imaging of idiopathic intracranial hypertension · quincke in 1893 as a meningitis serosa and since...
TRANSCRIPT

Imaging of Idiopathic IntracranialHypertension
Anna Zimny and Marek J. Sąsiadek
ContentsDefinition and Terminology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Clinical Presentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Clinical Evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Neuroimaging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Changes Within the Orbits . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Changes Within the Intracranial Compartment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Suggested Imaging Approach . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Checklist for MR Reporting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Treatment and Prognosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Clinical Scenario . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Patient History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Clinical Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Purpose of MR Study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11MR Technique . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
This publication is endorsed by: European Society ofNeuroradiology (www.esnr.org)
A. Zimny (*) · M. J. SąsiadekDepartment of General Radiology, InterventionalRadiology and Neuroradiology, Wroclaw MedicalUniversity, Wroclaw, Polande-mail: [email protected]; [email protected]
# Springer Nature Switzerland AG 2019F. Barkhof et al. (eds.), Clinical Neuroradiology,https://doi.org/10.1007/978-3-319-61423-6_13-1
1

Full Findings (MR Report) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Interpretation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Comments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
AbstractIdiopathic intracranial hypertension (IIH) is asyndrome due to increased intracranial pres-sure without any evident cause, previouslyknown as pseudotumor cerebri. We discussthe etiology, epidemiology, clinical symptoms,treatment options, and radiological findings ofIIH, a rare condition with a predominance inobese women of reproductive age but also seenin men and children. The pathophysiology ofIIH is not well understood, and several mech-anisms are suggested to play a role such asexcessive cerebrospinal fluid (CSF) produc-tion, impaired CSF absorption, increased intra-vascular volume, or increased intracranialvenous pressure. Known risk factors are cer-tain medications, hormonal alterations, infec-tions, as well as autoimmune disorders. Mainclinical symptoms of IIH are headache andvision loss, less frequently pulsatile tinnitus,diplopia, photopsia, eye pain, or cranial nervepalsies. Ophthalmological evaluation usuallyreveals papilledema. Lumbar puncture demon-strates elevated opening CSF pressure. Therole of clinical neuroradiology is firstly toexclude causes of secondary intracranialhypertension due to space-occupying masses,hydrocephalus, infection, or vascular patholo-gies including venous sinus thrombosis. Sec-ondly, imaging can show findings that supportthe diagnosis of IIH such as enlargement of theperioptic CSF spaces, tortuosity of the opticnerves, flattening of the posterior aspect ofsclera, intraocular protrusions of optic nerveheads and their contrast enhancement, partiallyempty sella, enlarged Meckel’s cave, smallmeningoceles within the skull base, slit-likeventricles, acquired tonsillar ectopia, and trans-verse sinus narrowing. Recommended radio-logical protocol includes contrast-enhancedMR examination of the brain and orbitsfollowed by MR venography.
KeywordsIntracranial hypertension · Pseudotumorcerebri · Thunderclap headache · Papilledema ·Empty sella · Cerebrospinal fluid
AbbreviationsCISS Constructive interference in steady
stateCN Cranial nerveCSF Cerebrospinal fluidCT Computed tomographyDRIVE Driven equilibriumDWI Diffusion-weighted imagingFIESTA Fast imaging employing steady-
state acquisitionIIH Idiopathic intracranial hypertensionMR Magnetic resonanceMRI Magnetic resonance imagingMRV Magnetic resonance venographyONS Optic nerve sheathSWI Susceptibility-weighted imagingTOF Time of flight
Definition and Terminology
Idiopathic intracranial hypertension (IIH) is aclinical syndrome with signs and symptoms ofincreased intracranial pressure without an identi-fiable cause. It was first described by HeinrichQuincke in 1893 as a meningitis serosa and sincethen kept changing names through decades. Thepreviously used terms such as “pseudotumorcerebri” and “benign intracranial hypertension”are suggested to be avoided and have beenreplaced by IIH. However, this term may also bemisleading since in 14–90% of patients with IIH,there is a potential identifiable cause present suchas venous sinus stenosis or coexisting conditionsincluding certain medical disorders, medications,and infections which may lead to increased intra-cranial pressure (Table 1). This shows that
2 A. Zimny and M. J. Sąsiadek

probably purely idiopathic intracranial hyperten-sion is a rare entity.
IIH needs to be differentiated from secondarycauses of raised intracranial pressure which areassociated with easily identifiable causes such asspace-occupying lesions, hydrocephalus, infec-tion or venous sinus thrombosis, etc.
Etiology
The precise etiology of IIH is largely unknown.According to the Monro-Kellie doctrine, the cra-nium is a non-compressible structure with a fixedvolume and three major compartments of theintracranial space (brain tissue, CSF, and blood)
kept in a state of dynamic volume equilibrium.Thus, the increased intracranial pressure may becaused by many different mechanisms leading notonly to the elevated CSF volume (due to increasedCSF production, decreased CSF resorption, orincreased CSF outflow resistance) but also ele-vated cerebral volume (due to increased intersti-tial fluid capacity) or raised venous or arterialblood volumes (due to increased arterial or venouspressure, loss of cerebral autoregulation, orobstruction in the venous drainage) (Walker2001).
There is also a strong correlation between IIHand certain diseases or hormonal conditions. Along list of known risk factors which show strongassociation with development of IIH is demon-strated in Table 1. Several recent studies have alsorevealed an increased incidence of transversesinus stenosis among the patients with IIH; how-ever it is still debatable whether narrowing ofthese sinuses is a primary cause or a secondaryeffect of IIH.
Epidemiology
IIH is a rare condition occurring in the generalpopulation with an incidence of 0.9 cases per100,000 inhabitants with a strong female predom-inance (female/male ratio of 8:1). It occurs mostoften in young adults between 22 and 40 years ofage and shows strong association with obesityespecially with a rapid weight gain (19 cases per100,000 among obese women) (Chen and Wall2014). According to the old concept, the develop-ment of IIH in obese patients was explained by theelevation of both intraabdominal and intrathoracicpressure leading to the elevation of the centralvenous pressure and finally resulting in theincreased intracranial pressure. Most recently bio-chemical factors such as a prothrombotic state,enhanced estrogenicity, inflammatory cytokineexpression, or endocrinologic dysfunction arebelieved to trigger the development of IIH.
While the most common clinical scenario forIIH is an overweight woman in the reproductiveage, IIH may also occur in older women, men, or
Table 1 Risk factors of IIH. (Adopted from Chen et al.2014)
Highly likely risk factors
Female genderObesity/weight gainEndocrine disorders (Addison’s disease,hypoparathyroidism, steroid withdrawal, growthhormone use in children)Nutritional disorders (hypervitaminosis A,hyperalimentation)
Probable risk factors
Chlordecone (kepone)Ketoprofen and indomethacinThyroid replacement therapyTetracycline and its derivativesUremia
Possible risk factors
Sleep apneaSystemic lupus erythematosusAmiodaroneHypovitaminosis AIron-deficiency anemiaLithium carbonateNalidixic acidSarcoidosisSulfa antibioticsHypophosphatasia
Unlikely or unproven risk factors
Corticosteroid intakeHyperthyroidismArterial hypertensionMultivitamin intakeMenarcheMenstrual irregularitiesPregnancyOral contraceptive use
Imaging of Idiopathic Intracranial Hypertension 3

even in the pediatric population with greater fre-quency in postpubertal females.
Clinical Presentation
The most common clinical symptom of IIH is apressure-like, throbbing, and usually unremittingheadache with retro-ocular pain often accompa-nied by nausea. It occurs in 90–94% of patientswith IIH.
The second most frequent complaint is a visionloss which is usually rapid but transient in natureand is found in 68–85% of patients. It may presentas deficits in the visual field, typically tunnelvision. Partial or total vision loss may becomepermanent if symptoms of IIH persist. Blindnessis the most serious complication of chronic IIH.
Pulse-synchronous tinnitus is another com-monly reported symptom of IIH occurring inabout 58% of patients. It may be exacerbated bypositional changes and relieved by jugular com-pression. Other common symptoms includephotopsia which is a presence of perceived flashesof light (54%), eye pain (44%), and diplopia(38%) or rarely cranial nerve palsies usually ofthe abducens nerve (10–20%).
Less frequently some patients with long-lasting IIH and meningoceles may develop signsof CSF leaks such as rhinorrhea, otorrhea, intra-cranial hypotension, and recurrent bacterialmeningitis.
Patients with IIH may also be asymptomatic(Degnan and Levy 2011).
Clinical Evaluation
Ophthalmologic assessment reveals diminishedvisual acuity, visual field losses, and most strik-ingly papilledema on fundoscopy. It has to bestressed that papilledema may not be present inevery subject; it occurs in around 40% of patientsand may be uni- or bilateral.
Neurological examination is usually normalwith an exception of patients with the sixthnerve palsy. Measurements of CSF pressure dur-ing lumbar puncture performed in the lateral
decubitus position reveal increased opening pres-sure of CSF above 200 mmH2O in normal weightsubjects and above 250 mmH2O in obese patients.Composition of CSF is normal.
Since 2013 revised diagnostic criteria pro-posed by Friedman et al. have been used to diag-nose IIH in adults and children (Table 2).
Neuroimaging
Major goals of neuroimaging are to exclude sec-ondary causes of intracranial hypertension as wellas to detect typical signs of IIH.
The most frequent causes of secondary intra-cranial hypertension are intracranial space-occupying lesions (tumors, abscesses), increasedCSF production (i.e., choroid plexus papilloma),decreased CSF absorption (ependymitis, adhe-sions within subarachnoid space, subarachnoidhemorrhage), obstructive hydrocephalus, orobstruction in the venous outflow (due to cerebralvenous sinus thrombosis, jugular vein compres-sion, etc.).
Table 2 Revised diagnostic criteria for IIH in adults andchildren. (Adopted from Friedman et al. 2013)
If papilledema is present
Normal neurological examination except for cranialnerve abnormalities
NeuroimagingNormal brain parenchyma without evidence ofhydrocephalus, mass, or structural lesion, and noabnormal meningeal enhancement on MRIIf MRI is unavailable or contraindicated, contrast-enhanced CT may be used
Normal CSF composition
Elevated CSF opening pressure (�250 mmH2O in adultsand �280 mmH2O in children, [250 mmH2O if the childis not sedated and not obese]) in a properly performedlumbar puncture
If papilledema is not present
Either a CN6 palsy (unilateral or bilateral) or �3neuroimaging criteria must be additionally satisfied:1. Empty sella2. Flattening of the posterior aspect of the globe3. Distention of the perioptic subarachnoid space with orwithout a tortuous optic nerve4. Transverse venous sinus stenosis
4 A. Zimny and M. J. Sąsiadek

Typical imaging signs of IIH regard changeswithin orbits and intracranial space including thebrain, skull base, and transverse dural venoussinuses.
Changes Within the Orbits
Optic nerves are outpouchings of diencephalonsurrounded by CSF and meninges. The opticnerve sheath (ONS) is composed of CSF withinperioptic subarachnoid space and dura. The imag-ing features found in IIH are uni- or bilateralenlargement of ONS diameter to more than5 mm (Fig. 1) and vertical tortuosity of the opticnerves seen in about 45–67% of patients (Fig. 2).Orbital abnormalities may be explained by adirect transmission of the elevated intracranialand CSF pressure via subarachnoid space sur-rounding the optic nerves, but their appearancedoes not correlate with the clinical symptoms ofpapilledema.
Radiological signs associated withpapilledema and visual disturbances are flatteningof the posterior part of the globe, intraocular pro-trusions, and contrast enhancement of the opticnerve heads (Fig. 3). These signs are reported tobe present in 50–80% of patients with IIH. Theyreflect increased intracranial pressure transferredto the globe as well as venous congestion, capil-lary leakage, and possibly breakdown of theblood-retinal barrier within posterior sclera(Suzuki et al. 2001, Degnan and Levy 2011,Bidot et al. 2015).
Orbital abnormalities may be demonstrated onaxial or coronal images using thin-slicedT2-weighted images. To enhance their detection,fat-saturated T2-weighted images or 3D heavilyT2-weighted steady-state sequences such as3D-DRIVE (Philips), 3D-CISS (Siemens), and3D-FIESTA (GE) are recommended.
Fig. 1 Fat-saturated T2-weighted (a, c) and 3D heavily T2-weighted steady-state (b, d) images showing enlargedperineural arachnoid space around the optic nerves
Imaging of Idiopathic Intracranial Hypertension 5

Fig. 2 Tortuous course of the optic nerves within orbits better appreciated on fat-saturated T2-wieghted images (a)compared to T2-weighted images without fat suppression (b)
Fig. 3 Typical findings of IIH within eye balls: (a) flat-tened posterior aspect of the sclera on T2-weighted sagittalimage, (b) intraocular protrusions of optic nerve heads on
3D heavily T2-weighted axial image, (c, d) contrastenhancement of optic nerve heads after gadolinium admin-istration on 3D post-contrast T1-weighted images
6 A. Zimny and M. J. Sąsiadek

Changes Within the IntracranialCompartment
Majority of imaging signs found within the intra-cranial space are due to enlargement of the arach-noid space and its outpouchings.
One of them is a partially empty sella signoccurring in 70–80% of IIH patients. It is pro-duced by a downward herniation of arachnocelethrough the diaphragma sellae and subsequentflattening of the pituitary gland. This sign requirestime to be developed (Fig. 4). Normal height ofthe pituitary gland in adults changes in lifereaching 3–10 mm in younger population andbelow 3 mm in people above 50 years old. Par-tially empty sella may be a normal appearance inthe senior population. It is best depicted on sagit-tal T1- or T2-weighted images.
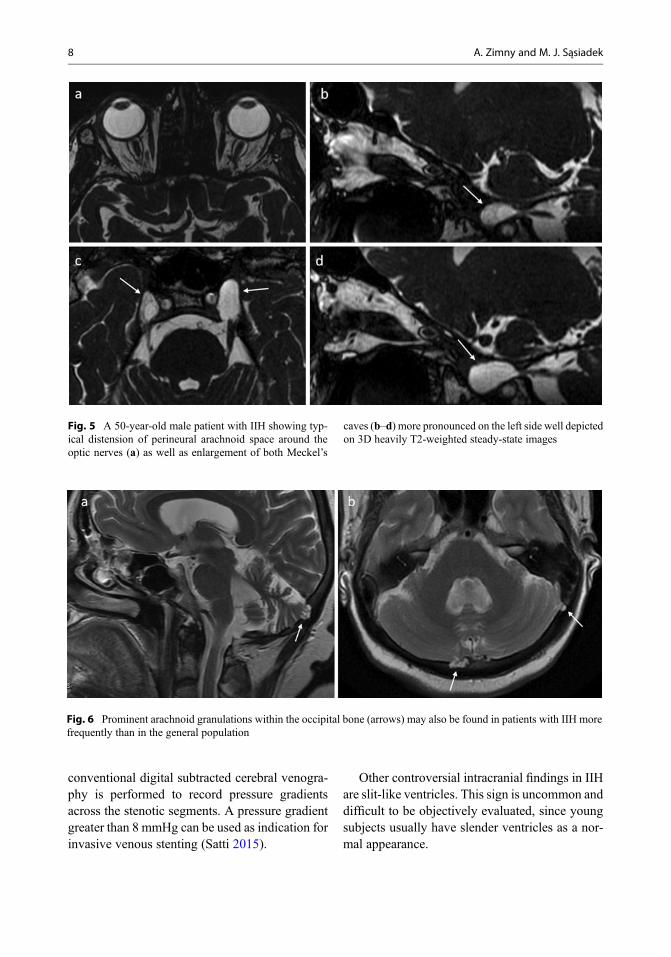
Increased volume of the arachnoid space in IIHmay also result in the enlargement of Meckel’scaves (their normal diameter should not exceed6–8 mm in transverse plane and 3–5 mm in coro-nal plane), enlarged CSF space around the oculo-motor nerve in the cavernous sinus (oculomotorcistern), prominent arachnoid granulations, and/orlarge spontaneous protrusions of the meninges
called meningoceles usually within the skullbase (Figs. 5 and 6).
Meningoceles may cause bone scalloping anderosions as well as CSF leaks when ruptured.Patients with CSF leaks often do not have clinicalsymptoms of intracranial hypertension suggestingthat CSF leaks probably decompress the elevatedintracranial pressure. Clinical symptoms of IIHappear again when the CSF leaks undergo spon-taneous repair. Imaging sequences of choice tovisualize the above arachnoid space abnormalitiesare T2-weighted images especially 3D heavilyT2-weighted steady-state sequences (CISS/FIESTA/DRIVE). In case of CSF leaks, intrathe-cal contrast-enhanced CT or MR cisternographymay be required (Bialer et al. 2014).
Transverse sinus narrowing has been recentlyreported to be found in 65–90% of patients withIIH undergoing contrast-enhanced MR or CTvenography. Narrowing is usually located withinlateral aspects of transverse sinuses with theabsence of previous or current thrombosis(Fig. 7). It is still unclear whether bilateral venousstenosis plays a role in pathogenesis of IIH (due tovenous outflow obstruction) or is the secondaryresult of the increased intracranial pressure lead-ing to venous wall compression. Invasive
Fig. 4 Changes of the size of the pituitary gland in thecourse of IIH in a 36-year-old female patient with pulsatileheadaches, worse vision in the right eye and bilateralpapilledema: (a) initial MR examination demonstrating
normal pituitary gland and follow-up MR examination(b) after 3 months of treatment with acetazolamid with anew onset of clinical symptoms showing decreased size ofthe pituitary gland
Imaging of Idiopathic Intracranial Hypertension 7
conventional digital subtracted cerebral venogra-phy is performed to record pressure gradientsacross the stenotic segments. A pressure gradientgreater than 8 mmHg can be used as indication forinvasive venous stenting (Satti 2015).
Other controversial intracranial findings in IIHare slit-like ventricles. This sign is uncommon anddifficult to be objectively evaluated, since youngsubjects usually have slender ventricles as a nor-mal appearance.
Fig. 5 A 50-year-old male patient with IIH showing typ-ical distension of perineural arachnoid space around theoptic nerves (a) as well as enlargement of both Meckel’s
caves (b–d) more pronounced on the left side well depictedon 3D heavily T2-weighted steady-state images
Fig. 6 Prominent arachnoid granulations within the occipital bone (arrows) may also be found in patients with IIH morefrequently than in the general population
8 A. Zimny and M. J. Sąsiadek

Acquired tonsillar ectopia may also be presentin around 10–20% of patients with IIH which isoften misinterpreted as Chiari 1 malformation. Incontrast to Chiari 1 malformation, this conditiondoes not respond to decompression surgery butrequires CSF shunting surgery (Aiken et al. 2012)(Table 3).
Suggested Imaging Approach
MR imaging is the method of choice in the eval-uation of patients with IIH. However, IIH patientswith acute clinical symptoms such as thunderclapheadache and rapid visual deterioration mightpresent at emergency departments and undergohead CT as their initial neuroimaging examina-tion. In some cases, major features of IIH will bepossible to be evaluated on the basis of emergencyCT examination such as enlargement of opticnerve sheath, tortuous course of the optic nerve,or empty sella (Fig. 8).
The MR protocol needs to be tailored in orderto rule out secondary causes of intracranial hyper-tension (especially space-occupying lesions,hydrocephalus, intracranial infection, dural sinusthrombosis, and vascular malformations) as wellas to detect typical neuroimaging signs of IIH.MR imaging should cover orbits and intracranialspace in one examination. Radiological evalua-tion of the intracranial space should include thor-ough evaluation of the brain, skull base(especially pituitary gland), dural venous sinuses,and cranio-cervical junction. The recommendedMR protocol is shown in Table 4.
Checklist for MR Reporting
Step 1 – exclude major causes of secondary intra-cranial hypertension– Space-occupying lesions– Hydrocephalus– Intracranial infection– Vascular malformations– Cerebral venous thrombosis
Step 2 – look for typical imaging signs of IIH– Optic nerve sheath enlargement above
5 mm in diameter– Tortuous course of the optic nerves– Intraocular protrusions of the optic nerve
heads
Fig. 7 Two-dimensional time-of-flight MR venography ina patient with IIH showing loss of signal in the lateralaspects of both transverse sinuses what may indicate bilat-eral stenoses. The image requires further investigation withcontrast-enhanced 3D MR venography or invasive digitalsubtracted venography if stenting procedure is planned
Table 3 Imaging signs of IIH
Orbits (uni- or bilaterally)aDistension of the optic nerve sheath diameter above5 mmTortuous course of the optic nerveaFlattening of the posterior part of the globeaIntraocular protrusions of the optic nerve headsContrast enhancement of the optic nerve heads
Intracranial spaceaPartially empty sellaEnlargement of Meckel’s cavesProminent arachnoid granulationsMeningoceles within skull baseCSF leaksSlit-like ventriclesAcquired tonsillar ectopiaaTransverse sinus stenosis (uni- or bilateral)aImaging signs with the highest specificity in diagnosis ofIIH
Imaging of Idiopathic Intracranial Hypertension 9

Fig. 8 A 43-year-old female admitted to the emergencyunit with severe headache and signs of bilateralpapilledema. CT of the head showed typical orbitalchanges such as bilateral distension of ONS and tortuous
course of both optic nerves well depicted on axial (a, b) aswell as reformatted coronal images (c) with partially emptysella demonstrated in the reformatted sagittal view (d)
Table 4 Recommended MR protocol in IIH
MR sequenceCoveredanatomy Major indications
Sagittal T1-weighted Head To rule out empty sella, to evaluate cranio-cervical junction
Axial T2-weighted andFLAIR
Intracranialspace
To rule out space-occupying lesions, hydrocephalus, or other brainpathologies causing secondary intracranial hypertension
3 mm axial and coronalfat-saturated T2-weighted
Orbits To evaluate optic nerve sheath diameter and optic nerve course
3D heavily T2-weightedsteady state(FIESTA/DRIVE/CISS)
Orbits and skullbase
To evaluate optic nerve sheath diameter, optic nerve course,flattening of the posterior aspects of the globes or intraocularprotrusions of the optic nerves, and enlargement of the arachnoidspaces at the skull base
3D post-contrastT1-weighted
Orbits andintracranialspace
To rule out optic nerve head enhancement, intracranial pathologicalenhancement, and venous sinus thrombosis
Alternatively:MR venography – TOF and3D post-contrast MRV
Intracranialvenous system
To rule out venous sinus thrombosis and narrowing of thetransverse sinuses
10 A. Zimny and M. J. Sąsiadek

– Enhancement of the optic nerve heads– Partially empty sella– Transverse sinus narrowing
Step 3 – assess additional findings which may bepresent only in some cases– Enlargement of Meckel’s caves– Meningoceles within skull base– Prominent arachnoid granulations– CSF leaks– Slit-like ventricles– Acquired tonsillar ectopia
Treatment and Prognosis
IIH may be a self-limiting condition, but in manycases, it becomes chronic and requires treatment.Treatment of IIH has two major goals which arethe alleviation of symptoms mainly headache andpreservation of vision. Weight loss isrecommended to all obese patients as it bringsvery good clinical results. Other treatment optionsinclude management with medications reducingCSF production such as acetazolamide ortopiramate. Therapeutic lumbar punctures arenot recommended since they bring only short-term result. CSF shunting (ventriculoperitonealor lumboperitoneal) is only reserved for certaincases usually with fulminant clinical course andrapid visual loss. Optic nerve sheath fenestrationmay also be performed in fulminant cases notresponding to medical management.
Some centers propose the use of endovascularstenting of the transverse sinus in patients withIIH refractory to medical management, but thismethod is still under debate. A recent meta-analysis of venous sinus stenting in total136 patients showed improvement of headachein 83%, decrease of papilledema in 97%, andimprovement of visual acuity in 78% of patientswith a rate of complications of 2.9%, which issimilar to optic nerve sheath fenestration andmuch lower compared to neurosurgical shunting(Satti 2015). Further research including a random-ized head-to-head trial is necessary to determinethe best surgical procedure to offer patients withfulminant or drug refractory IIH.
Clinical Scenario
Patient History
A 26-year-old obese female patient with chronicheadache was admitted to the emergency unit withexacerbation of headache for 2 days and increas-ingly blurred vision for 1 day. Her neurologicalstatus was normal. Fundoscopy showed unilateralpapilledema in the right eye. Emergency CT scanof the head was normal. The patient was admittedto the hospital and had a brain MRI performed onthe next day (Fig. 9). Lumbar puncture wasplanned in order to measure CSF opening pres-sure. Due to the patient’s obesity, there were tech-nical problems with this procedure on the ward(the ward neurologist could not find the midlineon palpation). The clinical neurologist thereforeasked a neuroradiologist to perform an X-ray-guided lumbar puncture (Fig. 9). This was suc-cessfully performed at the L2/3 level with X-rayscreening in both lateral and PA directions. Theopening CSF pressure was 400 mmH2O and CSFcomposition was normal. 20 ml of CSF was col-lected, and the closing pressure was reduced to230 mmH2O. She reported immediate improve-ment in her headache and blurred vision.
Clinical Diagnosis
Intracranial hypertension of the unknown cause.
Purpose of MR Study
To exclude secondary causes and to assess intra-cranial as well as intraorbital abnormalities due toclinically suspected intracranial hypertension.
MR Technique
Standard brain MRI protocol with contrast injec-tion (axial T1-weighted, axial, coronal and sagittalT2-weighted, axial FLAIR, and DWI and SWIimages followed by post-contrast 3DT1-weighted images) with two additional
Imaging of Idiopathic Intracranial Hypertension 11
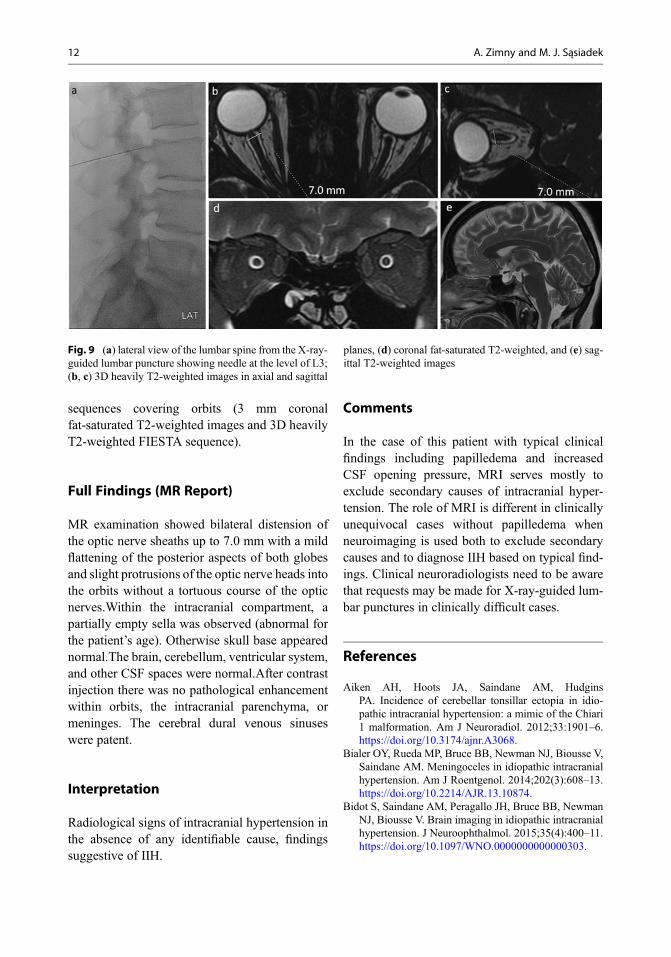
sequences covering orbits (3 mm coronalfat-saturated T2-weighted images and 3D heavilyT2-weighted FIESTA sequence).
Full Findings (MR Report)
MR examination showed bilateral distension ofthe optic nerve sheaths up to 7.0 mm with a mildflattening of the posterior aspects of both globesand slight protrusions of the optic nerve heads intothe orbits without a tortuous course of the opticnerves.Within the intracranial compartment, apartially empty sella was observed (abnormal forthe patient’s age). Otherwise skull base appearednormal.The brain, cerebellum, ventricular system,and other CSF spaces were normal.After contrastinjection there was no pathological enhancementwithin orbits, the intracranial parenchyma, ormeninges. The cerebral dural venous sinuseswere patent.
Interpretation
Radiological signs of intracranial hypertension inthe absence of any identifiable cause, findingssuggestive of IIH.
Comments
In the case of this patient with typical clinicalfindings including papilledema and increasedCSF opening pressure, MRI serves mostly toexclude secondary causes of intracranial hyper-tension. The role of MRI is different in clinicallyunequivocal cases without papilledema whenneuroimaging is used both to exclude secondarycauses and to diagnose IIH based on typical find-ings. Clinical neuroradiologists need to be awarethat requests may be made for X-ray-guided lum-bar punctures in clinically difficult cases.
References
Aiken AH, Hoots JA, Saindane AM, HudginsPA. Incidence of cerebellar tonsillar ectopia in idio-pathic intracranial hypertension: a mimic of the Chiari1 malformation. Am J Neuroradiol. 2012;33:1901–6.https://doi.org/10.3174/ajnr.A3068.
Bialer OY, Rueda MP, Bruce BB, Newman NJ, Biousse V,Saindane AM. Meningoceles in idiopathic intracranialhypertension. Am J Roentgenol. 2014;202(3):608–13.https://doi.org/10.2214/AJR.13.10874.
Bidot S, Saindane AM, Peragallo JH, Bruce BB, NewmanNJ, Biousse V. Brain imaging in idiopathic intracranialhypertension. J Neuroophthalmol. 2015;35(4):400–11.https://doi.org/10.1097/WNO.0000000000000303.
Fig. 9 (a) lateral view of the lumbar spine from the X-ray-guided lumbar puncture showing needle at the level of L3;(b, c) 3D heavily T2-weighted images in axial and sagittal
planes, (d) coronal fat-saturated T2-weighted, and (e) sag-ittal T2-weighted images
12 A. Zimny and M. J. Sąsiadek

Chen J, Wall M. Epidemiology and risk factors for idio-pathic intracranial hypertension. Int Ophthalmol Clin.2014;54(1):1–11. https://doi.org/10.1097/IIO.0b013e3182aabf11.
Degnan AJ, Levy LM. Pseudotumor cerebri: brief reviewof clinical syndrome and imaging findings. Am JNeuroradiol. 2011;D32:1986–93. https://doi.org/10.3174/ajnr.A2404.
Friedman DI, Liu GT, Digre KB. Revised diagnosticcriteria for the pseudotumor cerebri syndrome in adultsand children. Neurology. 2013;81:1159–65.
Satti SR. Meta-analysis of CSF diversion procedure anddural venous sinus stenting in the setting of medicallyrefractory IIH. Am J Neuroradiol. 2015;36:1899–904.
Suzuki H, Takanashi J, Kobayashi K, Nagasawa K,Tashima K, Kohno Y. MR imaging of idiopathic intra-cranial hypertension. Am J Neuroradiol.2001;22:196–9.
Walker RW. Idiopathic intracranial hypertension: any lighton the mechanism of the pressure? J Neurol NeurosurgPsychiatry. 2001;71:1–7.
Suggested Readings
Chaudhry S, Bryant T, Peeler CE. Venous sinus stenting inidiopathic intracranial hypertension: a safer surgicalapproach? Curr Opin Ophthalmol. 2016;27:481–5.https://doi.org/10.1097/ICU.0000000000000315.
Hingwala DR, Kesavadas C, Thomas B, KapilamoorthyTR, Sarma PS. Imaging signs in idiopathic intracranialhypertension: are these signs seen in secondary intra-cranial hypertension too? Ann Indian Acad Neurol.2013;16(2):229–33. https://doi.org/10.4103/0972-2327.112476.
Holbrook J, Saindane AM. Imaging of intracranial pres-sure disorders. Neurosurgery. 2017;80:341–54. https://doi.org/10.1227/NEU.0000000000001362.
Imaging of Idiopathic Intracranial Hypertension 13