igwe, augustine asiduba - university of nigeria, nsukka augustine asiduba.pdf · cervical traction,...
TRANSCRIPT

1
BENEFITS OF USING UPRIGHT AND FLEXION TECHNIQUE
OF CERVICAL TRACTION IN THE TREATMENT OF
CERVICAL SPONDYLOSIS
BY
IGWE, AUGUSTINE ASIDUBA
PG/M.Sc/05/45015
A DISERTATION SUBMITTED TO
THE DEPARTMENT OF MEDICAL REHABILITATION
FACULTY OF HEALTH SCIENCES AND TECHNOLOGY
COLLEGE OF MEDICINE, UNIVERSITY OF NIGERIA.
ENUGU CAMPUS.
IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE AWARD OF
MASTER OF SCIENCE IN MEDICAL REHABILITATION.
…………………………………..
SUPERVISOR: PROF. G. C. OKOYE
APRIL, 2012.

2
APPROVAL PAGE
NAME: IGWE, AUGUSTINE ASIDUBA
DEGREE: MASTER OF SCIENCE (M.Sc) IN
MEDICAL REHABILITATION
TITLE OF DISSERTATION: BENEFITS OF USING UPRIGHT
AND FLEXION TECHNIQUE OF
CERVICAL TRACTION IN THE
TREATMENT OF CERVICAL
SPONDYLOSIS
EXAMINING COMMITTEE
1. HEAD OF DEPARTMENT ………………………….. MR. S. E. IGWE 2. PROJECT SUPERVISOR ………………………….. PROF. G. C. OKOYE 3. EXTERNAL EXAMINER ………………………….. PROF. P. U. NWOHA 4. INTERNAL EXAMINER …………………………..
5. APPROVAL DATE …………………………..

3
DEDICATION
I dedicate this work to all my patients as a clinical personnel
especially those that volunteered to participate in this study.

4
ACKNOWLEDGEMENTS
I wish to acknowledge the following without whose
contributions; this work would not have been completed. My
greatest thanks go to my supervisor Prof. G. C. Okoye, Dean
Faculty of Health Sciences and Technology, College of Medicine,
University of Nigeria, Enugu Campus for all his encouragement,
patience and dedication towards nurturing this project to
completion. I also express my gratitude to Mr. S. E. Igwe, Head
Department of Medical Rehabilitation, Faculty of Health
Sciences and Technology, College of Medicine University of
Nigeria, Enugu Campus, for his kindness and assistance. I also
express my gratitude to Dr. G. O. Eyichukwu, Chairman,
Research, Education and Training, National Orthopaedic
Hospital Enugu for his advice and assistance.
My thanks also go to Dr. C. U. Eze, Head, Department of
Medical Radiography and Radiological Sciences, Faculty of
Health Sciences and Technology, College of Medicine University
of Nigeria, Enugu Campus, for his help. I also appreciate the
assistance of departmental secretary and all those who
contributed in one way or the other in bringing this work to

5
conclusion. Most of all I thank the almighty God for giving me
the courage to persevere in bring the work to conclusion.

6
Abstract
In this study an attempt was made to assess the use of cervical
traction for the treatment of pain in cervical spondylosis. Thirty
(30) patients (18 male and 12 female), mean age 50. 20 ± 8.51
years, mean weight 86.31 ± 14.83 were available for this study
whereby a cross over research design was used to evaluate infra
red radiation only as a control paradigm, and cervical traction
combined with infra-red radiation as experimental paradigm.
Infra red radiation was applied three times a week for six weeks
before a wash out period of 7 days and then cervical traction
and infra red radiation were applied on the same patients to
observe their therapeutic effect for the same six weeks at three
times per week.
The pain score using Numeric rating scale was evaluated before
the treatment, after two weeks, four weeks and then after the
sixth week. The patients were treated three times per week each
for 6 weeks. The result showed that both infra red radiation
alone and cervical traction combined with infra red radiation
showed relief of pain but infra red combined with cervical
traction was superior to infra red radiation alone in the
treatment of pain in cervical spondylosis (p < 0.05).

7
TABLE OF CONTENTS Title Page Title Page………………………………………………………………………….i Approval Page……………………………………………………………..ii Dedication…………………………………………………………………iii Acknowledgements………………………………………………………iv Abstract………………………………………………..…………………..v Table of Contents………………………………………………..………vi List of Figures ……………………………………………………………ix List of Plates……………………………………………………………….x List of Tables……………………………………………………………..xi List of Graphs..………………………………………………………….xii CHAPTER ONE Introduction 1.1 Background of the study ……………………………………...1 1.2 Statement of problem …………………………………………..7 1.3 The main purpose of study……………………………………9 1.4 Objectives of study……………………………………………...9 1.5 Research Questions…………………………………………….9 1.6 Hypothesis………………………………………………….……10 1.7 Significance of the study……………………………………..10 1.8 Scope of study…………………………………………………..11 1.9 Definition of terms………………………………………….….11 CHAPTER TWO Literature Review 2.1 Relevant anatomy of the neck………………………………14 2.2 Aetiology of cervical spondylosis……………………………20 2.3 Prevention of cervical spondylosis…………………………21 2.3.1 Primary prevention……………………………………………21 2.3.2 Secondary prevention………………………………………..22 2.3.3 Tertiary prevention……………………………………………22 2.3.4 Sitting…………………………………………………….……22 2.3.5 Lying………………………………………………………….…24 2.4 Pathophysiology……………………………………………...24 2.5 Symptoms……………………………………………………..27

8
2.6 Examination and test………………………………………30 2.6.1 Physical finding……………………………….…………... .31 2.6.2 Radiological Exam…………………………………………..32 2.6.3 Differential diagnosis………………………………………32 2.6.4 Comparison of cervical spondylosis with Acute
Cervical Joint Lock and cervical sprain………………34 2.6.5 Histologic findings………………………………..……….35 2.7 Rehabilitation programme……………………………....35 2.7.1 Physical Therapy………………………………………..…35 2.7.2Occupational Therapy……………………………………37 2.7.3 Recreational Therapy…………………………………….38 2.7.4 Medical Complications…………………………………..38 2.7.5 Surgical Intervention…………………………………….39 2.7.6 Consultations with the following Specialists
may be helpful…………………………………………….40 2.7.7Medication…………………………………….…………...40 2.7.8Deterence/Prevention………………………………….. 41 2.7.9Prognosis……………………………………..…………….42 2.8 Infra red radiation…………………………….…………42 2.9 Cervical traction………………………………………….43 CHAPTER THREE Subjects, Materials and Methods 3.1 Introduction……………………………………………….49 3.2 Research design……………………………………….…49 3.3 Area of the study…………………………………………49 3.4 Target population………………………………………..50 3.5 Sampling Technique…….……………………………...50 3.6 Sample size……………………………………………….51 3.7 Subject description……………………………………..52 3.8 Selection Criteria………………………………………..52 3.8.1 Inclusion Criteria………………………………………..52 3.8.2 Exclusion Criteria………………………………………52 3.9 Materials………………………………………………….53 3.10 Procedure for data collection…………………………54 3.10.1Ethical consideration…………………………………54 3.10.2 Subject Recruitment…………………………………55 3.10.3 Anthropometric and biodata collection………….55 3.10.4 Physiotherapy diagnosis……………………………56 3.10.5 Measurement………………………………………….56 3.10.6 Treatment…………………………………….………..55

9
3.11 Method of Data Analysis……………………………59 CHAPTER FOUR Results and Discussions 4.1 Results………………………………………………….60 4.2 Test of Hypothesis……………………………………77 4.3 Discussion……………………………………………..79 CHAPTER FIVE Summary, Conclusion and Recommendation 5.1 Summary…………………………………………..…..81 5.2 Conclusion……………………….……………………82 5.3 Recommendation……………….……………………82 5.4 References………………………….………………….84 Appendices: Ethical Approval Master Sheet of Data Collected

10
List of Figures
Figure I Spinal Skeleton………………………………………… 14 Figure II Fourth Cervical Vertebra…………………………… .16 Figure III Zygapophyseal Joint………………………………… 17

11
List of Plates
Plate I Infra Red to the neck…………………………………… 56 Plate II Cervical Traction Inflexion ……………………………. 58 Plate III Cervical Traction in Extension ……………………. 58

12
List of Tables
Table I Basic Data on Patients used………………………… 61 Table II Analysis of Control Group Infra Red
Radiation only………………………………………… 62 Table III Analysis of the Experimental Group – Cervical Traction and Infra Red Radiation………………………… 67 Table IV Comparing the Control (Infra Red Radiation) and Experimental Group (Cervical Traction and Infra Red Radiation) ……………………………………….… 72

13
List of Graphs
Graph a. Comparing the Relief of pain in Infra Red Radiation and Cervical Traction plus Infra Red Radiation. …..75 Graph b. Sex in relationship to the relief of pain in the patients ………………………………………………………………….76 Graph c. Age in relationship to the relief of pain in the patients…………………………………………………………………. 77

14
List of Figures
Figure I Spinal Skeleton………………………………………… 14
Figure II Fourth Cervical Vertebra……………………………. 16
Figure III Zygapophyseal Joint…………………………………. 17

15
List of Plates
Plate I Infra Red to the neck…………………………………… 56
Plate II Cervical Traction Inflexion ……………………………. 58
Plate III Upright distraction……………… ……………………. 58

16
List of Tables
Table I Basic Data on Patients used………………………… 61
Table II Analysis of Control Group Infra Red
Radiation only…………………………………………… 62
Table III Analysis of the Experimental Group – Cervical
Traction and Infra Red Radiation………………………… 67
Table IV Comparing the Control (Infra Red Radiation)
and Experimental Group (Cervical Traction and
Infra Red Radiation) ……………………………………….… 72

17
List of Graphs
Graph a. Comparing the Relief of pain in Infra Red
Radiation and Cervical Traction plus Infra Red Radiation. …..75
Graph b. Sex in relationship to the relief of pain in the
patients ………………………………………………………………….76
Graph c. Age in relationship to the relief of pain in the
patients…………………………………………………………………. 77

18
CHAPTER ONE
Introduction
1.1 Background to the study
Cervical spondylosis is a very common and painful condition
affecting many people. It is a disorder caused by abnormal wear
and tear of the cartilage and bones of the neck (cervical
vertebrae) leading to degeneration and mineral deposits in the
cushions between the vertebrae (cervical disk) (Freedman 2006).
It can also be thought of as “grey hair” of the spine (Garfin and
Bono, 2011). Over the years, there had been divergent opinions
on the relevance of cervical traction in the management of neck
pain. The controversy was based on appropriate weight needed
for cervical traction on one side and the appropriate type of
conditions of neck pain that needs cervical traction on the other
side (Saunders, 1998). Consequently, there is no common
conclusive scientific opinion on this issue. The above
controversy makes it relevant for this study to be conducted in
order to assess the efficacy of this type of intervention in neck
pain management, especially with regards to pains associated
with cervical spondylosis.

19
Most neck pains are caused by a strain and can be treated
without surgery. Affected patients may be required to undergo
cervical traction, wear a cervical collar to limit neck movement
and support one’s head, in addition to short term bed rest
which allows one to rest neck muscles (Freedman, 2006). Of all
these treatment options cervical traction appears to be a more
relevant non-invasive approach in managing pains related to
cervical spondylosis. This form of treatment gently pulls apart
the head and stretches neck muscles thereby allowing the
cervical vertebrae which lie in between the head and the
thoracic spine to distract, thus relieving nociceptive pressure
exerted on nerve roots which emerge from discal spaces to
supply the muscles of the neck and upper limbs (Last, 1986). A
portable cervical traction device can be used at home or office.
Most studies (Hinderer and Biglin, 2002) have concluded that
elongation of cervical spine, by 2 – 20mm, can be achieved with
12.5kg or more of tractive force, 5kg of which is needed to
counter balance the weight of the head (less in some persons,
more in others). It is proposed that prolonged pull on the
cervical spine with adequate force leads to fatigue of cervical
paraspinal muscles, which are potentially of therapeutic value

20
in pain management when muscle spasm is present (Hinderer
and Biglin, 2002).
The amount of pull should be specified in the traction
prescription. Ordinarily cervical traction must comfortably pull
the head upward and forward at an angle of 30o from the
horizontal, and must be applied twice daily, and for periods of
30 minutes at a time. For cervical spine, distraction, forces
above 12.5kg needs to be achieved, but forces above 25kg
probably do not provide any additional advantage (Hinderer and
Biglin, 2002). In essence, available literature suggests that
properly applied cervical traction has great value in cervical
problems and needs to be further explored when pains arising
from cervical spondylosis are involved.
TYPES OF CERVICAL TRACTION
i. Halter Traction
This is a standard home cervical traction which is usually
accomplished in a sitting position. This apparatus affixes
to the back of an internal door and consists of a cervical
halter, a length of a cord over a pulley attached to the door
frame and weight most commonly a plastic bag filled with

21
water or a metallic weight corresponding to certain
kilogrammes
ii. Cervical Traction in supine position without force exerted
on the chin.
iii. Manual Mobilization and/or manipulation of the cervical
spine. This is indicated for patients younger than 45years
old. This age limit however, is not absolute (Winkel, et, al,
1996).
In limitation of motion in the upper cervical spine,
mobilization is indicated only when instability in that area
has been specifically ruled out. Mobilization is indicated in
functional disturbance of the cervical column even without
the presence of a disc lesion; of course all contraindication
must first be ruled out (Winkel, et al, 1996)
iv. Self Treatment
This is a series of technique proposed by Mckenzie which
employs application of repeated movements and sustained
positions that centralizes and abolishes the patient’s
symptoms (Rath 1984)

22
v. Cervical Airtrac
This is a scientific design; orthopaedic ambulatory traction
apparatus anatomically designed, thin weight, allows
nearly a full range, while wearing. “Airtrac 3000” helps
relieve weak shoulder muscle stress and radiating
discomfort. Soon after wearing cervical Airtrac 3000, the
disc compression and protruded cervical disc is reduced
due to the elongated intervertebral disc spaces and
foramina by cervical Airtrac Traction function. This
Cervical Airtrac elongates intervertebral disc resulting in
relief of the irritated nerve roots. By using Airtrac several
minutes each time, several times a day, Airtrac promotes
reduction of discomfort and relief of symptoms.
vi. Cervical Traction “Airplus or Airplus Deluxe”
Cervical Traction “Airplus” or “Airplus Deluxe” is a unique
designed neck elongation, and traction exercise device. It
relieves muscle spasm, stress and pressure in the neck,
shoulders, head and cervical vertebrae which gives result
in just a few short minutes after use. The main function is
based on relieving pressure from cervical disc.

23
vii. Dr Riter’s “Real-Ease” Neck and Shoulder Relaxer
This cervical and shoulder support system is very
comfortable whenever one can lean back or lie down on it
for 10-15 minutes. The Real-Ease shoulder and neck
relaxer will do the rest by aiding in relaxation.
1.2 Statement of the problem
The Royal College of General Practitioners in London
reported that “traction does not appear to be effective for
neck pain and low back pain” (Saunders, 1998). This
conclusion was given a three star rating which means that
the weight of evidence was a general consistent finding.
However, Saunders (1998) disagreed with the conclusion
of the Royal College of General Practitioners and based her
assertion on the possibility that their study either involved
the patients who could not benefit from cervical traction or
that the patients were under-loaded. Nevertheless, the
findings of another study conducted by Al-shatoury and
Galhom (2009) seem to support earlier view demonstrating
that traction in treatment of cervical pain is not better
than placebo in 2 randomized group treated. However,
their views were contradicted by a more recent study by

24
(Shakoor, et, al, 2010), and involved two groups of patients
suffering from cervical spondylosis who were treated with
cervical traction plus exercises and non-steroidal anti-
inflammatory drug (NSAID), respectively. It was found that
the improvement or relieve of pain among the patients
with cervical spondylosis was more in the group treated
with cervical traction plus exercise than those treated with
NSAID alone.
In essence, there is lack of convergence of expert opinions
on the clinical benefits of cervical traction prescription in
pain management among patients suffering from pain due
to cervical spondylosis. This suggests the need to reassess
the relevance of cervical traction as an adjunct therapy in
the physiotherapy treatment of patients with cervical
spondylosis. Moreover available literature suggests there is
no contemporary work of this kind in Nigeria, and thus
informs the need for this study.
1.3 The main purpose of the study
The main purpose of this study is to assess the use of
cervical traction with regard to physical management of

25
cervical spondylosis in order to determine its relevance as
a clinical tool required to relieve pain among patients in
such conditions
1.4 Objectives of the study
1. To determine if cervical traction could significantly relieve
pain in patients with cervical spondylosis compared to
infra-red radiation alone.
2. To determine the influence of age on the rate of pain relief
after cervical traction in patients with cervical spondylosis.
3. To determine the influence of sex on the rate of pain relief
after cervical traction in patients with cervical spondylosis.
1.5 Research questions
1. Does cervical traction relieve pain in patients with cervical
spondylosis?
2. What is the influence of age on the rate of pain relief after
cervical traction, among patients with cervical
spondylosis?
3. What is the influence of sex on the rate of pain relief after
cervical traction, among patients with cervical
spondylosis?

26
1.6 Hypothesis
This study sought to test that
1. Cervical traction when applied as a treatment modality in
patients with cervical spondylosis will reduce pain
significantly compared to infra–red radiation alone.
2. The rate of relief of pain using cervical traction therapy in
patients suffering from cervical spondylosis will be more in
younger than older patients.
3. Sex will have influence on the rate of relief of pain in
cervical spondylosis patients using cervical traction as a
therapy.
1.7 Significance of the study
1. If cervical traction relieved pain significantly in patients
with cervical spondylosis, this would help the clinicians to
prescribe straight forward adequate treatment instead of
under treating with only infra-red radiation in such
condition.
2. If the influence of age on the extent of pain relief after
cervical traction is determined it would be easier to plan
treatment regimen for the use of cervical traction for

27
various age groups of patients suffering from such
conditions.
3. If the influence of sex on the extent of pain relief after
cervical traction is determined, dosage, frequency and
duration of cervical traction prescription to patients of
various gender groups would be easier to perform.
1.8 Scope of study
The study will be delimited to patients with pain arising
from uncomplicated cervical spondylosis referred to the
Physiotherapy Department, National Orthopaedic hospital,
Enugu. Study will be limited to demonstrating the efficacy
of cervical traction in the relief of pain arising from cervical
spondylosis using numerical rating scale.
1.9 Definition of terms
i. Cervical Spondylosis: This is a type of disorder caused by
abnormal wear and tear on the cartilage and bone of the
neck with degeneration and mineral deposits in the
cushions between the vertebrae.

28
ii. Operational Definition of Terms
a. Level of pain: The degree or magnitude of noxious
discomfort which in the opinion of the patient represents
the scale of limitation to comfortable activities of living due
to cervical spondylosis
b. Uncomplicated cervical spondylosis: This refers to any
case of cervical spondylosis with no other disability than
pain and parasthesia.
c. Therapeutic Value: This refers to immediate benefits
arising from treatment that leads to pain reduction among
patients with cervical spondylosis.
d. Patients with cervical spondylosis: Patients who have
problem of cervical spondylosis and have been diagnosed
with this condition for at least 1 month prior to the study.
e. Parasthesia: This is a term used to signify diminished
sensory information. This refers to tingling and numbness
of the affected body area and may be the result of lesion of
any part of the afferent system.
f. Pain: Noxious discomfort which in the opinion of the
patient represents the scale of limitation to comfortable
activities of living due to cervical spondylosis.

29
CHAPTER TWO
Literature Review
2.1 Relevant anatomy of the neck
The cervical spine is the most mobile region of the spinal
column. The connection of the cervical spine with the head
leads to significant functional consequences in this area.
The first thoracic vertebra lies at the highest part of the sloping
thoracic operculum. From its upper border rises the cervical
spinal column, gently convex forward and supporting the skull.
A mass of extensor musculature lies behind the vertebrae. It is
supplied segmentally by posterior primary rami and supports
the cervical spine and head. The center of gravity of head lies
relatively forward. A much smaller amount of prevertebral flexor
musculature lies in front of the vertebrae and more laterally is
attached to the thoracic operculum and the scapula. It is
supplied segmentally by anterior primary rami. This
musculature comprises longus coli, rectus capitis anterior and
rectus capitis lateralis, longus capitis, scalenus anterior,
scalenus posterior and levator scapulae. Further back the neck
extends as high as the base of the skull. On each side of the

30
pharynx is a carotid sheath with the cervical sympathetic trunk
behind it. Emerging into the neck are the ninth, tenth, eleventh
and twelfth cranial nerves. Finally surrounding the whole neck
is a collar of fascia the investing layer of deep cervical fascia
which contains trapezius and sternomastoid muscle.
Functionally, the cervical spine is composed of two segments.
The upper consists of occiput, atlas (C1) and the axis (C2) while
the lower comprises functional units C3 - C7 vertebrae, flexion
and extension movements occur at the atlanto occipital joint.
The movement at C3 – C7 results in all above motions to a
variable extent at various segments.
(See diagram below)

31
Figure 1: The spinal skeleton (Adapted from Spine Universe, 2007)

32
The head is a lot to carry around. It can weigh about 7kg or
more. Not only does the neck fully support all that weight, it
enables one to nod, shake and turns ones head. There is no
other part of ones spine that has the ability to move so much;
90o of forward motion, 90o of backward motion, 180o of side-to-
side motion and almost 120o of tilt to either shoulder.
Technically, the neck is called the cervical spine and it begins
at the base of the skull. It contains 7 small bones (vertebrae)
which is labeled C1 – C7 the (‘C’ means cervical). The number 1
to 7 indicates the level of the vertebrae. C1 is closest to the
skull while C7 is closest to the chest.
In between each vertebrae are tough fibrous-absorbing pads
called the intervertebral discs. Each disc is made up of a tyre-
like outer band (annulus fibrosus) and a gel-like inner
substance (nucleus pulposus).
Besides the bones and the discs, the neck has joints, muscles
and ligaments. They are what make the neck so moveable.
They also stabilize the neck.
The neck houses the upper part of the spinal cord, nerve roots
and an elaborate system of arteries and veins. The nerves in

33
the neck help the brain communicate with the shoulders,
arms and chest. The arteries and veins circulate blood
between the brain and the heart.
All in all, the neck is amazing and intricate. However, because
it has such freedom of movement, it’s at a high risk of pain
and injury (see figure below).
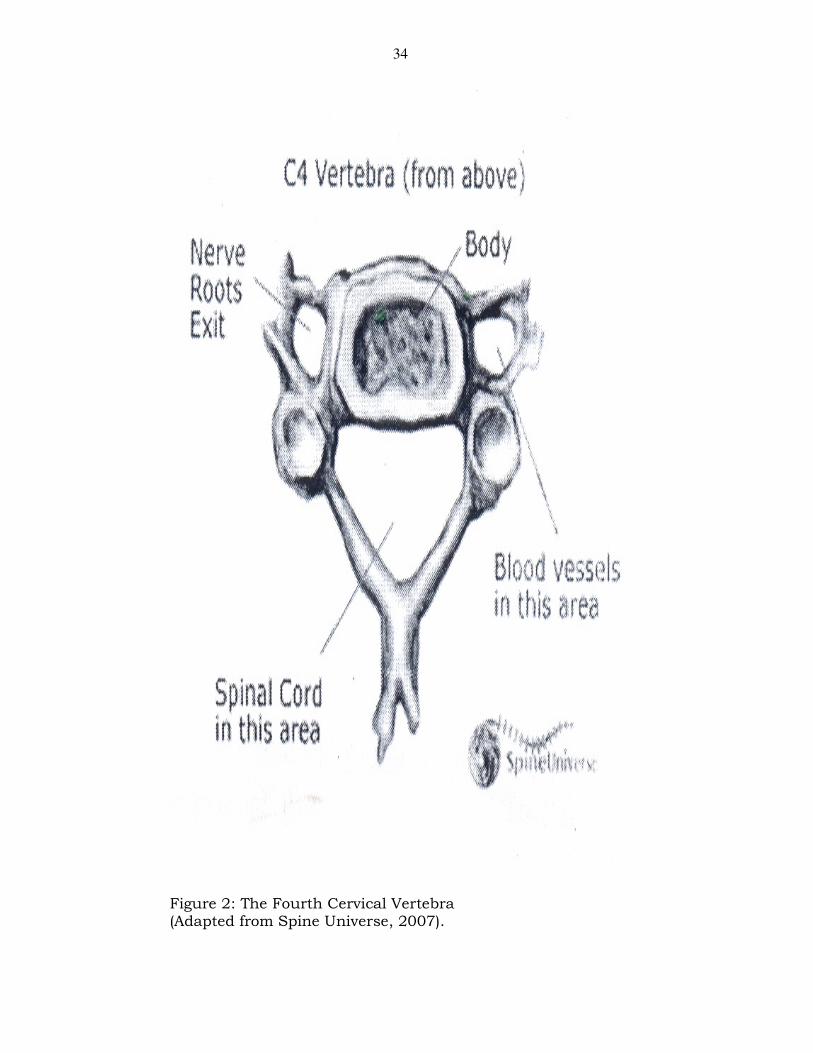
34
Figure 2: The Fourth Cervical Vertebra (Adapted from Spine Universe, 2007).

35
Zygapophyseal Joints
On the posterior aspect of the cervical vertebrae lie two superior
articular processes and two inferior articular processes. They
form joints with the adjacent cranial and caudal vertebrae,
respectively (See figure below).

36
Figure 3: Zygapophyseal Joint between two cervical vertebrae. The joint lies within the box 1. Superior articular process: 2. Inferior articular process. (Adapted from diagnosis and treatment of the spine by Winkel et al, 1996).

37
The capsule of these joints is rather loose except at the aspect
where the laxity of the capsule decreases. The position of the
joint surfaces in the frontal plane is nearly horizontal. In the
parasagital plane, the joint facets are oriented in such a way
that when an imaginary line is drawn parallel to the joint
surface, these lines converge cranially in the direction of the
eyes. The facets of the upper disc containing segments are
oriented approximately 40o in relation to the transverse plane.
The facets of the lower disc containing segments are inclined
approximately 65o in relation to the transverse plane. To a great
extent, the position of these articular surfaces determines the
movement possibilities of the cervical spine from C2 to C7.
The zygapohyseal joints contain so called meniscoid folds which
have grown into joints from the capsule. It is still not clear
whether or not these structures are innervated and thus can
cause pain. Bogduk and Engel (1984) stated that pain does not
occur through damage to the meniscus itself but rather, for
instance because of tearing of the meniscus from the capsule.

38
Pain
Pain of cervical origin has long been a challenge to physicians
and a plague to mankind. The timeless phrase “pain in the
neck” has characterized the human condition for centuries.
Mountcastle (2004) states that “pain is that sensory experience
evoked by stimuli that injure or threaten to destroy tissue,
defines introspectively by every man as that which hurts”. The
tissue sites where nociception occur are the posterior
longitudinal ligaments, nerve roots and their dural sheaths, the
facet capsule and the neck muscles. Nociception occurs from
injury, irritation, or infection of the sites. The intervertebral disc
consists of annular fibers within a mucopolysaccharide matric
with blood supply and no nerve ending other than minimal
unmyelineated nerve endings in the outer peripheral annulus
fibrosus.
Consequently only damage to the outer annular fibers can
conceivably cause pain. The nerve root emerge from cervical
spine through the foramina which contain the dorsal root
ganglion and their dural sheath both sides of nociception.
Flexion opens the foramina and extension closes them. Rotation
and lateral flexion of the neck close the foramina on the

39
concave side and open those on the convex side. Passive and
active movement of the neck triggers pain by nerve compression
(Cailliet, 2002).
A functional unit is two adjacent vertebrae separated by an
intervertebral disc and posteriorly two lamina, two pedicles and
zygapophyseal joints termed facets.
2.2 Aetiology of cervical spondylosis
Cervical spondylosis results from degeneration of the cervical
spine including the cushions between the cervical vertebrae and
joints between the bones of the cervical spine. There may be
abnormal growth or “spurs” on the vertebrae. These
accumulated changes caused by degeneration can gradually
compress one or more of the nerve roots. This can lead to
increasing pain in the neck and arm, weakness and changes in
sensation.
In advanced cases, the spinal cord becomes involved. This can
affect not only the arms but the legs as well. A previous neck
injury (which may have occurred several years prior can
predispose to spondylosis, but the major risk factor is aging. By
age 60, 76% of women and 85% of men show changes, that is

40
osteophytes, marginal lipping and narrowing of disc spaces;
consistent with cervical spondylosis on x-ray (Freedman, 2006).
2.3 Prevention of cervical spondylosis
The concept of prevention can be classified into primary,
secondary and tertiary prevention.
2.3.1 Primary prevention
Primary prevention in technology entails the prevention of
harmful influences on humans during the developing stages of
products, technical systems and processes. For example, this
primary prevention occurs when government requirements are
placed on certain products or processes. These are protective
regulations in relation to noise, radiation, fire, vehicles, harmful
materials and electrical safety or house hold products. In these
instances, there is an obvious relationship; between the cause
and the possible detrimental result.
2.3.2 Secondary prevention
This concerns the early detection of physical problems and early
diagnoses. In this sense, periodic preventive examinations are
important.

41
2.3.3 Tertiary prevention
Tertiary prevention can be described as prevention of worsening
of a situation. Specific technical resources are used in this
instance.
2.3.4 Sitting
Sitting on chair, should not be taken for granted. Still today, in
many countries, people squat, kneel or sit on the ground. The
origin of chairs probably lies in the boulder or other platform on
which the tribal chief sat, as time went on, ornate chairs were
made not to sit on, rather as status symbols. Even today the
status elements in thrones and directors’ chairs can be
recognized. The chair was also a symbol indicating the
scholarly, in the University setting, one still speaks of a
professorial chair. Western society without chairs is
unimaginable. Chairs can be classified roughly into upright
(hard) chairs and easy chairs.
Sitting for prolonged periods is required in schools and office
settings. Office workers spend up to three fourths of their
working time sitting. Half the working force consists of office
workers. There is much to criticize about office chairs.

42
Furthermore, the chairs found in homes are more often bad
than good. Most of the time, the biomechanical requirement
that should be incorporated into a chair’s body supporting
surfaces to guarantee relaxed mood (passive sitting) is not
observed (Winkel et al, 1996).
Arm rest for supporting the arm while sitting is of advantage by
unloading of the shoulder girdle and subsequently also of the
cervical spine. The height of the arm rest should correspond to
the level of the elbows with the arms in a slightly abducted
position. This also applies to the levels of the tabletops. Without
arm rests; the individual crosses the arms in front of the body
leaning on the table; or flexes the spine to rest the arms in the
laps. In automobiles an individual often props one arm on the
edge of the window pane or car door, or with the other arm
reaches across the back rest of the passenger seat. Seldom does
an individual drive for a long period with the hand in a “ten and
two position”. If the work requires that the centre of gravity of
the arms lies in front of the shoulders rather than underneath,
easing the work load can be attained by hanging up the arms.

43
2.3.5 Lying
When lying down on a bed, pillows could be easily deformable
and at the same time provide a good support for the head as
well as the neck.
2.4 Pathophysiology
Intervertebral disc loses hydration and elasticity with age and
these losses lead to other surrounding ligaments also losing
their elastic properties and developing traction spurs because of
loss of hydration. The disc subsequently collapses as a result of
biomechanical incompetence, causing the annulus to bulge
outward. As the disc space narrows, the annulus bulges and
the facets override. This change in turn increases motion at
that spinal segment and further hastens the damage of the
disk. Annulus fissures and herniation may complicate chronic
spondylotic changes.
As the annulus bulges, the cross-sectional area of the canal is
narrowed. This effect may be accentuated by hypertrophy of the
facet joints (posteriorly) and the ligamentum flavium, which
becomes thick with age. Neck extension causes the ligaments to

44
fold inwards, reducing the anterior-posterior (AP) diameter of
the spinal canal (Galholm, 2007).
As disc degeneration occurs, the uncinate process overrides and
hypertrophies, compromising the ventrolateral portion of the
foramen. Likewise, facet hypertrophy decreases the dorsolateral
aspect of the foramen. This change contributes to the
radiculopathy associated with cervical spondylosis. Marginal
osteophytes begin to develop. Additional stresses such as
trauma or long term heavy use may exacerbate this process.
These osteophytes stabilize the vertebral bodies adjacent to the
level of the degenerating disk and increases the weight bearing
surface of the vertebral end plates. The result is decreased
effective force on each of these structures.
Degeneration of the joints surface and ligaments decreases
motion and can act as a limiting mechanism against further
deterioration. Thickening and ossification of the posterior
longitudinal ligament (OPLL) also decreases the diameter of the
canal.
The blood supply of the spinal cord is an important anatomic
factor in pathophysiology. Radicular arteries in the dural

45
sleeves tolerate compression and repetitive minor trauma
poorly. The spinal cord and canal size are also factors. A
congenitally narrow canal does not necessarily predispose a
person to myelopathy, but symptomatic disease rarely develops
in individuals with canal larger than 13mm (Galhom, 2007).
Age
� Cervical spondylosis is a disease observed most commonly
in elderly individuals.
� Among those younger than 40 years, 25% have
degenerative disk disease (DDD) and 4% have foraminal
stenosis, as confirmed with magnetic resonance imaging
(MRI).
� In those older than 40 years, almost 60% have DDD, and
20% have foraminal stenosis, as confirmed with MRI (Galhom,
2007).
Trauma
� The role of trauma in spondylosis is controversial
� Repetitive subclinical trauma probably influences the
onset and rate of progression of spondylosis.

46
Work activity
Cervical spondylosis is significantly higher in patients who
carry loads on their heads than those who do not.
2.5.1 Symptoms
� Neck pain (may radiate to the arm or shoulder)
� Loss of sensation or abnormal sensation of the
shoulders, arms, or (rarely) legs.
� Weakness of the arm or (rarely) legs
� Neck stiffness that progressively worsens
� Loss of balance
� Headaches, particularly in the back of the head
� Loss of control of the bladder or bowels if spinal
cord is compressed (Freedman, 2006).
History
Common cervical syndromes associated with cervical
Spondylosis includes:
Cervical Pain
� Chronic suboccipital headache may be present. Mechanism
includes direct nerve compression, degenerative disk, joint or
ligamentous lesions and segmental instability.

47
� Pain can be perceived locally, or it may radiate to the occiput,
shoulder, scapula, or arm.
� The pain, which is worse when the patient is in certain
positions, can interfere with sleep.
Cervical Radiculopathy
� Compression of the cervical nerve roots leads to ischaemic
changes that cause sensory dysfunction (e.g. radicular pain)
and/or motor dysfunction (e.g. weakness). Radiculopathy most
commonly occurs in those aged 40 - 50 years.
� An acute herniated disk or chronic spondylosis changes
can cause cervical radiculopathy and or myelopathy.
� The C6 root is most commonly affected because of the
predominant degeneration at the C5 – C6 interspace, the next
most common sites are C7 and C5.
� Most cases of cervical radiculopathy resolve with conservative
management, few require surgical intervention (Freedman
2006).
Cervical Myelopathy
� Cervical myelopathy is the most serious consequence of
cervical intervertebral disk degeneration, especially when it is
associated with a narrow cervical canal.

48
� Cervical myelopathy has an insidious onset, which typically
become apparent in those aged 50 – 60 years. Complete
reversal is rare once myelopathy occurs.
� Involvement of the sphincters is unusual at presentation,
as based on the patient’s perception of symptoms.
� Five categories of cervical spondylotic myelopathy are
described; these are based on the predominant neurological
findings; as follows:
- Motor syndrome: This primarily involves the
corticospinal or anterior horn cells.
- Central cord syndrome: Motor and sensory
involvement is greater in the upper extremities than
the lower extremities.
- Brown sequard syndrome: Unilateral cord lesion with
ipsilateral corticospinal tract involvement and
contralateral analgesia are present below the level of
the lesion.
- Brachialgia and cord syndrome: Predominant upper
limb pain is present with some associated long tract
involvement.

49
Less Common Manifestations
� Primary sensory loss may be present in a glove like
distribution.
� Tandem spinal stenosis is a simultaneous cervical and
lumber stenosis due to spondylosis. It is a triad of findings:
neurogenic claudication complex gait abnormality and a
mixed pattern of upper and lower motor neuron signs.
� Dysphagia may be present if the spurs are large enough to
compress the oesophagus.
� Vertebrobasilar insufficiency and vertigo may be observed.
� Elevated hemidiaphragm, due to spondylotic compression of
C3 – C4 may be another finding.
2.6 Examination and test
A pain in the neck that continues to get worse is a sign
ofcervical spondylosis. It may be the only symptom in many
cases. Examination often shows limited ability to flex the hand
to the side (bend the head towards the shoulder) and limited
ability to rotate the head.
Weakness or sensation losses indicate damage to specific
nerve roots or the spinal cord. Reflexes are often reduced.

50
2.6.1 Physical finding
Finding at physical diagnosis may include the following:
� Spurling Sign: Radicular pain is exacerbated by extension
and lateral bending of the neck towards the side of the lesion,
which results in further foraminal compromise.
� Lhermite Sign: This generalized electrical shock sensation is
associated with neck extension.
� Hoffman Sign: Reflex contraction of the thumb and index
finger occur in response to nipping of the middle finger. This
sign is evidence of an upper motor neuron lesion. A Hoffman
sign may be significant if present bilaterally.
� Distal Weakness
� Decreased range of motion (ROM) in the cervical spine
especially with neck extension.
� Hand Clumsiness
� Loss of sensation
� Increased reflexes in the lower extremities and in the upper
extremities below the level of the lesion.
� Gait characteristically broad-based, stoop, and spastic
� Extensor planter reflex in severe myelopathy

51
2.6.2 Radiological exam
� A spine or neck x-ray shows abnormalities that
indicate cervical spondylosis.
� A computerized tomography scan (CT scan) or Spine
MRI confirms the diagnosis.
� A myelogram (X – ray or CT scan after injection of
dye into the spinal column) may be recommended to
clearly identify the extent of injury.
� An EMG may also be recommended
� An x-ray of the lower (lumbar) spine may reveal
degenerative changes in this region (Freedman 2006).
2.6.3 Differential diagnosis
� Adhesive Capsulitis
� Brown Sequard Syndrome
� Cervical Disc Disease
� Cervical Myofascial pain
� Cervical Sprain and Strain
� Chronic Pain Syndrome
� Diabetic Neuropathy
� Multiple Sclerosis
� Myofacial Pain

52
� Neoplastic Brachial Plexopathy
� Osteoporosis and Spinal Cord Injury
� Radiation-Induced Brachial Plexopathy
� Rheumatoid Arthritis
� Traumatic Brachial Plexopathy
Other problems to be considered:
- Ossification of the posterior longitudinal ligament (OPLL)
- Occipital neuralgia as a result of spondylotic changes
at C1 – C2
- Shoulder Problems
- Primary Spinal Cord Tumours
- Syringomyelia
- Extramedularly lesions – Tumours And Thoracic Disk
herniation
- Hereditary spastic paraplegia
- Normal pressure hydrocephalus
- Spinal cord infarction
- Spinal sepsis
- Whiplash syndrome-hyper extension
- Hyperflexion injury

53
- Double Crush Syndrome – coexistence of a radiculopathy
and peripheral nerve compression in the carpal or cubital
tunnel.

54
2.6.4 TABLE 1 Comparison Of Cervical Spondylosis With Acute Cervical Joint Lock And Cervical Sprain ASSESSMENT VARIABLES
ACUTE CERVICAL JOINT LOCK
CERVICAL SPONDYLOSIS
CERVICAL SPRAIN
Age of occurrence Late adolescence Usually over 30 Variable
History Sudden onset associated with quick movement but no
trauma
Gradual onset that may be related to minor trauma
Related to trauma
Common protective deformity
Rotation and lateral flexion away from the side of pain with slight flexion
Rotational and lateral flexion away from the side of pain with significant flexion
Often held rigid and unable to move in any direction
Area of pain Local cervical (C4 to C6
area) on the affected side away from which the head is tilted
More lateral (C4-C7 area)
may spread to ipsilateral scapulae often referred to ipsilateral limb and to occipital area
Varies but often
bilateral and generalized, including anterior upper chest and neck area
Neurological Findings
None The signs of altered nerve conductions may
be found
Extremely variable
Tissues likely responsible
Apophyseal joint Intervertebral junction (disk) and or osteophytes
Muscles, ligaments, tendons, joints
and discs.

55
2.6.5 Histologic Findings
Thinning and fragmentation of the articular cartilage may be
observed. The normal, smooth white articular surface becomes
irregular and yellow. Continued loss of articular cartilage leads
to exposure of areas of subchondral bone, which appears as
shiny foci on the surface (eburnation). Fibrosis, increased bone
formation, cystic changes frequently occur in the underlying
bone. Loss of articular cartilage stimulates new bone formation
usually in the form of nodules (osteophytes) at the bone edges.
2.7 Rehabilitation Programme
2.7.1 Physical Therapy
Immobilization of the cervical spine is a good treatment for
patients with cervical spondylosis. Immobilization limits the
motion of the neck, thereby reducing nerve irritation. Soft
cervical collars are recommended for daytime use only (Galhom
et al, 2007) but they are unable to appreciably limit the motion
of the cervical spines.
More rigid orthosis (e.g. Philadelphia Collar, Minerva Body
Jacket) can significantly immobilize the cervical spine. With the
use of any of the braces, the patient’s tolerance and compliance

56
are considerations. A program of isometric cervical exercise may
help limit the loss of muscle tone that results from the use of
more restrictive orthosis.
Model cervical pillow can better align the spine during sleep and
provide symptomatic relief for some patients:
� Cervical traction is also of benefit to patients
� The use of cervical exercises has been advocated in
patients with cervical spondylosis. Isometric exercises often
are beneficial to maintain strength of the neck muscles.
Neck and upper back stretching exercises as well as light
aerobic activities also are recommended. The exercise
programs are best initiated and monitored by a physical
therapist (Galhom et al, 2007).
� Passive modalities generally involve the application of heat
to the tissues in the cervical region, either by
means of superficial devices (e.g. moist heat packs) or
mechanism for deep heat transfers (e.g. ultra sound,
diathermy).
� Manual therapy (e.g. massage, mobilization, manipulation)
may provide further relief for patients with cervical
spondylosis. Mobilization is performed by a physical

57
therapist and is characterized by application of gentle
pressure within or at the limits of the normal motion with
the goal of increasing the ROM. Manual traction may be
better tolerated than mechanical traction in some patients.
Manipulation is characterized by a high velocity thrust,
which is often delivered at or near the limit of the ROM.
The intention is to increase articular mobility or realign
the spine. Contraindications to manipulative therapy
include mylopathy, severe degenerative changes, fracture
or dislocation, infection, malignancy, ligamentous
instability and vertebrobasilar insufficiency.
2.7.2 Occupational therapy
Patients with upper extremity weakness often lose their ability
to perform activities of daily living (ADL), vocational activities or
recreational activities. Lifestyle modifications may involve an
evaluation of workplace ergonomics, postural training, neck
school (supervised small-group therapy), stress management
and vocational assistance. Disability can be improved with
specific strengthening exercises of the upper extremities, special
splinting to compensate for weakness, and the use of assistive

58
devices that allow the patient to perform previously impossible
activities.
2.7.3 Recreational therapy
The recreational therapist can use recreational and community
activity to:
a. Help the patient maintain their physical strength, social
skills and motivation.
b. Assist the patient and family in adjusting to the disability.
c. Decrease the patient’s dependence.
d. Reinforce other therapies.
e. Provide community integration and
f. further evaluate the level of functioning in cases of severe
disability due to cervical spondylosis.
2.7.4 Medical complications
Cervical spondylosis may result in complications including:
� Cervical myelopathy
� Paraplegia
� Tetraplegia
� Recurrent chest infection
� Pressure sores

59
� Recurrent urinary tract infection
2.7.5 Surgical intervention
� Indications for surgery include the following:
a. Progressive neurological deficits
b. Documented compression of the cervical nerve root, spinal
cord, or both;
c. Intractable pain
� The aim of surgery is to relieve pain and neuronal
structured compression and to achieve stabilization in
select cases.
� Approaches for surgery are anterior or posterior
� Anterior approaches include the following diskectomy
without bone graft, diskectomy with bone graft, and
cervical instrumentation.
� Posterior approaches include the following decompressive
laminectomy, and foraminetomy, hemilaminectomy, and
laminoplasty.
2.7.6 Consultations with the following specialists may be
helpful:
� Psychologist or psychiatrist

60
� Neurologist
� Neurosurgeon and/or orthopaedic spinal surgeon
� Urologist
� Internist
� Occupational therapist
� Physical therapist
� Recreational therapist
� Social worker
2.7.7 Medication
The goal of pharmacology is to reduce morbidity and prevent
complications.
Drug Category Used
Non steroid anti inflammatory drugs – these agents are used in
the treatment of cervical spondylosis. If one class seems to be
ineffective after a 2 – week trial, a formulation from another
class may be tried – the most commonly used drugs are:
Ibuprofen, acetylsalicyclic acid, naproxen, indomethacin,
mefenamic acid, and piroxicam.
2.7.8 Deterrence/prevention

61
� Patients may apply the following measures to help prevent
cervical spondylosis or its complications:
- Avoid high impact exercise (e.g. running, jumping)
- Maintain cervical Rom with daily Rom exercise
- Maintain neck muscle strength, especially neck extensor
strength
- Avoid holding period (e.g. while driving or watching TV).
- Avoid prolong neck extension
- Be careful when performing physical activities that are done
infrequently; such activities can trigger a flare in symptoms.
� If the patient has early morning stiffness, a long, hot shower
every day may help.
� Cervical spondylosis is difficult to prevent because it is a part
of the normal ageing process. Individuals may reduce their
risk by maintaining good neck strength and flexibility, along
with leading an active and healthy life style. Preventing neck
injuries (e.g. using proper equipment in contact sports, head
rest and seat belt use in automobiles) may also reduce the
risk of developing this condition.
2.7.9 Prognosis

62
� Cervical spondylosis is a slowly progressive, chronic joint
disability especially when it is associated with neuronal
compression.
� Cervical spondylotic myelopathy is the most serious
consequence.
� High – signal intensity lesions can be seen on MRIs of spinal
cord compression; this finding indicates a poor prognosis.
2.8 Infra – red radiation
Infra-red radiation is emitted by luminous sources (bulbs of
various wattages) and non luminous sources (heating elements
or resistant materials). Since skin is a poor heat conductor, the
radiation penetrates the skin surface less than 10mm before
being absorbed by the tissue and converted to heat energy. A
rise in the skin temperature over 42.8oC rapidly produces
arteriolar flare and wheal. The patient feels the heat instantly.
Infra-red is commonly used for relaxation inducing relief of pain
from muscle spasm or tension, myofibrositis and rheumatic
joints. It has also been used to dry the skin over the inguinal
and perineal areas and gluteal fold to prevent bedsores. It
should not be used if the patient is sensitive to light. Reactions

63
such as heat induced urticaria have been observed (Weics,
Wodell and Brown 1976).
2.9 Cervical traction
Traction for disorders in the cervical spine ranges from
skeletal traction for fractures and for deformities, to the
use of manual traction with Turkish towel under the
occiput to separate the articular surfaces of the
zygapophyseal joints (Rath, 1984).
According to Rath (1984) cervical traction has the
following effects
a. Prevention and free up of adhesion within the dural
sleeves, nerve roots and adjacent capsular structures.
b. Relief of nerve root compression and irritation within the
intervertebral foramen
c. Separation (distraction) of the articular surfaces of the
apophyseal joint.
d. Improvement of the circulatory status within the epidural
spaces of the spinal and lateral root canals
e. Decompression of the intervertebral joint with reduction of
derangement of disk; and

64
f. Reduction of the inflammatory response pain and
subsequent muscle spasm (Rath 1984).
The intervertebral discs lying between successive vertebral
bodies from the second cervical vertebra downwards are
composed of fibro cartilage, the outer portion of which consists
chiefly of concentric rings of fibrous tissue; the annulus
fibrosous while the center of the disc nucleus pulposus is softer
and gelatinous.
The normal disc is capable of withstanding heavy load with
relatively little deformation and serves as an efficient shock
absorber. It can adapt to spinal movements and should
distribute rapidly changing stresses evenly up and down the
spine. Research suggests that many spines fail to achieve even
distribution of stresses (Mowat and Wood 1985). The tissue
sites where nociception occurs are the posterior longitudinal
ligaments, nerve root and their dural sheaths, the facet capsule
and the neck muscles.
Properly applied, cervical traction has great value in cervical
problems. It must comfortably pull the head upward and
forward at a 30 degree angle and be applied twice daily and for
65
a period of 30 minutes (Caillet 2002). Elnaggar et al (2009) was
of the opinion that both intermittent and continuous cervical
traction have a significant effect on neck and arm pain
reduction, a significant improvement in nerve function and a
significant increase in neck mobility.
In general sense, traction is another form of immobilization.
Additionally and probably most importantly, traction provides
mechanical distraction of the cervical spine. In a study carried
out by American Physical Therapy Association (2008), they
stated that clinicians should consider the use of mechanical
intermittent cervical traction, combined with other interventions
such as manual therapy and strengthening exercises for
reducing pain and disability in patients with neck and related
arm pain.
Theoretically, this opens the neuro foramen and tends to flatten
a bulging disc by placing the posterior longitudinal ligament
under stretch. Furthermore, if accompanied with some flexion,
it may relieve the pressure of osteophytes on the vertical floor of
the neural canal (Murphy and Lieponis 1989). Some however,
believe that it may increase ischaemia in the synovial tissue of

66
these joints. Quantitative changes in the cervical neural
foramen resulting from axial traction, noted a significant
increase in intervertebral foraminal area and height after each 5
kg increment in traction weight compared with the position in
which no weight was applied (Spine, 2008).
Whatever the mechanism, traction generally produced some
relief of pain particularly in the patients who exhibit a radicular
component (Murphy and Lieponis 1989). The presence of long
tract signs or myelopathy is a relative contraindication to
cervical traction in patients with severe spondylosis or disc
disease. Patients with frank disk herniation may also complain
of increased pain or radiculopathy and once traction has been
initiated, this complaint should prompt further evaluation by
means such as CT, MRI or Myelography.
Patients with massive para-cervical muscle spasm may also
complain of increased neck pain and spasm with initiation of
traction. Generally, it is advisable to control the spasm
adequately before initiation of traction.
The method of applying traction is very important. Although
some physical therapy centres have special apparatus for

67
applying cervical traction in the supine position, it has been
impractical to reproduce at bed rest. The standard home
cervical traction is usually accomplished in the sitting position.
This apparatus affixes to the back of an interior door and
consists of a cervical halter, a length of a cord over a pulley
attached to a door frame and a weight most commonly a plastic
bag that can be filled with a specific level corresponding to a
certain number of kilogram (kg). It has been found that the
optimum position imparting mild cervical flexion is achieved
with the patient facing door. As general, 4 to 6 kg of traction is
applied for 14 to 20 minutes per session. These parameters can
be adjusted according to patient’s tolerance and several
sessions per day, may be optimum tractions. Traction is
continued so long as it appears to contribute to clinical
improvement (Murphy and Lieponis, 1989).
An experiment was carried out by Cyriax (1971) to find out how
much pull is exerted when reducing cervical disc displacement.
The maximum was found to be 140kgf. Radiology was carried
out before and during fairly strong traction on the neck. It
showed that traction increased each joint space by 2.5mm. In
other words, it almost doubled the distance between the bones.

68
This is why disc lesions are not difficult to reduce as long as the
traction is adequate. In chronic or severe cases of cervical
spondylosis, the patient is admitted for halter traction (1-3
week), when the pain is severe (Murkle 1986).
In the management of cervical pain, if the traction (distraction)
manoeuvre relieves pain, cervical spine traction should be
considered (Bonica and Sola 1990). The amount of pull should
be specified in traction prescription. For cervical spine
distraction forces > 12.5kg need to be achieved but forces
>25kg probably do not provide any additional advantage
(Hinderer and Biglin, 2002). Studies (Renkens 2011) have
shown that neck traction must be constant so that the muscles
may tire and the strain fall on the joints. It generally takes 2
minutes of sustained traction before the intervertebral spaces
begin to widen. Forces between 10 and 25 kg are commonly
used to achieve intervertebral separation (Renkens, 2011). A
retrospective study found that cervical traction provided
symptomatic relief in 81% of the patients with mild-to-
moderately severe cervical spondylosis syndromes (Rana and
Crystal, 2011).

69
CHAPTER THREE
Subjects, materials and methods
3.1 Introduction
This chapter presented a detailed account of all aspects of the
method employed in this study including the study design, the
sampling process, materials for the study, procedure for data
collection and projected methods for data analysis. It also dealt
with ethical issues, reliability and validity of the instruments
that were employed in the study.
3.2 Research design
This study employed a case cross-over design. This was
adequate because the patients that were recruited for this study
already had cervical spondylosis. The response to the
experimental treatment was compared against a control
paradigm in the same patients to determine their therapeutic
effects. Thus a cross-over research design proved more relevant
to achieve the research objectives of this study.
3.3 Area of the study
The study was carried out at the Department of Physiotherapy,
National Orthopaedic Hospital, Enugu. National Orthopaedic

70
Hospital Enugu was established in the year 1974 with the
mission of taking care of those that sustained injury during the
1967-1970 Nigerian Civil War and also to take care of accident
and degenerative diseases in the former Eastern region of
Nigeria and environ. The National Orthopaedic Hospital Enugu
is a metropolitan hospital made up of approximately 8 wards
and 3 theatres. It has an estimated land mass of 120 acres of
land with a staff strength of 838 which includes 51 doctors, 217
nurses, 11 physiotherapists, 38 pharmacists, 44 laboratory
scientists, 8 radiographers amongst others.
3.4 Target population
The population of this study comprised all adult patients
between the age range of 30 – 60 years, suffering from cervical
spondylosis who were referred to the physiotherapy department
of the National Orthopaedic Hospital, Enugu between June and
October 2010. The population was made up of both male and
female patients.
3.5 Sampling technique
The study was a total study; all the patients that met the
selection criteria were included in the study.

71
3.6 Sample size
The minimum sample size for a finite population according to
Colditz (1994) is given by relation n = Z2P (1-P)/d2.
Where n = Sample Size
Z = 1.96 at 95% confidence interval
P = estimated population based on prevalence
d = precision allow 5% = 0.05.
Since the value of P is not known, the prevalence rate of cervical
spondylosis at the National Orthopaedic Hospital Enugu was
used to determine the number of patients to be involved in this
research. The prevalence rate of cervical spondylosis at National
Orthopaedic Hospital Enugu as at 2005, 2006, 2007, 2008,
2009 were 2.0%, 2.09%, 2.07%, 2.06% and 2.25% respectively
but that of the most current, that is 2009 was used thus
n = {1.962 x 0.0225 (1 – 0.0225)}/0.052 = 32
But all the available patients referred for physiotherapy
treatment within the duration of study were involved. The
number available was 30 which is less than the minimum size
of 32 and therefore allows for possible error.

72
3.7 Subject description
Subjects recruited for the study were only those with
uncomplicated cervical spondylosis between 30 and 60 years of
age.
3.8 Selection criteria
The following inclusion and exclusion criteria were applied to
this study.
3.8.1 Inclusion criteria
1. Only the patients who had uncomplicated cervical
spondylosis were included in the study
2. Only patients between 30 and 60 years of age were
included in the study
3. Only patients without visual, communication and hearing
disabilities were recruited for the study.
4. Only patients with a history of pain arising from diagnosed
cervical spondylosis, for at least 1 month prior to the
study, were involved
3.8.2 Exclusion criteria
a. Patients who had neck pain due to
i. Infection

73
ii. Trauma
iii. Tumour and
iv. Instability of the cervical spine were not included
b. Those patients with complications such as
i. Paralysis of the upper limbs
ii. Bedridden
iii. Severe hypertension or diabetes were not included
c. Patients with poor/absent thermal sensation were excluded
from the study.
3.9 Materials
- Traction kit (Model PA 51933 Cincinnati Ohio USA): A set
of traction kit (halter traction kit) was used to apply the
cervical traction on the patients.
- Graded Weights (kg, UK): Graded weights were used to
load the traction kit for traction of the cervical spine.
- Infra-red radiation lamp (Model Hanua Sollux 70 150W,
250V, UK): Infra-red lamp (luminous) was applied to the
patients to improve circulation of blood and relax muscle
spasm.
- A numeric rating scale instrument (NRS): This pain rating
scale was used for measuring the level of pain before

74
initiating treatment and at regular two weeks interval after
instituting the treatment intervention. The NRS
instrument is calibrated from 0 to 10 where 0 means no
pain and 10 is the worst pain ever experienced by the
patients.
- Soap, towel and sponge: For skin toileting to remove oil
and enhance vasodilation.
3.10. Procedure for data collection
3.10.1 Ethical Consideration
When carrying out a research, it is envisaged that this should
cause no harm or distress to the subjects for this reason ethical
permission and approval should be given. For this research
involving human subject, ethical approval from the Ethical
Committee of National Orthopaedic Hospital, Enugu was
obtained before conducting the study. All participants’
confidentiality was maintained using code numbers instead of
names and ensuring that records were destroyed after the
study. Informed consent was obtained from participants, which
means that they had adequate information regarding the
research and were capable of comprehending the information
and had the power of free choice enabling them to voluntarily

75
consent to participation in the research or decline participation.
In line with the views canvassed by Polit and Hungler (1993), it
was made clear to the participants of the study that they had
the right to refuse to participate or to withdraw at any stage of
the project.
3.10.2 Subject Recruitment
The patients were recruited from the physiotherapy clinic of the
National Orthopaedic Hospital, Enugu. Patients were enrolled in
the physiotherapy clinic at the hospital. The diagnosis of
cervical spondylosis were made at the out-patient department of
National Orthopaedic Hospital and confirmed by a referral letter
from their respective medical consultants. All the patients with
uncomplicated cervical spondylosis registered in the
physiotherapy clinic during the time of research (June –
October 2010) were recruited for the study.
3.10.3 Anthropometric and bio-data collection
The bio-data and anthropometric data (age, height, weight) of
the patients were obtained and recorded. The subjects were
required to fill a consent form after the purposes of the
experiment had been explained to them. The anthropometric
data was obtained using weighing scale (kg) and height scale

76
(cm) whereas the bio-data of the subjects were obtained based
on information given by the subjects.
3.10.4 Physiotherapy diagnosis
Physical diagnosis of cervical spondylosis was performed by
employing the Spurling Test. This was performed by
reproducing the radicular pain by extending the neck, rotating
it to one side, and pressing down on the head towards the side
of complaint. A positive test reproduces the radicular pain
(Cailliet, 2002). The cervical X-ray or radiograph was also
examined for classic features of cervical spondylosis including
the pressure of osteophytes, marginal lippings and narrowing of
discal spaces as well as degenerative changes of the cervical
vertebrae.
3.10.5 Measurement
Height
The patient’s height was obtained using the standiometer. Each
subject was asked to stand, backing the standiometer,
barefooted and eyes looking straight ahead, while the
researcher read off the height to the nearest 0.01 meter. The
measurement was taken thrice and average taken and recorded.

77
Weight
This was obtained using the weighing scale. The subjects
dressed in light clothes and were asked to stand barefooted on
the weighing scale looking ahead while the weight was read off
to the nearest kilogram. The measurement was taken thrice and
the average taken and recorded.
Pain Score
The pain intensity perceived by the subjects was obtained
through the Numeric Rating Scale of 0 – 10 (verified by Moran
et al, 2002). The procedure was explained and the subject
requested to point at the number that corresponded to the pain
he/she experiences, whereby 0 is no pain and 10 is worst
imaginable pain. The value chosen by the subject was then
recorded as the pain score. The procedure was carried out
before the treatment then at two weeks interval till the sixth
week.

78
3.10.6 Treatment
Control paradigm
Application of Infra-Red Radiation
The subjects came into the cubicle dressed in light clothing and
were administered with numeric rating scale measurement
before initiating treatment. Their necks were exposed. After a
thermal sensation test, the standing infra-red lamp was set
perpendicular to the neck for 15 minutes at a distance of 75cm
from the body to avoid scalding, after skin toileting. The
treatment was performed thrice a week for six weeks and
numeric rating scale (NRS) measurement was administered
after every two week and finally after 6 weeks. After the control
paradigm there was a 7 days wash-out before experimental
treatment was administered on the same patients.

79
Plate 1: Infra Red to the neck
Experimental Paradigm
Infra-red is applied as in the control paradigm followed by
application of load using cervical traction.
The subjects came into the treatment cubicle with light
clothing. Then he or she was instructed to sit on an
armless chair in the traction unit with both hips and
knees flexed at right angle to the vertical and horizontal
respectively. Then the canvas was hooked to the head and
the halter, and suspended on the over hanging pulley with
a cord on which opposite end was attached to the
appropriate weight. There was alternation of extension
(backing the door) and flexion (facing the door) at
subsequent visits. The weights were graded in kg and were

80
added until the tolerable weight was reached. Then 1kg
weight was removed to make the subject bear the weight
with ease for 15 minutes. The treatment was performed
thrice a week for six weeks and numerical rating scale
(NRS) measuring instrument was administered before
initiating treatment and after every two weeks and finally
at the end of 6th week.

81
Plate 2: Cervical Traction in flexion
Plate 3: Cervical Traction in upright distraction

82
Method of Data Analysis
Descriptive statistics for mean and standard deviation was
obtained and compared before and after treatment and
also obtained for age and sex. For test of significance in
the difference in mean, that is, before and after treatment
paired t-test was used (t-value < 0.05). For test of
significance in the difference in the various groups that is,
male and female and age category, independent t-test was
used. In this case the procedure was first tested F(1) equal
variance is assumed and (2) equal variance not assumed.

83
CHAPTER FOUR
Results and Discussions
Table 2 Baseline characteristics of patients evaluated at
initial assessment.
N Range Mean (x + SD)
Age (years)
Duration (months) Before treatment
Height (m)
Weight (kg)
Valid N
30
30
30
30
30
30 – 60
1-48
1.45 – 1.90
61 – 128
50.20 ± 8.51
12.53 ± 1.28
1.62 ± 0.13 86.30 ± 14.83
Note: X ± SD = mean ± standard deviation
The above table shows the baseline characteristics of the
participants of the study. It shows that the age range of the
participants is between 30 and 60 years old and that the
participants who came for the study earliest came 1 month after
the beginning of the problem and one that came latest came 48
months after and that their average age was 50.20 ± 8.51 and
that the heaviest patient was 128 kg and lightest 61kg.

84
Table 3 Pain relief with time in control group
Group N Mean (x + SD) Correlation (r) T p- Value
Pair NRS Before 1. Treatment x/10 and NRS after 2
weeks of treatment. Pair NRS Before 2. Treatment x/10 and NRS after 4 weeks of
treatment x/10 Pair NRS Before 3. Treatment x/10
and NRS after 6 weeks of treatment x/10
30
30
30
0.53 ± 0.57
0.90 ± 0.61
1.53 ± 0.87
0.91
0.90
0.91
5.11
8.12
14.70
0.00
0.00
0.00
NRS = Numerical Rating Scale
X ± SD = mean ± standard deviation
There is progressive increase in mean NRS difference as weeks
go by. The above table shows progressive increase in mean
numeric rating scale from the period before treatment to the 6th
week of treatment and the 2nd, 4th and 6th weeks shows p-value
at 0.00 which means p <0.05, that is significant.

85
Table 4. Difference in rate of pain relief by sex in control
group
Sex
N Mean (x + SD) t F P- Value
Difference in NRS After Treatment
Equal variance
assumed
Male
Female
18
12
1.56 ± 0.51
1.50 ± 0.67
0.257
1.67
0.799
X ± SD = mean ± standard deviation NRS = Numeric Rating Scale When p < 0.05 = Significant p > 0.05 = Non significant
The table above shows that the mean numeric rating scale
difference in the male at 1.56 ± 0.51 is not much different from
that of the female group at 1.50 ± 0.67. The p-value is 0.79.
That is p > 0.05, showing non-significance.

86
Table 5 Difference in rate of pain relief by age in control group.
Age N Mean (x ± SD)
t f-value
p-value
Difference in NRS after Treatment X/10
Equal variance assumed
Equal variance
30 – 44yrs
45 – 60 yrs
8
22
1.88 ± 0.64
1.4 ± 0.50
2.09
0.23
0.04
NRS = Numeric rating scale X ± SD = Mean ± Standard Deviation When P< 0.05 = Significant P> 0.05 = Non-Significant The table above shows that there is reasonable difference
between the mean numeric rating scale difference in younger
age group at 1.88+ 0.64 and older age group at 1.4. ± 0.50.
That is the younger is greater by 0.47 and P< 0.05, that is
significant.

87
Table 6 Pain relief with time in experimental group
N Mean (X ± SD)
Correlation t-value p-value
1. Pair NRS before Treatment x/10 - NRS after 2 weeks of Treatment pair
2. Pair NRS before Treatment
x/10 - NRS After 4 weeks of Treatment x/10 3. Pair NRS before Treatment
x/10 - NRS After 6 weeks of Treatment x/10
30
30
30
2.77 ±1.04
4.93 ± 1.57
6.10 ± 1.35
0.65
0.01
0.12
14.57
17.17
24.79
0.00
0.00
0.00
NRS = Numeric rating scale X ± SD = Mean ± Standard Deviation When p < 0.05 = Significant P>0.05 = non significant
The table above shows that there is progressive increase in the
mean numeric rating scale difference from before treatment to
the sixth week of treatment and the p- value for the 2nd 4th and
6th weeks showed 0.00 that is p<0.05 that is significant.

88
Table 7
Difference in rate of pain relief by sex in experimental group.
Sex N Mean (x ± SD)
t f-value p-value
Difference in NRS after Treatment X/10 Difference in NRS after
treatment X/10 Equal variance assumed
Male Female
18 12
5.94 ± 1.16 5.83 ± 1.53
0.23
0.24
0.82
NRS = Numeric Rating Scale X ± SD = Mean ± Standard Deviation The table above shows that the difference in mean numeric
rating scale difference between male and female groups is very
minimal, that is male 5.94 ± 1.16 and female 5.83 ± 1.53
and p-value is 0.82. That is the P>0.05, showing non
significant.

89
Table 8 Difference in rate of pain relief by age in
experimental group
Age Mean
(X ± SD)
t f-Value P-Value
Difference in NRS after Treatment x/10
Equal variance
assumed Difference in
30 – 44yrs 45 – 60yrs
X ± SD 6.75 ± 1.58 5.59 ± 1.05
26.81
47.46
0.00
Note x ± SD = mean ± standard deviation P< 0.05 = significant P>0.05 = non significant The above table shows that the mean numeric rating scale
difference is more in younger age group that is 30 -44 year
group at 6.75+ 1.58 than the older age group that is 45-60
years group at 5.59+ 1.05. And the p-value 0.00 shows high
level of significance.

90
Table 9 The difference between the control and experimental group in pain relief.
MEAN
Difference
F t-value P-Value
IRR, NRS X/10 IRR, Cervical
Traction NRS x/10
1.53
6.100
0.93
38.71
4.80
24.38
0.34
0.00
When P< 0.05 = Significant P> 0.05 = Non Significant The table above shows high mean numerical rating scale
difference that is 6.10 the experimental that is IRR + Cervical
Traction group compared to 1.53 in the control that is IRR
group and the level of P-value 0.00 in infra red + cervical
traction is very high comparable to infra red alone at 0.34.

91
a.
After 6 WeeksAfter 4 WeeksAfter 2 WeeksBefore
Treatment Period
7
6
5
4
3
2
1
0
Me
an
NR
S x
/10
IRR,Cervical Traction
IRR
Treatment Received
Fig a Comparing the relief of pain in Infra Red Radiation and Cervical Traction plus Infra Red
Radiation
The above graph shows that there is drastic progressive
decrease in numerical rating scale tending to zero in cervical
traction plus infra red group comparable to infra red alone.

92
b.
IRR
,Cervic
al T
ractio
nIR
R
Treatm
en
t Receiv
ed
After 6 WeeksAfter 4 WeeksAfter 2 WeeksBefore
Treatment Period
7
6
5
4
3
2
1
0
Mean
NR
S x
/10
7
6
5
4
3
2
1
0
Mean
NR
S x
/10
Female
Male
Sex
Fig. b. Sex in relationship to relief of pain in the patients
The above graph shows that in both cervical traction plus infra
red and infra red alone, there is no sex difference in the rate of
relief of pain.

93
IRR
,Ce
rvic
al T
ra
ctio
nIR
R
Tre
atm
en
t Re
ce
ive
d
After 6 WeeksAfter 4 WeeksAfter 2 WeeksBefore
Treatment Period
7
6
5
4
3
2
1
0
Mea
n N
RS
x/1
0
7
6
5
4
3
2
1
0
Me
an
NR
S x
/10
45-60 yrs
30-44 yrs
Age
Fig. c. Age in relationship to relief of pain in the patients
The above graph shows that there in both cervical traction plus
infra red and infra red alone there is slight difference in age
pain relief.

94
4.2 Test of Hypothesis
Hypothesis I
Statement: cervical traction when applied treatment modality in
patients with cervical spondylosis will reduce pain significantly
compared to Infra-red radiation therapy only.
For cervical traction and infra red
Before treatment:
NRS mean value: 6.13
After 6 weeks:
NRS mean value: 0.03
For IRR only:
Before treatment:
NRS mean value: 6.13
After 6 weeks 4.60
P – Value for CT + IRR: 0.00: significant
P – Value for IRR only: 0.338: not significant (p > 0.05)
So the hypothesis is upheld.

95
Hypothesis II
Statement: The rate of relief of pain using cervical traction
therapy in patients suffering from cervical spondylosis will be
more in younger than older patients.
For Age 30 – 44yrs
Mean difference in NRS after treatment: 6.75
For Age 45 – 60yrs
Mean difference in NRS after treatment: 5.59 which gave a
difference of: 1.16 more in younger adult (that is 30 – 44yrs) so
the hypothesis is upheld.

96
Hypothesis III
Statement: sex will have influence on the rate of relief of pain in
cervical spondylosis patients using cervical traction.
For male:
Mean difference in NRS after treatment: 5.94
For female:
Mean difference in NRS after treatment: 5.83
The difference: 0.11
P – Value: 0.878
Not significant (P > 0.05)
So the hypothesis is rejected.

97
4.3 Discussion
4.3.1 To determine if cervical traction could significantly
relieve pain in patients with cervical spondylosis compared
to infra red radiation alone.
Cervical traction relieved pain very significantly in experimental
group compared to the result got in the control group that is
infra red alone. This is in agreement with Shakoor et, al 2012
who stated in the research where they had two groups, cervical
traction plus exercise and non-steroidal anti inflammatory drug
respectively that relieve of pain in group with cervical traction
and exercise was more than that of the group with non steroidal
anti inflammatory drug. Also the use of high weight starting
from 12.5kg for the cervical traction was beneficial and this is
in line with Hinderer and Biglin (2002) and Renkens (2011) who
stated that at least 12.5kg weight is necessary to distract the
cervical spine. The benefit of cervical traction was also
documented by Rana and Crystal (2011) who found in their
retrospective study that cervical traction provided symptomatic
relief in 81% of the patients with mild to moderately severe
cervical spondylosis syndromes. The effect of traction was also

98
demonstrated by Murphy and the Lie- ponis, (1989) who
observed that flexion traction with 4 to 6kg weight takes care of
pressure of osteophytes on the vertical floor of the neural canal.
It was observed in the study that the rate of relief of pain in
experimental group that is cervical traction and infra red
combined was visible even by the second week. This might be
probably because of alternation of upright distraction and
flexion traction which is unique for this study.
4.3.2 To determine the influence of age on the rate of
pain relief after cervical traction in patents with cervical
spondylosis
The study shows that relief of pain after cervical traction is
slightly more pronounced a younger age group than the older in
both control and experimental group but this distinction was
not very sharply defined probably because of the small number
of patents who participated in the study. It is likely that
involving higher number of participants will give a better
outcome. No available current literature has come out with an
authentic view on this (Ellenberg et, al, 1994).

99
4.3.3 To determine the influence of sex on the rate of pain
relief after cervical traction in patients with cervical
spondylosis
From the result of the study it was noticed that sex has no
influence on the rate of relief of pain. This fact is shown in both
control and experimental group. This implies that sex has no
effect on the rate of pain relief. The past literatures have not
had any authentic documentation on this fact (Ellenberg et, al,
1994).

100
CHAPTER FIVE
Summary, Conclusion and Recommendation
5.1 Summary
Cervical Spondylosis is a disorder caused by abnormal wear on
the cartilage and bones of the neck with degeneration and
mineral deposits in the cushions between the vertebrae. It is a
degenerative disease which comes up with the aging process.
This makes it a bit difficult to treat. This study aims at
assessing the use of cervical traction as an adjunct treatment
for this condition. Literature was reviewed in the relevant
anatomy of the neck spine, the pathophysiology of cervical
spondylosis, the different types of cervical traction application
and infra red radiation. A Standiometer and weighing scale were
used at initial visit. Age was got from the patients while
Numeric Rating Scale was used to ascertain pain intensity at
initial visit, after two weeks, four weeks and after the sixth
week. A total of 30 patients who met the criteria for selection
participated in the study. All the patients were referred by the
medical consultant at National Orthopaedic Hospital Enugu
Out Patients Department. All the data obtained were analyzed
using the statistical package for social sciences (SPSS) version

101
13.0. The results of the measurements and out outcome of
analysis were also presented.
The Infra Red only paradigm showed significant improvement
after the 6th week but quite insignificant comparable to infra red
and cervical traction paradigm, that is experimental paradigm.
That is to say that cervical traction and infra red combined is
superior to only infra red treatment (P < 0.05).
5.2 Conclusion
1. Each of the treatment, cervical traction combined with
infra red, infra red alone significantly reduced patients
pain
2. Cervical traction combined with infra red radiation showed
a better outcome than the infra red radiation only
treatment.
3. When infra red radiation only treatment outcome was
compared with infra red radiation and cervical traction
therapy, the outcome of infra red only was not significant.
5.3 Recommendation
1. Cervical traction should be included in all the treatment of
cervical spondylosis.

102
2. Where selection criteria allows, heat modality should
always be combined with cervical traction for the
management of cervical spondylosis.
3. The influence of sex, Age, height and weight on the rate of
pain relief should be investigated.
4. The study should be replicated using larger sample size.
5. Other forms of heat therapy such as shortwave diathermy
and ultra sound therapy should be used in alternative to
infra red radiation to investigate their effect on cervical
spondylosis.
5.4 Limitations Of The Study
1. Small number of patients involved in the study may have
affected the optimum accuracy of the study.
2. Other prevailing health of the problems among the
participants could have interfered with the result.
3. Some medication the patients were using might have
affected the result of the study.

103
References
Akinbo S.R.A, Noronha C.C., Okankwom A.O; Danesi M.A.
(2005). Comparative Efficacy study of Morind citrifolia
(NONI) with selected Physiotherapy Modalities in the
management of patients with cervical spondylosis, Nig
Jour. of Medical Rehabilitation Vol. 10 No. 18,
35 – 41.
Allen W.B.S (2007) Spinal Traction. Spine Universe 1-3
http://www.spineuniverse.com/displayarticle1472html.
Al-shatoury H.A.H. Galhom A.A. (2009). Cervical Spondylosis.
e-medicine, physical medicine and Rehabilitation.
http://emedicine.medscape.com/article/306036treatment
http://www.orthoinfo.aaos.org/topic:cfmTopic=400369.
American Academy of Orthopaedic Surgeons (2007). Cervical
spondylosis 1-3 American Physical Therapy Association
(2008) Neck Pain. Jour Orthopaedic Sports and Physical
Ther. 38 (9): A1 - 34
Bogduk N., Engel R (1984). The Menisci of the lumbar
zygapophyseal joints: A Review of their Anatomy and
clinical significance. Spine: 9: 454.

104
Bonica, J. Sola A.E. (1990). Neck pain. The management of pain
2nd ed. Lea & Febiger. Pennsylvania; pp. 848 – 868.
Cailliet, R (2002) Neck pain. Physical Medicine and
Rehabilitation secrets 2nd ed. Hanley and Belfus Inc.
Philadelphia; pp 251 – 253.
Cervical traction support and Exercises system (2007) 1-9
http://www.buymag.com/neck-pain.html.
Cyriax J. (1971) Treatment of cervical lesion. Cervical
spondylosis. Butter worth and co (publisher) Ltd pp. 67-
80.
Department of Orthopaedic Surgery Stellen Bosch University
(2007). Halter Traction, Skull Traction
http://www.sur.al.za/orth/weblt-ortho/general/trac-
3/html.
Ellenberg M, Honet J.C, Trancer WJ (1994) cervical
Radiculopathy. Arch. Phys med. Rehabilitation 75; 3: 342-
52.
Elnaggar (2009) Cervical Traction. Egypt J. Neurol. Psychiat.
Neurosurg. Vol. 46 (2) – July.

105
Freedman, K.B. (2006). Cervical spondylosis. medicine plus
http://www.n/m.nih.gov/medlineplus/ency/article/0043
6
Galhom A.A; Wagner, F.C., Al-Shatoury H.A (2007).cervical
spondylosis. medicine 1-21
http://www./medicine.com/pmr/topic27.html
Garfin S. R. and Bono C. M. (2011) Cervical Spondylosis:
Patient History and Case. Spine Universe
http://www.spineuniverse.com/conditions/spondylosis/
cervicalspondylosis.
Hinderer, S.R., Biglin, P.E.(2002). Traction Manipulation and
Massage. Physical Medicine and Rehabilitation secrets. 2nd
ed. Pp 528 – 532.
Judovic, B.D. (1952). Herniated Disc a new form of Traction
Therapy. American jour. of surgery No. 12 pp 646 - 656
Last R.J. (1986) Anatomy Regional and Applied 7th ed. Longman
Publishers Singapore pp. 465 – 468.
Medline plus medical Encyclopedia:(2007) cervical
spondylosis1-3
http://www.n/m.nih.gov/medlineplus/ency/article/0004
36.html.
106
Moran, Mawdley, Roberta H, Kelley A, Conniff, Lisa A (2002):
Reliability of two commonly used scales with Elderly
patients. Jour. of Geriatric physical therapy.
Mowat A.G., Wood, P.M. (1985). Degenerative Arthritis of the
spine and intervertebral Disc Disease. Cash Text book of
Orthopaedic and Rheumatology for physiotherapists pp.
230 – 248 first Indian ed.
Muckle, P.S. (1986). Spinal problem including Disc syndromes.
Outline of Orthopaedic practice. John Wright and Sons Ltd,
Bristol, England; pp. 75 – 104.
Murphy, M.J., Lieponis J.V. (1989) Non-operative Treatment of
cervical spine pain. The cervical spine 2nd ed.; pp 671 –
677.
Rana S. S. and Crystal H. A. (2011) Diagnosis and
Management of Cervical Spondylosis
medscapehttp:/emedicinemedscape.com/article/1144951
–treatment. May.
Renkens (2011) Neck Pain. http://www.neckpain traction.com
Saunders, H.D. (1998). The controversy over Traction for Neck
and Low Back pain. Physiotherapy; 84 (16):285 - 288

107
Shakoor M.A; Ahmed MS, Kibria G, Khan AA, Mian MA, Hasan
SA, Nahars, Hossain MA (2010) Effect of cervical Traction
and Exercise in cervical spondylosis medline
http://www.ncbi.n/m.gov/pubmed/12825763
Spine(2008) Cervical Traction. Spine Jour. July – Aug; 8 (4):
pp: 619 – 23.
Walker K. A. (2011) Physical Therapy for Spondylosis. Spine
Universe. April
http://www.spineuniverse.com/conditions/spondylosis/
physical-thera.
Winkel D, Aufdemkampe G, Meijer O.G., Matthijs O. Phelps V
(1996). Cervical spine. Diagnosis and Treatment of the
spine pp 542 – 714.