implementation of bundles in nicu - perinatal 16 rosana richmann bundles... · implementation of...
TRANSCRIPT

Implementation of Bundles in
NICU
Rosana Richtmann, M.D.
Instituto de Infectologia Emilio Ribas
Hospital e Maternidade Santa Joana – São Paulo
Presidente da Sociedade Paulista de Infectologia - SPI

AGENDA
What is a “BUNDLE”?
How to develop a BUNDLE in a NICU?
How to develop a BUNDLE in a Brazilian
NICU?
How to put the BUNDLE in practice,
working with “Medical Doctors…”?


AGENDA
What is a “BUNDLE”?
How to develop a BUNDLE in a NICU?
› CVC
› VAP
How to develop a BUNDLE in a Brazilian
NICU?
How to put the BUNDLE in practice,
working with “Medical Doctors…”?

➥Individual measures that when put
together have much better results!
➥Considered a standard of care!
INSTITUTE FOR HEALTHCARE IMPROVEMENT
Guidelines X Bundles:
What is the difference?
Which one is better to the ICC?
X
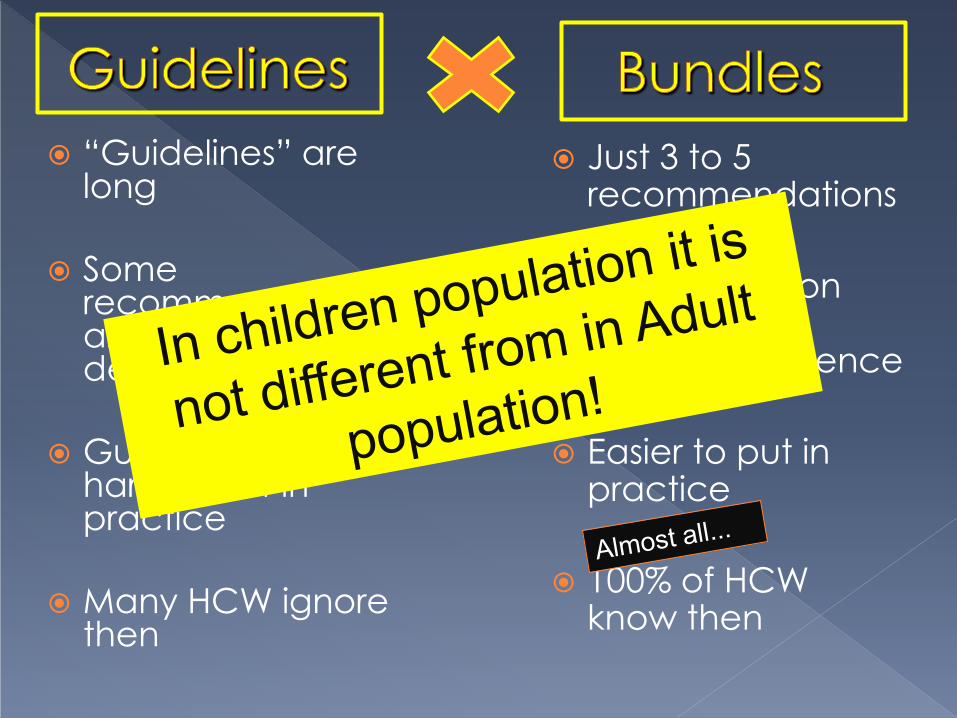
“Guidelines” are long
Some
recommendations are not well defined
Guidelines are very hard to put in practice
Many HCW ignore then
Just 3 to 5 recommendations
100% based on HIGH level of scientific evidence
Easier to put in practice
100% of HCW know then

“Bundles Brigde the Guideline Gap”
Evidence Guideline Practice
Bundles
Guidelines X Bundles: What is the diference?
AGENDA
What is a “BUNDLE”?
How to develop a BUNDLE in a NICU?
How to develop a BUNDLE in a Brazilian NICU?
How to put the BUNDLE in practice, working with “Medical Doctors…”?
“Healthcare-acquired infection (HAI) in children
may have been considered inevitable in the past.”
A ocorrência da IH não é mais aceita como uma
consequência da internação em Unidade de
terapia intensiva pediátrica ou neonatal
The Classical Central Line Bundle (for adults…)
Hand hygiene
Maximum barrier precautions,
Chlorhexidine site disinfection,
Avoiding the femoral site,
Promptly removing unnecessary central venous catheters

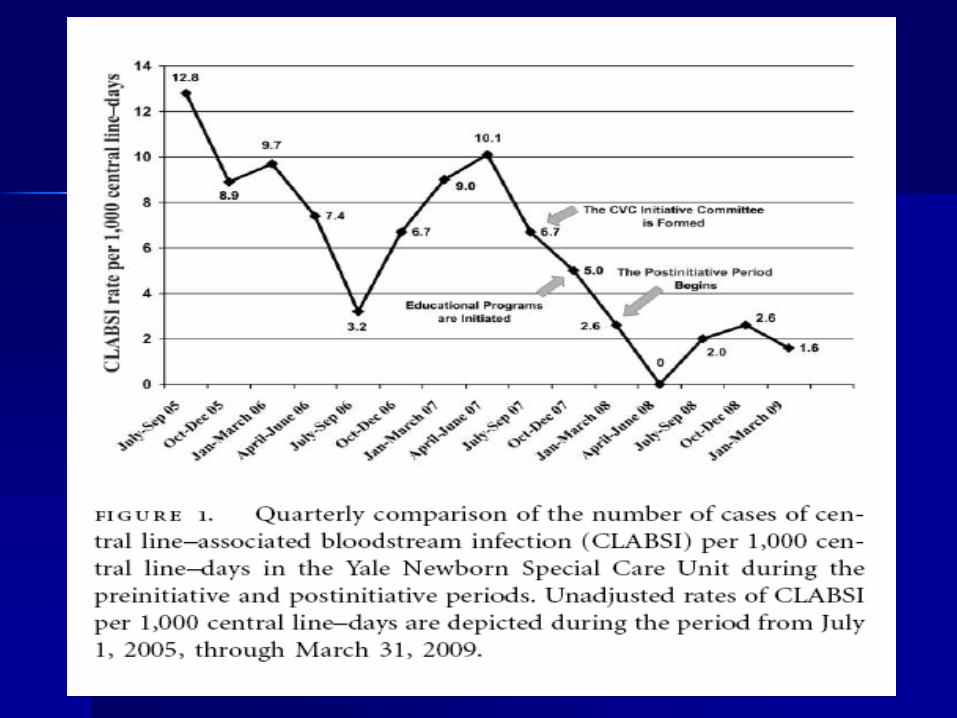
The Yale–New Haven Children’s Hospital 54- Beds.
Decrease the BSI rate
quasi-experimental study of an educational intervention
July 2005 - June 2007
multidisciplinary quality improvement committee – Review published data
– create guidelines for CVC placement and management.

Pre intervention
1. CVC insertion with different techniques
2. Use of Povidone iodine with 70% isopropyl alcohol
3. Dressing changes without routine recommendations
4. TPN infusion + other medicaments
5. 70% alcohol for hub disinfection
6. No routine in the decision to Remove CVCs (on medical demand)
Post intervention
1. Insertion of CVC = HCW from the Catheter team
2. sustained
3. When damp, loosened or soiled
4. CVC exclusive for TPN
5. chlorhexidine gluconate on the hub
6. Daily analysis on the necessity of the CVC

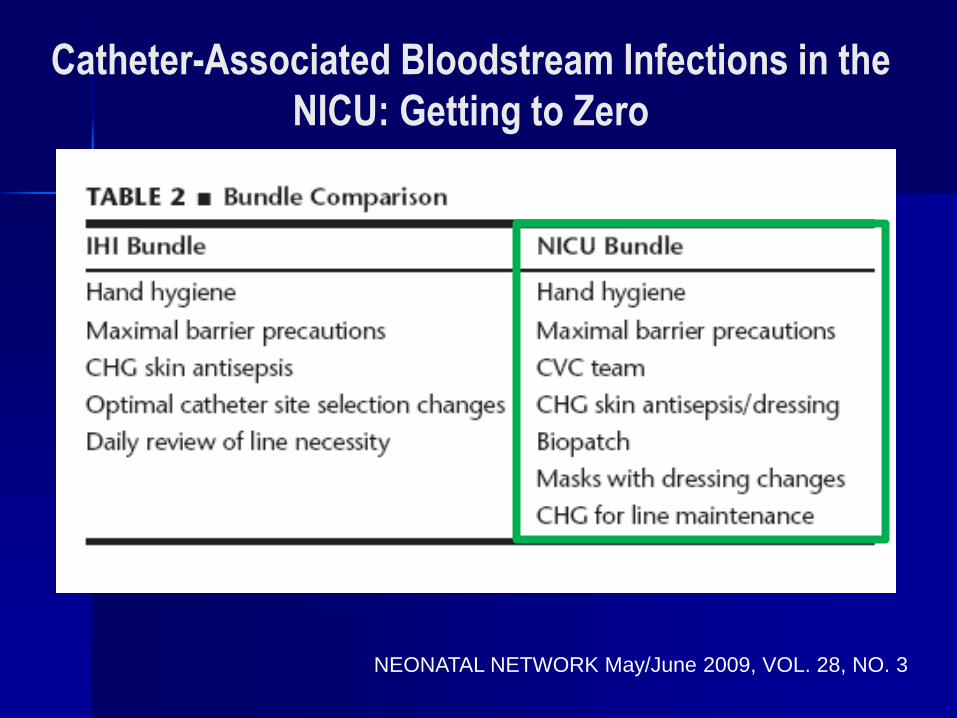
Catheter-Associated Bloodstream Infections in the
NICU: Getting to Zero
NEONATAL NETWORK May/June 2009, VOL. 28, NO. 3
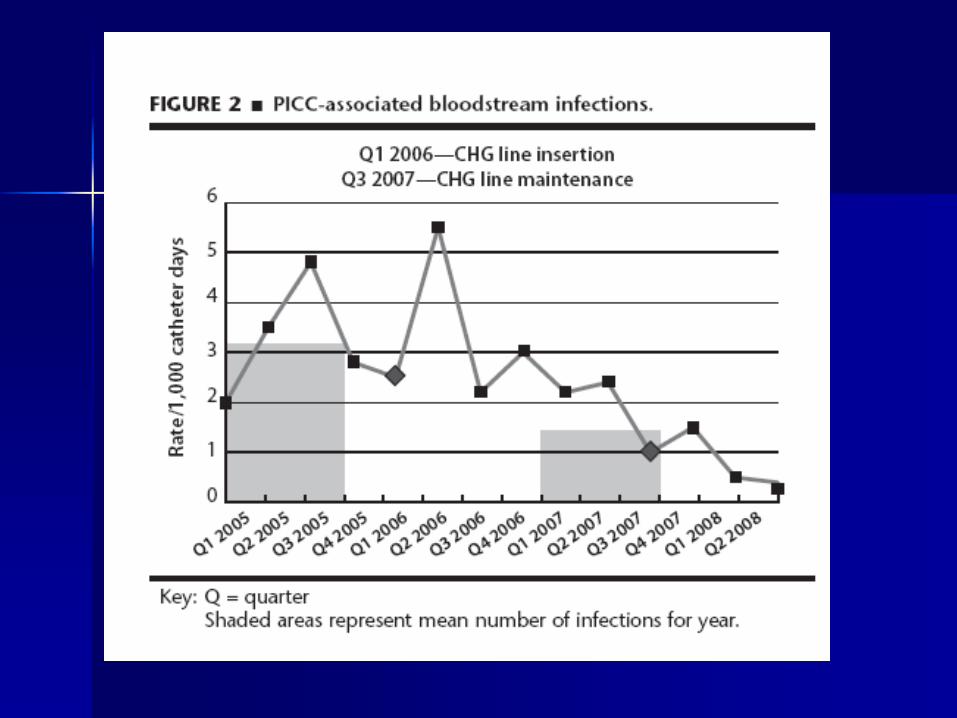
Arkansas Children’s Hospital
NCIU with 85 beds
800 admission /year
PICC line/ Broviac (exclusive for GI surgery and TPN)
AGENDA
What is a “BUNDLE”?
How to develop a BUNDLE in a NICU?
How to develop a BUNDLE in a Brazilian NICU?
How to put the BUNDLE in practice, working with “Medical Doctors…”?

CLABSI in Brazil?
How big is the Problem?
181 published papers about CLABSI
CLABSI rates: 3.2 - 40.4/1000 cvc-d
Higher incidence in ICU (specially =
NICU)
Mortality rate: 6,7% a 75%
– Higher mortality: Pseudomonas/Acineto/
Candida
APECIH – Infecção Associada ao uso de Cateteres
Vasculares, 2005

poorly defined
1%
ParasitaryInfections
4%
GI infections8% Meningites
1%
IRA5%
Pneumonias8%
Nutricional issues
3%
Sepsis3%
Neonatal issues 61 %
Total of Deaths: 325.763
Mortality causes in < 1y in Latin America countries,
OPS 2003

10% 5%
32 %
24%
29 %
Mortality causes in < 1y in Latin America countries,
OPS 2003

EUA: Gaynes, 1996
n = 13'179
40%
15%14%
8%
8%
15%
BSI PNEU EENT SST GI OTHERS
Sites of Neonatal Infections
BSI – Blood Stream infection
PNEU - pneumonia
EENT – eyes, ear, nose and mounth
SST – skin and soft tissues
GI - gastrointestinal
Europa: Raymond, 2000
n = 80
68%17%
14%1%
BSI PNEU GI Outros
Brasil: Pessoa-Silva, 2004
n = 1'494
50%
15%
14%
7%6% 8%
BSI PNEU EENT SST GI Outros
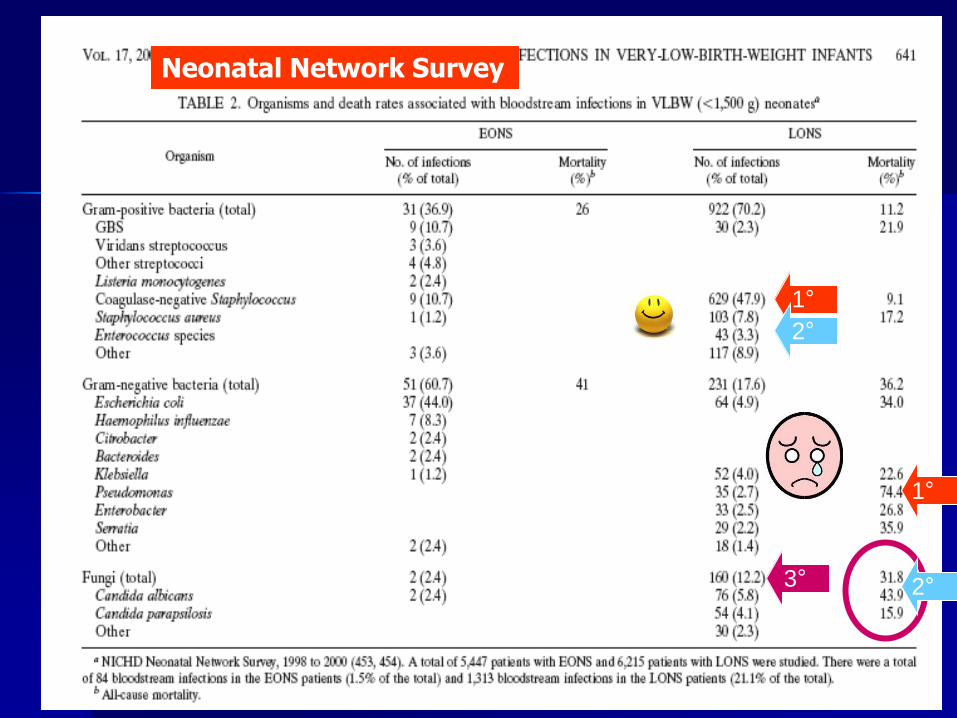
Neonatal Network Survey
1°
2°
3° 2°
1°

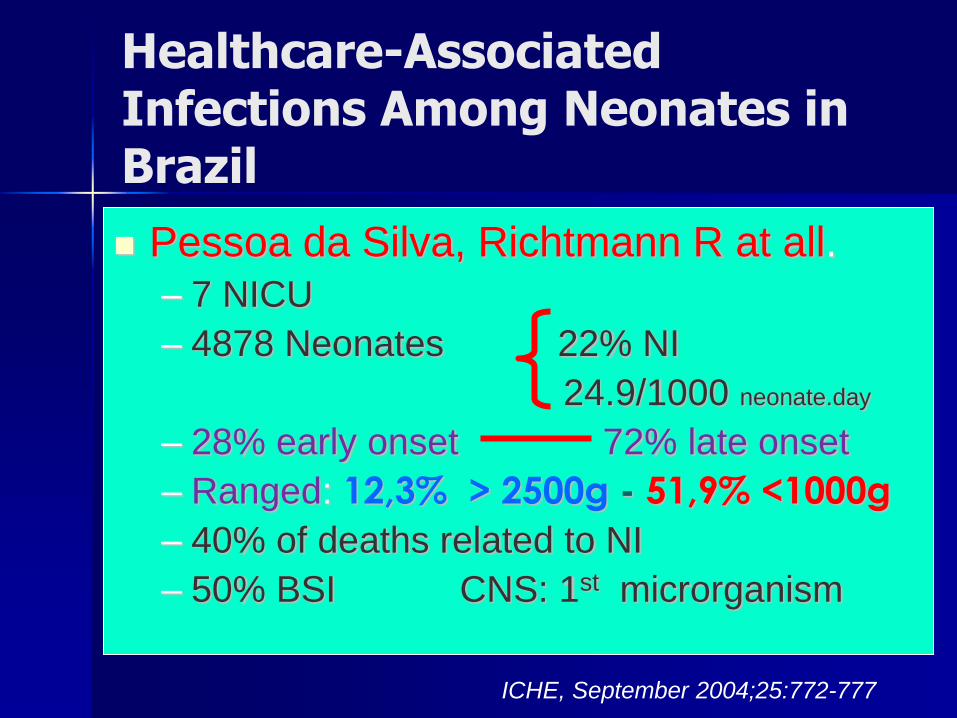
Healthcare-Associated Infections Among Neonates in Brazil
Pessoa da Silva, Richtmann R at all.
– 7 NICU
– 4878 Neonates 22% NI
24.9/1000 neonate.day
– 28% early onset 72% late onset
– Ranged: 12,3% > 2500g - 51,9% <1000g
– 40% of deaths related to NI
– 50% BSI CNS: 1st microrganism
ICHE, September 2004;25:772-777
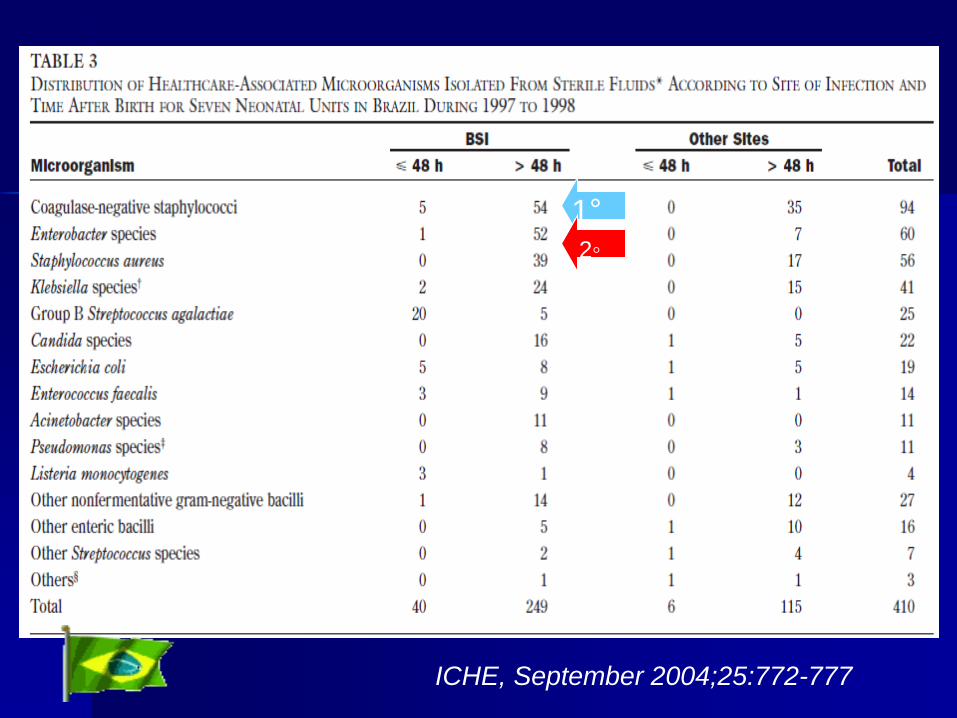
1°
ICHE, September 2004;25:772-777
2◦

• To evaluate DA-HAI
• From sept 2003 to Feb 2010
• 13.251 patients
• 30 NICU
• 15 countries
CLA-BSI and PAV
Low-income
Lower-middle-income
Upper-middle-income


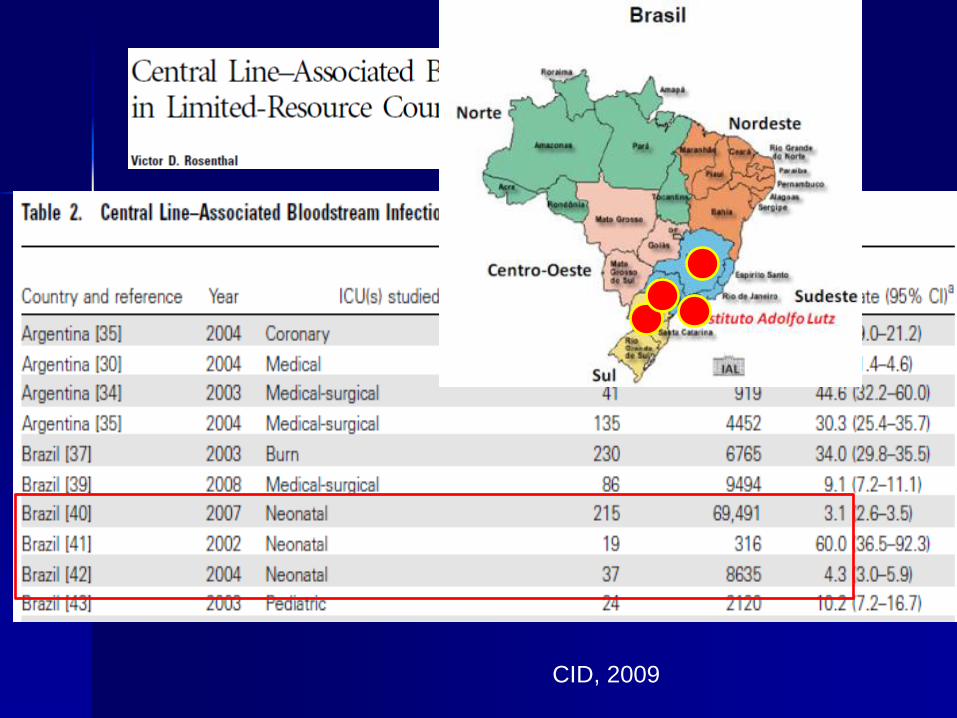
CID, 2009
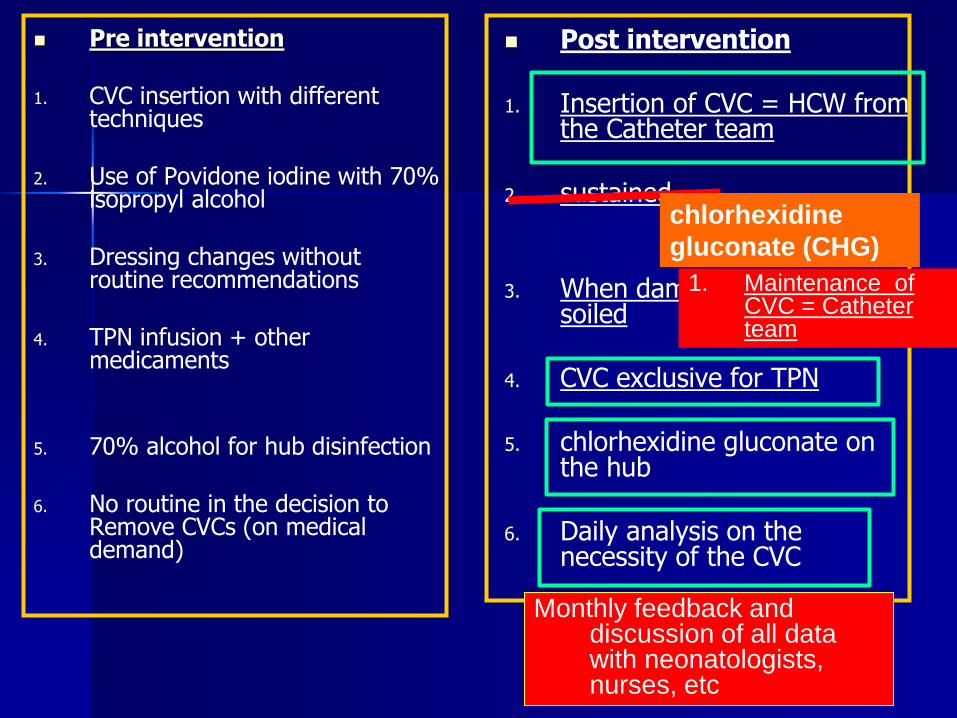
Pre intervention
1. CVC insertion with different techniques
2. Use of Povidone iodine with 70% isopropyl alcohol
3. Dressing changes without routine recommendations
4. TPN infusion + other medicaments
5. 70% alcohol for hub disinfection
6. No routine in the decision to Remove CVCs (on medical demand)
Post intervention
1. Insertion of CVC = HCW from the Catheter team
2. sustained
3. When damp, loosened or soiled
4. CVC exclusive for TPN
5. chlorhexidine gluconate on the hub
6. Daily analysis on the necessity of the CVC
chlorhexidine
gluconate (CHG)
1. Maintenance of CVC = Catheter team
Monthly feedback and discussion of all data with neonatologists, nurses, etc

Pneumonia Bundle

Prevenção de Pneumonia Associada a
Ventilação Mecânica
Institute for Healthcare Improvement
1-Elevação da cabeceira entre 30 a 45
graus
2-“Despertar diário”
3-Prevenção de úlcera péptica
4-Profilaxia de trombose venosa

Fatores de risco para aquisição de BCP associada à VM
Adulto:
– Duração da VM
– Aspiração orofaríngea
– Uso de antibiótico
– Dispositivos respiratórios
RN:
– IG
– Peso
– Sexo
– Duração VM
– Aspiração traqueal
– Reintubação
– Dreno de tórax

How-to-guide
Pediatric supplement
Ventilator Associated
Pneumonia
Pediatric Affinity Group

Modificações para o Bundle Pediátrico/RN
Manter decúbito 15 – 30 º para RN .
Despertar diário da sedação não é recomendado pelo risco de extubação não planejada. Recomenda-se avaliação diária para a possibiidade de extubação através de check list diário ou durante as rondas.
Profilaxia de úlcera gástrica de acordo com a idade da criança
Profilaxia de trombose venosa de acordo com a idade da criança respeitando sempre as contra indicações.
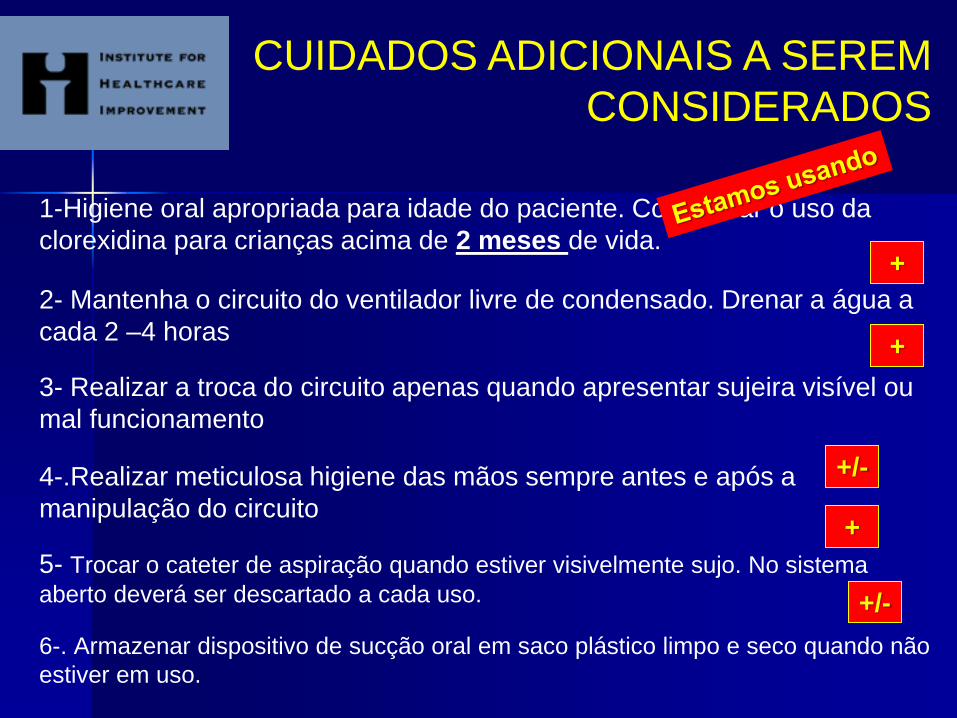
1-Higiene oral apropriada para idade do paciente. Considerar o uso da
clorexidina para crianças acima de 2 meses de vida.
2- Mantenha o circuito do ventilador livre de condensado. Drenar a água a
cada 2 –4 horas
3- Realizar a troca do circuito apenas quando apresentar sujeira visível ou
mal funcionamento
4-.Realizar meticulosa higiene das mãos sempre antes e após a
manipulação do circuito
5- Trocar o cateter de aspiração quando estiver visivelmente sujo. No sistema
aberto deverá ser descartado a cada uso.
6-. Armazenar dispositivo de sucção oral em saco plástico limpo e seco quando não
estiver em uso.
CUIDADOS ADICIONAIS A SEREM
CONSIDERADOS
+
+
+/-
+
+/-

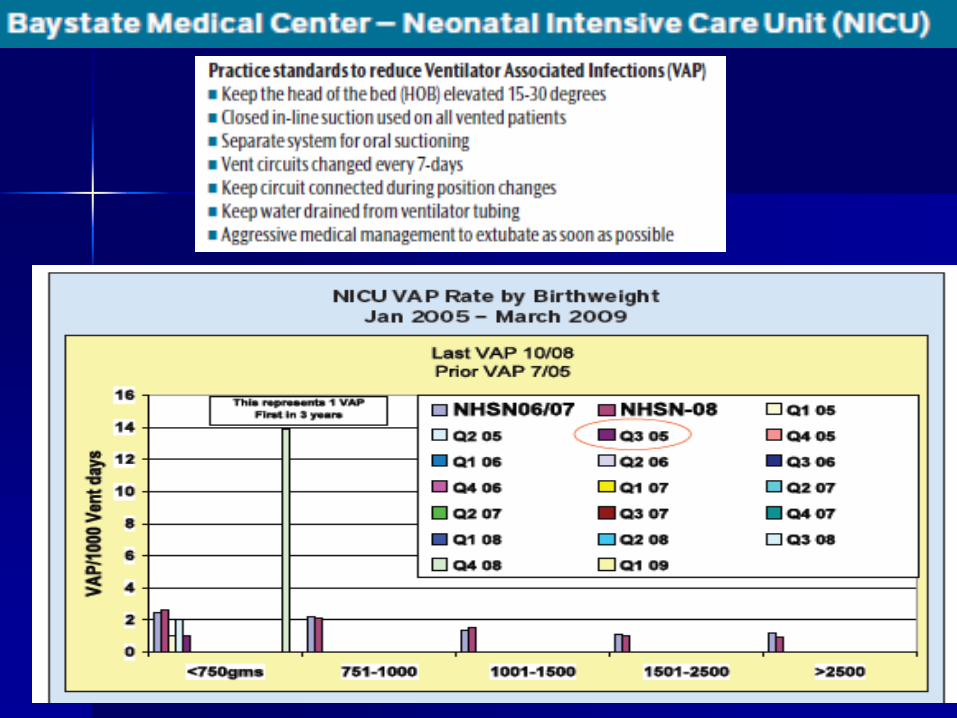
Cincinnati Children’s Hospital
Medidas implementadas de acordo com as recomendações do IH para pediatria.
Educação dos profissionais envolvidos Implementação das medidas
Início em agosto de 2005 6.0/1000vm dia
Agosto de 2006 1.4/1000vm dia
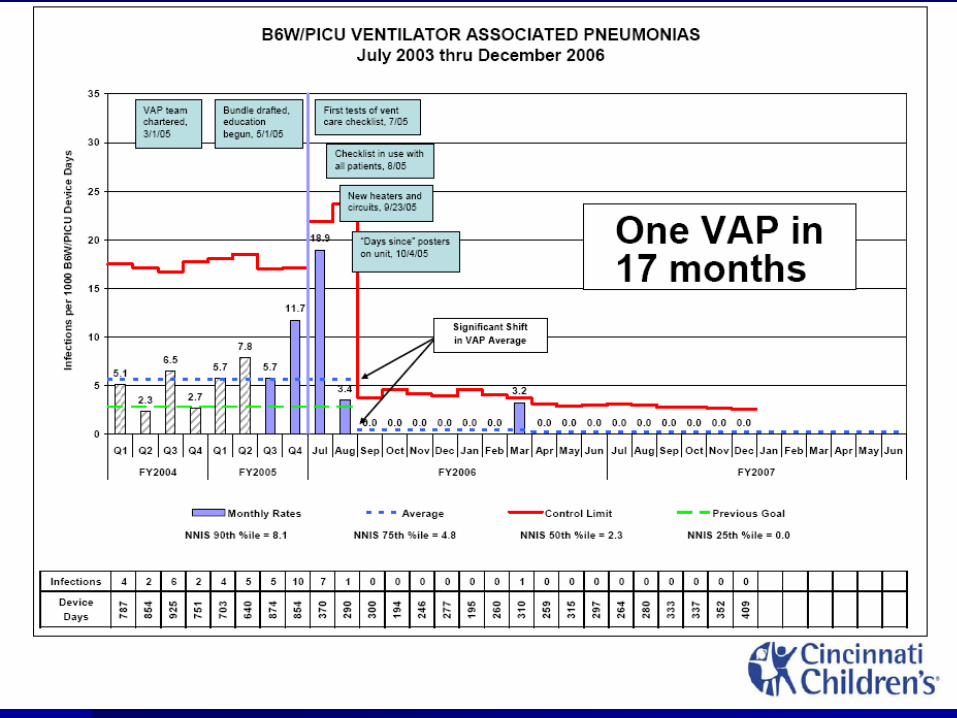

Creating and Implementing a Bundle to Reduce VAP in the NICU (IMPROVEMENT REPORT)
Cuidados com tubo endotraqueal
Instalar cord clamp apenas após IOT
Evitar ao maximo extubações não programadas .
Utilização de sistema de fechado para aspiração traqueal.
Avaliação cuidadosa para indicar intubação. Escolher suporte ventilatório menos invasivo possível
Central DuPage Hospital
Winfield, Illinois, USA - IHI

Massachusetts Hospital Association (MHA) have been offering programming to
support the prevention of hospital-acquired infections throughout the Bay State

Analise geral Bundle BCP em Neonatologia
Número maior de medidas X adulto
Medidas que se repetem: – Troca do circuito
– Sistema de aspiração fechado
– Higiene oral
– Decúbito elevado
Prevenção de úlcera gástrica?
Prevenção de trombose venosa?
AGENDA
What is a “BUNDLE”?
How to develop a BUNDLE in a NICU?
How to develop a BUNDLE in a Brazilian NICU?
How to put the BUNDLE in practice, working with “Medical Doctors…”?