importance of clinical suspicion by: dr....
TRANSCRIPT
Morbidity and Mortality
Importance of clinical suspicion
By: Dr. Rabinovich

Patient
• 52 year old black male (big and solid)• Recent immigrant, primary language is
French with poor English• HPI: Involved in an MVA on May 25, 2005,
high speed, possible roll over, seat-belted, no airbag, and query LOC at scene.
• Presents to HGH ER room in “stable” condition.
Patient
• ER MD does primary survey and controls patients pain and vitals
• Patient and MD have a major language barrier, but after a careful review the following history is obtained:
• NKDA, No Meds, PHx of Eye Surgery
On Examination by ER MD• BP 120/80, HR 80-90, RR 18-22, afebrile,
Sat 98 % on room-air.• Patient a/o X 3, GCS 15, PEARL 3mm• Bilateral breath sounds equal and normal• Heart sounds normal, no active external
bleeding• No neck pain, neurovascular status intact• No obvious facial trauma• Moves all limbs spontaneously
On Examination
• L Shoulder pain with deformity midshaft• R Hip pain with no deformity• Bilateral posterior chest wall pain• Bilateral abdominal quadrant pain
• Any clinical suspicions yet !!!! ?
ER Orders• C-Spine Xrays read as normal by ER• L-Spine Xray read as normal by ER
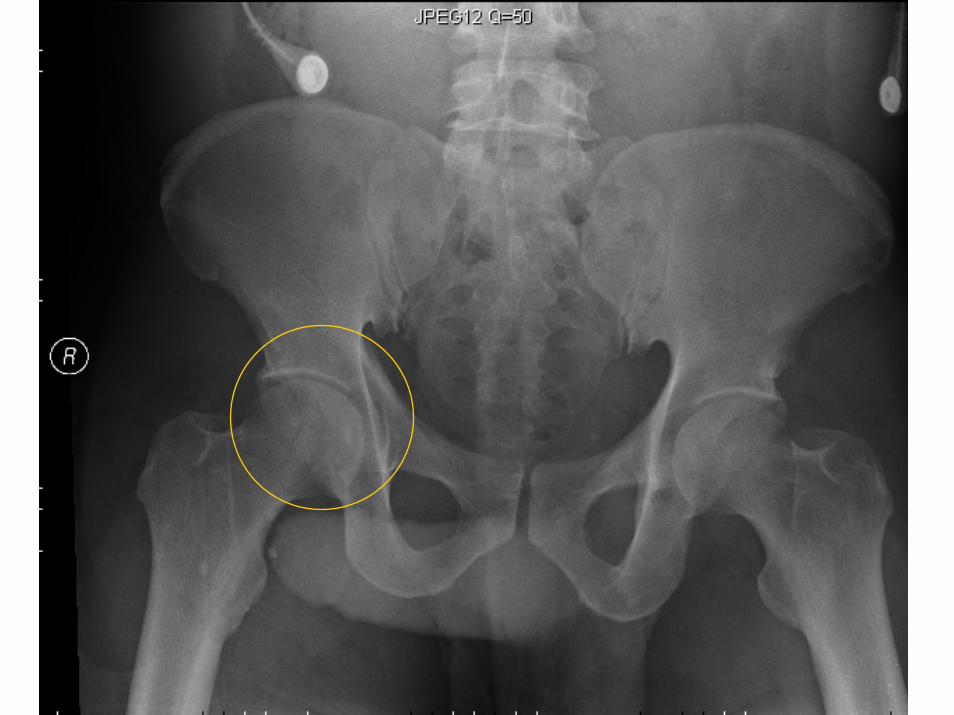
• L-Humerus Midshaft fracture• Pelvis/Hips read as normal by ER
• CXR Bilateral rib #’s, Mild Atelectasis, no pneumo/hemo-thorax
ER Labs
• Glucose 8.5, BUN 5.8, Cr 106, Na 139, K 3.3, Cl 103, Total C02 26, Amylase 127, CK 384, Trop <0.04 X2, LKC 9.8, HB 139, PLT 166.
• Patient is referred to Orthopaedics for “isolated” L humerus fracture.
• Lets review the x-rays …
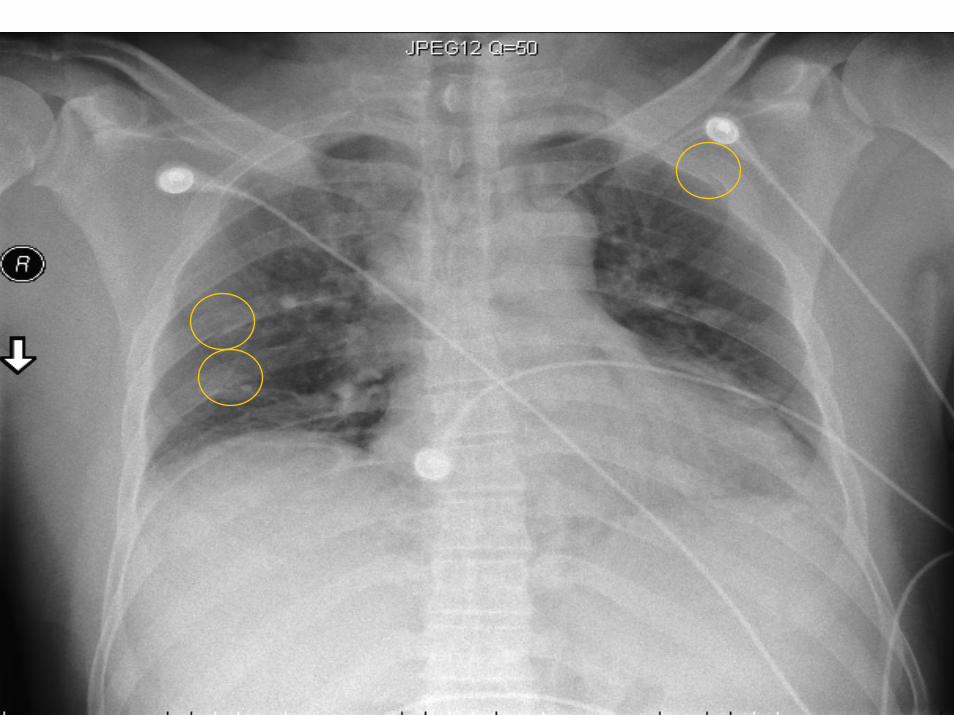
CXR


After the review
• Orthopaedics is consulted to put a hanging cast on the humerus and to d/c the patient home.
• While reviewing the x-rays, Orthopaedics identifies the R. Acetabulum #.
• Patient is then admitted for observation.
On the ward
• Orthopaedics sees the patient daily, and plans to d/c patient home if ok by OT/PT.
• After 48 hours on the ward, the patient starts experiencing more abdominal pain, tachycardia and his blood pressure starts falling!
• Any clinical suspicions yet !!! ???

Let’s reassess
• Next blood work, done on May 28, 2005.• HB 86, PLT 82, LKC 9.3, CK 1039
• Patient is placed in SDU for monitoring
• Trauma is called stat for primaryassessment and assistance

Trauma service to the rescue
• Patient is monitored and given fluids for resuscitation
• Stat CT Head normal• Stat CT Chest/Abd/Pelvis
• Bilateral multiple rib #’s• Bilateral atelectasis• Free Fluid Grade 4 Spleen Laceration



What to do?
• General surgery consulted stat• Patient is rushed to OR for Splenectomy• Patient admitted to ICU post-op• 72 hours in ICU the patient is stabilized
and extubated d/c to 6 South SDU
• Orthopaedics applies hanging cast brace to L. Humerus, and NWB 6 wks R. Leg
The results
• Gen Sx is happy with post-op recovery and patient is stabilized to be d/c from SDU.
• While in hospital, patient develops pneumonia and started on antibiotics.
• Doing well, and planning to d/c to restbitefor orthopaedic recovery
The lessons we learned1. Clinical Suspicion for more serious injuries
should always be high for an MVA with long bone fractures.
2. If you find multiple fractures, suspect internal organ damage.
3. Don’t hesitate to use your resources (Trauma, Gen Sx …)
4. Just because the patient looks like a big tough person, the internal organs are still soft.
5. Monitor labs carefully for the first 48-72 hours, it’s the least we can do.
• Thank you