hysterectomy: current controversies · risks of chd (hr 1.17) and lung cancer (hr 1.26) were...
TRANSCRIPT

HYSTERECTOMY: CURRENT CONTROVERSIES
Catherine Matthews, MDAssociate Professor and Division Chief
Obstetrics and GynecologyUniversity of North Carolina, Chapel Hill
Disclosure
I have received grant support from Boston Scientific, American Medical Systems, Pelvalon, and Intuitive Surgical. None of these grants pertain to the CME topic discussed today.
My content will include reference to commercial products; however, generic and alternative products will be discussed whenever possible.
I do not intend to discuss any unapproved or investigative use of commercial products or devices.
CURRENT CONTROVERSIES?
49 yo G2P2 AAF with worsening menorrhagia and dysmenorrhea. She has failed management with NSAIDS. Hx/o DVT with OCPsFH: Breast cancer in mother at age 55PE: BMI 45 BP 160/90
14 week mobile fibroid uterusBenign secretory endometriumHgb 10.2
What is her “optimal” management?
Mode of hysterectomy?TAH?TVH?TLH with or without robotic-assistance?SCH?
How should the uterine tissue be extracted?Power morcellation?Vaginal morcellation?Laparotomy?
What should be done about the tubes and ovaries?
Objectives
Discuss the following controversies surrounding hysterectomy:1. Optimal route of surgery
a. Overall morbidityb. Morcellationc. Vaginal cuff dehiscenced. Cost
2. Cervix preservation versus removal?3. Fallopian tube preservation versus removal?4. Ovarian preservation versus removal?
Controversy # 1: Mode of hysterectomy

“ ‘Minimally invasive’ is an impact, not an incision.”
Ted Anderson, MD PhD, Vanderbilt University
Which mode of hysterectomy has lowest morbidity?Vaginal > Laparoscopic > Abdominal
34 trials, N=4495
Route of Hysterectomy RatesWright JD, et al. JAMA 2013
Robot Total costs $2189 (95% CI, $2030-$2349)
Overuse
Underuse
TVH
Why are rates of TVH so low?
Perceived as “difficult”
Requires specialized skill
Requires directed training

Increased training needed Money may drive TVH training
COSTS?
Surgical costsHospital stay
ROBOTIC TECHNOLOGY RESULTED IN
SUBSTANTIALLY MORE COSTS
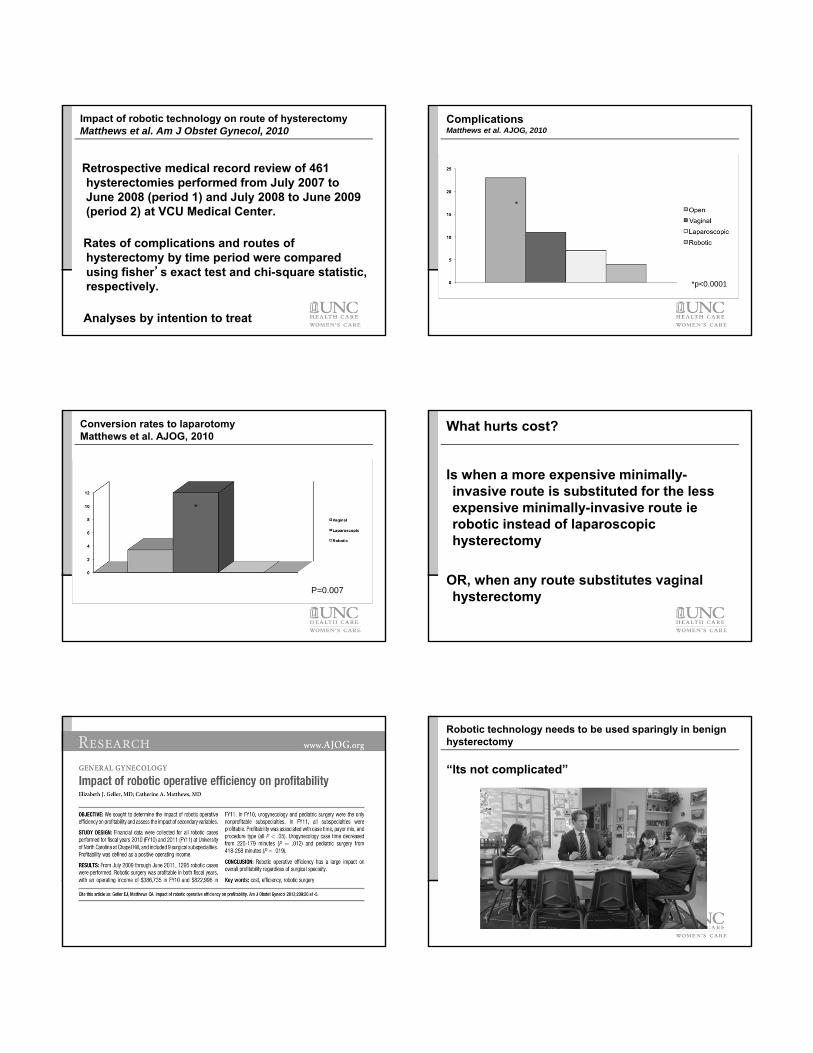
Impact of robotic technology on route of hysterectomyMatthews et al. Am J Obstet Gynecol, 2010
Retrospective medical record review of 461 hysterectomies performed from July 2007 to June 2008 (period 1) and July 2008 to June 2009 (period 2) at VCU Medical Center.
Rates of complications and routes of hysterectomy by time period were compared using fisher’s exact test and chi-square statistic, respectively.
Analyses by intention to treat
ComplicationsMatthews et al. AJOG, 2010
*
*p<0.0001
Conversion rates to laparotomyMatthews et al. AJOG, 2010
*
P=0.007
What hurts cost?
Is when a more expensive minimally-invasive route is substituted for the less expensive minimally-invasive route ierobotic instead of laparoscopic hysterectomy
OR, when any route substitutes vaginal hysterectomy
Robotic technology needs to be used sparingly in benign hysterectomy
“Its not complicated”

Controversy # 2: How should tissue be extracted?
What we know
Minimally invasive approach to hysterectomy or myomectomy results in:
Lower EBLShorter hospital stayReduced painReduced incidence of VTEReduced incidence of wound complicationsShorter convalescenceBetter cosmesis
Morcellation creates a diagnostic and therapeutic challenge with occult LMS
What we know about leiomyosarcoma
It is a disease with poor prognosis
Stage Spread 5-year survival
Stage I Confined to uterus 60%
Stage II Confined to pelvis 35%
Stage III Abdominal spread, local nodes
28%
Stage IV Bladder / rectum or distant mets
15%

Emerging evidence
Morcellation worsens prognosis of patients with LMSGeorge S et al. Retrospective cohort study evaluating the impact of intraperitoneal
morcellation on outcomes of localized uterine leiomyosarcoma. Cancer. 2014 Retrospective review of all patients w LMS 2007-2012 at Dana-Farber and BWHn=58; 19 morcellation (power and scalpel); 39 TAH
TAH (n=39) Morcellation(n=19)
P-value
Age 56 49 0.01
Stage I 87% n/a n/a
Recurrence 51% 74% 0.002
Recurrence abd / pelvis
20% 86% 0.001
Overall survival 67% 58% 0.22
Challenges
Preoperative identificationImaging – difficult to distinguish from benign disease
Dynamic MRI + LDH + LDH isoenzyme-3 (degenerating myomas vs. LMS)
Diffusion-weighted-imaging (DWI), apparent diffusion coefficient (ADC)Endometrial biopsy – rarely positiveUterine biopsy – may miss disease or seed cellsClinical factors
“Rapid” growthAgeAfrican-American women twice as likely to get LMSPelvic radiationRetinoblastoma gene
ACOG on Consent
Incidence of occult sarcoma, including LMS, is unknown. However, the risk estimate of approximately 2:1000 women who undergo hysterectomy or myomectomy should be discussed.
If occult malignancy is present, power morcellation increases the likelihood of intraperitonealdissemination. It may also worsen prognosis, make a definitive diagnosis and accurate staging difficult, and result in additional surgery, medical management, or both
If fragments of benign tissue are disseminated through morcellation, there is the possibility of seeding viable ectopic tissue as a result (e.g., leiomyoma, endometriosis, adenomyosis, and ovarian remnants). This potentially may require additional intervention.
If power morcellation is to include the use of a specimen bag, potential concerns should be discussed, including insufficient bag size, disruption of the bag by the morcellator, and reduced visualization as a result of using the bag.
Alternatives to the use of power morcellation should be discussed, including removal of intact tissue through mini-laparotomy, laparotomy, or colpotomy incisions, or by total abdominal hysterectomy, vaginal hysterectomy, or laparoscopic vaginal hysterectomy.
Decision Analysis: LH + morcellation v AHSiedhoff et al. AJOG in press100,000 subject hypothetical cohort
5-year time horizonDecision: Abdominal hysterectomy vs laparoscopic hysterectomy
with morcellationOutcomes:
Transfusion, wound infection, cuff dehiscence, VTE, herniaLeiomyosarcomaDeath from leiomyosarcoma
Assumed occult LMS cases would be FIGO stage I-II (59% death 5-yr)
Assumed morcellation would escalate to FIGO stage III (72% death 5-yr)Death from hysterectomy
UtilitiesValue and duration determined from literature, 1-mo increments
Results
Outcome LH: Base-case [range] AH: Base-case [range] Incremental Difference (LH– AH)
Leiomyosarcoma cases 120 120 n/a
Leiomyosarcoma deaths 86 [50-353] 71 [41-289] 15
Hysterectomy-related deaths 12 [10-12] 32 [28-32] -20
Total deaths 98 [60-365] 103 [69-321] -5
Transfusion 2,400 [1,300-3,500] 4,700 [4,300-4,700] -2,300
Venous thromboembolism 690 [30-900] 840 [720-840] -150
Vaginal cuff dehiscence 640 [200-890] 290 [150-600] 350
Abdominal wound infection 1,500 [55-1,500] 6,300 [6,300] -4,800
Hernia 710 [140-900] 4,500 [4,500-9,800] -8,090
Quality-adjusted life years 499,171 [499,062-499,280] 490,711 [482,733-486,270] 8,460 *
* LH experience 0.85 additional QALYs (1.02 mos) over 5 years
Decision Analysis Conclusions
Model predicted lower mortality and higher quality of life with LHSupports existing recommendations for a minimally invasive approach to hysterectomy when feasible (ACOG, AAGL)
StrengthsDecision analysis helpful when RCT not feasibleConsiders procedure-related mortality, not just mortality associated with morcellationEvaluates additional clinical outcomes, complicationsRobust in sensitivity analyses

Conclusions regarding morcellation
The issue appears confined to power morcellation
Vaginal morcellation has been done for years without controversy
Recommendation: Remove uterine tissue through the vagina or mini-lap
Controversy # 3: How to close the vaginal cuff?
Laparoscopic hysterectomy associated withhigher rates of vagina cuff complications
Vaginal cuff closure is better
Controversy # 4: Take or leave the cervix? 9 trials, N=1553No benefit on urinary, bowel or sexual sx
Ongoing cyclic VB 16x higher

If you perform supracervical hysterectomy
You have to deal with tissue extraction….And cyclic vaginal bleedingAnd cervical cytology surveillance
For no evidence-based benefit
Controversy # 5: Take or leave the fallopian tubes?
Origin of ovarian cancer? Paradigm Shift: The Tubal Hypothesis
Prophylactic Salpingectomy
Potential decreased risk for ovarian cancer and other fallopian tube complications
Advocated by many during hysterectomy, sterilization, or other pelvic surgery
• 600,000 hysterectomies
• 700,000 tubal sterilizations
Proposed as a temporary measure for BRCA carriers wishing to avoid oophorectomy
Opportunity for Intervention
Hysterectomy
Tubal Sterilization
• Interval
• Postpartum or Cesarean
Other Pelvic or Abdominal Surgery

Risk:Benefit Ratio of salpingectomy
Benefits?Potential reduction in ovarian cancer
Reduction in re-operation for benign disease
Risks?Potential decrease in ovarian blood flow
Operative complications
Complications of Retained Fallopian Tubes
Retained
Fallopian
Tubes
Hydrosalpinx
Tubal Prolapse/Torsion
Chronic PID/TOA
Hydatid Cyst
Fallopian Tube/Peritoneal
Cancer
Ovarian Blood Supply Tubal Sterilization Considerations
Salpingectomy most effective tubal sterilization method
Women should routinely be offered salpingectomy
Creinin, MD, et al. Female Tubal Sterilization: The Time Has Come to Routinely Consider Removal. Obstetrics and Gynecology. 2014; 124(3): 596-9.
Controversy # 5: Take or leave the fallopian tubes?
This actually isn’t a controversy: Take the tubes!
Controversy # 6: Take or leave the ovaries?

< 40 74%40-44 62%45-49 41%50-60 25%60-64 31%
Cardiovascular diseaseParker WH et al. Obstet Gynecol 2009; 113:1027-37
Nurse’s Health Study demonstrated that among participants with BSO (16,345) vs conservation (13,035), risks of CHD (HR 1.17) and lung cancer (HR 1.26) were increased
Risks of breast, ovarian, and total cancer were decreased but total cancer mortality increased (HR 1.17)
BSO at time of hysterectomy for benign disease was associated with an increased risk of all cause mortality: Over 35 years, 1 additional death would be expected for every 9 oophorectomies performed
Parker WH et al. Ovarian conservation at the time of hysterectomy and long-term health outcomes. Obstet Gynecol. 2009
Garbage in, garbage out?
Results based on a Markov modelConclusions entirely drawn from use of a RR of 2.2 for women < 45 who had BSO.
Not based on any observations of real patientsSummary: Women with BSO < 55 have 8.58% excess mortality; BSO < 59, 3.92% excess mortality

For pre-menopausal women
Leave ovaries behind unless there is a strong FHx of ovarian or breast cancer suggesting a germline mutation
REMOVE TUBES
For women aged 52-65
No evidence for benefit on CHD
No evidence for benefit on hip fracture
Conflicting data on sexual fxn
Recommend BSO for ovarian cancer reduction
Remove tubes
For women > 65
Perform elective BSO
Remove entire specimen

For our case…..
Most reasonable to recommend:
Vaginal hysterectomy and bilateral salpingectomy
References
Ilyas S. Aleem, Emil H. Schemitsch, and Beate P. Hanson. What is a clinical decision analysis study? Indian J Orthop. 2008 Apr-Jun; 42(2): 137–139.
Wu JM, Wechter ME, Geller EJ, Nguyen TV, Visco AG. Hysterectomy rates in the United States, 2003. Obstet Gynecol 2007;110:1091-5.
Wright JD, Herzog TJ, Tsui J, Ananth CV, Lewin SN, Lu YS, et al. Nationwide trends in the performance of inpatient hysterectomy in the united states. Obstet Gynecol 2013;122:233-41.
Jacoby VL, Autry A, Jacobson G, Domush R, Nakagawa S, Jacoby A. Nationwide use of laparoscopic hysterectomy compared with abdominal and vaginal approaches. Obstet Gynecol. 2009;114:1041-8.
Lee J, Jennings K, Borahay MA, Rodriguez AM, Kilic GS, Snyder RR, et al. Trends in the national distribution of laparoscopic hysterectomies from 2003-2010. J Minim Invasive Gynecol 2014; 21:656-61
Patel PR, Lee J, Rodriguez AM, Borahay MA, Snyder RR, Hankins GD, et al. Disparities in use of laparoscopic hysterectomies: A nationwide analysis. J Minim Invasive Gynecol 2014;21:223-7.
Cucinella G, Granese R, Calagna G, Somigliana E, Perino A. Parasitic myomas after laparoscopic surgery: An emerging complication in the use of morcellator? A description of four cases. Fertil Steril 2011;96:90-6.
Epstein JH, Nejat EJ, Tsai T. Parasitic myomas after laparoscopic myomectomy: Case report. Fertil Steril2009;91:932.
Kumar S, Sharma JB, Verma D, Gupta P, Roy KK, Malhotra N. Disseminated peritoneal leiomyomatosis: An unusual complication of laparoscopic myomectomy. Arch Gynecol Obstet 2008;278:93-5.
References
Larrain D, Rabischong B, Khoo CK, Botchorishvili R, Canis M, Mage G. "Iatrogenic" parasitic myomas: Unusual late complication of laparoscopic morcellation procedures. J Minim Invasive Gynecol2010;17:719-24.
Leren V, Langebrekke A, Qvigstad E. Parasitic leiomyomas after laparoscopic surgery with morcellation. Acta Obstet Gynecol Scand 2012;91:1233-6.
Moon HS, Koo JS, Park SH, Park GS, Choi JG, Kim SG. Parasitic leiomyoma in the abdominal wall after laparoscopic myomectomy. Fertil Steril 2008;90:1201.
Schuster MW, Wheeler TL, Richter HE. Endometriosis after laparoscopic supracervical hysterectomy with uterine morcellation: A case control study. J Minim Invasive Gynecol 2012;19:183-7.
Sinha R, Sundaram M, Lakhotia S, Kadam P, Rao G, Mahajan C. Parasitic myoma after morcellation. J Gynecol Endosc Surg 2009 Jul;1:113-5.
Takeda A, Mori M, Sakai K, Mitsui T, Nakamura H. Parasitic peritoneal leiomyomatosis diagnosed 6 years after laparoscopic myomectomy with electric tissue morcellation: Report of a case and review of the literature. J Minim Invasive Gynecol 2007;14:770-5.
Seidman MA, Oduyebo T, Muto MG, Crum CP, Nucci MR, Quade BJ. Peritoneal dissemination complicating morcellation of uterine mesenchymal neoplasms. PLoS One 2012;7:50058.
Oduyebo T, Rauh-Hain AJ, Meserve EE, Seidman MA, Hinchcliff E, George S, et al. The value of re-exploration in patients with inadvertently morcellated uterine sarcoma. Gynecol Oncol 2014;132:360-5.
References
The Lancet O. Patient safety must be a priority in all aspects of care. Lancet Oncol. 2014 Feb;15(2):123,2045(14)70042-7.
Goff BA. SGO not soft on morcellation: Risks and benefits must be weighed. Lancet Oncol 2014;15.
Web site: Food and Drug Administration. Laparoscopic Uterine Power Morcellation in Hysterectomy and Myomectomy: FDA Safety Communication. Available at: http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm393576.htm. Retrieved April 17, 2014.
Vilos GA, Marks J, Ettler HC, Vilos AG, Prefontaine M, Abu-Rafea B. Uterine smooth muscle tumors of uncertain malignant potential: Diagnostic challenges and therapeutic dilemmas. A report of 2 cases and review of the literature. J Minim Invasive Gynecol 2012;19:288-95.
Wu TI, Yen TC, Lai CH. Clinical presentation and diagnosis of uterine sarcoma, including imaging. Best Pract Res Clin Obstet Gynaecol 2011;25:681-9.
Leibsohn S, d'Ablaing G, Mishell DR, Schlaerth JB. Leiomyosarcoma in a series of hysterectomies performed for presumed uterine leiomyomas. Am J Obstet Gynecol 1990;162:968-76.
Reiter RC, Wagner PL, Gambone JC. Routine hysterectomy for large asymptomatic uterine leiomyomata: A reappraisal. Obstet Gynecol 1992;79:481-4.
Parker WH, Fu YS, Berek JS. Uterine sarcoma in patients operated on for presumed leiomyoma and rapidly growing leiomyoma. Obstet Gynecol 1994;83:414-8.
Takamizawa S, Minakami H, Usui R, Noguchi S, Ohwada M, Suzuki M, et al. Risk of complications and uterine malignancies in women undergoing hysterectomy for presumed benign leiomyomas. GynecolObstet Invest. 1999;48:193-6.
References
Sinha R, Hegde A, Mahajan C, Dubey N, Sundaram M. Laparoscopic myomectomy: Do size, number, and location of the myomas form limiting factors for laparoscopic myomectomy? J Minim Invasive Gynecol2008;15:292-300.
Kamikabeya TS, Etchebehere RM, Nomelini, R S., Murta, E F. Gynecological malignant neoplasiasdiagnosed after hysterectomy performed for leiomyoma in a university hospital. European journal of gynaecological oncology 2010;31:651-3.
Leung F, Terzibachian JJ. Re: "The impact of tumor morcellation during surgery on the prognosis of patients with apparently early uterine leiomyosarcoma". Gynecol Oncol 2012;124:172-3.
Rowland M, Lesnock J, Edwards R, Richard S, Zorn K, Sukumvanich P. Occult uterine cancer in patients undergoing laparoscopic hysterectomy with morcellation. Gynecologic oncology 2012;127:29.
Theben JU, Schellong AR, Altgassen C, Kelling K, Schneider S, Grosse-Drieling D. Unexpected malignancies after laparoscopic-assisted supracervical hysterectomies (LASH): An analysis of 1,584 LASH cases. Arch Gynecol Obstet 2013 Mar;287:455-62.
Park JY, Park SK, Kim DY, Kim JH, Kim YM, Kim YT, et al. The impact of tumor morcellation during surgery on the prognosis of patients with apparently early uterine leiomyosarcoma. Gynecol Oncol 2011 Aug;122:255-9.
Nieboer TE, Johnson N, Lethaby A, Tavender E, Curr E, Garry R, et al. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev 2009;8:CD003677.
References
ACOG committee opinion no. 444: Choosing the route of hysterectomy for benign disease. Obstet Gynecol2009;114:1156-8.
AAGL Advancing Minimally Invasive Gynecology Worldwide. AAGL position statement: Route of hysterectomy to treat benign uterine disease. J Minim Invasive Gynecol 2011;18:1-3.
Clarke-Pearson DL, Geller EJ. Complications of hysterectomy. Obstet Gynecol 2013;121:654-73.
Loft A, Andersen TF, Bronnum-Hansen H, Roepstorff C, Madsen M. Early postoperative mortality following hysterectomy. A Danish population based study, 1977-1981. Br J Obstet Gynaecol 1991;98:147-54.
Wingo PA, Huezo CM, Rubin GL, Ory HW, Peterson HB. The mortality risk associated with hysterectomy. Am J Obstet Gynecol 1985;152:803-8.
McPherson K, Metcalfe MA, Herbert A, Maresh M, Casbard A, Hargreaves J, et al. Severe complications of hysterectomy: The VALUE study. BJOG 2004;111:688-94.
Wallenstein MR, Ananth CV, Kim JH, Burke WM, Hershman DL, Lewin SN, et al. Effect of surgical volume on outcomes for laparoscopic hysterectomy for benign indications. Obstet Gynecol 2012;119:709-16.
Wiser A, Holcroft CA, Tolandi T, Abenhaim HA. Abdominal versus laparoscopic hysterectomies for benign diseases: Evaluation of morbidity and mortality among 465,798 cases. Gynecological surgery 2013;10:117-22.

References
Kosary CL. SEER survival monograph: Cancer survival among adults: U.S. SEER program, 1988-2001, patient and tumor characteristics. In: Ries LAG, Young JL, Keel GE, Eisner MP, Lin DY, Horner MD, editors. Cancer of the corpus uteri. Bethesda (MD): National Cancer Institute, SEER Program, NIH; 2007. p. 123-32.
Raut CP, Nucci MR, Wang Q, Manola J, Bertagnolli MM, Demetri GD, et al. Predictive value of FIGO and AJCC staging systems in patients with uterine leiomyosarcoma. Eur J Cancer 2009;45:2818-24.
Zivanovic O, Leitao MM, Iasonos A, Jacks LM, Zhou Q, Abu-Rustum NR, et al. Stage-specific outcomes of patients with uterine leiomyosarcoma: A comparison of the international federation of gynecology and obstetrics and american joint committee on cancer staging systems. J Clin Oncol 2009;27:2066-72.
Lim D, Wang WL, Lee CH, Dodge T, Gilks B, Oliva E. Old versus new FIGO staging systems in predicting overall survival in patients with uterine leiomyosarcoma: A study of 86 cases. Gynecol Oncol2013;128:322-6.
Briggs AH. Handling uncertainty in cost-effectiveness models. Pharmacoeconomics 2000;17:479-500.
Web Site: The American Congress of Obstetricians and Gynecologists. Power morcellation and occult malignancy in gynecologic surgery: A special report. Available at: http://www.acog.org/Resources_And_Publications/Task_Force_and_Work_Group_Reports/Power_Morcellation_and_Occult_Malignancy_in_Gynecologic_Surgery. Retrieved May 9, 2014
AAGL Advancing Minimally Invasive Gynecologic Surgery Worldwide. AAGL Practice Report: Morcellationduring uterine tissue extraction. J Minim Invasive Gynecol 2014;21:517-30.
Web Site: American Urogynecologic Society. AUGS position statement on power morcellation. Available at: http://www.augs.org/p/bl/et/blogid=16&blogaid=201. Retrieved May 14, 2014.
References
.
Web Site: European Society for Gynecological Endoscopy. Statement on morcellation. Available at: http://www.esge.org/article/218. Retrieved May 2, 2014.
Nieboer TE, Hendriks JC, Bongers MY, Vierhout ME, Kluivers KB. Quality of life after laparoscopic and abdominal hysterectomy: A randomized controlled trial. Obstet Gynecol 2012;119:85-91.
Perron-Burdick M, Yamamoto M, Zaritsky E. Same-day discharge after laparoscopic hysterectomy. ObstetGynecol 2011;117:1136-41.
Hur HC, Donnellan N, Mansuria S, Barber RE, Guido R, Lee T. Vaginal cuff dehiscence after different modes of hysterectomy. Obstet Gynecol 2011;118:794-801.
Koo YJ, Kim DY, Kim JH, Kim YM, Kim YT, Nam JH. Vaginal cuff dehiscence after hysterectomy. Int J Gynaecol Obstet 2013;122:248-52.
Uccella S, Ceccaroni M, Cromi A, Malzoni M, Berretta R, De Iaco P, et al. Vaginal cuff dehiscence in a series of 12,398 hysterectomies: Effect of different types of colpotomy and vaginal closure. ObstetGynecol 2012;120:516-23.
Ritch JM, Kim JH, Lewin SN, Burke WM, Sun X, Herzog TJ, et al. Venous thromboembolism and use of prophylaxis among women undergoing laparoscopic hysterectomy. Obstet Gynecol 2011;117:1367-74.
Harkki-Siren P, Sjoberg J, Kurki T. Major complications of laparoscopy: A follow-up Finnish study. ObstetGynecol 1999;94:94-8.
References
Brown SR, Goodfellow PB. Transverse verses midline incisions for abdominal surgery. Cochrane Database Syst Rev 2005;4:CD005199.
Bickenbach KA, Karanicolas PJ, Ammori JB, Jayaraman S, Winter JM, Fields RC, et al. Up and down or side to side? A systematic review and meta-analysis examining the impact of incision on outcomes after abdominal surgery. Am J Surg 2013;206:400-9.
Le Huu Nho R, Mege D, Ouaissi M, Sielezneff I, Sastre B. Incidence and prevention of ventral incisional hernia. J Visc Surg 2012;149:3-14.
Hussain A, Mahmood H, Singhal T, Balakrishnan S, Nicholls J, El-Hasani S. Long-term study of port-site incisional hernia after laparoscopic procedures. JSLS 2009;13:346-9.
Swank HA, Mulder IM, la Chapelle CF, Reitsma JB, Lange JF, Bemelman WA. Systematic review of trocar-site hernia. Br J Surg 2012;99:315-23.
O'Sullivan AK, Thompson D, Chu P, Lee DW, Stewart EA, Weinstein MC. Cost-effectiveness of magnetic resonance guided focused ultrasound for the treatment of uterine fibroids. Int J Technol Assess Health Care 2009;25:14-25.
Klarenbach S, Manns B, Reiman T, Reaume MN, Lee H, Lloyd A, et al. Economic evaluation of erythropoiesis-stimulating agents for anemia related to cancer. Cancer 2010;116:3224-32.
Chatterjee A, Krishnan NM, Rosen JM. Complex ventral hernia repair using components separation with or without synthetic mesh: A cost-utility analysis. Plast Reconstr Surg 2014;133:137-46.
Spangler EL, Dillavou ED, Smith KJ. Cost-effectiveness of guidelines for insertion of inferior vena cava filters in high-risk trauma patients. J Vasc Surg 2010;52:1537-45.
References
Hynes DM, Stroupe KT, Luo P, Giobbie-Hurder A, Reda D, Kraft M, et al. Cost effectiveness of laparoscopic versus open mesh hernia operation: Results of a department of veterans affairs randomized clinical trial. J Am Coll Surg 2006;203:447-57.
Reichardt P, Leahy M, Garcia Del Muro X, Ferrari S, Martin J, Gelderblom H, et al. Quality of life and utility in patients with metastatic soft tissue and bone sarcoma: The sarcoma treatment and burden of illness in north america and europe (SABINE) study. Sarcoma 2012;2012:740279.
Health Quality Ontario. KRAS testing for anti-EGFR therapy in advanced colorectal cancer: An evidence-based and economic analysis. Ont Health Technol Assess Ser 2010;10:1-49.
Goto A, Takeuchi S, Sugimura K, Maruo T. Usefulness of Gd-DTPA contrast-enhanced dynamic MRI and serum determination of LDH and its isozymes in the differential diagnosis of leiomyosarcoma from degenerated leiomyoma of the uterus. Int J Gynecol Cancer 2002 Jul-Aug;12(4):354-361.
Sato K, Yuasa N, Fujita M, Fukushima Y. Clinical application of dif- fusion-weighted imaging for preoperative differentiation between uterine leiomyoma and leiomyosarcoma. Am J Obstet Gynecol 2014 Apr;210(4):368.e1-368.e8.