ias–usa eric s. daar, md professor of medicine david geffen school of medicine at university of...
TRANSCRIPT

IAS–USA
Eric S. Daar, MDProfessor of Medicine
David Geffen School of Medicineat University of California Los Angeles
Antiretrovirals in the Management of HIV Infection: Case-Based, Panel Discussion
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.

Slide 2 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
When to Start: Case 1
– 30 yo white man
– Diagnosed on routine insurance examination
– PMHx remarkable for HTN, diet controlled
– No medications
– Understands treatment issues and wants to begin therapy if you think it is appropriate
Adapted from Mike Saag

Slide 3 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
When to Start: Case 1b
– 30 yo white man
– Diagnosed on admission to jail for disorderly conduct
– PMHx remarkable for HTN, diet controlled and paranoid schizophrenia
– Doesn’t take any medications and doesn’t want to

Slide 4 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
Effect on inflammation in predicting mortality higher in HIV disease than the general population (SOCA/SCOPE)
Hunt et al CROI 12

Slide 5 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
T cell “activation” is lower in treated than untreated adults, but consistently higher than “normal”
Hunt et al JID 2003, PLoS ONE 2011 and unpublished
% C
D38
+H
LA
DR
+C
D8+
T C
ells
0
20
40
60
80
HIVNegative(n=82)
Non-Controller
(n=65)
HAART(n=132)
P < 0.001
P < 0.001
HIV –(n=132)
HIV +ART
(n=65)
HIV +Untreated
(n=82)

Slide 6 of 42
Permanent Loss of CD4 if Wait to Start
• CD4 count increases on sustained suppressive (<400 c/mL) ARV treatment (n=655) by baseline count– >350 cells/mm3:
CD4 counts return to near-normal levels
– ≤350 cells/mm3: CD4 counts significantly increased but plateau after 4 years below normal range
• Differences in CD4 counts associated with differences in morbidity and mortality
Median CD4 Counts Over 6 YearsStratified by Baseline CD 4 Count
Moore RD, Keruly JC. Clin Infect Dis 2007;44:441-446.
900
800
700
740
500
400
300
200
100
00 1 2 3 4 5 6
Years After Starting HAART
CD
4 C
ou
nt
(cel
ls/m
m3 )
<200 201–350 >350
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.

Slide 7 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
Reasons to Start Early:
• The Biology• Association of Inflammation and Disease• Better Tolerated/Easier to Take
Medications• Randomized Controlled Trial Data• Cohort Data• Irreversible Damage• Public Health

Slide 8 of 42
Most New Infections Transmitted by Persons Who Do Not Know Their
Status
~25% Unaware
of Infection
~42% Aware
of Infection
account for…
~54% New
Infections
~46% of New
Infections
Source: G. Marks et al. AIDS 2006
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.

Slide 9 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
HPTN 052
1763 HIV discordant couples (HIV+ partner CD4 350-550)
874 delayed HAART (CD4 250)
*96% reduction in HIV transmission to HIV-negative partner median follow-up 2 years
1 transmission* & 3 cases of
extrapulmonary TB
886 immediate HAART
All receiving HIV prevention services
27 transmissions*& 17 cases of
extrapulmonary TB

Slide 10 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
So ….what is the harm?
• Destruction of lymphoid tissue• Inflammation• Increased cardiovascular events• Increased incidence of certain
malignancies• Increased ‘aging’• Accelerated cognitive decline

Slide 11 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
When to Start Treatment
Clinical CategoryCD4 Count (cells/mm3)
HIV RNA(copies/mL)
2/13/13DHHS
Guidelines
2012IAS-USA
Guidelines
AIDS-defining illness or severe symptoms
Any value Any value Treat
Asymptomatic <500 Any value Treat
>500 Any value Treat
Pregnant women Any value Any value Treat
HIV-associated nephropathy
Any value Any value Treat
HIV/HBV coinfection when HBV treatment is indicated
Any value Any value Treat
DHHS. Available at: http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf. Revision February 2013; Thompson MA, et al. JAMA. 2012;308:387-402.
*Unless elite controller (HIV RNA <50 copies/mL) or has stable CD4 cell count and low-level viremia in absence of therapy. The IAS-USA guidelines also recommend initiating antiretroviral therapy in HIV-infected patients with active hepatitis C virus infection, active or high risk for cardiovascular disease, and symptomatic primary HIV infection.

Slide 12 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
When to Start: Case 2
• 34 yo woman is diagnosed with TB• As part of evaluation she is found to be HIV+• Initial lab values
– CD4 82 cells/µL– VL 76,000 c/mL
• No other significant medical condition• She is started on 4-drug anti-TB therapy
(including INH and rifabutin)• Virus is wild-type virus

Slide 13 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
When to Start ARV with Complications• ARVs within 0-2 weeks of diagnosis
– Infections for which there is no specific treatment (e.g. dementia, cryptosporidium, microsporidium, PML) (AIII)
– Other OIs, e.g. PCP (AI)• Consider deferring therapy for crypto meningitis• Tuberculosis
– Within 2 weeks for CD4 <50 cells/uL (AI)– Within 2-4 weeks for severe symptoms with CD4 50-200
(BI) and >200 cells/uL (BIII)– Within 8-12 weeks for mild symptoms and 50-500
cells/uL (AI) and >500 cells/uL (BIII)– Meningitis 2 months (AI) in RLS, perhaps earlier in other
settings (CIII)DHHS. Available at: http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf. Revision February 2013; Thompson MA, et al. JAMA. 2012;308:387-402.

Slide 14 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
A 49 year old asymptomatic man presents to your clinic after recently being diagnosed with HIV
• History of HTN with CrCl ~42 mL/min• HBsAb+, HCV antibody negative• CD4 cells repeatedly 700-420 cells/uL• Plasma HIV RNA 30-50,000 copies/mL• Not anxious to start antiretrovirals but willing
if you think it is necessary

Slide 15 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
Factors to consider in choosing first-line therapy
• Patient’s willingness to commit to therapy• Baseline resistance• Efficacy data• Tolerability• Convenience• Comorbid conditions• Consequences of failure (resistance)
• Since the introduction of potent ARV therapy preferred regimens all include NRTIs + third drug

Slide 16 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
Boosted-Protease Inhibitors
Adapted from: 1. Eron J, et al. Lancet 2006; 368:476-482; 2. Mills A, et al. AIDS May 29, 2009 3. Molina J-M, et al. 48th ICAAC/46th IDSA , Washington, DC, 2008. Abst. H-1250d
ARTEMIS2
(ITT, TLOVR)96 weeks
LPV/r QD or
BID
DRV/r 800/100
QD
7971
n=343n=3460
20
40
74
80
100
CASTLE3
(ITT, NC=F)96 weeks
ATV/r300/100
QD
LPV/r400/100
BID
6874
0
20
40
74
80
100
n=443 n=440
KLEAN1
(ITT-E, TLOVR)48 weeks
LPV/r400/100
BID
FPV/r 700/100
BID
6665
N=444n=4340
20
40
74
80
100

Slide 17 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
ATV/r vs. EFVPrimary Endpoint
Daar ES, et al. Ann Intern Med 2011; 154:445-456.

Slide 18 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
STARTMRK: RAL vs. EFV
Rockstroh J, et al, 19th IAC; Washington, DC; July 22-27, 2012; Abst. LBPE19.
ITT, NC=F
281 278 279 280 281 281 274 280 281 281 274 279282 282 282 281 282 282 281 281 282 282 282 279
Raltegravir 400 mg BIDEfavirenz 740 mg QHS
Number of Contributing Patients
0 12 24 48 72 96 120 144 168 192 216 240Weeks
0
20
40
74
80
100
Per
cent
age
of P
atien
ts w
ithH
IV R
NA
Leve
ls <
50 C
opie
s/m
L
86
82
81
79
42
69
76
67
71
61
CD4 Change: RAL +374 vs. EFV +312

Slide 19 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA. Rimsky L, et al. 50th ICAAC 2010, Boston, MA. Abst. H-1810
84.3%82.3%
Pooled ECHO and THRIVE: Virologic Response (ITT-TLOVR)

Slide 20 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
Rimsky L, et al. 50th ICAAC 2010, Boston, MA. Abst. H-1810
Pooled ECHO and THRIVE: Virologic Response (ITT-TLOVR)
Slide 21 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
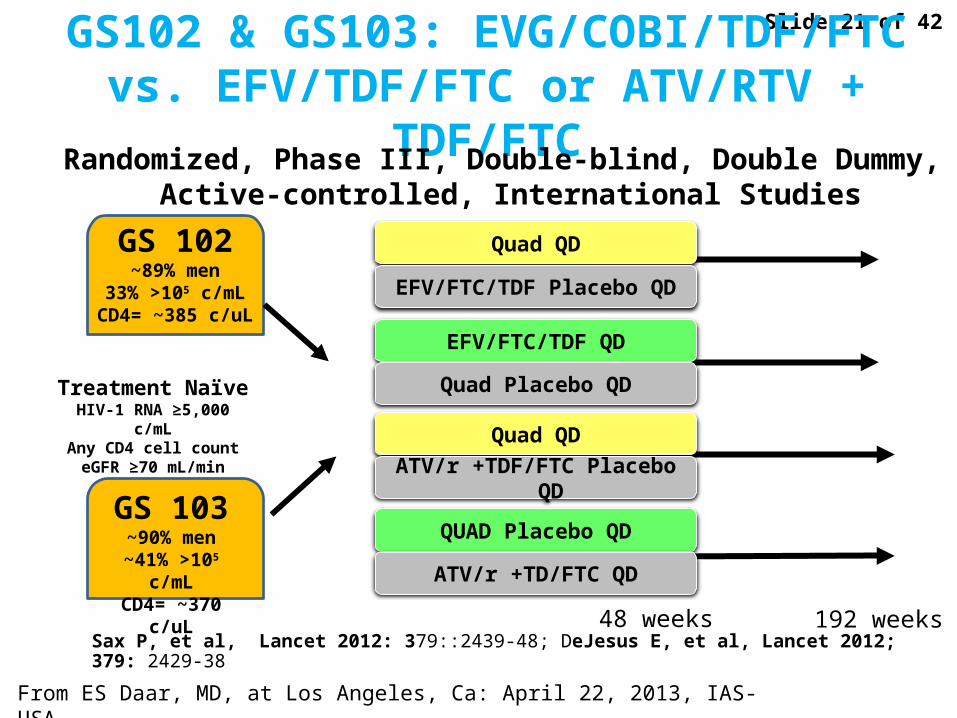
GS102 & GS103: EVG/COBI/TDF/FTC vs. EFV/TDF/FTC or ATV/RTV + TDF/FTC
Sax P, et al, Lancet 2012: 379::2439-48; DeJesus E, et al, Lancet 2012; 379: 2429-38
Randomized, Phase III, Double-blind, Double Dummy, Active-controlled, International Studies
Treatment Naïve HIV-1 RNA ≥5,000 c/mL
Any CD4 cell counteGFR ≥70 mL/min
48 weeks 192 weeks
GS 102~89% men
33% >105 c/mLCD4= ~385 c/uL
GS 103~90% men
~41% >105 c/mLCD4= ~370 c/uL
Quad QD
EFV/FTC/TDF Placebo QD
EFV/FTC/TDF QD
Quad Placebo QD
Quad QD
ATV/r +TDF/FTC Placebo QD
QUAD Placebo QD
ATV/r +TD/FTC QD

Slide 22 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
Study 236-102: Primary Endpoint:HIV-1 RNA < 50 copies/mL
+3.6%, 95% CI 3.6 (-1.6% to +8.8%)
CD4+ change: Quad +239 vs. EFV +206 c/mm3 (p=0.009)No difference by baseline characteristics
Sax P, et al. 19th CROI; Seattle, WA; March 5-8, 2012. Abst. 101.

Slide 23 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
Study 236-102:Common Adverse Events
Quad(n=348)
EFV/FTC/TDF(n=352)
Treatment Emergent Adverse Events in ≥ 10% of subjects (%)Diarrhea 23% 19%Nausea * 21% 14%Abnormal Dreams ^ 15% 27%Upper Respiratory Infection 14% 11%Headache 14% 9%Fatigue 12% 13%Insomnia * 9% 14%
Depression 9% 11%
Dizziness ^ 7% 24%
Rash # 6% 12%
* p<0.05; ^ p<0.001; # p=0.009Sax P, et al, Lancet 2012: 379::2439-48

Slide 24 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
Study 236-103: ATV/r vs. TDF/FTC/COBI/EVG HIV-1 RNA < 50 c/mL
QUAD ATV/r
100
90
80
70
74
50
40
30
20
10
0Per
cen
t w
ith
HIV
RN
A <
50 c
/mL
(IT
T, M
=F
)
BL 2 4 8 12 16 24 32 40 48
Week
Diff: 3.5% (95% CI: -1.0 to 8.0)
92%
88%
Changes in CD4+ count: Quad +207 vs. ATV/r +211 cells/mm3 (p=0.61)No difference by baseline characteristics
DeJesus E, et al, Lancet 2012; 379: 2429-38

Slide 25 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
Study 236-103: Adverse Events
Adverse Events > 10% in Either Group
Discontinuation rates due to renal events were identical in both arms (0.3%)
Quad(n=353)
ATV/r + FTC/TDF(n=355)
Diarrhea 22% 27%
Nausea 20% 19%
Upper respiratory infection 15% 16%
Headache 15% 12%
Fatigue 14% 13%
Ocular icterus 1% 14%
DeJesus E, et al, Lancet 2012; 379: 2429-38

Slide 26 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
TDF/FTC/EVG/COBI vs. EFV or ATV/r: Lipid changes
P =0.001P <0.001 P= 0.001 P =0.44 P =0.006
Conclusion: While some lipid fractions better with Quad than EFV or ATV/r, overall differences were modest and unlikely to be of clinical significance.
Sax P, et al, Lancet 2012: 379::2439-48; DeJesus E, et al, Lancet 2012; 379: 2429-38
Slide 27 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
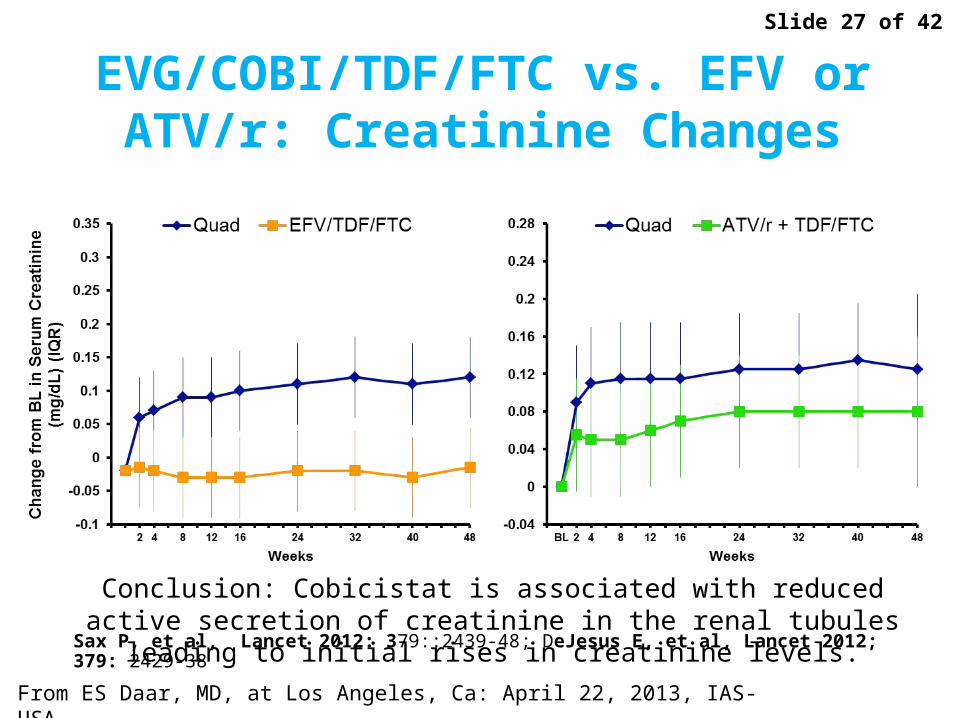
EVG/COBI/TDF/FTC vs. EFV or ATV/r: Creatinine Changes
Conclusion: Cobicistat is associated with reduced active secretion of creatinine in the renal tubules leading to initial rises in creatinine levels.
Sax P, et al, Lancet 2012: 379::2439-48; DeJesus E, et al, Lancet 2012; 379: 2429-38

Slide 28 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
A5202: Study Design
Stratified by screening HIV-1 RNA (< or ≥ 100,000 c/mL)
Enrolled 2005-2007Followed through Sept 2009, 96 wks after last pt enrolled
HIV-1 RNA ≥1000 c/mLAny CD4+ count
> 16 years of age
ART-naïve
N=1858
Randomized 1:1:1:1
TDF/FTC QD
ABC/3TC Placebo QD
EFV
QD
ABC/3TC QD
TDF/FTC Placebo QD
EFV
QD
TDF/FTC QD
ABC/3TC Placebo QD
ATV/rQD
ABC/3TC QD
TDF/FTC Placebo QD
ATV/r
QD
A
B
C
D
Arm
ART-naïve
1857 enrolled
Randomized 1:1:1:1
TDF/FTC QD EFV
QD
ABC/3TC QD
TDF/FTC Placebo QD
EFV
QD
TDF/FTC QD
ABC/3TC Placebo QD
ATV/rQD
ABC/3TC QD
TDF/FTC Placebo QD
ATV/r
QD

Slide 29 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
No. at Risk
ABC-3TC 398 363 313 267 222 188 137 87 49 20
TDF-FTC 399 361 321 284 236 204 174 104 65 23
A5202: Time to Virologic Failure in Patients with HIV RNA >100,000 c/mL
Sax PE, et al. NEJM 2009;361:2230-2240.
0
20
40
60
80
100
0 12 24 36 48 60 72 84 96 108Pro
ba
bil
ity
of
No
Vir
olo
gic
F
ail
ure
(%
)
Weeks since Randomization
P<0.001, log-rank testHazard ratio, 2.33 (95% CI, 1.46-3.72)
TDF-FTC (26 events)
ABC-3TC (57 events)
Probability of No Virologic Failure

Slide 30 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
ABC/3TC vs. TDF/FTCLow Viral Load Stratum
Sax PE, et al. JID 2011: 204:1191-1201.

Slide 31 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
HEAT: Virologic Failure by Baseline HIV-1 RNA (A5202 Efficacy Endpoint)
90 8787 90
0
20
40
60
80
100
<100,000 ≥100,000
ABC/3TC
Perc
ent w
ithou
t Viro
logi
c Fa
ilure
n = 188 155 140205
Pappa K, et al. 17th IAC, Mexico City, 2008. Abst. THAB0304.Young B, et al. 48th ICAAC/46th IDSA, Washington, DC, 2008. Abst. H-1233.
ABC/3TC TDF/FTC
≥500,000 c/mL250,000 - <500,000 c/mL
100,000 - <250,000 c/mL
<100,000 c/mL
41%
63%
18%
19%18%
4%22%
15%
0%
20%
40%
74%
80%
100%
Prop
ortio
n of
Sub
ject
s w
ith V
F
~59%
~37%

Slide 32 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
Concerns regarding NRTIs
• Conflicting results regarding relationship between ABC and CV events
• TDF-associated with greater decline in bone mineral density
• TDF-associated with variable decline in renal function

Slide 33 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
Preferred Regimens
• EFV/TDF/FTC• ATV/r + TDF/FTC• DRV/r (once daily) + TDF/FTC• RAL + TDF/FTC[Pregnant Women Only: LPV/r (twice daily) + ZDV/3TC]
AlternativeRegimens
• EFV + ABC/3TC• RPV + (TDF or ABC)/(FTC or 3TC)• ATV/r or DRV/r + ABC/3TC• FPV/r or LPV/r (qd or bid) ABC/3TC or TDF/FTC• RAL + ABC/3TC• EVG/COBI/TDF/FTC (9/18/12)
AcceptableRegimens
• EFV or RPV + ZDV/3TC• NVP + TDF/FTC or ZDV/3TC or ABC/3TC• ATV + (ABC or ZDV)/3TC• ATV/r, DRV/r, LPV/r, FPV/r , RAL + ZDV/3TC• MVC + ZDV or ABC/3TC• SQV/r + TDF/FTC or ABC/3TC or ZDV/3TC (with caution)
DHHS Guidelines for Adolescents/Adults:What to Start
DHHS Guidelines. Available at: http://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf. Revision March 27, 2012.

Slide 34 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
ART: What to StartIAS–USA Recommendations, 2012
Thompson MA, et al. JAMA. 2012;308(4):387-402
Component Recommended Regimens
NNRTI plus nRTIs
• Efavirenz/tenofovir/emtricitabine (AIa)• Efavirenz plus abacavir/lamivudine (AIa)
in HLA-B*5701-negative patients with baseline plasma HIV-1 RNA <100,000 copies/mL
PI/r plus nRTIs
• Darunavir/r plus tenofovir/emtricitabine (AIa)• Atazanavir/r plus tenofovir/emtricitabine (AIa)• Atazanavir/r plus abacavir/lamivudine (AIa)
in patients with plasma HIV-1 RNA <100,000 copies/mL
InSTI plus nRTIs • Raltegravir plus tenofovir/emtricitabine (AIa)

Slide 35 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
A 45 year old African American woman presents to your clinic having been diagnosed with HIV and severe thrush/onychomycosis• Clinically stable on fluconazole• History mild depression, diabetes, HTN and
dyslipidemia on ACE, metformin, atorvastatin• Laboratories
– HBsAg and HCV antibody negative– AST/ALT- 42/82 IU/mL, CrCl~70 mL/min (relatively stable),
HgbA1C=7.1%, UA- 3+ proteinuria– CD4= 78 cells/uL, HIV-RNA= 219,000 copies/mL– HIV genotype- WT
• Ready to start antiretrovirals if recommended with no specific concerns regarding various adverse events but would prefer simple regimen

Slide 36 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
Patient starts TDF/FTC/EFV, TMP/SMX and continues other meds. At 2 months CD4 190 cells/uL, HIV RNA 220 copies/mL, but patient has increasing depression and persistent neurologic symptoms thought to be associated with EFV. CrCl is repeatedly ~70 mL/min. She is seeing psych and on antidepressants.
A 45 year old African American woman• H/O depression, DM, HTN, dyslipidemia, CKD• CrCl- 70 mL/min with proteinuria• CD4 nadir= 78 cells/uL and BL HIV RNA 212,000 copies/mL

Slide 37 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
Switch TDF/FTC + EFV to RPV (N=49)
Mills A, et al. 51st ICAAC; Chicago, IL; September 17-20, 2011. Abst. H2-794c.
RPV mean Ctrough in ECHO/THRIVE

Slide 38 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
Patient switched to TDF/FTC + ATV/r and continued other meds. After 4 months neurologic symptoms resolved, CD4 250 cells/uL, HIV RNA <40 copies/mL but patient CrCl has gradually declined (now off TMP/SMX) to 40-45 mL/min with no change in other labs or UA (glucosuria and proteinuria).
A 45 year old African American woman• H/O depression, DM, HTN, dyslipidemia, CKD• CrCl- 40-45 mL/min with proteinuria (HLA-B5701-negative)• CD4 nadir= 78 cells/uL and BL HIV RNA 212,000 copies/mL

Slide 39 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
D:A:D Study: NRTIs and Risk of MI
Lundgren J, et al. 16th CROI, Montreal, Canada, 2009. Abst. 44LB. Sabin C, et al. Lancet 2008;371:1417-26.
ZDV ddI ddC d4T 3TC ABC TDF#PYFU: 138,109 74,407 29,676 95,320 153,009 53,300 39,157#MI: 533 331 148 405 554 221 139
1.9
1.5
1.2
1
0.8
0.6Recent Exposure*: yes/noCumulative Exposure: per year
**
Rel
ativ
e R
isk
of
MI
(95%
CI)
Adjusting for eGFR does not change ABC MI finding:Adjusted RR 1.89; 95% CI (1.46 – 2.44; P=0.0001)
* Recent use=current or within the last 6 months. **Not shown (low number of patients currently on ddC)

Slide 40 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
VA Case Registry: Use of ABC or TDF in Last Regimen and Risk of MI
Bedimo R, et al. Clin Inf Dis. 2011;53:84-91.
Unadjusted HR of AMI for each PY of exposure to each one of the categories
Adjusted for estimated GFR prior to regimen onset (by MDRD method)
ABC TDF Both ABC and TDF
Haz
ard
rat
io
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
2.0
2.2
NRTI in Last Regimen During Observation Period

Slide 41 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
Cumulative Exposure to ARVs and Risk of CKD
Cockcroft-Gault (n=225)
MDRD (n=274)CKD-EPI (n=258)INSIGHT def (n=129)Censoring ATVCensoring TDFCensoring boosted PI
Tenofovir
Indinavir
Atazanavir
Lopinavir/r
0.9 1.4Mocroft A, et al. AIDS. 2010; 53:1667-78

Slide 42 of 42
From ES Daar, MD, at Los Angeles, Ca: April 22, 2013, IAS-USA.
A5202: ABC/3TC vs. TDF/FTCMedian Change in Creatinine Clearance
ABC/3TC
ATV/r
ABC/3TC
TDF/FTC
TDF/FTC
EFVN= 191 173 217 191 186 157 200 178
Wk 48, p<0.001Wk 96, p<0.001
Wk 48, p=0.83Wk 96, p=0.14
Week 96
Week 48
p-values: ABC/3TC vs. TDF/FTC
Ch
ang
e in
Cal
cula
ted
C
reat
inin
e C
lear
ance
, (m
L/m
in)
>25% decr(%): 3 2 7 6 2 3 1 3Daar ES, et al. Ann Intern Med 2011; 154:445-456.