image-guided surgery in resection of benign cervicothoracic spinal tumors: a report of two cases
TRANSCRIPT
The Spine Journal 5 (2005) 109–114
Image-guided surgery in resection of benign cervicothoracic spinaltumors: a report of two cases
Timothy Moore, MDa, Robert F. McLain, MDb,*aDepartment of Orthopaedic Surgery, The Cleveland Clinic Foundation, 9500 Euclid Avenue, Desk A 41, Cleveland, OH 44195, USA
bSurgical Staff, Department of Orthopaedic Surgery and The Cleveland Clinic Spine Institute, The Cleveland Clinic Foundation,9500 Euclid Avenue, Desk A 41, Cleveland, OH 44195, USA
Received 12 November 2003; accepted 24 June 2004
Abstract BACKGROUND CONTEXT: Osseous spinal tumors are an uncommon cause of persistent axialpain and muscle spasm, but even benign lesions may grow to cause deformity or neurological signs.Traditional treatment approaches to resection can be debilitating even when the tumor is benign.PURPOSE: Emerging technologies allow surgeons to diagnose and treat osseous neoplasms whileminimizing the collateral damage caused by surgical exposure and tumor excision.STUDY DESIGN: Technical considerations are presented through two cases of benign osseousneoplasm occurring in the cervicothoracic spine of competitive athletes, demonstrating the meth-ods used to provide effective treatment while maintaining maximal functional capacity.METHODS: Stereotactic imaging and intraoperative guidance was used as an adjunct to tumorcare in these patients. Used in combination with minimally invasive, microsurgical techniques,stereotactic guidance localized and verified excision margins of benign vertebral lesions, minimizingsoft tissue trauma and collateral damage.RESULTS: Computer-assisted stereotactic localization allowed us to successfully ablate theselesions from their anatomically challenging locations, without disrupting the shoulder girdle or neckmusculature, and without extensive bony resection.CONCLUSIONS: Image guidance can accurately localize and guide excision of benign vertebrallesions while minimizing soft tissue trauma and collateral damage, allowing patients a rapid andcomplete return to high-demand function. � 2005 Elsevier Inc. All rights reserved.
Keywords: Spine; Tumor; Stereotactic guidance; Sports; Osteoblastoma; Osteoid osteoma
Introduction
Although focal, persistent pain might be treated expec-tantly in a normally active teen or young adult, seriousspinal pathology can occasionally be overlooked. Osseousspinal tumors are an uncommon cause of neck and backpain, but they do occur in young, healthy individuals [1].When a spinal column tumor is identified, the primary goalis to determine its nature, benign or malignant, and thesecond is to provide effective treatment to control or curethe lesion. If the lesion is benign, treatment should be carried
FDA device/drug status: not applicable.Nothing of value received from a commercial entity related to this
research.* Corresponding author. Robert F. McLain, MD, Orthopaedic Spine
Research, The Department of Orthopaedic Surgery, The Cleveland ClinicFoundation, 9500 Euclid Avenue, Desk A 41, Cleveland, OH 44195, USA.Tel.: (216) 444-2744; fax: (216) 444-3328.
E-mail address: [email protected] (R.F. McLain)
1529-9430/05/$ – see front matter � 2005 Elsevier Inc. All rights reserved.doi:10.1016/j.spinee.2004.06.020
out without unnecessarily disrupting subsequent function.Traditional surgical approaches can be damaging to sur-rounding tissues, resulting in long-term impairment thatwould preclude return to high-demand activities. In athleteswho throw, disruption of the shoulder girdle and cervicothor-acic junction can be career ending.
When operative treatment is necessitated by persistentpain and/or neurological symptoms, traditional surgical ap-proaches reliably control these tumors, but at a significantcost in muscular injury and functional impairment [2–4].Benign, locally invasive lesions may require extensive dis-section for definitive control.
Beyond reliably extirpating the lesion, the surgeonshould consider the effect the surgical approach will haveon function. While advances have been made in minimallyinvasive treatment of some tumors, percutaneous techniquescannot be safely applied immediately adjacent to the spinalcord [5,6]. Open techniques are still necessary in thesecircumstances.

T. Moore and R.F. McLain / The Spine Journal 5 (2005) 109–114110
Stereotactic image guidance (SG), combined with micro-surgical techniques, allows surgeons to use a minimallyinvasive approach to accurately localize and excise thesebenign tumors, minimizing surgical morbidity and optimiz-ing rapid return to unrestricted function. Application of theseprinciples is illustrated by two cases of competitive athletespresenting with benign neoplasms of the cervicothoracicjunction.
Case reports
Case 1
A 16-year-old soccer player presented with left-sided neckand shoulder pain of 5 month’s duration, first noticed whileplaying soccer. The pain began insidiously but was sharplyexacerbated when heading the ball. Initial X-rays showedno shoulder or neck abnormality, but bone scan revealed focaluptake at the C7 level.
Initially relieved with aspirin, the pain became less re-sponsive over time. It was often present at night and onwaking in the morning, without inciting events. The pain lo-calized to the low cervical region just left of the midline,with radiation to the left shoulder, but it did not radiate distallyinto the arm. There were no right-sided symptoms.
Despite full range of motion, the patient experienced painwith extremes of flexion, extension and rotation, and whiletilting his head to the right. He had no atrophy, but had mildweakness in his left-hand intrinsics. Deep tendon reflexeswere equal bilaterally in the upper extremities, and his lowerextremity examination was normal.
A computed tomography (CT) scan revealed a lesion inthe left pedicle of C7, suggestive of osteoid osteoma (Fig. 1,top). Based on his progressive symptoms and the failureof conservative measures to maintain adequate function,surgical excision was indicated. A fine-cut CT was obtainedand downloaded into the stereotactic workstation.
Through a 2.5-cm dorsal incision, a microsurgical ap-proach was made to the C7 lamina. The SG system wasregistered to the C7 vertebra, using the spinous process andthe adjacent facet margins for triangulation. The SG wand wasthen used to select the proper entry point, through the laminarsurface, based on the position and depth of the intraosseouslesion (Fig. 1, middle). A 1.2-cm window was made through
�Fig. 1. (Top) Axial computed tomography image demonstrating well-cir-cumscribed lytic lesion in cervical pedicle, with erosion of medial cortexinto the neural canal. (Middle) Intraoperative stereotactic image after regis-tration, showing probe tip over cortical entry point providing optimalaccess to osteoid osteoma. (Bottom) Intraoperative stereotactic image dem-onstrating probe tip at base of void created during excision of tumor nidus.Stereotactic image guidance permitted complete ablation of tumor withoutrisk of entry into the canal.
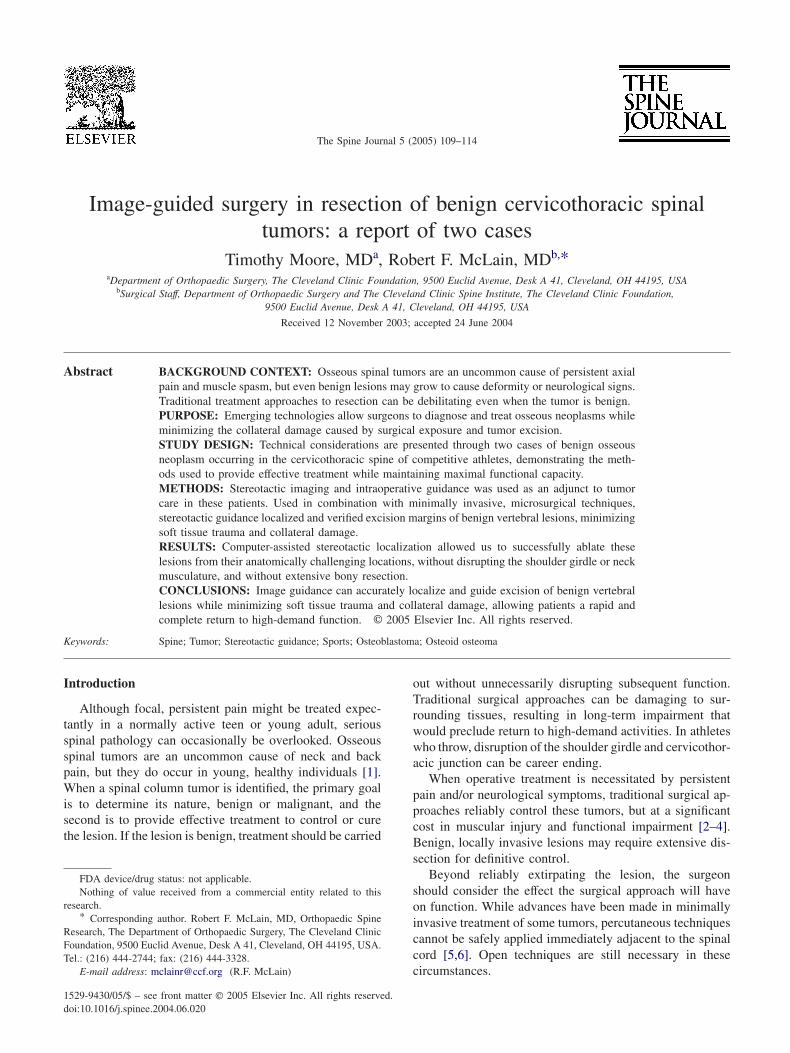
the laminar cortex with the bur, and a vertical shaft wasdeveloped down to the tumor nidus. The lesion was removedwith a microcurette, and the SG system confirmed theresection margins (Fig. 1, bottom). The nidus of the osteoidosteoma was confirmed histologically.
Recovery was uneventful, and the patient was dischargedon the first postoperative day. Symptoms resolved, and at6 weeks he had only mild incisional pain. At 4 monthshe was fully active. X-rays of the cervicothoracic junctionshowed normal alignment. After reconditioning and physicaltherapy, he was released to return to athletic competition.Follow-up 26 months after excision revealed no clinicalevidence of disease and no neck symptoms. Radiographswere unremarkable.
Case 2
A 22-year-old right-hand-dominant professional baseballpitcher presented for treatment of an upper thoracic spinetumor. He first experienced pain in his left shoulder 6 monthsbefore evaluation, but the pain had worsened over the last2 months. He had night pain, which was not relieved byanti-inflammatory medications. He felt weak in grip strengthbilaterally, but denied bowel and bladder dysfunction, numb-ness or tingling.
He had pain in his upper back and shoulder with neckrange of motion. Rotation and lateral bending were normalwith pain at the extremes. Upper extremity strength wasintact except that bilateral wrist flexion and extension were5-/5. Deep tendon reflexes were bilaterally symmetrical.Neurologic examination of the lower extremities was normal,and there were no pathologic reflexes.
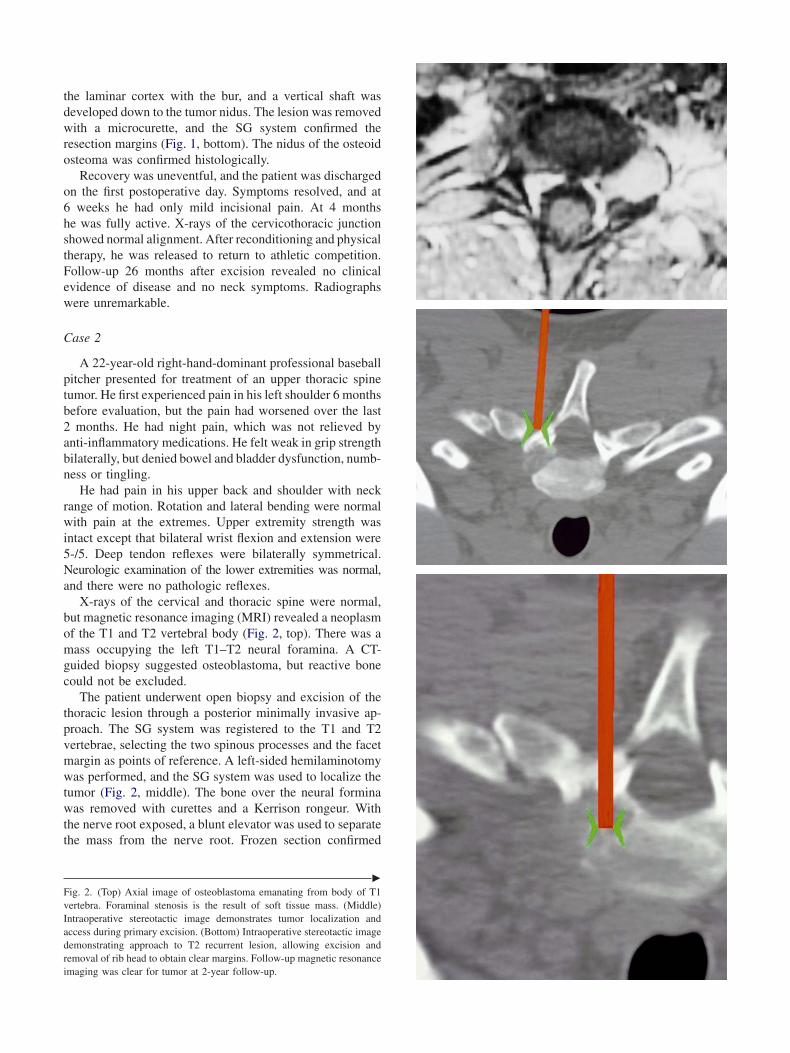
X-rays of the cervical and thoracic spine were normal,but magnetic resonance imaging (MRI) revealed a neoplasmof the T1 and T2 vertebral body (Fig. 2, top). There was amass occupying the left T1–T2 neural foramina. A CT-guided biopsy suggested osteoblastoma, but reactive bonecould not be excluded.
The patient underwent open biopsy and excision of thethoracic lesion through a posterior minimally invasive ap-proach. The SG system was registered to the T1 and T2vertebrae, selecting the two spinous processes and the facetmargin as points of reference. A left-sided hemilaminotomywas performed, and the SG system was used to localize thetumor (Fig. 2, middle). The bone over the neural forminawas removed with curettes and a Kerrison rongeur. Withthe nerve root exposed, a blunt elevator was used to separatethe mass from the nerve root. Frozen section confirmed
�
Fig. 2. (Top) Axial image of osteoblastoma emanating from body of T1vertebra. Foraminal stenosis is the result of soft tissue mass. (Middle)Intraoperative stereotactic image demonstrates tumor localization andaccess during primary excision. (Bottom) Intraoperative stereotactic imagedemonstrating approach to T2 recurrent lesion, allowing excision andremoval of rib head to obtain clear margins. Follow-up magnetic resonanceimaging was clear for tumor at 2-year follow-up.

T. Moore and R.F. McLain / The Spine Journal 5 (2005) 109–114112
the diagnosis of osteoblastoma. The remaining tumor wasremoved with curettes and a nerve hook. The resection mar-gin was verified with the stereotactic wand and confirmedhistopathologically.
The patient went home on the first postoperative day.Six weeks after surgery he began a graded rehabilitationprogram. At 6 months he was throwing full speed and wasready to return to competition.
Follow-up MRI at 9 months revealed a focal recurrenceof the neoplasm at the adjacent vertebra (Fig. 2, bottom).Because of the lesion’s proximity to the spinal cord, adjuvanttherapy was not a consideration, and a repeat excision wasnecessary. The microsurgical approach was repeated, andSG was used to carry out a more extensive bony excision atthe T2 level, without extending the soft tissue dissection.The patient’s recovery was again rapid, and he returned toprogressive rehabilitation without further difficulties. At 6months after surgery, he was released to return to competi-tion. MRI showed the patient to be free of recurrence at 2-year follow-up, at which point he had returned to competitionat the Major-League level.
Surgical technique
The best approach to surgical excision of any spinalcolumn tumor is dictated by the tumor type, level, locationwithin the vertebra and size [7]. When benign neoplasmsare encountered within the spinal column, an attempt canbe made to eradicate the lesion without disrupting the sur-rounding uninvolved tissues, but locating the tumor anddetermining its margins often requires a more extensivedissection and exposure [8]. The surgical exposure disruptsmuscle, ligamentous tissues and bony elements importantto stability. The soft tissue dissection can severely impairfunctional recovery, even assuming tumor removal is com-pletely successful. For athletes involved in throwing activi-ties or “heading,” disruption of the cervicothoracic junction,shoulder girdle musculature or chest wall can be career ending.
Minimally invasive techniques have significantly im-proved recovery and return to activity among spine surgerypatients but have had limited application in cases of spinalcolumn tumor. SG has proven helpful in localizing intracran-ial lesions that traditionally required more extensive surgicalexposure. SG uses a number of different image correlationtechnologies to provide localizing feedback to the surgeonbased on recognizable surface or cortical landmarks. Three-dimensional data are provided once the actual anatomy isregistered and are correlated to previously acquired CT data.In the spine, SG has proven reliable in guiding placementof transpedicular and cervical transarticular screws [9].
In tumor care, SG allows the surgeon to localize subcorti-cal pathology without wide operative exposure, then excise itand confirm proper margins, all through the smallest incisionpossible. Preoperative CT data, acquired by spiral CT in fine-cut sections, are downloaded into the image analysis works-tation (Viewpoint Stereotactic Navigation System; Z-Kat
Systems, Cleveland, OH) and converted to a three-dimen-sional display that can be manipulated in real time in theoperating room. In the system used here, a light-emittingdiode (LED) sensor array is tracked by a binocular sens-ing system positioned at the foot of the surgical station.Specific instruments are designed and calibrated within thesystem to provide precise localization of the instrument tipin space, based on the LED alignment.
Surgical treatment requires exposure of just enough bonyarchitecture to allow the surgeon to identify three distinctnonlinear points on the bony surface. These registry pointsmust be prominent enough to show on the CT image andat the surgical site. In unilateral spinal exposures these maybe the spinous process, the transverse processes, the apexof a facet or any distinct osteophyte or prominence. Afterregistering the selected points with the LED wand, the SGsystem reconciles the area described by the three points tothe anticipated area described by the target points andprovides an estimate of error. If an acceptable error is calcu-lated, the system can correlate the position and orientation ofthe wand tip with respect to the vertebral elements (Fig. 3).Using the system as described, accuracy has been shown torange from 1.1�0.8 mm in early pedicle screw studies [9]to the submillimeter range in more recent studies with currentimage guidance tools [10]. Using this system, no outriggerassembly is needed, because the existing anatomy providesan absolute reference. The surgical excision can then becarried out without dissecting normal, uninvolved anatomyto acquire visualization, locate landmarks or apply an outrig-ger. The neoplastic lesion can be approached directly throughthe least destructive corridor and excised to the marginswithout disrupting the adjacent facets or surrounding bonyarchitecture.
Discussion
Even though the tumor may be benign, surgery is indi-cated in many cases of spinal column tumor, either by pain
Fig. 3. Registry points selected for three-dimensional correlation to storedcomputed tomography (CT) data. Three nonlinear points are selectedand correlated with well-defined CT landmarks. Accuracy of correlationis calculated by the software based on spatial resolution of the known CTlandmarks and those selected in real time.

T. Moore and R.F. McLain / The Spine Journal 5 (2005) 109–114 113
or progressive instability or threat of local extension. Thereis a risk of surgery causing more long-term dysfunction than itprevents, however. The need to minimize the morbidity ofsurgery, while maintaining effectiveness, is something thesurgeon should consider.
Osteoid osteoma and osteoblastoma are primary bonetumors with a benign nature [11–19]. Osteoid osteomas ac-count for about 10% to 11% of all primary bone tumors.Between 10% and 20% of osteoid osteomas occur in theposterior elements of the spine. Osteoblastomas are uncom-mon tumors accounting for only 1% of tumors, but theyhave an affinity for the spine [11]. About 40% occur inthe vertebral column [11,14]. Large lesions can produceinstability or encroach on nervous tissue [15].
Surgical treatment of spinal osteoid osteomas is compli-cated by the inaccessibility of the lesion. Even with a stan-dard open surgical approach, care must be taken to accuratelylocalize the nidus of the lesion [20]. There have beenmany techniques described to aid in localizing the tumornidus [21–23]. The goal is to remove the nidus entirelywithout causing pathologic fracture or instability. The classicsurgical procedure involves saucerizing a wide section ofthe overlying cortex to expose the lesion at the base.
Less invasive techniques have been developed to treatosteoid osteoma in the extremities. Percutaneous ablation,removing the nidus by drilling percutaneously through thebone to the lesion [24], has been used to treat osteoid osteo-mas within the lumbar vertebral body, but not in proximityto the spinal cord [25]. Radiofrequency ablation has alsobeen used to percutaneously ablate extremity and lumbarosteoid osteomas. Thin optical fibers emitting low-powerlaser light energy, introduced percutaneously, destroy tumorby direct heating [6,26]. The technique has been usedsparingly in treating lumbar osteoid osteomas, but never indirect proximity to the spinal canal [5,27,28].
Vertebral osteoblastomas are best treated with direct exci-sion or aggressive curettage [29]. Percutaneous treatmentmodalities have no role in treating these tumors. The largersize of the tumor usually dictates a more extensive dissectionand greater tissue disruption, and an intralesional margin isoften the best that can be obtained. Tumor recurrence has beencommon, therefore, unless adjuvant therapy such as cryo-therapy or phenol is added after surgery. These adjuvantscannot be used around the spinal cord, so an extensive de-bridement is often substituted to limit the likelihood of recur-rence. In cervical and cervicothoracic lesions, extensiveresection can be debilitating.
The minimally invasive, image-guided approach de-scribed here removes less bone and requires less softtissue dissection than the classic open techniques, yet stillallowed a full resection of the tumor in our cases [8,29].The use of computer-assisted stereotactic localization refinedintraoperative localization of the tissue to be excised. Thistechnique allowed successful ablation of benign, painfullesions in an anatomically challenging location, without dis-rupting the shoulder girdle or neck musculature, and without
extensive bony resection. To our knowledge, this approachhas been reported in only one case of spine tumor [30].
The traditional en-bloc excision of a cervicothoracic tumorrequires a more extensive dissection and exposure of addi-tional vertebral levels, often requiring laminectomies andsubsequent instrumentation. The more extensive soft tissueinjury and potential for instability can greatly affect the returnto function, particularly in high-demand activities and ath-letic participation. The use of the stereotactic imaging systemallowed us to localize the tumor margins with great accuracy.Used more commonly for guidance during pedicle screwand atlantoaxial screw placement [9], this system allowedfor safe and complete excision in immediate proximity ofvital neurovascular structures. In both of these cases, contra-lateral spinal musculature was undisturbed. Localization wasaccomplished by exposing the lamina and spinous process ofonly a single motion segment. The end result was directaccess and complete surgical excision of the lesion withsoft tissue injury comparable to a trochar biopsy. Localrecurrence of the osteoblastoma occurred after our initialexcision (a 10% risk following traditional approaches),but even here, wider resection of the recurrent lesion wasstill accomplished through a minimally invasive approach.Although any patient should warrant the benefits of function-preserving treatment offered by this approach, the extraordi-nary physical demands upon the throwing athlete illustrate thepotential for excellent functional outcome after image-guidedresection of a spinal tumor.
Summary
Although osseous spinal tumors are uncommon, they dooccur in young, active individuals and can present in thecompetitive athlete. Once the benign nature of the osseousneoplasm has been established, one of the primary difficult-ies in treating an athlete with a spinal tumor is minimizingthe collateral damage caused by the surgical exposure andtumor excision. Stereotactic imaging can be a usefuladjunct to tumor care in properly selected patients. Imageguidance, in combination with evolving minimally inva-sive surgical techniques, can accurately localize and guideexcision of benign vertebral lesions while minimizing softtissue trauma and collateral damage, allowing patients arapid and complete return to preoperative function. It mustbe noted, however, that experience with this approach islimited and that the results obtained in these patients maynot be typical. It should also be noted that the intralesionalapproach used in these cases would not be appropriate forprimary malignant lesions arising from the spinal column.
References
[1] Weinstein JN, McLain RF. Primary tumors of the spine. Spine 1988;12(9):843–51.

T. Moore and R.F. McLain / The Spine Journal 5 (2005) 109–114114
[2] Fielding JW, Keim HA, Hawkins RJ, et al. Osteoid osteoma of thecervical spine. Clin Orthop Rel Res 1977;128:163–4.
[3] Kirwan EO, Hutton PA, Pozo JL, et al. Osteoid osteoma and benignosteoblastoma of the spine. Clinical presentation and treatment. JBone Joint Surg 1984;66B(1):21–6.
[4] Pettine KA, Klassen RA. Osteoid-osteoma and osteoblastoma of thespine. J Bone Joint Surg 1986;68B(3):354–61.
[5] Osti OL, Sebben R. High-frequency radio-wave ablation of osteoidosteoma in the lumbar spine. Eur Spine J 1998;7(5):422–5.
[6] Rosenthal DI, Hornicek FJ, Wolfe MW, et al. Percutaneous radiofre-quency coagulation of osteoid osteoma compared with operative treat-ment. J Bone Joint Surg 1998;80A(6):815–21.
[7] McLain RF, Weinstein JN. Tumors of the spine. In: Herkowitz H,Garfin S, Balderston R, Eismont F, Bell G, Weisel S, editors. Rothmanand Simeone: the spine, 4th ed. Philadelphia: W.B. Saunders Com-pany, 1999:1171–206.
[8] Ward WG, Echardt JJ, Shatestehfar S, et al. Osteoid osteoma diagnosisand management with low morbidity. Clin Orthop Rel Res 1993;291:229–35.
[9] Kalfas IH, Kormos DW, Murphy MA, et al. Application of framelessstereotaxy to pedicle screw fixation of the spine. J Neurosurg 1995;83(4):641–7.
[10] Choi WW, Green BA, Levi ADO. Computer-assisted fluoroscopictargeting system for pedicle screw insertion. Neurosurgery 2000;47:872–8.
[11] Marsh BW, Bonfiglio M, Brady LP, Enneking WF. Benign osteo-blastoma: range of manifestations. J Bone Joint Surg 1975;57A(1):1–9.
[12] Ciabattoni G, Tamburrelli F, Greco F. Increased prostacyclin biosyn-thesis in patients with osteoid osteoma. Eicosanoids 1991;4(3):165–7.
[13] Bottner F, Roedl R, Wortler K, et al. Cyclooxygenase-2 inhibitor forpain management in osteoid osteomas. Clin Orthop Rel Res 2001;393:258–63.
[14] Griffin JB. Benign osteoblastoma of the thoracic spine. J Bone JointSurg 1978;60A(6):833–5.
[15] Schneider M, Sabo D, Gerner HJ, et al. Destructive osteoblastomaof the cervical spine with complete neurologic recovery. Spinal Cord2002;40(5):248–52.
[16] Bucci MN, Feldenzer JA, Phillips WA, et al. Atlanto-axial rotationallimitation secondary to osteoid osteoma of the axis. J Neurosurg 1989;70(1):129–31.
[17] Goldstein GS, Dawson EG, Batzdorf U. Cervical osteoid osteoma:a cause of chronic upper back pain. Clin Orthop Rel Res 1977;129:177–80.
[18] Hershman E, Bjorkengren AJ, Fielding JW, et al. Osteoid osteomain a cervical pedicle. Resection via transpillar approach. Clin OrthopRel Res 1986;213:115–7.
[19] Jones DA. Osteoid osteoma of the atlas. J Bone Joint Surg 1987;69B(1):149.
[20] Sim FH, Dahlin CD, Beabout JW. Osteoid-osteoma: diagnostic prob-lems. J Bone Joint Surg 1975;57(20):154–9.
[21] Ayala AG, Murray JA, Erling MA, et al. Osteoid-osteoma: intraopera-tive tetracycline-fluorescence demonstration of the nidus. J BoneJoint Surg 1986;68A(5):747–51.
[22] Ghelman B, Thompson FM, Arnold WD. Intraoperative radioactivelocalization of an osteoid-osteoma. J Bone Joint Surg 1981;63A(5):826–7.
[23] Szypryt EP, Hardy JG, Colton CL. An improved technique of intra-operative bone scanning. J Bone Joint Surg 1986;68B(4):643–6.
[24] Donahue F, Ahmad A, Mnaymneh W, et al. Osteoid osteoma. Com-puted tomography guided percutaneous excision. Clin Orthop RelRes 1999;366:191–6.
[25] Labbe JL, Clement JL, Duparc B, et al. Percutaneous extraction ofvertebral osteoid osteoma under computed tomography guidance.Eur Spine J 1995;4(6):368–71.
[26] Dupuy DE, Hong R, Oliver B, et al. Radiofrequency ablation of spinaltumors: temperature distribution in the spinal canal. Am J Roentgenol2000;175(5):1263–6.
[27] Lindner NJ, Ozaki T, Roedl R, et al. Percutaneous radiofrequencyablation in osteoid osteoma. J Bone Joint Surg 2001;83B(3):391–6.
[28] Woertler K, Vestring T, Boettner F, et al. Osteoid osteoma: CT-guidedradiofrequency ablation and follow-up in 47 patients. J Vascular In-tervent Radiol 2001;12(6):717–22.
[29] Levine AM, Boriani S, Donati D, et al. Benign tumors of the cervicalspine. Spine 1992;17:S399–406.
[30] Patel N, Sandeman DR, Cobby M, et al. Interactive image-guidedsurgery of the spine. J Neurosurg 1997;11(1):60–4.