hypertension in hemodialysis patients dr. shahrokh ezzatzadegan department of internal medicine...
DESCRIPTION
Relationship between BP and mortality in dialysis patients Luther JM Kidn Int 2008;73:TRANSCRIPT

Hypertension In Hemodialysis
Patients
Dr. Shahrokh EzzatzadeganDepartment of Internal MedicineShiraz University of Medical Sciences

Prevalence of hypertension in chronic HD pts
50 to 60 % of hemodialysis patients 30 % of PD patients

Relationship between BP and mortality in dialysis patients
Luther JM Kidn Int 2008;73:667-668

Mechanism of HTN
•Sodium and volume overload.•Sympathetic nervous system activity• Inappropriate renin secretion.• Alteration in endothelin and nitric oxide.• Erythropoietin therapy.• Hyperparathyroidism.• Other:
• Uremic toxins, Nocturnal hypoxemia and sleep disturbances
Nephrol Dial Transplant. 2004 May; 19(5):1058-68

Volume overload
• Hypervolemia is the major factor
• Achieving DW will control 60% of cases of HTN
The absence of edema does not exclude hypervolemia.

K/DOQIBlood Pressure Goals in Hypertensive ESRD Patients
≤ 140/90 mmHg (predialysis)
≤ 130/80 mmHg (postdialysis)

When and How to measure the BP in dialysis patients?
• Predialysis SBP overestimated mean SBP by an average of 10 mm Hg
• Postdialysis SBP underestimated mean SBP by an average of 7 mm Hg
• BP reasings over a period of 1 to 2 weeks rather than isolated readings should be used

Home blood pressure monitoring is of greater prognostic value than hemodialysis units recordings
Alborzi et al. CJASN 2007;2:1228-1234

Management

Management of Hypertension
• Step 1: Lifestyle modifications and control of volume status with lifestyle modifications.
• Step 2: Control of volume status with dialysis.
• Step 3: Administration of antihypertensive drugs.

Treatment of hypertension in patients on hemodialysis
Treatment of hypertension is often a multiple-step, multidisciplinary process to reach KDOQI guidelines of predialysis BP values of <140/90 mm Hg.
The key to successful treatment is patience; it often takes 4-6 weeks to achieve results. (This represents the lag phenomenon )

Chronic volume expansion
Vascular Na/K ATPase
NO SynthetaseADMA
DLIS etc
NO
iCa++
Vaso-constriction
Sustained UF & Na restriction
ECV
DLIS etc
ADMA
LAG
BP
Lag period between normalisation of ECF and optimal control of BP
DLIS:digoxin-like immunoreactive substance ADMA:asymmetric-dimethyl arginine

Treatment of Intradialytic Hypertension The step-by-step approach



Control of volume status
• Limit interdialytic weight gain
• Achieve dry weight• Frequent dialysis & Longer dialysis time
Agarwal R, et al. Hypertension. 2009 Mar; 53(3):500-7.

Choice of antihypertensive drugs
All classes of antihypertensive drugs can be used in dialysis patients, with the sole exception of diuretics, which are not commonly used because of their lack of efficacy.
Therefore, with the exceptions of diuretics, the criteria for drug selection are quite similar to those used in non-dialysis patients.

Postdialysis dosing or extra doses after HD may be necessary for certain antihypertensive agents:
•Angiotensin converting enzyme inhibitors (ACE-I): all are dialyzable except fosinopril
•Angiotensin receptor blockers (ARB): none are dialyzed
•B-blockers: atenolol and metoprolol are dialyzable but labetolol and carvedilol are not
•Calcium channel blocker: amlodipine is not dialyzable

Resistant Hypertension
•The use of NSAID drugs• Renovascular hypertension
• Increasing cysts in polysystic kidney disease
• Compliance

Peritoneal dialysis
• Patients undergoing hemodialysis who are noncompliant and in whom volume status and hypertension cannot be controlled may also benefit by switching to peritoneal dialysis.
• Nearly all peritoneal dialysis patients can become normotensive with strict adherence to volume control.
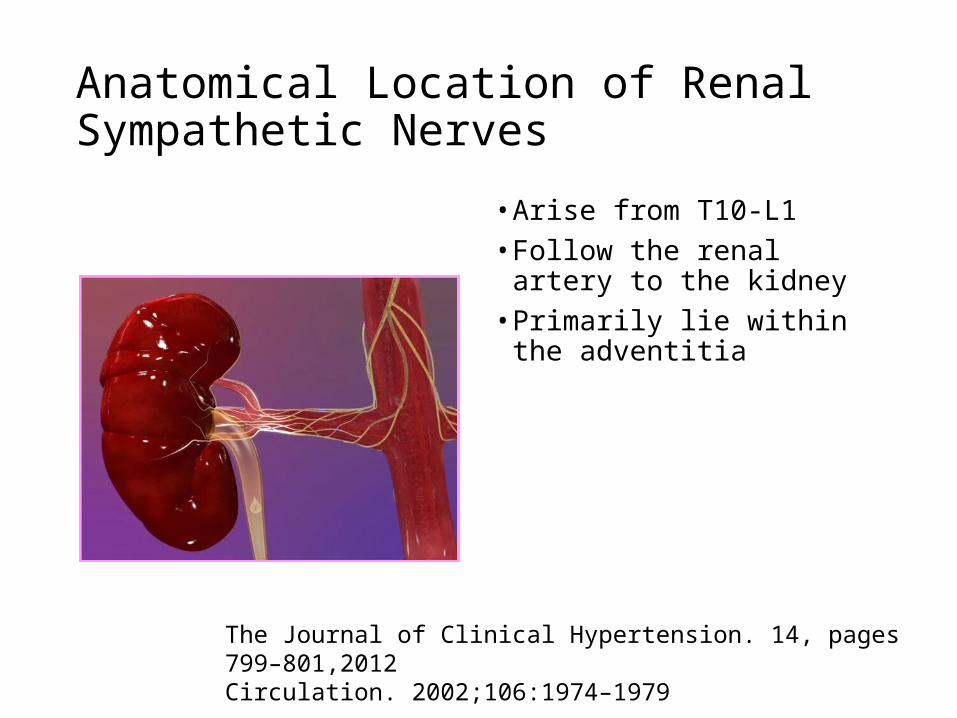
Anatomical Location of Renal Sympathetic Nerves
• Arise from T10-L1• Follow the renal artery to the
kidney• Primarily lie within the
adventitia
The Journal of Clinical Hypertension. 14, pages 799–801,2012Circulation. 2002;106:1974–1979

Bilateral nephrectomy
• May be considered in the rare, noncompliant individual with life-threatening hypertension unable to be controlled with any dialysis modality.

Intradialytic hypertension
• 5-15%
• Mechanism• Extracellular volume overload• Increased cardiac output• Changes in sodium levels • Activation of the renin–angiotensin–aldosterone system• Overactivity of the sympathetic nervous system• Endothelial cell dysfunction.• Removal of anti HTN during dialysis

Intradialytic Hypertension
• Carvedilol, which blocks endothelin-1 release, appears to be effective in this setting.
• This was suggested by a 12-week pilot study in which the initiation of carvedilol titrated to 50 mg twice daily was associated with a decrease in the frequency of intradialytic hypertensive episodes from 77 to 28 percent of hemodialysis sessions.


HTN following erythropoietin
• ↑BP in 20 to 30 % of IV EPO
• SQ<IV

HTN following erythropoietin
• Intravenous administration (versus subcutaneous)
• HD> peritoneal dialysis (CAPD)
• Family history of hypertension
• Higher hemoglobin (Hb) target
• Higher EPO dose

HTN following erythropoietinPREVENTION AND TREATMENT
• The risk of hypertension can be ameliorated by raising the Hb slowly.
• Patients who still remain hypertensive can be treated with fluid removal and the administration of antihypertensive agents.
• The dose of erythropoietin should be reduced or discontinued for several weeks in severe cases or when other therapeutic measures are ineffective.

Summary
• Sodium excess and extracellular volume expansion is the major factor in the development of hypertension.
• Lifestyle modifications is critical.• Control of volume status (Dietary salt and fluid restriction).• Correcting adequately volume expansion with dialysis.• All classes of antihypertensive drugs can be used in dialysis patients
