imaging of the breast in young women - 108 harley street · imaging of the breast in young women...
TRANSCRIPT

Imaging of the Breast in Young Women
William Teh
Northwick Park Hospital
North London Breast Screening Centre
The London Breast Clinic Symposium
6th May 2010

Two main rationale:
Breasts relatively radiosensitive under the age of 35
In absence of risk factors, probability of malignancy increases with age
Imaging of the Breast By Age

Below 12 years: Rarely required – most commonly occasional breast buds in toddlers and pre-pubertal breast changes
12 – 16: Ultrasound
16 – 25: Ultrasound: most common solid lesions are fibroadenomas. If needle biopsy required usually FNA
25-35: Ultrasound. Core biopsy preferred
35 and above: Mammography and US. Core biopsy if abnormality detected.
Imaging of the Breast By Age

Full field digital mammography superior in multi-centre trials for cancer detection in:
Pre/peri-menopausal women
Women with dense breasts / HRT
Women < 50
Not indicated unless symptomatic in under 40s
DMIST 2005
Mammography in pre-menopausal
women

> 75% mammographic density => 4-5x risk
Women with decrease of breast density over 6 years – 28% lower risk
?higher aromatase levels (converts androgens to oestrogens)
16% higher risk of cancer recurrence
American Association for Cancer Research 2010
Cancer 2009
San Antonio 2008
Mammographic density and risk of
breast cancer

Tomosynthesis
Digital contrast examinations
Quantification of risk using mammographic density
Mammographic developments

Not as good as mammography in fatty breasts, adipose breasts or large breasts.
Limited application in young women with benign breast change
Shown to be slightly more effective than mammography but significantly inferior to MRI in women with family history
High risk studies: mammography + US – 52% sensitivity vs mammography + MRI – 92.7% sensitivity
ACRIN6666 study shows high false positive detection (only 8.8% biopsies were cancers)
Ultrasound of the Breast:
Alternative to screening mammograms?

Most sensitive method for detection of breast cancer
Contrast enhanced – vascularity of tumours
Multiple applications –
Implant assessment
Scar vs. cancer recurrence
Further evaluation of proven malignancy: local staging & multi-focality (NICE 2009)
Detection of occult breast cancer in axillary lymph node metastasis
Screening high-risk pre-menopausal women
Monitoring neo-adjuvant chemotherapy
MRI: Form… and function

North West London Hospitals NHS
Trust
MRI and Silicone Implants
Meta-analyses 1099 implants over 7 years
Median life-span 16.4 years; 79.1% intact
at 10 years, falling to 48.7% by 15 years
sensitivity specificity
Mammo 28.4 92.9
US 59 76.8
MRI 78.1 80
Goodman CM et al. Annals of Pl Surg 1998;41(6):577-585

North West London Hospitals NHS
Trust
MRI:
Implants

North West London Hospitals NHS
Trust
Pre-operative MRIIncreasingly used to assess extent of biopsy proven cancer, multi-focality/centricity, dense breasts, invasive lobular carcinoma
Surgical treatment changed in 13% -34%
Multi-focality / multicentricity 16%
Contralateral malignancy 3.1% (ACRIN 6667 study NEJM 2007)
Lehman et al NEJM 2007
Martinez-Cecilia et al ECCO 2008
Krishnan M et al, Antonella et al, Lehman C et al ARRS 2008
Houssammi et al, J Clin Oncol 2008
North West London Hospitals NHS
Trust
Pre-operative MRIOffer magnetic resonance imaging (MRI) of the breast to
patients with invasive breast cancer:
if discrepancy regarding extent of disease from clinical examination, mammography and ultrasound assessment for planning treatment
if breast density precludes accurate mammographic assessment
to assess the tumour size if breast conserving surgery is being considered for invasive lobular cancer.
NICE 2009

North West London Hospitals NHS
Trust
Pre-operative MRIMay delay definitive surgery due to delays in MRIs and investigations of false positives (41 days vs 27 days)
Unnecessary investigations and biopsies (40-50%)
Risk influencing unnecessary mastectomies (12.5-33%)
No evidence of impact on local recurrence rate or mortality benefit as yet
Sandberg A et al, Krishnan M et al. ARRS 2008

North West London Hospitals NHS
Trust
Pre-operative MRI8.1% conversion from wide local excision to mastectomy due
to true positive findings
1.1% conversion from wide local excision to mastectomy due
to false positive findings
3.0% conversion from wide local excision to wider/additional
excision due to true positive findings;
4.4% conversion from wide local excision to wider/additional
excision due to false positive findings.
Over-treatment can be decreased by using second look
US/MRI guided biopsy
Houssami 2008
Eusoma 2010

North West London Hospitals NHS
Trust
Pre-operative MRI: EUSOMA
(2010)Patients with invasive lobular cancer
Patients at high risk of breast cancer
Patients <60 with discrepancy of >1cm between mammographic findings and US findings
Patients eligible for partial breast irradiation
Patients must be aware of risks and benefits
Delay should not be > 1 month
MRI biopsy/localisation should be accessible

North West London Hospitals NHS
Trust

North West London Hospitals NHS
Trust

North West London Hospitals NHS
Trust

North West London Hospitals NHS
Trust
MRI in axillary metastases
McMahon K, Medoro L, Kennedy D Australas Radiol. 2005
Sensitivity 85.7% accuracy 86.7%
78% confirmed histologically
55% suitable for conservative surgery
Morris et al – 9/12 (75%) detected; 8/12 (66.7%)
suitable for conservation
Koh et al 2007 – 10/12 (83%) detected; 2/12
remain disease free at 39 and 44 months

North West London Hospitals NHS
Trust
38 yo right metastatic axillary nodes – dense breasts cysts.

North West London Hospitals NHS
Trust

North West London Hospitals NHS
Trust
MRI for neoadjuvant
chemotherapyMonitoring response to neoadjuvant chemotherapy
Baseline, mid-cycle, completion of chemo
Assessment of response may be possible after one or two cycles
Particularly useful to assess if conservative surgery feasible
BUT does not exclude presence of residual disease – eg Belli et al 2007 – 90.5% sensitivity, 100% specificity, 91.3% accuracy in detecting residual disease

North West London Hospitals NHS
Trust

North West London Hospitals NHS
Trust

10% breast cancers run in families (only 2%
identified mutations)
Young women who had radiotherapy for
lymphoma
MRI improves breast cancer detection even
when other tests normal (2X more cancers
detected)
MRI in high-risk premenopausal
women

North West London Hospitals NHS
Trust
Mammography & MRI screening
guidelines
UK NICE May 2004 / October 2006
American Cancer Society Guidelines Aug 2007
NICE Breast Cancer Management 2009
Eusoma 2010

North West London Hospitals NHS
Trust
NICE guidance: High risk10-year risk of 8% aged 30–39 & 10-year risk
of 12% aged 40–49 years:
2 close relatives diagnosed with average age < 30*
3 close relatives diagnosed with average age < 40*
4 close relatives diagnosed with average age < 50*
A genetic test required to determine a 10-year risk ≥20% in women 40–49.
*All relatives must be on the same side of the family and one must be a mother or sister of the woman.

North West London Hospitals NHS
Trust
NICE guidance: High risk
BRCA1/2 – aged 30-49
TP53 – aged 20+
.50% risk of carrying mutation in gene
tested family or untested/inconclusive
tested family with 60% risk of
BRCA1/TP53
In England, 2,500/49.8 million
population

North West London Hospitals NHS
Trust
Surveillance in high-risk
premenopausal womenInformed consent – pros and cons including
false positive/negatives
Protocols
Counselling
Genetic testing
Surveillance audited and according to
NHSBSP standards

North West London Hospitals NHS
Trust
Mammography in high-risk
premenopausal women
According to NHSBSP standards
Higher sensitivity for DCIS (Kriege 2004)
DCIS more common in BRCA2
Should be digital mammography

North West London Hospitals NHS
Trust
Mammography in high-risk
premenopausal womenEvidence of benefits in 40-49
No evidence of benefits in 30-39
Mammo for 30-39 ‘only as part of a approved
research study/audited service’ and ‘
individualised strategies for exceptional cases,
such as BRCA1, BRCA2 or TP53and women
with equivalent high breast cancer risk.
Not to occur in < 30s
>50s: NHSBSP
North West London Hospitals NHS
Trust
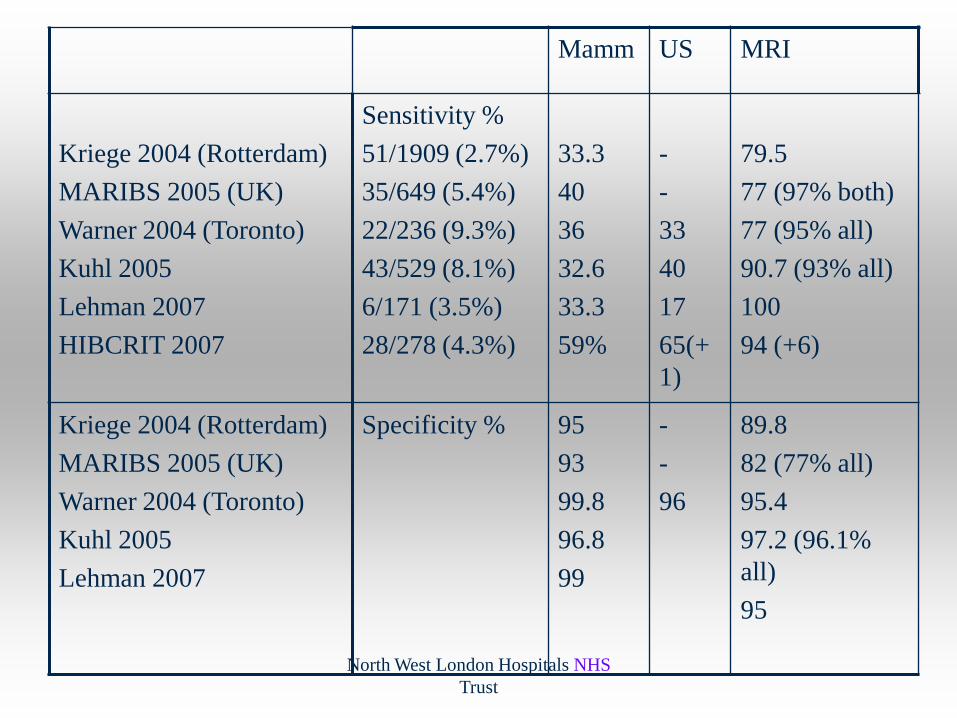
Mamm US MRI
Kriege 2004 (Rotterdam)
MARIBS 2005 (UK)
Warner 2004 (Toronto)
Kuhl 2005
Lehman 2007
HIBCRIT 2007
Sensitivity %
51/1909 (2.7%)
35/649 (5.4%)
22/236 (9.3%)
43/529 (8.1%)
6/171 (3.5%)
28/278 (4.3%)
33.3
40
36
32.6
33.3
59%
-
-
33
40
17
65(+
1)
79.5
77 (97% both)
77 (95% all)
90.7 (93% all)
100
94 (+6)
Kriege 2004 (Rotterdam)
MARIBS 2005 (UK)
Warner 2004 (Toronto)
Kuhl 2005
Lehman 2007
Specificity % 95
93
99.8
96.8
99
-
-
96
89.8
82 (77% all)
95.4
97.2 (96.1%
all)
95

EVA Multi centre trial (ASCO 2008)
687 high risk women 2002-2005 (27 cancers overall
incidence 16.1/1000)
FFDM, US, MRI
FFDM only – 9 cancers
FFDM + US – 4 additional cancers
FFDM + MRI – all cancers (2 DCIS on FFDM only)
US + MRI – no additional cancers
US vs MRI in high risk

North West London Hospitals NHS
Trust
NICE guidance (summary):
Age Risk Mammo MRI
20+ TP53 No Yes
30-39 TP53, BRCA1/2
10yr risk > 8%
(Yes) Yes
40-49 TP53 (50% risk)
BRCA1/2 (50%
risk)
10 yr risk > 20%
10yr risk > 12%
and ‘dense’ breasts
Yes
Yes
Yes
Yes
Yes
Yes
Yes

North West London Hospitals NHS
Trust
Breast Surveillance In Young Women Post
Supradiaphragmatic Irradiation (SDI) for
Hodgkin’s DiseaseSDI < 17 y.o. – screen from age 25
SDI 17-35: screening to begin 8 years after completion of treatment.
EAG 2003
Age (years) Recommended surveillance
< 25 No imaging
25-29 Annual MRI (if contraindicated annual US)
30-50 Baseline mammograms. ± MRI (breast desnity)
>50 NHS BSP

North West London Hospitals NHS
Trust
Risk Groups - questions
Other groups:
?follow-up for treated breast cancer
? Atypia
? Dense breasts
What about > 50s?
What about MRI in moderate risk groups?

North West London Hospitals NHS
Trust
High risk screening to be aligned with
NHSBSP
Investment include Digital Mammography
MRI screening QA criteria requires critical
volume and radiological expertise (already
required for Hodgkin’s)
UK Cancer Reform Strategy
Dec 2007:

North West London Hospitals NHS
Trust
Minimum technical standards
Double reading (minimum 5,000 mammo
and 100 MRI/year)
MRI vacuum biopsy – minimum 100 non-
MR and 12 MR-vacuum biopsies / year
Standards low – currently only 1 centre in
UK exceeds 12 MR vacuum biopsies / year!
Draft NHSBSP MRI Screening:

North West London Hospitals NHS
Trust
Progress so far:
Only 6/82 NHSBSP units have gone digital
Only 1 NHSBSP service in London fully digital
Only 1 MRI unit in UK undertakes more than 12 MRI guided biopsies a year

North West London Hospitals NHS
Trust
Summary
Imaging (US and mammograms) straified by age
(US < 35)
Digital mammography best in < 50s / pre/peri-
menopausal
MRI used effectively in high risk screening,
optimised by MDT for pre-operative staging, neo-
adjuvant chemotherapy, implant complication and
occult axillary metastases
Research questions for other sub-groups