hypertension in esrd
TRANSCRIPT

HYPERTENSION IN ESRD
Oleh : Muhammad Haris
Stase Nefrologi Pediatric
PPDS Ilmu Penyakit Jantung dan Kedokteran Vaskuler
FK UGM

INTRODUCTION
Pediatric hypertension widely observed. Major cause of morbidity and mortality in United States and other countries
The true incidence of hypertension in children is not known
Standart of Blood Pressure for Children was made by NHLBI by using 11 surveys of more than 83.000 infants and children
Last, widely used The Fourth Report
Category : Pre hypertension : above 9oth percentile & below 95th percentile
Stage 1 hypertension : above 95th percentile & below 95th percentile plus 5 mmHg
Stage 2 hypertension : above 95th percentile plus 5 mmHg

CKD stage 1 65 % affected hypertension
CKD stage 4 & 5 80 %
And more than 50 % children with ESRD have uncontrolled hypertension

WORK UP
Laboratory studies : CBC (anemia Chronic Renal Disease), Creatinine (Renal Disease), Hypokalemia (Hyperaldosteronism), Blood hormone (high plasma renin renal vascular hypertension), Urine dipstick (+proteinuria problem in renal)
Echocardiography : LVH from chronic hypertension start for therapy (usually concentric morphology
Abdominal USG may reveal tumors or structural anomalies of kidneys or renal vasculare
Angiography to reveal the structure of renal vessels
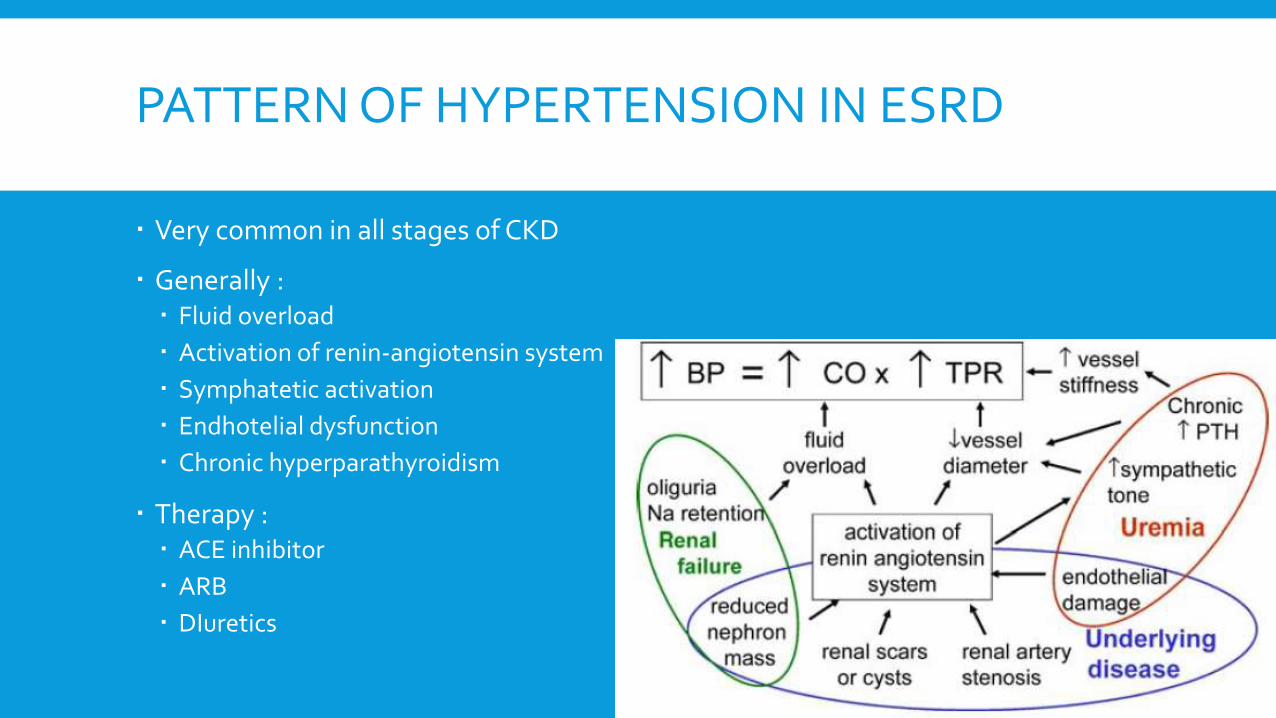
PATTERN OF HYPERTENSION IN ESRD
Very common in all stages of CKD
Generally : Fluid overload
Activation of renin-angiotensin system
Symphatetic activation
Endhotelial dysfunction
Chronic hyperparathyroidism
Therapy : ACE inhibitor
ARB
DIuretics
PATHOFISIOLOGY
Mechanisme of muscle sympathomimetic in elevated BP still unclear
Maybe connected with afferent afferent signal, dopaminergic abnormalities & accumulation of leptin in CKD
Another postules about renal ischemia
Renalase (amino oxidase expressed in kidney) activity usually reduced in patients with ESRD. Lower blood pressure and heart rate
In uremic patients, reduced NO stimulation leads to reduced agonist endhotelium-dependent vasodilatation
Corelated with higher concentration of ADMA

(Hadstein, 2007)

DRUG ASSOCIATED WITH HT
Erythropoietin cause elevated BP for several weeks
Related with arterial wall remodeling causing vascular resistance (Schiffl H et al 1998) and voltage independent calcium channel in smooth muscle activity sensitivity NO decreased (Vaziri et al, 1999)
Glucocoticoid lead to fluid retention by their mineralocorticoid effect
Cyclosporine A causes vasoconstriction of glomerular afferent arterioles and hyperplasia of juxtaglomerular apparatus

MANAGEMENT
PHARMACOTHERAPY
Based on epidemiology : 75% children with CKD stages 2-4 can reduces blood pressure (<95th percentile) with monotheraphy oh antihypertensive
More aggressive therapy needed if targetted <50th percentile
Start with single dose and titrate upward
ACE inhibitorand ARB is the most useful drug not only reduce BP but also slow down the progession of renal failure
Mechanism : Reduced proteinuria
Lower intaglomerular pressure
Anti inflamatory
Anti fibrotic

PHARMACOTHERAPY (2)
Diurretics used when hypervolemia
Thiazides are a popular first line therapy in mild to moderate CKD but less efective when GFR falls below 60 ml/min per 1.73 m2 body surface area
Not efective when below 30 ml/min . Shoul used furosemide when the status is ESRD
CCB very potent vasodilators and do not have cardiac side effect (have side effect proteinuria and increase intaglomerular pressure)
Beta Blocker can be used as a second line therapy for renal hypertension in children. Contraindications in asthma and can cause fatigue.

TERIMA KASIH & MOHON ASUPAN