impact of respiratory compromise in u.s. healthcare · impact of respiratory compromise in ......
TRANSCRIPT
Lee A. Fleisher, M.D.
Robert D. Dripps Professor and Chair
Department of Anesthesiology and Critical Care
Professor of Medicine
Impact of Respiratory Compromise in
U.S. Healthcare

“Respiratory compromise” (RC) is defined as a state in
which there is a high likelihood of decompensation into
respiratory failure or death, but in which continuous
monitoring and early intervention might prevent or mitigate
decompensation.
Respiratory Compromise Institute
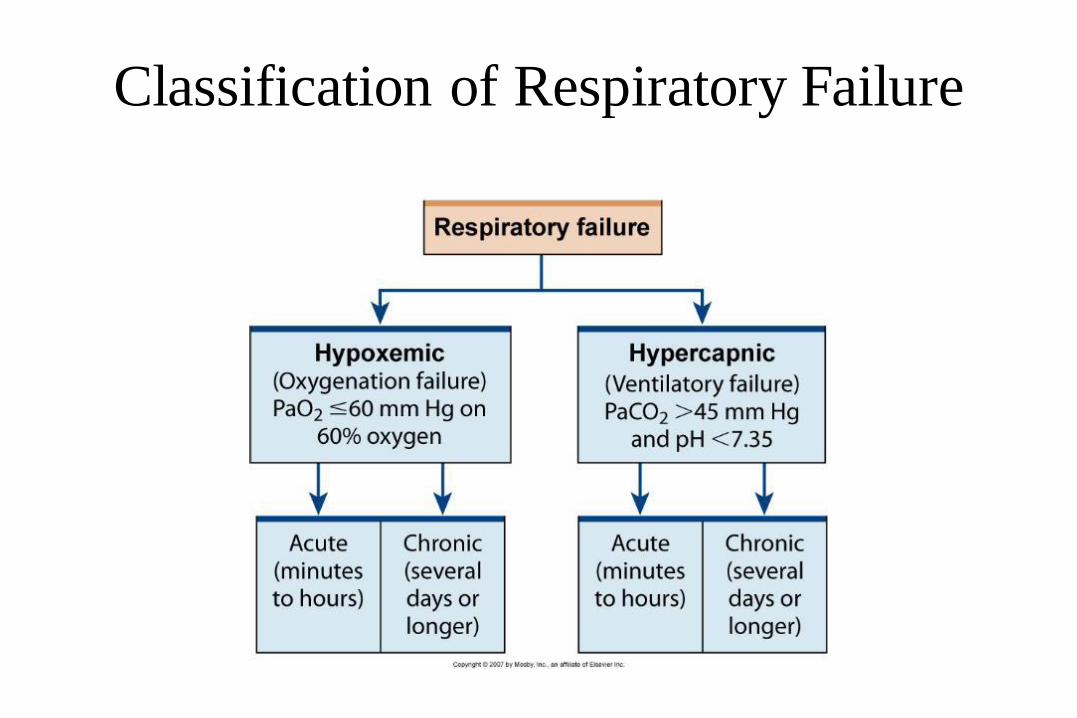
Classification of Respiratory Failure

Cascade
Respiratory Compromise
Respiratory Failure
Respiratory Arrest

2016
30%
85%
2018
50%
90%
Target percentage of payments in ‘FFS linked to quality’ and ‘alternative payment models’ by 2016
and 2018
2014
~20%
>80%
2011
0%
68%
Goals Historical Performance
Alternative payment models (Categories 3-4)
FFS linked to quality (Categories 2-4)
All Medicare FFS (Categories 1-4)

The bundled payment model targets 48 conditions with a single payment for an episode of care
Incentivizes providers to take accountability for both cost and quality of care
Growth from 102 Awardees and 167 Episode Initiators in Phase 2 as of January 2015 to
Current Participation at 360 Awardees and 1,755 Episode Initiators across four Models: Model 1: Retrospective acute care hospital stay only
11 Awardees
Model 2: Retrospective acute care hospital stay plus post-acute care
205 Awardees
536 Episode Initiators
Model 3: Retrospective post-acute care only
135 Awardees
1,218 Episode Initiators
Model 4: Prospective Acute care hospital stay only
9 Awardees
Bundled Payments for Care Improvement has grown significantly
6

Respiratory insufficiency on the
general ward • 1,620,985 discharges from AHRQ database
• 0.91% had a diagnosis code for Respiratory Insufficiency, Arrest and Failure
(RIAF) that was not present on admission.
• Mortality rates were higher for RIAF cases (34.6%) than non-RIAF cases (1.2%,
p<0.001).
• Lengths of hospital and ICU stays were higher for RIAF cases (11.5, 5.8 days)
than non-RIAF cases (4.1, 2.9 days), respectively.
• Total hospital costs were higher for RIAF cases ($24,578) than non-RIAF cases
($6,370).
– About 40% of the costs of RIAF cases were attributed to ICU stay.
Kelley et al. Crit Care Med 2012

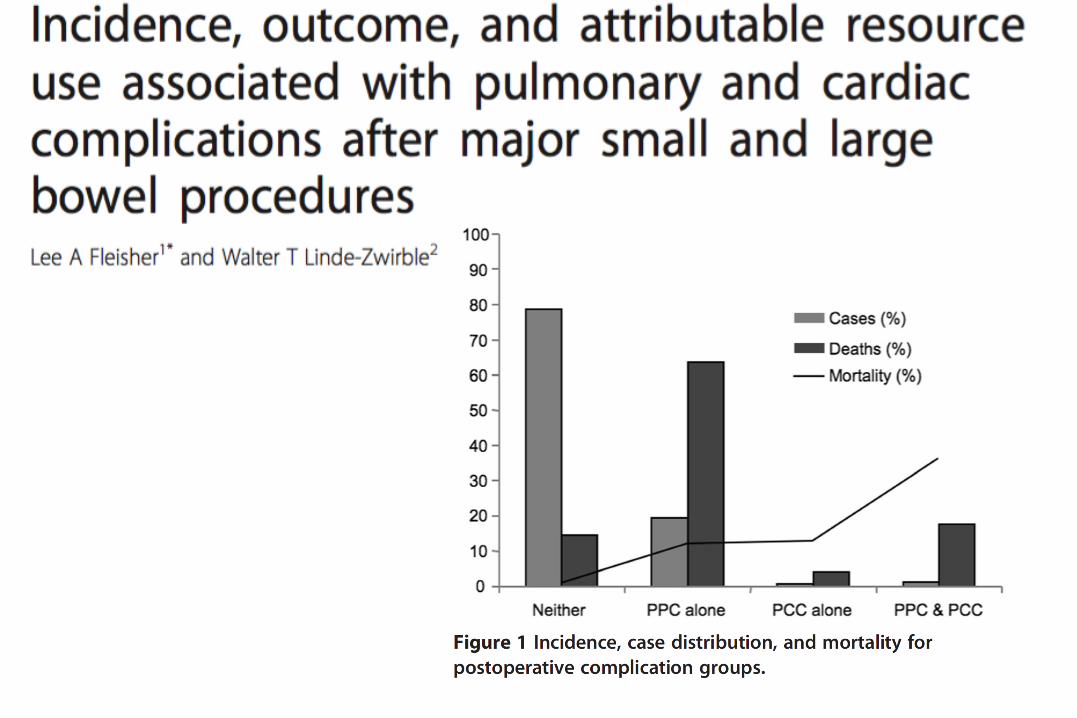
Surgical Patient

Dimick et al. JACS 2004
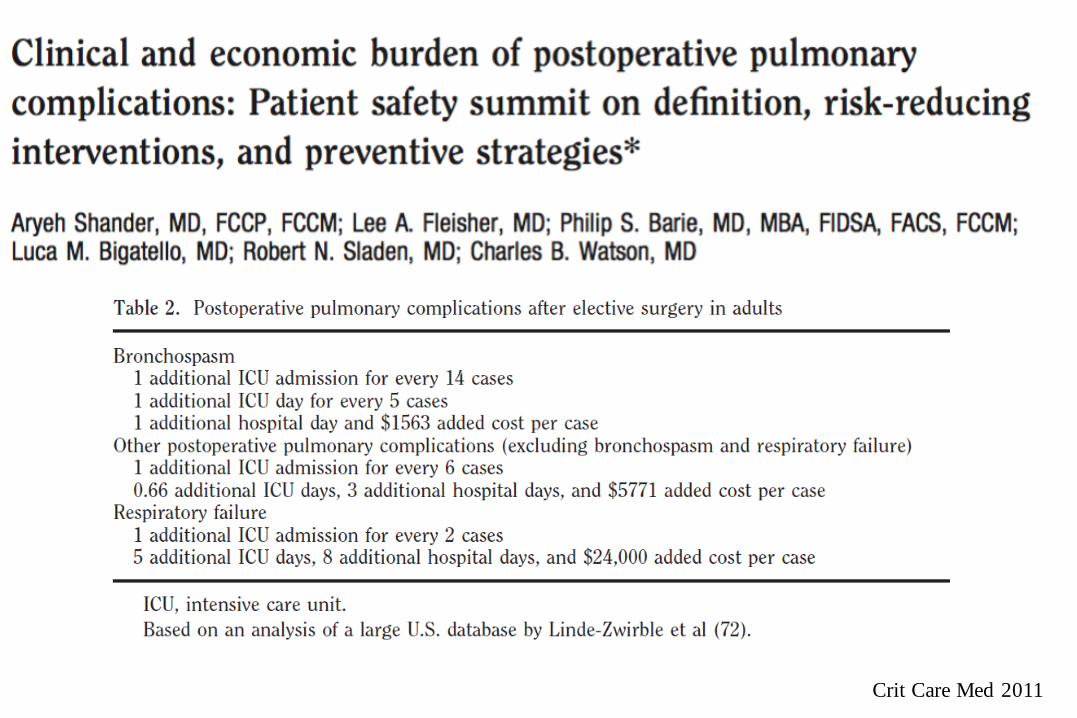
Crit Care Med 2011

The cost part of the value equation
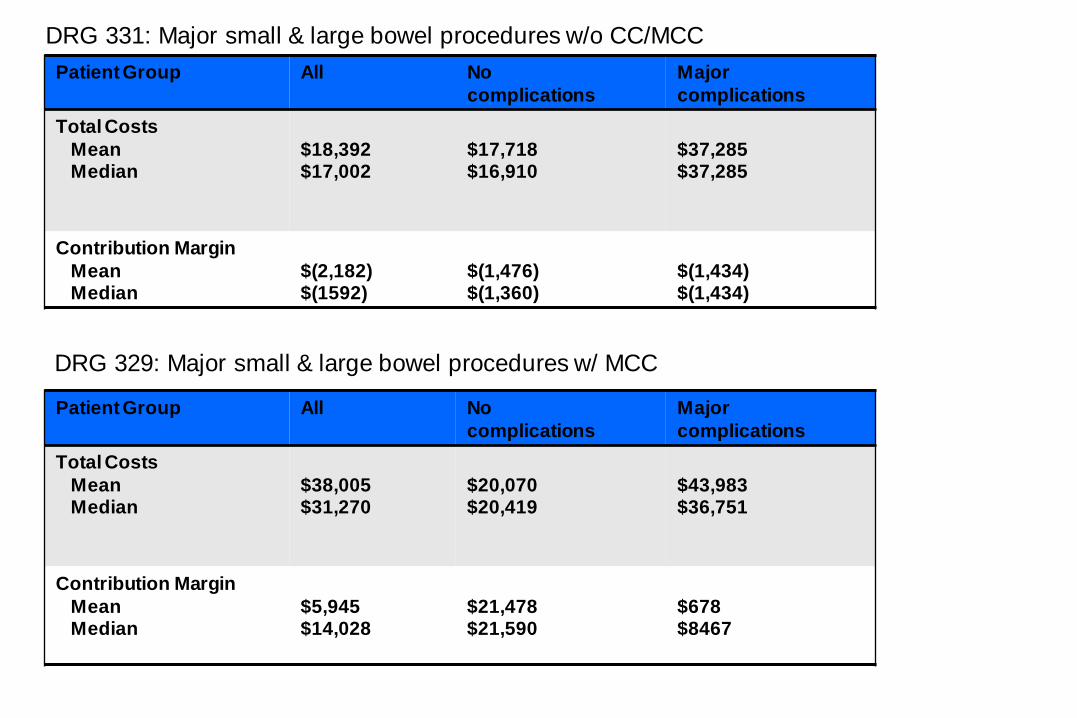
Patient Group All No
complications
Major
complications
Total Costs
Mean Median
$18,392 $17,002
$17,718 $16,910
$37,285 $37,285
Contribution Margin
Mean Median
$(2,182) $(1592)
$(1,476) $(1,360)
$(1,434) $(1,434)
Patient Group All No
complications
Major
complications
Total Costs
Mean Median
$38,005 $31,270
$20,070 $20,419
$43,983 $36,751
Contribution Margin
Mean Median
$5,945 $14,028
$21,478 $21,590
$678 $8467
DRG 331: Major small & large bowel procedures w/o CC/MCC
DRG 329: Major small & large bowel procedures w/ MCC
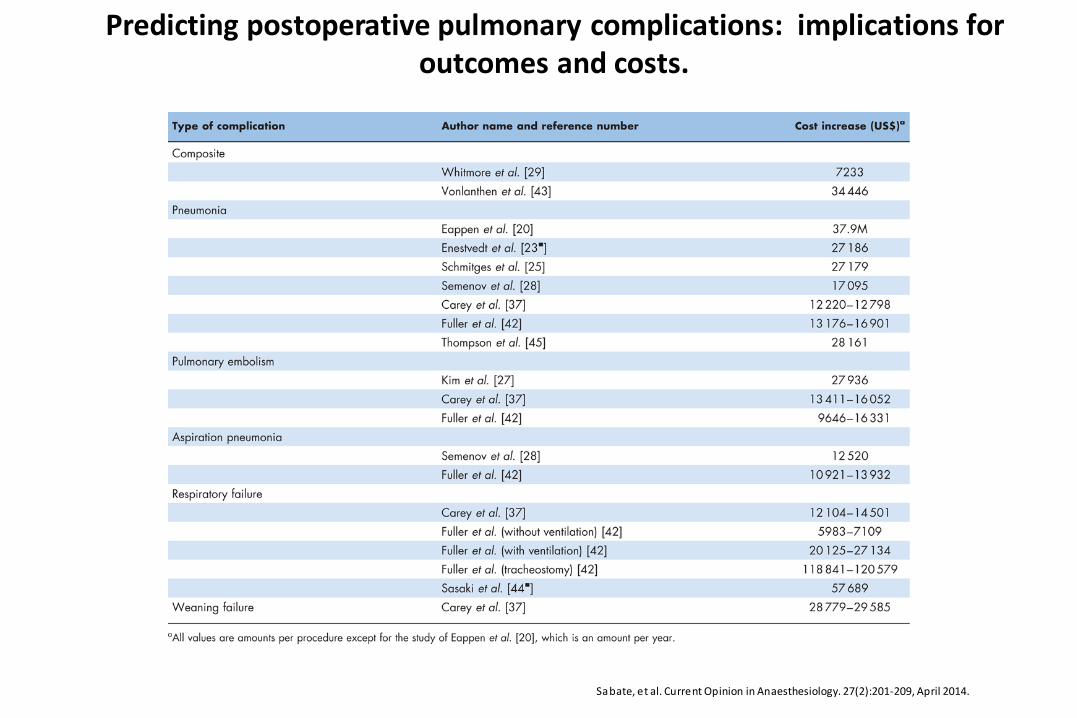
Predicting postoperative pulmonary complications: implications for outcomes and costs.
Sabate, et al. Current Opinion in Anaesthesiology. 27(2):201-209, April 2014.
Can we identify a high risk subset or
condition and intervene?


5 Sabate, et al. Current Opinion in Anaesthesiology. 27(2):201-209, April 2014.
Predicting postoperative pulmonary complications: implications for outcomes and costs.

5
Obesity and Surgical Outcomes
Si lber, et al. Annals of Surgery. 256(1):79-86, July 2012.
Postoperative Opioids

2 Lam, et a l. Current Opinion in Anaesthesiology. 29(1):134-140, February 2016.
Obstructive sleep apnea, pain, and opioids

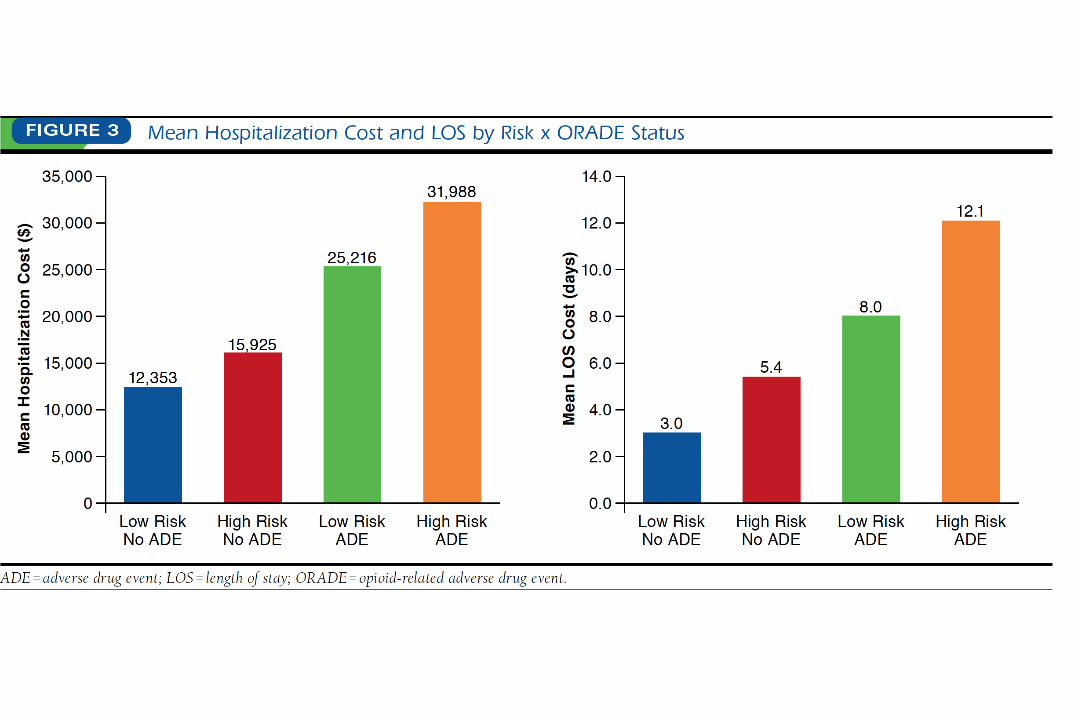
Cost and Quality Implications of Opioid‐Based
Postsurgical Pain Control
Kessler et al. Pharmacotherapy 2013

Kessler et al.
Pharmacotherapy
2013

Postoperative Opioid Overdose
(POOD) in US Hospitals • Major elective operation from 2002
to 2011 in the Nationwide Inpatient
Sample
• Among 13,982,557 patients, 11,669
(0.083%) had POOD
• POOD died more frequently during
hospitalization (1.7% vs. 0.47).
• Substance abuse history was the
strongest predictor of POOD
• Gender, age, race, income,
geographic location, operation type,
and comorbid diseases were
significant predictors
Cauley et al. Academic Surgical Congress 2015
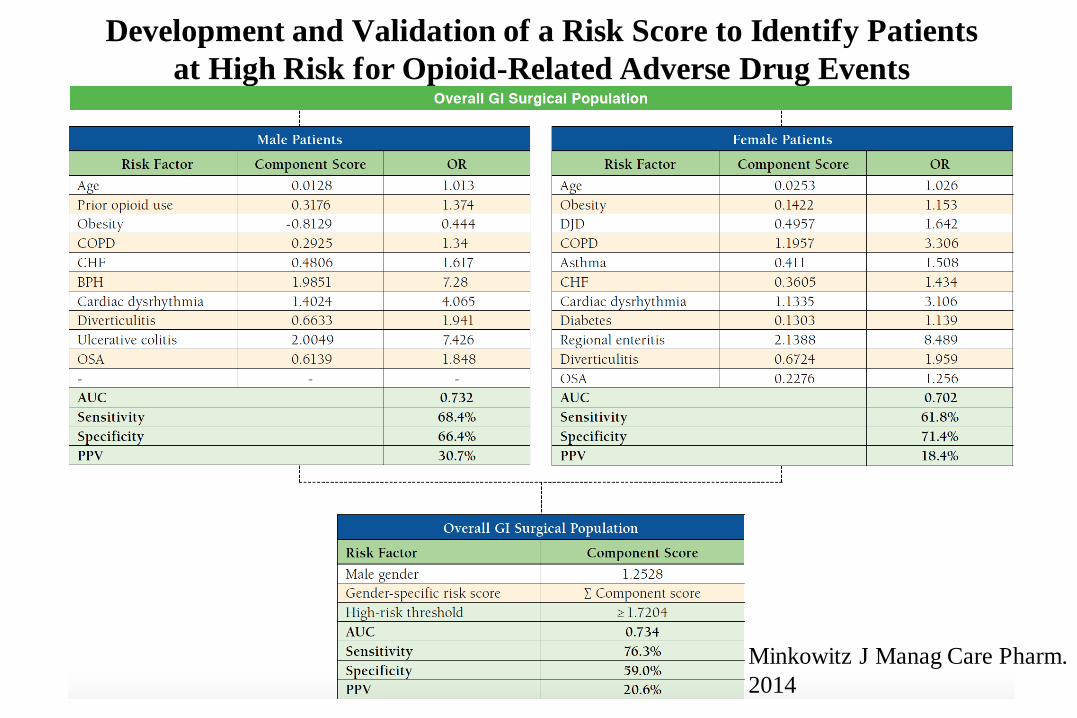
Development and Validation of a Risk Score to Identify Patients
at High Risk for Opioid-Related Adverse Drug Events
Minkowitz J Manag Care Pharm.
2014

6
Perioperative Complications in Obstructive Sleep Apnea Patients Undergoing Surgery: A Review of the Legal Literature.
Fouladpour, et al. Anesthesia & Analgesia. 122(1):145-151, January 2016.

Time between last nursing check and discovery of opioid-induced
respiratory depression
Postoperative Opioid-induced Respiratory Depression:
A Closed Claims Analysis
Anesthesiology. 2015;122(3):659-665
Monitoring to detect respiratory
compromise


Silber et al. HSR 2016

Silber et al. JAMA Surg 2016
Magnet vs. Non-magnet Hospitals

Capnography



Summary
• Respiratory compromise is a common occurrence
in our hospitals
• It is associated with increased costs and morbidity
and mortality
• OSA and opioids increase the risk
• New opioid prescribing and respiratory
monitoring strategies will be required to reduce
the risk