identification of intrarenal fibrin deposition · identification ofintrarenalfibrin deposition fig....
TRANSCRIPT

J. clin. Path., 1973, 26, 102-112
Identification of intrarenal fibrin depositionA. M. DAVISON, D. THOMSON, MARY K. MACDONALD, J. K. RAE,W. S. UTTLEY, AND A. R. CLARKSON
From the Department ofPathology, University of Edinburgh, the Royal Hospital for Sick Children,Edinburgh, and the Medical Renal Unit, Department of Medicine, Royal Infirmary, Edinburgh
SYNOPSIS The site and extent of intrarenal fibrin deposition has been examined by routine histo-logical staining, immunofluorescence, and electron microscopy in 109 patients with a wide varietyof renal diseases. The findings have been correlated with the amount of urinary fibrin/fibrinogendegradation product (FDP) excretion as measured by the tanned red cell haemagglutination in-hibition immunoassay. The results show that routine histological stains (Martius Scarlet Blue andPicro Mallory) are unreliable, particularly where there is mesangial accumulation of material or
where the amount of fibrin deposited is small and confined to a subendothelial position. Similarly theelectron -microscope may overassess the degree of fibrin deposition, particularly if this is associatedwith the deposition of immunoglobulins and complement. There is a close relationship between thesite and extent of fibrin, as detected by immunofluorescence, and the maximal urinary FDP excretion.
The role of intravascular coagulation in both experi-mental (Vassalli, Simon, and Rouiller, 1963) andhuman (McCluskey, Vassalli, Gallo, and Baldwin,1966) renal diseases has recently attracted muchattention. Lendrum, Fraser, Slidders, and Henderson(1962) described histological methods for stainingfibrin of varying age and since then the techniques ofimmunofluorescence and electron microscopy havebeen applied to the assessment of fibrin deposition.It is thus important to determine the accuracy,limitations, and value of the methods currentlyavailable for the detection of fibrin in renal biopsymaterial.
In this study of human renal biopsies a compari-son has been made between the detection of fibrin/fibrinogen by immunofluorescence and the assess-ment of fibrin deposition as observed with routinelyused histological fibrin stains and by electronmicroscopy. These results have been correlated withthe urinary fibrin/fibrinogen degradation product(FDP) excretion.
Methods
Percutaneous renal biopsy was performed on 109unselected patients, adults and children, with variousrenal diseases of both immunological and non-immunological origin (Table I). The extent anddistribution of fibrin as determined by routine
Received for publication 19 December 1972.
Proliferative glomerulonephritisMembranous glomerulonephritis.Mesangiocapillary glomerulonephritisDiabetic glomerulosclerosis.Polyarteritis.Acute tubular necrosisMinimal lesion glomerulonephritisRenal amyloidosisDiffuse intravascular coagulation.Systemic lupus erythematosusScleroderma.Partial lipodystrophy.Essential hypertensionLeptospirosis canicola, toxaemia of pregnancy, subacute bacterialendocarditis, Bartter's syndrome, Henoch-Schonlein purpura,pyelonephritis, mesangial IgG/IgA disease, malignancy-associatednephroticsyndrome.
54458554432223
8
Table I Histological diagnosis ofpatients studied
histological stains, electron microscopy, and im-munofluorescence microscopy was assessed by threeindependent observers. The assessments were madewithout knowledge of a histological or clinical diag-nosis and the results compared one with the otheronly on completion of the study. Further, a compari-son was made of the extent and distribution ofintrarenal fibrin estimated by each method with theurinary excretion of FDP measured before and afterthe biopsy by two other independent investigators.
HISTOLOGICAL STAININGTissue was fixed in corrosive formol for 18 to 24hours, sectioned at 2,u, and stained by the Picro-Mallory V (PM) method employing acid Fuchsin
102
copyright. on A
pril 26, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.26.2.102 on 1 F
ebruary 1973. Dow
nloaded from

Identification of intrarenal fibrin deposition
Fig. 1 Between glomerular capillary basement membrane and endothelium lies a rarefied layer in which thin fibrilsare seen. Electron microscopic grade +. x 30 000
(Acid Violet 19)1 and the Martius Scarlet Blue (MSB)method employing Brilliant Crystal Scarlet 6R (AcidRed 44)2 of Lendrum et al (1962).The distribution of red staining was recorded on
the following scale: 0, no positive material; +,positive material in fewer than half of the glomeruli;1Hopkin and Williams, Chadwell Heath, Essex.2L. B. Holliday, Huddersfield, England.
+ +, positive material in more than half of theglomeruli, and + + +, large depositis of positivematerial in glomeruli and also frequently in bloodvessels.
Biopsies containing fewer than six glomeruli werenot included in the study. Adequate material stainedby MSB was obtained in 100 cases and by PM in 77cases.
103
copyright. on A
pril 26, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.26.2.102 on 1 F
ebruary 1973. Dow
nloaded from

104 A. M. Davison, D. Thomson, Mary K. MacDonald, J. K. Rae, W. S. Uttley, and A. R. ClarAkson
Fig. 2 Deposits ofgranular and fibrillar material, apparently continuous with the basement membrane, lie betweenmembrane and endothelium, sometimes invaginating into the endothelium. Electron microscopic grade + --. 16 000
ELECTRON MISCROSCOPYTissue was fixed in 1 0 osmium tetroxide, sometimeswith preliminary glutaraldehyde fixation, dehydratedin graded alcohols and embedded in Araldite.Sections were cut on a Porter Blum MT2 ultratomeat 50 nm, stained with lead citrate and uranyl acetate,and viewed in an AEI EM. 6 electron microscope.The amount of fibrin deposited in a single glome-
rulus in 87 cases was assessed on the following scale:
0, no abnormal deposits; + a rarefied layer betweenthe basement membrane and the endotheliumcontaining strands of osmiophilic material (Fig. I);+ + the presence, in addition, of definite focaldeposits of dark, fibrillar, or granular materialbetween the basement membrane and the endo-thelium, these often showing apparent continuitywith the basement membrane (Fig. 2); + + + similarbut more abundant material sometimes present also
copyright. on A
pril 26, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.26.2.102 on 1 F
ebruary 1973. Dow
nloaded from

Identification of intrarenal fibrin deposition
Fig. 3 The subendothelial deposits are more abundant than in Fig. 2, and are associated with reaction of themesangial cytoplasm, which can be seen here between basement membrane and endothelium. The deposited materialis in contact with the lumen through the fenestrae. Electron microscopic grade + + +. x 12 000
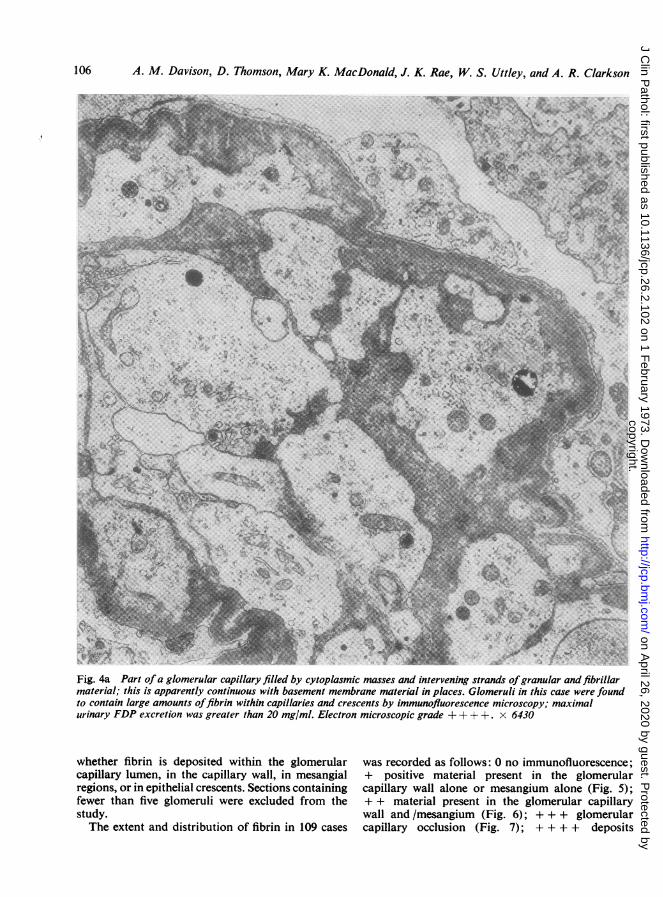
in the capillary lumen and often associated with amesangial reaction (Fig. 3); + + + + completeocclusion of the glomerular capillary lumen bythrombus (Fig. 4a).
IMMUNOFLUORESCENCE MICROSCOPYFresh tissue was 'snap-frozen' with Drikold andsectioned at 2 to 3u in a cryostat. After fixation with
950% alcohol for 10 min, sections were incubatedwith fluorescein isothiocyanate conjugated (FITC)antihuman fibrin/fibrinogen serum (Hoechst) for30 min in a dark, moist chamber at room tempera-ture. Additional sections were incubated with FITCconjugated antisera to IgG, IgM, IgA, and comple-ment (C3).
Using this technique it is possible to decide
105
copyright. on A
pril 26, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.26.2.102 on 1 F
ebruary 1973. Dow
nloaded from
106 A. M. Davison, D. Thomson, Mary K. MacDonald, J. K. Rae, W. S. Uttley, and A. R. Clarkson
1.
Fig. 4a Part ofa glomerular capillary filled by cytoplasmic masses and intervening strands ofgranular and fibrillarmaterial; this is apparently continuous with basement membrane material in places. Glomeruli in this case were foundto contain large amounts offibrin within capillaries and crescents by immunofluorescence microscopy; maximalurinary FDP excretion was greater than 20 mg/ml. Electron microscopic grade + + + +. x 6430
whether fibrin is deposited within the glomerular was recorded as follows: 0 no immunofluorescence;capillary lumen, in the capillary wall, in mesangial + positive material present in the glomerularregions, or in epithelial crescents. Sections containing capillary wall alone or mesangium alone (Fig. 5);fewer than five glomeruli were excluded from the + + material present in the glomerular capillarystudy. wall and /mesangium (Fig. 6); +++ glomerularThe extent and distribution of fibrin in 109 cases capillary occlusion (Fig. 7); + + + + deposits
copyright. on A
pril 26, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.26.2.102 on 1 F
ebruary 1973. Dow
nloaded from

Identification of intrarenal fibrin deposition
Fig. 4b The appearances are similar to Figure 4a. The glomerular capillary lumen contains granular and fibrillarmaterial lying between cytoplasmic masses and in some foci this appears continuous with the basement membrane.By immunofluorescence microscopy the glomeruli contained a large amount of IgG, IgM, and complement (C) butonly small amounts offibrin/fibrinogen; maximal urinary FDP excretion was in the range of2 to 5 mg/ml. x 7500
within glomeruli and elsewhere such as epithelial products (FDP) in the urine was measured in 94crescents, interstitial spaces, or intertubular blood patients by the tanned red cell haemagglutinationvessels (Fig. 8). inhibition immunoassay (Merskey, Kleiner, and
Johnson 1966; Das, 1970), as modified for urineURINARY FIBRIN/FIBRINOGEN DEGRADATION (Clarkson, Morton, and Cash, 1970) employingPRODUCTS commercially obtained human fibrin/fibrinogenThe concentration of fibrin/fibrinogen degradation antiserum (Hoechst). Consecutive early morning
107
copyright. on A
pril 26, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.26.2.102 on 1 F
ebruary 1973. Dow
nloaded from

108 A. M. Davison, D. Thomson, Mary K. MacDonald, J. K. Rae, W. S. Uttley, and A. R. Clarkson
Fig. 5 Deposition offibrin/fibrinogen within capillary Fig. 6 Fibrin/.fibrinogen within the capillary walls andwalls in a patient with proliferative glomerulonephritis. mesangial regions of a patient with proliferative glom-Immunofluorescence grade +. x 400 erulonephritis. Immunofluorescence grade + +. x 400
urine samples collected for periods between threeand 25 days before renal biopsy and between fourand 150 days after biopsy were assayed and theresults expressed in micrograms of fibrinogenequivalent per millilitre of urine. Maximum valuesobtained were compared with the results of thehistological, immunofluorescence, and electronmicroscopic study.Due to technical difficulties, such as inadequate
biopsy material, all five possible investigations were
performed in only 46 patients; 43 patients had fourinvestigations, 15 had three, and five patients had two.
Results
ROUTINE HISTOLOGICAL STAINING
Table II shows the histological grading as estimatedby 'fibrin stains' compared with the immunofluo-rescence microscopy grading employing specificFITC antihuman fibrin/fibrinogen serum. MSB-positive material was present in only 24 of 62 sections
in which fibrin was detected by immunofluorescence,and in nine of 36 sections in which there was no
specific immunofluorescence.Examples of positive immunofluorescence with
negative MSB staining were found in all histologicalgroups. Negative immunofluorescence and positiveMSB staining occurred in glomerulonephritis,amyloidosis, and diabetic glomerulosclerosis whenthere was predominant mesangial accumulation of
Immuno- Martius-Scarlet-Blue Picro-Malloryfluorescence -
0 + + + +++ 0 + ++ ++±
0 27 6 3 19 3 3+ 20 6 3 15 3 4++ 9 5 1 4 6 1+++ 5 2 1 2 3 1 1-±-++++ 4 4 2 5 2 2
Table If Detection offibrin by immunofluorescencemicroscopy and histological staining''See methods for details of grading
copyright. on A
pril 26, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.26.2.102 on 1 F
ebruary 1973. Dow
nloaded from

Identification of intrarenal fibrin deposition
Fig. 7 Glomerular capillary occlusion with fibrinl Fig. 8 Fibrin/fibrinogen within glomerular capillaryfibrinogen thrombi in a patient with malignancy- walls and also peritubular capillaries in a patient withassociated nephrotic syndrome. Immunofluorescence haemolytic uraemic syndrome. Immunofluorescence gradegrade + + +. x 250 + 4- + +. x 400
material. Similar results were obtained with PMstaining.
Table III shows the electron microscopic gradingcompared with the presence of positively stainingmaterial by routine 'fibrin stains'. The resultsobtained were essentially similar to those obtainedwith immunofluorescence except that there werefewer cases with positive histological staining in the
EM grading Martius-Scarlet-Blue Picro-Mallory
0 + +±+ +±+-+ 0 + ++-F +++
0 6 2 4 1 1+ 14 5 12 3++ 17 2 12 2 2++-+ 13 7 2 8 10 2+±+++ 4 5 1 2 2 2
Table IfI Electron microscopic grading offibrin andhistological staining''See methods for details of grading
absence of electron microscopic detection of fibrin.Material positive with MSB was present in one caseof acute renal failure and one of amyloidosis in whichno fibrin was detected by electron microscopy; PM-positive material was present in one case of resolvingproliferative glomerulonephritis and one of amyloid-osis in which no fibrin was detected by electronmicroscopy.
There were 73 cases with both adequate MSB andPM staining. In 53 cases there was concordancebetween these two methods, while in 12 there waspositive staining by PM only and eight were positiveby MSB only.
ELECTRON MICROSCOPYTable III shows the electron microscopic gradingcompared with MSB and PM staining.
Table IV shows the electron microscopic assess-ment compared with the maximum urinary FDPexcretion. The correlation between these two
109
copyright. on A
pril 26, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.26.2.102 on 1 F
ebruary 1973. Dow
nloaded from

110 A. M. Davison, D. Thomson, Mary K. MacDonald, J. K. Rae, W. S. Uttley, and A. R. Clarkson
Glomerular Maximum Urine FDP Concentration (iAg/ml)FibrinElectron 0-1 1-2 2-5 5-10 10-20 > 20MicroscopicGrading
0 6 2 1+ 5 4 6 1 1++ 5 3 2 2 1 2+++ 3 2 1 4 3 4++++ 1 1 6 1 2
Table IV Relation between urinary fibrin/fibrinogendegradation products and extent of intraglomerular fibrindeposition as judged by electron microscopy (69 patients)'
'See methods for details of grading
measurements is good (p < 0O001) but with a slighttendency towards overassessment by electronmicroscopy, eg, eight patients were considered as+ + + + by electron microscopy but had a urinaryFDP concentration of 5 ,ug/ml or less. In thesepatients fibrin was present, but in no case was itassessed as greater than + + by immunofluorescence.In addition these patients had considerable depositsof jmmunoglobulin, particularly IgG and IgM, andcomplement (C3) (Fig. 4b). The histological diagno-sis of these patients was proliferative glomerulone-phritis in six and mesangiocapillary glomerulone-phritis in one; one patient had clinical partiallipodystrophy. Of the two patients with high urinaryFDP concentration but little electron microscopicevidence of fibrin deposition, one had acute tubularnecrosis (urine FDP 5-10 ,ug/ml; EM grading 0) andthe other had a mild proliferative glomerulonephritis(urine FDP > 20 ,ug/ml; EM grading +).
Table V shows the relationship between theelectron microscopy and the immunofluorescencefindings. There is a wide distribution, again withevidence of overassessment by electron microscopy.Twelve patients graded as + + or greater byEM hadno fibrin detectable by immunofluorescence; thehistological diagnosis of this group was diabetesmellitus (5), proliferative glomerulonephritis (3),membranous glomerulonephritis (2), polyarteritis (1),
Immuno- Electron Microscopic Grading'fluorescence
0 + ++ +++ ++++
0 8 7 6 5 1+ 1 8 8 5 4++ 2 2 3 4 5++1+ 1 5 1
++++ 1 2 5
Table V Detection offibrin by immunofluorescencemicroscopy and electron microscopy (86 patients)"See methods for details of grading
and scleroderma (1). Only four of this group, twomembranous, one polyarteritis, and one focalproliferative, showed any evidence of immuno-globulin deposition, but in all four the presence ofIgM could be demonstrated. Nine patients were
graded + + + + by electron microscopy but showedonly + or + + fibrin deposition by immuno-fluorescence; seven of these had proliferativeglomerulonephritis, one mesangiocapillary glomeru-lonephritis, and one partial lipodystrophy. However,in all the presence of IgG could be shown, IgM ineight and complement (C3) in seven.
IMMUNOFLUORESCENCE MICROSCOPYTable VI shows the immunofluorescence grading ofintrarenal fibrin deposition and the maximumurinary FDP concentration. The relationship be-tween these two methods is highly significant(P < 0-001). Two patients with an immunofluore-scence rating of + + and with a urinary FDP con-centration of 0 to 1 ,tg/ml were receiving therapy,one with corticosteroids and one with indomethacin.One patient with a urinary FDP concentration of5 to 10 ,ug/ml and no immunofluorescence for fibrinhad acute renal failure due to infection with Lepto-spirosis canicola.
Fibrin/ Maximum Urine FDP Concentration (Mg/mi)'FibrinogenImmuno- 0-1 1-2 2-5 5-10 10-20 >20fluorescence
0 20 8 1 1+ 9 6 7 1 2++ 2 9 3+++ 1 3 3 2++++ 2 3 6
Table VI Relation between urinary fibrin/fibrinogendegradation products and immunofluorescence to fibrinlfibrinogen (88 patients)
'See methods for details of grading
Table II compares the immunofluorescence findingswith routine histological stains. Table V shows theimmunofluorescence findings compared with theelectron microscopic grading.
URINARY FDPTable VI compares the maximal urinary FDPconcentration with the immunofluorescence findings.The most consistently elevated values were foundwhere fibrin was seen in extraglomerular positions,ie, within crescents, interstitium, blood vessels, ortubules. In all patients with glomerular capillarydeposition of fibrin the abnormal FDP excretion wascyclical, with varying intervals of minimal excretion
copyright. on A
pril 26, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.26.2.102 on 1 F
ebruary 1973. Dow
nloaded from

Identification of intrarenal fibrin deposition
between periods of more marked abnormality(two to 25 days). This was most apparent in patientswith proliferative glomerulonephritis.
Table IV shows the maximal urinary FDP con-centration compared with the electron microscopyfindings.
Discussion
The intravascular deposition of fibrin is a dynamicprocess beginning with the alteration of fibrinogenby thrombin, progressing to the formation of fibrin,and eventually to the production of various degra-dation products. It would seem unlikely, therefore,that the presently available routine histologicalstains would have an equal affinity for the widevariety of forms through which fibrin passes. In thisstudy we have found a poor relationship betweenhistological stains and the immunofluorescentdetection of fibrin, though this may be due to someextent to the fact that we have not carried out theprolonged fixation for two to three weeks in aqueousmercuric chloride or the degreasing recommendedby Lendrum and his coworkers (1962). We omittedthese steps because (1) the quantity of material weemployed, obtained by needle biopsy, was small andtherefore fixed readily, and (2) in most instances theclinical necessity for diagnosis merited more rapidprocessing. False positive histological results occurin diseases where there is predominantly mesangialaccumulation of material while the lack of immuno-logical characteristics of fibrin could be due to thedestruction of antigenic sites on the fibrin moleculefollowing phagocytosis by the mesangial cell; it isprobable that the accumulated material actuallycontains little or no fibrin. False negative results mayoccur because of different sensitivities of the methodsemployed; it is unlikely that histological stains candetect small amounts of fibrin deposited in a sub-endothelial position as seen in grade + by electronmicroscopy or grade + by immunofluorescencemicroscopy. As in most renal diseases continuationof the coagulation process occurs until remission,spontaneous or drug induced, all stages of fibrinformation and removal are likely to be found. Thusthe use of dyes which predominantly stain early orlate fibrin is likely to be of little value, although it didseem that the early staining PM possessed a closerrelationship to immunofluorescence microscopy thanMSB.For years it was believed that the detection of
fibrin by electron microscopy was dependent uponobserving fibrillar material with a characteristicperiodicity of approximately 200 A. However, it hasbeen shown that fibrin may not have this characteris-tic appearance. In addition, although fibrin and the
111
largest of the degradation products may exist asfilamentous fibres with characteristic periodicity, theother intermediate and end products appear asrudimentary fibrils or amorphous granular structures.This leads to difficulty in the interpretation ofelectron micrographs; in the present study there is areasonable relationship between the identification offibrin by the electron microscope and the excretionof FDP in the urine, but there is a tendency to over-diagnosefibrin byelectron microscopycompared withidentification by immunofluorescence microscopy,and this is probably explained by the similar appear-ance of certain products of fibrin formation anddegradation and of other protein deposits. This wasconfirmed by finding considerable deposits ofimmunoglobulins and complement in those biopsiesscored as + + or greater by electron microscopy andcontaining FDP in the urine of less than 5 /g/ml(Figs. 4a and b). In addition, of the eight patientswithdiabetes mellitus five were graded as + + or greaterby electron microscopy, but showed no specificimmunofluorescence. With the currently availabletechniques, the electron microscope cannot clearlydistinguish the exact nature of protein deposits;certain features such as the apparent continuity ofdeposits with the basement membrane and thepresence of a rarefied and slightly fibrillar sub-endothelial layer suggest that the material present isfibrin, but definite identification is not possiblewithout typical periodicity.The immunofluorescence microscopy grading of
fibrin deposits is not strictly comparable with theelectron microscopic assessment. However, itprobably represents a more accurate estimation ofthe distribution of intrarenal fibrin, since it is possibleto visualize several glomeruli and other importantstructures such as blood vessels. Immunofluorescencegrading depends more on distribution than on aquantitative assessment. This is necessarily so asmethods of immunofluorescence microscopy quan-titation on tissue sections are difficult, time con-suming, and unlikely to reveal much additionalinformation when employed on a routine basis.There is a very close agreement between the fibrin
distribution as assessed by immunofluorescence andthe maximal excretion ofFDP in the urine. Where thefibrin deposits were confined to the glomerulus andpresent only in the capillary wall or mesangium,there was a slight increase in urine FDP excretion.This was presumably due to a limited activation ofthe coagulation system with adequate removal bylysis and phagocytosis. However, where fibrin wasdetected occluding the capillary lumen, in epithelialcrescents, or in peritubular capillaries, urinary FDPconcentrations were considerably increased. Mostpatients in this group were found to have progressive
copyright. on A
pril 26, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.26.2.102 on 1 F
ebruary 1973. Dow
nloaded from

112 A. M. Davison, D. Thomson, Mary K. MacDonald, J. K. Rae, W. S. Uttley, and A. R. Clarkson
proliferative glomerulonephritis or acute ischaemicrenal failure. Since the urinary excretion of FDP isepisodic in many cases of proliferative glomerulone-phritis, it is important to measure daily urineconcentrations for up to 25 days to ensure thatpositive cases are not missed. The serial measurementof urinary FDP provides a good method of followingthe state of intrarenal fibrin deposition and thereforethe natural history or response to therapy of the basicpathological process.
This study therefore confirms the involvement ofthe coagulation system in a wide variety of renaldiseases. It has demonstrated the limitations of theroutine histological stains and of electron microscopyin assessing the degree of fibrin deposition in renalbiopsy specimens. The close relationship between theintrarenal fibrin as detected by specific immuno-fluorescence and the maximum urinary FDP excre-
tion confirms the value of the latter technique infollowing patients over considerable time intervals.In addition it suggests that the distribution of fibrin,as viewed by immunofluorescence, may be of more
significance than an estimate of the total amountdeposited.
We are grateful for the technical assistance of MissLeslie Taylor, Mr Robert Donaldson, Mr JamesBarclay, and Mrs Heather Maxwell.
Financial support has been given by the LawsonTait Medical and Scientific Trust, the Scottish Homeand Health Department and the Scottish HospitalEndowments Research Trust, the Winston ChurchillMemorial Trust of Australia, and the ResearchEndowment Fund of the Royal Hospital for SickChildren, Edinburgh.We wish to thank the many physicians under
whose care these patients were investigated. We aregrateful to Drs J. S. Robson and J. D. Cash foradvice and encouragement with this study.
References
Clarkson, A. R., Morton, J. B., and Cash, J. D. (I 970). Urinary fibrin,fibrinogen degradation products after renal homotranisplanta-tion. Lancet, 2, 1220-1223.
Das, P. C. (1970). Assay of seru:ei fibrin degradation products byagglutination-inhibition of coated erythrocytes. J. clin. Pat/i.,23, 299-303.
Lendrum, A. C., Fraser, D. S., Slidders, W., and Henderson, R. (1962).Studies on the character and staining of fibrin. J. clin. Path., 14,401-413.
McCluskey, R. T., Vassalli, P., Gallo, G., and Baldwin, D. S. (1966).An immunofluorescent study of pathogenic mechanisms inglomerular diseases. New Eng/. J. Ale(d., 274, 695-701.
Merskey, C., Kleiner, G. J., and Johnson, A. J. (1966). Quantitativeestimation of split products of fibrinogen in human serum,relation to diagnosis and treatment. Blood, 28, 1-18.
Vassalli, P., Simon, G., and Rouiller, C. (1963). Electron microscopicstudy of glomerular lesions resulting from intravascular fibrinformation. Anmer. J. Path., 43, 579-617.
copyright. on A
pril 26, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.26.2.102 on 1 F
ebruary 1973. Dow
nloaded from