icu acquired weakness (icuaw) and early rehabilitation
DESCRIPTION
TRANSCRIPT

ICU Acquired Weakness&
Early Rehabilitation
東京慈恵会医科大学附属病院麻酔科・集中治療部
福島東浩1
ICU Acquired Weakness(ICUAW)
2

• 1892 Osler: 'rapid loss of flesh' in prolonged sepsis.
The discovery of critical illness polyneuropathy.Bolton CF. Eur J Anaesthesiol Suppl. 2008;42:66-7
3

• 1961 Mertens: ‘coma-polyneuropathies’
• 1971 Henderson: polyneuropathy in patients with burns.
• 1977 MacFarlane: Severe myopathy after status asthmaticus.
The discovery of critical illness polyneuropathy.Bolton CF. Eur J Anaesthesiol Suppl. 2008;42:66-7
4
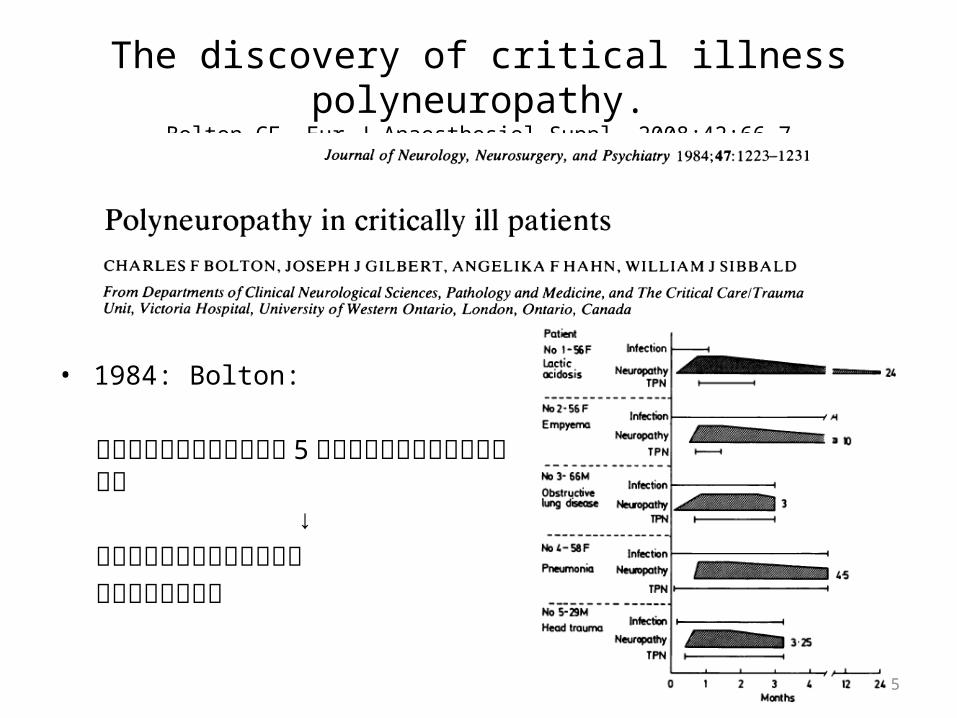
• 1984: Bolton:
呼吸器離脱困難の重症患者 5 症例について筋電図評価を報告
↓重症患者における筋力低下の病態生理を示した
The discovery of critical illness polyneuropathy.Bolton CF. Eur J Anaesthesiol Suppl. 2008;42:66-7
5

• 1996 Latronico:
敗血症,多臓器不全で深部腱反射消失を伴う麻痺が進行した 24 例筋電図,筋生検を施行
↓形態学的な病理変化から病態を説明
The discovery of critical illness polyneuropathy.Bolton CF. Eur J Anaesthesiol Suppl. 2008;42:66-7
Lancet. 1996 Jun 8;347(9015):1579-82.
6

CIPNM 発症のリスク因子検証Setting: Single center, Prospective observational study,1994. 3 – 1996. 6, St Elisabeth Hospital, Medical ICU, Tilburg Netherland, Methods/Patients: 4 日以上人工呼吸器管理された患者 98 人 Results: 32 人 (33%) が CINM と診断
Risk factors for the development of polyneuropathy and myopathy in critically ill patients.
de Letter MA, Schmitz PI, Visser LH,. Crit Care Med. 2001 Dec;29(12):2281-6.
P=0.04
APACH III 上がる毎にリスク上昇 SIRS でリスク上昇
7

ARDS 患者の Quality of Life を 1 年間調査
6 Minute Walking Distance : 281 m (3 month)
成人の平均 ; 500-630mSF-36: Physical Function; 35
成人の平均 ; 85( 全年齢 ), 88(45-55 歳 ), 59(≥75 歳 )
Physical Role; 0 (3 month) 成人の平均 ; 85( 全年齢 ), 84(45-54), 62(≥75 歳 )
CMAJ. 2000 Aug 8;163(3):265-71.
ARDS 患者の筋力低下 .
8
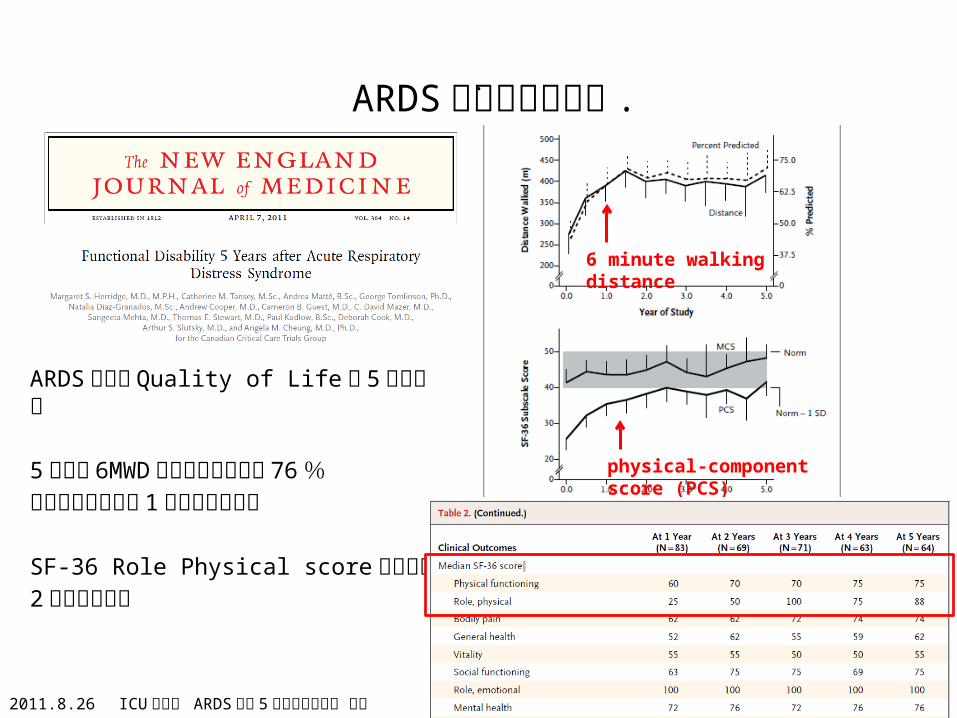
ARDS 患者の Quality of Life を 5 年間調査
5 年後の 6MWD の回復は予測値の 76 %それまで退院から 1 年半以上かかる
SF-36 Role Physical score の回復は2 年以上かかる
.
9
ARDS 患者の筋力低下 .
physical-component score (PCS)
6 minute walking distance
2011.8.26 ICU 勉強会 ARDS 発症 5 年後の機能障害 参照

• Bed rest
• Mechanical Ventilation
• Critical Illness Polyneuropathy and MyopathySepsis
ICU 筋力低下の主な原因
10

重症患者における筋力低下患者の呼称は混在Crit Care Med. 2009 Oct;37(10 Suppl):S299-308.
11

2009 年 9 月Round Table Conference in BrusselsJeans-Louis Vincent as conchairs
ICUAW の権威が一堂に会す
October 2009 - Volume 37 – SupplementICU-Acquired Weakness: Proceedings of a Round Table Conference in Brussels, Belgium, March 2009 10 12
臨床症状から定義
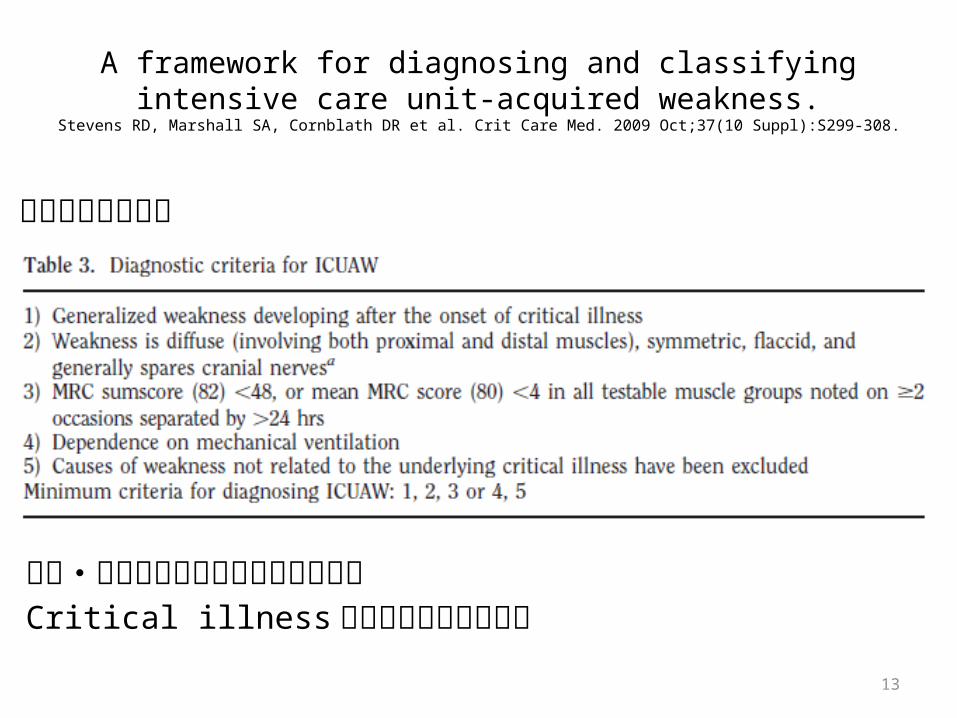
A framework for diagnosing and classifying intensive care unit-acquired weakness.
Stevens RD, Marshall SA, Cornblath DR et al. Crit Care Med. 2009 Oct;37(10 Suppl):S299-308.
神経・筋疾患の存在がないことが前提Critical illness に伴って起こったもの
13

• Bed rest
• Mechanical Ventilation
• Critical Illness Polyneuropathy and MyopathySepsis
14

Resistance exercise maintains skeletal muscle protein synthesis during bed rest.
Ferrando AA, Tipton KD, Bamman MM et al. J Appl Physiol. 1997 Mar;82(3):807-10.
成人ボランティアのベッド上での筋肉のたんぱく質合成を検証
Methods/Patients:成人ボランティア 11 人 (28±7 歳 )Bed rest 14daysBR (n=5): Bed restBREx (n=6): Bed rest + Resistance training終了後,筋生検施行し分析
Results:
BR 群で安静前より 46 %減少 (p<0.04)
15
BR
BREx
BREx
BR

Effect of 10 days of bed rest on skeletal muscle in healthy older adults.Kortebein P, Ferrando A, Lombeida J et al. JAMA. 2007 Apr 25;297(16):1772-4.
16
安静による筋力低下を検証対象 : 成人ボランティア ( 平均 67 歳 )
Results:窒素バランス : 安静後 6-10 日で安静前より減少 ( 生成 < 分解 ) (Figure)
安静後 10 日後 : 安静前に比べ , 筋肉の合成率は下がり , 筋肉はやせ , 筋力は低下する (Table)

• Bed rest
• Mechanical Ventilation
• Critical Illness Polyneuropathy and Myopathy
17

人工呼吸器による横隔膜の委縮を観察
脳死患者 (case): 脳死・臓器移植ドナー 14 人人工呼吸器 ; 18-69 時間
Control: 良性または限局した悪性の肺腫瘍手術患者 8人
術中に横隔膜生検人工呼吸器 ; 2-3 時間
Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans.
Levine S, Nguyen T, Taylor N et al. N Engl J Med. 2008 Mar 27;358(13):1327-35.
18
横断面の面積
2025±745 1878±589
4725±1547 3949±1805
Case 群の横隔膜で有意に萎縮を認める
57% 減少 (p=0.0001)
53% 減少 (p=0.01)

人工呼吸器管理された既往のある高齢者の機能予後を検証Design: Retrospective cohortSetting/Patients: 1996-2003, Medicare Current Beneficiary Survey のデータベース65 歳以上 , 入院中に人工呼吸管理 (MV) の有無でそれぞれ抽出Results退院後の ADL Modified Katz Activities of Daily Living Scale (ADL disability score)
With MV; 22.5 [18.8–26.2], without MV 15.3 [14.2–16.4] Rosow-Breslau Functional Health Scale (mobility difficulty score)
with MV; 46.2 [42.7–49.6], without MV 37.9 [36.8–39]
Disability among elderly survivors of mechanical ventilation.Barnato AE, Albert SM, Angus DC et al. Am J Respir Crit Care Med. 2011 Apr 15;183(8):1037-42.
19
ADL disability score
mobility difficulty score
人工呼吸あり
人工呼吸あり
人工呼吸なし
人工呼吸なし

• Bed rest
• Mechanical Ventilation
• Critical Illness Polyneuropathy and MyopathySepsis
20

A framework for diagnosing and classifying intensive care unit-acquired weakness.
Stevens RD, Marshall SA, Cornblath DR et al. Crit Care Med. 2009 Oct;37(10 Suppl):S299-308.
21

1a) Pathway to Nerve dysfunctionEndotoxin, Hyperglycemia,Inflammatory mediator….↓Blood nerve barrier の破綻↓Hypoperfusion and lack of oxygenEndoneural hyperkalemiaAcidemic metabolism↓Endoneural membrane depolarization
↓Nerve dysfunction
Critical Illness Polyneuropathy CIPN
Am J Respir Crit Care Med. 2013 Feb 1;187(3):238-46.
1b) Pathway to DenervationPassive uptake of glucose, Deficient scavenging,Compressive neuropathy due to atrophy↓Axon damageDistal loss of connection to muscle
22

2a) Pathway to muscle atrophy
Inactivity, Inflammation ↓
Muscle cell nuclei ↓Transcription
・ Proautophagy protein・ Atrogen-1, MuRF-1 ↓
・ Autophagy・ Ubiquitin - proteasome system(UPS) ↓
Loss of muscle (Proteolysis > Synthesis)
Critical Illness Myopathy CIM
Am J Respir Crit Care Med. 2013 Feb 1;187(3):238-46.
2b) Pathway to decreased force Inflammation
↓ Oxidative stressMitochondrial stress
Leaky (Ca release channel) → Excitation-Contraction Uncoupling Sodium channelopathy → Membrane Inexitability 23

病理組織 Lancet Neurol. 2011 Oct;10(10):931-41.
CIPN 患者の神経組織 ( 坐骨神経 )( 光学顕微鏡 , トルイジンブルー染色 )
軸索の変性によりミエリン線維の密度が小さくなっている
CIM 患者の筋組織(左 : 光学顕微鏡 H-E 染色 前脛骨筋 , 右 : 電子顕微鏡 大腿四頭筋 )
筋線維の壊死を認める (左 )ミオシン線維の欠損を認める (右 )
電気刺激による診断
Anesthesiology. 2013 Jan;118(1):202-15.24
Acute skeletal muscle wasting in critical illness. Puthucheary ZA, Rawal J, McPhail M, et al. JAMA. 2013;310(15):1591-600. PMID:
24108501.
Design: prospective observational studySetting: King’s College Hospital NHS Trust and the Whittington Hospital NHS TrustPatients: 63 critical ill patients.
intubated for longer than 48 hours, spend more than 7 days in critical care, and to survive ICU stay.
Methods:• Muscle loss was determined through serial ultrasound measurement of the
rectus femoris cross-sectional area (CSA) on days 1, 3, 7, and 10. • Histopathological analysis was performed. • muscle protein synthesis, breakdown rates, and respective signaling
pathways were characterized.
25
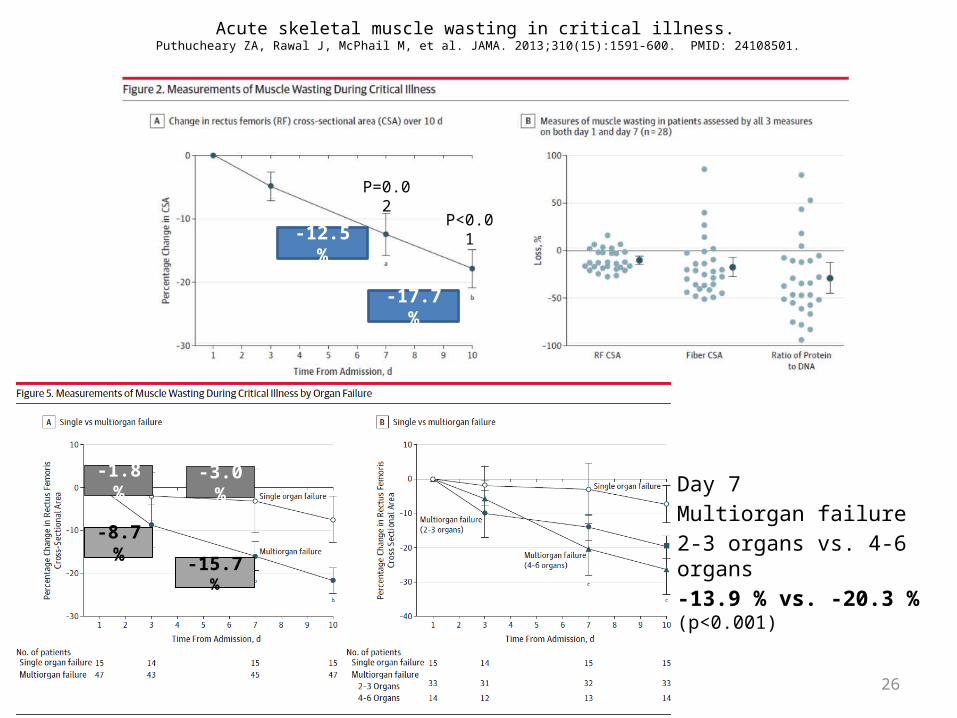
Acute skeletal muscle wasting in critical illness. Puthucheary ZA, Rawal J, McPhail M, et al. JAMA. 2013;310(15):1591-600. PMID: 24108501.
26
-12.5 %
-17.7 %
P=0.02
P<0.01
-1.8 %
-8.7 %
-3.0 %
-15.7 %
Day 7 Multiorgan failure2-3 organs vs. 4-6 organs-13.9 % vs. -20.3 % (p<0.001)

Acute skeletal muscle wasting in critical illness. Puthucheary ZA, Rawal J, McPhail M, et al. JAMA. 2013;310(15):1591-600. PMID: 24108501.
Day 1: Healthy muscleDay 7: muscle with necrosis and cellular infiltration
27

A framework for diagnosing and classifyingintensive care unit-acquired weakness.
Stevens RD, Marshall SA, Cornblath DR et al. Crit Care Med. 2009 Oct;37(10 Suppl):S299-308.
28
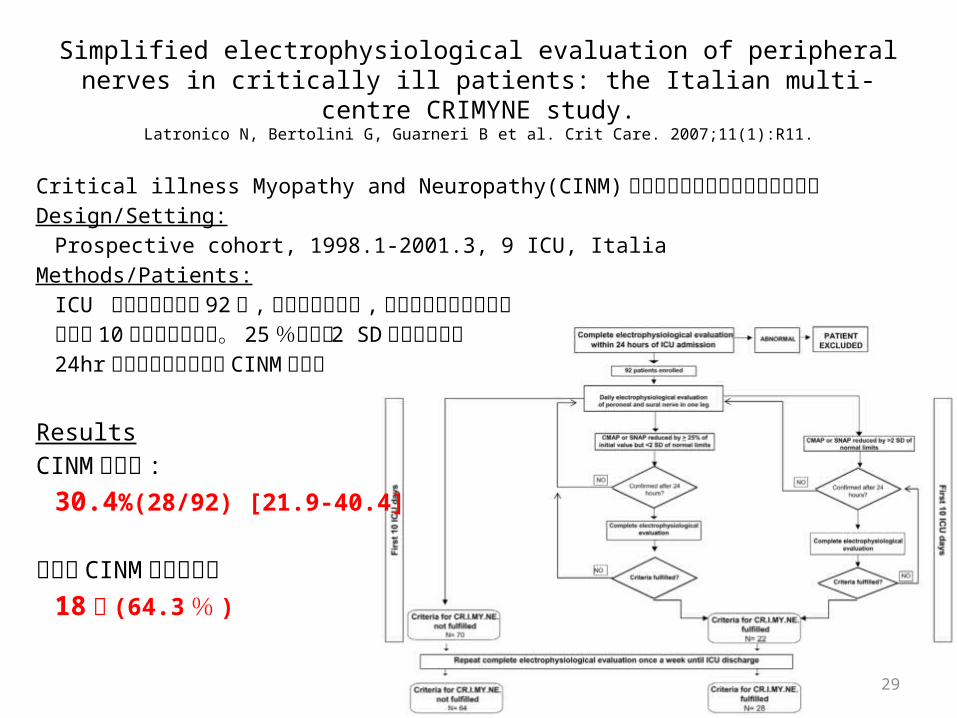
Critical illness Myopathy and Neuropathy(CINM) に対する電気生理学的検査の検証Design/Setting:
Prospective cohort, 1998.1-2001.3, 9 ICU, Italia Methods/Patients:
ICU に入室した患者 92 人 ,片側の腓腹神経 ,腓骨神経の活動を測定入室後 10 日間は毎日測定。 25 %または 2 SD 以上の減退が24hr 後も継続していたら CINM と診断
Simplified electrophysiological evaluation of peripheral nerves in critically ill patients: the Italian multi-centre CRIMYNE study.
Latronico N, Bertolini G, Guarneri B et al. Crit Care. 2007;11(1):R11.
ResultsCINM 発症率 :
30.4%(28/92) [21.9-40.4]
退院時 CINM の徴候あり18 例 (64.3 % )
29

CINM 発症までの日数全 28 例が 13 日以内に発症89.3% は 11 日以内に発症
CMAP の精度 (reduced by more than 2SD)
Sensitivity: 100%
Specificity: 67%
Simplified electrophysiological evaluation of peripheral nerves in critically ill patients: the Italian multi-centre CRIMYNE study.
Latronico N, Bertolini G, Guarneri B et al. Crit Care. 2007;11(1):R11.
30

Acquired weakness, handgrip strength, and mortalityin critically ill patients.
Ali NA, O‘Brien JM Jr, Hoffmann SP et al. Am J Respir Crit Care Med. 2008 Aug 1;178(3):261-8.
握力による ICU AW の診断Cutoffs: 男性 11 kg , 女性 7 kg
Sensitivity: 80.6%
Specificity: 83.2%Negative predictive value: 92.3%Positive predictive value: 63.0%MRC score との相関係数 : 0.643 (p<0.001)
Handgrip
Cut off: 11 kg
Cut off: 7 kg
31
予後
32
ICU acquired paresis (ICU AP) の予後評価Design: Multicenter Prospective cohortSetting: 1999.3-2000.6, 3 Medical ICU and 2 surgical ICU in 4 hospital, FranceMethods/Patients:
人工呼吸管理 (MV) を 7 日以上行い,毎日起こしている患者神経筋疾患が元々なく, MV7 日目以降に ICU AP が疑われる患者ICU AP: MRC score < 48
Outcome: ICU acquired paresis の期間 リスクファクター MV 時間
Results:
7 日以上の MV; 332 人 (26.6 %) → 95 人を検証 ICU AP (n=24) vs. Control (n=71)
Paresis acquired in the intensive care unit: a Prospective multicenter study.
De Jonghe B, Sharshar T, Lefaucheur JP, JAMA. 2002 Dec 11;288(22):2859-67.
33
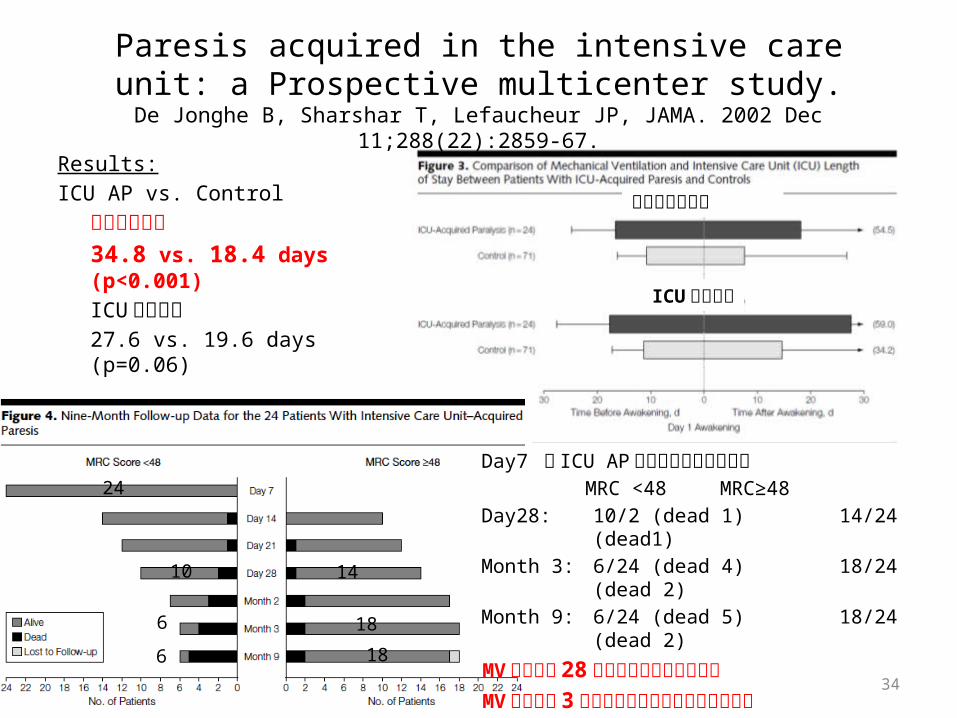
Paresis acquired in the intensive care unit: a Prospective multicenter study.
De Jonghe B, Sharshar T, Lefaucheur JP, JAMA. 2002 Dec 11;288(22):2859-67.
Results:ICU AP vs. Control
人工呼吸期間34.8 vs. 18.4 days (p<0.001)ICU滞在日数27.6 vs. 19.6 days (p=0.06)
Day7 で ICU AP 診断された患者の経過MRC <48 MRC≥48
Day28: 10/2 (dead 1) 14/24 (dead1)Month 3: 6/24 (dead 4) 18/24 (dead 2)Month 9: 6/24 (dead 5) 18/24 (dead 2)
MV 開始から 28 日後までに半数以上回復MV 開始から 3 か月以降はほとんど回復認めない
10 14
6
6
18
18
24
人工呼吸器期間
ICU 滞在期間
34

Acquired weakness, handgrip strength, and mortalityin critically ill patients.
Ali NA, O‘Brien JM Jr, Hoffmann SP et al. Am J Respir Crit Care Med. 2008 Aug 1;178(3):261-8.
ICU acquired paresis の予後を検証Design: Prospective multicenter cohort study Setting/Patients:
2005.5-2007.4, MICU 5 施設(Midwest Critical Care Consortium 参加 )
最低 5 日間人工呼吸管理されている患者
Primary outcome: In-hospital mortality
Secondary outcome: Hospital ICU-free daysICU readmissionRecurrent respiratory failure
35
Results: ICU AP vs. no ICU AP
ICU滞在日数 : 21±11 vs. 12±6 days (p<0.001)
在院日数 : 34±21 vs. 20±12 days (p<0.001)

Acquired weakness, handgrip strength, and mortality in critically ill patients.
Ali NA, O‘Brien JM Jr, Hoffmann SP et al. Am J Respir Crit Care Med. 2008 Aug 1;178(3):261-8.
36
MRC score, 握力が弱い症例で顕著に死亡率増加
MRC score 1.0-3.7: 29.4 % 握力 0-5 : 30.6 %
MortalityMortality
OR for Mortality

ICU AW
• 重症患者では筋力の低下が高い
• 原因は安静や人工呼吸器,敗血症による神経・筋障害など
• 筋力低下を認めた患者の予後は悪い
37

Hibernating bears (Ursidae): metabolic magicians of definite interest for the nephrologist.
Stenvinkel P, Jani AH, Johnson RJ. Kidney Int. 2013 Feb;83(2):207-12
熊は冬眠で何か月も動かず ,食事しないのに廃用が起きない
• 冬眠中は体温維持のために定期的にシバリング ( つまり筋収縮 ) している
• 尿素からたんぱく質へ素早く再生産させる代謝機構腸内細菌により尿素からアンモニアが生産 ,再吸収によりアミノ酸が産生
38
• 冬眠中の熊は中枢性甲状腺機能低下状態でテストステロン生産が上昇 , それが同化と異化のバランスを保ち筋肉の消費を防ぐ
などが理由に挙げられる
しかし,ヒトは熊にはなれないので…

Early Rehabilitation
39

理学療法の実際
リハビリテーションとは?1. 機能・形態障害:心理的・生理的・解剖学的な構造や機能の異常( 例 ) 運動麻痺,筋力低下,関節拘縮・変形,切断,失語症など
2. 能力低下:生活に必要な活動の低下( 例 ) ADL 障害,コミュニケーション障害,移動障害,家事困難など
3. 社会的不利:個人の年齢などの社会文化的な条件に相応する役割が果たせないこと( 例 ) 家庭復帰困難,復職困難,交通手段獲得困難な
ICU におけるリハビリテーション呼吸リハビリテーション 日常生活動作の維持神経リハビリテーション 心臓リハビリテーション…… 40

呼吸リハビリテーション• リラクゼーション・胸郭可動域訓練呼吸筋ストレッチ,徒手胸郭捻転法など
• 呼吸訓練・呼吸筋訓練横隔膜呼吸訓練,口すぼめ呼吸 など
• 排痰法体位排痰法,排痰手技,咳嗽 など
• 上・下肢筋の訓練歩行,エルゴメーター,など
http://karada-design.seesaa.net/upload/detail/bihaku/intercostal01.jpg.html
リラクゼーション( 呼吸筋ストレッチ )
呼吸筋訓練(腹式呼吸 )
胸郭可動域訓練(肋骨捻転法 )
呼吸筋訓練( 横隔膜 )
例
呼吸筋
41

日常生活動作 (Activity of Living ADL)維持
• 端坐位,移乗,歩行などの ADL訓練
• 筋力増強訓練
• ROM exercise 関節可動域訓練
42
肩の屈曲運動
肩・肘の屈伸運動
手指の屈伸運動股関節の屈曲運動
歩行訓練
腸腰筋トレーニング
大腿四頭筋トレーニング
慈恵医大リハビリテーション科パンフレットより
ROM exercise 例
筋力トレーニング例

43Arch Phys Med Rehabil 2010;91:536-42.

Safety/Feasibility
44

Feasibility of physical and occupational therapy beginning from initiation of mechanical ventilation.
Pohlman MC, Schweickert WD, Pohlman Aset al. Crit Care Med. 2010 Nov;38(11):2089-94
人工呼吸器患者 の早期理学・作業療法を検証Design: Descriptive study Setting: University of Chicago Medical center,
University of Iowa Hospital.Patients:
24 時間以上人工呼吸管理 ,72 時間以上必要であると予測される患者(ARDS; 43%, COPD; 8%)
Intervention
452011.4.19 ICU 勉強会 ICU における理学療法 ( 一部改変 )

Adverse event: 80/498 (16%)
・ SpO2 5% 以上低下 ; 31/498 (6 %), ・ HR 20% 上昇 ; 21/498 (4.2 %),
・頻呼吸 ; 20/498 (4.2 %) ・ Agitation/discomfort; 10/498 (2 %)
・ device removal (N-G tube, A line, rectal tube); 4/498 (0.8 %) 理学療法 /作業療法の中止 : 19/498 (4 %); agitation, 人工呼吸器との不同調
Feasibility of physical and occupational therapy beginning from initiation of mechanical ventilation.
Pohlman MC, Schweickert WD, Pohlman Aset al. Crit Care Med. 2010 Nov;38(11):2089-94
SOFA 0 1 2 3 4Cardiovascularb
Hypotension No hypotension MAP <70 DOA </=5 or DOB (any) DOA >5 or NAd </=0.1 DOA >15 or NAd >0.1
462011.4.19 ICU 勉強会 ICU における理学療法 ( 一部改変 )

Team Approach
47

Early intensive care unit mobility therapy in the treatment ofacute respiratory failure
Morris PE, Goad A, Thompson C et al. Crit Care Med 2008;36:2238-43
Patients: 人工呼吸器管理を必要とする患者 330 人挿管 48 時間以内 , ICU 入室 72 時間以内Severe sepsis (non pneumoniae); 15% Out-patient pneumoniae; 20%
Methods: Protocol (n=165): 右図 Usual care (n=165): 看護師による Passive ROMICU Mobility Team; Critical care nurse, Nursing assistant, Physical therapist 人工呼吸器開始後 48 時間以内に開始一般病棟に退室したら終了治療制限 ( 中止含む );
SpO2<88%, MAP < 65 mmHg, 新しく発症した心筋梗塞 ,不整脈の記載 ,PSV から A/Cへの変更
2011.4.19 ICU 勉強会 ICU における理学療法 ( 一部改変 )48
ICU mobility team による介入の検証Design: Single center, Prospective cohort study,Setting: Medical ICU, Wake Forest University Baptist Hospital, North Carolina U.S.A

ResultsUsual Care群 vs. Protocol群離床までの日数 : 11.3 [11.7-15.7] vs. 5.0[4.3-5.9] days (p<0.001)
ICU滞在日数 : 6.9 [5.9-8.0] vs. 5.5 [4.7-6.3] days (p=0.025)
在院日数 : 14.5 [127-16.7] vs. 11.2 [9.7-12.8] days (p=0.006)
人工呼吸期間 : 10.2 [8.7-11.7] vs. 8.8 [7.4-10.3] days (p=0.163)
Early intensive care unit mobility therapy in the treatment ofacute respiratory failure
Morris PE, Goad A, Thompson C et al. Crit Care Med 2008;36:2238-43
2011.4.19 ICU 勉強会 ICU における理学療法 ( 一部改変 )49

Early activity is feasible and safe in respiratory failure patients.Bailey P, Thomsen GE, Spuhler VJ et al. Crit Care Med. 2007 Jan;35(1):139-45.
Early activity の安全性を検証Design: Prospective cohort studySetting: 2003.1.1 - 2003.12.31, Single center, Respiratory ICUPatients: 4 日以上 RICU で人工呼吸器管理されている患者Intervention:
“Early”: 生理学的に安定状態になった時点入室後 24 時間から介入検討Activity event: 端坐位,ベッドから椅子へ移乗しての坐位,歩行Adverse events; 膝から落ちる, tube が抜ける,事故抜管, SBP>200 mmHg or >90 mmHg , SpO2<80%
歩行 219
椅子 229
端坐位 145
593/1,449
Results:呼吸不全患者 :103 人
Sepsis; 41/103, Pneumoniae; 20/103, Cardiovascular disease; 10/103
ICU 入室からの時間端坐位 ;6.6±5.5 日 , 椅子の坐位 8.8±7.6日 ,歩行 11.3±10.1 日
Adverse event: 14/1,449 (0.96 %)SBP > 200 mmHg; 1/14, < 90 mmHg; 4/14SpO2 < 80%; 3/14, N-G抜去 ; 1/14
Total: 1,449 activity event
502011.4.19 ICU 勉強会 ICU における理学療法 ( 一部改変 )

Early physical and occupational therapy in mechanicallyventilated, critically ill patients: a randomized Controlled trial
Schweickert WD, Pohlman MC, Pohlman AS et al. Lancet 2009;373:1874-82
Design: Multicenter Randomized Controlled trialSetting: 2005.6-2007.10, Medical ICU,
University of Chicago Medical Center, University of Iowa Hospital, USAMethods/Patients:
24 時間以上の人工呼吸器管理 (MV) が予測 , 人工呼吸器管理が 72 時間以内の患者 104 人入院 2週間前までの Barthel Index ≥ 70Intervention 群 (n=49): 早期に理学療法と作業療法Control 群 (n=55): プライマリーケアチームによってオーダーされた時に治療行うルーチーンの理学療法は MV開始 2週間は行わない
Early exercise and mobilization:毎朝鎮静を中断し,四肢の受動運動→コミュニケーションがとれれば能動運動→座位→立位→ベッドから椅子への移動→歩行と段階的に PT/OT が行う。治療の中止・継続は下記の項目を基に PT/OT が決定 : MAP ≥ 110mmHg or < 65mmHg, SBP > 200mmHg, HR <40/min or > 130/min, RR <5/min or >40/minSpO2 < 88%, 治療中の疾患の悪化を認めたとき ( 出血,頭蓋内圧亢進など )MV非同調 , 患者の強いストレス , 患者が攻撃的 ,鎮静薬の追加を必要とする場合 ,新規の不整脈 ,心筋虚血の可能性 ,気道トラブル ,
512011.4.19 ICU 勉強会 ICU における理学療法 ( 一部改変 )

Results: Intervention vs. ControlPT/OT の初回介入 ; 1.5 [1.0-2.1] vs. 7.4 [6.0-10.9] days (p<0.0001)退院時の最大歩行距離 ; 33.4 [0-91.4] vs. 0 [0-30.4] m (p=0.004)挿管から ADL 上昇までの期間 (days)
離床 ; 1.7 [1.1-3.0] vs. 6.6 [4.2-8.3] , 立位 ; 3.2 [1.5-5.6] vs. 6.0 [4.5-8.9] 足踏み ; 3.3 [1.6-5.8] vs. 6.2 [4.6-9.6], 移乗 ; 3.1 [1.8-4.5] vs. 6.2 [4.5-8.4]歩行 ; 3.8 [1.9-5.8] vs. 7.3 [4.9-9.6] ( すべて p<0.0001)
Early physical and occupational therapy in mechanicallyventilated, critically ill patients: a randomized Controlled trial
Schweickert WD, Pohlman MC, Pohlman AS et al. Lancet 2009;373:1874-82
↑ 独立した ADL は Intervention群で有意に多い
522011.4.19 ICU 勉強会 ICU における理学療法 ( 一部改変 )

Results: Intervention vs. Control
退院時に自立した身体機能の回復 ; 29 (59%) vs. 19 (35%) (p=0.02)
ICU せん妄 ;2.0 [0.0-6.0] vs. 4.0 [2.0-7.0] days (p=0.03)ICU 期間中のせん妄割合 ;
33% [0-58] vs. 57% [33-69] (p=0.02)在院中せん妄 ;
2.0 [0.0-6.0] vs. 4.0 [2.0-8.0] days (p=0.02)入院中のせん妄割合 ; 28% [26] vs. 41% [27] (p=0.01)
退院時 Barthel Index score;75[7.5-95] vs. 55 [0-85] (p=0.05)
退院時 ICU acquired paresis; 15(31%) vs. 27(49%) (p=0.09)
人工呼吸 Free days;23.5 [7.4-25.6] vs. 21.1 [0.0-23.8](p=0.05)
ICU 滞在日数 ; 5.9 [4.5-13.2] vs. 7.9 [6.2-12.9] (p=0.08)在院日数 ; 13.5[8.0-23.1] vs. 12.9 [8.9-19.8] (0.93)
自立した身体機能の回復 ;Control 群は Intervention 群に比べて約 2 週間遅かった
Functional independence
Control
Intervention
532011.4.19 ICU 勉強会 ICU における理学療法 ( 一部改変 )

Physical Therapy for the Critically Ill in the ICU: A Systematic Review and Meta-Analysis.
Kayambu G, Boots R, Paratz J. Crit Care Med. 2013 Mar 29.
Design: Meta-analysis, 10 RCTs, 5 reviewsOutcome: Mortality, Length of Hospital Stay, Length of ICU Stay, Physical Function,
Quality of Life, Muscle Strength, Ventilator-Free days
Favours standard care
Favoursphysical therapy
Favours standard care
Favoursphysical therapyPhysical Function
Quality of Life
Physical therapy で有意に効果ありPhysical Function, Quality of Life,Respiratory Muscle Strength, Ventilator-Free days
54
Respiratory Muscle strength
Ventilator-Free Days

Physical Therapy for the Critically Ill in the ICU: A Systematic Review and Meta-Analysis.
Kayambu G, Boots R, Paratz J. Crit Care Med. 2013 Mar 29.
Favours standard care
Favoursphysical therapyLength of Hospital stay
Length of ICU stay
55
在院日数 ,ICU 滞在日数を短縮
在院日数 :
Hedge’s g -0.34 [-0.53 to -0.15, p<0.001]
ICU 滞在日数 :
Hedge’s g -0.34 [-0.51 to -0.18, p<0.001]

Standardized Rehabilitation for ICU Patients With Acute Respiratory Failure
Peter E. Morris, Michael J. Berry ClinicalTrials.gov Identifier: NCT00976833
現在進行中急性呼吸不全患者に対する早期リハビリテーション効果の検証
Design: Randomized, open Label, Phase3
Setting: 2009.10-2014.8 Wake Forest University Health Sciences, North Carolina U.S.A
Patients: Acute Respiratory Failure, 人工呼吸器または NPPV で管理
ntervention: Standardized Rehabilitation vs. Usual CareStandardized Rehabilitation; 3 component Rehabilitation approach( Passive Range of Motion, Physical Therapy and Progressive Resistance Training )
Usual Care; Usual Physical Therapy
Primary outcome: 在院日数
56

TEAM: An Multi-centre Observational Study of Early Activity and Mobilization in Australia and New Zealand
Carol Hodgson, Amanda Martin ClinicalTrials.gov identifier: NCT01674608
現在進行中重症患者に対する早期リハビリテーション効果の検証
Design: Multicenter Prospective cohort
Setting: 2012.7-2013.11, The Alfred in Australia, Wellington hospital in New Zealand
Patients: 24 時間以内に人工呼吸管理となり 72 時間以上 ICU 在室した患者
Primary outcome: ADL
57

Early Rehabilitation
• 呼吸器管理中の患者でも安全に行うことができる
• ADL を回復させ QOL を保つことが期待できる
58

Technology
59

Ergometer
MOTOmed letto2 60

Early exercise in critically ill patients enhances short-term functional recovery
Burtin C, Clerckx B, Robbeets C, Crit Care Med 2009;37:2499-2505
ICU におけるエルゴメーターの効果を検証
Design: Randomized Controlled trialSetting: 2005.12-2007.2, Single center, University Hospital Gasthuisberg, Leuven, Belgium,
Patients:ICU に 7 日以上滞在すると思われる患者 90人
2011.4.19 ICU 勉強会 ICU における理学療法 ( 一部改変 )
Intervention:第 5ICU 病日より開始Control群 : Standard mobilizationTreatment群 : Standard mobilization + Bedside ergometer
Standard mobilization; 呼吸療法と手足の自動的・他動的運動Bedside ergometer; 5 回 /週, 20 分 /day (MOTOmed Letto 2, RECK-Technik GmbH & Co.KG)
Primary outcome: 病院退院時の 6MWD, SF-36
61

Result:対象患者のほとんどが術後患者QOL (Control vs. Treatment)
6MWD; 143[37–226 ]; vs. 196 [126–329 ] m (p <0.05)SF-36 PF score; 15 points [14–23] vs. 21 points [18–23]( p <0.01)
筋力の回復 (ICU 退室時 vs. 病院退院時 )Treatment 群 ; 1.83±0.91 vs. 2.37±0.62 N ・ kg-1 (p<0.01)Control 群 ; 1.86±0.78 vs. 2.03±0.75 N ・ kg-1(p=0.11)
weaning 時間, ICU ・病院滞在時間では有意差は見られず
Early exercise in critically ill patients enhances short-term functional recovery
Burtin C, Clerckx B, Robbeets C, Crit Care Med 2009;37:2499-2505
6MWD SF-36, PF 筋力の回復
62

EMSElectromuscular stimulation
63

64
Crit Care Med 2009; 37[Suppl.]:S436 –S441

Prevention of disuse muscle atrophy by means of electrical stimulation: maintenance of protein synthesis.
Gibson JN, Smith K, Rennie MJ. Lancet. 1988 Oct 1;2(8614):767-70.
Patients: 下腿を骨折し大腿までギプスをして約 40 日間動かさなかった患者 21 人Stimulation (n=14) vs. no stimulation (n=7)
Methods: Quadriceps cross-section area (CSA) に電気刺激 70 V, 30Hz 2s on / 9s off, 1hr,
その後筋生検して分析
Results
65

Peripheral muscle strength training in bed-bound patients with COPD receiving mechanical ventilation: effect of electrical stimulation.
Zanotti E, Felicetti G, Maini M et al. Chest. 2003 Jul;124(1):292-6.
人工呼吸器管理の COPD 患者に対する EMS の効果を検証Design/Setting
Randomized Controlled study, respiratory high-dependency care unit, ItalyMethods/Patients気切され人工呼吸器管理中の COPD 患者 , 体表の筋肉に萎縮を認める慢性の高 CO2 血症 , High care unit, ICU含め 30 日以上。4週間以上急性増悪なし。ステロイドの吸入 , 全身投与されている患者
は除外28 日間のリハビリプログラムを施行ALM/ES群 vs. ALM群
ALM/ES群 (n=12): active limb mobilization + : electrical stimulationALM群 (n=12): active limb mobilization only
66

Peripheral muscle strength training in bed-bound patients with COPD receiving mechanical ventilation: effect of electrical stimulation.
Zanotti E, Felicetti G, Maini M et al. Chest. 2003 Jul;124(1):292-6.
Results: 両群ともに介入前後で筋力上昇ALM/ES 群で筋力回復の大きさが有意に大きい (p=0.02)
ベッドから車椅子移乗できるまでの日数ALM/ES 群で有意に短いALM/ES vs. ALM : 10.75±2.41 vs. 13.33±2.53 days (p=0.001) 67

Improvement in quadriceps strength and dyspnea in daily tasks after 1 month of electrical stimulation in severely deconditioned and malnourished COPD.
Vivodtzev I, Pépin JL, Vottero G et al. Chest. 2006 Jun;129(6):1540-8.
人工呼吸器管理の COPD 患者に対する EMS の効果を検証Design/Setting
Randomized Controlled study, Pulmonary rehabilitation center
PatientsSevere COPD, 急性期に ICU に滞在し, 1 か月間入院していた患
者 ,%FEV ≤50%, FEV/FVC ratio <70%, BMI<22Quadriceps muscle atrophy,
Methodsinability to perform cycle exercise (< 3-5 min), ES + UR 群 (n=9) vs. UR 群 (n=8)ES: electro stimulation
4 日 /週 , 大腿四頭筋に EMS30min. 1-5mA/ 日。5Hz400μs-5min, 35Hz400μs-25min, 5Hz400μs-7s
UR: usual rehabilitation4 日 /週 ,PT指導の下 ALM 施行。最大で 2.5Kg の負荷をかけながら 5-10 分歩行
Results: ES + UR 群 vs. UR 群MVC (N); Pre 279±210 vs. 250±126
Post 376±205 vs. 287±134Distance (m); Pre 185±93 vs. 179±123
Post 248±80 vs. 209±112MVC: maximum voluntary contraction 最大随意収縮 68

Effect of transcutaneous electrical muscle stimulation on muscle volume in patients with septic shock.
Poulsen JB, Møller K, Jensen CV et al. Crit Care Med. 2011 Mar;39(3):456-61.
Sepsis 患者に対する EMS の効果を検証Design/Setting: randomized, open label, mixed ICU,
Methods/Patients: 72 時間以内に septic shock と診断された患者 8 人 Non-EMS vs. EMSEMS群 : 大腿四頭筋 4 か所に EMSパッドを装着 ,1 回 60 分 ,7 日間施行CT にて大腿四頭筋の容量を計測
Results:ICU 入室 7 日後 , 両群で筋肉の容量低下両群に有意差なし
69

Neuromuscular electrical stimulation for intensive care unit-acquired weakness: protocol and methodological implications for a randomized, sham-Controlled, phase II trial.
Kho ME, Truong AD, Brower RG et al. Phys Ther. 2012 Dec;92(12):1564-79.
現在進行中Randomized, sham-Controlled, concealed, Phase II pilot studySetting: Johns Hopkins university HospitalPatients: Medical ICU, MV 1day or more, NMES を大腿四頭筋,腓腹筋,ヒラメ筋に装着。 60 分 / 日。Primary outcome: 下肢の筋力,
70

Wii
71

Feasibility and observed safety of interactive video games for physical rehabilitation in the intensive care unit: a case series.Kho ME, Damluji A, Zanni JM, Needham DM. J Crit Care. 2012 Apr;27(2):219.e1-6
72
Wii使用について実行可能性と安全性を検証Wii はリハビリテーションプログラムの 1 部に組み込まれ, Wii の施行は PT によって判断Design: Prospective observationSetting: 2009.9-2010.10, Medical ICU, Johns Hopkins Hospital Results: PT + Wii (n=22) vs. PT only(n=388)
ICU滞在日数 : 8.5 [2.8-28.8] vs. 4.0 [2.0-8.0] (p=0.014)在院日数 : 30.5 [8.9-52.3] vs. 13.0 [7.0-25.0] (p=0.008)

50% が歩行可能な患者Wii 施行目的の 52% がバランス保持一番人気はボクシングラインやチューブは 6割以上がつけたまま
Feasibility and observed safety of interactive video games for physical rehabilitation in the intensive care unit: a case series.Kho ME, Damluji A, Zanni JM, Needham DM. J Crit Care. 2012 Apr;27(2):219.e1-6
73

Cost Saving
74

Early physical medicine and rehabilitation for patients with acute respiratory failure: a quality improvement project.
Needham DM, Korupolu R, Zanni JM et al. Arch Phys Med Rehabil. 2010 Apr;91(4):536-42
ICU でリハビリテーション介入を進めるために院内で Quality Improvement Project(QI project) を敢行。
ICU early physical rehabilitation programs: financial modeling of cost savings.
Lord RK, Mayhew CR, Korupolu R, Crit Care Med. 2013 Mar;41(3):717-24
QI project より得られたデータを基にリハビリテーションにより医療経済効果を試算
75
Johns Hopkins Hospital での取り組み

Early physical medicine and rehabilitation for patients with acute respiratory failure: a quality improvement project.
Needham DM, Korupolu R, Zanni JM et al. Arch Phys Med Rehabil. 2010 Apr;91(4):536-42
Design: Prospective before-afterSetting: Johns Hopkins University, MICU, 16 床 ,
Staff-to-patient;1:2(Attending, Fellow, Resident physicians / Registered nurses) Patients: 4 日以上の人工呼吸器患者 57 人
病院内に QI project team を設置Initial phase (2006.4-2007.8): Engage, Educate processExecution phase (2007.5-8): 早期リハビリテーション介入 , QI periodPre-QI (2007.2-4) vs. QI period (2007.5-7), MICU
76
Quality Improvement Process1. より大きなヘルスケアシステムの問題点を理解する2. 異業種間のカイゼンチームを創造する3. 適切にカイゼンを行った場合 ,影響を受ける利害関係者をリストアップ4. 4Es (Engage, Educate, Execute, Evaluate) の通じて変えていく

Early physical medicine and rehabilitation for patients with acute respiratory failure: a quality improvement project.
Needham DM, Korupolu R, Zanni JM et al. Arch Phys Med Rehabil. 2010 Apr;91(4):536-42
77
First step (Engage)関係各所との話し合い ,プロジェクトの周知 , 患者との知識共有 , リハビリ経験のフィードバック
Second step (Education)ICUAW の長期予後と早期リハビリの有用性を PT,OT,看護師に対して講義する。
Third step (Execution)ICU 入室時の指示を“安静”から“耐えられるまで”に変更ベンゾジアゼピンの持続投与から“必要に応じてボーラス”へPT,OT のコンサルテーションガイドラインを作成安全ガイドラインの作成ICU 入室患者への理学療法士による指導の導入筋力低下が長引いた場合の神経内科医へのコンサルトの回数を増やす
Fourth Step (Evaluate)毎週関係各所とミーティングを開き ,問題点 , 障壁 , 解決法を話し合う
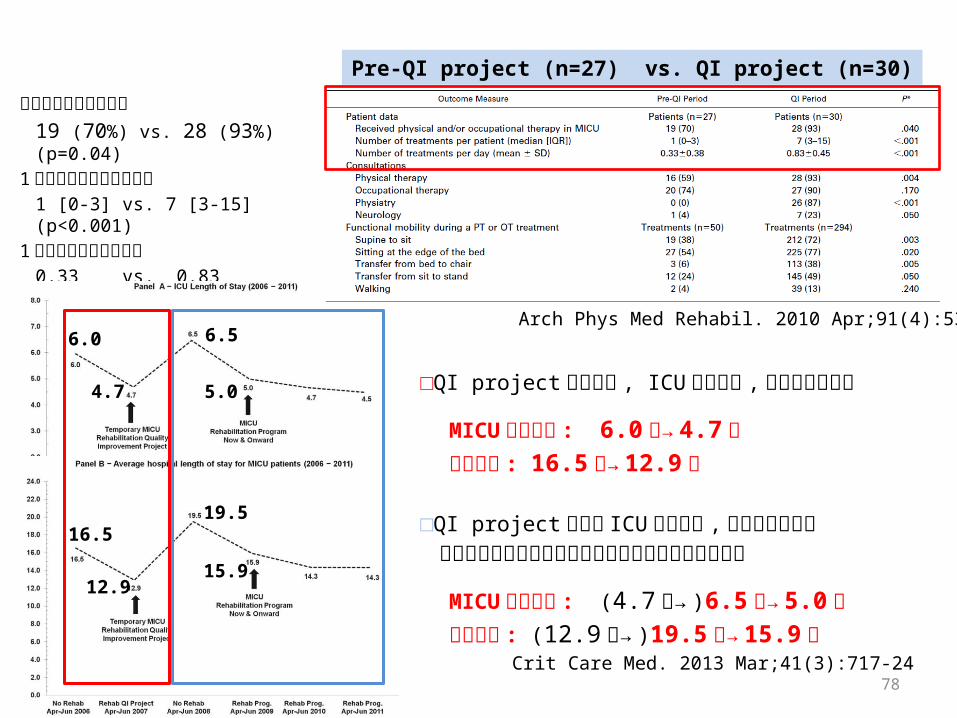
理学療法を受けた割合 19 (70%) vs. 28 (93%) (p=0.04)
1 人当たりの理学療法回数1 [0-3] vs. 7 [3-15] (p<0.001)
1 日当たりの理学療法数0.33 vs. 0.83 (p<0.001)
78
Arch Phys Med Rehabil. 2010 Apr;91(4):536-42
Pre-QI project (n=27) vs. QI project (n=30)
□QI project によって , ICU 在室日数 , 在院日数は減少
MICU 滞在日数 : 6.0 日→ 4.7 日 在院日数 : 16.5 日→ 12.9 日
□QI project 終了後 ICU 在室日数 , 在任日数は増加リハビリテーションプログラムを本格運用後再び低下
MICU 滞在日数 : (4.7 日→ )6.5 日→ 5.0 日 在院日数 : (12.9 日→ )19.5 日→ 15.9 日
Crit Care Med. 2013 Mar;41(3):717-24
6.0
4.7
6.5
5.0
16.519.5
12.915.9

ICU early physical rehabilitation programs: financial modeling of cost savings.
Lord RK, Mayhew CR, Korupolu R, Crit Care Med. 2013 Mar;41(3):717-24
リハビリテーションプログラム導入による経済効果を試算Methods:Johns Hopkins Hospital の QI project を基に計算Variables for the Financial model
Example Scenario: QI project の平均値によるモデルBest Scenario: QI project で平均値以上の値によるモデルConservative Scenario: 米国の 188私立病院 271ICU のデータを基にしたモデル
それぞれのモデルで病床数ごとの医療コストを試算
Directed-variable cost;検査 ,輸血 ,X 線など消費された医療コスト( 医療スタッフの給与は含ない )
医療スタッフのコスト試算

QI project によるコスト削減効果(1 年間あたり )
リハビリプログラムにより削減された費用 :
$ 817,836
全体での削減費用 : $ 1,176,312
リハビリプログラムでかかった費用 :
$ 358,475
一人あたりの削減費用 : $1,307
在院短縮による費用削減試算
ICU 入室 2000件 / 年の場合 (最大で )
Best-case scenario: $ 3,763 / 年Conservative-case scenario: $257/ 年

まとめ
• 重症患者では安静や人工呼吸器,敗血症などが原因で筋力低下が起きる
• 筋力低下を認めた患者の予後は悪い
• 呼吸器管理中の患者でも早期のリハビリテーションは安全に行うことができる
• 理学療法の他 ,様々な器具の使用によって ADL を回復させ ,QOL を保つことが期待できる
81

これからの展望
• “ベッド上安静”の“指示”は可能な限り出さない
• リハビリテーションは積極的に行う
• “患者を動かす”ということを常に念頭に置く
82
参考資料
83

予後評価
Crit Care Med. 2013 Mar 29.84

Six-Minute Walk Distance
固く平らな平地での 6 分間の歩行距離
目安
健康成人 : 男性 580-630 m 女性 500 m
severe COPD: 54 m (O2 4 l/min) 95 m
85
Am J Respir Crit Care Med. 2002 Jul 1;166(1):111-7.

SF-36項目 下位尺度名 要約概念
激しい活動
身体機能 physical function:
PF
身体的健康
適度の活動
少し重いもの
階段を数階
階段を1階
体を曲げる
1キロメートル以上歩く
数百メートル以上歩く
百メートル歩く
入浴・着替え
身体的理由による活動時間の減少
日常役割機能 role-physical :
RP
身体的理由による活動不可能
身体的理由による活動の一部制限
身体的理由による活動困難
痛みの程度 体の痛み bodily pain :
BP痛みによる生活制限
健康状態の評価全体的健康感 general health
perception:GH
病気になりやすい
健康は悪くなる
健康状態は非常に良い
項目 下位尺度名 要約概念
元気いっぱい
活力 vitality :
VT
精神的健康
活力にあふれていた
疲れ果てていた
疲れを感じた
付き合いの減少 社会生活機能 social function :
SF付き合い時間の減少
心理的理由による活動時間減少
日常役割機能 (精神 )
role-emotional :RE
心理的理由による活動制限
心理的理由による活動困難
神経質
心の健康 mental health :
MH
落ち込み
穏やかな気分
憂鬱な気分
楽しい気分 日本腰痛会誌 2002; 8: 38-4386

MRC score
Crit Care Med. 2007 Sep;35(9):2007-15.
87

Activity ScoreFeeding0 = unable5 = needs help cutting, spreading butter, etc., or requires modified diet10 = independent
0, 5, 10
Bathing0=dependent5 = independent (or in shower)
0, 5
Grooming0 = needs to help with personal care5 = independent face/hair/teeth/shaving (implements provided)
0, 5
Dressing0 = dependent5 = needs help but can do about half unaided10 = independent (including buttons, zips, laces, etc.)
0, 5, 10
Bowels0 = incontinent (or needs to be given enemas)5 = occasional accident10 = continent
0, 5, 10
Bladder0 = incontinent, or catheterized and unable to manage alone5 = occasional accident10 = continent
0, 5, 10
Activity ScoreToilet Use0 = dependent5 = needs some help, but can do something alone10 = independent (on and off, dressing, wiping)
0, 5, 10
Transfers (bed to chair and back)0 = unable, no sitting balance5 = major help (one or two people, physical), can sit10 = minor help (verbal or physical)15 = independent
0, 5, 10, 15
Mobility (on level surfaces)0 = immobile or < 50 yards5 = wheelchair independent, including corners, > 50 yards10 = walks with help of one person (verbal or physical) > 50 yards15 = independent (but may use any aid; for example, stick) > 50 yards
0, 5, 10, 15
Stairs0 = unable5 = needs help (verbal, physical, carrying aid)10 = independent
0, 5, 10
TOTAL (0 - 100) _______
Barthel index
88

Rosow Breslau Mobility Difficulty.
The mobility difficulty score Beneficiaries responses to three items taken from the Rosow Breslau scale:‐
• Stooping• lifting a 10 lbs.• extending arms above shoulder• writing, • walking¼mile
1 5 scale(no‐ difficulty, little difficulty, some difficulty, a lot of difficulty, and unable), yielding a score that ranged from 5 to 25. For ease of interpretation, we transformed the scores to a 0 100 scale by subtracting ‐5, dividing by 20 and multiplying by 100.
89
Am J Respir Crit Care Med. 2011 Apr 15;183(8):1037-42.

ADL Disability.
The ADL disability score beneficiaries’ responses regarding difficulty with common activities of daily living
• Bathing• Dressing• Chair transfer• Walking• Toileting
The MCBS survey collected data on difficulty (yes/no),receipt of assistance, and receipt of standby help only. If a beneficiary indicated they do not do a task, then they were asked specifically if that was because of health reasons. These responses were mapped to categories of assistance as defined by Finch, et al.
90
Am J Respir Crit Care Med. 2011 Apr 15;183(8):1037-42.