implementation of national/regional programs to prevent copd nan shan zhong chinese medical...
TRANSCRIPT

Implementation of National/Regional programs
to prevent COPD
Nan Shan Zhong
Chinese Medical Association

The first five leading causes of death in China (2007)
Rank
Urban Rural
Disease(ICD-10)
Mortality(1/100,000) %
Disease (ICD-10)
Mortality (1/100,000)
%
1 Malignant tumor 176.2 28.5 Malignant tumor 114.2 24.8
2 Cerebrovascular diseases 111.5 18.0 Cerebrovascular
diseases 119.7 20.6
3Heart diseases 100.6 16.3 Respiratory Respiratory
diseasesdiseases 100.2 16.2
4 Respiratory Respiratory diseasesdiseases 80.9 13.1 Heart diseases 86.0 14.8
5Trauma/ Poisoning 37.6 6.1
Trauma/ Poisoning 52.1 9.0

Prevalence of COPD in China:
Population (>40y ): 8.2% (M-12.4% ,F-5.1% ) Total: 32.8 millions32.8 millions
8.1%-24.1% (perennial:25.6% of total)
CRD in China
Current patient
COPD 32.8 millionsCOPD 32.8 millions
Asthma 15.0 millionsAsthma 15.0 millions
Allergic rhinitis 113 millionsAllergic rhinitis 113 millions

19.30% (1.4M)19.30% (1.4M)
19.10% (1.4M)19.10% (1.4M)Cerebrovascular diseaseCerebrovascular disease
17.60% (1.28M)17.60% (1.28M)COPDCOPD
15.0% (1.0M)15.0% (1.0M)Cardiovascular diseaseCardiovascular disease
1.2% (90,000)1.2% (90,000)DiabetesDiabetes
0%0% 2%2% 4%4% 6%6% 8%8% 10%10% 12%12% 14%14% 16%16% 18%18% 20%20%
% Cause of death (2000)% Cause of death (2000)
COPD: one of the first leading causes of death in China (2000)
MOH Disease Control Department and NCDC. Report on Chronic Disease in China. 2006.MOH Disease Control Department and NCDC. Report on Chronic Disease in China. 2006.
Kong Lingzhi. 2005 Report in NCDC Annual Conference. Kong Lingzhi. 2005 Report in NCDC Annual Conference.
TumorTumor

GARD China Network
China Asthma Alliance China COPD Alliance
China GARD AllianceDept of Chronic Disease
Control, Ministry of Public Health, China
Chinese Association of Respir.
Dis

CRD listed as priority in the 15year plan of the control and prevention of chronic non communicable diseases
(MOH 2007-2022)
Hypertension
Diabetes
Heart disease
Malignant tumor
Chronic respiratory disease

National/Regional programs to manage COPD
↓Risk factors (Smoking cessation, reducti
on of indoor/outdoor air pollution)
Intervention as early as possible
Development of effective and affordable
medication



WHO Framework Convention on Tobacco Control (WHO/FCTC)
• Government ratified: Aug 28th, 2005
• Enforcement: Jan 9th, 2006

Ministry of Health
China CDC- National Tobacco Control Office
WHO Collaborating Center for Tobacco or Health
China Association On Tobacco Control
National Health Education Institute
Tobacco Control Organizations in China

11th, March 2008 22th, May 2009
Policy on Smoke Free Healthcare Facilities
Smoking forbidden in hospitals in China 50% hospitals at the end of 2010 100% hospitals at the end of 2011
MOH Document 21st May 2009
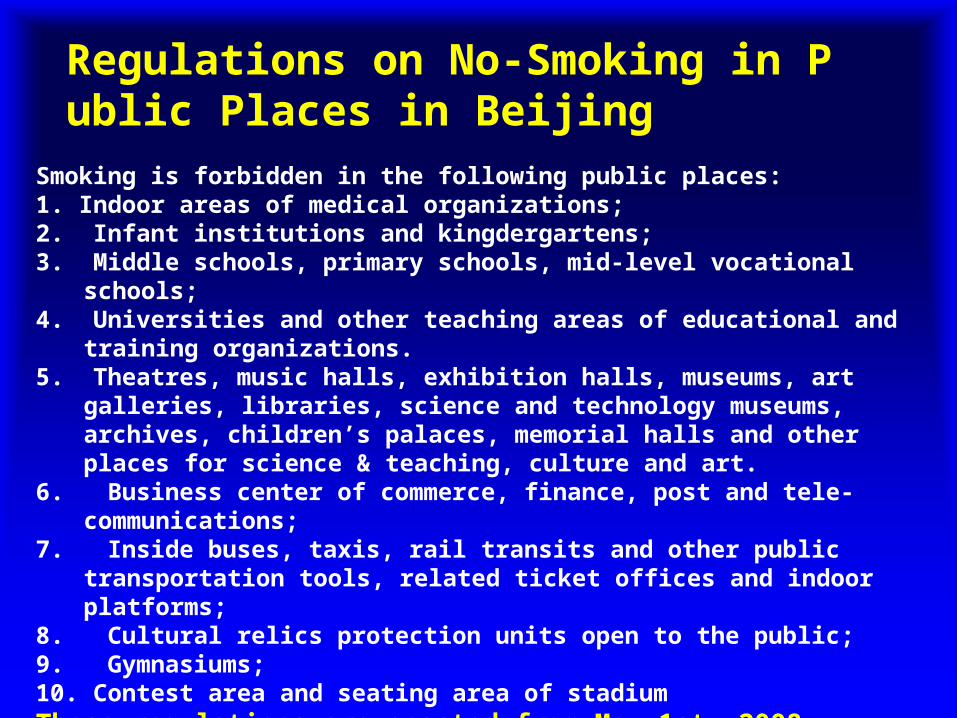
Smoking is forbidden in the following public places:1. Indoor areas of medical organizations;2. Infant institutions and kingdergartens;3. Middle schools, primary schools, mid-level vocational schools;4. Universities and other teaching areas of educational and
training organizations.5. Theatres, music halls, exhibition halls, museums, art galleries,
libraries, science and technology museums, archives, children’s palaces, memorial halls and other places for science & teaching, culture and art.
6. Business center of commerce, finance, post and tele-communications;
7. Inside buses, taxis, rail transits and other public transportation tools, related ticket offices and indoor platforms;
8. Cultural relics protection units open to the public;9. Gymnasiums;10. Contest area and seating area of stadiumThese regulations are enacted from May 1st, 2008
Regulations on No-Smoking in Public Places in Beijing

YearYear 1984 1984 1996 1996 2002 20092002 2009
Total smoking rate 33.9%Total smoking rate 33.9% 37.6% 37.6% 35.8% 35.8% (Aged>15)(Aged>15) MaleMale 66.9% 66.9% 66.0% 48%66.0% 48% FemaleFemale 4.2% 4.2% 3.08% 2.6% 3.08% 2.6% Smoking rate inSmoking rate in 60.0% 60.0% 56.8%56.8%male medical doctorsmale medical doctors
YearYear 1984 1984 1996 1996 2002 20092002 2009
Total smoking rate 33.9%Total smoking rate 33.9% 37.6% 37.6% 35.8% 35.8% (Aged>15)(Aged>15) MaleMale 66.9% 66.9% 66.0% 48%66.0% 48% FemaleFemale 4.2% 4.2% 3.08% 2.6% 3.08% 2.6% Smoking rate inSmoking rate in 60.0% 60.0% 56.8%56.8%male medical doctorsmale medical doctors
Three National Prevalence Surveys
Three National Prevalence Surveys

Haze in large cities

“Hazy sky” (NO VOC O3 etc) firstly listed in the category of air pollution in the Pearl River Delta Region
Document of Guangdong Government 1th May 2009

National/Regional programs to manage CRD
↓Risk factors (Smoking cessation reducti
on of indoor/outdoor air pollution)
Intervention as early as possible
Development of effective and affordable
medication
The trend towards development of medicine
——Early prevention and intervention——Early prevention and intervention
A 3P modality Predictive
Preventive
Personalized
Strategy of COPD management : moving to the community level

Early Early preventionprevention
Early Early managementmanagement
Clinical
management
Rescue
Early Early preventionprevention
Early Early managementmanagement
ClinicalClinicalmanagementmanagement RescueRescue
Medical costs
Medical costsMedical costs

How to improve COPD management at the community level
Increase government investment
Education among medical staff at the
community medical system
Research to early implement
intervention ;to develop “effective,
affordable, simple and safe” medications

China’s total health expenditure takes up only 17% of government’s budget, compared with a mean of
40% in developing countries
0
10
20
30
40
50
60
70
80
1980 1990 1995 2000 2002 2003 2004 2005
Government budget
Soci al securi ti es
Out of pocket
Data from MoH China (2006)

Increased government investment
More investment in the community health care system (in the next 3 years) Additional healthcare budget
850 billion Yuan Wen Jiabao
National People’s Congress 2009

Routine (regular) lung function test in the community
Health care system

How to improve community health-care
Increase government investment
Education among medical staff at the
community medical system
Research to early implement
intervention ;to develop “effective,
affordable, simple and safe” medications

2007;175

Diagnosed Rate of COPD Before Epidemiologic Survey
0. 0
5. 0
10. 0
15. 0
20. 0
25. 0
30. 0
35. 0
40. 0
total popul at i on COPD popul at i on
prev
alen
ce o
f do
ctor
-dia
gnos
is chroni c bronchi t i s
emphysema
bronchi al asthma
COPD
one of above
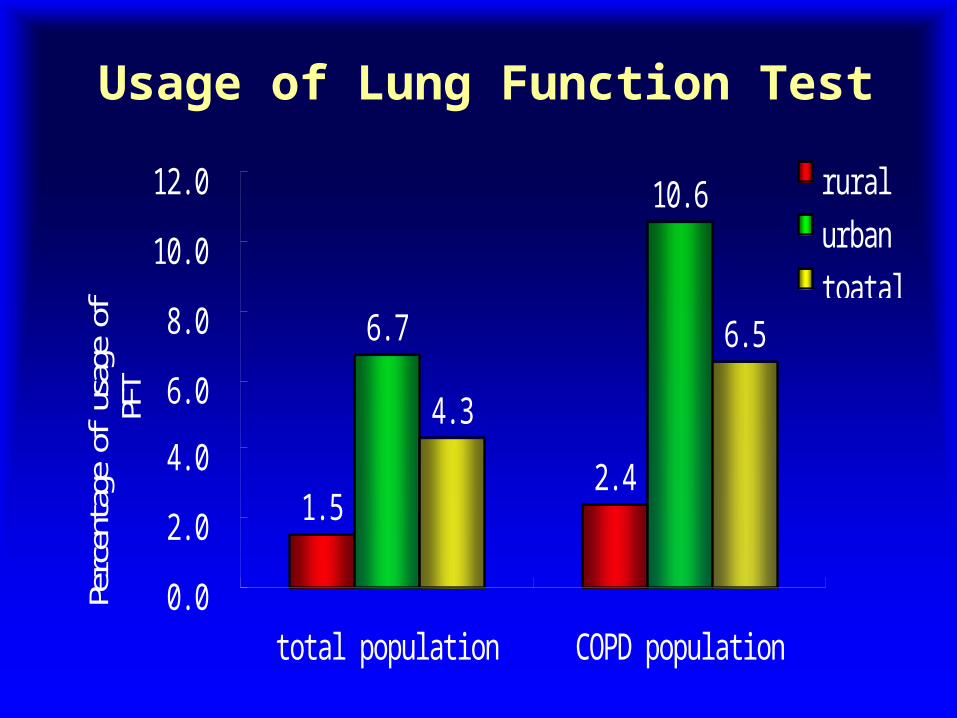
Usage of Lung Function Test
1. 52. 4
6. 7
10. 6
4. 3
6. 5
0. 0
2. 0
4. 0
6. 0
8. 0
10. 0
12. 0
total popul at i on COPD popul at i on
Perc
enta
ge o
f us
age
ofPF
Trural
urban
toatal

The Launch Meeting of China COPD Alliance in Guangzhou, Nov 4, 2006

Program of COPD Prevention & Management
Awareness: burden ,smoking hazards, air pollu
tion (including biomas fuels)Smoking cessation campaignReduction of outdoor/indoor pollutionPublic education (TV newspaper)Research work:
a/ Early intervention-more treatable and reversible b/ Develop effective and affordable medication

Beijing Feb 25Beijing Feb 25
Tianjin Feb 26Tianjin Feb 26
Shanghai Mar 4Shanghai Mar 4Chongqing Mar 5Chongqing Mar 5
Haerbin Mar 19Haerbin Mar 19
Guangzhou Mar 11Guangzhou Mar 11
Wuhan Mar 12Wuhan Mar 12Nanjing Mar 25Nanjing Mar 25
Shenyang Mar 26Shenyang Mar 26
Jinan Apr 1Jinan Apr 1
Hangzhou Mar 18Hangzhou Mar 18
1st turn
2nd turn
Training programme of the medical staff in the community health care system (Early 2007)

Beijing Sep 10Beijing Sep 10
Shanghai Sep 23Shanghai Sep 23Chendu Sep 16Chendu Sep 16
Haerbin Sep 9Haerbin Sep 9
Guangzhou Oct 8Guangzhou Oct 8
Wuhan Oct 21Wuhan Oct 21Nanjing Sep 17Nanjing Sep 17
Shenyang Oct 14Shenyang Oct 14
Jinan Sep 24Jinan Sep 24
Hangzhou Oct 15Hangzhou Oct 15
1st turn
2nd turn
Training programme of the medical staff in the community health care system (late 2008)


The Launch Meeting of China Asthma Alliance in Zhengzhou, June , 2005

Asthma AllianceImplementation of 2008 GINA Guidelines
Training program of physicians in community level
Knowledge of prevention and management of asthma in the public and media
Development of a simplified guideline available for the rural area (cost-effective)
Boycott fake medicine

Effective and affordable
Carbocisteine, theophylline in COPD
Half of GINA recommended dose in ast
hma
Chinese traditional medicine

THANKS