il trattamento dei daa nei consumatori di sostanze
TRANSCRIPT

Danilo TacconiMalattie Infettive – Asl Toscana Sud Est
Il trattamento dei DAA nei consumatori di sostanze: efficacia e sicurezza


Previsto un incremento degli stadi avanzati della malattia epatica e di HCC nella popolazione dei SERD

Difficoltà al trattamento nel passato
• Complessità gestione
• Scarsa adesione ai trattamenti
• Presenza di eventi avversi correlati alla terapia
• Rischio di reinfezione
Rivedere il paradigma

Responsabilità /barriere
• Serd
• Minore consapevolezza e importanza screening (T0 e successivi)
• Incremento carichi di lavoro per aumento popolazione con dipendenze
• Maggiore orientamento verso parte psichiatrica-sociale
• Percepita mancanza di valore nel trattamento di alcuni pazienti

Responsabilità /barriere
• Epatologi (Infettivologi, Gastroenterologi, Internisti)
• Fino a poco tempo fa considerati una popolazione scomoda per essere trattata
• Incremento carichi di lavoro per tutti gli altri pazienti HCV+ e le varie emergenze
• Percepita mancanza di valore nel trattamento di alcuni pazienti
• Preoccupazioni per l'adesione

Responsabilità/barriere
• Pazienti
• Comorbidità
• Altre priorità
• Difficoltà abitative e di trasporto
• Conoscenza limitata di HCV e sue conseguenze
• Diffidenza per esperienze negative in ambito sanitario

VIEKIRAX - EXVIERA
HARVONI
SOVALDI
MAVIRET
HEPCLUSA
ZEPATIER
VOSEVIOLYSIO
DAKLINZA

Manns, von Hahn, Nat Rev Drug Discov 2013
Direct Acting Antiviral Againts HCV

Great Tools Available
3’UTR5’UTR Core E1 E2 NS2 NS3 NS5A NS5BP7
Ribavirin
(RBV)
Polymerase
Daclatasvir (DCV)
Elbasvir (EBR)
Ledipasvir (LDV)
Ombitasvir (OBV)
Velpatasvir (VEL)
Pibrentasvir (PIB)
Sofosbuvir
(SOF)
Dasabuvir
(DSV)
NS5B
NUC
Inhibitors
(-buvir)
NS5A
Replication
Complex
Inhibitors
(-asvir)
NS5B
Non-NUC
Inhibitors
(-buvir)
Grazoprevir (GZR)
Paritaprevir/Ritonavir
(PTV/RTV)
Simeprevir (SMV)
Voxilaprevir (VOX)
Glecaprevir (GLE)
NS3
Protease
Inhibitors
(-previr)
Protease
Structural Domain
4A NS4B
Nonstructural Domain
NS5A


• Secondo gli ultimi dati dell’AIFA (Agenzia Italiana del Farmaco), aggiornati al 7 ottobre 2019, sono 193.815 i trattamenti finora avviati nei soli pazienti eleggibili, con almeno una scheda di dispensazione farmaco.
• Si tratta di numeri importanti, ma non ancora sufficienti: risultano infatti ancora da trattare fra 60.000 e i 120.000 pazienti.
• Si stima, inoltre, che siano ancora oltre 200.000 le persone con virus ignare della propria condizione.

I DAA avvicinano sempre più il momento in cui sarà possibile
eliminare HCV e le patologie correlate

Obiettivi raggiungibili con la risposta virologica sostenuta (SVR)
• Ridurre la necro-infiammazione
• Fermare la progressione della fibrosi
• Prevenire la cirrosi e le sue complicazioni
• Prevenire l’epatocarcinoma
• Ridurre le manifestazioni extra-epatiche
• Incrementare la sopravvivenza
Schinazi & Asselah. From HCV to HBV cure. Liver Int. 2017;37 S1:73-80

Il trattamento come modello di prevenzione
(Treatment as Prevention - TasP)

HCV Treatment Scale-up in High-Risk Populations Can
Prevent Onward Transmission
� Observed and modeled HCV chronic prevalence among PWID in Melbourne, Australia
Slide credit: clinicaloptions.comMartin. Hepatology. 2013;58:1598.
HC
V C
hro
nic
Pre
vale
nce
Am
on
g P
WID
(%
)
Yr
Data
No scale-up from baseline (3/1000 PWID annually)
Scale-up to 10/1000 PWID annually
Scale-up to 20/1000 PWID annually
Scale-up to 40/1000 PWID annually
Scale-up to 80/1000 PWID annually
100
80
60
40
20
02007 2012 2017 2022 20272002

Global Call for HCV Elimination
• WHO vision[1]: “Eliminate viral
hepatitis as a major global public
health threat by 2030”
• US HBV/HCV Elimination Strategy (National Academies of Sciences, Engineering, and Medicine)[2]
• “Elimination” = 90% reduction in incidence by 2030
• HCV elimination in US not feasible without engaging, treating PWID
• 30.5% of all HCV infections in North America are among people with recent IDU[3]
2030 Targets
90% Diagnosed
80% Treated
65% Reduced mortality
1. WHO. Global Health Sector Strategy on Viral Hepatitis, 2016-2021. 2. NASEM. A national strategy for the elimination of hepatitis B and C.
Washington, DC: The National Academies Press; 2017. 3. Grebely. Addiction. 2019;114:150.

The Challenge: HCV Care Cascade Among PWID
Grebely. Nat Rev Gastroenterol Hepatol. 2017;14:641. Iversen. Int J Drug Policy. 2017;47:77. Slide credit: clinicaloptions.com
100
90
80
70
60
50
40
30
20
10
0
Nu
mb
er
of
Pe
op
le (
Th
ou
san
ds)
Cured (SVR)PWID Screened
for HCV
Antibody
HCV
Antibody
Positive
Confirmatory
HCV RNA or
GT Test
HCV
Specialist
Assessment
Treated

Lo screening
• lo screening per HCV deve essere proposto a tutti i consumatori di sostanze;
• la proposta dello screening deve essere accompagnata da un counseling psicoeducazionale e motivazionale;
• la proposta dello screening deve essere associata alla distribuzione di materiale informativo sulla malattia, sui trattamenti e sulle modalita di contagio;
• lo screening se negativo deve essere riproposto periodicamente (almeno ogni 3 mesi);
• lo screening se rifiutato deve essere riproposto periodicamente abbinato ad un counseling motivazionale (almeno ogni mese);
• lo screening deve essere proposto ai consumatori attivi trattati con successo con DAA per la diagnosi precoce della reinfezione (almeno ogni 3-6 mesi).

Checklist for Choosing a Regimen:
A Few Things to Know
� Fibrosis assessment: Essential in ALL patients!
‒ Presence of cirrhosis increases urgency of therapy and may affect regimen, duration, use of ribavirin
‒ If cirrhosis:
‒ Any history or signs of decompensation
‒ Need for post-SVR follow up
� Genotype & subtype for GT 1
‒ Still necessary?
� Treatment history
‒ Regimen + duration
� Comorbidities
‒ CKD, coinfection (HIV/HBV)
‒ Drug-drug interactions
‒ Ongoing risk exposures: drug use, sex, alcohol
Slide credit: clinicaloptions.com

Can We Avoid Genotyping?
� It’s a delicate balancing act
Slide credit: clinicaloptions.com
Maximizing SVR in Individual Patient
� Genotyping may be helpful
� Helpful in cirrhosis, particularly GT3
Maximize SVR in the Population
� Simplicity is key
� Genotyping adds some: cost, delay, and
complexity
A Reasonable
CompromiseGenotype only for:
Cirrhosis
Treatment-experienced
(DAA/IFN)

Other Labs?
� Work-up for other liver diseases?
‒ Could do pretreatment or else wait for post-SVR if ALT still high
‒ Iron saturation
‒ Maybe nothing else
� HBV
‒ HBsAg is important
‒ Anti-HBc not very important (but very common!)
� HIV
‒ Important due to common risk factors and importance of diagnosis

Fibrosis Assessment: How To
� Transient elastography
‒ > 12.5 KPa = cirrhosis
� Serum tests
‒ FibroTest (0.75 = cirrhosis)
‒ APRI or FIB-4 – very attractive, can be done anywhere by any provider
‒ Very good negative predictive value – rule out cirrhosis
� What about ultrasound – needed in all patients?
‒ Insensitive for cirrhosis – only needed if cirrhotic to exclude HCC before treatment
� Biopsy rarely needed

AIFA: criterio 12
A partire dal 17/10/2019, nei Registri AIFA dei farmaci ad azione antivirale diretta di ultima generazione (DAAs) per il trattamento dell’epatite C cronica verrà introdotto un nuovo criterio di trattamento (cosiddetto “criterio 12”) che è stato così formulato: “Epatite cronica o cirrosi epatica in pazienti che non possono accedere alla biopsia epatica e/o al fibroscan per motivi socio-assistenziali”. Solo per questo criterio sarà possibile utilizzare dei punteggi clinico-laboratoristici quali l’APRI (AST to Platelet Ratio Index) o il Fib-4 (Fibrosis 4 Score) per la valutazione preliminare della compromissione epatica (cirrosi/non cirrosi).


The Long Journey to an HCV Diagnosis . . .
Anti-HCV antibody
(physician)Phlebotomy
(phlebotomist)
Receive diagnosis
(physician)
Central lab
Antibody test
1-2 wks
Phlebotomy
(phlebotomist)
Central lab
RNA test
1-2 wks
Receive diagnosis
(physician)
Visit #1 Visit #2 Visit #3 Visit #4 Visit #5
Grebely. Expert Rev Mol Diagn. 2017;17:1109. Slide credit: clinicaloptions.com
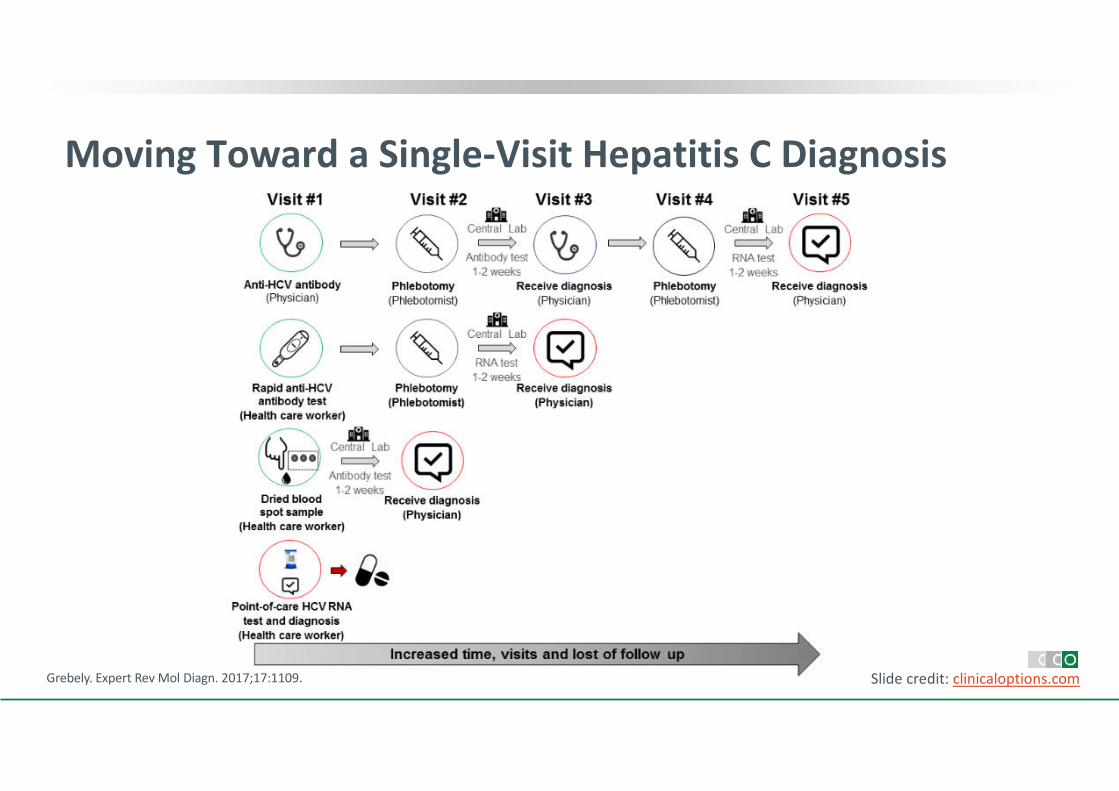
Moving Toward a Single-Visit Hepatitis C Diagnosis
Grebely. Expert Rev Mol Diagn. 2017;17:1109. Slide credit: clinicaloptions.com

Trattamento
• tutti i pazienti HCV RNA + possono essere eleggibili al trattamento;
• tutti i pazienti eleggibili al trattamento devono essere inviati allo specialista (infettivologo/epatologo);
• tutti i pazienti che vengono inviati allo specialista (infettivologo/epatologo) per il trattamento devono ricevere un programma strutturato di riduzione del danno;
• tutti i pazienti che presentano i criteri clinici per l’inizio del trattamento devono essere trattati con i DAA;
• tutti i pazienti devono ricevere un programma strutturato di riduzione del danno (con training di abilità);
• il monitoraggio del trattamento deve prevedere la valutazione dell’aderenza alla terapia e la valutazione del raggiungimento degli outcome infettivologici, tossicologici e comportamentali;
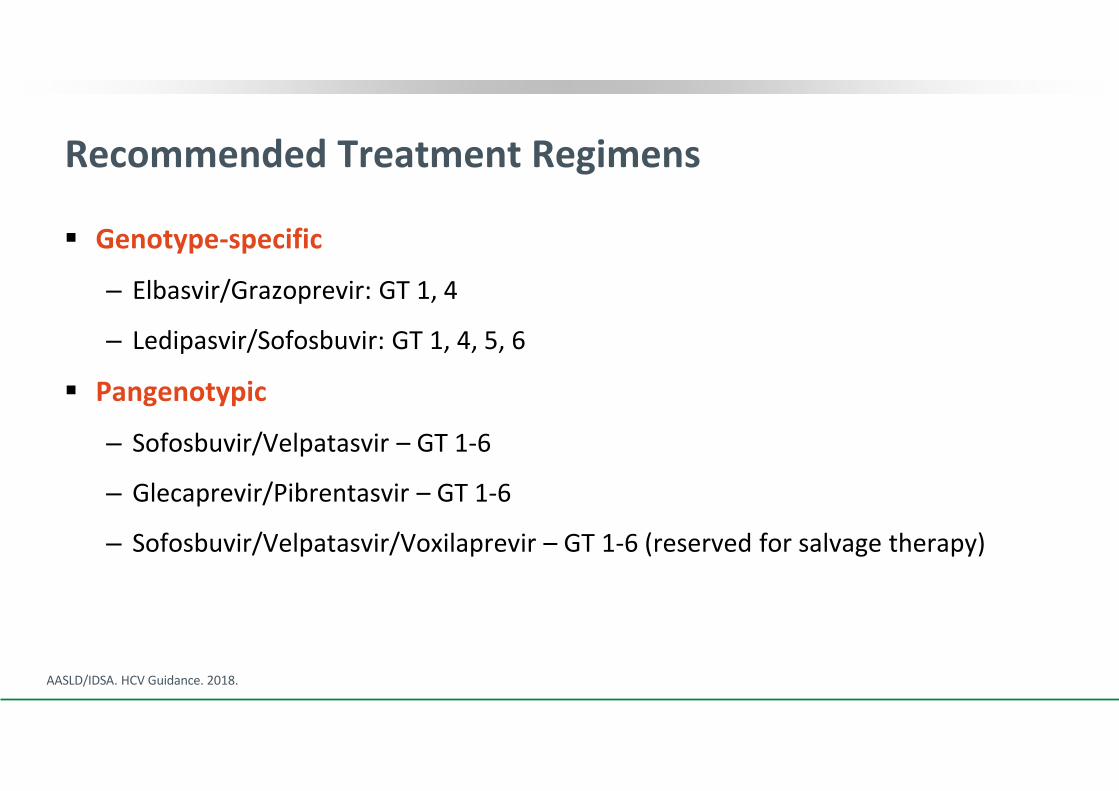
Recommended Treatment Regimens
� Genotype-specific
‒ Elbasvir/Grazoprevir: GT 1, 4
‒ Ledipasvir/Sofosbuvir: GT 1, 4, 5, 6
� Pangenotypic
‒ Sofosbuvir/Velpatasvir – GT 1-6
‒ Glecaprevir/Pibrentasvir – GT 1-6
‒ Sofosbuvir/Velpatasvir/Voxilaprevir – GT 1-6 (reserved for salvage therapy)
AASLD/IDSA. HCV Guidance. 2018.

Comparison of Pangenotypic HCV Regimens for
Treatment-Naive Patients Without Cirrhosis
Comparative Measure GLE/PIB SOF/VEL
Regimen constituents Protease inhibitor/NS5A inhibitor NS5B inhibitor/NS5A inhibitor
Dosing 3 pills QD 1 pill QD
Duration 8 wks 12 wks
Food requirement Yes No
Select DDI
considerations
Anticonvulsants, statins, St John’s
wort, warfarin
Anticonvulsants, proton pump
inhibitors, rifampin, St. John’s wort,
warfarin
Contraindications� Severe hepatic impairment (CP C)
� Concurrent ATV or rifampin use
� Do not use with RBV in patients
with RBV contraindication
Warnings/precautions � HBV reactivation risk
� HBV reactivation risk
� Bradycardia with amiodarone
coadministration
GLE/PIB [package insert]. SOF/VEL [package insert]. Slide credit: clinicaloptions.com

Treating This Patient’s HCV Infection:
SVR Rates High Among PWID, Even With Ongoing IDU
� 90.4% in C-EDGE CO-STAR (n = 136)
� 94% in SIMPLIFY (n = 102)
� 98% in pooled analysis from 6 phase III trials (mITT; n = 63)
Feld. NEJM. 2014;370:1594. Puoti. AASLD 2014. Abstr 1938. Grebely. EASL 2017. Abstr FRI-236. Grebely. CID. 2016;63:1405.
Grebely. CID. 2016;63:1479. Zeuzem. Ann Intern Med. 2015;163:1. Dore. Ann Intern Med. 2016;165:625. Foster. AASLD 2017. Abstr 1182.
0
60
80
40
20
10095-98
SV
R1
2 (
%)
91-96
No OST
(n > 7000)
OST
(n = 622)
SVR12 rates also > 90% among
patients with current/recent IDU
Slide credit: clinicaloptions.com


HCV DAA Therapy Is Effective Among PWID, Even in the
“Real-World”
� In meta-regression, clinical trials significantly associated with higher SVR rates vs observational studies
‒ aOR: 2.18 (95% CI: 1.27-3.75; P = .006)
� Difference due to loss to follow-up, not virologic failure
0
60
80
40
20
100 87.4
(82.0-92.8)
Po
ole
d S
VR
12
(%
)
90.7
(88.5-93.0)
Recent IDUOAT
Slide credit: clinicaloptions.comHajarizadeh. Lancet Gastroenterol Hepatol. 2018;3:754
Recent IDU
Bielen 2017
Boglione 2017
Boscaillou 2017
Conway 2017
Grebely 2018
Mazhnaya 2017
Milne 2017
Valencia 2017
Overall
83.3 (60.8-94.2)
93.9 (89.1-96.6)
80.4 (73.0-86.2)
96.7 (88.8-99.1)
94.2 (87.9-97.3)
64.0 (44.5-79.8)
87.4 (80.2-92.2)
74.4 (59.8-85.1)
87.4 (82.0-92.8)
Study SVR, % (95% CI)



SIMPLIFY: Adherence to 12 Wks of SOF/VEL Among
Persons With Recent (Within 6 Mos) IDU
� 97% (100/103) completed treatment; median treatment adherence: 94%
� 32% had < 90% adherence (nonadherent)
� SVR rate 94% in adherent and nonadherent group (P = .944)
Cunningham. Int J Drug Policy. 2018;62:14. Slide credit: clinicaloptions.com
Sample Daily Adherence for 4 Participants
Adherent Nonadherent
Tim
e o
f D
ay
6 AM12 PM
6 PM
6 AM12 PM
6 PM
Day Day

Drug-Drug Interactions
http://www.hep-druginteractions.org/
Don’t trust your memory – look up all drugs including OTC!
Slide credit: clinicaloptions.com

OST and HCV Therapy: Drug–Drug Interactions
https://www.hep-druginteractions.org Slide credit: clinicaloptions.com
EBR/GZR GLE/PIB LDV/SOF SOF/VEL SOF/VEL/VOX
Buprenorphine
Methadone
Naloxone
Naltrexone
Do not coadminister
Potential weak interaction
No interaction expected


DDIs Between DAAs and Hormonal Contraception
Slide credit: clinicaloptions.comhttps://www.hep-druginteractions.org
Contraceptive Drug EBR/GZR GLE/PIB LDV/SOF SOF/VEL SOF/VEL/VOX
Desogestrel
Dienogest
Drospirenone
Estradiol
Ethinylestradiol
Etonogestrel (implant)
Etonogestrel (vaginal ring)
Levonorgestrel (COC)
Levonorgestrel (implant)
Levonorgestrel (IUD)
Levonorgestrel (POP)
Medroxyprogesterone (depot injection)
Medroxyprogesterone (oral)
Norethisterone
Do not coadminister Potential weak interaction No interaction expected

HCV Reinfection Rates After SVR Among PWIDs
Slide credit: clinicaloptions.comHajarizadeh. EASL 2019. Abstr SAT-233.
• With OAT (methadone/ buprenorphine)
• Meta-analysis of 25 studies
3.81/100 PY
(95% CI: 2.51-5.80)
• With recent IDU
• Meta-analysis of 28 studies
5.86/100 PY
(95% CI: 3.96-8.66)
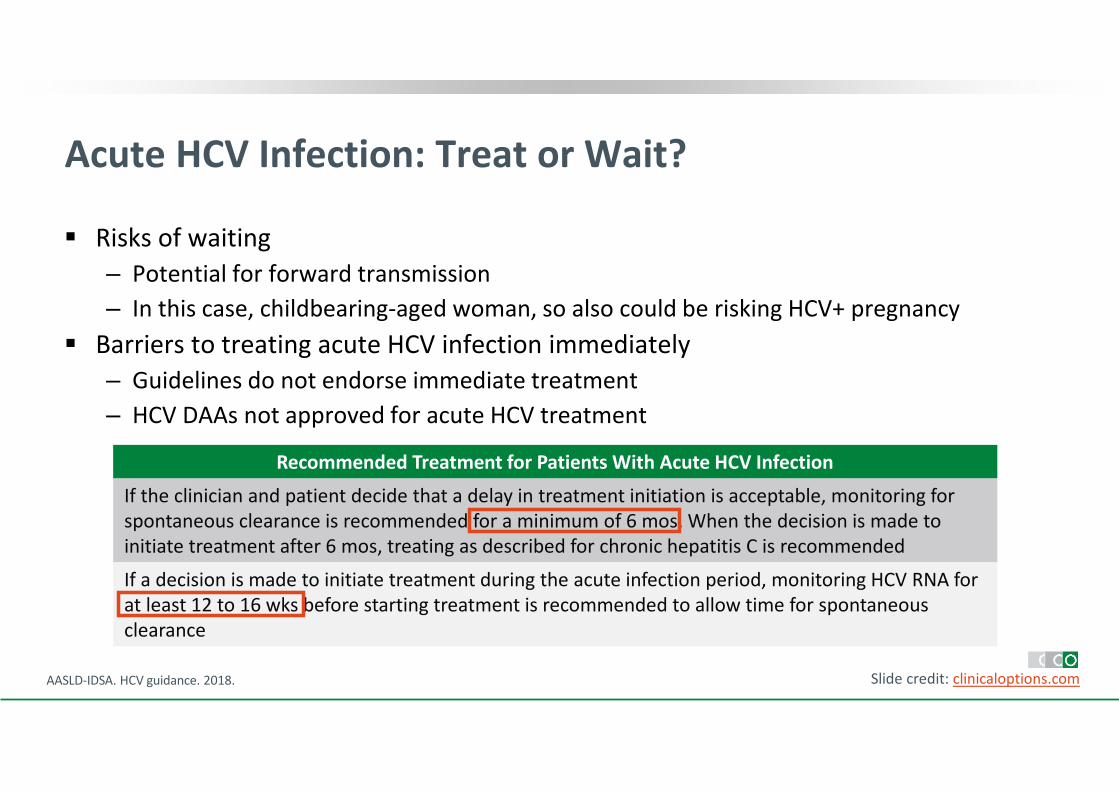
Acute HCV Infection: Treat or Wait?
� Risks of waiting
‒ Potential for forward transmission
‒ In this case, childbearing-aged woman, so also could be risking HCV+ pregnancy
� Barriers to treating acute HCV infection immediately
‒ Guidelines do not endorse immediate treatment
‒ HCV DAAs not approved for acute HCV treatment
Slide credit: clinicaloptions.comAASLD-IDSA. HCV guidance. 2018.
Recommended Treatment for Patients With Acute HCV Infection
If the clinician and patient decide that a delay in treatment initiation is acceptable, monitoring for
spontaneous clearance is recommended for a minimum of 6 mos. When the decision is made to
initiate treatment after 6 mos, treating as described for chronic hepatitis C is recommended
If a decision is made to initiate treatment during the acute infection period, monitoring HCV RNA for
at least 12 to 16 wks before starting treatment is recommended to allow time for spontaneous
clearance

Issues After Treatment
� Consequences of liver disease
‒ Only an issue with cirrhosis (fibrosis assessment pretreatment!)
‒ HCC risk
‒ Liver function – MELD purgatory
� Reinfection risk
‒ Ongoing exposures – HCV RNA testing every 6-12 mos
‒ No ongoing exposures – annual ALT, promote liver health (diet & alcohol), and nothing else!
Slide credit: clinicaloptions.com

HCV Elimination Requires More Than Good Drugs
SVR in individuals SVR in the population
Grebley. JID. 2013;207(S1):S19. Slide credit: clinicaloptions.com
Pa
tie
nts
Ach
iev
ing
SV
R (
%)
0
20
40
60
80
100
1998 2001 2012 2018P
op
ula
tio
n L
eve
l SV
R (
%)
0
20
40
60
80
100
1998 2001 2012 2018
IFN
IFN + RBV
PegIFN + RBV
PegIFN + RBV + PI
IFN-free

Potential benefits of treatment in PWIDSocietal and individual benefits
Bamvita JM, et al. Hepat Res Treat 2014;2014:631481;

DOT
Semplificazione esami pretrattamento
Incremento Centri prescrittori
(SERD)
Telemedicina
Monitoraggio durante il trattamento
Epatologo al SERD
Pacchetto DAY SERVICE
Screening universale HBV-HCV-HIV-MTS
Ritiro dei farmaci al SERD
Follow-up post-trattamento
Rischio reinfezione, stili di vita
Interventi per ridurre le barriere al trattamento
Testing Linkage to careTreatment uptake
Treatment adherence Viral suppression
Treatment uptake
Treatment adherence


HCV Elimination Requires More Than Good Drugs

