cost effectiveness of an intensive blood glucose control policy in patients with type 2 diabetes: economic analysis alongside randomised controlled trial UKPDS 41”, BMJ 2000;320:1373-1378
68. UKPDS, “Intensive blood glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complication sin patients with type 2 diabetes UKPDS 38” Lancet 1998;352:877-883
Chronic Disease Management Appendix E-5 Improved Management of Diabetes Report from the Diabetes Working Group
69. UKPDS, “Effect of intensive blood glucose control with metformin on complications in overweight patients with type 2 diabetes UKPDS 34”, Lancet 1998;352:854-865
70. Valmadrid, C., et al., “The Risk of Cardiovascular Disease Mortality Associated with Microalbuminuria and Gross Proteinuria in Persons with Older-Onset Diabetes Mellitus” Arch Intern Med 2000;160:1093-1100
71. Vancouver/Richmond Health Board Report, Integrated Diabetes Care: An Application of the Chronic Care Model, February, 2002
72. Vladeck, B., “You Can’t Get There From Here: Obstacles to Improving Care of the Chronically Ill” Health Affairs November/December 2001:175-179
73. Vrijhoef, H.J.M., “Adoption of disease management model for diabetes in region of Maastricht” BMJ 2001;323:983-985
74. Wagner E, Austin B, Von Korff M. Improving outcomes in chronic illness. Managed Care Quarterly 1996; 4(2); 12 -15.
75. Wagner, E., “A Population-Based Approach to Diabetes Management in a Primary Care Setting: Early Results and Lessons Learned”, Effective Clinical Practice 1998:12-22
76. Wagner, E., “The role of patient care teams in chronic disease management”, BMJ 2000;320:569-572
77. Wagner, E. et al., “Improving Chronic Illness Care: Translating Evidence into Action”, Health Affairs 2001;20:64-78
78. Wagner, E., “Designing Practice for Chronically Ill Patients: The Chronic Care Model”, Academy Health, Annual General Meeting, June, 2001
79. Wagner, E., “Meeting the needs of chronically ill people”, BMJ 2001;323:945-946
80. Wagner, E. et al., “Effect of Improved Glycemic Control on Health Care Costs and Utilization”, JAMA 2001;285
81. Wagner, E., “The Business Case for Better Chronic Illness Care”, IHI National Forum 2001
82. Wolpert, H., “Management of diabetes: are doctors framing the benefits from the wrong perspective?”, BMJ 2001;323:994-996