impact of time to antibiotics on survival in patients with
TRANSCRIPT

Clinical Investigations
Impact of time to antibiotics on survival in patients with severesepsis or septic shock in whom early goal-directed therapy wasinitiated in the emergency department*
David F. Gaieski, MD; Mark E. Mikkelsen, MD, MSCE; Roger A. Band, MD;Jesse M. Pines, MD, MBA, MSCE; Richard Massone, MD; Frances F. Furia, MD; Frances S. Shofer, PhD;Munish Goyal, MD
I t has been estimated that onepatient presents to an emer-gency department (ED) in theUnited States with severe sepsis
or septic shock every minute, and mor-tality ranges from 25% to 50% (1, 2).Until recently, treatment options were
limited. Antibiotic therapy has longbeen one of the mainstays of treatment.New therapies have emerged in the pastdecade, including early goal-directedtherapy (EGDT), which uses an algo-rithmic resuscitation strategy, system-atically measuring and correcting cen-tral venous pressure, mean arterialpressure, and central venous oxygensaturation (ScvO2) at the most proximalphase of critical infection (3). In a ran-domized, single-center trial, EGDT pro-duced a 16% absolute reduction in in-hospital mortality. In patients withhemodynamic instability, the initialsteps of care, including establishingvascular access and fluid resuscitation,may take precedence over early antibi-otic administration (4). It is notablethat in the original EGDT trial, 13.7%of the patients in the EGDT group and7.6% of the patients in the standardtherapy group did not receive antibiot-ics during the first 6 hrs of their ED
stay (3). However, in a study by Kumaret al (5), examining the duration ofhypotension until the administration ofappropriate antimicrobials in patientswith septic shock, each hour’s delay toantibiotic administration was associ-ated with, on average, a 7.6% increasein mortality. Therefore, what priorityearly antibiotic administration shouldbe given in an algorithmic resuscitationstrategy remains unclear.
The Surviving Sepsis Campaign’s2008 “International guidelines for themanagement of severe sepsis and septicshock” recommend that appropriate an-timicrobial therapy be administeredwithin 1 hr of recognition of severesepsis or septic shock (4). The recom-mendation was primarily based on thestudy by Kumar et al (5) and on oneother retrospective study (6). Given thecompeting demands that exist in manyEDs, administration of antimicrobialtherapy within this 1-hr time frame can
*See also p. 1211.From the Department of Emergency Medicine
(DFG, JMP, RAB, RM, FFF, FSS), Division of Pulmonary,Allergy, and Critical Care, Department of Medicine(MEM), the Center for Clinical Epidemiology and Bio-statistics (JMP, MEM), and the Leonard Davis Institutefor Health Economics (JMP), University of Pennsylva-nia, Philadelphia, PA; and the Department of Emer-gency Medicine (MG), Washington Hospital Center,Georgetown University School of Medicine, Washing-ton, DC.
The authors have not disclosed any potential con-flicts of interest.
For information regarding this article, E-mail:[email protected]
Copyright © 2010 by the Society of Critical CareMedicine and Lippincott Williams & Wilkins
DOI: 10.1097/CCM.0b013e3181cc4824
Objective: To study the association between time to antibioticadministration and survival in patients with severe sepsis orseptic shock in whom early goal-directed therapy was initiated inthe emergency department.
Design: Single-center cohort study.Setting: The emergency department of an academic tertiary
care center from 2005 through 2006.Patients: Two hundred sixty-one patients undergoing early
goal-directed therapy.Interventions: None.Measurements and Main Results: Effects of different time
cutoffs from triage to antibiotic administration, qualification forearly goal-directed therapy to antibiotic administration, triage toappropriate antibiotic administration, and qualification for earlygoal-directed therapy to appropriate antibiotic administration onin-hospital mortality were examined. The mean age of the 261patients was 59 � 16 yrs; 41% were female. In-hospital mortalitywas 31%. Median time from triage to antibiotics was 119 mins(interquartile range, 76–192 mins) and from qualification to an-
tibiotics was 42 mins (interquartile range, 0–93 mins). There wasno significant association between time from triage or time fromqualification for early goal-directed therapy to antibiotics andmortality when assessed at different hourly cutoffs. When ana-lyzed for time from triage to appropriate antibiotics, there was asignificant association at the <1 hr (mortality 19.5 vs. 33.2%;odds ratio, 0.30 [95% confidence interval, 0.11–0.83]; p � .02)time cutoff; similarly, for time from qualification for early goal-directed therapy to appropriate antibiotics, a significant associ-ation was seen at the <1 hr (mortality 25.0 vs. 38.5%; oddsratio, 0.50 [95% confidence interval, 0.27–0.92]; p � .03) timecutoff.
Conclusions: Elapsed times from triage and qualification forearly goal-directed therapy to administration of appropriate anti-microbials are primary determinants of mortality in patients withsevere sepsis and septic shock treated with early goal-directedtherapy. (Crit Care Med 2010; 38:1045–1053)
KEY WORDS: sepsis; early goal-directed therapy; antimicrobialtiming; appropriateness; outcomes; resuscitation
1045Crit Care Med 2010 Vol. 38, No. 4

be a difficult task to accomplish unlessspecific protocols are implemented tostreamline ordering and delivery of an-tibiotics. The 2006 Emergency Depart-ment Management Guidelines (7) cre-ated by the ED-SEPSIS Working Groupstate, “Although there are insufficientdata to conclude that delays on the or-der of hours are deleterious, adminis-tration of antibiotics within the time ofED care and as soon as possible oncethere is a reasonable suspicion of severesepsis/septic shock will likely increasethe chance of favorable outcome com-pared with later administration.”
We studied the impact of antibiotictiming on survival in patients receivinga standardized resuscitation algorithm(EGDT) for severe sepsis or septic shockin our ED. We hypothesized that earlieradministration of antimicrobial therapyin patients receiving EGDT (within thetime frame recommended by the Sur-viving Sepsis Campaign) would be asso-ciated with improved survival.
MATERIALS AND METHODS
Study Design and Setting. After obtainingapproval from our Institutional Review Board,we conducted a retrospective analysis of a co-hort of patients with severe sepsis and septicshock treated with EGDT in the Hospital ofthe University of Pennsylvania’s ED betweenJanuary 5, 2005, and December 31, 2006. TheHospital of the University of Pennsylvania isan urban, tertiary care medical center with anannual ED volume of approximately 55,000adult patients.
Inclusion Criteria. Inclusion criteria in-cluded 1) inclusion in the severe sepsis andseptic shock database; 2) initiation of EGDT(defined as algorithmic volume resuscitation,placement of central venous catheter, andmeasurement of central venous pressure,mean arterial pressure, and ScvO2) during thepatient’s ED stay.
Data Collection. The data used in thisstudy were part of a prospective quality im-provement initiative to evaluate the impactof an EGDT program on survival in patientswith severe sepsis and septic shock in theHospital of the University of PennsylvaniaED (see Appendix A for EGDT protocol).Generally accepted definitions of severe sep-sis and septic shock were used (Appendix B)(8). Patients qualified for EGDT if they had:1) cryptic septic shock, defined as severesepsis with a lactate �4 mmol/L as a markerof significant tissue hypoperfusion; or 2)septic shock as defined in Appendix B (3).The EGDT program started actively treatingpatients in January 2005, and two authors(DFG, MG) were contacted by pager or e-mail about all of the patients included in the
present study. More than 150 data pointswere collected per patient. Severity of illnesswas calculated using an ED Acute Physiol-ogy and Chronic Health Evaluation II score(3, 9, 10). There were no specific recommen-dations in the EGDT protocol regarding an-tibiotic timing or type; however, an ED-based severe sepsis antibiogram (AppendixB) was available for guidance in antibioticchoice if desired. Data were recorded usingstandard database software (Access; Mi-crosoft Corporation, Redmond, WA). Theretrospective study was completed in accor-dance with established standards for chartreviews in emergency medicine (11, 12).Data entry on standardized forms was doneby five data entry personnel (one emergencymedicine attending; one critical care fellow;two emergency medicine residents; and onemedical student), including four authors(DFG, RM, FFF, MEM), who were trainedbefore the start of the study. Each personentered a minimum of 30 charts, using a pri-ori-determined rules, available in a standard-ized glossary, for data entry in each category,including triage time, time of qualification forEGDT, time of initial antibiotic administra-tion, appropriateness of antibiotic selection,and time of appropriate antibiotic administra-tion (Appendix C). One author (DFG) met reg-ularly (at least once a month) with each dataabstractor to review data entry and to resolveconflicts about data coding and timing inter-vals. The research hypothesis was generatedafter data entry was completed and, therefore,the data abstractors were blinded to the hy-pothesis of this study. Kappa value of interra-
ter reliability comparing one investigator’s(DFG’s) assignment of time from triage toantibiotics with those of the other data entrypersonnel was calculated using Cohen’s kappacalculation.
Data Analysis. Descriptive data are pre-sented as mean (SD) for continuous data,medians with interquartile ranges (IQRs) fortime variables, and frequencies and percentsfor categorical data. We compared in-hospital mortality in patients receiving an-tibiotics at different time cutoffs, usingFisher’s exact test. We examined time toantibiotics in four ways: elapsed time fromtriage to antibiotic administration; fromqualification for EGDT to antibiotic admin-istration; from triage to appropriate antibi-otic administration; and from qualificationfor EGDT to appropriate antibiotic adminis-tration. Timing cutoffs included: �1 hr vs.�1 hr; �2 hrs vs. �2 hrs; �3 hrs vs. �3 hrs;�4 hrs vs. �4 hrs; and �5 hrs vs. �5 hrs.
Multivariable logistic regression wasused to adjust for potential confounding inthe association between time to antibioticsand in-hospital mortality. We consideredage, Acute Physiology and Chronic HealthEvaluation II score, initial lactate, initialsystolic blood pressure, initial temperature,and amount of intravenous fluid given dur-ing the first 6 hrs and over the total ED stayas potential confounders. Potential con-founders were determined a priori and wereforced into the final model. We present theadjusted odds ratio for in-hospital mortalityand 95% confidence interval. Statistical sig-nificance was defined as a p value �.05. To
Table 1. Baseline characteristics of patients (n � 261)
Variable Value SD or IQR Range
Age, yrs 59 16.1 22–101Female gender, % 41Race
Black, % 48White, % 43Other, % 9
APACHE II score 17.9 6.4Qualified for EGDT at presentation to ED, % 47SIRS criteria
Temperature, °F 99.2 2.7 91.7–107.0Heart rate, beats/min 115.2 25.9 30–182Respiratory rate, breaths/min 22.1 7.3 6–64Partial pressure of CO2, mm Hg 34.5 11.4 12–95White blood count, per mm3 14.7 10.9 0.1–90.5
Early goal-directed therapy criteriaSystolic blood pressure, mm Hg 107.8 27.2 32–173Lactate, mmol/L 5.6 3.6 0.8–26.5
Baseline laboratory valuesHemoglobin, mg/dL 11.8 2.9 2.8–19.8Platelets, per mm3 233.0 156.0 5–1098CO2, mg/dL 20.6 6.5 1–56International normalized ratio 1.46 0.59 1–�50Total bilirubin, mg/dL 2.5 4.0 0.1–26.6
IQR, interquartile range; APACHE, Acute Physiology and Chronic Health Evaluation; EGDT, earlygoal-directed therapy; ED, emergency department; SIRS, systemic inflammatory response syndrome.
1046 Crit Care Med 2010 Vol. 38, No. 4

calculate the probability of death, we used amarginal standardization approach whereinwe used the estimates from the multivari-able logistic regression to determine the av-erage predicted probability of death for agiven group (13). Statistical analyses wereperformed using SAS (version 9.1; SAS In-stitute, Cary, NC) and STATA (version 10;StataCorp, College Station, TX) statisticalsoftware.
RESULTS
The average age of the 261 patientsreceiving EGDT studied was 59 � 16yrs; 41% were female; 48% were black,and 43% were white. Forty-seven per-cent (n � 123) of the patients qualifiedfor EGDT at triage; 53% (n � 138)qualified later during their ED stay.Cryptic shock was the qualifying diag-nostic category for 48% (n � 126) ofthe patients; septic shock was the qual-ifying diagnostic category for the re-maining 52% (n � 135). Mean AcutePhysiology and Chronic Health Evalua-tion II score was 17.9 � 6.4 (Table 1).
All patients received antibiotics dur-ing their ED course. The median lengthof time from triage to antibiotics was119 mins (IQR, 76 –192 mins); fromqualification for EGDT to antibioticswas 42 mins (IQR, 0 –93 mins); fromtriage to appropriate antibiotics was127 mins (IQR, 79 –224 mins); and fromqualification for EGDT to appropriateantibiotics was 47 mins (IQR, 0 –108mins). Kappa value of interrater reli-ability for time to antibiotics � 0.91.The most common sources of infectionwere: respiratory (30.6%), genitouri-nary (22.8%), gastrointestinal (19.7%),and primary bacteremia (14.9%) (Table2). Cultures were positive in 148(56.7%) patients. Our ED antibiogramwas followed in all of the culture-negative cases (Appendix B); 126(85.1%) of the culture-positive cases re-ceived appropriate initial antibioticcoverage during their ED stay; 22(14.9%) of the culture-positive caseswere initially given inappropriate anti-biotics. Two patients who initially re-ceived inappropriate antibiotics weresubsequently given appropriate antibi-otics before transfer from the ED.
In-hospital mortality was 31.0% forthe cohort as a whole; it was 35.1% forculture-positive patients vs. 25.7% (p �.11) for culture-negative patients (Table3). Mortality for culture-positive pa-tients who received appropriate initialantibiotics in the ED was 32.5%; mor-
tality for culture-positive patients whodid not receive appropriate initial anti-biotics in the ED was 50.0% (p � .15).
We found no relationship betweentime from triage to administration ofantibiotics and mortality outcome afteradjusting for potential confounders.The lack of relationship between time ofantibiotic administration and mortalityoutcome extended to �5 hrs from tri-age to antibiotic administration. Simi-larly, we found no relationship betweentime from qualification for EGDT toantibiotic administration and mortality.In the analysis examining time fromtriage to appropriate antibiotic admin-istration, mortality was significantlydecreased when antibiotics were givenin �1 hr vs. �1 hr. Finally, in theanalysis examining time from qualifica-tion for EGDT to appropriate antibiot-ics, mortality was significantly de-creased when antibiotics were given in�1 hr vs. �1 hr (Tables 4–7; Figs. 1– 4).
Table 2. Source of infection
Source Percent
Respiratory 30.6Genitourinary 22.8Gastrointestinal 19.7Primary bacteremia 14.9Skin/soft tissue 7.5Central venous catheter 5.9Central nervous system 2.4Surgical site 2.0Endocarditis 1.6Other 5.8Total 306 sites
Forty-three patients had two or more primarysources.
Table 3. Culture results
Number Percent
Total patients 261Culture-negative patients 113 43.3Culture-positive patients 148 56.7
Urine 71 27.2Blood 83 31.8Other 50 19.2Polymicrobial 25 9.6Multiple sources 42 16.1
Total positive cultures 204 N/AGram-positive organisms 67 25.7
Enterococcus 18 6.9Streptococcus pneumoniae 14 5.4MSSA 14 5.4MRSA 8 3.1Group B Streptococcus 5 2.0Streptococcus viridans 4 1.5Other staphylococci
(S. hominis, S. lugdunensis)3 1.2
Group A Streptococcus 1 0.4Gram-negative organisms 96 36.6
Escherichia coli 30 11.5Klebsiella 21 8.0Pseudomonas species 15 5.7Citrobacter 6 2.3Acinetobacter 5 1.9Enterobacter species 5 1.9Proteus mirabilis 4 1.5Haemophilus influenzae 2 0.8Serratia 2 0.8Stenotrophomonas 1 0.4Morganella 1 0.4Other gram-negative organisms 4 1.5
Anaerobic organisms 9 3.4Clostridium difficile 4 1.5Bacteroides fragilis 3 1.2Other Clostridia 1 0.4
Fungi 6 2.3Candida albicans 5 1.9Candid glabrata 1 0.4
Legionella species 1 0.4
MSSA, methicillin-sensitive Staphylococcus aureus; MRSA, methicillin-resistant S. aureus; N/A,not applicable.
1047Crit Care Med 2010 Vol. 38, No. 4

These findings were supported by thesensitivity analyses at other time cut-offs. Similar results were seen when thepatients were divided into two catego-ries (patients with cryptic shock andpatients with septic shock), which weresubsequently analyzed as described pre-viously (not shown in tables).
DISCUSSION
Severe sepsis and septic shock arevexing healthcare problems in theUnited States and around the world.There is a large burden of disease andhigh mortality; outcomes have, untilrecently, remained relatively static, and
the incidence is increasing. The optimaltreatment strategy is constantly evolv-ing and includes initial resuscitation,rapid diagnosis, timely administrationof appropriate antibiotics, source iden-tification and control, and meticulousED and intensive care unit (ICU) man-agement. The question of how antibi-otic administration should be priori-tized in the initial resuscitationsequence of patients with severe sepsisand septic shock has been unanswered.We hypothesized that earlier antibioticadministration would be associatedwith lower in-hospital mortality in pa-tients treated with a uniform resuscita-tion strategy (EGDT). We examinedtime from triage to antibiotic adminis-tration (a commonly tracked perfor-mance measure) and time from quali-fication for EGDT to antibiotic admin-istration, which is much more in keep-ing with the Surviving Sepsis Cam-paign’s recommendation of rapidantibiotic administration after recogni-tion of severe sepsis or septic shock.The results of our study identify threeimportant factors in the relationshipbetween mortality and timing of antibi-otic administration in severe sepsis andseptic shock: 1) the time the patientqualified for EGDT; 2) the length oftime from triage to administration ofappropriate antibiotics; and 3) thelength of time from qualification forEGDT to administration of appropriateantibiotics. Based on the results of thisstudy, we recommend that practitio-ners administer appropriate antibioticsas rapidly as possible once there is areasonable suspicion of severe sepsisand septic shock and place a high pri-ority on developing systems to stream-line their timely administration. Appro-priate antibiotics should be givenwithin 1 hr of qualification for EGDT.Of note, in our study, there were onlyfive patients (four of whom died) whoreceived inappropriate antibioticswithin 1 hr of triage and only 10 pa-tients (five of whom died) who receivedinappropriate antibiotics within 1 hr ofqualification for EGDT. Given this, themortality benefit of timely antibiotics islikely driven by the timely administra-tion of appropriate antibiotics.
Our findings support the recommen-dations on timeliness of antibiotic ad-ministration published by the SurvivingSepsis Campaign. Their recommenda-tions are based primarily on expertopinion and the results of two retro-
Table 4. In-hospital mortality: Triage to ED antibiotics
Adjusted
Cutoffs NumberMortality,
%Difference,
% OR 95% CI pProbabilityof Death
�1 hr 46 26.1 6.0 0.51 0.21–1.22 .13 .20 vs. .28�1 hr 215 32.1�2 hrs 136 30.9 0.3 0.72 0.38–1.37 .30 .25 vs. .28�2 hrs 125 31.2�3 hrs 187 29.4 5.7 0.64 0.32–1.29 .21 .25 vs. .31�3 hrs 74 35.1�4 hrs 217 30.0 6.4 0.80 0.35–1.84 .59 .27 vs. .29�4 hrs 44 36.4�5 hrs 237 32.1 �11.2 0.86 0.56–6.15 .31 .28 vs. .16�5 hrs 24 20.8
ED, emergency department; OR, odds ratio; CI, confidence interval.
Table 5. In-hospital mortality: Qualified for EGDT to ED antibiotics
Adjusted
Cutoffs NumberMortality,
%Difference,
% OR 95% CI pProbabilityof Death
�1 hr 154 26.6 10.8 0.58 0.31–1.08 .09 .22 vs. .34�1 hr 107 37.4�2 hrs 218 29.8 7.4 0.77 0.34–1.70 .51 .26 vs. .34�2 hrs 43 37.2�3 hrs 239 30.1 10.8 0.62 0.23–1.69 .36 .26 vs. .39�3 hrs 22 40.9�4 hrs 252 30.6 13.9 0.77 0.17–3.59 .74 .27 vs. .37�4 hrs 9 44.4�5 hrs 257 31.1 �6.1 1.33 0.12–14.20 .82 .27 vs. .24�5 hrs 4 25.0
EGDT, early goal-directed therapy; ED, emergency department; OR, odds ratio; CI, confidenceinterval.
Table 6. In-hospital mortality: Time from triage to appropriate antibiotics
Adjusted
Cutoffs NumberMortality,
%Difference,
% OR 95% CI pProbabilityof Death
�1 hr 41 19.5 13.7 0.30 0.11–0.83 .02 .13 vs. .29�1 hr 220 33.2�2 hrs 124 28.2 5.4 0.54 0.29–1.03 .06 .22 vs. .31�2 hrs 137 33.6�3 hrs 172 27.9 9.2 0.53 0.27–1.01 .05 .23 vs. .34�3 hrs 89 37.1�4 hrs 200 28.5 10.8 0.62 0.31–1.24 .18 .25 vs. .34�4 hrs 61 39.3�5 hrs 218 30.7 1.8 0.82 0.37–1.79 .62 .27 vs. .29�5 hrs 43 32.6
OR, odds ratio; CI, confidence interval.
1048 Crit Care Med 2010 Vol. 38, No. 4
spective studies (5, 6). The first studydemonstrated a logarithmic relation-ship between the duration of hypoten-sion before administration of appropri-ate antimicrobials and mortality inpatients admitted to the ICU with septicshock. Direct admissions from the EDaccounted for 44.4% of the patients in-cluded. In this study, each hour’s delayfrom the onset of hypotension to ad-ministration of appropriate antibioticswas associated with an average increasein in-hospital mortality of 7.6% (5). Thesecond study found that delaying anti-fungal therapy for �12 hrs after theinitial positive fungal culture wasdrawn was an independent predictor ofhospital mortality (6).
How early is early enough for anti-biotic administration in severe sepsisand septic shock? A handful of recentstudies have attempted to answer thisquestion. For example, a retrospectiveanalysis of patients with severe pneu-monia resulting from Legionella pneu-mophilia, found that delays to antibi-otic administration �8 hrs from ICUadmission were associated with in-creased mortality (14). Another retro-spective study examining predictors of30-day mortality in critically ill patientswith cancer with septic shock foundthat mortality was increased when timefrom ICU admission to first antibioticadministration was �2 hrs (15). Fi-nally, the Finnsepsis Study Group (16)examined how early treatment guide-lines, including early antibiotic admin-istration and early hemodynamic opti-mization, were being adopted in thetreatment of septic shock in Finland.They examined 92 patients with septicshock admitted from the ED to the ICU,dividing them into patients receivingantibiotics in �3 hrs vs. �3 hrs fromED admission. They found that a “de-layed start of antibiotics was the mostsignificant individual early treatmentvariable resulting in increased mortal-ity.” However, compliance with EGDTscreening and resuscitation end pointswas unsatisfactory in their cohort: lac-tate measurement occurred during thefirst 6 hrs in 58%; antibiotics weregiven in �3 hrs in 53%; central venouspressure was measured during the first6 hrs in 37%; mean arterial pressure�65 mm Hg was achieved in 74%; andScvO2 was measured within 6 hrs in19.6%. This variability of care makes ithard to generalize from the patientswith septic shock in their cohort to a
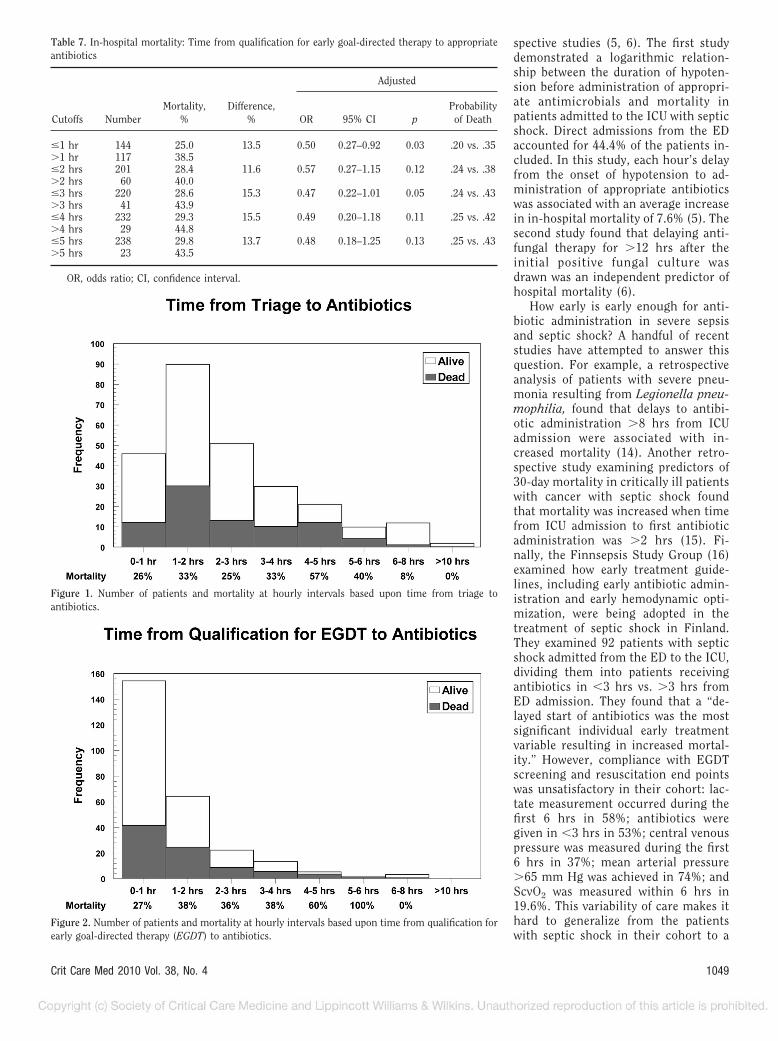
Figure 1. Number of patients and mortality at hourly intervals based upon time from triage toantibiotics.
Figure 2. Number of patients and mortality at hourly intervals based upon time from qualification forearly goal-directed therapy (EGDT) to antibiotics.
Table 7. In-hospital mortality: Time from qualification for early goal-directed therapy to appropriateantibiotics
Adjusted
Cutoffs NumberMortality,
%Difference,
% OR 95% CI pProbabilityof Death
�1 hr 144 25.0 13.5 0.50 0.27–0.92 0.03 .20 vs. .35�1 hr 117 38.5�2 hrs 201 28.4 11.6 0.57 0.27–1.15 0.12 .24 vs. .38�2 hrs 60 40.0�3 hrs 220 28.6 15.3 0.47 0.22–1.01 0.05 .24 vs. .43�3 hrs 41 43.9�4 hrs 232 29.3 15.5 0.49 0.20–1.18 0.11 .25 vs. .42�4 hrs 29 44.8�5 hrs 238 29.8 13.7 0.48 0.18–1.25 0.13 .25 vs. .43�5 hrs 23 43.5
OR, odds ratio; CI, confidence interval.
1049Crit Care Med 2010 Vol. 38, No. 4

group of patients managed with a moreuniform resuscitation strategy.
How do our findings diverge fromthose of prior studies investigating therelationship between time to antibioticsand mortality in patients with septicshock? All 261 patients in our cohortunderwent hemodynamic optimizationduring the first 6 hrs of their hospitalpresentation. This included assessmentof serum lactate, early volume resusci-tation, and invasive monitoring for cen-tral venous pressure, mean arterialpressure, and ScvO2. Despite variationsin presentation, the median time fromtriage to antibiotics was 119 mins,97.6% received antibiotics within 6 hrsof triage, and all of the patients receivedantibiotics before transfer from the ED
to the ICU. Within this aggressive, uni-form resuscitation strategy at the mostproximal point of critical infection,time from qualification for EGDT toappropriate antibiotic administrationhad a significant effect on in-hospitalmortality outcome. This effect was notpresent when time from triage to anti-biotic administration was analyzed; thissuggests that the commonly used per-formance measure of time from triageto antibiotics in diseases such as pneu-monia needs to be modified to take intoaccount the appropriateness of the an-tibiotics that were given and the patho-physiological implications of the timeof onset of hemodynamic instability.We did not find the logarithmicchanges in mortality seen in the study
of Kumar et al, and we hypothesize thatthe reason for this is threefold: 1) in thestudy of Kumar et al, the median timeto appropriate antibiotics was 6 hrs(IQR � 2–15 hrs), whereas in our study,it was just over 2 hrs (127 mins [IQR,79 –224 mins]); 2) resuscitation strate-gies were heterogeneous over time andlocation in the study of Kumar et al,whereas a single, algorithmic hemody-namic optimization strategy initiated inthe ED was used in all patients in ourstudy; and 3) the study of Kumar et albenefited from a much larger samplesize.
Results of animal studies using anintra-abdominal sepsis model suggest acritical inflection point between 12 and15 hrs after induction of septic shock;this inflection point coincides with theonset of persistent hypotension and thedevelopment of significant lactic acido-sis. When antibiotic administration isdelayed beyond this point, mortality in-creases dramatically (17). Our data areconsistent with this finding and suggestthat a similar inflection point exists inpatients presenting to the ED with se-vere infections, who qualify for goal-directed hemodynamic optimizationstrategies. This inflection point may co-incide with triage (47% of our patientsqualified for EGDT at triage) or maydevelop during the initial hours of eval-uation and treatment in the ED (53% ofour patients qualified at some point af-ter triage). When appropriate antibiot-ics are administered before or coinci-dent with this inflection point,mortality is significantly lower thanwhen appropriate antibiotic adminis-tration is delayed beyond that point.Our findings support the SurvivingSepsis Campaign’s recommendation ofantibiotic administration within 1 hr ofrecognition of septic shock and suggestthat the recommendations from theED-SEPSIS Working Group that “ad-ministration of antibiotics within thetime of ED care and as soon as possibleonce there is a reasonable suspicion ofsevere sepsis/septic shock will likely in-crease the chance of favorable outcomecompared with later administration”are not rigorous enough given our cur-rent understanding of the role of appro-priate antibiotics in the treatment oflife-threatening severe sepsis.
This study has several limitations. Itwas performed at a single center usinga uniform, algorithmic resuscitationstrategy, and caution should be taken in
Figure 3. Number of patients and mortality at hourly intervals based upon time from triage toappropriate antibiotics.
Figure 4. Number of patients and mortality at hourly intervals based upon time from qualification forearly goal-directed therapy (EGDT) to appropriate antibiotics.
1050 Crit Care Med 2010 Vol. 38, No. 4

generalizing these results to the treat-ment of patients with severe sepsis andseptic shock in institutions with differ-ent resources or that use other manage-ment strategies. Despite analyzing ourdata from multiple perspectives, wecannot rule out that sicker patients re-ceived antibiotics sooner and that theresults are confounded by these pa-tients being at higher risk of death;however, this confounding should biastoward the null. It is possible that dif-ferences in times to EGDT end pointsnot considered in this analysis played arole in mortality outcome. In addition,it is possible that the fact that one au-thor met with the other data abstrac-tors on a regular basis to address ques-tions about data entry injected biasinstead of accuracy into time calcula-tions and classification assignments.Because of overall sample size, we mayhave been unable to demonstrate anhour-to-hour increase that would bepresent in a larger cohort.
CONCLUSIONS
Our study demonstrates that timefrom qualification for EGDT to admin-istration of appropriate antibiotics is animportant determinant of outcome inpatients with severe sepsis and septicshock who qualify for hemodynamic op-timization strategies. Administration ofappropriate antibiotics is one of manyearly resuscitation interventions thatmust be performed as soon as possiblein patients with critical infections. Ap-propriate antibiotics should be admin-istered within 1 hr of qualification forEGDT. However, the exact timing of theantibiotic administration must be tai-lored to the resuscitation of the specificpatient and will depend on the priorityof interventions in the individual pa-tient including airway management,volume resuscitation, vasopressor ad-ministration, correction of myocardialdysfunction, and source control. In
general, the delivery of antibioticsneeds to be moved toward the begin-ning of this resuscitation algorithm,and protocols and systems must be de-veloped to ensure the timely adminis-tration of potentially life-saving antibi-otics. These include identifyingantibiotics that can be given rapidly byintravenous push vs. those that requireinfusion over an extended time frame.Also, the central antibiotics in an institu-tion’s severe sepsis and septic shock an-tibiogram must be immediately availablein the ED and ICUs, eliminating delays toorder, prepare, and deliver medicationsfrom centralized pharmacies.
ACKNOWLEDGMENTS
The investigators recognize the in-valuable contributions of Andrea Miltia-des, BA, to data abstraction and data en-try for this study.
REFERENCES
1. Wang HE, Shapiro NI, Angus DC, et al: Na-tional estimates of severe sepsis in UnitedStates emergency departments. Crit CareMed 2007; 35:1928–1936
2. Angus DC, Linde-Zwirble WT, Lidicker J, etal: Epidemiology of severe sepsis in theUnited States: Analysis of incidence, out-come, and associated costs of care. CriticalCare Medicine 2001; 29:1303–1310
3. Rivers E, Nguyen B, Havstad S, et al: Earlygoal-directed therapy in the treatment of se-vere sepsis and septic shock. N Engl J Med2001; 345:1368–1377
4. Dellinger RP, Levy MM, Carlet JM, et al:International guidelines for management ofsevere sepsis and septic shock: 2008. CritCare Med 2008; 36:296–327
5. Kumar A, Roberts D, Wood KE, et al: Dura-tion of hypotension before initiation of effec-tive antimicrobial therapy is the critical de-terminant of survival in human septic shock.Crit Care Med 2006; 34:1589–1596
6. Morrell M, Fraser VJ, Kollef MH: Delayingthe empiric treatment of candida blood-stream infection until positive blood cultureresults are obtained: A potential risk factor
for hospital mortality. Antimicrob AgentsChemother 2005; 49:3640–3645
7. Nguyen HB, Rivers EP, Abrahamian FM,et al: Review of the literature and emer-gency department management guidelines.Ann Emerg Med 2006; 48:28 –54
8. Levy MM, Fink MP, Marshall JC, et al: Inter-national Sepsis Definitions C. 2001 SCCM/ESICM/ACCP/ATS/SIS International SepsisDefinitions Conference. Intensive Care Med2003; 29:530–538
9. Nguyen HB, Corbett SW, Menes K, et al:Early goal-directed therapy, corticosteroid,and recombinant human activated protein Cfor the treatment of severe sepsis and septicshock in the emergency department. AcadEmerg Med 2006; 13:109–113
10. Shapiro NI, Howell MD, Talmor D, et al:Implementation and outcomes of the Mul-tiple Urgent Sepsis Therapies (MUST) pro-tocol. Crit Care Med 2006; 34:1025–1032
11. Gilbert EH, Lowenstein SR, Koziol-McLain J,et al: Chart reviews in emergency medicineresearch: Where are the methods? AnnEmerg Med 1996; 27:305–308
12. Lowenstein SR: Medical record reviews inemergency medicine: The blessing and thecurse. Ann Emerg Med 2005; 45:452– 455
13. Localio A, Margolis D, Berlin J: Relative risksand confidence intervals were easily com-puted indirectly from multivariable logisticregression. J Clin Epidemiol 2007; 60:874–882
14. Gacouin A, Le Tulzo Y, Lavoue S, et al: Se-vere pneumonia due to Legionella pneumo-phila: Prognostic factors, impact of delayedappropriate antimicrobial therapy. IntensiveCare Med 2002; 28:686–691
15. Larche J, Azoulay E, Fieux F, et al: Improvedsurvival of critically ill cancer patients withseptic shock. Intensive Care Med 2003; 29:1688–1695
16. Varpula M, Karlsson S, Parviainen I, et al:Community-acquired septic shock: Earlymanagement and outcome in a nationwidestudy in Finland. Acta Anaesthesiol Scand2007; 51:1320–1326
17. Kumar A, Haery C, Paladugu B, et al: Theduration of hypotension before the initia-tion of antibiotic treatment is a criticaldeterminant of survival in a murine modelof Escherichia coli septic shock: Associa-tion with serum lactate and inflammatorycytokine levels. J Infect Dis 2006; 193:251–258
1051Crit Care Med 2010 Vol. 38, No. 4
APPENDIX B: A PRIORI RULESFOR DEFINING SEPTIC SHOCK,CRYPTIC SHOCK, ANDQUALIFICATION FOR EARLYGOAL-DIRECTED THERAPY,ASSIGNING TIMES TOQUALIFICATION FOR EARLYGOAL-DIRECTED THERAPY ANDANTIBIOTIC ADMINISTRATION,AND ASSESSINGAPPROPRIATENESS OFANTIBIOTIC ADMINISTRATION
Definitions of Septic Shock and Cryp-tic Shock. Generally accepted defini-tions of severe sepsis and septic shockwere used: 1) severe sepsis was definedas two or more systemic inflammatoryresponse syndrome criteria: tempera-ture �96°F or �100.4°F; heart rate�90 beats/min; respiratory rate �20breaths/min or PaCO2 �32 mm Hg; andwhite blood cell count �4000/mm3,�12,000/mm3, or �10% bands; a pre-sumed or documented source of infec-tion; and at least one organ dysfunc-tion, including change in mentalstatus, acute renal dysfunction, plate-lets �100/mm3, lactate �3 mmol/L,and total bilirubin �4 mg/dL amongothers; septic shock was defined as twoor more systemic inflammatory re-sponse syndrome criteria, a presumedor documented source of infection, anda systolic blood pressure (SBP) �90mm Hg after a fluid challenge of 20 to30 mL/kg over 30 mins; a patient wasalso considered to be in septic shock iftheir SBP remained at least 40 mm Hgbelow a well-documented baseline SBPafter 20- to 30-mL/kg fluid challengeover 30 mins (8); conversely, if a patienthad a well-documented baseline lowSBP (between 75 and 90 mm Hg), thenthey were not considered to be in septicshock if their blood pressure was in thisrange. Cryptic shock was defined as se-vere sepsis with a lactate �4 mmol/L asa marker of significant tissue hypoper-fusion (3).
Definition of Qualified at Triage. Pa-tients were classified as “qualifying forEGDT at triage” if they were hypoten-sive in triage and remained so duringtheir initial intravenous fluid resuscita-tion in the ED (20 –30 mL/kg); if theybecame hypotensive during the first60 mins after triage and that hypoten-sive reading occurred after adequateinitial fluid resuscitation (20 –30 mL/
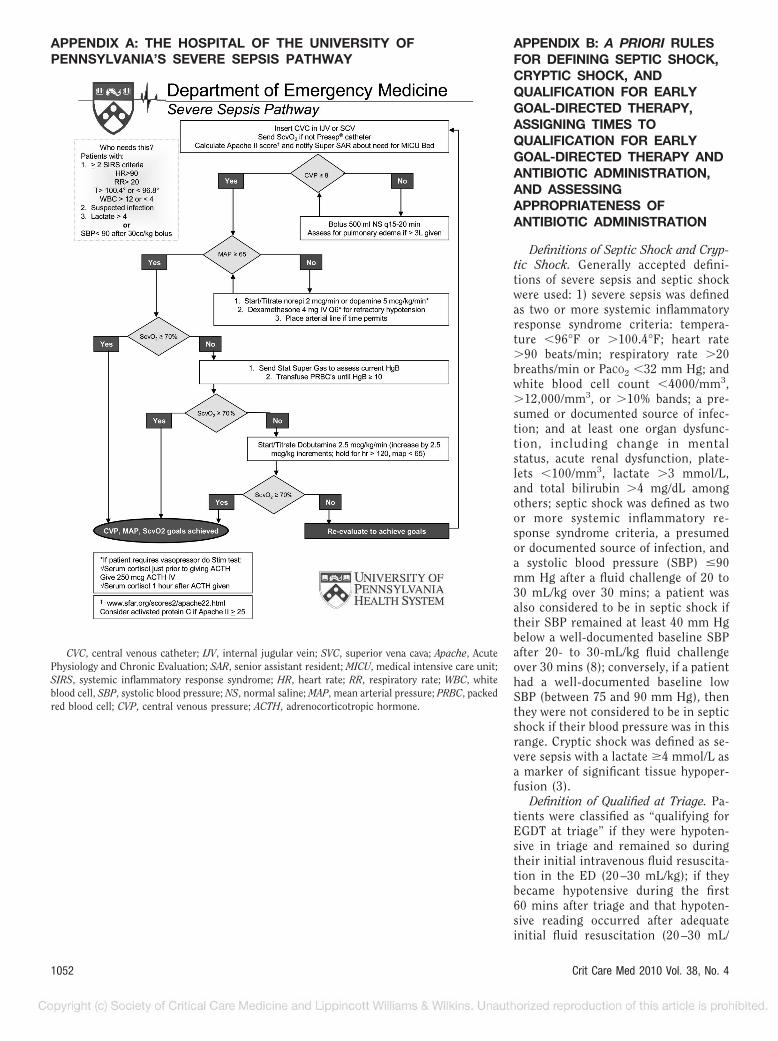
APPENDIX A: THE HOSPITAL OF THE UNIVERSITY OFPENNSYLVANIA’S SEVERE SEPSIS PATHWAY
CVC, central venous catheter; IJV, internal jugular vein; SVC, superior vena cava; Apache, AcutePhysiology and Chronic Evaluation; SAR, senior assistant resident; MICU, medical intensive care unit;SIRS, systemic inflammatory response syndrome; HR, heart rate; RR, respiratory rate; WBC, whiteblood cell, SBP, systolic blood pressure; NS, normal saline; MAP, mean arterial pressure; PRBC, packedred blood cell; CVP, central venous pressure; ACTH, adrenocorticotropic hormone.
1052 Crit Care Med 2010 Vol. 38, No. 4

kg); or if they had an elevated serumlactate (�4 mmol/L as a marker of sig-nificant tissue hypoperfusion) resultavailable on the ED electronic medicalrecord within 1 hr of triage. If thesecriteria were not met and the patientqualified at a later point, they were clas-sified as “not qualifying for EGDT attriage.”
Time From Triage to Antibiotic Ad-ministration. For analysis of time fromtriage to antibiotic administration,time zero was considered triage time orroom time, whichever time was earlier,and time of antibiotic administrationwas considered the time the first anti-biotic was started by the nurse caringfor the patient.
For analysis of time from qualifica-tion for EGDT to antibiotic administra-tion, time zero for cryptic shock wasconsidered the time the lactate value�4 mmol/L was received on the EDelectronic medical record and for septicshock was the time of the first hypoten-sive reading (SBP �90 mm Hg or �40mm Hg below baseline) after adequatevolume resuscitation (20 –30 mL/kg) orthe time of onset of hypotension if theSBP was always �90 mm Hg or �40mm Hg below baseline during the ini-tial resuscitation. For these patients,time of antibiotic administration wasconsidered the time the first antibioticwas started by the nurse caring for thepatient. Time from triage to appropriateantibiotic administration and time fromqualification for EGDT to appropriateantibiotic administration were defined
using the same time zero points givenpreviously, and defining time of appro-priate antibiotic administration as the timethe antibiotic covering the causative organ-ism was started, up to 36 hrs after triage orqualification; if the time of administrationof appropriate antibiotics was �36 hrs fromtime zero, the time to administration wasconsidered 36 hrs.
Appropriate Antibiotics. Appropriateantibiotics were defined as: 1) antibiotics
for which the causative pathogens weresensitive in vitro; 2) in cases of polymi-crobial infection, all pathogens felt tobe contributing to severe sepsis or sep-tic shock had to be covered by antibi-otics for which the organisms were sen-sitive in vitro; and 3) in cases ofculture-negative severe sepsis or septicshock, broad-spectrum antibiotics ap-propriate for the presumed site of in-fection.
APPENDIX C: EMERGENCY DEPARTMENT SEVERE SEPSISANTIBIOGRAM
PCN, penicillin; CNS, central nervous system; ETOH, ethyl alcohol; TPN, total parenteral nutrition.
1053Crit Care Med 2010 Vol. 38, No. 4