immunohistochemistry for carcinoma of … for carcinoma of unknown primary jason l hornick, md, ......
TRANSCRIPT

04/04/2016
1
Page 1
IMMUNOHISTOCHEMISTRY FOR CARCINOMA OF UNKNOWN
PRIMARY
Jason L Hornick, MD, PhD
Director of Surgical Pathology Director of Immunohistochemistry
Brigham and Women’s Hospital
Associate Professor of Pathology Harvard Medical School
Boston, MA, USA
Carcinoma of unknown primary
Definition: histologically confirmed metastatic carcinoma for which primary site cannot be identified after standard diagnostic approach:
• Detailed history and physical examination
• Blood counts and biochemical analysis
• Urinalysis and stool occult blood test
• CT of thorax, abdomen, and pelvis
• Histologic review including IHC
Carcinoma of unknown primary
• Account for 2-5% of malignancies diagnosed in the US
• 7th or 8th most frequent cancer
• 4th or 5th most common cause of cancer death in both sexes
• 31,000 new cases in the US in 2012 – down from 45,000 new cases in 1995
• Improved radiologic imaging
• Increasingly specific IHC markers

04/04/2016
2
Page 2
Origin of primary tumors (autopsy)
Organ Incidence
Pancreas 20-25%
Lung 15-20%
Colon/rectum 5-10%
Liver/biliary 5-10%
Stomach 5%
Kidney 5%
Ovary <5%
Prostate <5%
Breast 2%
Other 1%
Histologic groups of carcinoma of unknown primary
Histology Frequency
Well or moderately differentiated
adenocarcinoma 60%
Poorly differentiated adenocarcinoma
or undifferentiated carcinoma 30%
Squamous cell carcinoma 5%
Undifferentiated malignant neoplasm 5%
Overview
• Distribution of keratin family members in carcinomas
• Lineage-restricted markers and primary site determination
• Primary tumors of the liver and mimics
• Squamous cell carcinomas
• Primary site determination for metastatic neuroendocrine tumors

04/04/2016
3
Page 3
Keratin family members in carcinomas
• Low-molecular-weight keratins (CK8, CK18, CAM5.2) – Glandular epithelium, hepatocytes
• High-molecular-weight keratins (CK5, CK14, 34βE12) – Squamous epithelium, urothelium,
basal cells
Keratin family members in carcinomas: CK7 and CK20
• CK7 wide distribution in epithelial cells
• CK20 restricted to lower GI tract epithelium, umbrella cells of the urinary bladder, Merkel cells
CK7 and CK20 – are they (still) useful?
Phenotype Primary sites
CK7– / CK20+ Colon/rectum
CK7+ / CK20+ Bladder, upper GI, pancreas
CK7– / CK20– Uncommon (prostate, HCC)
CK7+ / CK20– Nearly everything else

04/04/2016
4
Page 4
CK20
Metastatic colonic adenocarcinoma
CK7
Metastatic colonic adenocarcinoma
CK20
Metastatic colonic adenocarcinoma

04/04/2016
5
Page 5
Primary site Marker
Bladder Uroplakin
Breast GCDFP-15
(prolactin-inducible protein)
Breast Mammaglobin
(SCGB2A1/A2)
Colon/rectum Villin
Lung Napsin A
Prostate Prostate-specific antigen
Prostate Prostatic acid phosphatase
Thyroid Thyroglobulin
IHC for lineage/site specification: cytoplasmic/membranous markers
IHC for lineage/site specification: cytoplasmic/membranous markers
• In general, expression is decreased (or entirely absent) with poor differentiation – significant impact on sensitivity
GCDFP
Breast carcinoma

04/04/2016
6
Page 6
Breast carcinoma
GCDFP
mammaglobin
Breast carcinoma
Expression of mammaglobin in other tumor types
Tumor type Frequency
Endometrial endometrioid
adenocarcinoma 20-40%
Skin adnexal carcinomas 20-40%
Salivary gland neoplasms 20-50%

04/04/2016
7
Page 7
PSA
Prostatic adenocarcinoma
Napsin A
Lung adenocarcinoma
Napsin A
• Warning: napsin A is also positive in most papillary renal cell carcinomas

04/04/2016
8
Page 8
IHC for lineage/site specification: nuclear transcription factors
• Insights gained from developmental and cell biology research
• Transcription factors involved in patterning of organ systems, lineage commitment
• Some are highly specific for particular cell type or visceral organ
• Others show expression limited to several tissue types
• Very helpful in determining primary site for CUP
• 10 years ago, very few were used in surgical pathology practice
–TTF1, CDX2, MYOG
• In 2016, over 50 markers with potential diagnostic applications are available
–Carcinomas, lymphomas, melanoma, germ cell tumors, sarcomas
IHC for lineage/site specification: nuclear transcription factors
IHC for lineage/site specification: nuclear transcription factors
Transcription factor Primary site
CDX2 Colon/rectum, upper GI
GATA3 Breast, bladder
NKX3-1 Prostate
OCT4 Seminoma, embryonal carcinoma
PAX8 Thyroid, kidney, Müllerian
SALL4 Germ cell tumors
SATB2 Colon/rectum
SF1 Adrenal cortex
TTF1 (NKX2-1) Lung, thyroid
WT1 Müllerian, mesothelioma
04/04/2016
9
Page 9
IHC for lineage/site specification: nuclear transcription factors
• In general, even poorly differentiated carcinomas maintain (relatively) diffuse expression in most cases – high sensitivity
• With increasing study, specificity decreases
• Beware of relying on a single diagnostic marker
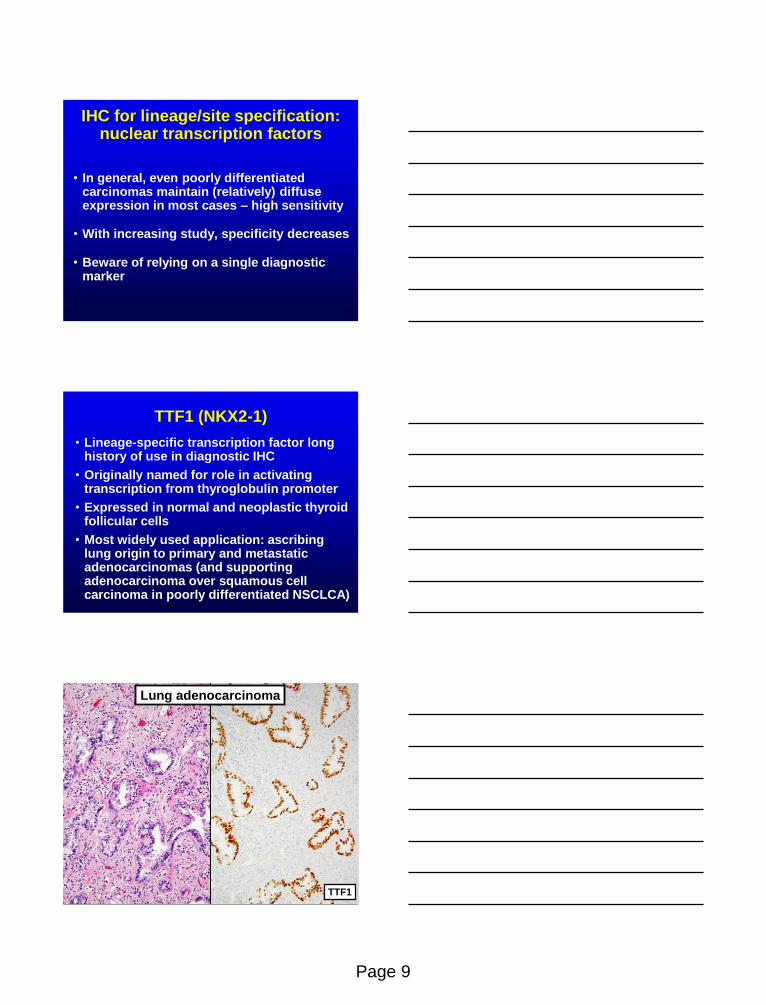
TTF1 (NKX2-1)
• Lineage-specific transcription factor long history of use in diagnostic IHC
• Originally named for role in activating transcription from thyroglobulin promoter
• Expressed in normal and neoplastic thyroid follicular cells
• Most widely used application: ascribing lung origin to primary and metastatic adenocarcinomas (and supporting adenocarcinoma over squamous cell carcinoma in poorly differentiated NSCLCA)
TTF1
Lung adenocarcinoma

04/04/2016
10
Page 10
Metastatic poorly differentiated lung adenocarcinoma
TTF1
Poorly differentiated (insular) thyroid carcinoma
TTF1
TTF1
• Warning: TTF1 is also positive in a subset of endometrial adenocarcinomas (most common in grade 3 endometrioid and serous)
• Some variation in sensitivity and specificity based on particular clone

04/04/2016
11
Page 11
Primary site Positive cases
Pulmonary (adenocarcinoma) 70-90%
Pulmonary (squamous cell carcinoma) <10%
Thyroid (all types) 80-100%
Cholangiocarcinoma (extrahepatic) 5-25%*
Endometrial 5-20%*
Ovarian 5-30%*
Expression of TTF1 in carcinomas I
*These cases usually show expression in only a small fraction of
tumor cells.
Primary site Positive cases
Gastric/esophageal <10%
Cervical <5%
Pancreatic <5%
Breast <5%
Urothelial <5%
Colorectal <5%
Hepatocellular <5%
Salivary gland (adenoid cystic) 30-50%
Salivary gland (other) <5%
Adrenal cortical <5%
Expression of TTF1 in carcinomas II
TTF1: potential diagnostic pitfall
• Cytoplasmic staining relatively common
• Diffuse staining in normal hepatocytes and many hepatocellular carcinomas
• Likely represents cross-reactivity with CPS1 (antigen recognized by HepPar-1 antibody)
• Subset of adenocarcinomas from various sites (especially foregut) also show cytoplasmic staining

04/04/2016
12
Page 12
Hepatocellular carcinoma
TTF1
WT1
• Wilms tumor 1
• Transcription factor plays diverse roles in cancer depending upon tumor type and biological context
• Expressed in malignant mesothelioma, serous carcinoma
• Positive in nearly all serous carcinomas of the ovary; uncommon in serous carcinomas of the endometrium (variable results in different studies)
WT1
Malignant mesothelioma

04/04/2016
13
Page 13
Metastatic mesothelioma
WT1
Metastatic serous carcinoma
WT1
WT1
• Among carcinomas, nuclear WT1 relatively specific for ovarian serous tumors
• Positive in <5% of breast, lung, gastric, colorectal, urothelial carcinomas
• Cytoplasmic staining detected in subset of other carcinomas and various other tumor types – only nuclear staining should be considered positive for ascribing site of origin

04/04/2016
14
Page 14
CDX2
• Caudal-type homeobox transcription factor involved in intestinal differentiation
• Nuclear expression in >90% colorectal adenocarcinomas
• Somewhat lower sensitivity in high grade and MSI-H carcinomas
• Widely used to support colorectal origin
• No significant loss of sensitivity in the metastatic setting
CDX2
Colonic adenocarcinoma
Metastatic colonic adenocarcinoma
CDX2

04/04/2016
15
Page 15
CDX2
• Also expressed in carcinomas from other gastrointestinal primary sites associated with intestinal differentiation – Esophagus and stomach
– Pancreas and biliary tree
• Often more heterogeneous staining in tumors from these other sites
• Particularly helpful in differential diagnosis between primary (poorly cohesive) gastric carcinoma and metastatic breast carcinoma
Gastric adenocarcinoma
CDX2
CDX2
• Warning: CDX2 can also be positive in mucinous adenocarcinomas from diverse anatomic sites
–Ovary
–Lung
–Pancreas
–Bladder

04/04/2016
16
Page 16
Primary site Positive cases
Colorectal and appendiceal 80-100%
Gastroesophageal 40-60%
Pancreatic/biliary 30-50%
Ovarian (mucinous and endometrioid) 40-60%
Ovarian (serous) <10%
Endometrial 5-10%
Pulmonary (mucinous) 70-80%
Pulmonary (non-mucinous) <5%
Bladder (adenocarcinoma) 30-50%
Bladder (urothelial) <5%
Prostatic <5%
Breast <5%
Renal <5%
Expression of CDX2 in carcinomas
GATA3
• Transcription factor originally recognized for role in T-cell function
• Clinically useful as marker for breast or urothelial origin
• Positive in >80% of breast and urothelial carcinomas
• No significant loss of sensitivity in the metastatic setting
• More recent large surveys revealed expression in wide range of tumor types
GATA3
Bladder urothelial carcinoma

04/04/2016
17
Page 17
Bladder urothelial carcinoma
GATA3
Breast carcinoma
GATA3
Breast carcinoma
GATA3

04/04/2016
18
Page 18
Expression of GATA3 in other tumors
Tumor type Frequency
Squamous cell carcinoma (skin) 80%
Squamous cell carcinoma (cervix) 33%
Squamous cell carcinoma (lung) 10%
Lung adenocarcinoma 5-10%
Skin adnexal carcinomas 80-100%
Mesothelioma 25-60%
Salivary gland tumors 20-50%
Pancreatic ductal adenocarcinoma 40%
Paraganglioma 80%
Choriocarcinoma 100%
Chromophobe renal cell carcinoma 50%
Potential value of GATA3 in differential diagnosis
Positive Negative
Metastatic lobular breast carcinoma Gastric signet-ring-cell carcinoma
Metastatic ductal breast carcinoma Lung/GI/ovarian adenocarcinoma
Urothelial carcinoma Prostatic adenocarcinoma
Squamous cell carcinoma of skin Squamous cell carcinoma of lung
Malignant mesothelioma Lung adenocarcinoma
Paraganglioma Other neuroendocrine tumors
Choriocarcinoma, yolk sac tumor Embryonal carcinoma, seminoma
Am J Surg Pathol. 38:13-22, 2014
NKX3-1
• Homeobox transcription factor, androgen-dependent
• Expression limited to prostate
• Usually more diffusely positive than conventional cytoplasmic markers
• Helpful to distinguish high grade prostatic adenocarcinoma from urothelial carcinoma
• Helpful to suggest prostatic origin in metastatic carcinoma

04/04/2016
19
Page 19
NKX3-1
Prostatic adenocarcinoma
Expression of NKX3-1 in carcinomas
Primary site Positive cases
Prostatic 90-100%
Breast (lobular) 15-30%
Breast (ductal) <10%
Bladder (urothelial and adenocarcinoma) <5%
Pancreatic/biliary <5%
Hepatocellular <5%
Renal <5%
Colorectal <5%
Gastroesophageal <5%
Pulmonary <5%
Thyroid <5%
SATB2
• More recently described transcription factor expressed in colorectal/appendiceal epithelium
• Similarly high sensitivity and likely higher specificity than CDX2
• Positive in 80-90% of primary and metastatic colorectal adenocarcinomas
• Higher sensitivity than CDX2 for medullary carcinomas
• Unlike CDX2, SATB2 rarely expressed in gastroesophageal and pancreaticobiliary adenocarcinomas

04/04/2016
20
Page 20
SATB2
Colonic adenocarcinoma
Poorly differentiated colonic adenocarcinoma
SATB2
Primary site Positive cases
Colorectal and appendiceal 80-100%
Renal 25-35%
Gastroesophageal 10-20%*
Pancreatic/biliary 10-20%*
Mullerian 10-20%*
Pulmonary 10-20%*
Bladder (urothelial) 10-20%*
Prostatic 5-15%*
Breast 5-15%*
Thyroid <5%*
Expression of SATB2 in carcinomas
*These cases show expression in only a small fraction of tumor cells.

04/04/2016
21
Page 21
PAX8
• One of the most widely used lineage-specific transcription factors in IHC approach to CUP
• Highly sensitive for carcinomas originating in ovary, kidney, thyroid
• >90% serous, endometrioid, and clear cell ovarian carcinomas positive for PAX8
• Much lower rate of expression in ovarian mucinous adenocarcinomas
• PAX2 largely supplanted by PAX8
Primary site Positive cases
Renal 85-95%
Thyroid (papillary, follicular, poorly diff) 90-100%
Thyroid (anaplastic, medullary) 60-80%
Ovarian (non-mucinous) 90-100%
Ovarian (mucinous) 10-40%
Endometrial 90-100%
Cervical 90-100%
Expression of PAX8 in carcinomas I
Renal cell carcinoma
PAX8

04/04/2016
22
Page 22
Ovarian clear cell carcinoma
PAX8
Metastatic serous carcinoma
PAX8
PAX8
Metastatic serous carcinoma

04/04/2016
23
Page 23
TTF1
Metastatic serous carcinoma
Papillary thyroid carcinoma
PAX8
TTF1
Poorly differentiated thyroid carcinoma
PAX8

04/04/2016
24
Page 24
Metastatic lung adenocarcinoma
TTF1
PAX8
Pan-PAX?
• Widely used polyclonal anti-PAX8 antibody not specific for PAX8
• Cross-reacts with other PAX family members (PAX5, PAX6, PAX3)
• Responsible for staining in B lymphocytes (PAX5)
• Responsible for staining in pancreatic well-differentiated neuroendocrine tumors (PAX6)
• PAX8-specific monoclonal antibodies available
PAX6
PAX5
PAX8

04/04/2016
25
Page 25
Primary site Positive cases
Thymic (polyclonal antibody) 80-90%
Pancreatic/biliary 5-10%
Bladder (urothelial) 10-20%
Gastric/esophageal 5-10%
Colorectal/appendiceal <5%
Hepatocellular <5%
Breast <5%
Pulmonary (adenocarcinoma) <5%
Pulmonary (squamous cell carcinoma) 0-30%
Head and neck (squamous cell
carcinoma) <5%
Adrenal cortical <5%
Skin (squamous cell carcinoma) <5%
Expression of PAX8 in carcinomas II
SF1
• Steroidogenic factor 1 (NR5A1)
• Recently investigated transcription factor
• Highly sensitive marker for sex cord-stromal tumor
• Highly sensitive marker for adrenal cortical carcinoma
• Particularly useful in distinguishing primary adrenal cortical carcinoma from metastatic renal cell carcinoma
SF1
Adrenal cortical carcinoma

04/04/2016
26
Page 26
ER and PR
• In addition to role as predictive biomarkers in breast cancer, can be useful to ascribe primary site in certain contexts
• Hormone receptor-positive breast carcinomas retain expression in metastatic foci in >90% of cases
• Most useful in patients with known history of hormone receptor-positive breast cancer and other known or suspected malignancies
ER and PR
• Also commonly expressed in primary carcinomas of gynecologic tract
• Most ovarian serous carcinomas express ER
• Can be helpful to distinguish serous from clear cell carcinoma
ER and PR
• ER consistently negative in colorectal, gastroesophageal, hepatocellular, pancreatic/biliary carcinomas
• ER positive (generally weak/focal) in small subset of lung adenocarcinomas
• PR less specific: positive in 30% of cholangiocarcinomas; positive in small subset of gastroesophageal, pancreatic, hepatocellular carcinomas

04/04/2016
27
Page 27
Embryonic stem cell transcription factors
• Transcription factors involved in maintenance of pluripotency
• Large body of literature on role in embryonic stem cell biology
• Some of these transcription factors useful in diagnostic IHC
• OCT4 (also known as OCT3/4) widely used in clinical practice
• Other markers less often used
Subtype SALL4 OCT4 NANOG SOX2
Seminoma ++++ ++++ ++++ –
Embryonal carcinoma ++++ ++++ ++++ ++++
Yolk sac tumor ++++ – – –
Teratoma – – – ++
Choriocarcinoma variable – – –
Expression of embryonic stem cell transcription factors in germ cell tumors
OCT4
Seminoma

04/04/2016
28
Page 28
Don’t forget to consider a primary liver tumor!
Hepatocellular carcinoma • Alpha fetoprotein (AFP)
– Low sensitivity
• Polyclonal carcinoembryonic antigen (CEA)
– Bile canalicular pattern
• Carbamoyl-phosphate synthase 1 (CPS1) = Hep-Par 1 antibody – Urea cycle enzyme
– Also expressed in 5-10% of adenocarcinomas of diverse sites
• Arginase 1 (ARG1) – Urea cycle enzyme
– Appears to be most sensitive and specific
pCEA
Hepatocellular carcinoma

04/04/2016
29
Page 29
CPS1/Hep-Par1
Hepatocellular carcinoma
ARG1
Hepatocellular carcinoma
Potential mimics of HCC
• Adrenal cortical carcinoma – Inhibin
– Melan-A/MART1 (MLANA) – A103 >> M2-7C10
– SF1 (steroidogenic factor 1; NR5A1)
• Renal cell carcinoma – RCC (renal cell carcinoma marker) – low
sensitivity in the metastatic setting
– PAX2 – less sensitive than PAX8
– PAX8 – highly sensitive marker, also positive in thyroid and Müllerian carcinomas
• Poorly differentiated cholangiocarcinoma

04/04/2016
30
Page 30
RCC
Metastatic renal cell carcinoma
Metastatic renal cell carcinoma
PAX8
Intrahepatic cholangiocarcinoma
• Radiologic features: – Large solitary mass +/- satellite lesions – Biliary dilatation – Hepatic capsular retraction – Delayed enhancement – Lobar/segmental atrophy
• Histology/immunophenotype essentially indistinguishable from pancreatic ductal adenocarcinoma – CK7/CK19 positive – Loss of SMAD4 (~50%)
• When you encounter a CK7+ AdCA in the liver, consider cholangiocarcinoma

04/04/2016
31
Page 31
Intrahepatic cholangiocarcinoma
Biliary dilatation Capsular retraction
Satellite
Intrahepatic cholangiocarcinoma
Capsular retraction Satellite
Intrahepatic cholangiocarcinoma

04/04/2016
32
Page 32
Intrahepatic cholangiocarcinoma
Pancreatic ductal carcinoma
SMAD4
Metastatic cholangiocarcinoma
SMAD4

04/04/2016
33
Page 33
Squamous cell carcinoma: P63 and P40
• Confirmation relatively straightforward – P63 (also positive in urothelial and subset of
adenocarcinomas; ~20% lung AdCA)
– P40 (much more specific for squamous cell and urothelial carcinomas)
• In general, IHC not helpful to determine primary site (other than P16: HPV-associated SCC of oropharynx, cervix, anal canal)
• In situ hybridization can be helpful (head and neck): – EBER – nasopharyngeal carcinoma
– High-risk HPV – oropharyngeal carcinomas (tonsil, base of tongue)
Lung squamous cell carcinoma
P40
Metastatic HPV-associated squamous cell carcinoma
P16

04/04/2016
34
Page 34
Well-differentiated neuroendocrine tumors
• 10-20% of NET present as metastasis of unknown primary
• Midgut (ileum) >> pancreas >> other
• Determination of primary site increasingly important for well-differentiated NET
• Recent introduction of effective systemic therapies
• Different efficacies for midgut vs pancreatic origin
Systemic therapy for metastatic well-differentiated neuroendocrine tumors
Agent Mechanism Efficacy
Midgut Pancreas
Octreotide Somatostatin analogue + +
Interferon-α Immune activation + +
Streptozocin Alkylating agent ̶ +
Temozolomide Alkylating agent ̶ +
Everolimus mTOR inhibitor +/ ̶ +
Sunitinib Tyrosine kinase inhibitor ̶ +
Bellizzi Adv Anat Pathol 2013
Transcription factor expression in well-differentiated neuroendocrine tumors
Transcription factor Primary sites
CDX2 Midgut (ileum), appendix >> pancreas
ISL1 Pancreas
PAX6 (pPAX8) Pancreas, duodenum, rectum
PDX1 Pancreas, duodenum
TTF1 Lung

04/04/2016
35
Page 35
Transcription factor expression in well-differentiated neuroendocrine tumors
Transcription factor Primary sites
CDX2 Midgut (ileum), appendix >> pancreas
ISL1 Pancreas
PAX6 (pPAX8) Pancreas, duodenum, rectum
PDX1 Pancreas, duodenum
TTF1 Lung
CDX2 expression in well-differentiated neuroendocrine tumors
Primary site Positive
Lung <5%
Stomach 15-30%
Duodenum 30-45%
Pancreas 15-20%
Jejunum/ileum 90%
Appendix 90%
Rectum 0-30%
CDX2 expression in well-differentiated neuroendocrine tumors
Primary site Positive
Lung <5%
Stomach 15-30%
Duodenum 30-45%
Pancreas 15-20%
Jejunum/ileum 90%
Appendix 90%
Rectum 0-30%

04/04/2016
36
Page 36
Metastatic well-differentiated neuroendocrine tumor from ileum
CDX2
Metastatic well-differentiated neuroendocrine tumor from ileum
CDX2
Metastatic well-differentiated neuroendocrine tumor from pancreas
CDX2

04/04/2016
37
Page 37
TTF1 expression in well-differentiated neuroendocrine tumors
Primary site Positive
Lung 30-70%
Stomach <5%
Duodenum <5%
Pancreas <5%
Jejunum/ileum <5%
Appendix <5%
Rectum <5%
Lung carcinoid tumor
TTF1
PAX6 expression in well-differentiated neuroendocrine tumors
Primary site Positive
Lung 0-10%
Stomach 15%
Duodenum 80%
Pancreas 55-70%
Jejunum/ileum 0%
Appendix 15%
Rectum 60%

04/04/2016
38
Page 38
PAX6 expression in well-differentiated neuroendocrine tumors
Primary site Positive
Lung 0-10%
Stomach 15%
Duodenum 80%
Pancreas 55-70%
Jejunum/ileum 0%
Appendix 15%
Rectum 60%
PAX6
PAX5
PAX8
Polyclonal PAX8 antibody
Pancreatic well-differentiated neuroendocrine tumor
pPAX8

04/04/2016
39
Page 39
Metastatic well-differentiated neuroendocrine tumor from ileum
pPAX8
Pancreatic well-differentiated neuroendocrine tumor
PAX6
Papillary thyroid carcinoma
PAX6

04/04/2016
40
Page 40
Lymph node
PAX6
PDX1
• Pancreatic and duodenal homeobox transcription factor
• Also known as insulin promoter factor 1
• Necessary for pancreatic development
• Plays role in maturation of islet cells that secrete insulin (β-cells) and somatostatin (δ-cells)
• In adult pancreas, strong nuclear expression in islet cells, weak staining in centroacinar cells
PDX1 expression in well-differentiated neuroendocrine tumors
Primary site Positive
Lung 0-5%
Stomach 60%
Duodenum 60%
Pancreas 55-80%
Jejunum/ileum 0%
Appendix 40%
Rectum 15%

04/04/2016
41
Page 41
PDX1 expression in well-differentiated neuroendocrine tumors
Primary site Positive
Lung 0-5%
Stomach 60%
Duodenum 60%
Pancreas 55-80%
Jejunum/ileum 0%
Appendix 40%
Rectum 15%
PDX1
Metastatic pancreatic well-differentiated neuroendocrine tumor
PDX1
Metastatic pancreatic well-differentiated neuroendocrine tumor

04/04/2016
42
Page 42
ISL1
• ISLET1
• Transcription factor with N-terminal LIM domains and C-terminal homeodomain
• Plays critical role in develop of pancreatic islets of Langerhans
• In adults, strong nuclear expression in islets
• Clinically used antibodies show cytoplasmic staining in perivascular smooth muscle
ISL1 expression in well-differentiated neuroendocrine tumors
Primary site Positive
Lung 10-15%
Stomach 0%
Duodenum 90%
Pancreas 70-85%
Jejunum/ileum <5%
Appendix 15-20%
Rectum 90%
ISL1 expression in well-differentiated neuroendocrine tumors
Primary site Positive
Lung 10-15%
Stomach 0%
Duodenum 90%
Pancreas 70-85%
Jejunum/ileum <5%
Appendix 15-20%
Rectum 90%

04/04/2016
43
Page 43
Pancreas
ISL1
Pancreatic well-differentiated neuroendocrine tumor
ISL1
ISL1
Metastatic well-differentiated neuroendocrine tumor from ileum

04/04/2016
44
Page 44
Small cell carcinoma
• Determination of primary site not important – All patients treated with cisplatin/carboplatin +
etoposide
• Localized Merkel cell carcinoma treated surgically
• TTF1 is not specific for lung in this setting – TTF1 positive in >90% of small cell carcinoma
of lung
– TTF1 positive in 30-50% of extrapulmonary small cell carcinoma
– TTF1 rarely positive in Merkel cell carcinoma
Metastatic small cell carcinoma
TTF1
Other transcription factors in small cell carcinoma
• Small cell carcinomas show marked transcription factor lineage ‘infidelity’!
• Common to detect expression of 5-10 (or more) different transcription factors in both pulmonary and extrapulmonary small cell carcinomas
• Important to be aware of this phenomenon to avoid misinterpretation

04/04/2016
45
Page 45
Transcription factor expression in
small cell and Merkel cell carcinomas
Courtesy of Dr. Andrew Bellizzi
IHC for evaluation of
metastatic WDNET of
unknown primary
Bellizzi Adv Anat Pathol 2013
Practice points
• Review radiologic findings (could the biopsy be from a primary liver tumor?)
• Pay close attention to histologic features – Guide judicious panel of IHC markers
• Increasing range of antibodies directed against transcription factors becoming available – for carcinomas and well-differentiated neuroendocrine tumors
• Be aware of reported cross-reactivity (i.e., specificity) to avoid misdiagnosis