improved yields of factor viii from heparinized plasma
TRANSCRIPT
Vox Sang. 36: 294-300 (1979)
Improved Yields of Factor VIII from Heparinized Plasma
G. A . Rock, W . H . Cruickshank, E. S . Tackaberry and D. S . Palmer The Canadian Red Cross and Faculty of Medicine, University of Ottawa, Ottawa, Ont.
Abstract. The Factor VIII procoagulant activity in plasma, cryoprecipitate, and their poly- ethylene glycol (PEG) precipitates is markedly increased if blood is collected into heparin rather than into citrate phosphate dextrose (CPD). There is a 34% increase in the initial level of the Factor VIII activity in the heparinized plasma with 78% of this initial activity (184 U) recovered in the cryoprecipitate. As well, the stability of the Factor VIII activity is improved: after 24 h of incubation at 22"C, 99% of the initial activity is retained in heparinized plasma whereas only 64% remains in CPD plasma. The cryoprecipitate prepared from heparinized plasma is equally stable after 24 h. The PEG concentrate prepared from the cryoprecipitate of heparinized plasma is increased to 128 U compared to only 54 U from CPD plasma. Rel- ative recoveries were 531 U/1 for heparinized plasma versus 215 U/1 for CPD plasma. This represents a 147% increase in yield.
Introduction
A major advance in the clinical treatment of hemophilia A occurred with the discovery that the cold insoluble fraction, or cryopre- cipitate, of thawed plasma was rich in Fac- tor VIII and could be conveniently produced for infusion using a closed system (6). Al- though this material provided a means of administering high doses of Factor VIII, it contained large amounts of other plasma proteins, particularly fibrinogen. Efforts were subsequently made to obtain more highly purified Factor VIII concentrates from cryoprecipitate. Generally, these were
precipitation techniques employing ethanol (4), polyethylene glycol (PEG) (9, or gly- cine (2). Although these procedures yield more potent Factor VIII concentrates, the final overall recovery is relatively poor, lead- ing to the loss of a therapeutically useful product, and making the cost per unit of Factor VIII recovered quite high.
The poor recovery of Factor VIII is due, in part, to the marked instability of the Fac- tor VIII molecule (12, 14). This is charac- terized by a biphasic decay curve in which 20-30% of the initial activity is lost during the first few hours with the remaining activi- ty stable for up to 100 h (13). The recovery

Yields of Factor VIII from Heparinized Plasma 295
of Factor VIII activity is also significantly affected by pH. When collecting blood into citrate phosphate dextrose (CPD) or acid citrate dextrose (ACD) solutions which have pH values below 5.8, there is a loss of 10% of the starting activity during the collection procedure (13).
A further loss of Factor VIII activity oc- curs during the process of cryoprecipitation. While the recovery of Factor VIII depends on the original concentration in the plasma (7,13), a value of 55+13% of the initial activity appears to be a representative re- covery in the cryoprecipitate from CPD plas- ma (3). Approximately 20% of the activity is left in the cryosupernatant with the re- maining 25% not accounted for.
We have recently shown that the presence of calcium markedly affects the molecular organization of the Factor VIII molecule with relatively more low molecular weight procoagulant activity detectable in the pres- ence of calcium (10). Since the molecular organization of Factor VIII is known to af- fect its cryoprecipitability ( 1 3 , we wished to examine the Factor VIII recovery in plas- ma and cryoprecipitate when physiological levels of calcium were maintained through- out the blood collection period. .Heparin was the anticoagulant chosen for this purpose since it inhibits clot formation by preventing the action of thrombin, but leaves the ionic composition of the plasma unaltered.
Methods
Collection of Blood. Blood was collected from random male donors into standard Fenwal blood bags which contained either sodium heparin (3-4 USP unitdm1 whole blood) or CPD as anticoagu- lant. To obtain a direct comparison of Factor VIII recovery in different anticoagulants, it was neces-
sary to first eliminate the possibility of individual variation in starting plasma Factor VIII levels. Therefore, three separate plasma pools were made by simultaneously collecting blood from three separate donors with each donor contributing one- third of a unit of blood (130cms) into each of three separate bags. This produced bags of blood of identical origin, and identical volume, but col- lected into different anticoagulant solutions. Red blood cells were separated from plasma by centrif- ugation and the plasma was decanted and either used immediately or stored at -80 O C .
Stability Study. To test the stability of Fac- tor VIII, blood samples were taken from each of 6 individual donors into separate tubes containing CPD, CPD plus heparin, or heparin alone. Follow- ing centrifugation, the plasmas were separated and kept at 22OC over a 24-hour period. Aliquots were removed for assay at various time intervals.
Cryoprecipitution. Fresh plasma was frozen at -85 OC in a Hams blast freezer (Model PCF-9). The frozen plasma was thawed by incubation in a 4 OC waterbath for 90 min, then immediately cen- trifuged at 4 OC for 7 min at 7,000 g. The super- natant was drained and saved, leaving approxi- mately 5 ml of cryoprecipitate. This cryoprecipitate was solubilized by incubating for 4min at 37OC then used at once.
PEG Precipitation. The method followed was essentially that of Wickerhauser (16). The pH of the plasma or cryoprecipitate from pooled donor blood was measured using a Radiometer PHM26 pH meter, and adjusted to pH 6.3; sufficient PEG 4000 was added to bring the PEG concentration to 4.5% (w/v). After mixing and centrifugation the supernatant was adjusted to pH 6.0 and the PEG concentration brought to 11%. The resulting pre- cipitate was immediately dissolved in a small vol- ume of glycine-citrated saline (1 part 0.1 M sodium citrate to 4 parts 0.9% saline, 0.1 M glycine, pH 7.2).
Factor Vl l l Assay. Factor VIII procoagulant activity was assayed in triplicate using a modifica- tion of the partial thromboplastin time method (one-stage assay) with Hyland AHF-PTC Reference Plasma as standard. The cryoprecipitates were

296 Rock/Cruickshank/Tackaberry/Palmer
diluted 1 : l O with Factor VIII deficient plasma (collected into ACD from a patient with severe classical hemophilia), and subsequently diluted with saline as required. Samples containing heparin were pretreated with sufficient protamine sulfate (Eli Lilly & Co.) to neutralize the effects of heparin on clot times. Specifically, several 0.1-ml aliquots from each heparin sample were neutralized with different concentrations of protamine sulfate be- fore dilution with 0.9 ml of saline. 0.1 ml of the diluted specimen was then immediately assayed for Factor VIII. The heparin level was indicated by the concentration of protamine sulfate provid- ing the fastest clot time. Addition of known amounts of heparin to standard plasma showed that l p g of heparin was neutralized by 1 pg of protamine sulfate. An excess of protamine sulfate resulted in extended clot times. This system could detect differences of 1 pg heparid0.l ml sample. The percent FactorVIIUml was derived from a standard curve of Hyland Reference Plasma to which the same amounts of heparin and protamine sulfate had been added before the final 1/10 dilu- tion. All assays were performed in triplicate and clot times were within 1 sec for each sample.
To permit absolute comparison of results with the different anticoagulants, equal volumes of plas- ma and anticoagulants were maintained throughout and the Factor VIII recovery was expressed as the total number of units per bag.
Results
High levels of Factor VIII are recovered when blood is collected directly into heparin. As shown in table I, the plasmas from 10 random donors, whose blood was individu- ally collected into bags containing heparin, had an average total of 293 U of Factor VIII or 116 U/100 ml plasma. The cryoprecipi- tate had an average Factor VIII activity of 227 U representing 78% of the starting ac- tivity. The coefficient of variation for these recoveries from the 10 donors is 0.115. The remaining 21% of the activity was found in the supernatant.
Table I. Factor VIII recovery in heparinized plasma from 10 random donors'
Plasma Cryo- cryo- precipitate supernatant
Total units 293 f 30 221 f 28 61 f 19 % recovery 100 1 8 f 9 2 1 f 5
480 cm3 of whole blood was collected into a standard Fenwal heparin bag; plasma volumes were 252% 18 ml.
When comparing the Factor VIII activity in plasmas obtained from the same individ- ual donors but collected into the different anticoagulants, it is evident that greatly in- creased yields are obtained by using only heparin: 235 U from heparinized plasma, 175U from CPD plasma and 189 U from CPD plus heparin plasma (table 11), repre- senting 103 versus 72 versus 81 U/lOO ml of plasma respectively. Thus, the total re- covery of Factor VIII in heparinized plasma represents a 43% improved over the stan- dard technique of collecting blood into CPD.
In addition to increasing the yields of Factor VIII, heparin also stabilized the Fac- tor VIII activity in the plasma. When the plasmas which were taken from individual donors into separate tubes containing CPD, CPD plus heparin, or heparin were allowed to stand at room temperature for 24 h, vir- tually all of the Factor VIII activity was re- tained in the heparinized samples. In con- trast, the samples with CPD plus heparin retained only 81% of the activity, and those with CPD alone only 64% (table 111).
The presence of heparin also produces a marked increase in the recovery of Factor VIII activity in the cryoprecipitate, with 184 U being obtained from heparinized plas- ma compared to 88 U from CPD plasma.
Yields of Factor VIII from Heparinized Plasma 297
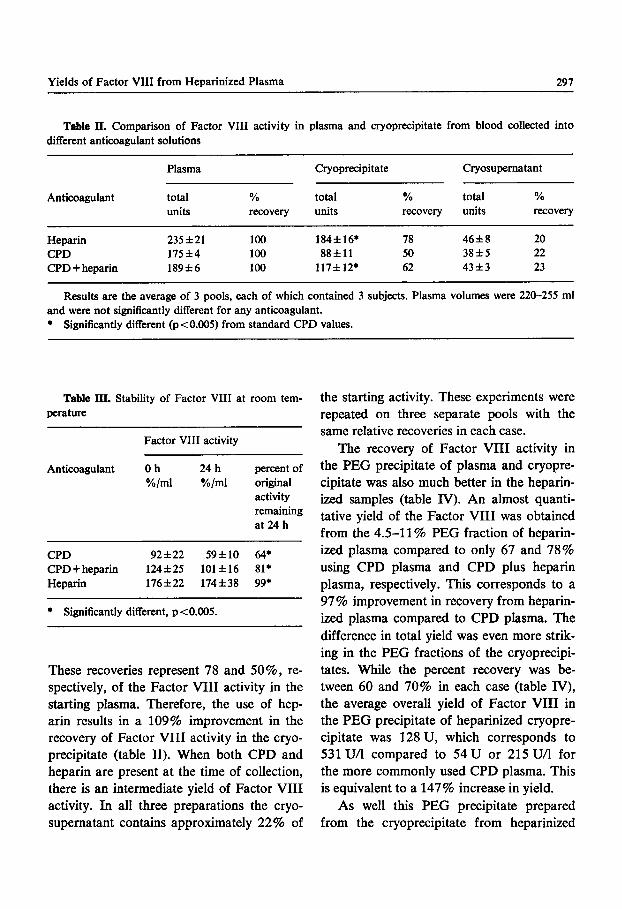
Table II. Comparison of Factor VIII activity in plasma and cryoprecipitate from blood collected into different anticoagulant solutions
Plasma Cryoprecipitate Cryosupernatant
Anticoagulant total % total % total %
Heparin 235 f 21 100 184f16* 78 46f 8 20 CPD 175f4 100 8 8 f l l 50 3 8 f 5 22 CPD +heparin 1 8 9 f 6 100 117f12* 62 43f3 23
units recovery units recovery units recovery
Results are the average of 3 pools, each of which contained 3 subjects. Plasma volumes were 220-255 ml and were not significantly different for any anticoagulant. * Significantly different (p<0.005) from standard CPD values.
Table III. Stability of Factor VIII at room tem- perature
~~~ ~~~
Factor VIII activity
Anticoagulant 0 h 24 h percentof %/ml %/ml original
activity remaining at 24 h
CPD 9 2 f 2 2 5 9 f 1 0 64* CPD+heparin 124f25 101f16 81* Heparin 176f22 174f38 99*
~~ ~~~
* Significantly different, p<0.005.
These recoveries represent 78 and 50%, re- spectively, of the Factor VIII activity in the starting plasma. Therefore, the use of hep- arin results in a 109% improvement in the recovery of Factor VIII activity in the cryo- precipitate (table 11). When both CPD and heparin are present at the time of collection, there is an intermediate yield of Factor VIII activity. In all three preparations the cryo- supernatant contains approximately 22% of
the starting activity. These experiments were repeated on three separate pools with the same relative recoveries in each case.
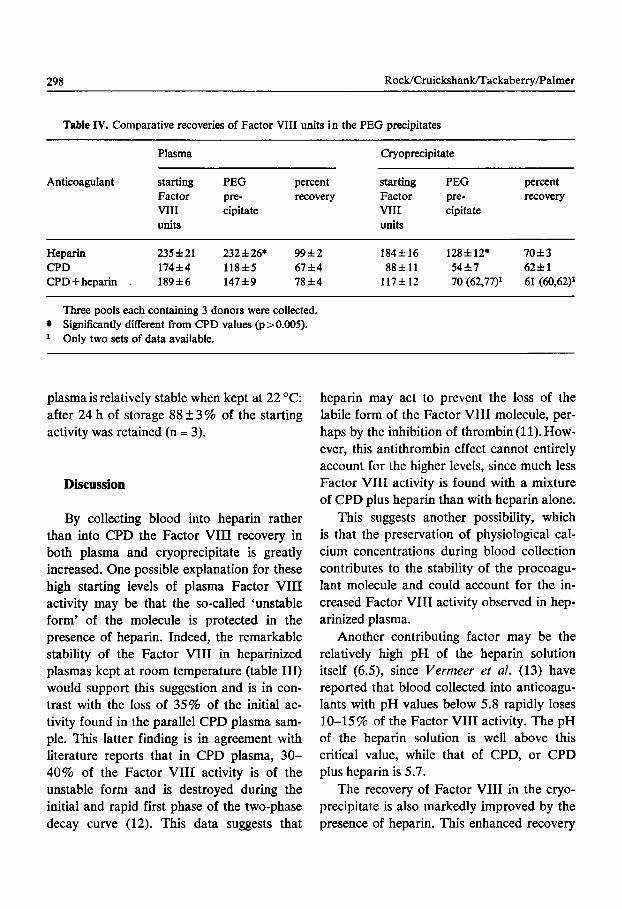
The recovery of Factor VIII activity in the PEG precipitate of plasma and cryopre- cipitate was also much better in the heparin- ized samples (table JY). An almost quanti- tative yield of the Factor VIII was obtained from the 4.5-11% PEG fraction of heparin- ized plasma compared to only 67 and 78% using CPD plasma and CPD plus heparin plasma, respectively. This corresponds to a 97% improvement in recovery from heparin- ized plasma compared to CPD plasma. The difference in total yield was even more strik- ing in the PEG fractions of the cryoprecipi- tates. While the percent recovery was be- tween 60 and 70% in each case (table IV), the average overall yield of Factor VIII in the PEG precipitate of heparinized cryopre- cipitate was 128 U, which corresponds to 531UA compared to 54U or 215UA for the more commonly used CPD plasma. This is equivalent to a 147% increase in yield.
As well this PEG precipitate prepared from the cryoprecipitate from heparinized
298 Rock/Cruickshanmackabeny/Palmer
Table IV. Comparative recoveries of Factor VIII units in the PEG precipitates
Plasma Cryoprecipitate
Anticoagulant starting PEG percent starting PEG percent Factor P E - recovery Factor pre- recovery VIII cipitate VIII cipitate Units units
Heparin 235f21 232f26* 9 9 f 2 184616 128f12* 7 0 f 3 CPD 174f4 118f5 67f4 8 8 f l l 5 4 f 7 6 2 f 1 CPD+heparin . 189f6 147*9 7 8 f 4 117f 12 70 (62,77)* 61 (60,62)'
Three pools each containing 3 donors were collected. Significantly different from CPD values (p>0.005). Only two sets of data available.
plasma is relatively stable when kept at 22 "C: after 24 h of storage 88 f 3 % of the starting activity was retained (n = 3).
Discussion
By collecting blood into heparin rather than into CPD the Factor VIII recovery in both plasma and cryoprecipitate is greatly increased. One possible explanation for these high starting levels of plasma Factor VIII activity may be that the so-called 'unstable form' of the molecule is protected in the presence of heparin. Indeed, the remarkable stability of the Factor VIII in heparinized plasmas kept at room temperature (table III) would support this suggestion and is in con- trast with the loss of 35% of the initial ac- tivity found in the parallel CPD plasma sam- ple. This latter finding is in agreement with literature reports that in CPD plasma, 30- 40% of the Factor VIII activity is of the unstable form and is destroyed during the initial and rapid first phase of the two-phase decay curve (12). This data suggests that
heparin may act to prevent the loss of the labile form of the Factor VIII molecule, per- haps by the inhibition of thrombin (1 1). How- ever, this antithrombin effect cannot entirely account for the higher levels, since much less Factor VIII activity is found with a mixture of CPD plus heparin than with heparin alone.
This suggests another possibility, which is that the preservation of physiological cal- cium concentrations during blood collection contributes to the stability of the procoagu- lant molecule and could account for the in- creased Factor VIII activity observed in hep- arinized plasma.
Another contributing factor may be the relatively high pH of the heparin solution itself (6.5), since Vermeer et al. (13) have reported that blood collected into anticoagu- lants with pH values below 5.8 rapidly loses 10-15% of the Factor VIII activity. The pH of the heparin solution is well above this critical value, while that of CPD, or CPD plus heparin is 5.7.
The recovery of Factor VIII in the cryo- precipitate is also markedly improved by the presence of heparin. This enhanced recovery

Yields of Factor W I from Heparinized Plasma 299
partially reflects the increased starting levels of Factor VIII in the plasma but, in addi- tion, the relative percent recovery of Fac- tor VIII is much greater following cryopre- cipitation of heparinized plasma than of CPD plasma (78 vs. 50%). As well, virtually all of the starting plasma Factor VIII activity is accounted for with heparinized plasma. In contrast, when CPD plasma is cryoprecip- itated approximately 28% of the starting activity is lost, with 50% recovered in the cryoprecipitate and 22% in the supernatant, a finding which agrees with other reports in the literature. This suggests that the increase in Factor VIII activity recovered in the cryo- precipitate of heparinized plasma is due to an increased stability of the procoagulant molecule during cryoprecipitation.
This difference in Factor VIII recovery in the cryoprecipitate cannot be accounted for by differences in the final pH since the heparinized plasma had a pH of 7.9, whereas the plasma collected into CPD plus heparin, or into CPD alone, had pH values of 7.6. Earlier work by Pool [7] indicates that there is no difference in Factor VIII recovery in cryoprecipitate prepared from plasmas with pH values between 6.8 and 8. It may be that the large amounts of procoagulant activity found in the heparinized plasma more read- ily aggregate, and are therefore recovered in the cryoprecipitate since, according to Weiss and Kochwu [15] all the Factor VIII activ- ity of cryoprecipitate is in a high molecular weight form. Indeed, when the cryoprecipi- tate from this heparinized plasma is subjected to column chromatography on Sepharose CL-6B all of the Factor VIII activity elutes at the void volume and reacts with rabbit antiserum to Factor VIII [lo]. This elution pattern is the same as the commonly described profile for Factor VIII activity in the cryo-
precipitate made from CPD plasma [9, 151, indicating that in the cryoprecipitates the Factor VIII molecules from CPD and hepa- rinized plasma are qualitatively similar.
Previous reports in the literature [8] have documented that up to ninety variables af- fect the ultimate recovery of Factor VIII. The present data implicates at least one ad- ditional variable which must be considered. However, it is clear that, by using heparin as the anticoagulant, it is possible to obtain considerably higher levels of Factor VIII activity in plasma, cryoprecipitate, and their PEG precipitates. The increased activity in the final product prepared from heparinized plasma is highly significant and suggests that these procedures may be applicable to pro- ducing purified Factor VIII concentrate on a large scale with significantly improved yields.
Acknowledgements
The authors wish to express their appreciation to Dr. G. Jarnieson for his comments and editorial assistance.
References
1 Bloom, A. L.; Giddings, J. C.; Bevan, B.; Let- ton, M., and Drummond, R. J.: Comparison of quick and slow thaw methods of producing cryoprecipitate antihaemophilic factor from fresh and 24 hour-old blood. J. clin. Path. 22: 447-452 (1969).
2 BMkhous, K. M.; Shanbrom, E.; Roberts, H. R.; Webster, W. P.; Fekete, L., and Wagner, R. H.: A new high-potency glycine-precipitated anti- hemophilic factor (AHF) concentrate. J. Am. med. Ass. 205: 67-71 (1968).
3 Burka, E. R.; Puffer, E. R., and Martinez, J.: The influence of donor characteristics and prep- aration methods on the potency of human cryoprecipitate. Transfusion 15: 323-328 (1975).

300 RocWCruickshank/Tackaberry/Palmer
Johnson, A. J.; Newman, J.; Howell, M. B., and Puszkin, S.: The preparation and some proper- ties of a clinically useful, high purity antihemo- philic factor (AHF). Abstr. XIth Congr. Int. SOC. of Blood Transfusion, Sydney 1966, p. 1109. Newman, J.; Johnson, A.; Karpatkin, M. H., and Puszkin, S.: Methods for the production of clinically effective intermediate and high-purity factor VIII concentrates. Br. J. Haemat. 22: 1- 20 (1971). Pool, J. G. and Shannon, A. E.: Production of high potency concentrates of antihemophilic globulin in a closed bag system. New Engl. J. Med. 273: 1443-1447 (1965). Pool, J. G.: The effect of several variables on cryoprecipitated factor VIII (AHG) concentrates. Transfusion 7: 165-167 (1967).
S Pool, J. G.: Cryoprecipitate quality and supply. Transfusion 15: 305-306 (1975).
9 Rick, M. E. and Hoyer, L. W.: Immunologic studies of antihemophilic factor ( A m , factor VIII). V. Immunologic properties of AHF sub- units produced by salt dissociation. Blood 42:
10 Rock, G. A.; Palmer, D. S.; Tackaberry, E. S., and Cruickshank, W. H.: The presence of high and low molecular weight forms of Factor VIII in heparinized plasma. Thromb. Res. 13: 85-96 (1978).
11 Smith, G. F.: The heparin-thrombin complex in the mechanism of thrombin inactivation by hep-
737-747 (1973).
arin. Biochem. biophys. Res. Commun. 77: 111- 117 (1977).
12 Stibbe, J.; Hemker, H. C., and Creveld, S. V.: The inactivation of factor VIII in vitro. Thromb. Diath. haemorrh. 27: 43-58 (1972).
13 Vermeer, C.; Soute, B. A. M.; Ates, G.; Hel- lings, J. A., and Brummelhuis, H. G. J.: Contri- butions to the optimal use of human blood. VIII. Stability of blood coagulation factor VIII during collection and storage of whole blood and plasma. Vox Sang. 32: 55-67 (1976).
14 Weiss, H. J.: A study of the cation- and pH- dependent stability of factors V and VIII in plasma. Thromb. Diath. haemorrh. 14: 32-51 (1965).
15 Weiss, H. J. and Kochwa, S.: Molecular forms of antihaemophilic globulin in plasma, cryopre- cipitate and after thrombin activation. Br. J. Haemat. 28: 89-100 (1970).
16 Wickerhauser, M.: Preparation of antihemo- philic factor from in-dated plasma. Transfusion 16: 345-350 (1976).
Received: May 18, 1978 Accepted: December 8, 1978
Dr. G. A. Rock, The Canadian Red Cross, 85 Plymouth Street, Ottawa, Ont. K1S 3E2 (Canada)