improving cardiovascular and diabetes care and outcomes cardiovascular and... · 2017 kentucky...
TRANSCRIPT
2017
Kentucky Department for Public Health
Improving Cardiovascular and Diabetes Care and Outcomes:
Change Package for Clinical Practice Teams

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 1
This page intentionally left blank.

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 2
Contents
Disclaimer ------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------ 4
Funding ------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------ 4
Suggested Citation --------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------- 4 Publishing Location (website) --------------------------------------------------------------------------------------------------------------------------------------------------------------------------- 4 Initial Publishing Date -------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------- 4
Contributing Sponsors -------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------- 5
Acknowledgments ------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------- 6
Measure Up / Pressure Down Provider Toolkit --------------------------------------------------------------------------------------------------------------------------------------------------------- 6
Together2Goal -------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------- 6
Introduction --------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------- 7
Focus Areas ---------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------- 8
How to Apply the Change Package --------------------------------------------------------------------------------------------------------------------------------------------------------------------------- 9
Model for Improvement -------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------- 9
Operational Efficiency ------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------ 10
1. Use Clinical Information Systems to Collect Pertinent Patient Information -------------------------------------------------------------------------------------------------------------- 10
2. Make Chronic Disease Management and Control a Practice Priority ---------------------------------------------------------------------------------------------------------------------- 10
Evidence-Based Interventions ------------------------------------------------------------------------------------------------------------------------------------------------------------------------------- 13
1. Use Evidence-Based Care Guidelines and Treatment Protocols in Systematic Ways -------------------------------------------------------------------------------------------------- 13
2. Implement a Policy and Process to Measure and Address A1C Every 3-6 Months for Every Patient with Diabetes ----------------------------------------------------------- 17
3. Implement Policy and Processes to Measure and Address Blood Pressure at Every Patient Encounter -------------------------------------------------------------------------- 18
4. Use Clinician-Managed Protocols for Medication Adjustments and Lifestyle Recommendations --------------------------------------------------------------------------------- 22
5. Integrate Compre-hensive Medication Management ------------------------------------------------------------------------------------------------------------------------------------------ 23
6. Train and Evaluate Direct Care Staff on Accurate BP Measurement and Recording--------------------------------------------------------------------------------------------------- 27

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 3
Patient Self-Management ------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------- 28
1. Empower Patients with Knowledge and Skills for Self-Management – Refer for Diabetes Self-Management Education and Support (DSMES) ---------------------- 28
2. Empower Patients with Knowledge and Skills for Self-Management – Refer for Self-Measured Blood Pressure Monitoring (SMBP).----------------------------------- 31
3. Equip Direct Care Staff to Facilitate Patient Self-Management Education and Support ---------------------------------------------------------------------------------------------- 32
4. Support Patients In Hypertension or Diabetes Self-Management During Their Routine Daily Activities (e.g., Not Related to Any Specific Visit) --------------------- 35
Data Driven Quality Improvement ------------------------------------------------------------------------------------------------------------------------------------------------------------------------- 38
1. Use Patient Registry to Identify, Track and Manage the Population of Patients with Hypertension and Diabetes ----------------------------------------------------------- 38
2. Use Practice Data to Drive Improvement ---------------------------------------------------------------------------------------------------------------------------------------------------------- 40

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 4
Disclaimer
This toolkit provides general guidance and does not take into account the unique health issues of individual patients. It is not intended to be used as a substitute for the independent judgment of a medical provider.
Funding This publication was supported by the Grant or Cooperative Agreement Number, DP004809, funded by the Centers for Disease Control and Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the Department of Health and Human Services.
Suggested Citation Kentucky Cabinet for Health and Family Services. The 2017 Improving Cardiovascular and Diabetes Care and Outcomes: Change Package for Clinical Practice Teams. Frankfort, KY: KY Cabinet for Health and Family Services, Department for Public Health, Division of Prevention and Quality Improvement, Chronic Disease Prevention Branch, Heart Disease and Stroke Prevention Program, and Diabetes Prevention and Control Program, 2017. Publishing Location (website)
http://www.kydiabetes.net/diabetesandhypertensionphysicianofficechangepackage.html Initial Publishing Date
November 2017

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 5
Contributing Sponsors

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 6
Acknowledgments
Measure Up / Pressure Down™ Provider Toolkit The American Medical Group Foundation and American Medical Group Association (AMGA) produced a toolkit for medical groups participating in Measure Up / Pressure Down™. The provider toolkit addresses many common challenges associated with effectively treating and managing hypertension. The comprehensive provider toolkit is available for download at: http://www.measureuppressuredown.com/HCProf/Find/provToolkit_find.asp.
Together2Goal® Together 2 Goal® Planks used with permission from the American Medical Group Foundation. The AMGA Foundation produced the Together 2 Goal® Campaign Toolkit to help implement best practices and address many of the common challenges associated with effectively managing type 2 diabetes. The comprehensive toolkit is available for download at: http://www.together2goal.org/Improve/toolkit_improve.html.

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 7
Introduction Medical practices see people with cardiovascular disease and type 2 diabetes on a daily basis. Management of these common health conditions is complex and quite challenging for both practitioners and their patients. To help support medical practices focused on optimizing chronic disease management, the Kentucky Department for Public Health and the Kentucky Regional Extension Center (Kentucky REC) have developed this toolkit: Improving Cardiovascular and Diabetes Care and Outcomes: Change Package for Clinical Practice Teams. The resource contains quality improvement materials including change concepts, actionable change ideas and related best practice tools and resources that target both hypertension and diabetes management. The terms “change concept” and “change idea” are credited to the Institute for Healthcare Improvement (IHI). Change concept is a general evidence-based improvement principle while the related change ideas are specific actionable items. Evidence-based tools and resources are supporting materials for the change ideas. Application of the toolkit concepts and ideas can help significantly improve process and outcomes related to hypertension and diabetes care management. The package contents are categorized in the following areas of focus:
Operational Efficiency
Evidence-Based Interventions
Patient Self-Management
Data Driven Quality Improvement

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 8
Focus Areas Operational Efficiency Evidence-Based
Interventions Patient Self-Management Data Driven Quality
Improvement Targeted to streamline clinical operations to reduce variations in recordings and results, these change concepts build on information systems as well as human skills development. They are best implemented with team input and with physician champions leading the quality improvement efforts. Following the mantra of “every patient, every time”, can lead to sustained success.
Research has shown that application of evidence-based clinical protocols, clinical decision support tools, provider and patient reminder systems have dramatic impact on the quality of care and provide long-term improvements in chronic disease management.
Patients with hypertension and diabetes are encouraged to be involved in self-care. Education and the right tools are essential care elements to develop the knowledge and skills needed for self-care. Some of the key change concepts offered in the change package focus heavily on patient education and engagement of patients and their families. Educating and empowering patients to take control is a critical step to improved patient outcomes. This change package offers opportunities at every step of the patient visit.
Monitoring and measuring a change process is what helps to identify the success of the change itself. Reliable practice data that helps to understand the impact of the change is essential to drive improvement.
1. Use Clinical Information Systems 2. Make Chronic Disease a Practice
Priority
1. Use Evidence-based Care
Guidelines 2. Implement A1C Policy 3. Implement Blood Pressure
Policy 4. Use Medication Adjustment
Protocols 5. Integrate Comprehensive
Medication Management 6. Train Staff on Accurate BP
Measurement
1. Refer for Diabetes Self-Management
Education and Support 2. Refer for Self-Measured Blood
Pressure Monitoring 3. Train Staff on Self-Management
Education and Support 4. Support Self-Management Outside
of Office
1. Use Patient Registry for
Population Health Management
2. Use Practice Data to Drive Improvement
Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 9
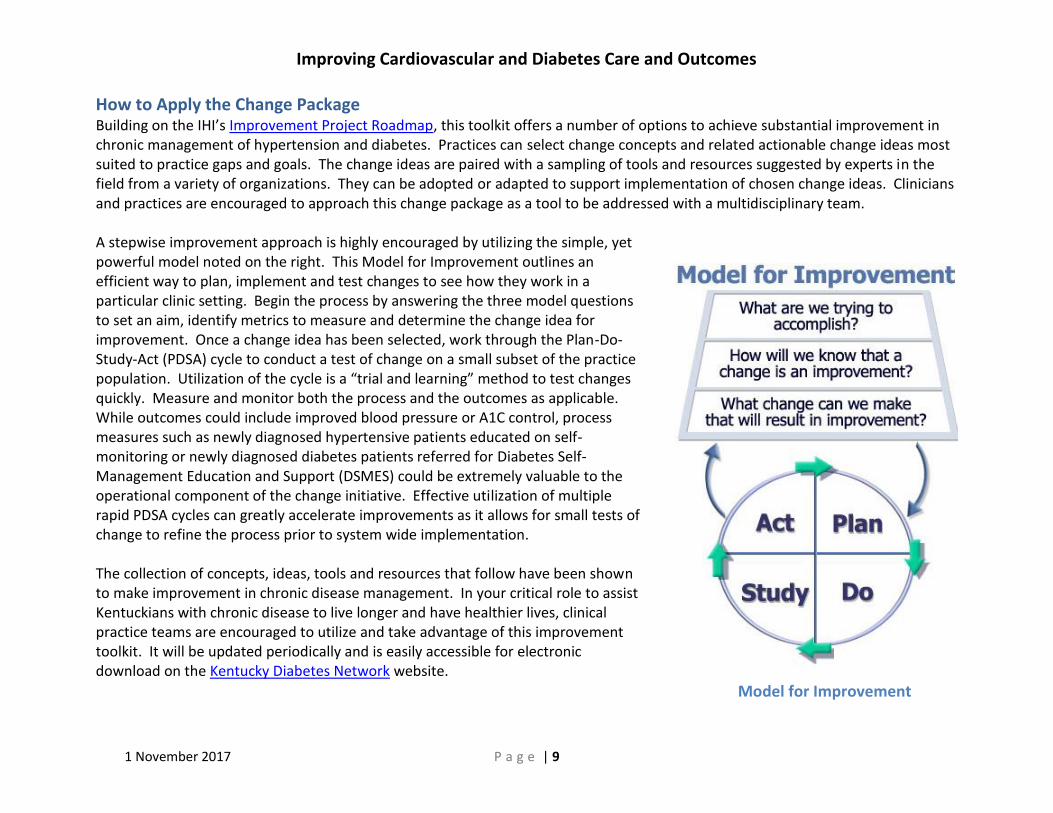
How to Apply the Change Package Building on the IHI’s Improvement Project Roadmap, this toolkit offers a number of options to achieve substantial improvement in chronic management of hypertension and diabetes. Practices can select change concepts and related actionable change ideas most suited to practice gaps and goals. The change ideas are paired with a sampling of tools and resources suggested by experts in the field from a variety of organizations. They can be adopted or adapted to support implementation of chosen change ideas. Clinicians and practices are encouraged to approach this change package as a tool to be addressed with a multidisciplinary team. A stepwise improvement approach is highly encouraged by utilizing the simple, yet powerful model noted on the right. This Model for Improvement outlines an efficient way to plan, implement and test changes to see how they work in a particular clinic setting. Begin the process by answering the three model questions to set an aim, identify metrics to measure and determine the change idea for improvement. Once a change idea has been selected, work through the Plan-Do-Study-Act (PDSA) cycle to conduct a test of change on a small subset of the practice population. Utilization of the cycle is a “trial and learning” method to test changes quickly. Measure and monitor both the process and the outcomes as applicable. While outcomes could include improved blood pressure or A1C control, process measures such as newly diagnosed hypertensive patients educated on self-monitoring or newly diagnosed diabetes patients referred for Diabetes Self-Management Education and Support (DSMES) could be extremely valuable to the operational component of the change initiative. Effective utilization of multiple rapid PDSA cycles can greatly accelerate improvements as it allows for small tests of change to refine the process prior to system wide implementation. The collection of concepts, ideas, tools and resources that follow have been shown to make improvement in chronic disease management. In your critical role to assist Kentuckians with chronic disease to live longer and have healthier lives, clinical practice teams are encouraged to utilize and take advantage of this improvement toolkit. It will be updated periodically and is easily accessible for electronic download on the Kentucky Diabetes Network website.
Model for Improvement

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 10
Operational Efficiency Change Concepts Actionable Ideas
for Change Evidence or Best Practice-Based Resources and Tools Organization / Source
1. Use Clinical Information Systems to Collect Pertinent Patient Information
A. Adopt a robust Electronic Health Record (EHR)
1) Practice Transformation Toolkit Use to implement a new or upgraded electronic health record (EHR) https://www.healthit.gov/providers-professionals/implementation-resources/practice-transformation-toolkit?mc_cid=a3e211a6db&mc_eid=497dbec33a
2) Contract Consultation and Technical Assistance Services for EHR Optimization
http://kentuckyrec.com/
1) Office of the National Coordinator for Health Information Technology
2) Kentucky Regional
Extension Center (Kentucky REC)
2. Make Chronic Disease Management and Control a Practice Priority
A. Designate a Chronic Disease Champion in the practice
1) Cardiovascular Physician Champion Role Description (Kaiser Permanente) Appendix A, page 13 https://millionhearts.hhs.gov/files/HTN_Change_Package.pdf
1) Centers for Disease Control and Prevention/Million Hearts®
B. Establish a core multi-disciplinary chronic disease team including the physician champion to oversee and be accountable for improvement efforts
1) Build an Accountable Diabetes Team Together 2 Goal® Campaign Toolkit, pages 19-32 http://www.together2goal.org/assets/PDF/Toolkit/buildAnAccountableDiabetesTeam.pdf
2) Redesigning the Health Care Team: Diabetes Prevention and Lifelong Management
http://www.niddk.nih.gov/health-information/health-communication-programs/ndep/health-care-professionals/team-care/Pages/publicationdetail.aspx
3) Team Approach to Type 2 Diabetes Management
http://outpatient.aace.com/type-2-diabetes/team-approach
1) American Medical Group Association
2) National Diabetes
Education Program
3) American
Association of Clinical Endocrinologists

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 11
Operational Efficiency Change Concepts Actionable Ideas
for Change Evidence or Best Practice-Based Resources and Tools Organization / Source
4) All Team Members Trained in Importance of BP Goals and Metrics Measure Up Pressure Down Provider Toolkit: Plank 7, pages 65-66 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank7.pdf
5) Team-Based Care to Improve Blood Pressure Control
Task Force Finding and Rationale Statement https://www.thecommunityguide.org/sites/default/files/assets/CVD-Team-Based-Care.pdf
6) Create a Strong Team Culture
STEPSforward CME Module, Downloadable Tools and Implementation Support https://www.stepsforward.org/modules/create-healthy-team-culture
7) Implementing Team-Based Care
STEPSforward, CME Module, Downloadable Tools and Implementation Support https://www.stepsforward.org/modules/team-based-care
4) American Medical Group Association
5) Community
Preventive Services Task Force
6) American Medical
Association 7) American Medical
Association
C. Implement practice-based screening to test high-risk patients and use EHR to identify those already meeting criteria for hypertension and/or type 2 diabetes but lack a diagnosis and/or problem list entry
1) Conduct Practice-Based Screening Together 2 Goal® Campaign Toolkit, pages 49-54 http://www.together2goal.org/assets/PDF/Toolkit/conductPracticeBasedScreening.pdf
1) American Medical Group Association

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 12
Operational Efficiency Change Concepts Actionable Ideas
for Change Evidence or Best Practice-Based Resources and Tools Organization / Source
D. Consider participating in an organized quality improvement initiative with other practices
1) Chronic Disease Pilot on Hypertension and Diabetes Improvement Contact the Kentucky REC for more information about this quality improvement project and resources at http://kentuckyrec.com/contact/
2) Enroll in Together 2 Goal® Campaign
http://www.together2goal.org/Involve/enroll_involve.html
1) Kentucky Regional Extension Center (Kentucky REC)
2) American Medical
Group Association

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 13
Evidence-Based Interventions Change
Concepts
Actionable Ideas for Change
Evidence or Best Practice-Based Resources and Tools Organization / Source
1. Use Evidence-Based Care Guidelines and Treatment Protocols in Systematic Ways
A. Utilize provider reminders or clinical decision support functions in EHRs to remind providers to consistently implement hypertension and diabetes guidelines for care
1) Embed Point-Of-Care-Tools Together 2 Goal® Campaign Toolkit, pages 91-101 http://www.together2goal.org/assets/PDF/Toolkit/embedPointOfCareTools.pdf
2) Standards of Medical Care in Diabetes - 2017
http://professional.diabetes.org/sites/professional.diabetes.org/files/media/dc_40_s1_final.pdf
3) Comprehensive Type 2 Diabetes Management Algorithm - 2017
Pages 228-238 https://www.aace.com/sites/all/files/diabetes-algorithm-executive-summary.pdf
4) Clinical Decision Support (CDS)
How to Implement EHRs https://www.healthit.gov/providers-professionals/clinical-decision-support-cds
5) Perspectives on Hypertension
https://blog.acc.org/post/perspectives-hypertension/ 6) Elements Associated with Effective Adoption and Use of a Protocol
Insights from Key Stakeholders https://millionhearts.hhs.gov/files/MH_Protocol_Implementation.pdf
1) American Medical Group Association
2) American Diabetes Association
3) American Association of Clinical Endocrinologists and American College of Endocrinology
4) The Office of the National Coordinator for Health Information and Technology
5) American College of Cardiology
6) Centers for Disease Control and Prevention / Million Hearts®
Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 14
Evidence-Based Interventions Change
Concepts
Actionable Ideas for Change
Evidence or Best Practice-Based Resources and Tools Organization / Source
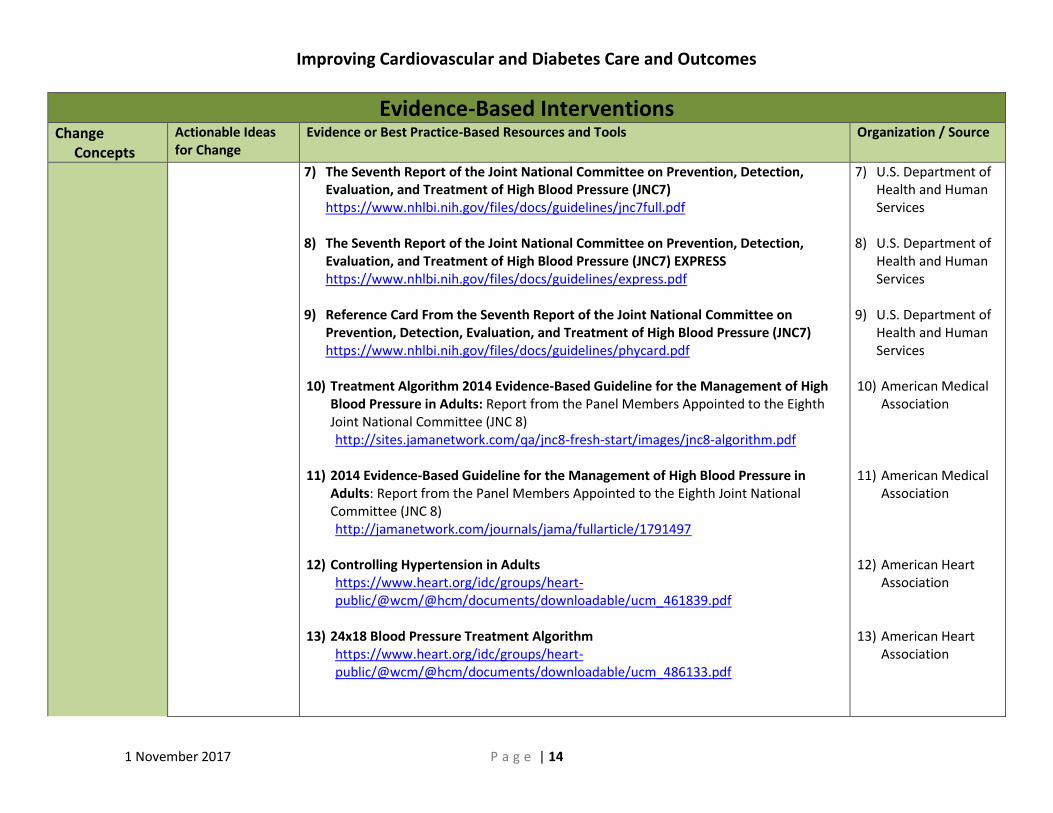
7) The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7) https://www.nhlbi.nih.gov/files/docs/guidelines/jnc7full.pdf
8) The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7) EXPRESS https://www.nhlbi.nih.gov/files/docs/guidelines/express.pdf
9) Reference Card From the Seventh Report of the Joint National Committee on
Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7) https://www.nhlbi.nih.gov/files/docs/guidelines/phycard.pdf
10) Treatment Algorithm 2014 Evidence-Based Guideline for the Management of High
Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) http://sites.jamanetwork.com/qa/jnc8-fresh-start/images/jnc8-algorithm.pdf
11) 2014 Evidence-Based Guideline for the Management of High Blood Pressure in
Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) http://jamanetwork.com/journals/jama/fullarticle/1791497
12) Controlling Hypertension in Adults
https://www.heart.org/idc/groups/heart-public/@wcm/@hcm/documents/downloadable/ucm_461839.pdf
13) 24x18 Blood Pressure Treatment Algorithm
https://www.heart.org/idc/groups/heart-public/@wcm/@hcm/documents/downloadable/ucm_486133.pdf
7) U.S. Department of Health and Human Services
8) U.S. Department of Health and Human Services
9) U.S. Department of Health and Human Services
10) American Medical Association
11) American Medical Association
12) American Heart Association
13) American Heart Association

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 15
Evidence-Based Interventions Change
Concepts
Actionable Ideas for Change
Evidence or Best Practice-Based Resources and Tools Organization / Source
B. Proactively utilize Health Information Technology (HIT) to generate patient data report, registry summary or flow sheet reports for status of guideline implementation for individual patients on a single sheet for a planned visit
1) Embed Point-of-Care-Tools Together 2 Goal® Campaign Toolkit, pages 91-101 http://www.together2goal.org/assets/PDF/Toolkit/embedPointOfCareTools.pdf
2) Diabetes Care Tool
http://www.kydiabetes.net/uploads/pdf/KDN_DM_Care_Tool_2014%20.pdf
1) American Medical Group Association
2) Kentucky Diabetes
Network
C. Deploy detailed protocols and algorithms to facilitate treating to target and intensifying therapy for hypertension and diabetes
1) Adopt Treatment Algorithm Together 2 Goal® Campaign Toolkit, pages 55-70 http://www.together2goal.org/assets/PDF/Toolkit/adoptTreatmentAlgorithm.pdf
2) Pharmacologic Approaches to Glycemic Treatment
Diabetes Care, Standards of Medical Care in Diabetes – 2017, figures 8.1 and 8.2 http://care.diabetesjournals.org/content/40/Supplement_1/S64.figures-only
3) Glycemic Control Algorithm 2017
Page 236 https://www.aace.com/sites/all/files/diabetes-algorithm-executive-summary.pdf
1) American Medical Group Association
2) American Diabetes
Association 3) American
Association of Clinical Endocrinologists

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 16
Evidence-Based Interventions Change
Concepts
Actionable Ideas for Change
Evidence or Best Practice-Based Resources and Tools Organization / Source
4) Evidence-based Treatment Protocols Cholesterol Management and Hypertension Treatment https://millionhearts.hhs.gov/tools-protocols/protocols.html
5) New York Develops Clinical Pathway to Identify and Manage Adult Hypertension
Million Hearts® Success Story. http://www.hcnny.org/WhitneyYoung_HTNProtocol.pdf
4) Million Hearts® 5) Centers for Disease
Control and Prevention / Association of State and Territorial Health Officials
D. Overcome treatment inertia
1) Blood Pressure Addressed for Every Hypertension Patient at Every Primary Care or Cardiology Visit Measure Up Pressure Down Provider Toolkit: Plank 3, pages 35-36 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank3.pdf
1) American Medical Group Association
E. Manage resistant hypertension effectively
1) Resistant Hypertension http://www.jabfm.org/content/25/4/487.full.pdf
2) Resistant Hypertension http://www.fpnotebook.com/cv/Htn/RstntHyprtnsn.htm
1) Journal of the American Board of Family Medicine
2) Family Practice
Notebook
F. Establish standing orders or diabetes order sets that can be initiated by non-physician staff members to facilitate A1C testing and
1) Measure HbA1c Every 3-6 Months Together 2 Goal® Campaign Toolkit, pages 71-72 http://together2goal.org/assets/PDF/Toolkit/measureHbA1cEvery3To6Months.pdf
2) Pre-Visit Laboratory Testing
STEPSforward, CME Module, Downloadable Tools and Implementation Support https://www.stepsforward.org/modules/pre-visit-laboratory-testing
3) Diabetes Care Standing Orders
http://www.kydiabetes.net/uploads/pdf/Diabetes_Standing_Orders.pdf
1) American Medical Group Association
2) American Medical
Association 3) Kentucky Diabetes
Network

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 17
Evidence-Based Interventions Change
Concepts
Actionable Ideas for Change
Evidence or Best Practice-Based Resources and Tools Organization / Source
other key standards of care
4) Standing Orders for Type 2 Diabetes http://www.migrantclinician.org/toolsource/tool-box/standing-orders-diabetes-care.html
4) Migrant Clinician’s Network
2. Implement a Policy and Process to Measure and Address A1C Every 3-6 Months for Every Patient with Diabetes
A. Develop a flowchart for how patients with diabetes will proactively be tracked and managed
1) Critical Pathway Approach to A1C Control Figure 4.2, page 31 https://www.hrsa.gov/sites/default/files/quality/toolbox/508pdfs/diabetesmodule.pdf
2) Planned Care Visit Workflow
http://www.ihi.org/education/Documents/ProgramMaterials/CDCMillionHeartsBloodPressureProject/PaloAltoMed_PlannedCareVisitWorkflow.pdf
1) Health Resources and Services Administration
2) Institute for
Healthcare Improvement and Palo Alto Medical Foundation
B. Incorporate educational interventions and tools on A1C and knowing the number
1) My Diabetes Care Record Aim for the Green Zone for Your A1C and Other Diabetes Care Goals http://www.kydiabetes.net/images/files/My%20Diabetes%20Care%20Record%20from%20Printer%2012%202015.pdf
2) Know Your A1C Number Poster
Companion piece to My Diabetes Care Record, http://www.kydiabetes.net/images/files/A1C%20Poster%20Final.pdf
1) Kentucky Diabetes Network
2) Kentucky Diabetes
Network
C. Provide blood pressure checks without appointment or co-pay
1) Walk-in Medical Assistant Blood Pressure Check Protocol (Kaiser Permanente) Measure Up Pressure Down Provider Toolkit: Plank 8, pages 81-84 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank8Tool3.pdf
1) American Medical Group Association

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 18
Evidence-Based Interventions Change
Concepts
Actionable Ideas for Change
Evidence or Best Practice-Based Resources and Tools Organization / Source
3. Implement Policy and Processes to Measure and Address Blood Pressure at Every Patient Encounter
A. Develop hypertension control policy and procedures
1) Blood Pressure Addressed for Every Hypertension Patient at Every Primary Care or Cardiology Visit Measure Up Pressure Down Provider Toolkit: Plank 3, pages 35-36 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank3.pdf
2) Blood Pressure Check Visit Policy and Procedure (Kaiser Permanente)
Measure Up Pressure Down Provider Toolkit: Plank 4, pages 1-4 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank4Tool3.pdf
1) American Medical Group Association
2) American Medical
Group Association
B. Leverage local Patient Centered Medical Home (PCMH) activities to help drive comprehensive approach to hypertension management
1) Improving the Screening, Prevention, and Management of Hypertension An Implementation Tool for Clinic Practice Teams, pages 18-33 The Eight Components of the PCMH https://www.healthit.gov/sites/default/files/13_bptoolkit_e13l.pdf
2) Local Coaching and Technical Assistance
The Kentucky REC offers coaching and technical assistance to Kentucky practices and organizations interested in National Committee for Quality Assurance (NCQA) Patient Centered Medical Home and Specialty Practice Recognition. Contact the Kentucky REC for more information at http://kentuckyrec.com/contact/
1) Washington State Department of Health
2) Kentucky Regional
Extension Center (Kentucky REC)
C. Develop a flowchart for how hypertensive patients will be proactively tracked and managed
1) Critical Pathway for Hypertension Control Figure 3.1 https://www.hrsa.gov/quality/toolbox/measures/hypertension/part3.html
2) Planned Care Visit Workflow (can be adapted for blood pressure control)
http://www.ihi.org/education/Documents/ProgramMaterials/CDCMillionHeartsBloodPressureProject/PaloAltoMed_PlannedCareVisitWorkflow.pdf
1) Health Resources and Services Administration
2) Institute for Healthcare Improvement

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 19
Evidence-Based Interventions Change
Concepts
Actionable Ideas for Change
Evidence or Best Practice-Based Resources and Tools Organization / Source
D. Contact patients to confirm upcoming appointments; instruct them to bring medications, medication list, and home blood pressure readings; tell them to take medications as instructed on day of visit; if possible, instruct them on submitting home blood pressure readings periodically via apps / portal
1) Key Message #1: Building Trust is Critical Improving the Screening, Prevention, and Management of Hypertension: An Implementation Tool for Clinic Practice Teams, page 49 https://www.healthit.gov/sites/default/files/13_bptoolkit_e13l.pdf
1) Washington State Department of Health
E. Design workflows and use tools to ensure that indicated orders / actions occur during the visit
1) Planned Care Visit Workflow Partnering in Self-Management Support: A Toolkit for Clinicians http://www.ihi.org/education/Documents/ProgramMaterials/CDCMillionHeartsBloodPressureProject/PaloAltoMed_PlannedCareVisitWorkflow.pdf
1) Institute for Healthcare Improvement / Palo Alto Medical Foundation

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 20
Evidence-Based Interventions Change
Concepts
Actionable Ideas for Change
Evidence or Best Practice-Based Resources and Tools Organization / Source
F. Provide patient with tools to support their visit agenda and goal setting
1) Action Plan Form http://www.ihi.org/education/Documents/ProgramMaterials/CDCMillionHeartsBloodPressureProject/SelfMgmt_ActionPlan.pdf
2) My Life Check - Life's Simple 7
http://www.heart.org/HEARTORG/Conditions/My-Life-Check---Lifes-Simple-7_UCM_471453_Article.jsp#.WOUAOlIzXbg
3) CARE Collaborative
Contact [email protected]
4) Check. Change. Control. Community Partner Resources http://www.heart.org/HEARTORG/Conditions/More/ToolsForYourHeartHealth/Check-Change-iControli-Community-Partner-Resources_UCM_445512_Article.jsp#.WOUAsFIzXbg
1) Institute for Healthcare Improvement
2) American Heart
Association 3) Kentucky Heart
Disease and Stroke Prevention Program
4) American Heart
Association
G. Measure, document and repeat blood pressure correctly as indicated; flag abnormal readings
1) Clinical Decision Supports (CDS) How to Implement EHRs https://www.healthit.gov/providers-professionals/clinical-decision-support-cds
2) Improving Blood Pressure Control for Patients with Diabetes in 4 Community Health Centers Meaningful Use Case Studies https://www.healthit.gov/providers-professionals/improving-blood-pressure-control-patients-diabetes-4-community-health
1) The Office of the National Coordinator for Health Information and Technology
2) The Office of the National Coordinator for Health Information and Technology

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 21
Evidence-Based Interventions Change
Concepts
Actionable Ideas for Change
Evidence or Best Practice-Based Resources and Tools Organization / Source
H. Use documentation templates to help capture key data such as patient treatment goals, barriers to adherence, etc.
1) Clinical Decision Supports (CDS) How to Implement EHRs https://www.healthit.gov/providers-professionals/clinical-decision-support-cds
2) Morisky Scale (Mercy Clinics, Inc.) Measure Up Pressure Down Provider Toolkit: Plank 4, page 41 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank4Tool1.pdf
1) The Office of the National Coordinator for Health Information and Technology
2) American Medical
Group Association
I. Use protocols to cover proactive outreach or patient reminders driven by registry use and/or in response to patient submitted home blood glucose levels and blood pressure readings
1) Protocol for Uncomplicated Hypertension Registered Nurse Titration of Lisinopril, Hydrochlorothiazide, Atenolol, and Amlodipine https://www.signup4.net/Upload/KAIS13A/PHYE116E/OC%20Standardized%20Protocol%20Nurse%20Clinic.pdf
2) Standing Order
Antihypertensive Initiation and Titration http://www.med.unc.edu/im/files/enhanced-care-files/HTN_Protocol_6.05.pdf
3) Blood Pressure Titration Protocol
Diabetes Planned Visit Notebook https://www.ahrq.gov/professionals/education/curriculum-tools/diabnotebk/diabnotebk212.html
4) Hypertension Standing Orders (Mercy Clinics, Inc.)
Measure Up Pressure Down Provider Toolkit: Plank 4, page 43 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank4Tool2.pdf
1) Kaiser Permanente 2) University of North
Carolina Health Care Center
3) Agency for
Healthcare Research and Quality
4) American Medical
Group Association

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 22
Evidence-Based Interventions Change
Concepts
Actionable Ideas for Change
Evidence or Best Practice-Based Resources and Tools Organization / Source
4. Use Clinician-Managed Protocols for Medication Adjustments and Lifestyle Recommendations
A. Use order sets (e.g., with prompts for medication titration; increase compliance via prescribing from patient insurance formulary, using once daily / fixed dose combinations when possible) and standing orders to support evidence-based and individualized care
1) Standing Orders Diabetes Care (can be adapted for blood pressure control) http://www.migrantclinician.org/toolsource/tool-box/standing-orders-diabetes-care.html
2) All Patients Not at Goal or with New Hypertension Rx Seen within 30 Days
Measure Up Pressure Down Provider Toolkit: Plank 4, page 39 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank4.pdf
3) Hypertension Standing Orders (Mercy Clinics, Inc.)
Measure Up Pressure Down Provider Toolkit: Plank 4, page 43 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank4Tool2.pdf
1) Migrant Health Network
2) American Medical
Group Association
3) American Medical
Group Association
B. Explore ways to incorporate community or onsite pharmacists on the healthcare team
1) The Patient-Centered Medical Home: Integrating Comprehensive Medication Management to Optimize Patient Outcomes, Resource Guide https://www.pcpcc.org/sites/default/files/media/medmanagement.pdf
2) Expert Practices in the Real World
Community Pharmacy and Patient-Centered Comprehensive Medication Management https://ww04.elbowspace.com/secure/20160701102005942203
1) Patient-Centered Primary Care Collaborative
2) Community
Pharmacy Foundation

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 23
Evidence-Based Interventions Change
Concepts
Actionable Ideas for Change
Evidence or Best Practice-Based Resources and Tools Organization / Source
5. Integrate Compre-hensive Medication Management
A. Ensure team is skilled in identifying / promoting patient medication adherence
1) Actions to Improve Medication Adherence Hypertension Control: Action Steps for Clinicians, Table 2 https://millionhearts.hhs.gov/files/MH_HTN_Clinician_Guide.pdf
2) Medication Adherence Time Tool Medication Adherence - Improving Health Outcomes http://www.acpm.org/?MedAdhereTTProviders
3) Medication Adherence Action Kit https://www1.nyc.gov/site/doh/providers/resources/public-health-action-kits-medication-adherence.page
4) Medication Adherence Tools and Tip Sheets https://millionhearts.hhs.gov/tools-protocols/medication-adherence.html
5) Medication Adherence STEPSforward, CME Module, Downloadable Tools and Implementation Support https://www.stepsforward.org/modules/medication-adherence
6) Promoting Medication Adherence in Diabetes https://www.niddk.nih.gov/health-information/health-communication-programs/ndep/health-care-professionals/medication-adherence/Pages/default.aspx
1) Centers for Disease Control and Prevention / Million Hearts®
2) American College of
Preventive Medicine
3) New York City
Department of Health
4) Centers for Disease
Control and Prevention / Million Hearts®
5) American Medical
Association 6) National Institute of
Diabetes and Digestive and Kidney Diseases
B. Assess individual risk and counsel using motivational interviewing
1) ASCVD Risk Estimator http://tools.acc.org/ASCVD-Risk-Estimator/
1) American College of Cardiology / American Heart Association
Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 24
Evidence-Based Interventions Change
Concepts
Actionable Ideas for Change
Evidence or Best Practice-Based Resources and Tools Organization / Source
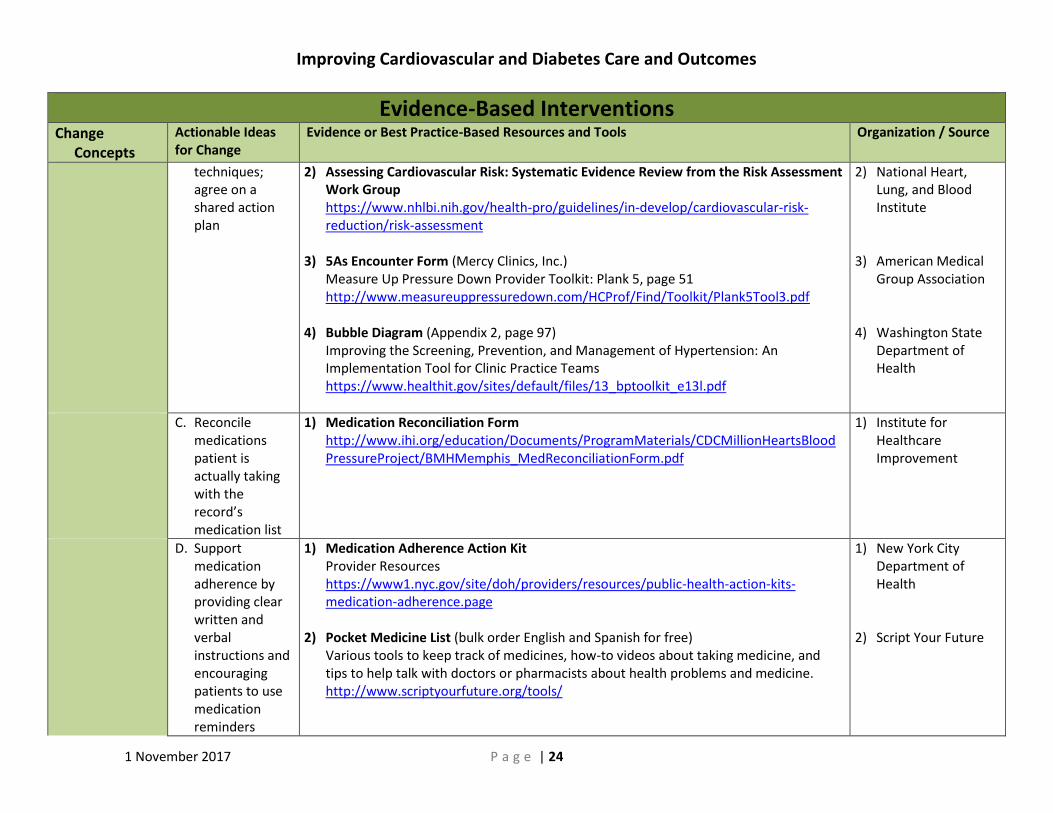
techniques; agree on a shared action plan
2) Assessing Cardiovascular Risk: Systematic Evidence Review from the Risk Assessment Work Group https://www.nhlbi.nih.gov/health-pro/guidelines/in-develop/cardiovascular-risk-reduction/risk-assessment
3) 5As Encounter Form (Mercy Clinics, Inc.)
Measure Up Pressure Down Provider Toolkit: Plank 5, page 51 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank5Tool3.pdf
4) Bubble Diagram (Appendix 2, page 97)
Improving the Screening, Prevention, and Management of Hypertension: An Implementation Tool for Clinic Practice Teams https://www.healthit.gov/sites/default/files/13_bptoolkit_e13l.pdf
2) National Heart, Lung, and Blood Institute
3) American Medical
Group Association
4) Washington State Department of Health
C. Reconcile medications patient is actually taking with the record’s medication list
1) Medication Reconciliation Form http://www.ihi.org/education/Documents/ProgramMaterials/CDCMillionHeartsBloodPressureProject/BMHMemphis_MedReconciliationForm.pdf
1) Institute for Healthcare Improvement
D. Support medication adherence by providing clear written and verbal instructions and encouraging patients to use medication reminders
1) Medication Adherence Action Kit Provider Resources https://www1.nyc.gov/site/doh/providers/resources/public-health-action-kits-medication-adherence.page
2) Pocket Medicine List (bulk order English and Spanish for free)
Various tools to keep track of medicines, how-to videos about taking medicine, and tips to help talk with doctors or pharmacists about health problems and medicine. http://www.scriptyourfuture.org/tools/
1) New York City Department of Health
2) Script Your Future

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 25
Evidence-Based Interventions Change
Concepts
Actionable Ideas for Change
Evidence or Best Practice-Based Resources and Tools Organization / Source
3) Medicines to Help You: High Blood Pressure https://www.fda.gov/downloads/ForConsumers/ByAudience/ForWomen/FreePublications/UCM282311.pdf
3) Food and Drug Administration / Office of Women’s Health
E. Assign staff responsibility for managing refill requests by refill protocol
1) Adult Primary Care Prescription Refill Guidelines for Ambulatory Services https://www.utmb.edu/policies_and_procedures/IHOP/Supporting_Documents/IHOP%20-%2009.11.05%20-%20Physician%20Orders%20(Adult%20Primary%20Care%20Prescription%20Refill%20Guidelines%20for%20Ambulatory%20Services).pdf
2) Use of Condition Specific Protocols: Frequently Asked Questions (FAQ)
https://mn.gov/boards/nursing/practice/faqs/use-condition-protocols-faq.jsp
3) Synchronized Medication Renewal CME Module, Downloadable Tools and Implementation Support https://www.stepsforward.org/modules/synchronized-prescription-renewal
1) University of Texas Medical Branch
2) Minnesota Board of
Nursing 3) American Medical
Association
F. Implement frequent follow-ups (e.g., e-mail, phone calls, text messages) with patients to make sure they are continuing their medication
No resource or tool for actionable idea for change
Not Applicable
G. Provide guidance on measuring
1) Checking Blood Pressures Nursing Competency (Sharp Rees-Stealy Medical Group) Measure Up Pressure Down Provider Toolkit: Plank 1, page 25-27 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank1Tool2.pdf
1) American Medical Group Association

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 26
Evidence-Based Interventions Change
Concepts
Actionable Ideas for Change
Evidence or Best Practice-Based Resources and Tools Organization / Source
blood pressure accurately
2) Correct Blood Pressure Measurement Technique Handout (Colorado Springs Health Partners) Measure Up Pressure Down Provider Toolkit: Plank 1, page 1 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank1Tool5.pdf
3) Standard Work Form, Blood Pressure Measurement in the Clinic (Park Nicollet) Measure Up Pressure Down Provider Toolkit: Plank 8, page 1 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank8Tool6.pdf
4) Standard Work Form, Automatic Omron Blood Pressure Measurement (Park Nicollet)
Measure Up Pressure Down Provider Toolkit: Plank 8, page 1 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank8Tool5.pdf
5) Blood Pressure Accuracy and Variability Quick Reference (HealthPartners)
Measure Up Pressure Down Provider Toolkit: Plank 1, pages 1-2 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank1Tool11.pdf
2) American Medical Group Association
3) American Medical
Group Association 4) American Medical
Group Association 5) American Medical
Group Association

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 27
Evidence-Based Interventions Change
Concepts
Actionable Ideas for Change
Evidence or Best Practice-Based Resources and Tools Organization / Source
6. Train and Evaluate Direct Care Staff on Accurate BP Measurement and Recording
A. Assess adherence to proper blood pressure measurement technique
1) Competency Checklist Blood Pressure Measurement (Cleveland Clinic) Measure Up Pressure Down Provider Toolkit: Plank 1, page 1 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank1Tool3.pdf
2) Blood Pressure Spot Check (Kaiser Permanente)
Measure Up Pressure Down Provider Toolkit: Plank 4, pages 1-2 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank4Tool4.pdf
3) New Employee Blood Pressure Measurement Initial Competency Checklist (HealthPartners) Measure Up Pressure Down Provider Toolkit: Plank 1, page 1 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank1Tool8.pdf
4) Quarterly Blood Pressure Auditing Tool (HealthPartners)
Measure Up Pressure Down Provider Toolkit: Plank 1, page 1 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank1Tool10.pdf
1) American Medical Group Association
2) American Medical
Group Association
3) American Medical Group Association
4) American Medical
Group Association

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 28
Patient Self-Management Change Concepts Actionable Ideas
for Change Evidence or Best Practice-Based Resources and Tools Organization / Source
1. Empower Patients with Knowledge and Skills for Self-Management – Refer for Diabetes Self-Management Education and Support (DSMES)
A. Educate providers and staff about the effectiveness and availability of DSMES program and referral process
1) Effectiveness of Diabetes Self-Management Education and Support (DSMES) Recorded 18-Minute-Long Recorded Webinar https://kyrec.webex.com/kyrec/lsr.php?RCID=72247a5bd3aaf3f082226c1135b25aae
2) Refer to DSMES and Support Programs
Together 2 Goal® Campaign Toolkit, pages 45-48 http://www.together2goal.org/assets/PDF/Toolkit/referToDSMEAndSupportPrograms.pdf
3) Supporting You, Empowering Your Patients
https://www.diabeteseducator.org/docs/default-source/legacy-docs/_resources/pdf/general/ProviderBrochure_Downloadable_Final.pdf
1) Kentucky Diabetes Prevention and Control Program and Kentucky REC
2) American Medical
Group Association 3) American
Association of Diabetes Educators
B. Adopt policies to focus initial DSMES referrals on four critical times: at diagnosis, on an annual basis as needed, when new complicating factors influence self-management and during transitions of care
1) Diabetes Self-Management Education and Support Algorithm for Adults with Type 2 Diabetes: Algorithm of Care https://www.diabeteseducator.org/docs/default-source/practice/algorithm-of-care.pdf?sfvrsn=2
2) Diabetes Self-Management Education and Support for Adults with Type 2 Diabetes:
Algorithm Action Steps https://www.diabeteseducator.org/docs/default-source/practice/algorithm-action-steps.pdf?sfvrsn=2
1) American Diabetes Association, the American Association of Diabetes Educators, and the Academy of Nutrition and Dietetics
2) American Diabetes
Association, the American Association of Diabetes Educators, and the Academy of Nutrition and Dietetics

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 29
Patient Self-Management Change Concepts Actionable Ideas
for Change Evidence or Best Practice-Based Resources and Tools Organization / Source
3) Diabetes Care Standing Orders http://www.kydiabetes.net/uploads/pdf/Diabetes_Standing_Orders.pdf
4) Standing Orders for Diabetes Care
http://www.migrantclinician.org/toolsource/tool-box/standing-orders-diabetes-care.html
3) Kentucky Diabetes Network
4) Migrant Clinician’s
Network
C. Identify nationally “recognized” or “accredited” DSMES programs or other DSMES classes offered in your service area and establish a DSMES program referral list
1) Kentucky Diabetes Resource Directory Listings of recognized or accredited or other Diabetes Self-Management Education and Support (DSMES) programs which can be queried by county and/or adjacent counties. https://prd.chfs.ky.gov/KYDiabetesResources/Search.aspx
2) Diabetes Education Accredited Programs/Branches
https://nf01.diabeteseducator.org/eweb/DynamicPage.aspx?Site=aade&WebCode=DEAPFindApprovedProgram
3) Recognized Diabetes Education Programs Listing
http://professional.diabetes.org/erp_list_zip
1) Kentucky Diabetes Prevention and Control Program
2) American
Association of Diabetes Educators
3) American Diabetes
Association
D. Develop an efficient, systematic DSMES referral process with communication back from the educational program regarding attendance and goal setting,
1) Diabetes Services Order Form - Diabetes Self-Management Training (DSMT) and Medical Nutrition Therapy (MNT) Services Meets requirements set forth by Medicare and most insurance companies. https://www.diabeteseducator.org/docs/default-source/default-document-library/diabetes-services-order-form7e32db36a05f68739c53ff0000b8561d.pdf?sfvrsn=0
2) Example Diabetes Self-Management Education and Support (DSMES) Referral Form
http://professional.diabetes.org/sites/professional.diabetes.org/files/media/erp-sample-referral-short.pdf
1) American Association of Diabetes Educators
2) American Diabetes
Association

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 30
Patient Self-Management Change Concepts Actionable Ideas
for Change Evidence or Best Practice-Based Resources and Tools Organization / Source
etc. (e.g., referral, prescription pad, referral forms, etc.)
E. Assign a staff member to be a key contact to work with DSMES provider agencies
1) Refer to DSMES and Support Programs Together 2 Goal® Campaign Toolkit, pages 45-48 http://www.together2goal.org/assets/PDF/Toolkit/referToDSMEAndSupportPrograms.pdf
1) American Medical Group Association
F. Explore ways to reduce or remove barriers to participation in DSMES classes such as lack of transportation, cost of service, language barriers, health literacy, etc.
1) Local Resources Use resources within community to mitigate the obstacles.
2) Local Diabetes Self-Management Education and Support (DSMES) Providers
Check with local DSMES providers to see if there are sliding scale or scholarship options. Some local health departments offer the service without charge.
1) Not Applicable 2) Not Applicable
G. Educate patients and their family members about the importance of developing self-management skills and how
1) Importance of DSMES Infographic Customizable to add Local DSMES Program Name http://www.kydiabetes.net/images/files/DSME%20Infographic%20fill%20in%202017.pdf
2) Importance of DSMES Infographic
Kentucky Diabetes Resource Directory for DSMES Availability http://www.kydiabetes.net/images/files/DSME%20Infographic%20with%20KDPCP%20Logo%20CA.pdf
1) Kentucky Diabetes Network
2) Kentucky Diabetes
Network

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 31
Patient Self-Management Change Concepts Actionable Ideas
for Change Evidence or Best Practice-Based Resources and Tools Organization / Source
DSMES can help
2. Empower Patients with Knowledge and Skills for Self-Management – Refer for Self-Measured Blood Pressure Monitoring (SMBP).
A. Support blood pressure self-monitoring: advise on choosing device / cuff size, check device for accuracy, train patient on use, provide BP logs (electronic / paper / portal)
1) How to Check Your Blood Pressure 8.5x5.5 booklets come in English & Spanish http://1.usa.gov/1nTAImf
2) Blood Pressure Tracking Card and Action Plan
http://www1.nyc.gov/assets/doh/downloads/pdf/csi/hyperkit-pt-bptrack-passport.pdf
3) My Blood Pressure Wallet Card
https://www.nhlbi.nih.gov/files/docs/public/heart/hbpwallet.pdf 4) Blood Pressure Tracking Card (Arch Health Partners)
Measure Up Pressure Down Provider Toolkit: Plank 4, pages 1-2 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank5Tool9.pdf
5) Blood Pressure Measurement Instructions
http://www.heart.org/idc/groups/heart-public/@wcm/@hcm/documents/downloadable/ucm_445846.pdf
6) Consequences of High Blood Pressure
http://www.localheart.org/idc/groups/heart-public/@wcm/@cmc/documents/downloadable/ucm_465197.pdf
7) Understanding and Managing High Blood Pressure
https://www.heart.org/idc/groups/heart-public/@wcm/@hcm/documents/downloadable/ucm_461840.pdf
1) Washington State Department of Health
2) New York City
Department of Health
3) National Heart,
Lung, and Blood Institute / Million Hearts®
4) American Medical
Group Association 5) American Heart
Association 6) American Heart
Association 7) American Heart
Association

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 32
Patient Self-Management Change Concepts Actionable Ideas
for Change Evidence or Best Practice-Based Resources and Tools Organization / Source
3. Equip Direct Care Staff to Facilitate Patient Self-Management Education and Support
A. Facilitate access to opportunities to acquire the latest core cardiovascular / diabetes knowledge and to build / strengthen self-management support skills (e. g., professional education, motivational interviewing, setting self-management goals, etc.)
1) Licensed Health Professions: ABCs of Diabetes Education and Facilitating Behavior Change https://nf01.diabeteseducator.org/eweb/DynamicPage.aspx?WebCode=OnlineCourse&pager=10
2) Health Educators and Certified Medical Assistants: Diabetes Paraprofessional Level 2
Course https://www.diabeteseducator.org/education-career/career-path-certificate/associate-level-2
3) Community Health Workers: Diabetes Paraprofessional Level 1 Course
https://www.diabeteseducator.org/education-career/career-path-certificate/associate-level-1
4) Community Health workers and Chronic Disease Training:
www.chwtraining.mcdph.org 5) Cardiovascular Assessment, Risk Reduction, and Education (CARE) Collaborative
Contact [email protected] 6) Partnering in Self-Management Support: A Toolkit for Clinicians
http://www.ihi.org/education/Documents/ProgramMaterials/CDCMillionHeartsBloodPressureProject/NHP_PartneringinSelfMgmtSupport_ToolkitforClinicians_2011_CDCMillionHearts.pdf
7) Target: BP™ Fact Sheet
http://www.heart.org/idc/groups/heart-public/@wcm/@mwa/documents/downloadable/ucm_482030.pdf
1) American Association of Diabetes Educators
2) American
Association of Diabetes Educators
3) American
Association of Diabetes Educators
4) Montgomery
County District Public Health
5) Kentucky Heart
Disease and Stroke Prevention Program
6) Institute for
Healthcare Improvement
7) American Heart
Association

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 33
Patient Self-Management Change Concepts Actionable Ideas
for Change Evidence or Best Practice-Based Resources and Tools Organization / Source
B. Consider attending Diabetes Self-Management Education and Support (DSMES) classes provided in your service area
1) Kentucky Diabetes Resource Directory https://prd.chfs.ky.gov/KYDiabetesResources/Search.aspx
1) Kentucky Diabetes Prevention and Control Program
C. Identify a few patient educational materials and tools to help with key self-management information and setting self-management goals: blood pressure, salt intake, exercise, and smoking
1) What is Diabetes? A variety of low literacy materials on key self-care behaviors from various sources http://www.kydiabetes.net/what_is_diabetes.html
2) Tools for Patients with Diabetes Diabetes and nutrition basics booklets as well as other items (English and Spanish versions available). http://chfs.ky.gov/dph/info/dpqi/cd/PatTools.htm
3) Healthy Living with Diabetes Tool for Setting Self-Management Goals
http://www.kydiabetes.net/images/files/DSME%20Plan%20Goal%20Setting%2016%20with%20Logo%20(2).pdf
4) Patient Education Library
http://professional.diabetes.org/search/site?f%5B0%5D=im_field_dbp_ct%3A32&retain-filters=1
5) Diabetes Tip Sheets
https://www.diabeteseducator.org/patient-resources/tip-sheets-and-handouts 6) 4 Steps to Manage Your Diabetes for Life
http://www.cdc.gov/diabetes/ndep/pdfs/97-ndep67-4steps-4c-508.pdf
1) Kentucky Diabetes Network
2) Kentucky Diabetes
Prevention and Control Program
3) Kentucky Diabetes
Prevention and Control Program
4) American
Association of Diabetes Educators
5) American
Association of Diabetes Educators
6) National Diabetes
Education Program

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 34
Patient Self-Management Change Concepts Actionable Ideas
for Change Evidence or Best Practice-Based Resources and Tools Organization / Source
7) Know Your Blood Pressure Numbers http://here.doh.wa.gov/materials/know-your-numbers/13_BPnosPst2_E15L.pdf
8) What’s the Big Deal about Controlling My Blood Pressure?
http://here.doh.wa.gov/materials/control-blood-pressure/13_BPbgPst_E15L.pdf 9) Know the Facts About High Blood Pressure
https://www.cdc.gov/bloodpressure/docs/consumered_hbp.pdf
10) Reducing Sodium in the Diet to Help Control Your Blood Pressure https://www.cdc.gov/salt/pdfs/Reducing_Sodium_Diet_BP_Control.pdf
11) Your Guide to Lowering Blood Pressure https://www.nhlbi.nih.gov/files/docs/public/heart/hbp_low.pdf
7) Washington State Department of Health
8) Washington State Department of Health
9) Centers for Disease
Control and Prevention
10) Centers for Disease
Control and Prevention
11) U.S. Department of
Health and Human Services
D. Consider starting a recognized Diabetes Self-Management Education and Support (DSMES) program
1) AADE Diabetes Education Accreditation Program https://www.diabeteseducator.org/practice/diabetes-education-accreditation-program-(deap)
2) Education Recognition Program
http://professional.diabetes.org/diabetes-education
1) American Association of Diabetes Educators
2) American Diabetes
Association
E. Establish a program to support home blood pressure monitoring
1) Self-Measured Blood Pressure Monitoring: Action Steps for Clinicians https://millionhearts.hhs.gov/files/MH_SMBP_Clinicians.pdf
1) Centers for Disease Control and Prevention / Million Hearts®

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 35
Patient Self-Management Change Concepts Actionable Ideas
for Change Evidence or Best Practice-Based Resources and Tools Organization / Source
4. Support Patients In Hypertension or Diabetes Self-Management During Their Routine Daily Activities (e.g., Not Related to Any Specific Visit)
A. Use an online patient portal or other approaches so that patients can access tools, information and practice staff outside face-to-face encounters to address home measured blood pressure readings and blood glucose monitoring values or trends and other needs
1) What is a Patient Portal? https://www.healthit.gov/providers-professionals/faqs/what-patient-portal
1) The Office of the National Coordinator for Health Information Technology and National Learning Consortium
B. Ensure that the self-management support provided to patients is helpful in their daily routine (e.g. when making food and lifestyle choices)
1) Diabetes Self-Management Support (DSMS) Plan http://c.ymcdn.com/sites/www.ncchca.org/resource/resmgr/imported/DSMS.pdf
2) My Diabetes Self-Management Support Plan
http://professional.diabetes.org/sites/professional.diabetes.org/files/media/erp-sample-DSMS-plan.pdf
3) Partnering in Self-Management Support: A Toolkit for Clinicians
http://www.ihi.org/resources/pages/tools/selfmanagementtoolkitforclinicians.aspx
1) Adapted from Hope National Diabetes Center
2) American Diabetes
Association 3) Institute for Health
Care Improvement

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 36
Patient Self-Management Change Concepts Actionable Ideas
for Change Evidence or Best Practice-Based Resources and Tools Organization / Source
C. Establish linkages with community organizations delivering self-management education support programs
1) Kentucky Diabetes Resource Directory Listings of diabetes support groups and other self-management support resources which can be queried by county and/or adjacent counties. https://prd.chfs.ky.gov/KYDiabetesResources/Search.aspx
1) Kentucky Diabetes Prevention and Control Program
D. Support medication adherence by providing clear written and verbal instructions and encouraging patients to use medication reminders
1) Medication Adherence Action Kit Provider Resources https://www1.nyc.gov/site/doh/providers/resources/public-health-action-kits-medication-adherence.page
2) Pocket Medicine List (bulk order English and Spanish for free)
Various tools to keep track of medicines, how-to videos about taking medicine, and tips to help talk with doctors or pharmacists about health problems and medicine. http://www.scriptyourfuture.org/tools/
3) Medicines to Help You: High Blood Pressure
https://www.fda.gov/downloads/ForConsumers/ByAudience/ForWomen/FreePublications/UCM282311.pdf
1) New York City Department of Health
2) Script Your Future 3) Food and Drug
Administration / Office of Women’s Health
E. Provide patients with a written self-management plan, visit summary, and follow-up guidance at the end of each visit
1) 5As Encounter Form (Mercy Clinics, Inc.) Measure Up Pressure Down Provider Toolkit: Plank 5, page 51 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank5Tool3.pdf
2) Providing Patients in Ambulatory Care Settings with a Clinical Summary of the Office
Visit http://www.nihb.org/hitech/docs/08162013/Provider_Clinical_Summary_fact_sheet.pdf
1) American Medical Group Association
2) The Office of the
National Coordinator for Health Information and Technology

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 37
Patient Self-Management Change Concepts Actionable Ideas
for Change Evidence or Best Practice-Based Resources and Tools Organization / Source
3) Patient Participation Handouts - English (Sharp Rees-Stealy Medical Group) Measure Up Pressure Down Provider Toolkit: Plank 5, pages 59-62 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank5Tool7.pdf
4) Action Plan Form http://www.ihi.org/education/Documents/ProgramMaterials/CDCMillionHeartsBloodPressureProject/SelfMgmt_ActionPlan.pdf
3) American Medical Group Association
4) Institute for Healthcare Improvement

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 38
Data Driven Quality Improvement Change Concepts Actionable Ideas
for Change Evidence or Best Practice-Based Resources and Tools Organization / Source
1. Use Patient Registry to Identify, Track and Manage the Population of Patients with Hypertension and Diabetes
A. Implement a hypertension and/or diabetes patient registry
1) Registry Used to Track Hypertension Patients Measure Up Pressure Down Provider Toolkit: Plank 6, pages 63-64 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank6.pdf
2) Use a Patient Registry
Together 2 Goal® Campaign Toolkit pages 89-90 http://www.together2goal.org/assets/PDF/Toolkit/useAPatientRegistry.pdf
3) Implementing a Point-of-Care Registry
STEPSforward, CME Module, Downloadable Tools and Implementation Support https://www.stepsforward.org/modules/point-of-care-registry
4) Provider Toolkit - Population Health Management & Registries
https://www.anthem.com/wps/portal/ahpprovider?content_path=provider/noapplication/f1/s0/t0/pw_e191222.htm&label=Provider%20Toolkit%20%E2%80%93%20Population%20Health%20Management%20%5E%20Registries&state=va
5) Diabetes Registries
http://ndep.nih.gov/hcp-businesses-and-schools/practice-transformation/information-systems/population-health.aspx
6) Population Health Management Software:
An Opportunity to Advance Primary Care and Public Health Integration http://phii.org/sites/www.phii.org/files/resource/files/Population%20Health%20Management%20Software%20Report.pdf
7) Computerized Disease Registries
https://healthit.ahrq.gov/key-topics/computerized-disease-registries
1) American Medical Group Association
2) American Medical
Group Association 3) American Medical
Association 4) Anthem BlueCross
BlueShield 5) National Institute of
Health 6) Public Health
Informatics Institute 7) Agency for
Healthcare Research and Quality

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 39
Data Driven Quality Improvement Change Concepts Actionable Ideas
for Change Evidence or Best Practice-Based Resources and Tools Organization / Source
B. Identify patients due or overdue for tests and exams or have uncontrolled hypertension ≥140/90 and/or diabetes (A1C > 9% may be starting point)
1) Undiagnosed Hypertension Find patients in your practice with undiagnosed hypertension who may be "hiding in plain sight". https://millionhearts.hhs.gov/tools-protocols/hiding-plain-sight/index.html
2) Use a Patient Registry
Together 2 Goal® Campaign Toolkit pages 89-90 http://www.together2goal.org/assets/PDF/Toolkit/useAPatientRegistry.pdf
3) Contact Patients Not at Goal and with Therapy Change within 30 Days
Together 2 Goal® Campaign Toolkit pages 85-88 http://www.together2goal.org/assets/PDF/Toolkit/contactPatientsNotAtGoalAndWithTherapyChangeWithin30Days.pdf
1) American Heart Association / Million Hearts®
2) American Medical
Group Association 3) American Medical
Group Association
C. Use a defined process for outreach (e.g. via phone, mail, email, text) to patients with uncontrolled hypertension and/or diabetes, those who are not up-to-date on recommended tests, self-management knowledge / skills and otherwise
1) Hypertension Recall Instructions (Redwood Community Health Coalition) page 14, Appendix B, Hypertension Control Change Package for Clinicians https://millionhearts.hhs.gov/files/HTN_Change_Package.pdf
2) Quality Improvement in a Primary Care Practice
Meaningful Use Case Studies https://www.healthit.gov/providers-professionals/quality-improvement-primary-care-practice
3) Contact Patients Not at Goal and with Therapy Change within 30 Days
Together 2 Goal® Campaign Toolkit, pages 85-88 http://together2goal.org/assets/PDF/Toolkit/contactPatientsNotAtGoalAndWithTherapyChangeWithin30Days.pdf
1) Centers for Disease Control and Prevention / Million Hearts®
2) The Office of the
National Coordinator for Health Information Technology
3) American Medical
Group Association

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 40
Data Driven Quality Improvement Change Concepts Actionable Ideas
for Change Evidence or Best Practice-Based Resources and Tools Organization / Source
needing follow-up
2. Use Practice Data to Drive Improvement
A. Determine cardiovascular and diabetes clinical quality measures / metrics for the practice (A1C poor control of >9 and blood pressure control of <140/90 are a good starting point and align with multiple quality measurement sets)
1) 2017 Merit-based Incentive Payment System Quality Measures https://qpp.cms.gov/measures/quality
2) Healthcare Effectiveness Data and Information Set (HEDIS) Comprehensive Diabetes
Care http://www.ncqa.org/hedis-quality-measurement/hedis-measures
3) Measures, Reports & Tools
http://www.qualityforum.org/measures_reports_tools.aspx 4) Specifications Hypertension Measures
http://www.hcnny.org/HCNNY_HTNMeasureSpecs.pdf 5) Reference Card From the Seventh Report of the Joint National Committee on
Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7) https://www.nhlbi.nih.gov/files/docs/guidelines/phycard.pdf
6) 2014 Hypertension Guideline Management Algorithm
From 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) http://sites.jamanetwork.com/qa/jnc8-fresh-start/images/jnc8-algorithm.pdf
1) Quality Payment Program, Centers for Medicare and Medicaid
2) National Committee
for Quality Assurance
3) National Quality
Forum 4) Health Center
Network of New York
5) U.S. Department of
Health and Human Services
6) American Medical
Association

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 41
Data Driven Quality Improvement Change Concepts Actionable Ideas
for Change Evidence or Best Practice-Based Resources and Tools Organization / Source
B. Regularly provide assessment and feedback dashboard or scorecard for the practice and for individual providers as compared to other providers in practice with metric baseline, target and performance.
1) Physician Quality Report Card (Cleveland Clinic) Measure Up Pressure Down Provider Toolkit: Plank , page 73 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank7Tool4.pdf
2) Publish Transparent Internal Reports Together 2 Goal® Toolkit, pages 103-110 http://www.together2goal.org/assets/PDF/Toolkit/publishTransparentInternalReports.pdf
3) Quality Improvement Scorecard Example An example template that could be utilized for an organization, clinic or individual provider. http://www.kydiabetes.net/images/files/QI%20Monthly%20Scorecard%20Example.pdf
4) HTN Report (Kaiser Permanente—Mid Atlantic States) Measure Up Pressure Down Provider Toolkit: Plank 7, page 67 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank7Tool1.pdf
5) Quarterly Status Report (Kaiser Permanente—Mid Atlantic States)
Measure Up Pressure Down Provider Toolkit: Plank 7, page 71 http://www.measureuppressuredown.com/HCProf/Find/Toolkit/Plank7Tool3.pdf
1) American Medical Group Association
2) American Medical
Group Association
3) Juniper Health, Inc. 4) American Medical
Group Association 5) American Medical
Group Association

Improving Cardiovascular and Diabetes Care and Outcomes
1 November 2017 P a g e | 42
This page intentionally left blank.