immunosuppression in renal graft failure patients on dialysis (1)
TRANSCRIPT

Immunosuppression in Renal Graft Failure Patients on
DialysisLauren Byrnes

Presentation Overview● Role of Immunosuppressive Therapy in Solid Organ Transplant
● Pathophysiology of Renal Graft Failure
● Question
● Augustine, et. al.
● Bayliss, et. al.
● Recommendations
● Conclusion
● Questions

Role of Immunosuppressive Therapy● Glucocorticoids
○ Usually prednisone
○ Bind to glucocorticoid receptors to down regulate pro-inflammatory cytokines and up regulate
anti-inflammatory cytokines
● Calcineurin Inhibitors (CNIs)
○ Cyclosporine (CSA) or tacrolimus
○ Inhibits calcineurin to prevent proliferation of T-cells
● Purine antagonists
○ Usually azathioprine
○ Pro-drug of 6-mercaptopurine
○ Blocks CD28 co-stimulation which induces T-cell anergy or apoptosis
van der Velden V. Glucocorticoids: mechanisms of action and anti-inflammatory potential in asthma. Mediators of Inflammation. 1998;7(4):229-237; Pillans P. Experimental and Clinical Pharmacology:
Immunosuppressants - mechanisms of action and monitoring. Aust Prescr. 2006;29(4):99-101; Maltzman J, Koretzky G. Azathioprine: old drug, new actions. Journal of Clinical Investigation. 2003;111(8):1122-1124.
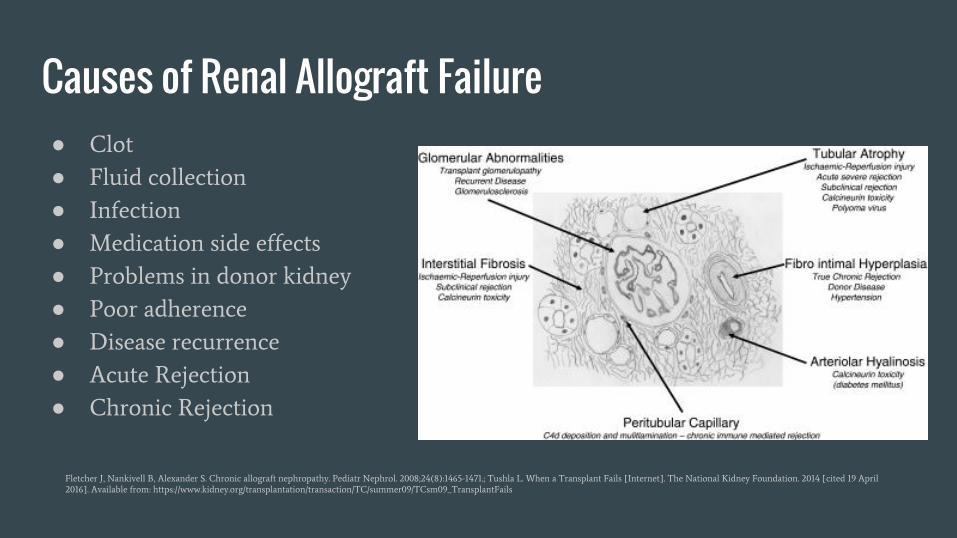
Causes of Renal Allograft Failure● Clot
● Fluid collection
● Infection
● Medication side effects
● Problems in donor kidney
● Poor adherence
● Disease recurrence
● Acute Rejection
● Chronic Rejection
Fletcher J, Nankivell B, Alexander S. Chronic allograft nephropathy. Pediatr Nephrol. 2008;24(8):1465-1471.; Tushla L. When a Transplant Fails [Internet]. The National Kidney Foundation. 2014 [cited 19 April
2016]. Available from: https://www.kidney.org/transplantation/transaction/TC/summer09/TCsm09_TransplantFails

Chronic Rejection● Patients often need to go back on dialysis in these cases due
to eventual allograft failure
● Immunosuppression increases risk for infection as does being
on dialysis
● Currently no set protocol for immunosuppressive therapy
continuation despite increasing number of patients with
allograft failure returning to dialysis
Issa N, Braun W. Renal Transplantation [Internet]. Clevelandclinicmeded.com. 2013 [cited 19 April 2016]. Available from: http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/nephrology/renal-
transplantation/; D'Agata E, Mount D, Thayer V, Schaffner W. Hospital-acquired infections among chronic hemodialysis patients. American Journal of Kidney Diseases. 2000;35(6):1083-1088. Bayliss G, Gohh R,
Morrissey P, Rodrigue J, Mandelbrot D. Immunosuppression after renal allograft failure: a survey of US practices. Clinical Transplantation. 2013;27(6):895-900.

Should Immunosuppressant Therapies be Continued in Dialysis Patients Who Have Recently Failed Renal Transplant?

Immunosuppression After Renal Allograft Failure: A Survey of US Practices
GP Bayliss, RY Gohh, PE Morrissey, JR Rodrigue and DA
Mandelbrot, 2013

Demographics● 93 different renal transplant programs
○ 46 respondents were program director nephrologist, 38 were program director surgeon and 2
responded as having other roles
● 43 performed both adult and pediatric kidney transplants
○ 37 performed adult only
○ 6 performed pediatric only
● 50 were university based transplant centers
○ 19 were private but affiliated with a university
○ 17 were not affiliated with a university at all
● 7 transplant programs did not respond about the characteristics of their programs
or the responder
Bayliss G, Gohh R, Morrissey P, Rodrigue J, Mandelbrot D. Immunosuppression after renal allograft failure: a survey of US practices. Clinical Transplantation. 2013;27(6):895-900.

Methods● List of medical and surgical directors for 235 US kidney transplant centers purchased from
UNOS
● Email addresses were looked up on the internet as they were not included in the purchase
from UNOS
○ 14 email addresses were unable to be found
● 18 question survey using Research Electronic Data Capture (REDCap) survey manager
○ Questions were evaluated for content and clarity by experts in nephrology, transplant surgery and
psychometric research
● Each email was sent 3 times from March 27, 2012 to May 2, 2012
● Analyses included t-tests for continuous variables, the Fisher exact test for variables with 2
categories or a two-tailed chi-square test for variables with three or more categories
Bayliss G, Gohh R, Morrissey P, Rodrigue J, Mandelbrot D. Immunosuppression after renal allograft failure: a survey of US practices. Clinical Transplantation. 2013;27(6):895-900.

Results: Immunosuppressive therapies
Bayliss G, Gohh R, Morrissey P, Rodrigue J, Mandelbrot D. Immunosuppression after renal allograft failure: a survey of US practices. Clinical Transplantation. 2013;27(6):895-900.

Results: Reasons for discontinuing immunosuppressive therapy
Bayliss G, Gohh R, Morrissey P, Rodrigue J, Mandelbrot D. Immunosuppression after renal allograft failure: a survey of US practices. Clinical Transplantation. 2013;27(6):895-900.

Discussion● Many factors are considered when tapering immunosuppressive therapies
○ Ongoing signs of rejection and plans to retransplant seem to be the factors most often prioritized
by physicians
○ Previous infection plays a role but is rarely the lead deciding factor
● Immunosuppressive therapy is frequently weaned one drug at a time
○ Antimetabolite therapy most commonly stopped first followed by calcineurin inhibitors
○ Glucocorticoids are usually left on even when all others have been taken off
● Only 1% of patients with graft failure remain totally immunosuppressed one year
after being restarted on dialysis
○ Over 70% have been weaned off entirely from immunosuppressive therapies
Bayliss G, Gohh R, Morrissey P, Rodrigue J, Mandelbrot D. Immunosuppression after renal allograft failure: a survey of US practices. Clinical Transplantation. 2013;27(6):895-900.

Limitations● No individual patient data or demographics obtained
● No way of confirming accurate reporting from centers
● 42% of programs responding may not reflect typical program in US
○ Mean program size for these programs were 94.3 kidney transplants in 2011
○ US mean was 74.9 transplants in 2011
● Required a p < 0.01 for statistical significance
○ Large number of possible associations examined
○ No associations reached this threshold

Independent of Nephrectomy, Weaning Immunosuppression Leads to Late Sensitization
After Kidney Transplant Failure
JJ Augustine, KJ Woodside, A Padiyar, EQ Sanchez, DE Hricik and
JA Schulak, 2012

Demographics● Original cohort of 300 patients with a history of renal transplant failure
○ Late panel reactive antibodies (PRA) levels available in 156 patients
■ 25 excluded for receiving transplant within 6 months of graft failure
■ 12 excluded for having PRA level of 20% or more at time of original transplant
○ N=119
● Average age at time of failure was 42
● 48% female
● 37% African-American
● 80% weaned from immunosuppressive therapy at time of late PRA testing
● 18% had both kidney and pancreatic (KP) transplant
● Median graft survival was 85 months
Augustine J, Woodside K, Padiyar A, Sanchez E, Hricik D, Schulak J. Independent of Nephrectomy, Weaning Immunosuppression Leads to Late Sensitization After Kidney Transplant Failure. Transplantation Journal. 2012;
94(7):738-743.

Results: Sensitization Risk Factors● Human Leukocyte Antigen (HLA) matching
○ For patients who were weaned from immunosuppressive therapies (n=95), there was a correlation
between number of HLA mismatches and late PRA levels
■ r=0.352, P<0.001
○ In the remaining immunosuppressed patients (n=24), there was no correlation between number of
HLA mismatches and late PRA levels
■ r=-0.150
● History of nephrectomy
○ 79% of patients who underwent nephrectomy before late PRA were highly sensitized
○ Weaning of immunosuppression was a prediction of needing nephrectomy
■ None of the 24 patients maintained on immunosuppression required nephrectomy
■ 41% of patients weaned from immunosuppressive therapy required nephrectomy
Augustine J, Woodside K, Padiyar A, Sanchez E, Hricik D, Schulak J. Independent of Nephrectomy, Weaning Immunosuppression Leads to Late Sensitization After Kidney Transplant Failure. Transplantation Journal. 2012;
94(7):738-743.

Results: Variables to predict PRA levels of >80%
Augustine J, Woodside K, Padiyar A, Sanchez E, Hricik D, Schulak J. Independent of Nephrectomy, Weaning Immunosuppression Leads to Late Sensitization After Kidney Transplant Failure. Transplantation Journal. 2012;
94(7):738-743.
Discussion● Most patients weaned from immunosuppressive therapy became highly sensitized
● Nephrectomy for cause was required exclusively in patients who had been
weaned from immunosuppressive therapy
● Authors concluded weaning of immunosuppression initiated immune system
activation and HLA antibody formation
● Recommend maintaining immunosuppression after failure to maintain residual
renal function
○ Increased infectious risk
○ High rate of death related to sepsis after transplant failure
● Early nephrectomy with maintained immunosuppressive therapy may be a
solution in allograft failure
Augustine J, Woodside K, Padiyar A, Sanchez E, Hricik D, Schulak J. Independent of Nephrectomy, Weaning Immunosuppression Leads to Late Sensitization After Kidney Transplant Failure. Transplantation Journal. 2012;
94(7):738-743.

Limitations● Absence of data on blood transfusions after allograft failure
○ Can contribute to sensitization after transplant failure
○ Anemia is common after transplant failure
● Small number of patients
○ Single site study
○ Details on immunosuppressive therapy weaning unavailable
● Retrospective analysis
Augustine J, Woodside K, Padiyar A, Sanchez E, Hricik D, Schulak J. Independent of Nephrectomy, Weaning Immunosuppression Leads to Late Sensitization After Kidney Transplant Failure. Transplantation Journal. 2012;
94(7):738-743.
Recommendations● Continuation of immunosuppressive therapies should be individualized for patients
restarting dialysis after graft failure
○ If graft had 2 or fewer differences in HLA proteins, it is likely safe to discontinue therapy
○ If graft failed after less than 1 year, a nephrectomy should be done before discontinuing therapy
○ If either of these criteria are not met and risks of discontinuing therapy outweigh benefit, therapy should be
continued
● If therapies need to be discontinued, discontinuing antimetabolite therapy is the safest to
remove followed by calcineurin inhibitors
○ Lowest risk of rejection exacerbation
○ Glucocorticoids should remain on for all patients unless otherwise contraindicated
● More studies need to be done
○ Prospective randomized trials to study risks and benefits of weaning versus maintaining different
immunosuppressants
○ Randomized control studies to determine rates of infection and sensitization from stopping or continuing
immunosuppression while on dialysis

Questions?

References1. van der Velden V. Glucocorticoids: mechanisms of action and anti-inflammatory potential in asthma. Mediators of
Inflammation. 1998;7(4):229-237.
2. Pillans P. Experimental and Clinical Pharmacology: Immunosuppressants - mechanisms of action and monitoring. Aust Prescr.
2006;29(4):99-101.
3. Maltzman J, Koretzky G. Azathioprine: old drug, new actions. Journal of Clinical Investigation. 2003;111(8):1122-1124.
4. Tushla L. When a Transplant Fails [Internet]. The National Kidney Foundation. 2014 [cited 19 April 2016]. Available from:
https://www.kidney.org/transplantation/transaction/TC/summer09/TCsm09_TransplantFails
5. Fletcher J, Nankivell B, Alexander S. Chronic allograft nephropathy. Pediatr Nephrol. 2008;24(8):1465-1471.
6. Issa N, Braun W. Renal Transplantation [Internet]. Clevelandclinicmeded.com. 2013 [cited 19 April 2016]. Available from: http:
//www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/nephrology/renal-transplantation/
7. D'Agata E, Mount D, Thayer V, Schaffner W. Hospital-acquired infections among chronic hemodialysis patients. American
Journal of Kidney Diseases. 2000;35(6):1083-1088.
8. Bayliss G, Gohh R, Morrissey P, Rodrigue J, Mandelbrot D. Immunosuppression after renal allograft failure: a survey of US
practices. Clinical Transplantation. 2013;27(6):895-900.
9. Augustine J, Woodside K, Padiyar A, Sanchez E, Hricik D, Schulak J. Independent of Nephrectomy, Weaning
Immunosuppression Leads to Late Sensitization After Kidney Transplant Failure. Transplantation Journal. 2012;94(7):738-743.