hypocomplementemic urticarial vasculitis.case report
TRANSCRIPT


Hypocomplementemic UrticarialVasculitis.Case Report.
• Azad A. Haleem1 , Mehvan Sh. Abdulrahman2
,Aziz B Abdulaziz3
• 1.Pediatrician &Lecturer at college of Medicine, University of Duhok/Kurdistan/Iraq.
2.Pediatric SHO in Heevi pediatrics teaching hospital, Duhok/Kurdistan/Iraq.
3. Pediatrician in Amedi hospital Duhok/Kurdistan/Iraq


Case Summary
Elevent years old girl ………
• Presented with frequent attacks of spontaneous Urticarial rash on the trunk and extremities when she was three years old,
• firstly diagnosed as a case of allergy treated by Antihistamine and sort course of steroids but unfortunately without benefits.

• After four months she developed urticarialrash and painful swelling of the joints in the upper and lower extremities, for that she received one course ( one month ) of prednisolone without knowing the definitive diagnosis became better but after stopping prednisolone the condition reappeared again.

• At the age of four years they consulted a doctor who diagnosed her as a case of SLEdepending on clinical features and simple labs test and the patient received Methotrexateand NSAID, on treatment the patient became well for one year.
• Then the family stopped the treatment suddenly because of family problem and economic problems.

• After one month the patient develop hematuria, hypertension and renal impairment admitted to hospital on conservative management ; Prednisolone, Amlodipin and Hydroxychloroquine.
• after discharge again the patient received Methotrexate till the age of 7 years.

• After that the patient did not become well with recurrent attack of urticaria, arthritis, and lower respiratory tract infections with frequent admissions to hospital.

• At the age of 8.5 years one doctor alter the diagnosis to Polyarteritis nodosa and put her on Azathioprine and small dose of prednisolone, but unfortunately she deteriorated more and did not respond to treatment.

• At the age of 9 years another doctor changed the diagnosis toward Churg-strauss disease and put the patient on Cyclophosphamide but without benefit.

• At the age of 10 years the patient admitted to Heevi pediatric hospital because of lower respiratory tract infection and hematuria, again unfortunately she had renal failure and bronchiectasis for which she was treated in ICU , became better after three weeks of intensive treatment.
On further enquiry
• By complete assessment of patient regarding history, physical examination and farther investigations , depending on clinical criteria and lab tests including serum complement level and renal biopsy.


Diagnosis…..

Treatment:
• She was treatment with hydroxychloroquineand Azathioprine with close observation and follow up.
• Now she is well …

Conclusion
• This case illustrates a young female with Hypocomplementemic Urticarial Vasculitistreated by many doctors in different places with variety of medications with wrong diagnoses.

Some theory …..

Vasculitis
• What is Vasculitis?
• The term vasculitis means inflammation of the wall of blood vessels. Various sizes of blood vessels may be involved.

How Common is Vasculitis in Children?
• Vasculitis are rare in the paediatric age group with varied incidence.
• Although many vasculitides affect both adults and children, some such as KD occur almost exclusively in childhood.
• On the other hand, temporal arteritis does not occur in children.

How Common is Vasculitis in Children?
• Only Henoch Schonlein purpura (HSP) and Kawasaki disease (KD) are more common in children than in adults, with each one affecting at least 10–20/100,000 pediatric patients per year.
• Systemic polyarteritis nodosa (PAN) is also rare in childhood with an estimated incidence of one per one million children.

How is Vasculitis Classified in Children?
• This schema uses vessel size for classification purposes
• The aorta and its main branches are termed large vessels; • The first branches of the aorta e.g., renal, mesenteric, coronary
vessels are regarded as mid-sized;• arterioles, capillaries and venules are regarded as small-sized;
granulomatous and non-granulomatous varieties.
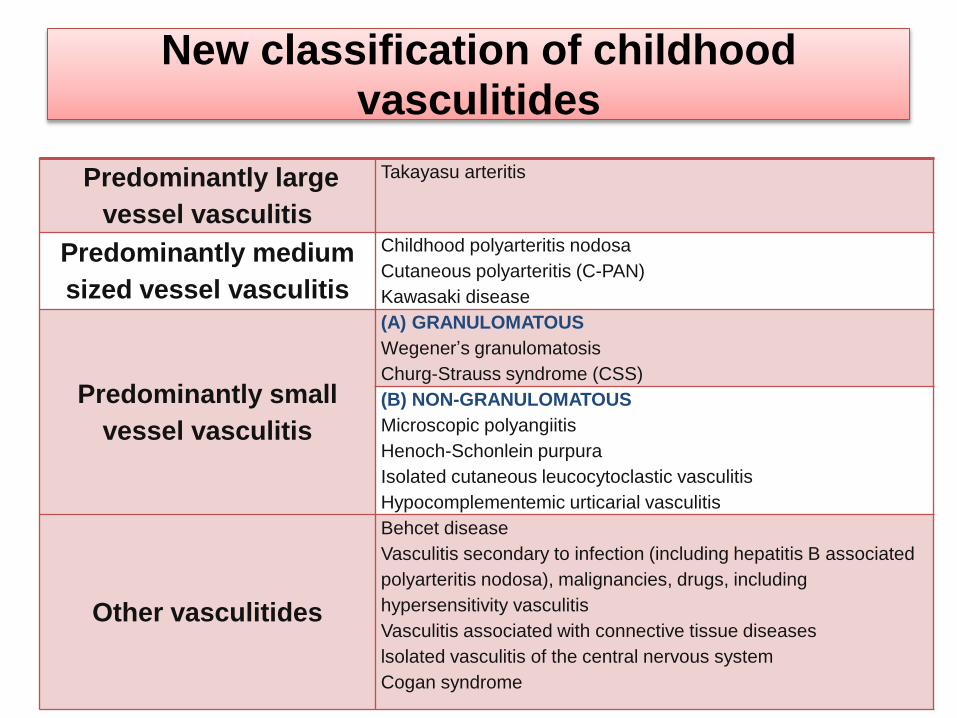
New classification of childhood vasculitides
Predominantly large
vessel vasculitis
Takayasu arteritis
Predominantly medium
sized vessel vasculitis
Childhood polyarteritis nodosa
Cutaneous polyarteritis (C-PAN)
Kawasaki disease
Predominantly small
vessel vasculitis
(A) GRANULOMATOUS
Wegener’s granulomatosis
Churg-Strauss syndrome (CSS)
(B) NON-GRANULOMATOUS
Microscopic polyangiitis
Henoch-Schonlein purpura
Isolated cutaneous leucocytoclastic vasculitis
Hypocomplementemic urticarial vasculitis
Other vasculitides
Behcet disease
Vasculitis secondary to infection (including hepatitis B associated
polyarteritis nodosa), malignancies, drugs, including
hypersensitivity vasculitis
Vasculitis associated with connective tissue diseases
lsolated vasculitis of the central nervous system
Cogan syndrome

When Should a Pediatrician Suspect Vasculitis in a Child?
• As a general rule, it would be appropriate to suspect vasculitis when confronted with multi-organ manifestations.
• in the presence of constitutional features such as fever, weight loss, fatigue, myalgia
• with the presence of inflammatory markers such as anemia, leukocytosis, thrombocytosisand a raised erythrocyte sedimentation rate (ESR).

Multisystem manifestations of systemic vasculitisOrgan/system
involved
Manifestation
Skin and mucosa Oral / nasal ulcers ,Exanthema, Livedo reticularis, Purpura,
Panniculitis, Nodules, Edema, Superficial ulcers, Deep ulcers,
Gangrene
Joints and Muscles Arthralgias / it is, Myositis
Kidneys and Genitals Hypertension, Hematuria, Proteinuria, Epidydymoorchitis
GI Tract Abdominal pain /colic, GI bleed, Gut infarction/, perforation,
Intussusception
ENT Epistaxis, Nasal septal perforation, Pan sinusitis /chronic ear
discharge, Sudden onset deafness, vertigo, Subglottic stenosis
Heart Myocardial infarction, cardiomyopathy ,Pericarditis, valvular
incompetence, bruits, Absent pulses,Hypertension, Discrepant
blood pressure, Claudication, Raynauds
Brain and Nerves Stroke, meningo-encepahilitis,cranial nerve palsy,paraparesis,
focal deficits, Mononeuritis multiplex
Eyes Painful red eye, Uveitis, keratoconjunctivitis, Sudden blindness,
Fundoscopic abnormalities e.g. exudates, hemorrhage
Lungs Tracheal stenosis, Hemoptysis, pulmonary hypertension, Nodules,
cavities, infiltrates Asthma , serositis

Investigative Approach for a Child with Vasculitis
• Radiology
• Digital Subtraction Angiography (DSA)
• MR Angiogram (MRA)
• Computerised Tomography (CT) and Ultrasonography (USG)
• 2 D Echocardiogram
• Serology
• Histology - Biopsy
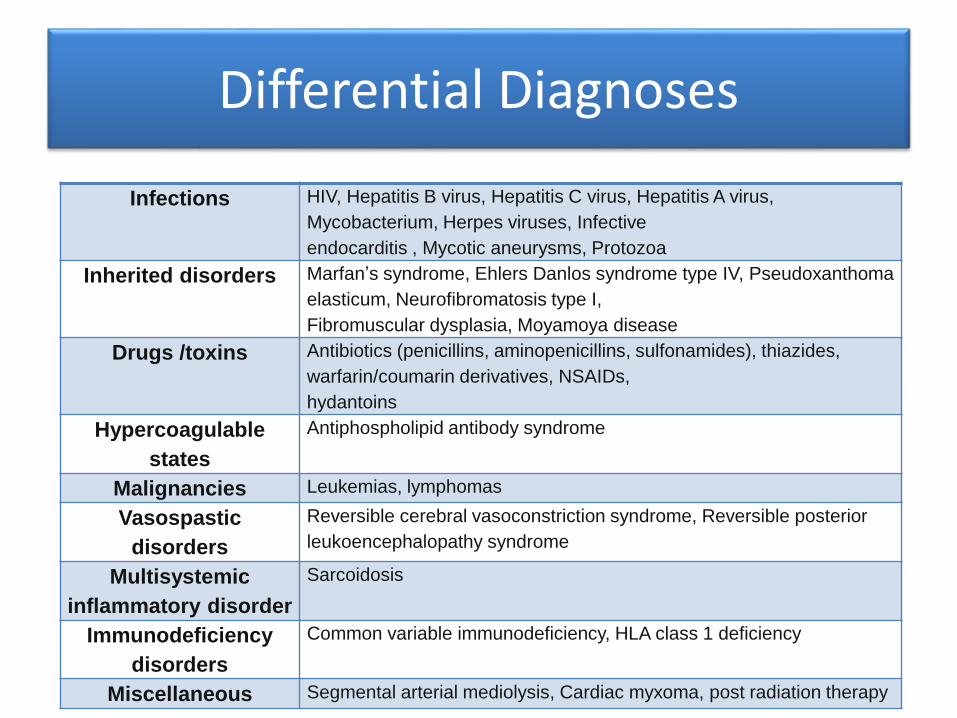
Differential Diagnoses
Infections HIV, Hepatitis B virus, Hepatitis C virus, Hepatitis A virus,
Mycobacterium, Herpes viruses, Infective
endocarditis , Mycotic aneurysms, Protozoa
Inherited disorders Marfan’s syndrome, Ehlers Danlos syndrome type IV, Pseudoxanthoma
elasticum, Neurofibromatosis type I,
Fibromuscular dysplasia, Moyamoya disease
Drugs /toxins Antibiotics (penicillins, aminopenicillins, sulfonamides), thiazides,
warfarin/coumarin derivatives, NSAIDs,
hydantoins
Hypercoagulable
states
Antiphospholipid antibody syndrome
Malignancies Leukemias, lymphomas
Vasospastic
disorders
Reversible cerebral vasoconstriction syndrome, Reversible posterior
leukoencephalopathy syndrome
Multisystemic
inflammatory disorder
Sarcoidosis
Immunodeficiency
disorders
Common variable immunodeficiency, HLA class 1 deficiency
Miscellaneous Segmental arterial mediolysis, Cardiac myxoma, post radiation therapy
How are Children with VasculitisManaged?
• The management of vasculitis is dependent upon the diagnosis, the nature of symptoms and the extent of organ involvement .
• From a quiet “wait and watch” or • symptomatic therapy to the use of steroids alone or in
combination with immunosuppresive agents such as cyclophosphamide or azathioprine, decisions are largely dependent on vessel size and which vascular bed is involved.
• Large vessel disease (TA) may be approached by a combination of drug therapy and invasive radiologic procedures such as dilatation or stenting.


Some theory …..

Hypocomplementemic urticarialvasculitis (HUV)
• Hypocomplementemic urticarialvasculitis (HUV) is a rare form of vasculitis (small blood vessels) and low levels of complement proteins in the blood.
• HUV causes recurrent episodes of urticariaand systemic, multiorgan involvement, causing arthritic joint pain; pulmonary (lung) disease; ocular (eye) inflammation; kidneyinflammation; or various other symptoms.
Etiology
• Both genetic and environmental factors are thought to play a role in causing HUV.
• It generally occurs sporadically, but familial cases have been reported.
• It is thought to develop due to an abnormal immune system response.
• In some cases HUV may be associated with an underlying infection or systemic diseases such as systemic lupus, Sjögren's syndrome, monoclonal gammopathy, or blood disorders.

Clinical features
Organ % Clinical features
Skin 100% Urticarial exanthema, urticarial vasculitis, palpable purpura, angioedema
Joints 70% Arthralgia and arthritis
Kidneys 50% Proteinuria, hematuria, renal insufficiency, rapid progressive glomerulonephritis (RPGN)
Gastrointestinal tract
30% Abdominal pain, nausea, vomiting, diarrhea, hepatomegaly, splenomegaly, ascites, serositis
Lungs 20% Shortness of breath, coughing, hemoptysis, pleural effusion, chronic obstructive pulmonary disease (COPD)
Eyes 10% Episcleritis, uveitis, conjunctivitis
Heart Rare Pericarditis, cardiac valve disease
Nervous system Rare Pseudotumor cerebri, aseptic meningitis, central or peripheral nerve palsy
Provided by : Human Phenotype Ontology (HPO)

Criteria for diagnosis of HUVS
• Major criteria– Chronic urticarial exanthema (at least 6 months)– Hypocomplementemia
• Minor criteria– Dermis (diagnosed by biopsy) Leukocytoclastic vasculitis– Arthralgia and arthritis– Uveitis or episcleritis (or conjunctivitis)– Glomerulonephritis– Abdominal pain– Positive C1q antibody.A diagnosis of HUV requires the presence of the two
major criteria, as well as at least two minor criteria.

Treatment
• The appropriate treatment of UV and HUVS is determined by the severity of the disease.
• Antihistamines represent the cornerstone of treatment for patients who have UV with only cutaneous lesions, serving to control the itching.
• Glucocorticoids (GC) are the agents most frequently employed to combat the inflammation and immune complex formation.
• Hydroxychloroquine.• Immunosuppressives are combined with GC, including
methotrexate, azathioprine, cyclophosphamide, cyclosporin, and mycophenolate mofetil.

Prognosis
• HUV varies from person to person.
• The prognosis largely depends on severity of systemic involvement and is influenced primarily by the severity of lung (pulmonary), heart, and kidney (renal) disease.
• Although HUV is uncommon in childhood, the prognosis is worse for those affected at younger ages because of more frequent, severe renal involvement.

THANKS FOR YOUR ATTENTION