idsr links with other surveillance programs · surveillance and response (idsr) strategy. the...
TRANSCRIPT

Letter from the EditorIDSR LaboratoryStrengthening StrategiesLaboratory confirmation of certain priority diseases is a keyelement of the Integrated DiseaseSurveillance and Response(IDSR) strategy. The TechnicalGuidelines for IDSR in theAfrican Region recommend thatfor epidemic-prone diseases, 5-10 suspected cases should be laboratory-confirmed once a disease-specific threshold hasbeen reached. In order tostrengthen national capacities for laboratory confirmation, theAfrican Regional Office of theWorld Health Organization(WHO/AFRO) in collaborationwith CDC has focused on the following priorities:
• Communications and informationnetworks
• Standard laboratory diagnosticmethods and materials
• Laboratory-based training
• Links to epidemiologic activities
• Links to other laboratory programs
• Quality control and qualityassurance programs
• Advocacy for the role of thepublic health laboratories
Progress has been made on severalfronts. Subregional conferencesof national public health laboratorydirectors have fostered communi-cations and information networksby allowing a forum for the discussion of common goals andchallenges. Computers and soft-ware, supplied to the nationalpublic health laboratories, willhelp to ensure the continueddevelopment of these networks.WHO/AFRO, in collaborationwith CDC, has adopted standardlaboratory diagnostic methods forbacterial epidemic-prone diseasesand supplied critical reagents forthese methods to national publichealth laboratories.
Dear Collaborators,
Disease prevention and control programs depend
on timely and reliable disease surveillance
information for evidence-based decision making.
In efforts to strengthen disease surveillance,
Integrated Disease Surveillance and Response
(IDSR) teams at CDC and the World Health
Organization (WHO) are partnering with several
programs to improve diagnostic information
and the capacity for surveillance and response.
These partnerships result in exchanging ideas
and expertise, sharing products and resources,
and conducting joint activities. These linkages
enrich and energize partner organizations and
help the ultimate beneficiaries of public health
programs--individuals in the community. This
issue highlights IDSR links with a pediatric
meningitis surveillance project supported by
the Global Alliance for Vaccines and
Immunization, and the Gates’ Foundation
Children’s Vaccine Program.
In this issue, you will find:
IDSR Links with Other
Surveillance Programs..................…..Page 1
Perspective from WHO HQ ..............Page 4
IDSR Efforts Support CDC Global
Immunization Strategies ....................Page 4
Publications ........................................Page 5
Calendar of events ..............................Page 5
• Editor, Bradley A. Perkins, M.D.Chief, Meningitis and Special Pathogens Branch, DMBD, NCID
• Managing Editor, Kathy Cavallaro, M.S.;[email protected]
• Contributing Editor, Helen Perry, M.A.
• Layout, Diane Speight, B.A.
IDSR Links with Other Surveillance Programs
Fall 2001
Standard laboratory methods for bacterial meningitis, cholera, and shigella werethe focus of the recent WHO-CDC workshop in Johannesburg, South Africa.

I D S U p d a t e B u l l e t i n • F A L L 2 0 0 1 P a g e 2
In June 2001, the first WHO-CDClaboratory-based training on stan-dard diagnostic methods was held.This practical workshop was con-ducted in conjunction with anotherprogram—the Hib-PediatricBacterial Meningitis (Hib-PBM)Surveillance Network—because ofcommon laboratory and epidemio-logic objectives.
Hib-Pediatric BacterialMeningitis SurveillanceNetworkThe Global Alliance for Vaccinesand Immunization (GAVI) supportsthe introduction of vaccines indeveloping countries. Theseinclude new vaccines for diseasessuch as Haemophilus influenzaetype B (Hib), Streptococcus pneu-moniae, and Neisseria meningitidis,all major causes of mortality andmorbidity in children in developingcountries. To evaluate the impact ofthese effective, yet costly vaccines,accurate and reliable information isneeded to show that the extra costof these vaccines is balanced by asignificant reduction in disease.
Surveillance data also play a keyrole in advocacy for the vaccines.Information on laboratory-con-firmed cases will give reliable dataabout disease burden. Physicianscan use these data to advocate with high-level political and health leaders for new vaccines.
To facilitate the collection of surveillance data on these diseases,the Gates’ Foundation Children’sVaccine Program (CVP) at theProgram for AppropriateTechnology in Health (PATH) hassupported WHO/AFRO in thedevelopment of the Hib-PBMSurveillance Network. This net-work is being implemented in one
major pediatric hospital in each ofmore than 20 countries in theAfrican region.
The program detects cases of menin-gitis caused by Hib, S. pneumoniae,and N. meningitidis in childrenunder 5 years of age in sentinel hospitals. Each case is laboratory-confirmed by CSF culture and isolation performed by a laboratoryat the sentinel site. To build theneeded laboratory capacity, the program looked to the the WHO-CDC laboratory-based workshop as a vehicle for transferring technicalexpertise to laboratories in the Hib-PBM Surveillance Network.
Joint WorkshopThe purpose of the WHO-CDC laboratory-based workshop was to build capacity in national publichealth laboratories for standardmethods for isolation and identifi-cation of bacterial agents of meningitis, cholera, and shigella.To ensure the use of standard meth-ods in the Hib-PBM SurveillanceNetwork, the workshop was alsomade available to the laboratoriansat the sentinel sites in the network.At the same venue, WHO conduct-ed an orientation to the Hib-PBMSurveillance Network for participat-ing epidemiologists, data managers,and laboratorians (See Table 1). TheWHO-CDC Joint Workshop wasconducted in June 2001 in collabo-
ration with the South AfricanInstitute for Medical Research(SAIMR), Johannesburg, SouthAfrica. Participants in the work-shop included laboratorians, epidemiologists, ExpandedProgramme for Immunization (EPI) managers, clinicians and data managers from national publichealth laboratories, ministries ofhealth, and the Hib-PMB surveil-lance network (See page 3).
A second workshop will be conducted in November 2001 fornational public health laboratoriansfrom 20 Francophone countries andlaboratorians from 9 Hib-PBM
sentinel sites. WHO/AFRO in collaboration with CDC will pro-vide follow-up technical assistanceto workshop participants over thecoming months on surveillance and laboratory issues.
This joint workshop brought togetherlaboratorians, epidemiologists, EPI managers, clinicians and datamanagers to collaborate on surveil-lance and laboratory activities.This collaboration allows variouspublic health disciplines to understandeach other’s roles, needs, and challenges in surveillance activitiesof priority diseases. The jointactivity demonstrates how IDSRcan link with targeted programssuch as GAVI to meet commongoals and objectives.
Participants from 22 countries in Africa attended the WHO-CDC JointWorkshop in Johannesburg, South Africa.

Table 1. Curriculum for WHO–CDC Joint Workshop, Johannesburg, South Africa, June 4-8, 2001
I D S U p d a t e B u l l e t i n • F A L L 2 0 0 1 P a g e 3
Learning Module Participants Learning Objectives Resources Provided to Participants
Countries Represented
StandardLaboratoryMethods forBacterialMeningitis,Cholera, andShigella
Establishment of a Hib PediatricBacterialMeningitisSurveillanceNetwork in theAfrican Region
• National public healthlaboratorians
• Laboratorians fromHib-PBM sentinel sites
• Clinicians and data managers from sentinel sites
• Data managers from sentinel sites
• National, sub-regional,and regional epidemiol-ogists and data man-agers
• Register specimens from suspected cases forlaboratory confirmation
• Perform standard methods for laboratoryconfirmation of bacterial meningitis, cholera,and shigella infection
• Report results to requestor and appropriateauthorities
• Identify children presenting with suspectedbacterial meningitis
• Register cases• Collect CSF for laboratory confirmation• Collect demographic and epidemiologic data
on patients • Collect indicators for quality of surveillance• Enter data into database and produce line lists• Report data to MoH, WHO/AFRO and partners• Advocate for new vaccines
• Support surveillance activities at sentinel sites• Analyze and interpret data• Report data• Review indicators
• Laboratorians fromHib-PBM sentinel sites
• Receive and register specimens• Send isolates to reference laboratory for
serotyping/grouping and susceptibility testing• Report results
• National publichealth laboratorians
• Support sentinel sites’ laboratory work• Ensure or facilitate serotyping/grouping
and susceptibility testing
• Manual: Laboratory Methods for theDiagnosis of Meningitis
• Manual: Laboratory Methods for theDiagnosis of Epidemic Dysentery andCholera
• Reagents for confirming bacterialmeningitis, cholera, and shigella
BotswanaBurundiEthiopiaEritreaThe GambiaGhanaKenyaLesothoMalawiMauritiusMozambiqueNamibiaNigeriaRwandaSouth AfricaSeychellesSierra LeoneSwazilandTanzaniaUgandaZambiaZimbabwe
• Manual: Hib-Paediatric BacterialMeningitis (Hib-PBM) SurveillanceNetwork Surveillance Manual
PARTICIPANTSKekitinwa AddyMekonnen AdmassuMercy Essel AhunCaroline Sekela AkimAbdulatif AliBeatrice C AmadiAli AmourGabriel M. AnabwaniTsighe AndebirhanGhirmay AndemichaelMtonga AnneOyenuga Oyebanji AnthonyGloria AsalaCornelia Afi AtsyorMamadou Malifa BaldeRobin BiellikN.I BikitshaLeon A.A. BiscornetOdipio John BoscoEmilio Isaac BuleFlywell E. ChintoloKennedy ChitalaOwen Chitsatso
CvandenberghPaul DazaNiyungeko DéogratiasThomas DhlaminiDudu DlaminiTagodoe DodjiFrancisco Paulo Dos SantosSeheye EmmanuelMohammed EndrisNellie Lloyd EvansMamodou FatajoTewolde G. FeshazionFilli Said FilliBarnabi Eusebio FumoIdrissa GamangaGuma GaspardHaile GherbregziabherNtombi P. GinindzaPhanuel HabimanaClare HamerMariatu JawandoEsnath KabengulaFestus M. KalokolaAkapaka Kalu
KandekeLoise Wandia KariukiAgnes KatsulukutaDaniel KerteszKetshabile KhonaOmar Juma KiduaErica KufaRosamund LewisLindiwe B. MadondoYussuf Hasi MakameDouglas M. MakewaKalifa MannehExevia MazaruraEshetu MesseretPascal MkandaJose MondlaneMotloheloa MotloheloaTshegohaco MotsemmeViola P. MsangiMuhirwaVictor MumbaMary MunyoroRosemary MukasaReuben MwendaMuganga Narcisse
K.J. NathooJulius Mwangi NdegwaWedu NdebeleNdihokubwayoAlemayehu NegatiAdelard NgabonzizaAlpha NjieMudzanani NthambeleniLeiviavia NunesLoveness NyirendaGrace N. OkoloJohn OnephillipsMargaret B. Quist-ThersonMitula PamelaLouis Anthony PaulineZitsamele Coddy ReneLona Awo RennerIsabel Maria da S. RuasMohamed SamaiAlhassan L. SeisayPhilile ShabanguElizabeth Ndafetwa ShipikiLinda Sikakwa
Bornwell SikateyoStanley SonoiyaMankapr B TholleyGotteried UaakaMudhokwani R.Webster
FACILITATORSCDCCheryl BoppBradford Kay (CDC/AFRO)Leslye LaClaireMac Otten (CDC/AFRO)Tanja PopovicSusanna SchminkMontse Soriano-GabarroJoy Wells
SAIMR1
Lorraine ArntzenHeather Crewe-BrownJohn FreanLinda DeGouvieaAnne von GottbergRobin Huebner
Karen KeddyTersia KrugerMarshagne SmithArvinda SookaAvril Wasas
WHO/HQMax HardimanChris NelsonPem NamgyalJay Wegner
WHO/AFROBrehima KoumareTarande ManzilaBekithemba MhlangaBernad NtsamaKeith ShabaIsaac Wamola
GAVI2
Rick Spiegel
LSHTM3
Norman Noah
Participants and Facilitators of WHO–CDC Joint Workshop
1South African Institute for Medical Research 2 Global Alliance for Vaccines and Immunization 3 London School of Hygiene and Tropical Medicine
I D S U p d a t e B u l l e t i n • F A L L 2 0 0 1 P a g e 4
The World Health Organization (WHO),in collaboration with CDC and theMinistries of Health, has developed aframework for supporting countries tostrengthen national surveillance andresponse. This system is based on anintegrated or multidisease approach.
The African Regional Office (AFRO)adopted the use of an integratedapproach in1998. This strategy aims atbuilding national surveillance andresponse systems that provide reliableand timely information on the occurrenceof priority communicable diseases. Suchinformation is critical for early detection,confirmation and timely response to out-breaks. It is also essential for priority set-ting, planning, resource mobilization andallocation, and monitoring and evalua-tion of public health interventions.
In addition to AFRO, other WHO regionsare piloting and implementing thisapproach. During the WHO Global
Meeting on Communicable DiseaseSurveillance and Monitoring in Cairo inJanuary 2001, multidisease surveillancewas approved by all regions. Withinthis paradigm, WHO Headquarters andthe Regional Offices, in collaborationwith donors and technical partners, sup-port Member States in building nationalcapacity for surveillance and response.This support involves system reviews,and support for field epidemiology,training and laboratory strengthening.Such support is reinforced through theprovision of standards and guidelines,tools (e.g., health mapping) and disease-specific interventions.
An example of this concerted support tomultidisease surveillance and response isthe elaboration of Technical Guidelinesfor Integrated Disease Surveillance andResponse in the African Region devel-oped by WHO/AFRO, in close collabo-ration with CDC. This set of generic
recommendations describes the implemen-tation of surveillance and response at eachlevel of the health system. Other achieve-ments include the following:
• harmonized integrated data collection,dissemination and reporting system(CISID) in the European Regional Office,
• integrated Early Warning and ResponseNetwork (EWARN) in South Sudan,Eastern Mediterranean Regional Office,
• Mekong Basin Multidisease SurveillanceNetwork of the South East Asia RegionalOffice and Western Pacific RegionalOffice, and
• Field Epidemiology Training Programsof Pan American Health Organization.
WHO and partners endorse the documenta-tion, sharing, dissemination and use of theseexperiences. The lessons learned, chal-lenges and successes from various WHOregions and countries foster global surveil-lance and ensure global health security.
Perspective from WHO Headquarters
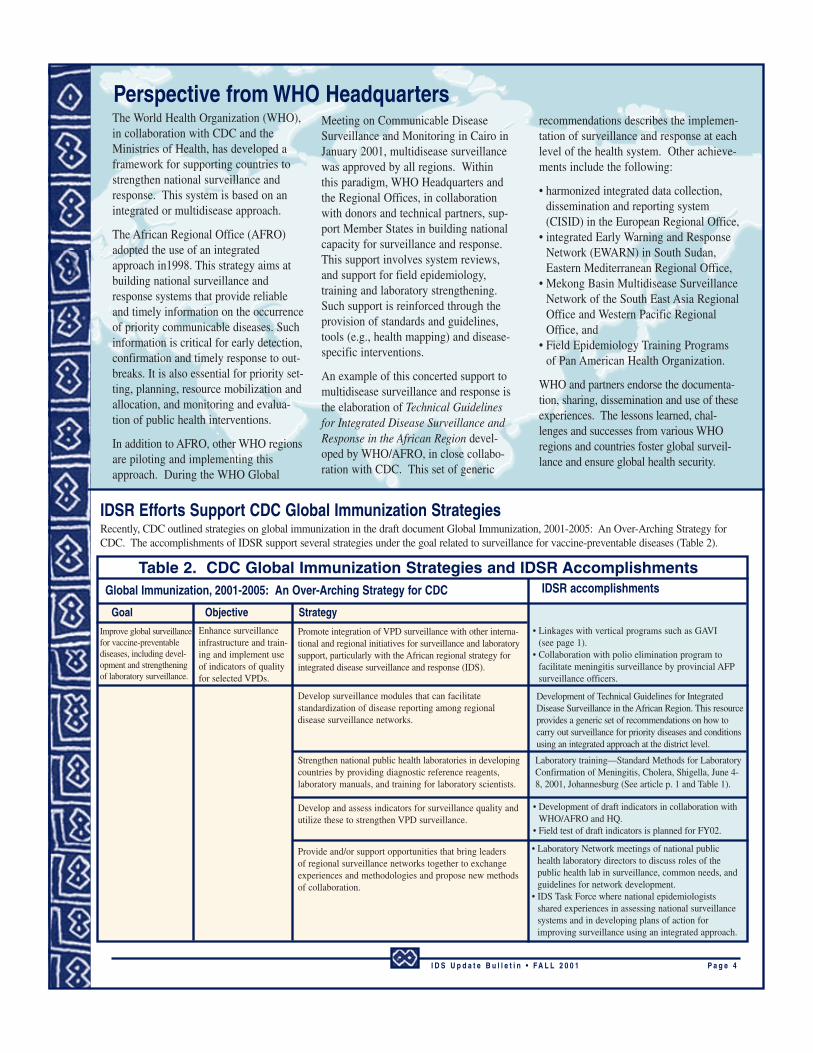
Table 2. CDC Global Immunization Strategies and IDSR AccomplishmentsGlobal Immunization, 2001-2005: An Over-Arching Strategy for CDC
Improve global surveillancefor vaccine-preventablediseases, including devel-opment and strengtheningof laboratory surveillance.
Goal Objective Strategy
Enhance surveillanceinfrastructure and train-ing and implement useof indicators of qualityfor selected VPDs.
Promote integration of VPD surveillance with other interna-tional and regional initiatives for surveillance and laboratorysupport, particularly with the African regional strategy forintegrated disease surveillance and response (IDS).
• Linkages with vertical programs such as GAVI(see page 1).
• Collaboration with polio elimination program tofacilitate meningitis surveillance by provincial AFPsurveillance officers.
Develop surveillance modules that can facilitate standardization of disease reporting among regional disease surveillance networks.
Development of Technical Guidelines for IntegratedDisease Surveillance in the African Region. This resourceprovides a generic set of recommendations on how tocarry out surveillance for priority diseases and conditionsusing an integrated approach at the district level.
Strengthen national public health laboratories in developingcountries by providing diagnostic reference reagents, laboratory manuals, and training for laboratory scientists.
Laboratory training—Standard Methods for LaboratoryConfirmation of Meningitis, Cholera, Shigella, June 4-8, 2001, Johannesburg (See article p. 1 and Table 1).
• Development of draft indicators in collaboration withWHO/AFRO and HQ.
• Field test of draft indicators is planned for FY02.
Develop and assess indicators for surveillance quality andutilize these to strengthen VPD surveillance.
Provide and/or support opportunities that bring leaders of regional surveillance networks together to exchangeexperiences and methodologies and propose new methodsof collaboration.
• Laboratory Network meetings of national publichealth laboratory directors to discuss roles of thepublic health lab in surveillance, common needs, andguidelines for network development.
• IDS Task Force where national epidemiologistsshared experiences in assessing national surveillancesystems and in developing plans of action forimproving surveillance using an integrated approach.
IDSR accomplishments
IDSR Efforts Support CDC Global Immunization StrategiesRecently, CDC outlined strategies on global immunization in the draft document Global Immunization, 2001-2005: An Over-Arching Strategy forCDC. The accomplishments of IDSR support several strategies under the goal related to surveillance for vaccine-preventable diseases (Table 2).

Publications and WebsitesCDC. Notice to Readers: Fever, jaundice, and multiple organ system failure associated with 17D-derived yellow fever vacci-nation, 1996—2001. MMWR 2001; 50(30);643-5.
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5030a3.htm
CDC. Notice to Readers: Publication of updated guidelines for evaluating public health surveillance systems. MMWR 2001;50(30);646.
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5030a5.htm
Lewis, R, Nathan, N, Diarra, L, Belanger, F, Paquet, C. Timely detection of meningococcal meningitisepidemics in Africa. Lancet, 2001;358(9278):287-293.
http://www.thelancet.com/journal/vol/iss/full/llan.358.9278.original_research.17005.1
Perkins, B. Prospects for prevention of meningococcal meningitis. Lancet 2001;358(9278):255-6.http://www.thelancet.com/journal/vol/iss/full/llan.358.9278.editorial_and_review.17017.1
United States General Accounting Office. Global Health: Challenges in improving infectious disease surveillance systems. GAO-01-722, August 31.
www.gao.gov under GAO Reports
IDS/Health Information Bulletin, WHO Country Office for Uganda, no. 2, September 2001.soon to be available at http://www.cdc.gov/epo/dih/idsafrica.html
I D S U p d a t e B u l l e t i n • F A L L 2 0 0 1 P a g e 5
WHO/AFROWondi Alemu
Peter Gaturuku
Antoine Kabore
Paul Lusamba-Dikassa
Mac Otten
Louis Ouedraogo
Idrissa Sow
WHO/HQStella Chungong
Guenael Rodier
Mike Ryan
Kathy Roth
CDC IDS TeamJudy Berry
Kathy Cavallaro
Bassam Jarrar
Bradford Kay
Sharon McDonnell
Peter Nsubuga
Bradley A. Perkins
Helen Perry
Nancy Rosenstein
Montse Soriano-Gabarro
USAIDConnie Davis
Mary Harvey
Hope Sukin
Murray Trostle
UN Foundation
Ministries of Health
African countries
IDS Teams
May 24-25 Joint Review and Planning Meeting on UNF Project: Strengthening Surveillance andControl of Vaccine Preventable and Epidemic Prone Diseases. Harare, Zimbabwe.
May 28-30 2nd Integrated Disease Surveillance and Response Task Force Meeting. Sponsoredby WHO/AFRO. Harare, Zimbabwe.
May 31- June 5 1st African Regional Conference, Training Programs in Epidemiology and PublicHealth Interventions Network (TEHPINET). Harare, Zimbabwe.
June 4-8 Joint WHO-CDC Workshop. Johannesburg, South Africa.• Standard Laboratory Methods for Diagnosis of Bacterial Meningitis, Cholera, and
Shigella• Workshop for the Establishment of a Haemophilus influenzae type B Pediatric
Bacterial Meningitis (Hib-PBM) Surveillance Network in the African Region
June 10-15 Assessment of National Surveillance System. Mozambique.
July 2 Interagency Coordination and Planning Meeting for IDSR. Accra, Ghana.
July 16-20 IDSR Plan of Action Workshop. Conakry, Guinée.
July 11 Planning meeting of USAID, PHR Plus, The CHANGE Project, and CDC to plan jointactivities for working with MoH Tanzania in the implementation of the MoH's workplan for Integrated Disease Surveillance and Response. Washington, DC.
October 1-3 Interagency Coordination and Planning Meeting for IDSR. Sponsored by MoH Mali,WHO, CDC. Bamako, Mali.
October 1-5 WHO-CDC Workshop. Johannesburg, South Africa.• Standard Laboratory Methods for Diagnosis of Plague
November 5-9 Joint WHO-CDC Workshop. Johannesburg, South Africa.• Standard Laboratory Methods for Diagnosis of Bacterial Meningitis,
Cholera, and Shigella• Workshop for the Establishment of a Haemophilus influenzae type B Pediatric
Bacterial Meningitis Surveillance Network in the African Region
December 3-7 Task Force on Immunization. Sponsored by WHO/AFRO. Addis Ababa, Ethiopia.
Calendar of Events