hyposplenism as a risk factor of infection, …doc/a-di-sabatino.pdf · igd memory 8.1% mature...
TRANSCRIPT

First Department of Medicine, University of Pavia, Fondazione IRCCS Policlinico S. Matteo, Pavia
Antonio Di Sabatino
HYPOSPLENISM AS A RISK FACTOR OF INFECTION, AUTOIMMUNITY AND
COMPLICATIONS IN COELIAC DISEASE

In 1955, Dameshek coined the term “hyposplenism” to describe a
patient with coeliac disease in whom Howell-Jolly bodies were
detected on peripheral blood smear and an atrophic spleen was
confirmed at post-mortem examination
Since then, hyposplenism has been regarded as an acquired disorder,
potentially associated with several diseases, sometimes
accompanied by a reduction in spleen size, and burdened by the
same complications occurring in surgical asplenia
Definition of hyposplenism
••••
••••
COMPARTMENT
White pulp
Marginal zone
Red pulp
PALS PALS
MZ MZ
STRUCTURE
Cords
Sinus
Follicle
Sinus
A
GCMn
HISTOLOGY
A
PALS
Follicle
MZ
Sinus
Cords
GC
Mn
FUNCTION
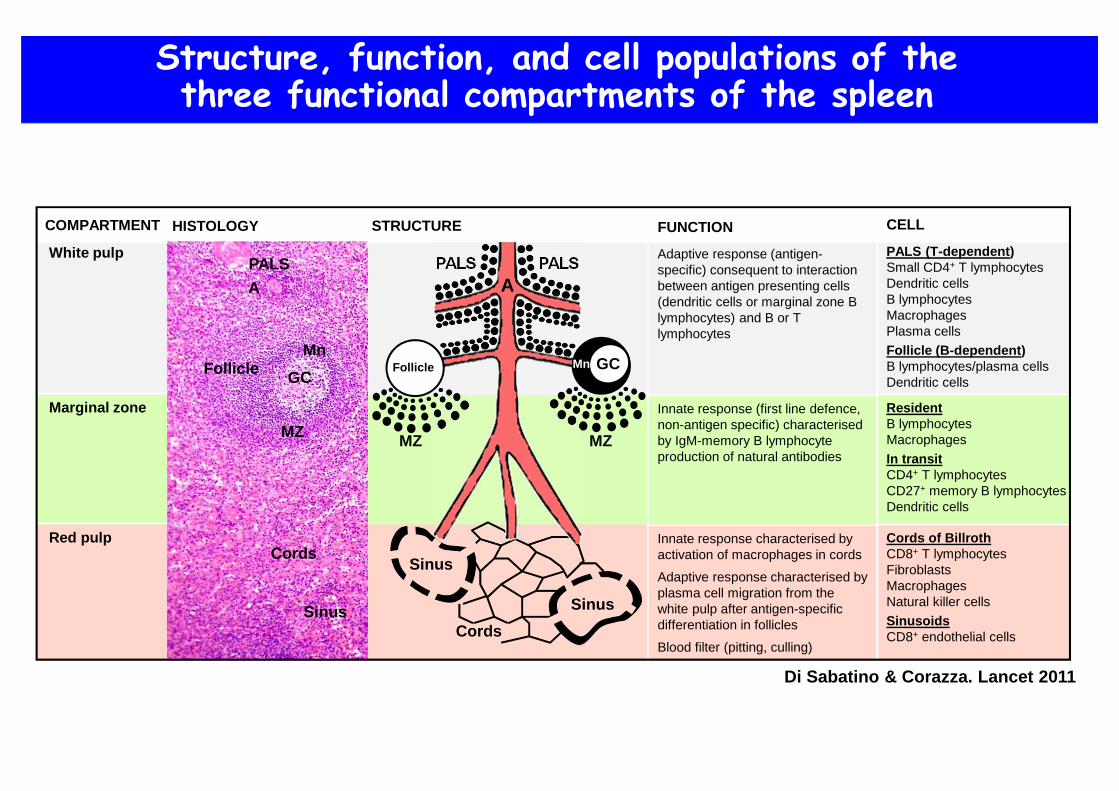
Adaptive response (antigen-specific) consequent to interaction between antigen presenting cells (dendritic cells or marginal zone B lymphocytes) and B or T lymphocytes
Innate response (first line defence, non-antigen specific) characterised by IgM-memory B lymphocyte production of natural antibodies
Innate response characterised by activation of macrophages in cords
Adaptive response characterised by plasma cell migration from the white pulp after antigen-specific differentiation in follicles
Blood filter (pitting, culling)
CELL
PALS (T-dependent)Small CD4+ T lymphocytesDendritic cellsB lymphocytesMacrophagesPlasma cells
Follicle (B-dependent)B lymphocytes/plasma cellsDendritic cells
ResidentB lymphocytesMacrophages
In transitCD4+ T lymphocytesCD27+ memory B lymphocytesDendritic cells
Cords of BillrothCD8+ T lymphocytesFibroblastsMacrophagesNatural killer cells
SinusoidsCD8+ endothelial cells
Structure, function, and cell populations of thethree functional compartments of the spleen
Di Sabatino & Corazza. Lancet 2011
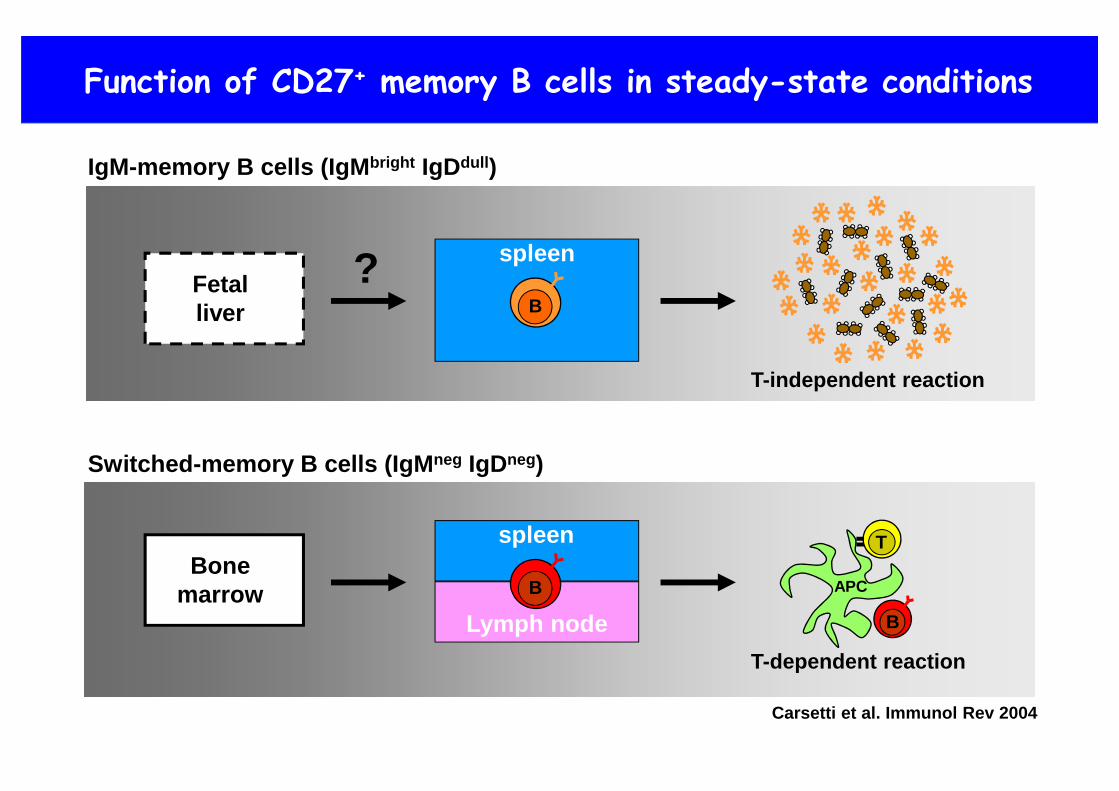
Function of CD27+ memory B cells in steady-state conditions
T
APC
Switched-memory B cells (IgM neg IgDneg)
Bonemarrow B
spleen
Lymph node B
T-dependent reaction
Carsetti et al. Immunol Rev 2004
IgM-memory B cells (IgM bright IgDdull )
Fetalliver B
spleen
T-independent reaction
?

IgM memory B cells controlling Streptococcus pneumoniaeinfections are generated in the spleen
Kruetzmann et al. J Exp Med 2003
100
102
103
101
104
100
102
103
101
104
010
210
310
110
4
memory4.8%
CD27
IgD
CD22
IgM10
010
210
310
110
4
Splenectomizedpatient (SP)
Controlsubject (CS)
memory54.3%
IgM mem3.6%
IgM mem21.5%
Switched Switched
mature mature10
0
104
103
102
100
104
103
102
1010
0
104
103
102
100
104
103
102
0
10
20
% o
f tot
al ly
mph
ocyt
es
SP CS
30
B cells
•••••
•
•
% o
f tot
al B
cel
ls
SP CS
B Memory
10
20%
of t
otal
B c
ells 30
IgM-mem Switched-mem
0
10
20
50
30
40
••••••••••••••••••
••
••••••••••••••••••••••••••••••••
60
••••••••••••••••••••••
•••••
••• •
•••••••••••••••••••••••••••••
p<0.001
0SP CS
••••••••• • •••••••• •• •••• ••• ••••••••
•••••••••••••••••••••••••
0
10
20
% o
f tot
al B
cel
ls
SP CS
30
40
p<0.0001
•••••••••••••••••••••••••••
•••••••••
••••••••••••••••••••••••
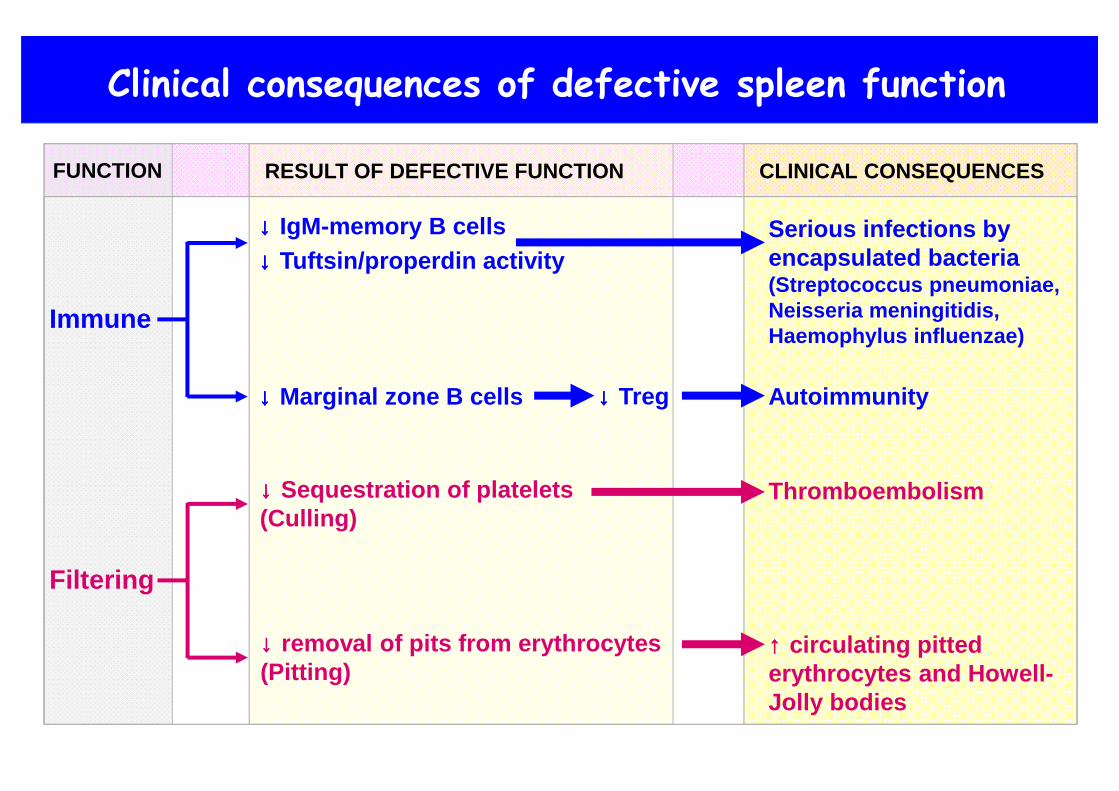
Clinical consequences of defective spleen function
Immune
Filtering
↓↓↓↓ IgM-memory B cells↓↓↓↓ Tuftsin/properdin activity
↓↓↓↓ Marginal zone B cells
↓↓↓↓ Sequestration of platelets(Culling)
FUNCTION RESULT OF DEFECTIVE FUNCTION CLINICAL CONSEQUENCES
Serious infections byencapsulated bacteria(Streptococcus pneumoniae,Neisseria meningitidis,Haemophylus influenzae)
Autoimmunity
Thromboembolism
↓↓↓↓ Treg
↓↓↓↓ removal of pits from erythrocytes(Pitting)
↑↑↑↑ circulating pittederythrocytes and Howell-Jolly bodies

Diagnostic techniques for spleen dysfunction
Di Sabatino & Corazza. Lancet 2011
99Tc Spleen scan Howell-Jolly bodies Pitted red cells

Flow cytometric analysis of IgM-memory B cellsas a diagnostic tool for spleen dysfunction
•• • •••• •
••••••
•••••••••
••••
•••••••
•••••••••
••••
IgM-memory B cells (% total B cells)
0 5 10 15 20 25 30 350
p=0.01
30
0
10
20
p<0.01
Pitt
ed re
d ce
lls (%
)
0 5 10 15 20 25 30 35
10
20 •
30
IgM-memory B cells (% total B cells)
Pitt
ed re
d ce
lls (%
)
SPLENECTOMIZED PATIENTS HYPOSPLENIC PATIENTS
Di Sabatino et al. Am J Gastro 2005
4 4
•
•
•
•••
•
•
••
•
• •
•
••
••
• •

Natural history of splenic hypofunction
0
4
8
Pitt
ed r
ed c
ells
(%
)
12
10
6
2
14
Pre-ifx Post-ifx
•
p<0.01
••
•
• •
•
••
•
•
•
•
••
•
•
•
•
•
0
4
8P
itted
red
cel
ls (
%)
12
10
6
2
14
Pre-ifx Post-ifx
REVERSIBLEHYPOSPLENISM
IRREVERSIBLEHYPOSPLENISM
SPLENICATROPHY
••
•
•
• •
•
••••
•
Responder Crohn’s disease pts Non-responder Crohn’s disease pts
Di Sabatino et al. IBD 2008Di Sabatino et al. IBD 2008
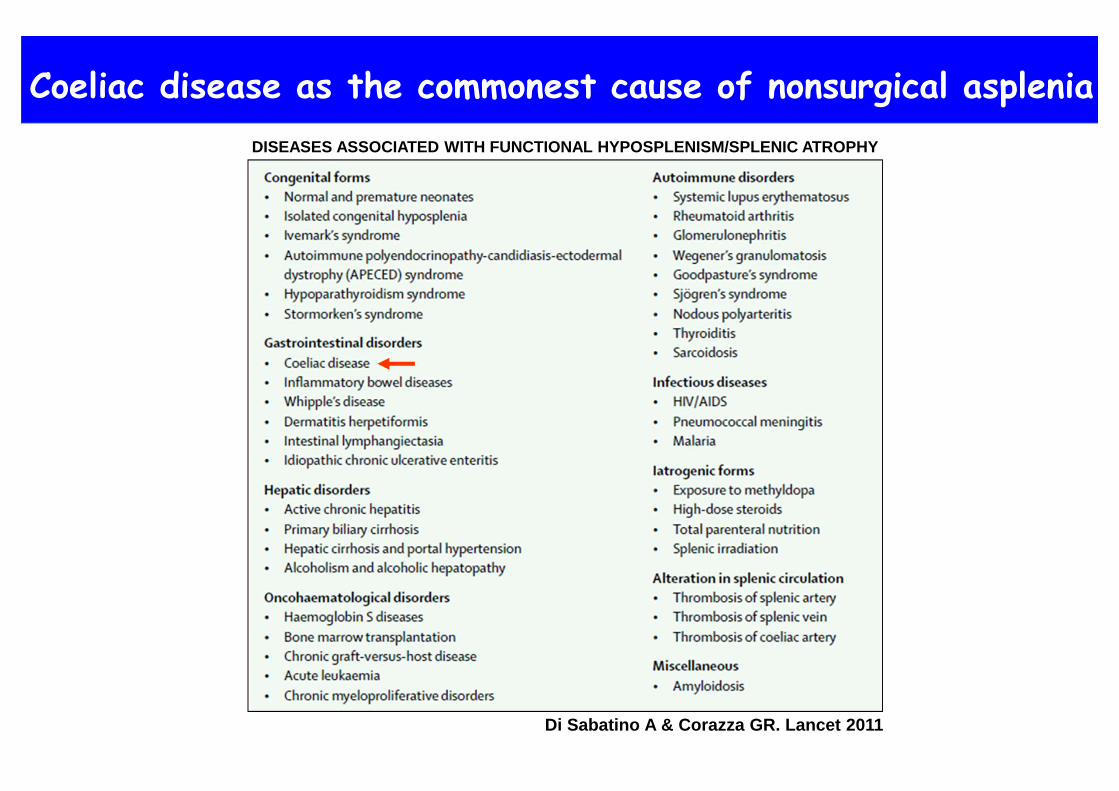
DISEASES ASSOCIATED WITH FUNCTIONAL HYPOSPLENISM/SPLENIC ATROPHY
Coeliac disease as the commonest cause of nonsurgical asplenia
Di Sabatino A & Corazza GR. Lancet 2011
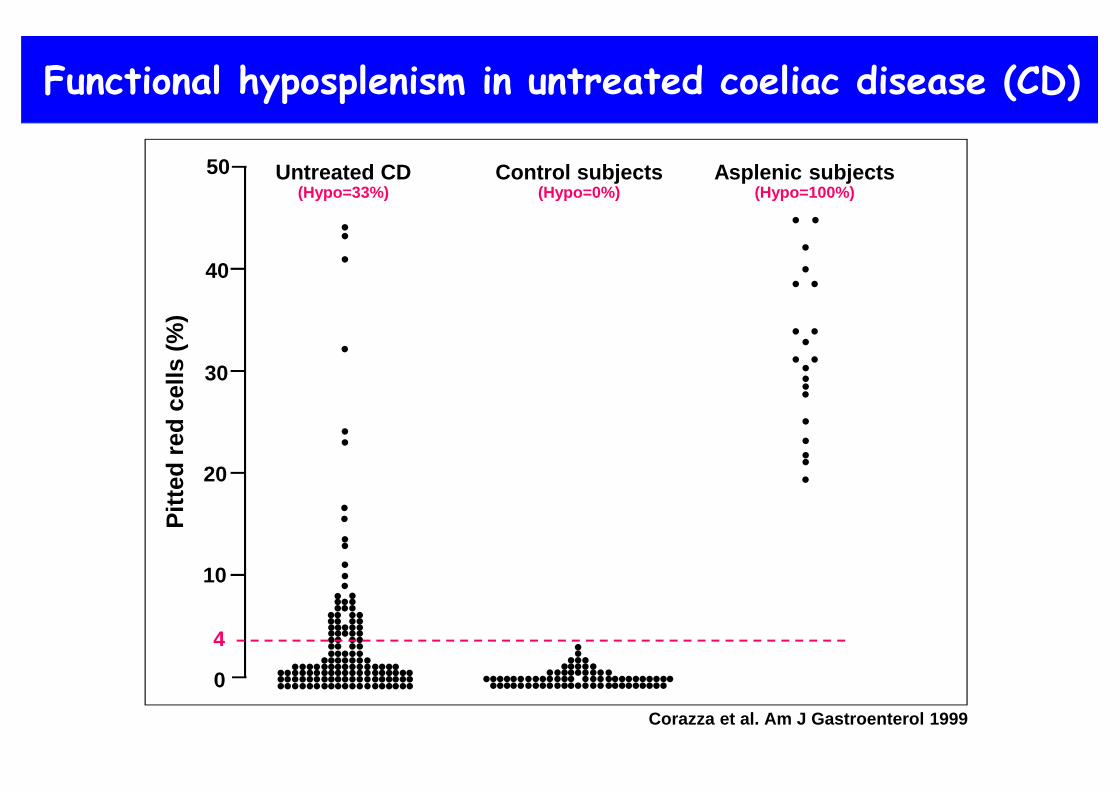
Functional hyposplenism in untreated coeliac disease (CD)
• • •• • ••• •• • • ••• ••• •• • •• • ••• •• • • ••• ••• •• • •• • ••• •• • • ••• ••• •• • •• •• •• • •• ••• •• ••• •• •• ••••• •••• •••
0
10
20
30
40
50
• •••• •••••• •••• ••• ••••••
•••
•
••
•••
••
•
•••
• • •• • ••• •• • ••• ••• •• • ••• ••• •• • •• • ••• •• • ••• ••• •• •••
•• •••••
• •• •• •• •• ••• ••
•••
••
••••••
•••
••••••
Pitt
ed r
ed c
ells
(%
)Untreated CD
(Hypo=33%)Control subjects
(Hypo=0%)Asplenic subjects
(Hypo=100%)
4
Corazza et al. Am J Gastroenterol 1999
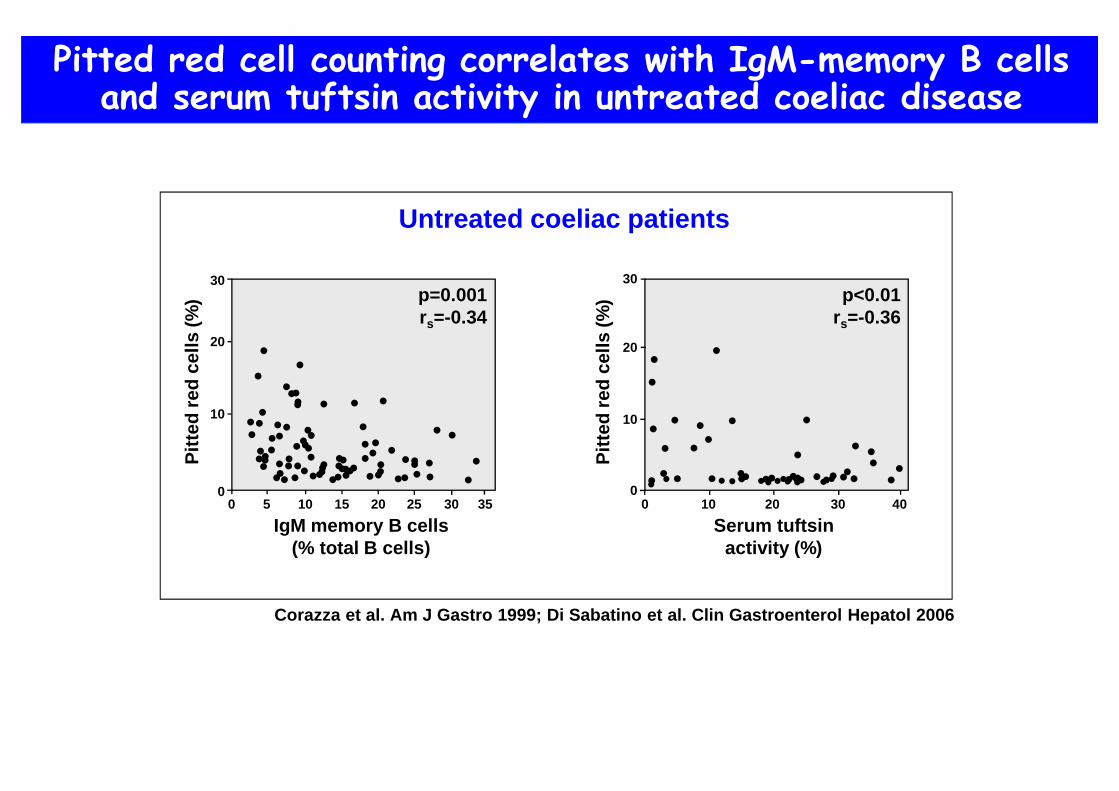
Pitted red cell counting correlates with IgM-memory B cellsand serum tuftsin activity in untreated coeliac disease
•• ••••• • • •• •
••••
••••••
•••
•••• ••
••••••••••••••••
•••••
••••••• ••••
••••••••
••••••
0 5 10 15 20 25 30 350
• •
••
•
••
•
• ••••
•• • • ••••
• ••
• • •••
•••••••••••••••• ••••0 10 20 30 40
0
10
20
30
10
20 •
30p=0.001rs=-0.34
p<0.01rs=-0.36
Pitt
ed re
d ce
lls (%
)
Pitt
ed re
d ce
lls (%
)
Serum tuftsinactivity (%)
IgM memory B cells(% total B cells)
Corazza et al. Am J Gastro 1999; Di Sabatino et al. Clin Gastroenterol Hepatol 2006
Untreated coeliac patients

30
20
10
0
Controlsubjects
Pitt
ed re
d ce
lls (%
)
••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••
••••
••••
••••••••••••••••••••••••••••••••••••
••••••••
EFFECT OF AGE AT ONSET
Corazza et al. Gut 1982
30
20
10
0
40
60
50
70
Hyp
ospl
enic
coe
liacs
(%)
Age (years)
15/19 20/29 30/39 40/49 50/59 60/69 >69
Age at study
Age at diagnosis
EFFECT OF AGE AT DIAGNOSIS
Effect of age at onset, age at diagnosisand gluten-free diet in patients with coeliac disease
EFFECT OF GLUTEN-FREE DIET
••••
••••
•••• ••••••••••••
••••••••••••
••••••••
••••••••••••••••
••••••••
••••
•••••••••••• ••••••••
••••••••••••
•••• •••• ••••••••
Pitt
ed re
d ce
lls (%
)
3
2
10
5
4
30
25
2015
40
35
0 2 4 6 8 10 12
Months of gluten-free diet
p<0.005
Coeliacchildren
Asplenicsubjects
4
Corazza et al. Am J Gastro 1999 Corazza et al. Gut 1983

0
10
20
Pitt
ed r
ed c
ells
(%
)
30
25
15
5
35
Splenectomizedpatients
(Hypo=100%)
CD patientswithout AID(Hypo=19%)
CD patientswith AID
(Hypo=59%)
••• •••
••
•
••••••
•
••
•••
••••
•
•
HealthyVolunteers(Hypo=0%)
••• •• ••••••••••• •• •••
•••••••
•• •
•
•
•••
•
••
•••••• •••• ••• •••• •• •••
••
••
••
•••••
•
•••••
•••••• ••• •••••
•
••••
•
•
Di Sabatino et al. Clin Gastroenterol Hepatol 2006
Splenic hypofunction and coeliac disease (CD)-associated autoimmune disorders (AID)
4
Di Sabatino et al. Clin Gastroenterol Hepatol 2006
10010
210
310
110
4
100
102
103
101
104 10
010
210
310
110
4
10010
210
310
110
4 10010
210
310
110
4
100
102
103
101
104
CD
27Ig
D
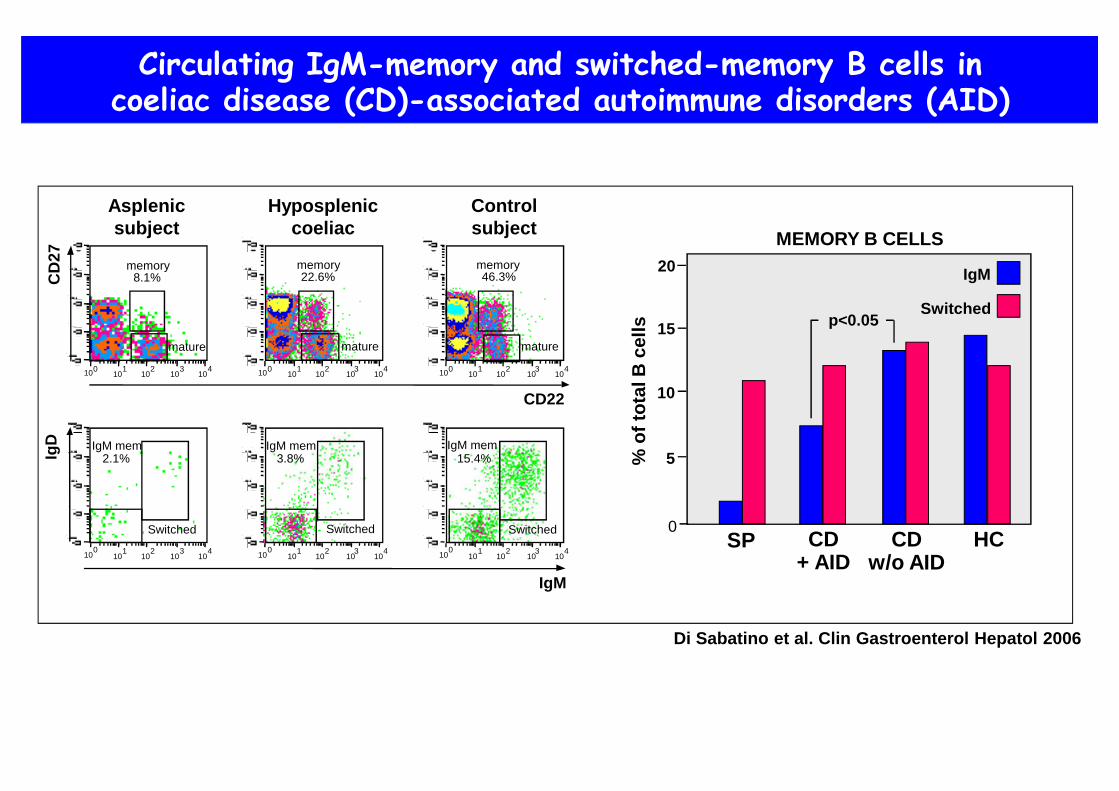
memory8.1%
mature
memory22.6%
mature mature
memory46.3%
IgM mem2.1%
Switched
IgM mem3.8%
IgM mem15.4%
Switched Switched
IgM
CD22
Asplenicsubject
Hypospleniccoeliac
Controlsubject
5
10
% o
f tot
al B
cel
ls 15
MEMORY B CELLS
0SP CD
+ AIDCD
w/o AIDHC
20
Circulating IgM-memory and switched-memory B cells incoeliac disease (CD)-associated autoimmune disorders (AID)
IgM
Switchedp<0.05
Di Sabatino et al. Clin Gastroenterol Hepatol 2006
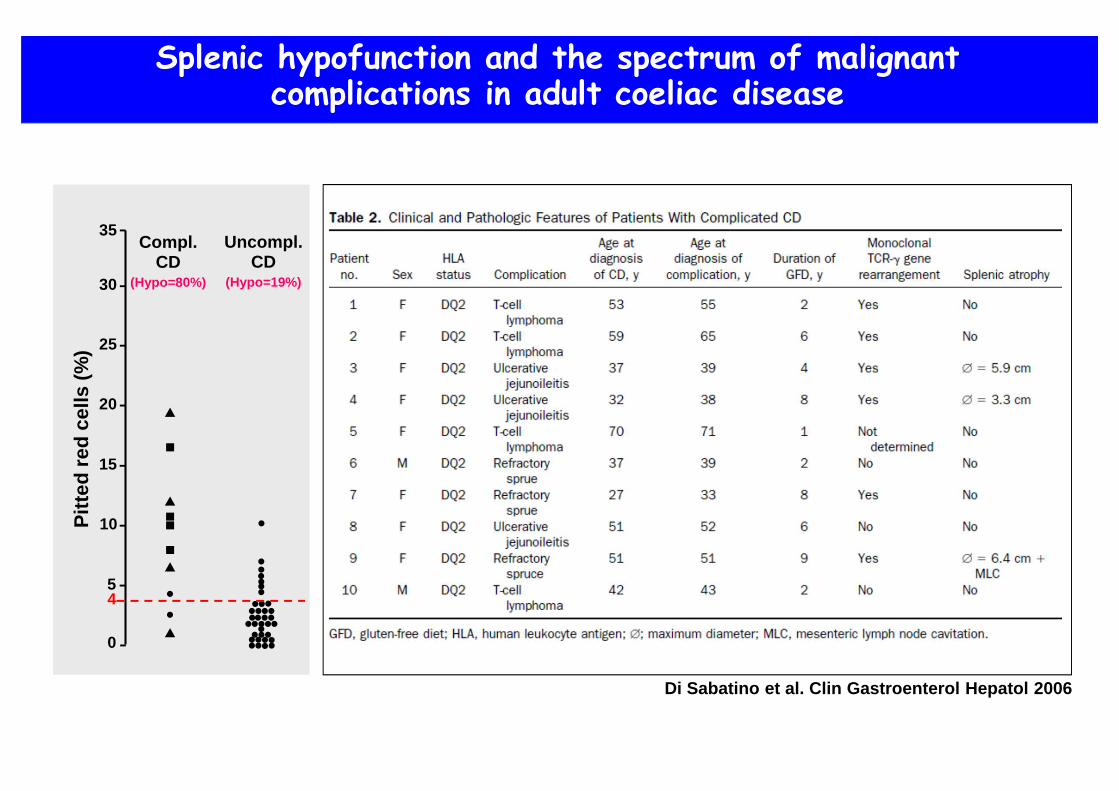
Splenic hypofunction and the spectrum of malignantcomplications in adult coeliac disease
0
10
20
Pitt
ed r
ed c
ells
(%
)
Uncompl.CD
(Hypo=19%)30
25
15
5
35
•••
•
••
••••••••••• ••••••• ••••
••
•
••••
••
Compl.CD
(Hypo=80%)
4
Di Sabatino et al. Clin Gastroenterol Hepatol 2006
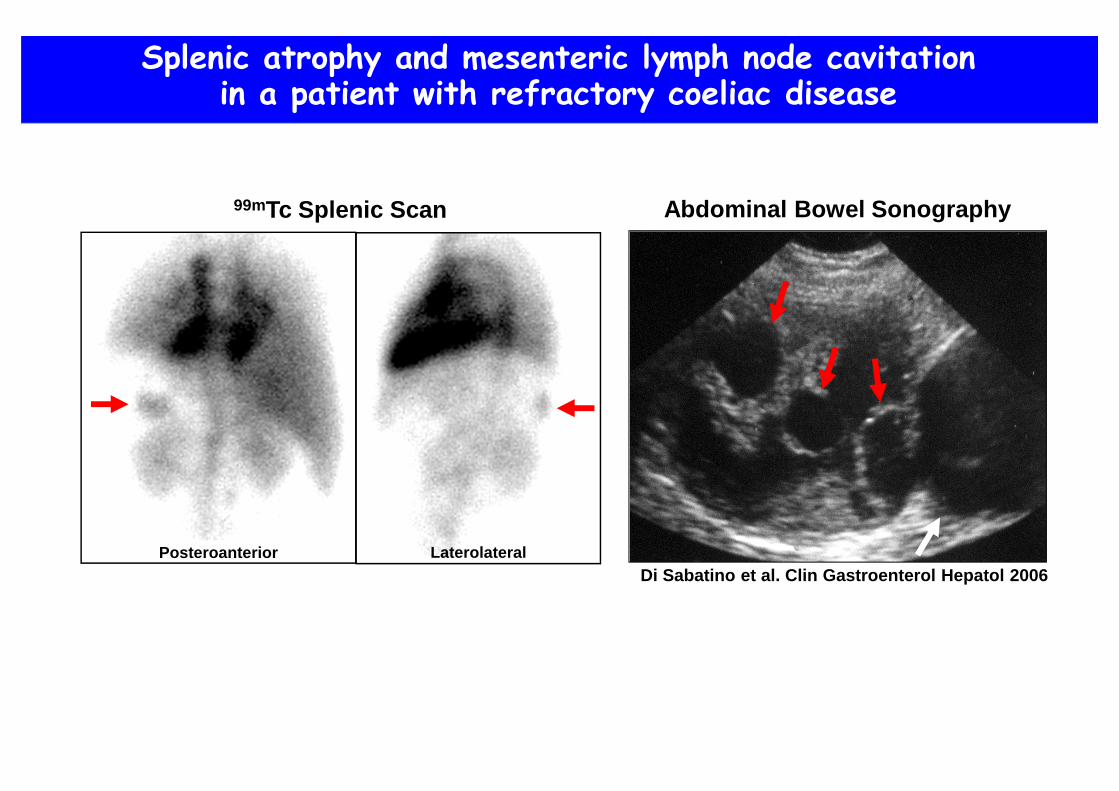
Splenic atrophy and mesenteric lymph node cavitationin a patient with refractory coeliac disease
Abdominal Bowel Sonography99mTc Splenic Scan
Posteroanterior Laterolateral

CD
45R
OC
D20
Controlsubject
Coeliacpatient
Control-PBL CD-PBL
Control-SPL CD-SPL
CD19+
CD19+
CD21bright
CD19+
CD27+
CD
27C
D27
IgD
0
2
4
6
8
10
12
Imm
unog
lobu
lins
(µµ µµg
/ml)
IgMIgA
IgG
Controlsubject
Coeliacpatient
Response to CpG-ODN
IgM
Splenic atrophy and coeliac disease.Morphological and functional aspects
Di Sabatino et al. J Allergy Clin Immunol 2007
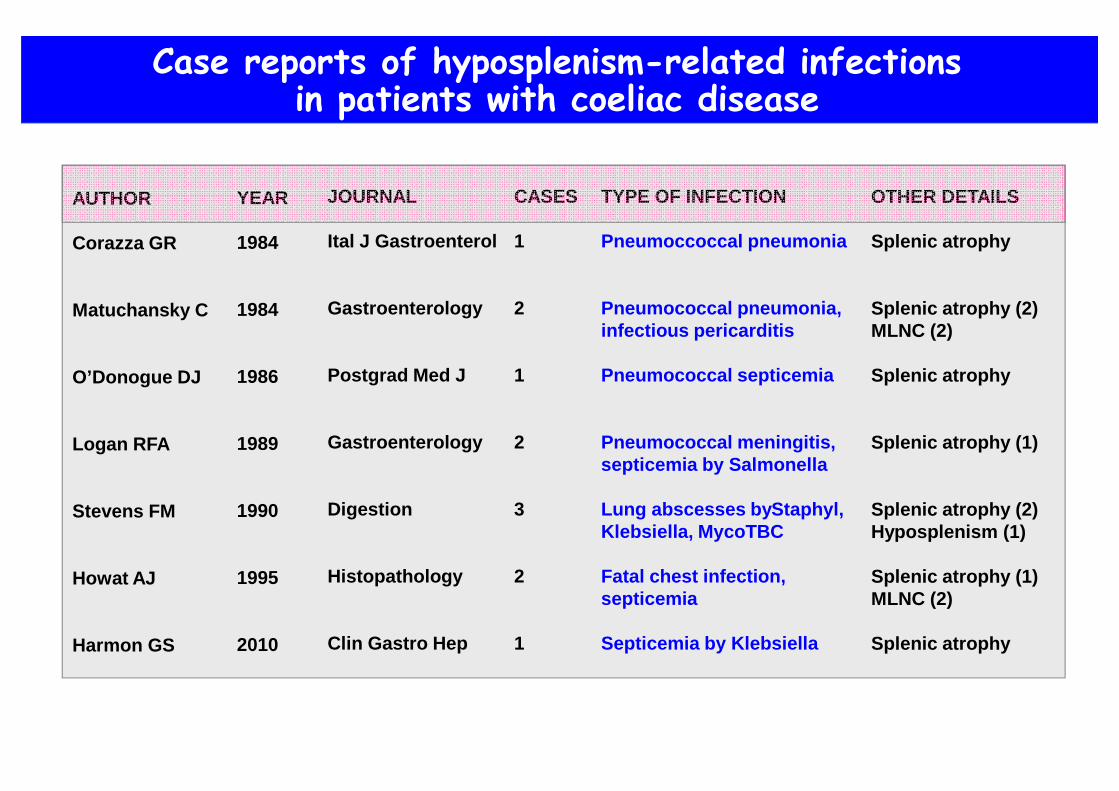
Case reports of hyposplenism-related infectionsin patients with coeliac disease
AUTHOR
Corazza GR
Matuchansky C
O’Donogue DJ
Logan RFA
Stevens FM
Howat AJ
Harmon GS
YEAR
1984
1984
1986
1989
1990
1995
2010
JOURNAL
Ital J Gastroenterol
Gastroenterology
Postgrad Med J
Gastroenterology
Digestion
Histopathology
Clin Gastro Hep
CASES
1
2
1
2
3
2
1
TYPE OF INFECTION
Pneumoccoccal pneumonia
Pneumococcal pneumonia,infectious pericarditis
Pneumococcal septicemia
Pneumococcal meningitis,septicemia by Salmonella
Lung abscesses by Staphyl,Klebsiella, MycoTBC
Fatal chest infection,septicemia
Septicemia by Klebsiella
OTHER DETAILS
Splenic atrophy
Splenic atrophy (2)MLNC (2)
Splenic atrophy
Splenic atrophy (1)
Splenic atrophy (2)Hyposplenism (1)
Splenic atrophy (1)MLNC (2)
Splenic atrophy

Ludvigsson et al. Gut 2008
vs general population
vs hospitalized patients Sepsis Hip
fracture Lymphoma
0
20
40
60
80
100
Abs
olut
e R
isk
Walters et al. Gut 2008
Risk for pneumococcal sepsis in coeliac disease
Thomas et al. EJGH 2008
0
1
2
3
4
5Coeliacpatients
Asplenicpatients
Rel
ativ
e R
isk
0
1
2
3
4
5
Rel
ativ
e R
isk
p<0.001p<0.01
15,325 coeliac patients14,494 hospitalized patients
2,044 coeliac patients
2,956 asplenic patients

Peters et al. Arch Intern Med 2003
0
5
10
Sta
ndar
dize
d M
orta
lity
Rat
io
Allinfections
15
2.9
Septicemia
7.1
Allmalignancies
1.7
Respiratorydiseases
2.8
Pneumonia
2.9
Septicemia and pneumonia as frequent causes of deathin coeliac patients: the Swedish cohort (10,032 pts)

80
0
60
40
20
% v
acci
nate
d pa
tient
s
2001 2002 2003 2004 2005 2001 2002 2003 2004 2005
Splenectomy(n. 2,001)
Coeliac disease / sickle cell anemia(n. 3,584)
Pebody et al. Epidemiol Infect 2008
Use of anti-pneumococcal vaccines in at risk populationsin UK (Q-research database 2001-2005)

Traditional polysaccharide and new conjugate anti-pneumococcal vaccines
used in the prophylactic management of asplenic/hyposplenic patients
VACCINE
PPV23
PCV13
BRAND NAME
Pneumovax®
Prevnar®
MECHANISM
T-cell independent
T-cell dependent
SEROTYPES
1, 2, 3, 4, 5, 6B, 7F, 8, 9N, 9V, 10A, 11A, 12F, 14, 15B,17F, 18C, 19A, 19F,20, 22F, 23F, 33F
1, 3, 4, 5, 6A, 6B,7F, 9V, 14, 18C,19A, 19F, 23F
STRUCTURE
Polysaccharide
Protein-conjugate(CRM197 protein)
INDICATIONS
- Asplenic or hyposplenicadults
- Asplenic or hyposplenicchildren > 5 yrs
- Asplenic or hyposplenicchildren < 5 yrs
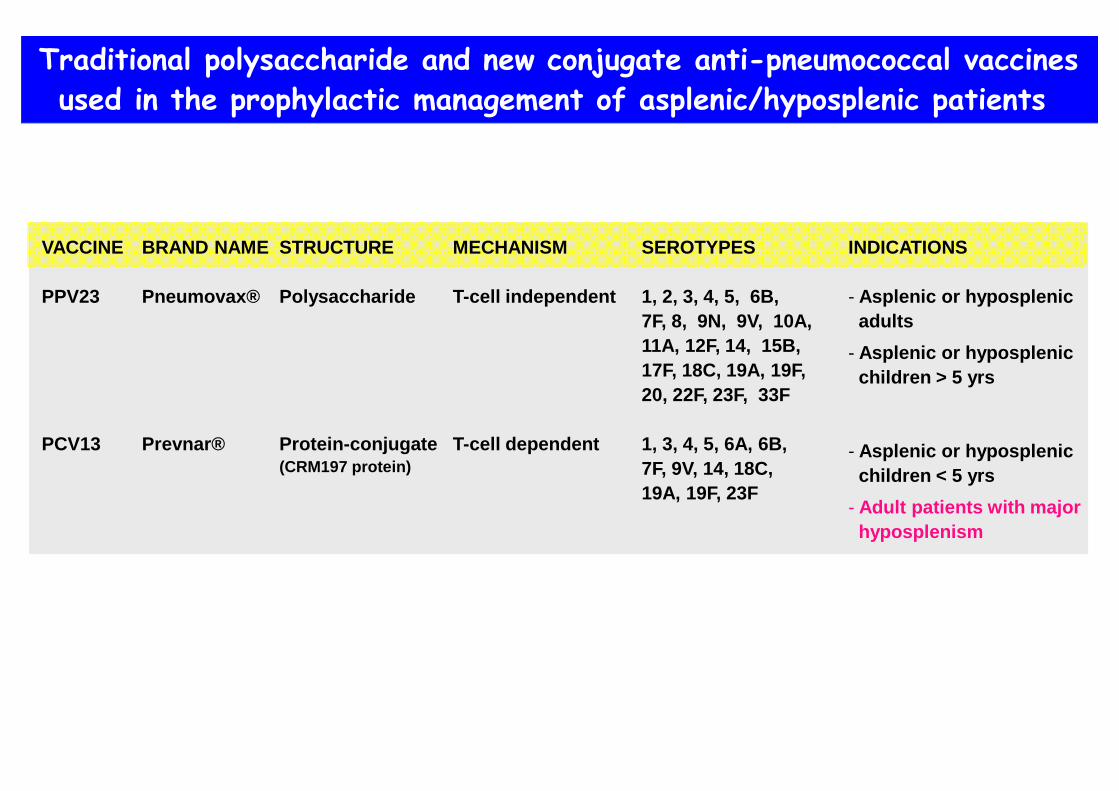
Traditional polysaccharide and new conjugate anti-pneumococcal vaccines
used in the prophylactic management of asplenic/hyposplenic patients
VACCINE
PPV23
PCV13
BRAND NAME
Pneumovax®
Prevnar®
MECHANISM
T-cell independent
T-cell dependent
SEROTYPES
1, 2, 3, 4, 5, 6B, 7F, 8, 9N, 9V, 10A, 11A, 12F, 14, 15B,17F, 18C, 19A, 19F,20, 22F, 23F, 33F
1, 3, 4, 5, 6A, 6B,7F, 9V, 14, 18C,19A, 19F, 23F
STRUCTURE
Polysaccharide
Protein-conjugate(CRM197 protein)
INDICATIONS
- Asplenic or hyposplenicadults
- Asplenic or hyposplenicchildren > 5 yrs
- Asplenic or hyposplenicchildren < 5 yrs
- Adult patients with majorhyposplenism

Asplenia/hyposplenism-related thromboembolism
� Splenectomy
� Coeliac disease
� Inflammatory bowel disease
� Whipple’s disease p=0.007rs=0.66
Platelet count (x10 3/µµµµl)
Pitt
ed r
ed c
ells
(%
)
Di Sabatino et al. Am J Gastro 2009

Risk of thromboembolism in 14,207 patients withcoeliac disease versus 69,048 matched reference individuals
Ludvigsson et al. Br J Haematol 2007
0
1
2H
azar
d ra
tios
Referenceindividuals
Coeliacpatients
1.86
p<0.001
0-15 yrs ≥16 yrs
1.97
p<0.001
Age at diagnosis

Critical issues in coeliac disease-associated hyposplenism
1. When to evaluate splenic function
2. How to measure splenic function
3. When to recommend prophylactic vaccination
4. What is the cause of hyposplenism
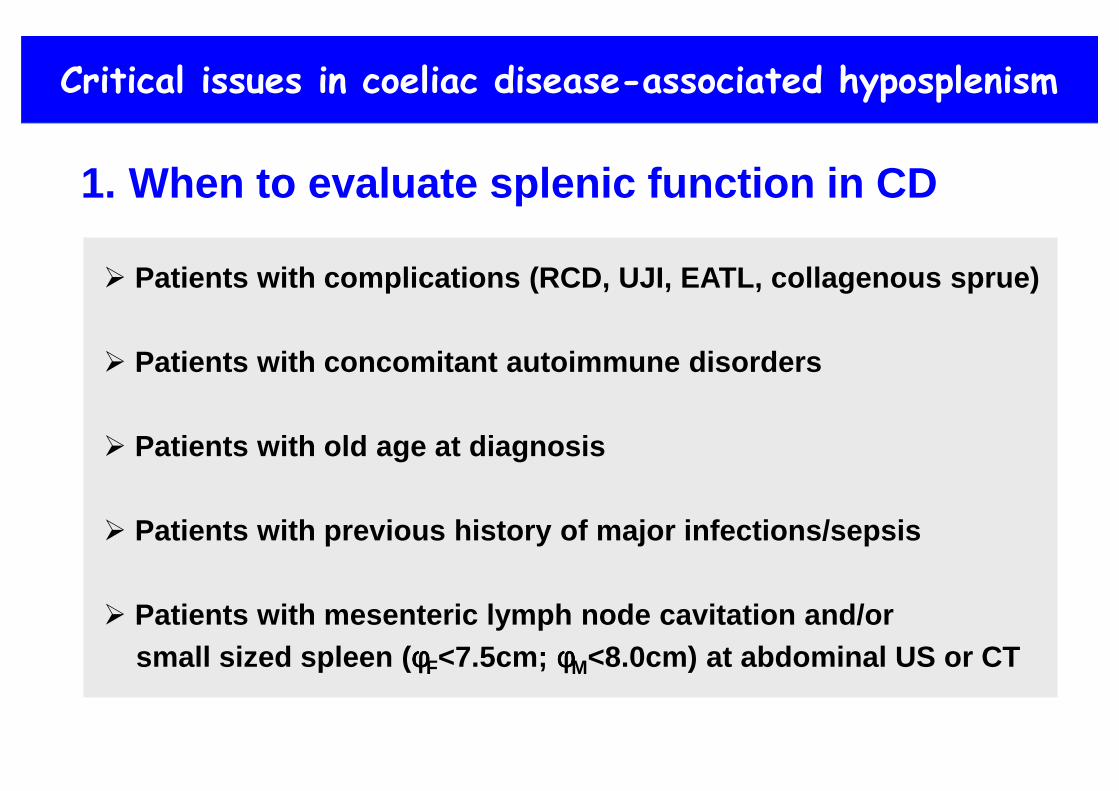
Critical issues in coeliac disease-associated hyposplenism
1. When to evaluate splenic function in CD
� Patients with complications (RCD, UJI, EATL, collagenous sprue)
� Patients with concomitant autoimmune disorders
� Patients with old age at diagnosis
� Patients with previous history of major infections/sepsis
� Patients with mesenteric lymph node cavitation and/orsmall sized spleen ( φφφφF<7.5cm; φφφφM<8.0cm) at abdominal US or CT

Two-thirds of individuals with small sized spleen (φφφφF<7.5cm; φφφφM<8.0cm)incidentally detected at abdominal US are hyposplenic
0
12
16
20
24
28
Splenectomized patients(n=52)
Patients with small sized spleen(n=128)
4
8
Pitt
ed r
ed c
ells
(%
)85 hyposplenic patients
Di Sabatino et al. Intern Emerg Med 2011

Critical issues in coeliac disease-associated hyposplenism
2. How to measure splenic function
� Pitted red cell counting by phase-interference microscopy
� Flow cytometric analysis of circulating memory B cells
� Flow cytometric detection of circulating Howell-Jolly bodies
•
•
•
•• •
••
•
•
•20 25 30
1.0
0.5
1.5
% PITTED RED CELLS
% H
JB (
CD
71- /T
OP
RO
+ ) p=0.0128rs=0.73
Splenectomized
10 15
0.2
0.1
0.3
% PITTED RED CELLS
p=0.002rs=0.83
Hyposplenic••• •
• •• •
•
• •

Critical issues in coeliac disease-associated hyposplenism3. When to recommend prophylactic vaccination
IgM-memory B cells (% total B cells)
0 10 20 300
30
0
10
20 •
Pitt
ed re
d ce
lls (%
)
•
0 10
•
•••
•
•
••
•
• •
•
••
••
20 30
20
30
IgM-memory B cells (% total B cells)
Pitt
ed re
d ce
lls (%
)
• •
SPLENECTOMIZED PATIENTS HYPOSPLENIC COELIAC PATIENTS
4 4
10
••
••
••• •
•
••
•
•• ••
•
••
••
••••
•• •
•
•• •
To clarify mutual connections between spleen and gut
4. What is the cause of hyposplenism
Spleen
Gut
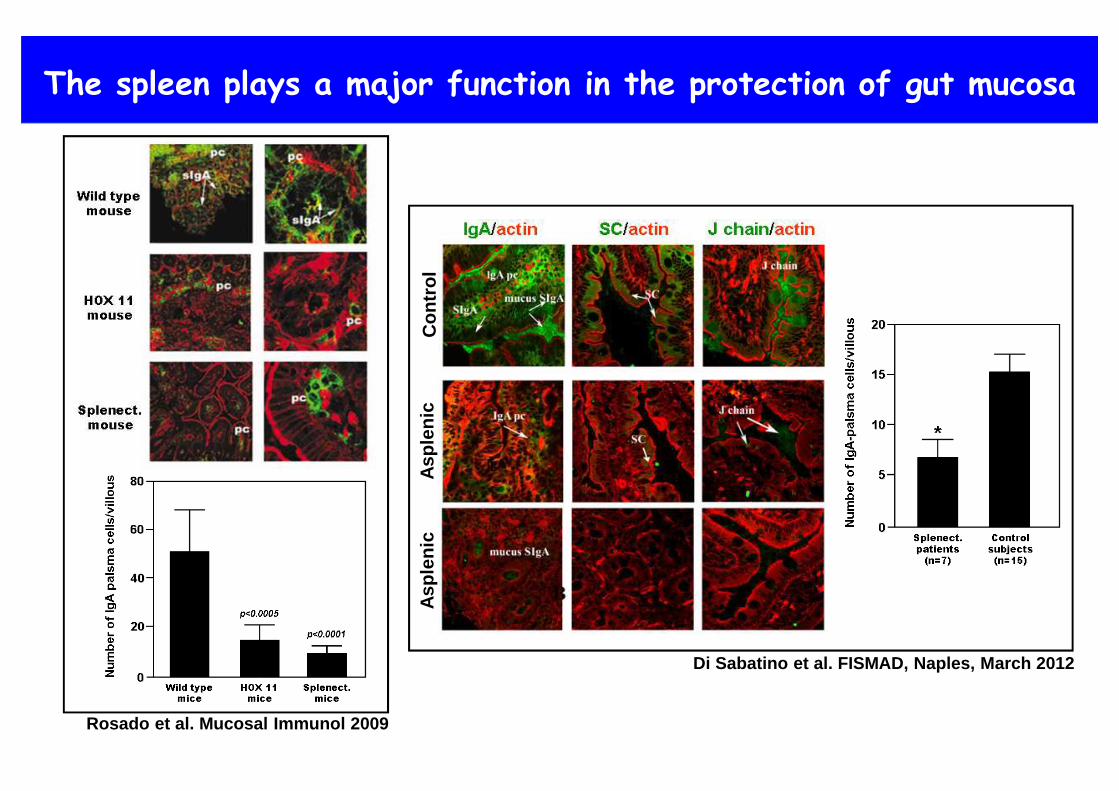
The spleen plays a major function in the protection of gut mucosa
Rosado et al. Mucosal Immunol 2009
Di Sabatino et al. FISMAD, Naples, March 2012
Con
trol
Asp
leni
cA
sple
nic

Oral tolerance to deamidated gliadin in HLA-DQ2 transgenic miceis predominantly mounted in the spleen
Du Pré et al. Gastroenterology 2011
Deamidated gliadin Ovalbumine


Response to pneumococcal vaccine in 10 patients with coeliac disease
Num
ber
of s
erot
ypes
in w
hich
pts
achi
eved
a 2
-fol
d ris
e in
ant
ibod
y le
vels
1
2
3
4
5
6
7
8
9
10
11
12
0Pt.#1 Pt.#2 Pt.#3 Pt.#4 Pt.#5 Pt.#6 Pt.#7 Pt.#8 Pt.#9 Pt.#10
Eusplenic coeliac patients Hyposplenic coeliac patients
McKinley et al. J Clin Gastroenterol 1995