hull and east yorkshire hospitals nhs trust clinical · pdf file1 hull and east yorkshire...
TRANSCRIPT

1
HULL AND EAST YORKSHIRE HOSPITALS NHS TRUST
Clinical Audit and Effectiveness Annual Report 2012/13
1. Introduction The Clinical Audit and Effectiveness Team now sits within the Quality, Governance and Assurance Directorate and works closely with the Quality Facilitators and Quality and Safety Managers. The Clinical Audit and Effectiveness Team manages the clinical audit project approval process, monitors participation in national audits and the implementation of any resulting actions, provides support and training to staff undertaking clinical audit projects and monitors compliance with the NICE guidance. The central team also co-ordinate the NCEPOD studies including the gap analyses and monitoring of actions. The role of the Quality Facilitators / Quality and Safety Managers is to monitor the audit plan for their Health Group, including obtaining outcome forms and monitoring of actions arising from audits. The Clinical Audit and Effectiveness Team consists of 1 Clinical Audit and Effectiveness Manager (0.5 WTE), supported by 2.4 WTE Clinical Audit and Effectiveness Facilitators. This year, there have only been 1.5 WTE Clinical Audit and Effectiveness Facilitators with the replacement post due to be filled in April 2013. In addition, the team is supported by an Audit Clerk (0.7 WTE), who is based at the Medical Records site. This report summarises the clinical audit and effectiveness activity for 2012/13 within the Trust. 2. Clinical Audit Priorities and Plan One of the Clinical Audit and Effectiveness Team’s responsibilities is to facilitate clinical audits within the Trust. Each Clinical Audit and Effectiveness Facilitator is linked with at least one Health Group and is able to assist clinicians with many aspects of the clinical audit process. This assistance can range from suggesting clinical audit topics to project design, data entry, sample identification, data analysis, data collection form or survey design, presentation preparation, case note retrieval and support with report writing. Once a CG1 registration form has been sent to the Clinical Audit and Effectiveness Facilitator, the department holds weekly approval meetings to ascertain whether the project is a quality clinical audit, and to discuss any implications for the Trust the clinical audit may have, such as Data Protection issues and patient opinion. All clinical audit projects approved during 2012/13 had a suitably completed CG1 and corresponding checklist completed, therefore all audits were conducted in line with the approved process for audit. Last year, the CG1 form was amended to include a section on information governance training. The Clinical Audit and Effectiveness Team have monitored this closely throughout the year and no audits were approved, unless the information governance training was in date for the whole audit project team. In March 2013, the Trust purchased Covalent, an integrated suite of applications that will enable more efficient monitoring of the audit plan and implementation of actions following an audit. Action
To transfer the audit plan and project documentation to Covalent to enable more efficient monitoring and reporting of the implementation of the plan – Clinical Audit and Effectiveness Manager

2
The Trust has a prioritised programme that relates to both local and national priorities with the overall main aim of improving patient outcomes. The priorities reflect a combination of both local and national priorities and are listed in the table below:-
TYPE OF AUDIT PRIORITY Assurance Framework audits 1 CQuIN audits 1 NPSA Audits (including Patient Safety Alert Notices, Rapid Response Alerts, Safer Practice Notices, Patient Safety Information)
1
NSF Audits 1 Peer Review 1 NICE Guidance (including Technology Appraisals, Interventional Procedures and Guidelines)
1
NCEPOD audits 1 National audits 1 NHSLA audits (eg. record keeping, consent) 1 Audits identified as a result of risk issues (including SUIs, incidents, PALS/complaints)
1
National Patient Surveys 1 Local patient surveys 2 Staff surveys 2 Local policy audits 2 Trust-wide audits 2 Care pathway/local guideline audits 3
Key
Priority 1 External or local ‘must do’ audit Priority 2 External or local ‘should do’ audit Priority 3 Local interest audit
A programme of audit projects was developed by the Health Groups based on the Trust audit priorities for 2013/14. See Appendix I for the audit plan 2013/14. 3. Monitoring of the Clinical Audit Plan During 2012/13, performance against the clinical audit plan was monitored via quarterly reports to the Clinical Audit and Effectiveness Committee. The table below shows the number of clinical audits commenced in relation to those included on the 2012/13 audit plan per Health Group.
Number of audits commenced
Current stage of audits Number of audits completed
271
Planning 1
222
Data collection 7 Data analysis 0 Report 1 Complete 222 Ongoing 14 Abandoned 26
Number of audits due to have commenced
Number of audits due to have been
completed
271
262
3
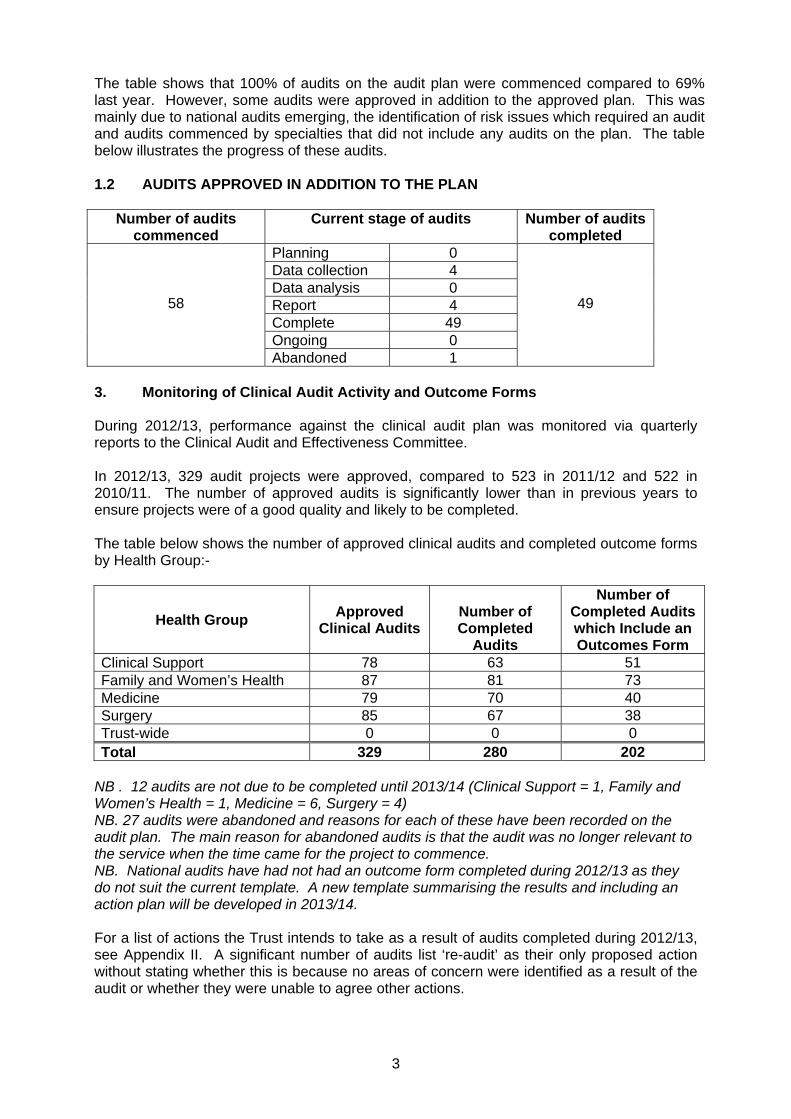
The table shows that 100% of audits on the audit plan were commenced compared to 69% last year. However, some audits were approved in addition to the approved plan. This was mainly due to national audits emerging, the identification of risk issues which required an audit and audits commenced by specialties that did not include any audits on the plan. The table below illustrates the progress of these audits. 1.2 AUDITS APPROVED IN ADDITION TO THE PLAN
Number of audits
commenced Current stage of audits Number of audits
completed
58
Planning 0
49
Data collection 4 Data analysis 0 Report 4 Complete 49 Ongoing 0 Abandoned 1
3. Monitoring of Clinical Audit Activity and Outcome Forms During 2012/13, performance against the clinical audit plan was monitored via quarterly reports to the Clinical Audit and Effectiveness Committee. In 2012/13, 329 audit projects were approved, compared to 523 in 2011/12 and 522 in 2010/11. The number of approved audits is significantly lower than in previous years to ensure projects were of a good quality and likely to be completed. The table below shows the number of approved clinical audits and completed outcome forms by Health Group:-
Health Group Approved
Clinical Audits
Number of Completed
Audits
Number of Completed Audits which Include an Outcomes Form
Clinical Support 78 63 51 Family and Women’s Health 87 81 73 Medicine 79 70 40 Surgery 85 67 38 Trust-wide 0 0 0 Total 329 280 202
NB . 12 audits are not due to be completed until 2013/14 (Clinical Support = 1, Family and Women’s Health = 1, Medicine = 6, Surgery = 4) NB. 27 audits were abandoned and reasons for each of these have been recorded on the audit plan. The main reason for abandoned audits is that the audit was no longer relevant to the service when the time came for the project to commence. NB. National audits have had not had an outcome form completed during 2012/13 as they do not suit the current template. A new template summarising the results and including an action plan will be developed in 2013/14. For a list of actions the Trust intends to take as a result of audits completed during 2012/13, see Appendix II. A significant number of audits list ‘re-audit’ as their only proposed action without stating whether this is because no areas of concern were identified as a result of the audit or whether they were unable to agree other actions.

4
Action
To devise a new template to record the results of national audits, which includes the action plan – Clinical Audit and Effectiveness Manager
To increase the number of outcomes forms for completed clinical audits – Health
Group Medical Directors
To improve the quality of outcome forms, including the requirement to state the reason for a re-audit being the only identified action – Health Group Medical Directors
4. Clinical Audit Policy In January 2012, the Clinical Audit Policy was ratified. The policy was created to meet the requirements of the NHSLA standards and in doing so, provide guidance to staff undertaking clinical audit projects within the Trust. The policy clearly details the stages of the clinical audit process with particular emphasis on the completion of the outcomes form at the end of the project, to ensure actions have been identified to improve practice. The policy includes a new form, the Clinical Audit Action Plan Monitoring template, which should be completed every 3 months until the actions have been implemented. The completed forms should be sent to the relevant Quality Facilitator / Quality and Safety Manager. Action
The effectiveness of the policy to be monitored via quarterly reports to the Clinical Audit and Effectiveness Committee – Clinical Audit and Effectiveness Manager
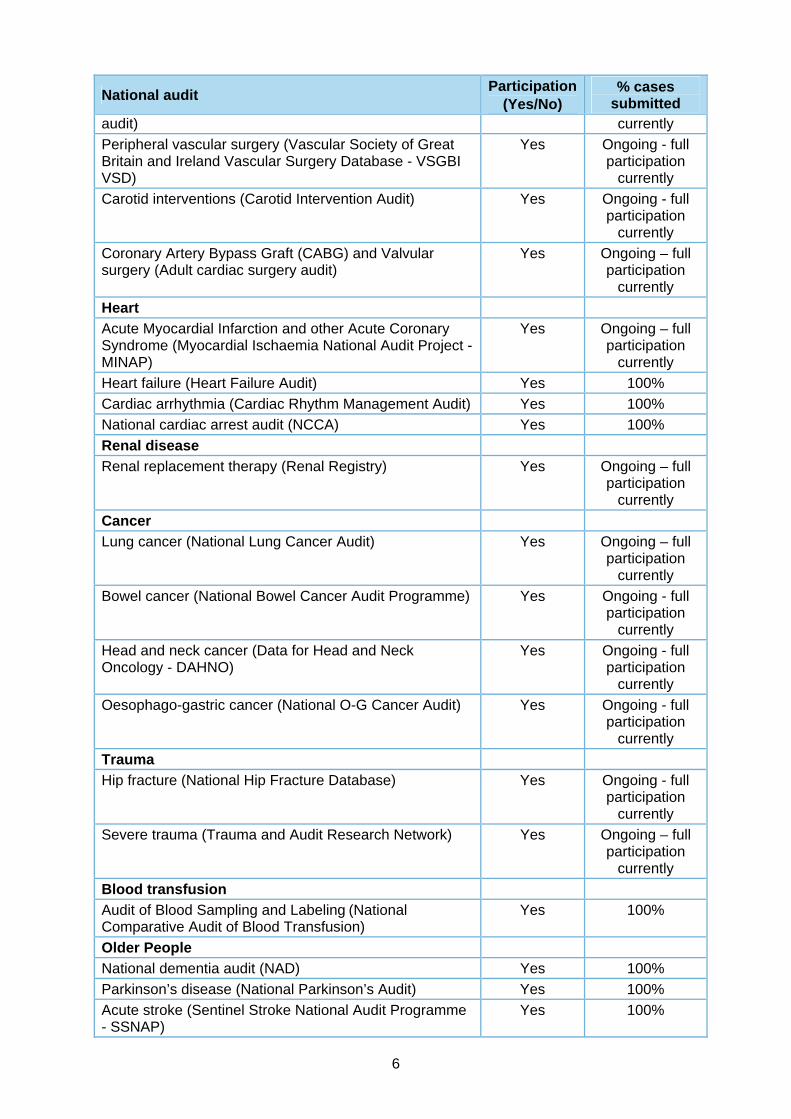
5. Clinical Audit and Effectiveness Committee The Clinical Audit and Effectiveness Committee met 6 times during this year. The committee is chaired by the Deputy Chief Medical Officer and there is representation from each Health Group, pharmacy, nursing and therapies. The Clinical Audit and Effectiveness Manager also attends. During the early part of the year, attendance from the Health Groups was poor and this issue was put on the risk register. However, attendance did improve and the Health Groups now usually send a deputy if the usual Health Group representative is unable to attend. The aim of the Committee is to monitor clinical audit and effectiveness activity within the Trust. This includes the monitoring of compliance with NICE guidance and NCEPOD recommendations. The Committee reports to the Operational Governance Committee. 6. National Audits During 2012/13, 44 national clinical audits covered NHS services that Hull and East Yorkshire Hospitals NHS Trust provides. During that period Hull and East Yorkshire Hospitals NHS Trust participated in 98% of national clinical audits which it was eligible to participate in. The national clinical audits that Hull and East Yorkshire Hospitals NHS Trust participated in, and for which data collection was completed during 2012/13, are listed overleaf alongside the number of cases submitted to each audit as a percentage of the number of registered cases required by the terms of that audit.

5
National audit Participation
(Yes/No) % cases
submitted
Peri- and Neonatal
Neonatal intensive and special care (National Neonatal Audit Programme - NNAP)
Yes Ongoing - full participation
currently
Children
Paediatric pneumonia (British Thoracic Society) Yes 100%
Paediatric asthma (British Thoracic Society) Yes 100%
Paediatric fever (College of Emergency Medicine) Yes 100%
Childhood epilepsy (Epilepsy 12 RCPH National Childhood Epilepsy Audit)
Yes 100%
Paediatric intensive care (Paediatric Intensive Care Audit Network - PICANet)
Yes Ongoing - full participation
currently
Diabetes (Royal College of Paediatrics and Child Health - RCPCH National Paediatric Diabetes Audit)
Yes Ongoing - full participation
currently
Acute care
Emergency use of oxygen (British Thoracic Society) Yes 100%
Adult community acquired pneumonia (British Thoracic Society)
Yes 100%
Non invasive ventilation (NIV) – adults (British Thoracic Society)
Yes 100%
Renal Colic (College of Emergency Medicine) Yes 100%
Adult critical care (Case Mix Programme) Yes Ongoing - full participation
currently
Potential donor audit (NHS Blood and Transplant) Yes Ongoing - full participation
currently
Long term conditions
Diabetes (National Adult Diabetes Audit) Yes Ongoing – full participation
currently
National Inpatient Diabetes Audit (NADIA) Yes 100%
Adult asthma (British Thoracic Society) Yes 100%
Bronchiectasis (British Thoracic Society) Yes 100%
Elective procedures
Hip, knee and ankle replacements (National Joint Registry)
Yes Ongoing - full participation
currently
Elective surgery (National Patient Reported Outcome Measures Programme - PROMs) Unilateral Hip Replacement Unilateral Knee Replacement Groin Hernia Surgery Varicose Vein surgery
Yes
94% 88% 92% 96%
Coronary angioplasty (National Institute for Clinical Outcome Research - NICOR Adult cardiac interventions
Yes Ongoing – full participation
6
National audit Participation
(Yes/No) % cases
submitted audit) currently
Peripheral vascular surgery (Vascular Society of Great Britain and Ireland Vascular Surgery Database - VSGBI VSD)
Yes Ongoing - full participation
currently
Carotid interventions (Carotid Intervention Audit) Yes Ongoing - full participation
currently
Coronary Artery Bypass Graft (CABG) and Valvular surgery (Adult cardiac surgery audit)
Yes Ongoing – full participation
currently
Heart
Acute Myocardial Infarction and other Acute Coronary Syndrome (Myocardial Ischaemia National Audit Project - MINAP)
Yes Ongoing – full participation
currently
Heart failure (Heart Failure Audit) Yes 100%
Cardiac arrhythmia (Cardiac Rhythm Management Audit) Yes 100%
National cardiac arrest audit (NCCA) Yes 100%
Renal disease
Renal replacement therapy (Renal Registry) Yes Ongoing – full participation
currently
Cancer
Lung cancer (National Lung Cancer Audit) Yes Ongoing – full participation
currently
Bowel cancer (National Bowel Cancer Audit Programme) Yes Ongoing - full participation
currently
Head and neck cancer (Data for Head and Neck Oncology - DAHNO)
Yes Ongoing - full participation
currently
Oesophago-gastric cancer (National O-G Cancer Audit) Yes Ongoing - full participation
currently
Trauma
Hip fracture (National Hip Fracture Database) Yes Ongoing - full participation
currently
Severe trauma (Trauma and Audit Research Network) Yes Ongoing – full participation
currently
Blood transfusion
Audit of Blood Sampling and Labeling (National Comparative Audit of Blood Transfusion)
Yes 100%
Older People
National dementia audit (NAD) Yes 100%
Parkinson’s disease (National Parkinson’s Audit) Yes 100%
Acute stroke (Sentinel Stroke National Audit Programme - SSNAP)
Yes 100%
7
National audit Participation
(Yes/No) % cases
submitted
Fractured neck of femur (College of Emergency Medicine)
Yes 100%
Action plans are developed as a result of the national audit reports that are produced. For a list of actions the Trust proposes to take, see Appendix III. Action
To monitor the actions identified in relation to national audit reports via the corporate action tracking template – Clinical Audit and Effectiveness Manager
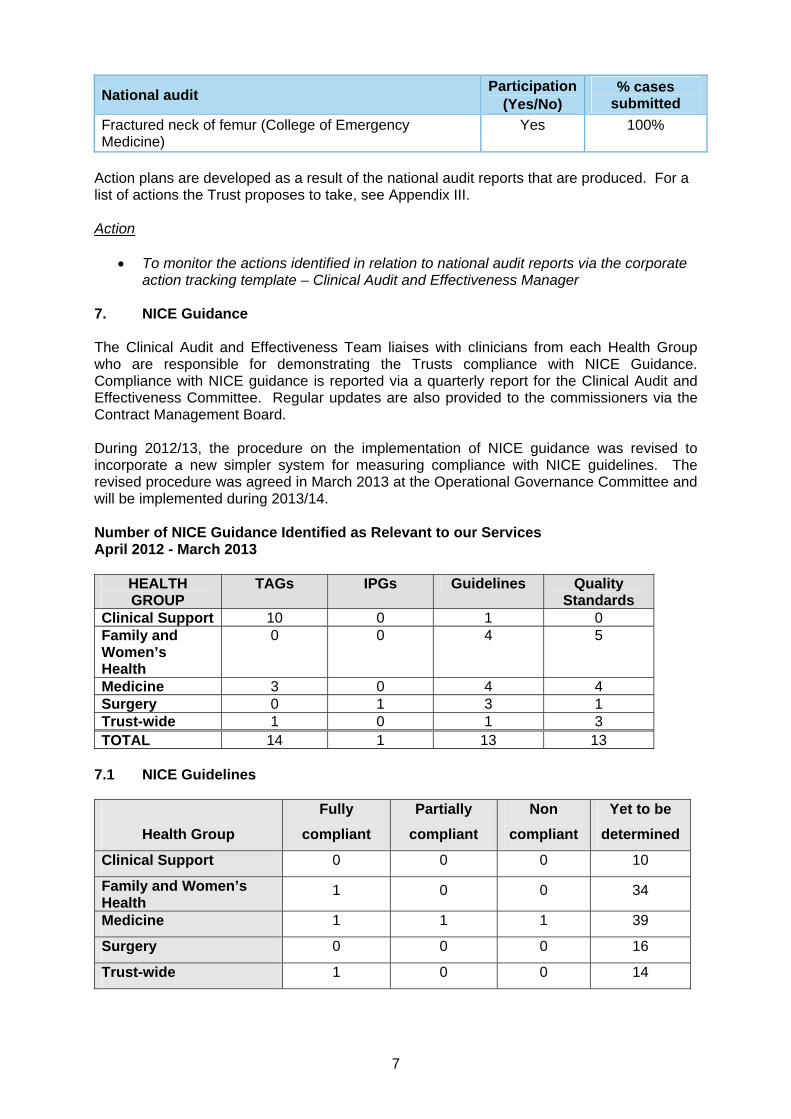
7. NICE Guidance The Clinical Audit and Effectiveness Team liaises with clinicians from each Health Group who are responsible for demonstrating the Trusts compliance with NICE Guidance. Compliance with NICE guidance is reported via a quarterly report for the Clinical Audit and Effectiveness Committee. Regular updates are also provided to the commissioners via the Contract Management Board. During 2012/13, the procedure on the implementation of NICE guidance was revised to incorporate a new simpler system for measuring compliance with NICE guidelines. The revised procedure was agreed in March 2013 at the Operational Governance Committee and will be implemented during 2013/14. Number of NICE Guidance Identified as Relevant to our Services April 2012 - March 2013
HEALTH GROUP
TAGs IPGs Guidelines Quality Standards
Clinical Support 10 0 1 0 Family and Women’s Health
0 0 4 5
Medicine 3 0 4 4 Surgery 0 1 3 1 Trust-wide 1 0 1 3 TOTAL 14 1 13 13
7.1 NICE Guidelines
Health Group
Fully
compliant
Partially
compliant
Non
compliant
Yet to be
determined
Clinical Support 0 0 0 10
Family and Women’s Health
1 0 0 34
Medicine 1 1 1 39
Surgery 0 0 0 16
Trust-wide 1 0 0 14

8
The above table shows that there was very little progress made in terms of completion of the Baseline Assessment Tools hence the revised procedure which now requires the completion of a much simpler Baseline Compliance Review form, with an action plan if required. Action
To email the Clinical Leads the revised BCR form for the NICE guidelines to determine compliance – Clinical Audit and Effectiveness Manager
8. NCEPOD activity 2012/13 The Clinical Audit and Effectiveness Manager is the named local reporter for NCEPOD and acts as a link between the non-clinical staff at NCEPOD and individual consultants. This role includes compiling and sending datasets requested by NCEPOD. The Trust participated in the studies below during 2012/13:- National Confidential Enquiry into Patient Outcome and Death (NCEPOD) study
Participation (Yes/No)
% cases submitted
Tracheostomy Yes Data collection is ongoing
Alcohol Related Liver Disease Yes 100%
Subarachnoid Haemorrhage Study Yes 100% Mothers and Babies: Reducing Risk through Audits and Confidential Enquires across the UK (MBBRACE – UK)
Participation (Yes/No)
% cases submitted
Maternal Infant and Perinatal programme Yes 100%
Other Enquiries/Reviews Participation
(Yes/No) % cases
submitted
Asthma Deaths (NRAD) Yes 100%
Child Health (CHR – UK) Yes Not known
This year, two NCEPOD reports were published that are relevant to this Trust. ‘Time to Intervene: Cardiac Arrest Procedures’ and ‘Too Lean a Service: Bariatric Surgery’ were published.
A gap analysis for the Cardiac Arrest Procedures report will be presented to the Clinical Audit and Effectiveness Committee in May 2013. A gap analysis, including an action plan, for the Bariatric Surgery report was agreed at the Clinical Audit and Effectiveness Committee and the actions have been fully implemented.
Action
To monitor the identified actions from the Cardiac Arrest study via the corporate action tracking template and report to the Clinical Audit and Effectiveness Committee – Clinical Audit and Effectiveness Manager
9. Clinical Audit Training The Clinical Audit and Effectiveness Team provided several clinical audit training sessions to specialties during this year, as requested. The team also provided 3 audit training sessions as part of the F2 doctors training and also provided training at specialty junior induction

9
sessions. The team has continued to provide individuals undertaking clinical audit projects with advice and support.
10
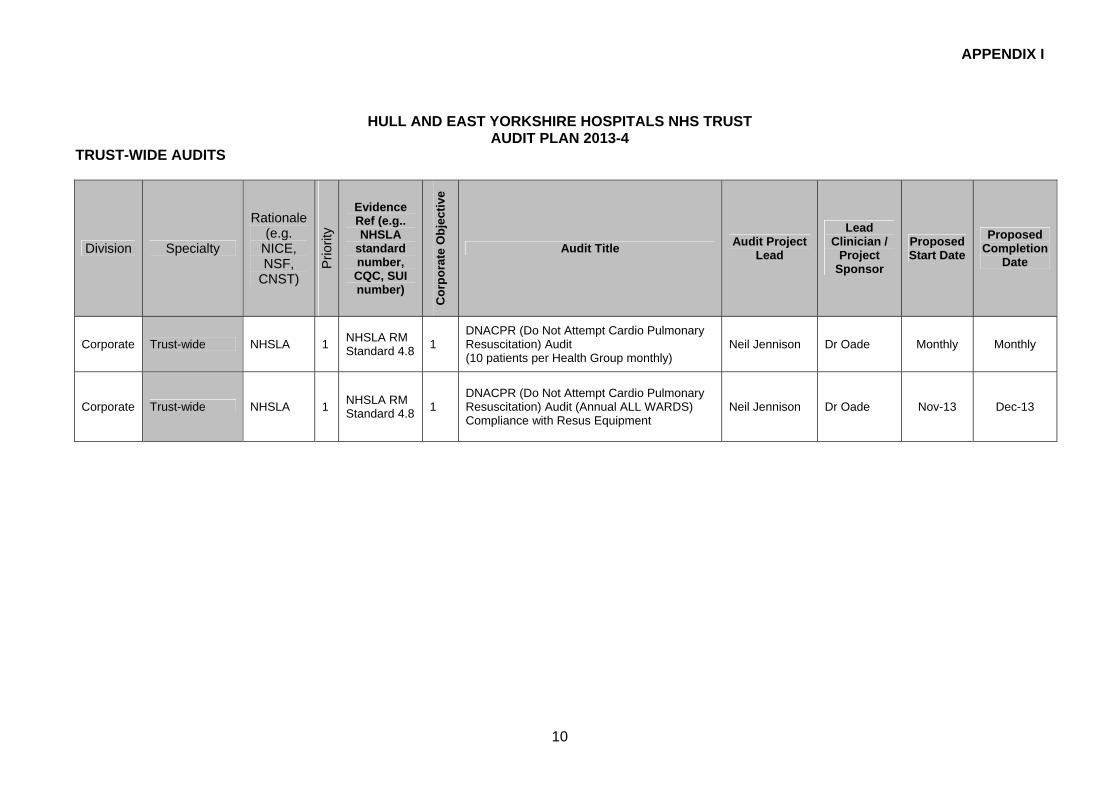
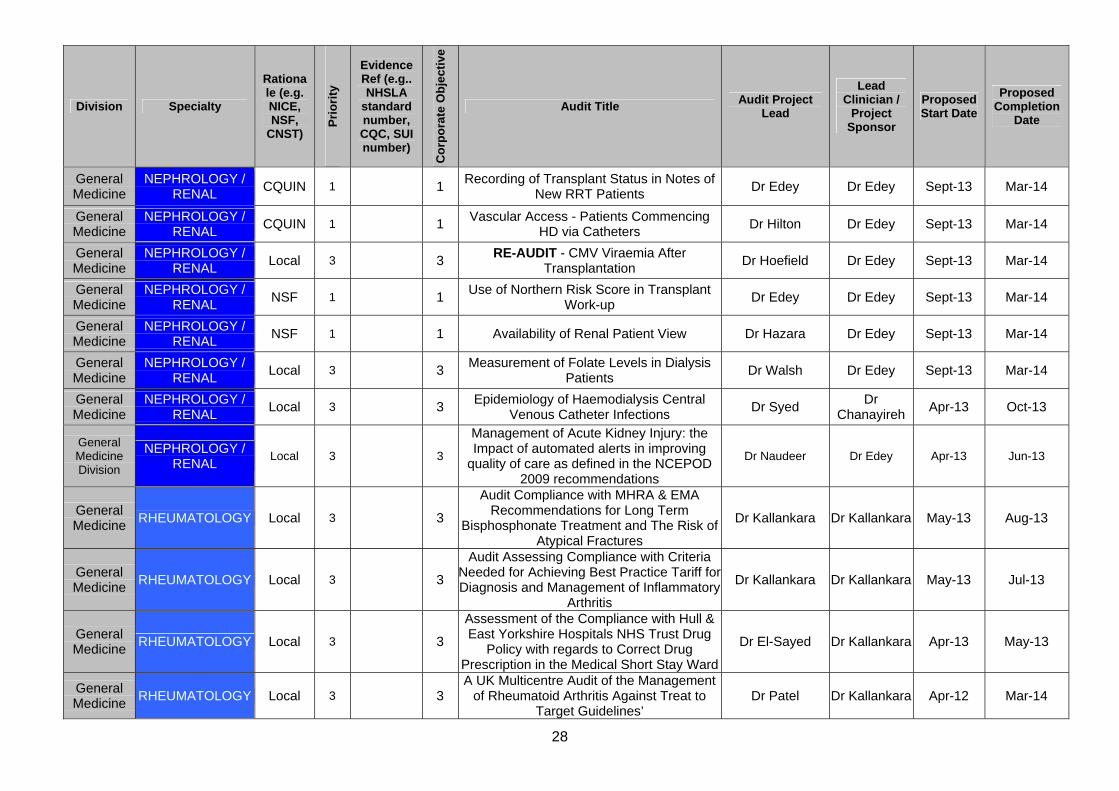
APPENDIX I
HULL AND EAST YORKSHIRE HOSPITALS NHS TRUST AUDIT PLAN 2013-4
TRUST-WIDE AUDITS
Division Specialty
Rationale (e.g.
NICE, NSF,
CNST)
Prio
rity
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
Corporate Trust-wide NHSLA 1 NHSLA RM Standard 4.8
1 DNACPR (Do Not Attempt Cardio Pulmonary Resuscitation) Audit (10 patients per Health Group monthly)
Neil Jennison Dr Oade Monthly Monthly
Corporate Trust-wide NHSLA 1 NHSLA RM Standard 4.8
1
DNACPR (Do Not Attempt Cardio Pulmonary Resuscitation) Audit (Annual ALL WARDS) Compliance with Resus Equipment
Neil Jennison Dr Oade Nov-13 Dec-13

11
CLINICAL SUPPORT AUDIT PLAN 2013-14
Division Specialty
Rationale (e.g. NICE, NSF,
CNST)
Pri
ori
ty
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project
Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion Date
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard
Health Record Keeping
1.8
1,5 Record Keeping Audit
(30 patients per Health Group, twice a year) Health Group Jul / Jan
Aug / Feb
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard
Health Record Keeping
4.8
1,5
Management of Acutely Ill Adult Patients in
Hospital (twice a year, all adult inpatients on a given day)
Outreach Team
Jul / Jan Aug / Feb
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard Discharg
e 4.10
1,5
Discharge (5 patients per ward per quarter)
Divisional Nurse
Managers
May / Aug / Nov / Feb
Jun / Sept / Dec / Mar
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard Transfusions 5.8
1,5
Policy for the Collection of Samples, Prescriptions, Collection and Transfusion of Blood
and Blood Components (20 casenotes per Health Group per quarter)
Hospital Transfusion
Team
May / Aug / Nov / Feb
Jun / Sept / Dec / Mar
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard Venous
Thromboembolism
5.9
1,5 VTE Policy and VTE Guideline Audit
(25 casenotes per Health Group 3 times per year)
Health Group Medical Directors
May / Sept / Jan
Jun / Oct / Feb
Health Group NHSLA Audit
1
NHSLA Standard MedicineManage
ment 5.10
1,5 Drug Policy Prescribing Standards
(annual, minimum 100 sample) Chief
Pharmacist Jun-13 Aug-13
Health Group NHSLA Audit
1 NHSLA
Standard 1,5
Audit of Medicines Reconciliation (annual, both sites, minimum of 30 on each site)
Chief Pharmacist
Oct-13 Dec-13

12
Division Specialty
Rationale (e.g. NICE, NSF,
CNST)
Pri
ori
ty
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project
Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion Date
MedicineManage
ment 5.10
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard Clinical
Handover of Care
4.9
1,5 Clinical Handover of Care (15 per Health Group
annually)
Divisional Nurse
Managers Sept-13 Mar-14
Imaging Division
RADIOLOGY
NHSLA Audit – Trust wide
1
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients)
Quality and Safety
Managers
Eileen Henders
on Aug-13 Mar-14
Imaging Division
RADIOLOGY Local 1 3 RE-AUDIT Quality of Posterior Anterior Chest X-Rays in CHH Match Up to the Standards Set Out
by the European Guidelines Sept-13 Mar-14
Imaging Division
RADIOLOGY Local 1 3 RE-AUDIT The Effects of Collimation and Lead Rubber Equivalent on Doses to the Thyroid and
Gonad in Relation to Chest Imaging Sept-13 Mar-14
Imaging Division
RADIOLOGY Local 1 3 RE-AUDIT Professional Practice Self Audit of
Clinical Reporting Skills 2012 Sept-13 Mar-14
Imaging Division
RADIOLOGY Local 3 3 Radiation Protection in the CT Department: A
Retrospective Patient Shielding Study Christopher
Burns
Dr Rowland-
Hill Feb-13 Jun-13
Imaging Division
RADIOLOGY Local 3 3 A Clinical Audit Investigating the Appropriate Usage of Gonad Shields on Paediatric Pelvic
Examinations within the Radiology Department Melanie Gray Dr Hauff Feb-13 Apr-13
Imaging Division
RADIOLOGY Local 3 3 An Audit of the Outcomes at our Institution Following Testicular Vein Embolisation for
Symptomatic Varicocele
Dr Shrivastava
Dr Robinson
Feb-13 May-13
Imaging Division
RADIOLOGY Local 3 3 The Use of Current Anatomical Markers in Plain
Film Radiography in the Emergency X-ray Department
Michael Atkinson
Dr Hauff Apr-13 May-13

13
Division Specialty
Rationale (e.g. NICE, NSF,
CNST)
Pri
ori
ty
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project
Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion Date
Imaging Division
RADIOLOGY Local 3 3 Accuracy of Request Cards in the CT Department Abigail Collins
Dr Hauff Apr-13 Jul-13
Specialist Service Division
CLINICAL HAEMATOLOGY
NHSLA Audit – Trust wide
1
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients)
Quality and Safety
Managers
Eileen Henders
on Aug-13 Mar-14
Specialist Service Division
CLINICAL HAEMATOLOGY
Local 3 3 Nutritional Support of Haematology Patients Having Undergone High Dose or Intensive
Chemotherapy – Retrospective Audit
Sadie Millington Mar-13 Apr-13
Specialist Service Division
CLINICAL HAEMATOLOGY
Local 3 3 Chronic Myeloid Leukaemia – Dasatinib, Nilotinib
and Standard Dose Imatinib Sadie
Millington Dr Ali Mar-13 Apr-13
Specialist Service Division
CLINICAL ONCOLOGY
NHSLA Audit – Trust wide
1
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients)
Quality and Safety
Managers
Eileen Henders
on Aug-13 Mar-14
Specialist Service Division
CLINICAL ONCOLOGY
Local 3 3 Audit of End of Life Care for Patients with End
Stage Liver Disease Dr Boland
Dr Saharia
Feb-13 May-13
Specialist Service Division
CLINICAL ONCOLOGY
Local 3 3 Concurrent Chemo-radiotherapy for Locally
Advanced Non Small Cell Lung Cancer Dr Wieczorek Apr-13 Mar-14
Specialist Service Division
CLINICAL ONCOLOGY
NICE 1 TAG268 3 Melanoma - Use of Ipilimumab Dr Roy Dr Roy Sept-13 Mar-14
Specialist Service Division
CLINICAL ONCOLOGY
NICE 1 TAG269 3 Melanoma - Use of Vemurafenib Dr Roy Dr Roy Sept-13 Mar-14
Specialist Service Division
CLINICAL ONCOLOGY
Local 3 3 A Retrospective Audit to Identify the Quality of
Palliative Care Patients Diagnosed with Head and Neck Cancer Receive Towards the End of Life
Debra Marsh Dr
Saharia Apr-13 Aug-13
Specialist Service Division
DIETETICS Local 3 Local 3
Audit to Assess the Indications for the Administration of Parenteral Nutrition (PN) to
Patients in the Queens Centre for Oncology and Haematology
Liz Graham Jul-13 Mar-14

14
Division Specialty
Rationale (e.g. NICE, NSF,
CNST)
Pri
ori
ty
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project
Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion Date
Specialist Service Division
DIETETICS Local 3 3 Referral and Dietetic Treatment Times for Adult
Inpatients
Sue Perry/ Jo Donaldson-Smith/ Tina McDougall
Apr-13 Sept-13
Specialist Service Division
DIETETICS Local 3 3 Dietetic Outcome Measures: A Baseline Audit
Sue Perry/ Jo Donaldson-Smith/ Tina McDougall
Sept-13 Mar-14
Specialist Service Division
PHARMACY Local 3 3 MDS (Monitored Dosage Systems) For Patients
Discharged from HEY Hospitals Mairin Flynn
Julie Randall
Jan-13 Sep-13
Specialist Service Division
PHYSIOTHERAPY Local 1 3 RE-AUDIT Physiotherapy Acute Respiratory
COPD Service (PARCS) Outcomes Measures Audit.
Claire Seabourne
Apr-13 Oct-13
Specialist Service Division
PHYSIOTHERAPY Local 3 3
Lower Limb Amputation Pathway Milestones: How Does HEY/ Contributory Regional Vascular Centres Perform Against Regionally Agreed
Quality and Operational Standards in Amputee Management
Amanda Hancock
Liz Minnich
Mar-13 Nov-13
Specialist Service Division
PHYSIOTHERAPY Local 3 3 Physiotherapy Workforce Review Nicola
Gilchrist May-13 Sep-13
Specialist Service Division
SPEECH AND LANGUAGE THERAPY
Local 3 3 Are Speech and Language Therapy Dysphagia
Recommendations Included on Immediate Discharge Letters?
Hannah Waterson
Apr-13 Sep-13
Specialist Service Division
OCCUPATIONAL THERAPY
Local 3 3
Evaluation of Occupational Therapy interventions to Patients Readmitted Within 30 Days of Original
Hospital Admissions to Identify Areas of Improvement to Practice
Debbie Parker Sept-13 Mar-14
Specialist Service Division
OCCUPATIONAL THERAPY
Local 3 3
Benchmarking the Occupational Therapy Service against the College of Occupational Therapists
Evidence Based Guidelines with People who have had Lower Limb Amputations
Karen Button Patience Young
Jan-13 Mar-14

15
Division Specialty
Rationale (e.g. NICE, NSF,
CNST)
Pri
ori
ty
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project
Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion Date
Specialist Service Division
OCCUPATIONAL THERAPY
Local 3 3 Does Occupational Therapy Input to AAU Impact
on Length of Stay? Ann Linnane-
Kelly
Ann Linnane-
Kelly Sept-13 Mar-14
Pathology Division
BLOOD TRANSFUSION
NHSLA Audit - Trustwi
de
1 CP113 1,5
NHSLA level 3 Audit on the process for the administration of transfusions, including patient identification and care of patients receiving a
transfusion
Transfusion team
Dr Ali Sept-13 Mar-14
Pathology Division
BLOOD TRANSFUSION
Local 2 CP113 1,5 Audit into Out of Hours Transfusion Requests
including Turnaround Times for Laboratory Tests and Administration of Transfusions
Transfusion team
Dr Ali Apr-13 Jun-13
Pathology Division
BLOOD TRANSFUSION
Local 2 SOPT 216
1,5 Audit into the Clinical Impact of Transfusion
Sample Rejection Transfusion
team Dr Ali Jun-13 Sep-13
Pathology Division
BIOCHEMISTRY Local 3 3 An Audit of HbA1c values in Hull and East
Yorkshire Diabetes Patients Following a Change in Test Units
Dr Kilpatrick Dr
Wilmot Mar-13 May-13
Pathology Division
INFECTIOUS DISEASES
Local 3 3 HIV Testing in TB clinic Dr Adams Sep-13 Mar-14
Pathology Division
MICROBIOLOGY Local 1 3 RE-AUDIT Adherence to NICE guidance of TB
Diagnosis – Sputum sample replicates for investigation of Tuberculosis
Dr Wearmouth
Dr Meigh Sept-13 Mar-14
Pathology Division
MICROBIOLOGY NICE 1 3
Diagnosis and Identification of Patient and Relatives with Definite or Possible Familial
Hypercholesterolarmia - adherence to NICE (CG71) guidelines
Dr Desborough
Dr Wilmot
Apr-13 Jul-13
Pathology Division
CYTOLOGY Nation
al 1 1 Audit of Invasive Cervical Cancers Sue Gilbert
Angela Carling
Ongoing Ongoing
Pathology Division
VIROLOGY Local 1 3 RE-AUDIT Time to Report of Respiratory Syncitial
Virus Testing Dr Meigh Dr Meigh Apr-13 Oct-13

16
FAMILY & WOMENS HEALTH AUDIT PLAN 2013-14
Division Specialty
Rationale (e.g.
NICE, NSF,
CNST)
Prio
rity
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard
Health Record Keeping
1.8
1,5 Record Keeping Audit
(30 patients per Health Group, twice a year)
Health Group Jul / Jan Aug / Feb
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard
Health Record Keeping
4.8
1,5
Management of Acutely Ill Adult Patients
in Hospital (twice a year, sample size to be
determined)
Outreach Team
Jul / Jan Aug / Feb
Health Group
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5
Discharge (5 patients per ward per quarter)
Divisional Nurse
Managers
May / Aug / Nov / Feb
Jun / Sept / Dec / Mar
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard Transfusions 5.8
1,5
Policy for the Collection of Samples, Prescriptions, Collection and Transfusion
of Blood and Blood Components (20 casenotes per Health Group per
quarter)
Hospital Transfusion
Team
May / Aug / Nov / Feb
Jun / Sept / Dec / Mar
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard Venous
Thromboembolism
5.9
1,5
VTE Policy and VTE Guideline Audit
(25 casenotes per Health Group 3 times per year)
Health Group Medical Directors
May / Sept / Jan
Jun / Oct / Feb
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard Clinical
Handover of Care
1,5 Clinical Handover of Care (15 per Health
Group annually)
Divisional Nurse
Managers Sep-13 Mar-14

17
Division Specialty
Rationale (e.g.
NICE, NSF,
CNST)
Prio
rity
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
4.9 Children
and Young
People's Services
NEONATES/ PICU
NHSLA Audit – Trust wide
1
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients)
Quality and Safety
Managers
Eileen Henderson
Aug-13 Mar-14
Children and
Young People's Services
NEONATES/ PICU
National 1 National 1 Neonatal Intensive and Special Care
(NNAP) Dr Wood Ongoing Ongoing
Children and
Young People's Services
NEONATES/ PICU
Local 3 Local 3 Thromboembolic Complication of
Neonatal Umbilical Lines Clare
Magson Dr Preece Feb-13 Aug-13
Children and
Young People's Services
NEONATES/ PICU
Local 3 Local 3 Outcome for Babies with Shoulder
Dystocia at Birth Simon
Richardson Dr Wood Mar-13 Jul-13
Children and
Young People's Services
NEONATES/ PICU
Local 3 Local 3 Admission Temperature Audit Michael Hayes
Dr Preece Mar-13 Jul-13
Children and
Young People's Services
NEONATES/ PICU
Local 3 Local 3 Audit of Home Nasogastric Tube Feeding
Programme Philippa
Satchwell Dr Preece Mar-13 Jul-13
Children and
Young People's
NEONATES/ PICU
Local 3 Local 3 Infants Nursed on Neonatal Unit Beyond
44+6 Weeks Corrected Gestation – A Service Evaluation
James Houston
Hassan Gaili
Mar-13 Jul-13

18
Division Specialty
Rationale (e.g.
NICE, NSF,
CNST)
Prio
rity
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
Services
Children and
Young People's Services
NEONATES/ PICU
NCEPOD 1 NCEPOD 1 Audit of Parenteral Nutrition Practice Dr Preece Jan-14 Mar-14
Children and
Young People's Services
PAEDIATRIC MEDICINE
National 1 National 1 Diabetes (Paediatric) Mr Mathew Ongoing Ongoing
Children and
Young People's Services
PAEDIATRIC MEDICINE
National 1 National 1 Epilepsy 12 Dr Jose Feb-13 Mar-14
Children and
Young People's Services
PAEDIATRIC MEDICINE
National 1 National 1 Paediatric Asthma (BTS) Dr Toko Nov-13 Jan-14
Children and
Young People's Services
PAEDIATRIC MEDICINE
National 1 National 1 Paediatric Intensive Care (PICANET) Dr Klonin Ongoing Ongoing
Children and
Young People's Services
PAEDIATRIC MEDICINE
National 1 National 1 Child Health Programme Dr Toko Ongoing Ongoing
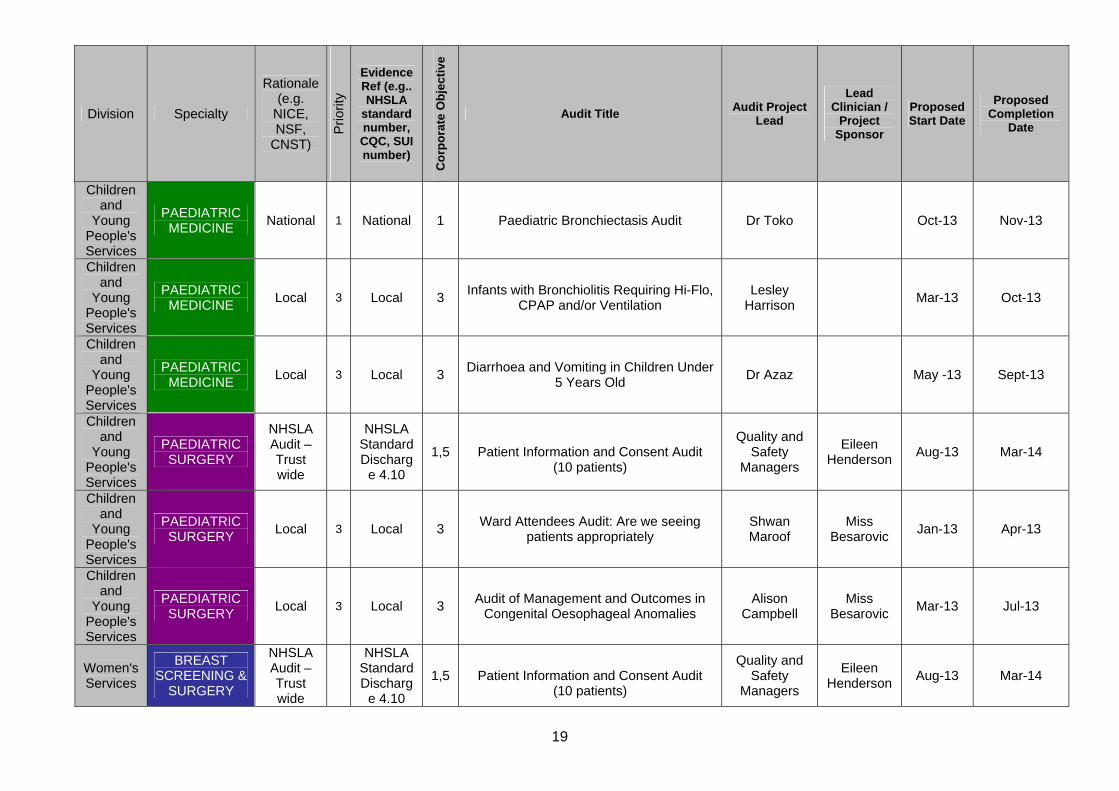
19
Division Specialty
Rationale (e.g.
NICE, NSF,
CNST)
Prio
rity
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
Children and
Young People's Services
PAEDIATRIC MEDICINE
National 1 National 1 Paediatric Bronchiectasis Audit Dr Toko Oct-13 Nov-13
Children and
Young People's Services
PAEDIATRIC MEDICINE
Local 3 Local 3 Infants with Bronchiolitis Requiring Hi-Flo,
CPAP and/or Ventilation Lesley
Harrison Mar-13 Oct-13
Children and
Young People's Services
PAEDIATRIC MEDICINE
Local 3 Local 3 Diarrhoea and Vomiting in Children Under
5 Years Old Dr Azaz May -13 Sept-13
Children and
Young People's Services
PAEDIATRIC SURGERY
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients)
Quality and Safety
Managers
Eileen Henderson
Aug-13 Mar-14
Children and
Young People's Services
PAEDIATRIC SURGERY
Local 3 Local 3 Ward Attendees Audit: Are we seeing
patients appropriately Shwan Maroof
Miss Besarovic
Jan-13 Apr-13
Children and
Young People's Services
PAEDIATRIC SURGERY
Local 3 Local 3 Audit of Management and Outcomes in
Congenital Oesophageal Anomalies Alison
Campbell Miss
Besarovic Mar-13 Jul-13
Women's Services
BREAST SCREENING &
SURGERY
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients)
Quality and Safety
Managers
Eileen Henderson
Aug-13 Mar-14

20
Division Specialty
Rationale (e.g.
NICE, NSF,
CNST)
Prio
rity
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
Women's Services
BREAST SCREENING &
SURGERY Local 3 Local 3
Initial Audit of the Outcomes of the Holistic Needs Assessment at the End of
the First Year of the Survivorship Programme for Breast Cancer follow up and Review of Number of Further Follow
up Contacts Required
Julia Massey Miss
McManus Dec-12 Jun-13
Women's Services
BREAST SCREENING &
SURGERY Local 3 Local 3
Re-excision Rates in Lobular Breast Cancer with and without MRI
Mr Kneeshaw May-13 Dec-13
Women's Services
GYNAECOLOGY
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients)
Quality and Safety
Managers
Eileen Henderson
Aug-13 Mar-14
Women's Services
GYNAECOLOGY National 1 National 1 Ovarian Mass RMI Audit Dr Flynn May-13 Mar-14
Women's Services
GYNAECOLOGY National 1 National 1 Cyto-reversion Rates at 8 months After
Treatment Kofi Yamoah Dr Flynn May-13 Mar-14
Women's Services
GYNAECOLOGY National 1 National 1 Confirmed Histological Treatment Failures
at 12 months Kofi Yamoah Dr Flynn May-13 Mar-14
Women's Services
GYNAECOLOGY Local 3 Local 3 Hysterectomy-approach and Outcome Mr Oboh Apr-13 Apr-14
Women's Services
GYNAECOLOGY Local 3 Local 3 Laparoscopic Surgical Injuries Mr Oboh Apr-13 Apr-14
Women's Services
GYNAECOLOGY Local 3 Local 3 Management of Pregnancy of Unknown
Location Mr Oboh Apr-13 Apr-14
Women's Services
GYNAECOLOGY Local 3 Local 3 Management of Tubal Ectopic Pregnancy Mr Oboh Apr-13 Apr-14
Women's Services
GYNAECOLOGY Local 3 Local 3 Management of Hyperemesis Gravidarum
in the Day-case Setting Mr Oboh Apr-13 Apr-14
Women's Services
GYNAECOLOGY Local 3 Local 3 Outcome of Hysteroscopic Sterilisation Mr Oboh Apr-13 Apr-14
Women's Services
GYNAECOLOGY Local 3 Local 3 Audit of Medical Termination of
Pregnancy Mr Oboh Apr-13 Sept-13
Women's Services
GYNAECOLOGY Local 3 Local 3 Audit of Local Anaesthetic Evacuation of
Products of Conception Mr Oboh Apr-13 Sept-13

21
Division Specialty
Rationale (e.g.
NICE, NSF,
CNST)
Prio
rity
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
Women's Services
GYNAECOLOGY Local 3 Local 3 Management of Urinary Stress
Incontinence Mr Oboh Apr-13 Apr-14
Women's Services
OBSTETRICS
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients)
Quality and Safety
Managers
Eileen Henderson
Aug-13 Mar-14
Women's Services
OBSTETRICS National 1 National 1 Maternal, Infant and Newborn Clinical
Outcome Review Programme (MBRRACE-UK)
Mr Lindow Ongoing Ongoing
Women's Services
OBSTETRICS CNST 1 CNST 1 Record Keeping Monthly Spot Checks
(Annual) Sue Cooper Apr-13 Mar-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Record Keeping Audit Local Supervising
Authority Supervisors of Midwives (Annual)
Lorraine Cooper
Apr-13 Mar-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Fetal Blood Sampling (Annual) Sept-13 Feb-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Use of Oxytocin (Annual) Julia
Chambers/ Mr Tyrrell
Sept-13 Feb-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Caesarean Section Grade 1 LSCS Audit
(Quarterly) Helen Dent
Apr/July/Oct/Jan
July/Oct/Jan/ Apr
Women's Services
OBSTETRICS CNST 1 CNST 1 Induction of Labour (6 monthly) Karen
Thompson May/Oct Aug/Jan
Women's Services
OBSTETRICS CNST 1 CNST 1 High Dependency Care (Annual) Julia
Chambers/ Mr Tyrrell
Sept-13 Feb-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Vaginal Birth After Caesarean Section
(Annual) Sept-13 Feb-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Severe Pre-eclampsia (including
Eclampsia) (Annual) MDT Team Oct-13 Mar-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Operative Vaginal Delivery (Annual) MDT Team Sept-13 Feb-14
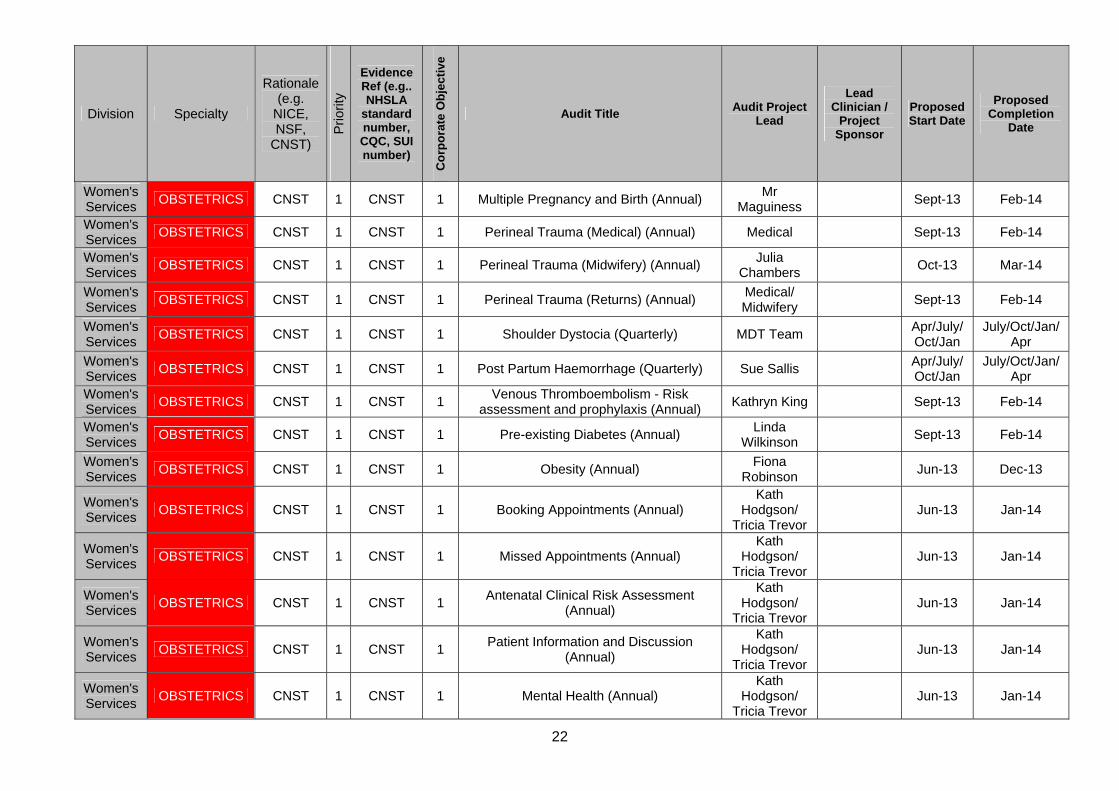
22
Division Specialty
Rationale (e.g.
NICE, NSF,
CNST)
Prio
rity
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
Women's Services
OBSTETRICS CNST 1 CNST 1 Multiple Pregnancy and Birth (Annual) Mr
Maguiness Sept-13 Feb-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Perineal Trauma (Medical) (Annual) Medical Sept-13 Feb-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Perineal Trauma (Midwifery) (Annual) Julia
Chambers Oct-13 Mar-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Perineal Trauma (Returns) (Annual) Medical/ Midwifery
Sept-13 Feb-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Shoulder Dystocia (Quarterly) MDT Team Apr/July/Oct/Jan
July/Oct/Jan/ Apr
Women's Services
OBSTETRICS CNST 1 CNST 1 Post Partum Haemorrhage (Quarterly) Sue Sallis Apr/July/Oct/Jan
July/Oct/Jan/ Apr
Women's Services
OBSTETRICS CNST 1 CNST 1 Venous Thromboembolism - Risk
assessment and prophylaxis (Annual) Kathryn King Sept-13 Feb-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Pre-existing Diabetes (Annual) Linda
Wilkinson Sept-13 Feb-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Obesity (Annual) Fiona
Robinson Jun-13 Dec-13
Women's Services
OBSTETRICS CNST 1 CNST 1 Booking Appointments (Annual) Kath
Hodgson/ Tricia Trevor
Jun-13 Jan-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Missed Appointments (Annual) Kath
Hodgson/ Tricia Trevor
Jun-13 Jan-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Antenatal Clinical Risk Assessment
(Annual)
Kath Hodgson/
Tricia Trevor Jun-13 Jan-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Patient Information and Discussion
(Annual)
Kath Hodgson/
Tricia Trevor Jun-13 Jan-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Mental Health (Annual) Kath
Hodgson/ Tricia Trevor
Jun-13 Jan-14

23
Division Specialty
Rationale (e.g.
NICE, NSF,
CNST)
Prio
rity
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
Women's Services
OBSTETRICS CNST 1 CNST 1 Handover of Care (Annual) Kath
Hodgson/ Tricia Trevor
Jun-13 Jan-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Maternal Transfer by Ambulance (Annual) Kath
Hodgson/ Tricia Trevor
Jun-13 Jan-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Non-obstetric Maternity Care (Annual) Kath
Hodgson/ Tricia Trevor
Jun-13 Jan-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Antenatal Screening Tests in Pregnancy
(Annual) Jane
McFarlane Jun-13 Jan-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Referral When Fetal Abnormality
Detected (Annual) Jane
McFarlane Jun-13 Jan-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Newborn Life Support - Documentation to
evidence resuscitation equipment is checked, stocked and fit for use (Annual)
Julia Chambers/Su
e Sallis Jan-14 Mar-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Admission to Neonatal Unit - Criteria for
aAdmission to NICU (Annual)
Dr Pairaudeau/r
Dr Gaili Sept-13 Feb-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Immediate Care of the Newborn (Annual) Dr Preece Sept-13 Feb-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Examination of the Newborn (Annual) Dr Preece Sept-13 Feb-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Bladder Care (Annual) Angie Rymer Aug-13 Feb-14
Women's Services
OBSTETRICS CNST 1 CNST 1 Recovery (Annual) Sue Sallis Jul-13 Dec-13
Women's Services
OBSTETRICS CNST 1 CNST 1 Support for Parents (Annual) Jacqui Powell Jul-13 Dec-13
Women's Services
OBSTETRICS Local 3 Local 3 Management of Postmenopausal
Bleeding Kofi Yamoah Dr Allen Mar-13 May -13
Women's Services
OBSTETRICS Local 3 Local 3 An Audit of Practice of Spinal
Anaesthesia for Parturients in our Dr Yusaf Dr Balaji Apr-13 Sept-13
24
Division Specialty
Rationale (e.g.
NICE, NSF,
CNST)
Prio
rity
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
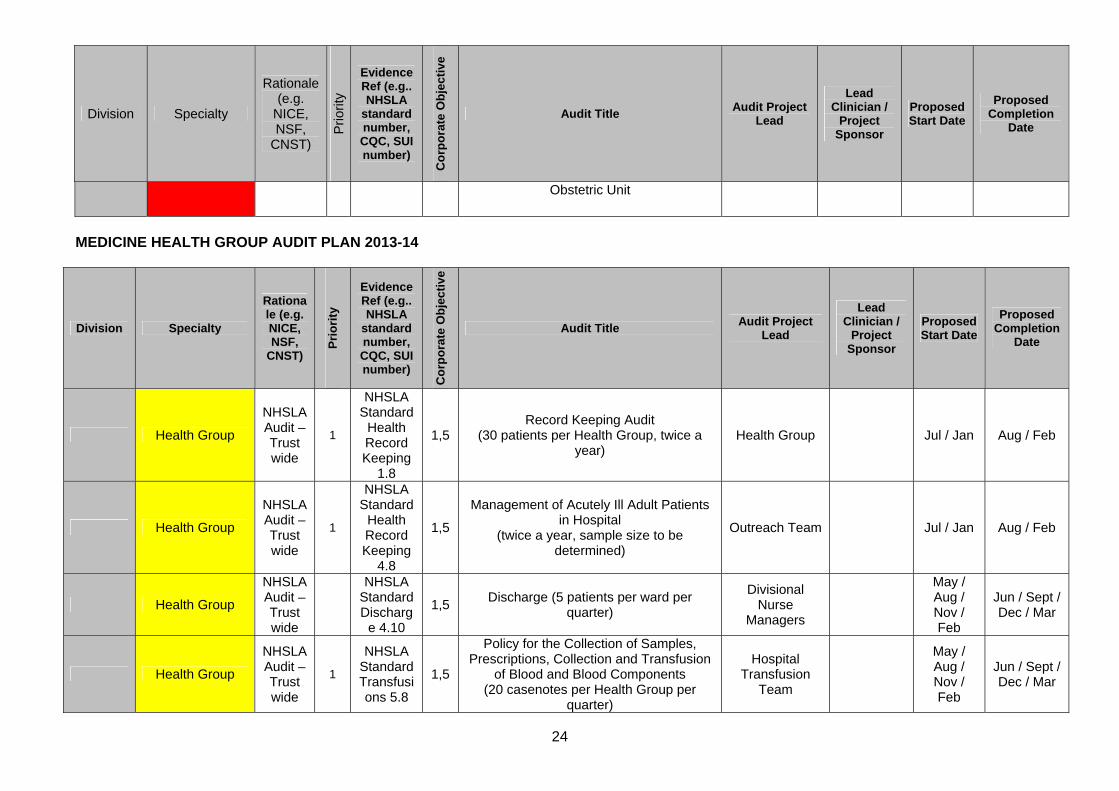
Obstetric Unit
MEDICINE HEALTH GROUP AUDIT PLAN 2013-14
Division Specialty
Rationale (e.g. NICE, NSF,
CNST)
Pri
ori
ty
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project
Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard
Health Record Keeping
1.8
1,5 Record Keeping Audit
(30 patients per Health Group, twice a year)
Health Group Jul / Jan Aug / Feb
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard
Health Record Keeping
4.8
1,5
Management of Acutely Ill Adult Patients
in Hospital (twice a year, sample size to be
determined)
Outreach Team Jul / Jan Aug / Feb
Health Group
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5
Discharge (5 patients per ward per
quarter)
Divisional Nurse
Managers
May / Aug / Nov / Feb
Jun / Sept / Dec / Mar
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard Transfusions 5.8
1,5
Policy for the Collection of Samples, Prescriptions, Collection and Transfusion
of Blood and Blood Components (20 casenotes per Health Group per
quarter)
Hospital Transfusion
Team
May / Aug / Nov / Feb
Jun / Sept / Dec / Mar

25
Division Specialty
Rationale (e.g. NICE, NSF,
CNST)
Pri
ori
ty
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project
Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard Venous
Thromboembolism
5.9
1,5
VTE Policy and VTE Guideline Audit
(25 casenotes per Health Group 3 times per year)
Health Group Medical Directors
May / Sept / Jan
Jun / Oct / Feb
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard Clinical
Handover of Care
4.9
1,5
Clinical Handover of Care (15 per Health
Group annually) Divisional
Nurse Managers
Sept-13 Mar-14
Emergency Medicine
ACUTE ASSESSMENT
UNIT (AAU) Local 3 3 Management of PE on AAU Dr Anand Dr Middleton Apr-13 Aug-13
Emergency Medicine
ACUTE ASSESSMENT
UNIT (AAU) Local 3 3 Audit of Ambulatory Care Dr Thakur Dr Middleton Sept-13 Mar-14
Emergency Medicine
ACUTE ASSESSMENT
UNIT (AAU) Local 1 3
RE-AUDIT Clinical Quality Indicators on AAU
Dr Thakur Dr Thakur Sept-13 Mar-14
Emergency Medicine
ACUTE ASSESSMENT
UNIT (AAU) Local 3 3 Antibiotic Prescribing in AAU Dr Middleton Dr Middleton Mar-12 May-13
Emergency Medicine
ACUTE ASSESSMENT
UNIT (AAU) Local 1 1 RE-AUDIT Management of Sepsis on AAU Dr May Dr Thakur Sept-13 Mar-14
Emergency Medicine
EMERGENCY DEPARTMENT
National Audit
1 1 Severe Sepsis and Septic Shock Dr Perez / Dr
Arundel Dr Rayner Sept-13 Mar-14
Emergency Medicine
EMERGENCY DEPARTMENT
National Audit
1 1 Paracetamol Overdose Dr Perez/ Dr
Gonzalez Dr Rayner Sept-13 Mar-14
Emergency Medicine
EMERGENCY DEPARTMENT
Local 3 3 Pneumonia Bundle in ED Dr Rayner / Dr
Manou Dr Rayner Sept-13 Mar-14
Emergency Medicine
EMERGENCY DEPARTMENT
Local 3 3 Audit of Management of Suspected
Scaphoid Fractures Presenting to the Dr Higson Dr Perez May-13 Jul-13

26
Division Specialty
Rationale (e.g. NICE, NSF,
CNST)
Pri
ori
ty
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project
Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
Emergency Department
Emergency Medicine
EMERGENCY DEPARTMENT
NICE 1 1 NICE Head Injury Guidance Dr Pickering Mr Rayner Apr-13 Dec-13
Emergency Medicine
EMERGENCY DEPARTMENT
National Audit
1 1 Asthma in Children Dr Perez Mr Rayner TBC TBC
Emergency Medicine
EMERGENCY DEPARTMENT
National Audit
1 1 Trauma Audit Research Network: Severe
Trauma (TARN) Chris Hampson Dr Rayner Ongoing Ongoing
Emergency Medicine
EMERGENCY DEPARTMENT
Local 3 3 Trauma Team Activation Dr Perez Dr Perez Aug-13 Mar-14
General Medicine
CHEST MEDICINE
NHSLA Audit – Trust wide
1
NHSLA Standard Discharge
4.10
1,5 Patient Information and Consent Audit
(10 patients) Quality and
Safety ManagersEileen
Henderson Aug-13 Mar-14
General Medicine
CHEST MEDICINE National
Audit 1 1 Emergency Oxygen Mark Major
Dr Greenstone
Aug-13 Nov-13
General Medicine
CHEST MEDICINE National
Audit 1 1 National COPD Audit TBC TBC TBC TBC
General Medicine
CHEST MEDICINE National
Audit 1 1 NLCA Lung Cancer Dr Anderson Dr Anderson Ongoing Ongoing
General Medicine
CHEST MEDICINE National
Audit 1 1 National Pulmonary Hypertension Database Mark Major
Professor Morice
Apr-13 Ongoing
General Medicine
DIABETES AND ENDOCRINOLOGY
National Audit
1 1 National Diabetes Audit - NHS DIABETES Dr Patmore Dr Patmore TBC TBC
General Medicine
DIABETES AND ENDOCRINOLOGY
National Audit
1 1 National Diabetes Inpatient Audit - NHS
DIABETES Dr Allan Dr Allan Sept-13 Sept-13
General Medicine
DIABETES AND ENDOCRINOLOGY
Local 1 3 RE-AUDIT Audit of Bone Density (DXA)
Requests Received Ann Goodby Ann Goodby Sept-13 Nov-13
General Medicine
DIABETES AND ENDOCRINOLOGY
National Audit
1 1 National Diabetes in Pregnancy Audit
(NCAPOP) Dr Allan/Mr
Lindow Dr Allan Apr-13 Ongoing
General Medicine
DIABETES AND ENDOCRINOLOGY
National Audit
1 1 National Post-Radioiodine Management of
Patients with Graves' Disease Dr Sathyaplan
Dr Sathyaplan
TBC TBC
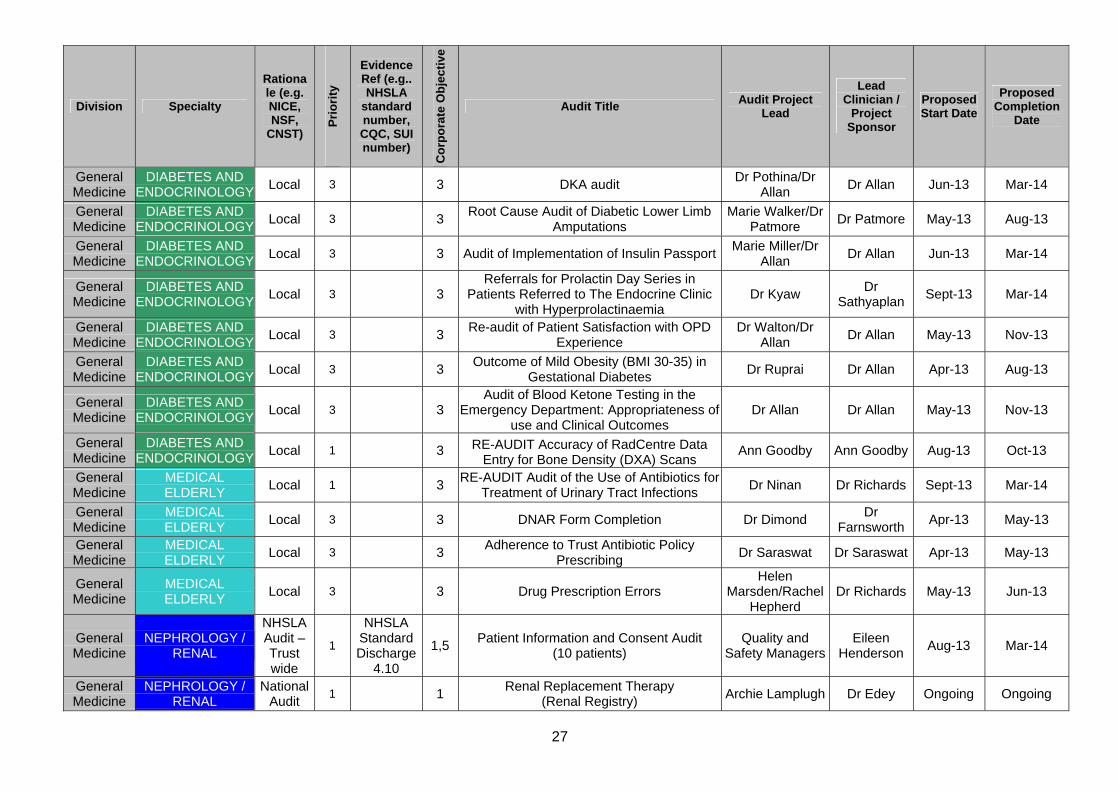
27
Division Specialty
Rationale (e.g. NICE, NSF,
CNST)
Pri
ori
ty
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project
Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
General Medicine
DIABETES AND ENDOCRINOLOGY
Local 3 3 DKA audit Dr Pothina/Dr
Allan Dr Allan Jun-13 Mar-14
General Medicine
DIABETES AND ENDOCRINOLOGY
Local 3 3 Root Cause Audit of Diabetic Lower Limb
Amputations Marie Walker/Dr
Patmore Dr Patmore May-13 Aug-13
General Medicine
DIABETES AND ENDOCRINOLOGY
Local 3 3 Audit of Implementation of Insulin PassportMarie Miller/Dr
Allan Dr Allan Jun-13 Mar-14
General Medicine
DIABETES AND ENDOCRINOLOGY
Local 3 3 Referrals for Prolactin Day Series in
Patients Referred to The Endocrine Clinic with Hyperprolactinaemia
Dr Kyaw Dr
Sathyaplan Sept-13 Mar-14
General Medicine
DIABETES AND ENDOCRINOLOGY
Local 3 3 Re-audit of Patient Satisfaction with OPD
Experience Dr Walton/Dr
Allan Dr Allan May-13 Nov-13
General Medicine
DIABETES AND ENDOCRINOLOGY
Local 3 3 Outcome of Mild Obesity (BMI 30-35) in
Gestational Diabetes Dr Ruprai Dr Allan Apr-13 Aug-13
General Medicine
DIABETES AND ENDOCRINOLOGY
Local 3 3 Audit of Blood Ketone Testing in the
Emergency Department: Appropriateness of use and Clinical Outcomes
Dr Allan Dr Allan May-13 Nov-13
General Medicine
DIABETES AND ENDOCRINOLOGY
Local 1 3 RE-AUDIT Accuracy of RadCentre Data Entry for Bone Density (DXA) Scans
Ann Goodby Ann Goodby Aug-13 Oct-13
General Medicine
MEDICAL ELDERLY
Local 1 3 RE-AUDIT Audit of the Use of Antibiotics for
Treatment of Urinary Tract Infections Dr Ninan Dr Richards Sept-13 Mar-14
General Medicine
MEDICAL ELDERLY
Local 3 3 DNAR Form Completion Dr Dimond Dr
Farnsworth Apr-13 May-13
General Medicine
MEDICAL ELDERLY
Local 3 3 Adherence to Trust Antibiotic Policy
Prescribing Dr Saraswat Dr Saraswat Apr-13 May-13
General Medicine
MEDICAL ELDERLY
Local 3 3 Drug Prescription Errors Helen
Marsden/Rachel Hepherd
Dr Richards May-13 Jun-13
General Medicine
NEPHROLOGY / RENAL
NHSLA Audit – Trust wide
1
NHSLA Standard Discharge
4.10
1,5 Patient Information and Consent Audit
(10 patients) Quality and
Safety ManagersEileen
Henderson Aug-13 Mar-14
General Medicine
NEPHROLOGY / RENAL
National Audit
1 1 Renal Replacement Therapy
(Renal Registry) Archie Lamplugh Dr Edey Ongoing Ongoing
28
Division Specialty
Rationale (e.g. NICE, NSF,
CNST)
Pri
ori
ty
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project
Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
General Medicine
NEPHROLOGY / RENAL
CQUIN 1 1 Recording of Transplant Status in Notes of
New RRT Patients Dr Edey Dr Edey Sept-13 Mar-14
General Medicine
NEPHROLOGY / RENAL
CQUIN 1 1 Vascular Access - Patients Commencing
HD via Catheters Dr Hilton Dr Edey Sept-13 Mar-14
General Medicine
NEPHROLOGY / RENAL
Local 3 3 RE-AUDIT - CMV Viraemia After
Transplantation Dr Hoefield Dr Edey Sept-13 Mar-14
General Medicine
NEPHROLOGY / RENAL
NSF 1 1 Use of Northern Risk Score in Transplant
Work-up Dr Edey Dr Edey Sept-13 Mar-14
General Medicine
NEPHROLOGY / RENAL
NSF 1 1 Availability of Renal Patient View Dr Hazara Dr Edey Sept-13 Mar-14
General Medicine
NEPHROLOGY / RENAL
Local 3 3 Measurement of Folate Levels in Dialysis
Patients Dr Walsh Dr Edey Sept-13 Mar-14
General Medicine
NEPHROLOGY / RENAL
Local 3 3 Epidemiology of Haemodialysis Central
Venous Catheter Infections Dr Syed
Dr Chanayireh
Apr-13 Oct-13
General Medicine Division
NEPHROLOGY / RENAL
Local 3 3
Management of Acute Kidney Injury: the Impact of automated alerts in improving
quality of care as defined in the NCEPOD 2009 recommendations
Dr Naudeer Dr Edey Apr-13 Jun-13
General Medicine
RHEUMATOLOGY Local 3 3
Audit Compliance with MHRA & EMA Recommendations for Long Term
Bisphosphonate Treatment and The Risk of Atypical Fractures
Dr Kallankara Dr Kallankara May-13 Aug-13
General Medicine
RHEUMATOLOGY Local 3 3
Audit Assessing Compliance with Criteria Needed for Achieving Best Practice Tariff for Diagnosis and Management of Inflammatory
Arthritis
Dr Kallankara Dr Kallankara May-13 Jul-13
General Medicine
RHEUMATOLOGY Local 3 3
Assessment of the Compliance with Hull & East Yorkshire Hospitals NHS Trust Drug
Policy with regards to Correct Drug Prescription in the Medical Short Stay Ward
Dr El-Sayed Dr Kallankara Apr-13 May-13
General Medicine
RHEUMATOLOGY Local 3 3 A UK Multicentre Audit of the Management
of Rheumatoid Arthritis Against Treat to Target Guidelines’
Dr Patel Dr Kallankara Apr-12 Mar-14

29
Division Specialty
Rationale (e.g. NICE, NSF,
CNST)
Pri
ori
ty
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project
Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
Specialist Medicine
DERMATOLOGY
NHSLA Audit – Trust wide
1
NHSLA Standard Discharge
4.10
1,5 Patient Information and Consent Audit
(10 patients) Quality and
Safety ManagersEileen
Henderson Aug-13 Mar-14
Specialist Medicine
DERMATOLOGY Local 1 3 RE-AUDIT Clinical Audit of Day Care
Management of Patients with Psoriasis within the Dermatology Department
Dr Graham Dr Walton Dec-13 Mar-14
Specialist Medicine
DERMATOLOGY Local 1 3 RE-AUDIT of Isotretinoin Prescribing in the
Dermatology Department Dr Graham Dr Walton Feb-14 Mar-14
Specialist Medicine
DERMATOLOGY National
Audit 1 1 Psoriasis National Audit
Dr Mohungoo/ Dr Walton
Dr Walton May-13 May-13
Specialist Medicine
DERMATOLOGY Local 3 3 Phototherapy audit Dr Mohungoo Sept-13 Dec-13
Specialist Medicine
CARDIOLOGY
NHSLA Audit – Trust wide
1
NHSLA Standard Discharge
4.10
1,5 Patient Information and Consent Audit
(10 patients) Quality and
Safety ManagersEileen
Henderson Aug-13 Mar-14
Specialist Medicine
CARDIOLOGY National
Audit 1 1 Heart Failure Mandy Walters
Professor Cleland
Ongoing Ongoing
Specialist Medicine
CARDIOLOGY National
Audit 1 1
Coronary Angioplasty (NICOR Adult Cardiac Interventions Audit)
Dr Oliver Dr
BragadeeshOngoing Ongoing
Specialist Medicine
CARDIOLOGY National
Audit 1 1 MINAP Wendy Holiday Dr Hoye Ongoing Ongoing
Specialist Medicine
CARDIOLOGY Local 3 3 MDT Patient Selection and Outcome Dr Waleed Dr Hoye Apr-13 Sept-13
Specialist Medicine
CARDIOTHORACIC SURGERY
NHSLA Audit – Trust wide
1
NHSLA Standard Discharge
4.10
1,5 Patient Information and Consent Audit
(10 patients) Quality and
Safety ManagersEileen
Henderson Aug-13 Mar-14
Specialist Medicine
CARDIOTHORACIC SURGERY
National Audit
1 1 Adult Cardiac Surgery (CABG and Valvular
Surgery) Mr Chaudhry Mr Chaudhry Ongoing Ongoing

30
Division Specialty
Rationale (e.g. NICE, NSF,
CNST)
Pri
ori
ty
Evidence Ref (e.g.. NHSLA
standard number, CQC, SUI number)
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project
Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
Specialist Medicine
CARDIOTHORACIC SURGERY Local 3 3 VATS Biopsy for Benign Lung disease Dr Hardman Mr Loubani Apr-13 May-13
Specialist Medicine
NEUROLOGY National
Audit 1 1
National Audit of Seizure Management (NASH)
Dr Ming Dr Ming Apr-13 Jul-13
Specialist Medicine
NEUROLOGY Local 3 3 Re-audit of the 2 week-wait Referral
Pathway for People with Suspected CNS Tumour
Dr Khalil Dr Harley Apr-13 May-13
Specialist Medicine
NEUROLOGY Local 3 3 Audit of Patient Medical Records Dr Agrawal Dr Harley Apr-13 Dec-13
Specialist Medicine
OPHTHALMOLOGY
NHSLA Audit – Trust wide
1
NHSLA Standard Discharge
4.10
1,5 Patient Information and Consent Audit
(10 patients annually) Quality and
Safety ManagersEileen
Henderson Aug-13 Mar-14
Specialist Medicine
OPHTHALMOLOGY National
Audit 1 1,5
Audit of Quality Measures in Ophthalmology Patients
Miss Cook Miss Cook Ongoing
Ongoing
Specialist Medicine
OPHTHALMOLOGY National
Audit 1 1,5 British Ophthalmological Surveillance Unit Miss Cook Miss Cook
Ongoing
Ongoing
Specialist Medicine
OPHTHALMOLOGY National
Audit 1 1,5
Prospective Audit of Retinal Detachment Surgery via BEAVRs website
Mr Costen Mr Costen Ongoing Ongoing
Specialist Medicine
STROKE National
Audit 1 1,5
SSNAP - Stroke National Audit Programme (combined Sentinel and SINAP)
Dr Abdul-HamidDr Abdul-
Hamid Ongoing Ongoing

31
SURGERY HEALTH GROUP AUDIT PLAN 2013-14
Division
Sp
ecia
lty
Rationale (e.g.
NICE, NSF,
CNST, risk, local
issue)
Pri
ori
ty
Evi
den
ce R
ef
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project
Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard
Health Record Keeping
1.8
1,5 Record Keeping Audit
(30 patients per Health Group, twice a year)
Jul / Jan Aug / Feb
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard
Health Record Keeping
4.8
1,5
Management of Acutely Ill Adult Patients
in Hospital (twice a year, sample size to be
determined)
Outreach Team
Jul / Jan Aug / Feb
Health Group
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5
Discharge (5 patients per ward per quarter)
Divisional Nurse
Managers
May / Aug /
Nov / Feb
Jun / Sept / Dec / Mar
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard Transfusions 5.8
1,5
Policy for the Collection of Samples, Prescriptions, Collection and Transfusion
of Blood and Blood Components (20 casenotes per Health Group per
quarter)
Hospital Transfusion
Team
May / Aug /
Nov / Feb
Jun / Sept / Dec / Mar
Health Group
NHSLA Audit – Trust wide
1
NHSLA Standard Venous
Thromboembolism
5.9
1,5
VTE Policy and VTE Guideline Audit
(25 casenotes per Health Group 3 times per year)
Health Group Medical Directors
May / Sept / Jan
Jun / Oct / Feb
Health Group NHSLA Audit – Trust
1 NHSLA
Standard Clinical
1,5 Clinical Handover of Care (15 per Health
Group annually)
Divisional Nurse
Managers Sept-13 Mar-14

32
Division
Sp
ecia
lty
Rationale (e.g.
NICE, NSF,
CNST, risk, local
issue)
Pri
ori
ty
Evi
den
ce R
ef
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project
Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
wide Handover of Care
4.9
Trauma NEUROSUR
GERY
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5 Patient Information and Consent Audit
(10 patients)
Quality and Safety
Managers
Eileen Henderson
Aug-13 Mar-14
Trauma NEUROSUR
GERY Local 3 Local 3
Imaging and Admission of Children with Head Injuries - Compliance with NICE
Guidelines
Sarah Braungart
Gerry O'Reilly
Mar-13 Jul-13
Trauma ORTHOPAE
DICS
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients per specialty, annually)
Quality and Safety
Managers
Eileen Henderson
Aug-13 Mar-14
Trauma ORTHOPAE
DICS National 1 National 1 National Joint Registry (NJR) Amr Mohsen Ongoing Ongoing
Trauma ORTHOPAE
DICS National 1 National 1 NHFD: Hip Fracture Amr Mohsen Ongoing Ongoing
Trauma ORTHOPAE
DICS Local 3 Local 3
Evaluation of Current Practice for the Use of Abduction Splints/Braces after Closed
Reduction of Dislocated THR Amr Elkhouly Mr Gopal Apr-13 Oct-13
Trauma PLASTIC
SURGERY
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients)
Quality and Safety
Managers
Eileen Henderson
Aug-13 Mar-14
Trauma PLASTIC
SURGERY Local 3 Local 3
Excision Margins of Cutaneous Squamous Cell Carcinoma of the Scalp
Simon Nicholson
Apr-13 Dec-13
Trauma PLASTIC
SURGERY Local 3 Local 3
Use of MRA in Breast Reconstruction with Free Abdominal Tissue Transfer
Simon Nicholson
Apr-13 Jan-14
Trauma PLASTIC
SURGERY Local 3 Local 3
Audit of Rates of Metastasis in Squamous Cell Carcinoma
Ryian Mohamed
Mr Matteucci
Mar-13 Jun-13

33
Division
Sp
ecia
lty
Rationale (e.g.
NICE, NSF,
CNST, risk, local
issue)
Pri
ori
ty
Evi
den
ce R
ef
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project
Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
General Surgery
VASCULAR SURGERY
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients)
Quality and Safety
Managers
Eileen Henderson
Aug-13 Mar-14
General Surgery
VASCULAR SURGERY
National 1 National 1 National Vascular Registry (NVR) Ongoing Ongoing
General Surgery
VASCULAR SURGERY
National 1 National 1 National Carotid Interventions Audit
(included in VSSGBI VSD) Mr Khan Ongoing Ongoing
General Surgery
VASCULAR SURGERY
Local 3 Local 3 EVAR Pathway Mr
Akomolafe Nov-13 Jan-14
General Surgery
VASCULAR SURGERY
Local 3 Local 3 Audit of Uptake of Exercise Programme
for Claudicants Mr
Akomolafe Oct-13 Dec-13
General Surgery
VASCULAR SURGERY
Local 3 Local 3 Audit of Vascular Waiting List Mr
Akomolafe Jul-13 Oct-13
General Surgery
ACUTE SURGERY
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients)
Quality and Safety
Managers
Eileen Henderson
Aug-13 Mar-14
General Surgery
ACUTE SURGERY
National 1 National 1 National Emergency Laparotomy Audit
(NELA) TBC TBC
General Surgery
ACUTE SURGERY
Local 3 Local 3 Audit of MRCP Protocol Mr Gunn Dec-13 Feb-14
General Surgery
ACUTE SURGERY
Local 3 Local 3 Diagnostic Value of Ultrasound on Acute
Surgical Floor Mr Gunn/Mr Lockwood
Jul-13 Oct-13
General Surgery
COLORECTAL SURGERY
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients)
Quality and Safety
Managers
Eileen Henderson
Aug-13 Mar-14
General Surgery
COLORECTAL SURGERY National 1 National Bowel Cancer (NBOCAP) Mr Gunn Ongoing Ongoing
General Surgery
COLORECTAL SURGERY Local 3 Local 3
Role of Early Diagnostic Laparoscopy in the Management of Lower Abdominal
Pain in Female Patients Arif Zafar Apr-13 Jan-14

34
Division
Sp
ecia
lty
Rationale (e.g.
NICE, NSF,
CNST, risk, local
issue)
Pri
ori
ty
Evi
den
ce R
ef
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project
Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
General Surgery
COLORECTAL SURGERY Local 3 Local 3
An Audit of the Incidence and Resource Implications of Perineal Hernias Post AP
Resection Adele Sayers Apr-13 Jan-14
General Surgery
COLORECTAL SURGERY Local 3 Local 3
The Use of Brush Cytology in the Diagnosis of Colorectal Cancer within the
Bowel Cancer Screening Programme
Ruth Loveday
Professor Duthie
Mar-13 Jul-13
General Surgery
UROLOGY
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients)
Quality and Safety
Managers
Eileen Henderson
Aug-13 Mar-14
General Surgery
UROLOGY National 1 National 1 Prostate Cancer Ongoing Ongoing
General Surgery
UROLOGY Local 3 Local 3 Adequacy of VTE Assessments Jamal Omara Mr Myatt Jun-13 Sept-13
General Surgery
UROLOGY Local 3 Local 3 Evaluation of Rectal Flora of Patients
Undergoing Trans-rectal Ultrasound and Biopsy
Ahmad Abdul-
Rahman Mr Myatt Nov-13 Feb-14
General Surgery
UROLOGY Local 3 Local 3 Role of MRI Baseline in Active
Surveillance Lehana Yeo Mr Myatt Nov-13 Feb-14
General Surgery
UROLOGY Local 3 Local 3 The Role of Contrast and Enhanced
Ultrasound in the Evaluation of Localised Prostate Cancer
Pejman Kheirandish
Mr Myatt Nov-13 Feb-14
General Surgery
UROLOGY Local 3 Local 3 Semenalysis in Patients who Have Been
Treated for Testes Cancer John Powell Mr Myatt Nov-13 Feb-14
Specialist Surgery
ENT
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients)
Quality and Safety
Managers
Eileen Henderson
Aug-13 Mar-14
Specialist Surgery
ENT National 1 National 1 Head and Neck Oncology (DAHNO) Mr England Ongoing Ongoing
Specialist Surgery
ENT National 1 National 1 Myringoplasty Audit Mr England Ongoing Ongoing

35
Division
Sp
ecia
lty
Rationale (e.g.
NICE, NSF,
CNST, risk, local
issue)
Pri
ori
ty
Evi
den
ce R
ef
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project
Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
Specialist Surgery
ENT Local 3 Local 3 Audit of Pharyngeal Pouch Management -
Surgical Outcomes Seb Wallis Mr England Apr-13 Mar-14
Specialist Surgery
ENT Local 3 Local 3 Audit of Thyroxine Replacement Post
Total Thyroidectomy Seb Wallis Mr England Apr-13 Dec-13
Specialist Surgery
GASTROENTEROLOGY & ENDOSCOPY
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients)
Quality and Safety
Managers
Eileen Henderson
Aug-13 Mar-14
Specialist Surgery
GASTROENTEROLOGY & ENDOSCOPY
National 1 National 1 Inflammatory Bowel Disease (IBD) Dr Sebastian Ongoing Ongoing
Specialist Surgery
GASTROENTEROLOGY & ENDOSCOPY
National 1 National 1 Audit of Blood Component Use in Patients
with Liver Cirrhosis Shairoz Samji
Dr Abouda Mar-13 Apr-13
Specialist Surgery
HEAD AND NECK MAX
FAX
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients)
Quality and Safety
Managers
Eileen Henderson
Aug-13 Mar-14
Specialist Surgery
HEAD AND NECK MAX
FAX Local 3 Local 3
Maxillofacial SHO Knowledge and Management of Dental Trauma in HRI
A&E Suresh Nayar May-13 May-13
Specialist Surgery
UPPER GI
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients)
Quality and Safety
Managers
Eileen Henderson
Aug-13 Mar-14
Specialist Surgery
UPPER GI National 1 National 1 Oesophago-gastric Cancer (NAOGC) Mr Jain Ongoing Ongoing
Critical Care
ANAESTHETICS
Local 3 Local 3 Muscle Relaxant Audit J Biddulph Dr Lanka Apr-13 Aug-13
Critical Care
ANAESTHETICS
Local 3 Local 3 Cardiothoracic Theatre Start Times C Haworth Dr
Ananthasayanam
Apr-13 Jul-13
Critical ANAESTHET Local 3 Local 3 Vertebroplasty and Kyphoplasty: audit of Philip Apr-13 Jan-14

36
Division
Sp
ecia
lty
Rationale (e.g.
NICE, NSF,
CNST, risk, local
issue)
Pri
ori
ty
Evi
den
ce R
ef
Co
rpo
rate
Ob
ject
ive
Audit Title Audit Project
Lead
Lead Clinician /
Project Sponsor
Proposed Start Date
Proposed Completion
Date
Care ICS Anaesthetic Service Provision Buckley Critical Care
ANAESTHETICS
Local 3 Local 3 An Audit of Rate of Dural Puncture After Epidural Insertion on the Labour Ward
Helen Doherty
Dan Mikl Apr-13 Aug-13
Critical Care
ICU AND HDU
National 1 National 1 Adult Critical Care (ICNARC) P Gray Ongoing Ongoing
Critical Care
ICU AND HDU
National 1 National 1 Potential Donor Audit T Heron Ongoing Ongoing
Critical Care
PAIN SERVICES
NHSLA Audit – Trust wide
NHSLA Standard Discharg
e 4.10
1,5
Patient Information and Consent Audit (10 patients)
Quality and Safety
Managers
Eileen Henderson
Aug-13 Mar-14

37
APPENDIX II
PROPOSED ACTIONS FROM LOCAL CLINICAL AUDITS 2012/13
Local audit Specialty Actions the Trust intends to take to improve the
quality of healthcare provided
Clinical Support
Information Governance Audit for Clinical Support Health Group
Health Group (1) To continue with the current local process ensuring that all elements of Information Governance
are being addressed (2) To undertake a re-audit in October 2013
Comparison of the Labelling Efficiency of White Cells with In-oxine using (i) cell-free plasma and (ii) 0.9% Aqueous Solution of Sodium Chloride
Nuclear Medicine (1) Change protocol to use of 0.9% saline rather than CFP. (2) On-going review of labelling efficiency.
Endoscopic/floroscopic Stenting Versus Operative Gastrojejunostomy for Malignant Gastric Outlet Obstruction
Radiology (1) Consider duodenal stenting when suitable as first line in palliating malignant gastric outlet
obstruction
Quality of Posterior Anterior Chest X-Rays in CHH Match Up to the Standards Set Out by the European Guidelines
Radiology (1) Re-audit (2) Refresh technique (3) Review of exposure factors

38
An Audit to Assess the Accuracy of the Red Dot System on Paediatric X-rays Within A&E Radiology Dept
Radiology
(1) Re-audit (2) More application of the red dot system on paediatric radiographs from radiographers including
better understanding of paediatrics anatomy (3) Review of the red dot system throughout the radiography department with interest to paediatric
abnormality and normality of radiographs
The Effects of Collimation and Lead Rubber Equivalent on Doses to the Thyroid and Gonad in Relation to Chest Imaging
Radiology (1) To amend the paediatrician protection guideline protocol to reflect recommendation of the audit (2) Re-audit. (3) Staff training
Clinical Re-audit of the Use of CT Scanning for Head Injury Patients
Radiology (1) Education of referrers and NICE guidelines (CG56) resent to ED team
Professional Practice Self Audit of Clinical Reporting Skills 2012
Radiology (1) Re-audit to ensure standards are met
Consent Audit for Vascular Radiology
Radiology (1) Re-audit in 18 months, after the day case is well established.
A Retrospective Audit of Barium Swallow Examinations: Accuracy in Cancer Detection in Oesophagus and Pharynx
Radiology (1) Re-audit in 1 year to ensure the accuracy of detection of these cancers
Embolisation of Renal Angiomyolipoma: Complications, Short-Term and Long-Term
Radiology
(1) CT follow-up yearly post embolisation with discontinuation of follow-up if significant size reduction (>30%) has occurred after 3 year
(2) If minor reduction is observed continued follow-up to detect regrowth, repeat embolisation if regrowth occurs at any stage during follow-up
(3) Long-term follow-up for patients with tuberous sclerosis, with techniques not involving ionising
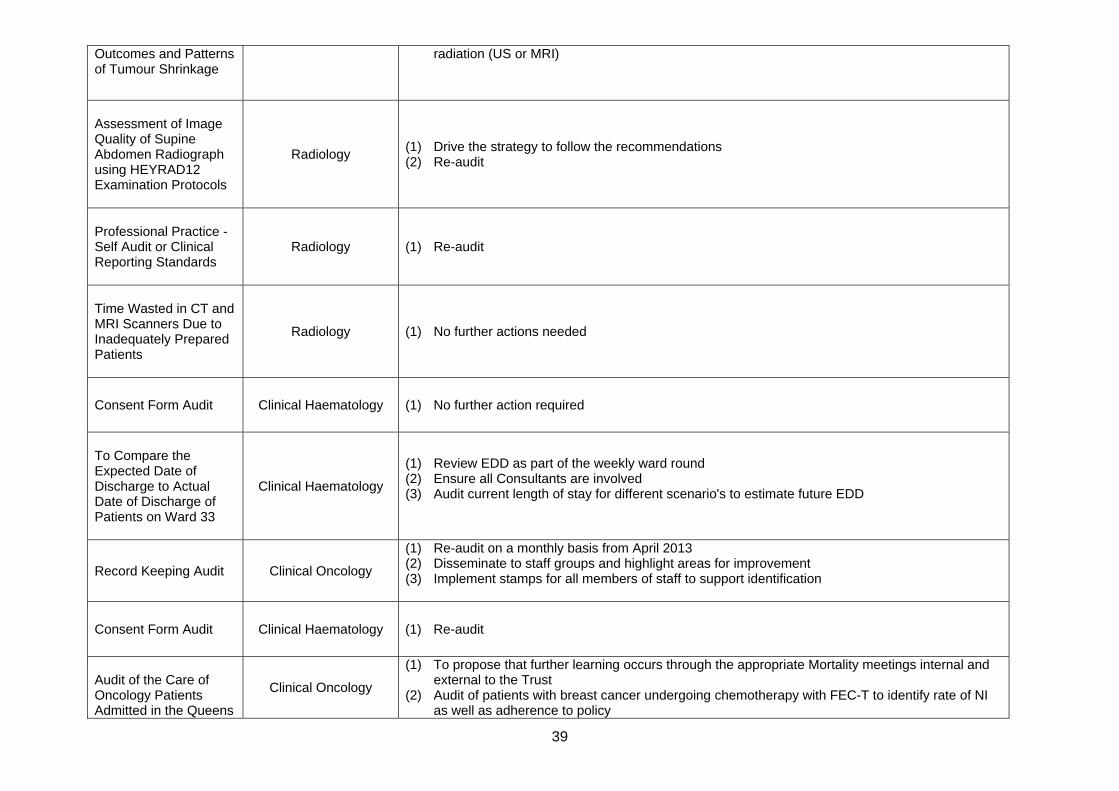
39
Outcomes and Patterns of Tumour Shrinkage
radiation (US or MRI)
Assessment of Image Quality of Supine Abdomen Radiograph using HEYRAD12 Examination Protocols
Radiology (1) Drive the strategy to follow the recommendations (2) Re-audit
Professional Practice - Self Audit or Clinical Reporting Standards
Radiology (1) Re-audit
Time Wasted in CT and MRI Scanners Due to Inadequately Prepared Patients
Radiology (1) No further actions needed
Consent Form Audit Clinical Haematology (1) No further action required
To Compare the Expected Date of Discharge to Actual Date of Discharge of Patients on Ward 33
Clinical Haematology
(1) Review EDD as part of the weekly ward round (2) Ensure all Consultants are involved (3) Audit current length of stay for different scenario's to estimate future EDD
Record Keeping Audit Clinical Oncology
(1) Re-audit on a monthly basis from April 2013 (2) Disseminate to staff groups and highlight areas for improvement (3) Implement stamps for all members of staff to support identification
Consent Form Audit Clinical Haematology (1) Re-audit
Audit of the Care of Oncology Patients Admitted in the Queens
Clinical Oncology
(1) To propose that further learning occurs through the appropriate Mortality meetings internal and external to the Trust
(2) Audit of patients with breast cancer undergoing chemotherapy with FEC-T to identify rate of NI as well as adherence to policy

40
Centre for Oncology and Haematology with Suspected Febrile Neutropenia
(3) Audit adherence to guidelines in the use of G-SCF for the management of NI (4) Continue with the rolling audit (5) Continue effective training of junior doctors in the management of neutropenic infections
Preferred Priorities/Place of Care - Point Prevalence Survey
Clinical Oncology
(1) Sharing of findings as those identified within the dissemination of results (2) Ward visits and planned teaching /awareness work plan programme incorporating the
recognition of Palliative End of life Care patients and the PPOC (3) Repeat Survey in 6 months’ time
Scoping Exercise to Measure the Awareness and Understanding of the Rapid Palliative Discharge Pathway Document
Clinical Oncology
(1) To share the findings of the exercise (2) To identify a link nurse for each of the top ten ward areas and to develop a two way
communication system to enable the cascading of information to support the safe and timely discharge of palliative end of life care patients
Assessment of the Completion of Immediate Discharge Letters Issued to Patients Discharge from the Queens Oncology Centre
Clinical Oncology (1) Re-audit 2014
Extravasation Audit 2012
Clinical Oncology (1) An extravasation form should be completed at time of any extravasation incident and kept with
chemotherapy documentation. To add the Datix number to allow future correlation and audit of data.
Audit to Assess the Indications for the Administration of Parenteral Nutrition (PN) to patients in the Queens Centre for Oncology and Haematology
Dietetics - Therapies
(1) Raise the profile of the nutrition team: Nutrition team to build relationships with ward staff at the Queens centre. Education of doctors around re-feeding syndrome PN, line care etc.
(2) Education of nurses - competency based training re line-care involving teacher practitioners, senior nurses (B6) and ward nutrition link nurses
(3) Repeat the audit using some of the NCEPOD data collection particularly around CVC access.

41
Could a New Approach to the Food Record Chart Help to Reduce Mortality in Hospital Inpatients?
Dietetics - Therapies (1) Training on nutrition screening tool and food chart (2) Re-audit of food charts to ensure compliance
Record Keeping Audit Infectious diseases (1) Re-audit
HIV testing in TB clinic Infectious Diseases (1) Re-audit in 6 months (2) To present the findings of the audit at the TB MDT and to discuss whether a clinic protocol is
needed
Virological/treatment Failure in HIV-infected Patients Established on ART (anti-rettoviral therapy)
Infectious Diseases
(1) Further study to look into other factors not identified such as naïve / experienced, adherence, individual factors and future viral local findings
(2) Closely monitor patients within the LLV group and assess virological and clinical progress and eventual prognosis
(3) Perform more resistance testing (although from real life experience it has invariably been technical limitation in processing the samples rather than requesting the test)
Venous Thromboembolism (VTE) Prophylaxis for Maternal Post Delivery
Pharmacy
(1) Pilot use of the new drug chart on postnatal wards (2) Revise and update TTO to include a space for documenting maternal weight. (3) Staff training on VTE risk assessment, VTE guideline and documentation of information
regarding VTE on drug chart, TTO and maternal record – to sign to confirm (4) Update VTE patient information leaflet regarding VTE prevention by early mobilisation and
hydration, and replace the previous version on the Trust intranet. (5) Update VTE guideline regarding the need to provide and discuss VTE leaflet to all postnatal
women on discharge at renewal date (6) Create and incorporate a discharge checklist for VTE into postnatal maternal records – staff to
sign to confirm information discussed with patients (7) Re-audit clinical compliance with VTE risk assessment.
Drug Policy: Do Doctors Prescribe According to the Prescribing Standards
Pharmacy (1) Further training to junior and senior doctors (2) Alterations to the drug chart (pre-printed amendments)
Appropriateness of Quinolone Prescribing at HEY
Pharmacy (1) Review of guidelines with consideration to making Ciprofloxacin an alert antibiotic (2) Encourage complete documentation, particularly with regards to outpatient prescriptions
Does PGP Affect Obstetric Outcome?
Physiotherapy - Therapies
(1) Staff training/monitoring of birth outcomes

42
Amputation to Cast Audit 2012
Physiotherapy - Therapies
(1) Use results of the audit to inform patients of average amputation to cast time (2) Agree service to monitor the future service (3) Re-audit 2013
Physiotherapy Acute Respiratory COPD Service (PARCS) Outcomes Measures Audit.
Physiotherapy - Therapies
(1) Research EQ-5D and begin trial of its use (2) Re-audit to reassess use of CCQ and to assess usefulness of EQ-5D
Is a Home Visit an Effective Use of Physiotherapy Time for Paediatric Cystic Fibrosis Patients Having Intravenous Antibiotics
Physiotherapy - Therapies
(1) Feedback information to CF team and Physiotherapy manager
Physiotherapy Fracture Management Service
Physiotherapy - Therapies
(1) Patient Satisfaction Survey for spinal # management pathway (2) Re-audit of Activity levels 2011-2012
An Audit of Physio Note keeping Standards
Physiotherapy - Therapies
(1) Re-audit 2014
Rehabilitation Services Head and Neck Cancer Care Pathway Audit/ Service Education
Physiotherapy - Therapies
(1) Larger scale audit of head and neck cancer rehabilitation pathway (2) Review of other cancer rehabilitation pathways
Re-audit- Neurosurgical Physio Phone Follow-up Service Activity 11-12 (previously 2430)
Physiotherapy - Therapies
(1) Activity to be re-audited on a yearly basis (NB – unless discharge to Consultants increases significantly it is not thought appropriate to continue to audit outcomes from clinic reviews)
Physiotherapy Dept Activity Audit
Physiotherapy - Therapies
(1) Review on duty activity and skill mix with Section heads at 1:1s, undertaking further audit as necessary (2) Re-audit annually to ensure clinical time is maximised (3) Development of band 2 physiotherapy helper role which will take on some of the non-clinical duties currently covered by band 3 and band 4 staff

43
A 6 Month Retrospective Analysis of the Neurosurgical Physiotherapy Service for Vertebroplasty Patients
Physiotherapy - Therapies
(1) No actions
Audit of Bereavement Protocols in Women's and Children’s Services Against HTA (Human Tissue Authority)
Histopathology (1) Monitor through joint monthly meetings of bereavement services and W&C (2) Develop guidance for induction training in labour and delivery suite (3) Re-audit in early 2014 - now that the bereavement pathway booklet is fully rolled out
Re-audit of Time to Report of Respiratory Syncytial Virus Testing
Virology (1) Report to Microbiology Audit Group (2) Report to Sister 120, Matron Paediatrics (3) Report to Clinical Support Governance Committee
Audit of Compliance with the Trust Guidelines for Initial Investigations for Sepsis in Adults
Microbiology
(1) Review antimicrobial guidelines (2) Dissemination and education (likely most effective if co-indices with new guidelines launch or
junior doctor induction) (3) Re-audit to ensure compliance

44
Local audit Specialty Actions the Trust intends to take to improve the
quality of healthcare provided Family and Women’s Health
Information Governance Audit
Health Group Wide
(1) Audit findings to be discussed at each of the speciality audit meetings and speciality governance meetings
(2) Discuss audit findings at Senior Staff Meeting (3) Continue to monitor compliance with undertaking Information Governance training through
monitoring at Speciality Governance meetings (4) Shared folders to be established by each speciality and all audit data to be stored within these
folders and to be shared by all members of the project team including the Supervisor/Educational Supervisor
(5) When project leads leave the speciality the audit project must be handed over and a new project lead established to ensure the project is completed
Record Keeping Audit Neonates (1) Add GMC number (2) Repeat audit next financial year as per policy
Audit of Management of Preterm Infants Born Before 28 Weeks Gestation - Re-audit
Neonates (1) Add to admission sheet to collect information on thermoregulation measures (2) Use green sheets for parental communication for antenatal counselling
Use of Epidurals on the Neonatal Unit
Neonates (1) Re-audit in July 2015 (only 4 patients per year) (2) Feedback findings to Guideline Development Group
Surfactant Administration for Preterm Babies at 28 Weeks Gestation
Neonates (1) To consider including prophylactic surfactant administration in babies at 28 weeks of gestation
after further discussion in perinatal meeting
Neonatal Abstinence Syndrome Guideline Audit
Neonates (1) Review 5 sets of notes to cross check morphine given (2) Discuss results with Obstetrics and Midwifery
Management of Babies with Invasive Group B Streptococcus Disease
Neonates (1) Review practice of treatment of grunting babies on PNW/NICU - using specials system and
badger admissions
Audit of Babies at Risk of Neonatal Abstinence Syndrome Admitted to
Neonates (1) Presentation of the audit to midwifery and obstetrics - through NDT audit meeting in May. (2) Presentation of associated audit of management of babies with NAS on the NNU at same
meeting.

45
Transitional Care or Postnatal Wards
(3) Discussion about findings at TC planning meetings
Neonatal Intubation Audit
Neonates
(1) Investigate ways of recording intubation on Badger (2) Ensure sedation for intubation included in induction teaching (3) To trail shared skills development plan for trainees (4) Laminate list of times to be documented after intubation and attach to intubation trolley
NLS Guideline Implementation for Babies Born Through Meconium at the HRI
Neonates (1) Ensure that management of new-borns born through meconium stained liquor is included in
neonatal junior staff induction training.
Clinical Audit of Pre-assessment for Elective Paediatric Surgical Patients
Paediatric Medicine (1) Re-audit (2) Implement Checklist (3) Update other specialities - Mr Daniel to email orthopaedic, ENT & Plastics
Audit of Part C Initial and Review Health Assessments forms
Paediatric Medicine
(1) Development and writing of standards of completion for initial and review health assessments and the reporting documents. Presentation of the standards to managers in CHCP, HEY and the LA for agreement.
(2) Development of training package and then training offered to professionals in community medical, health visitors, school nurses and members of the LAC nursing Team.
(3) Re-audit of quality of documentation completion
Screening for Congenital Hypothyroidism - Are we following the guidance?
Paediatric Medicine (1) Improved documentation in notes about screening results and issue of leaflets by Consultant. (2) Copying the clinic letter to health visitor and screening lab.
Insulin Pumps (CSII) – Are we following NICE guidance?
Paediatric Medicine (1) Improve promotion of pump education (2) Urgent need for more diabetic nurses (3) Re-audit in 3 years
IDLs on Children Admitted to HRI with Diagnosis of Diabetes
Paediatric Medicine (1) Diabetes team to put appropriate information in notes. (2) Including IDL requirements relating to diabetes IDL in junior doctors induction. (3) Re-audit.
Paediatric IDL Coding Audit
Paediatric Medicine
(1) Re-audit (2) Guideline/Protocol for IDL content to be given and available for doctors on wards? ensure
template has relevant prompts

46
Non-operative Management of Blunt Spleen and Liver Trauma
Paediatric Surgery (1) Consider implementing APSA trauma committee guidelines for haemodynamically stable
children with blunt spleen and liver injury
Breast Care Follow up Patient Survey
Breast Screening and Surgery
(1) Outcome form 2 (2) Re-audit August 2014. (3) Education Sessions (4) Telephone assessment appointments (5) To ensure patients are receiving their management plans. Asl patients to complete repeat
survey once plan has been received. (6) To audit the appropriateness of referrals to medical staff. Discussion needs to take place as to
how this audit can be developed. (7) Develop patient survey for patients to complete on discharge.
Impact of Long Acting Reversible Contraception
Gynaecology
(1) Staff and patient education regarding the effectiveness of LARC in reducing unwanted pregnancy.
(2) Address medical and nursing staff training and availability for the MTOP service. (3) Repeat uptake of LARC at MTOP. (4) Audit under 25 year old subgroup for repeat abortion vs. national statistics and method of
contraception at termination.
Gynaecology Miscarriage Audit
Gynaecology (1) Disseminate through audit meeting (2) Disseminate to EPAU Lead. (3) Disseminate to EPAU Nurse lead.
Audit of Pregnancy Advisory Service Against RCOG Evidence Based Guidelines
Gynaecology
(1) Feedback to staff . Raise awareness of need for completion of all parts of pathway; the prompts are there but not used/completed.
(2) Add to STI risk assessment on pathway as prompt. (3) Review arrangements for chlamydia screening in the clinics/ notes completion on the ward. (4) Continue drive to skill medical and nursing staff in discussing and providing all possible methods
of contraception for MTOPs. (5) Highlight need for bridging contraception if immediate method not available/ patient unsure; pre-
assessment medic to do. An Audit to Assess What Percentage of Pregnant Women with a BMI over 30Kg/M2 Attends Healthy Lifestyles Clinics Throughout Their Pregnancy
Obstetrics (1) Implement texting service.
Support for Parents Obstetrics
(1) Education of midwives and nurses on how to access services to support women with communication and language support needs and the importance of documenting the services provided.
(2) Development of a care pack for parents whose baby is receiving palliative care.

47
Record Keeping Monthly Spot Checks
Obstetrics
(1) Maintain and improve general standards of record keeping (2) All midwives to undertake some self-audit of records as per this standard (3) Monthly random spot check of 10 sets of notes using devised tool (4) Revision of spot check audit tool ref: CNST standards
Record Keeping Audit Local Supervising Authority Supervisors of Midwives
Obstetrics
(1) Maintain and improve general standards of record keeping (2) All midwives to undertake some self-audit of records as per this standard (3) Re-audit records on annual basis (4) Revision of self-audit tool/record keeping audit ref: CNST standards (5) Monthly spot check of records to be undertaken to be reported to SoM meetings on a monthly
basis and findings disseminated to managers/midwives issues to be escalated as required number will remain at 10 per month
(6) For record keeping to be re-introduced to mandatory training from February 2013 and all outcomes from the audit to be communicated within the training
Care of Women in Labour
Obstetrics
(1) To research documentation in other Trusts and devise a new Labour Record for use within this Trust.
(2) To continue with education of staff regarding the information which must be completed for the care of women in labour.
(3) Circulate results of this audit through Labour Ward Practitioners Newsletter & Team Training sessions.
(4) Present audit results at Labour Ward Forum.
Continuous Electronic Fetal Monitoring (Quarterly)
Obstetrics (1) Disseminate results (2) Launch Fresh Eyes Approach (3) Update staff as to changes in new guideline
Use of Oxytocin (Bi Annual)
Obstetrics
(1) Results dissemination (2) Audit presentation (3) Change the local guidelines (4) Re-audit
Induction of Labour (Quarterly)
Obstetrics (1) Re-audit to report June 2013. (2) Increase compliance re maternal observations and fetal monitoring through a reminder system. (3) Monitor planning for failed IOL.
High Dependency Care (Bi Annual)
Obstetrics (1) Continue audit through MDT meetings. (2) Highlight new guidelines to staff.
Vaginal Birth After Caesarean Section (Annual)
Obstetrics (1) Raise the profile of use of the VBAC Sticker. (2) Ensure the VBAC leaflet being given at booking appointments. (3) Re-audit 2013/14 to ensure improvement in compliance.

48
Severe Pre-eclampsia (Quarterly)
Obstetrics
(1) Continue to audit all identified cases through MDT and address individuals where appropriate as part of the feedback
(2) Highlight the guideline through YMET training (3) Develop discharge letter
Eclampsia (Quarterly) Obstetrics
(1) Continue to audit all identified cases through MDT & address individuals where appropriate as part of the feedback.
(2) Highlight the guideline through YMET training. (3) Develop discharge letter.
Operative Vaginal Delivery (Quarterly)
Obstetrics (1) Continue to audit all identified cases through MDT and Address individuals where appropriate as
part of the feedback (2) Feedback results through LWP Newsletter
Multiple Pregnancy and Birth (Yearly)
Obstetrics
(1) Report current discrepancies between NICE and Trust Guideline. Provide report to Trust Board to acknowledge working outside NICE Guidance.
(2) Feedback at next Obstetric and Gynaecology Governance meeting that we are working outside NICE Guidance and the results.
(3) Re-audit within the financial year 2013 - 2014.
Perineal Trauma (Bi annual)
Obstetrics
(1) Education of staff regarding importance of documentation of consent, swab/sharp checking and advice.
(2) Education of staff regarding what advice should be given to women post-delivery with regard to perineal care.
(3) Education of staff of the importance of appropriate pain relief for women post birth. (4) Review of paperwork in use to support staff in documentation completion.
Shoulder Dystocia (Quarterly)
Obstetrics
(1) Continue audit through MDT meetings, individual staff members addressed through feedback from these meetings
(2) Highlight new guidelines to staff (3) Importance of completion of proforma through yearly obstetric emergencies training
Post Partum Haemorrhage (Quarterly)
Obstetrics
(1) Continue audit through MDT meetings (2) Explore the new Trust Fluid balance charts and teaching programme (3) Address with individuals where fluid balance has not been appropriately completed via feedback
from MDT case reviews
Venous Thromboembolism - Risk assessment and prophylaxis (Quarterly)
Obstetrics
(1) To introduce a maternity specific VTE risk assessment form for booking and inpatient stays. (2) To update the VTE Guideline against CNST Maternity Standards and the RCOG Green Top
Guideline No 37a (November 2009) Reducing the risk of thrombosis and embolism during pregnancy and the pueperium.
(3) To educate all staff in maternity services surrounding the completion of VTE risk assessment documentation
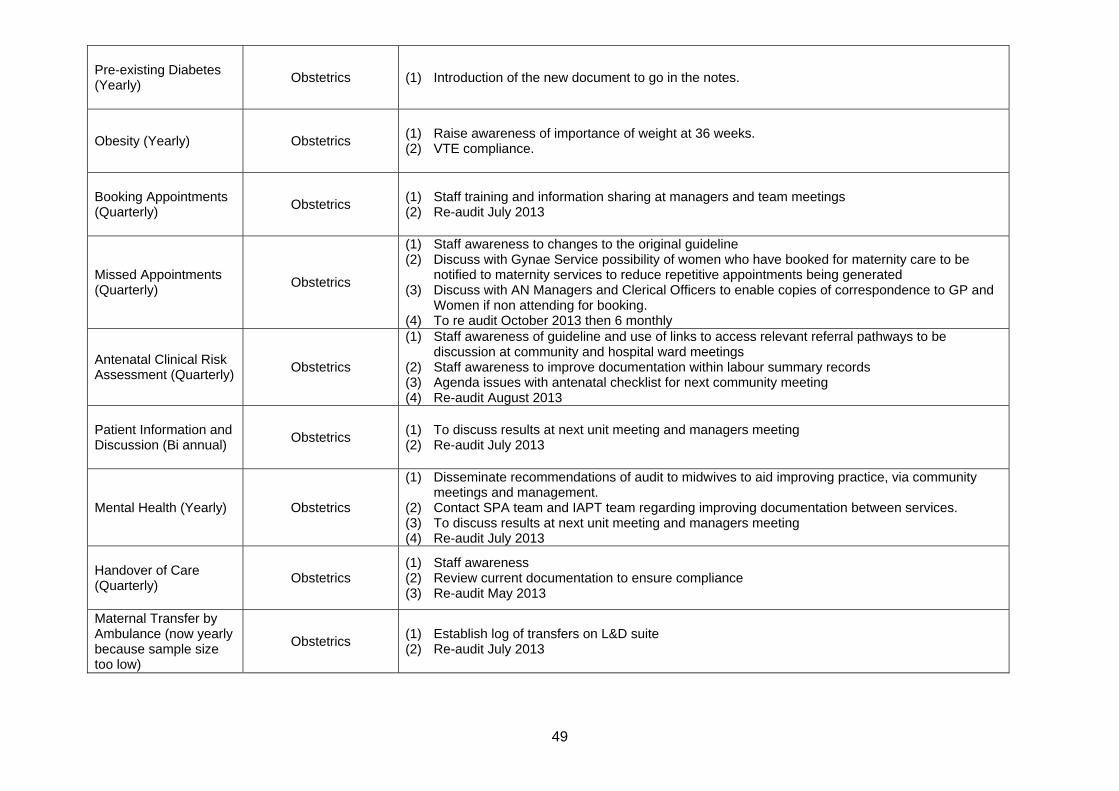
49
Pre-existing Diabetes (Yearly)
Obstetrics (1) Introduction of the new document to go in the notes.
Obesity (Yearly) Obstetrics (1) Raise awareness of importance of weight at 36 weeks. (2) VTE compliance.
Booking Appointments (Quarterly)
Obstetrics (1) Staff training and information sharing at managers and team meetings (2) Re-audit July 2013
Missed Appointments (Quarterly)
Obstetrics
(1) Staff awareness to changes to the original guideline (2) Discuss with Gynae Service possibility of women who have booked for maternity care to be
notified to maternity services to reduce repetitive appointments being generated (3) Discuss with AN Managers and Clerical Officers to enable copies of correspondence to GP and
Women if non attending for booking. (4) To re audit October 2013 then 6 monthly
Antenatal Clinical Risk Assessment (Quarterly)
Obstetrics
(1) Staff awareness of guideline and use of links to access relevant referral pathways to be discussion at community and hospital ward meetings
(2) Staff awareness to improve documentation within labour summary records (3) Agenda issues with antenatal checklist for next community meeting (4) Re-audit August 2013
Patient Information and Discussion (Bi annual)
Obstetrics (1) To discuss results at next unit meeting and managers meeting (2) Re-audit July 2013
Mental Health (Yearly) Obstetrics
(1) Disseminate recommendations of audit to midwives to aid improving practice, via community meetings and management.
(2) Contact SPA team and IAPT team regarding improving documentation between services. (3) To discuss results at next unit meeting and managers meeting (4) Re-audit July 2013
Handover of Care (Quarterly)
Obstetrics (1) Staff awareness (2) Review current documentation to ensure compliance (3) Re-audit May 2013
Maternal Transfer by Ambulance (now yearly because sample size too low)
Obstetrics (1) Establish log of transfers on L&D suite (2) Re-audit July 2013

50
Non-obstetric Maternity Care (Bi annual)
Obstetrics
(1) Send out copies of Guideline 59 and flowcharts from Guideline to Obstetric & Non Obstetric areas to inform of the process
(2) Establish system of labour/maple ward of where the information is to be recorded and investigate possibility of an Obstetric Communication Sheet
(3) Re-audit
Antenatal Screening Tests in Pregnancy (Quarterly)
Obstetrics
(1) Identify way in which maternity services can evidence review of infectious disease screening results within 10 days of them being taken
(2) Failsafe to be put in place in ANC/Community midwifery areas to ensure that all Downs Syndrome Screening tests taken can be accounted for within the required timeframe
(3) Audit proforma to be rewritten to also include requirement for screen positive test results to be audited
(4) Re-audit guideline quarterly
Referral When Fetal Abnormality Detected (Quarterly)
Obstetrics (1) Guideline change regarding ultrasound report
Immediate Care of the Newborn (Quarterly)
Obstetrics (1) Recommendations to be discussed at labour ward forum.
Examination of the Newborn (Quarterly)
Obstetrics (1) Complaint - no actions needed this quarter.
Bladder Care (Quarterly)
Obstetrics (1) 100% compliant - no actions (2) Full compliance positive feedback to be given via newsletter.
Recovery (Quarterly) Obstetrics
(1) To improve compliance with completion of fluid balance charts - actioned through spot check audits
(2) Compliance with discharge and transfer criteria from recovery (3) Compliance with completing set of observations on Recovery Chart (4) Fluid balance chart to be completed, staff to be informed. (5) Minimum observations to ensure staff compliant.

51
Local audit Specialty Actions the Trust intends to take to improve the
quality of healthcare provided
Medicine
Information Governance Audit for Medicine Health Group
Health Group (1) If further audit is required, Central Governance team to consider production of a central audit tool
Consent Audit Health Group
(1) Healthcare professionals should be reminded about the importance of completing each section of the consent form correctly. Medicine Health Group will make results available through Governance Structure (2) Continue annual Audit (3) Consider merging Consent Audit with Patient Information Leaflet Audit (including review of cohort) as per actions from Audit 3306
Trust-wide Patient Information Audit
Health Group
(1) Data collection proforma should be revised (2) Amalgamate audit with other Trust-wide audits (ie consent)
Record Keeping Audit
Acute Assessment Unit
(AAU)
(1) New audit cycle (2) Introduction of new section about importance of accurate record keeping on the Trust intranet site (3) Provision of more posters in the department
An Examination of Hull Royal Infirmary's DVT Re-scanning Policy
Acute Assessment Unit (AAU)
(1) Standards met (97% compliance). Re-audit
Clinical Quality Indicators in AAU
Acute Assessment Unit (AAU)
(1) Re-audit
Management of Sepsis on AAU
Acute Assessment Unit (AAU)
(1) Re-audit (2) Improve training (3) Poster display
Intravenous Peripheral Cannula Audit
Acute Assessment Unit (AAU)
(1) Provide Targeted Training Programme (2) Review Emergency Department assessment documentation (3) Review location of patient information within AAU (4) Monitor staff compliance via HII 2 Cannula Care Bundle (5) Re-audit of practice
Record Keeping Audit Emergency Department
(1) Consideration of changes to A&E Documentation to be discussed at Governance Forum. (2) Re-audit

52
Record Keeping Audit Chest Medicine (1) No actions specified - outcomes form needs re-doing
Clinical Re-audit on Performance and Interpretation of Spirometry
Chest Medicine (1) Spirometry training for junior doctors within first month of rotation
Clinical Audit on Performance and Interpretation of Spirometry (GICU2)
Chest Medicine (1) Spirometry teaching sessions for respiratory junior doctors 2. Re-audit
Clinical Re-audit on Performance and Interpretation of Spirometry (GICU2)
Chest Medicine (1) Spirometry training for junior doctors within first month of rotation
Record Keeping Audit Diabetes And Endocrinology
(1) Medical staff education to ensure proper medical note format including patient identifier, signature and staff designation
(2) Review requirement of bleep number to be recorded (3) Re-audit
Audit of Antibiotic Prescribing on Ward 10
Diabetes And Endocrinology
(1) Trust antibiotic guideline poster in ward - easy for all doctors to see (2) Regular consultants' review for prescribing antibiotics especially in AAU (3) Awareness of inappropriate use of co-amoxilar, to ensure consultants lead by example
Audit of Insulin Pump Service with Particular Focus on Emergency Admissions in Pump Patients and Pump Discontinuation Rates
Diabetes And Endocrinology
(1) The pump team should identify early individuals with no improvement in HbA1c and a record of clinic DNA for discussion about underlying issues as a barrier to achieving poor glycaemic control.
(2) Re-audit in three years.
Audit of Bone Density (DXA) Requests Received
Diabetes And Endocrinology
(1) Chief Technician to discuss implementation of electronic requesting with Clinical Lead (Dr Aye), and appropriate Trust staff.
(2) Re-audit once electronic requesting has been fully operational for at least 3 months
Accuracy of RadCentre Data Entry for Bone
Diabetes And Endocrinology
(1) No actions - re-audit in 2013

53
Density (DXA) Scans
The Use of Head CT Scans to Investigate Delirium in Older People
Medical Elderly
(1) Patients should be fully assessed neurologically for symptoms and signs of intracranial pathology (2) Posters showing the indications for head CT scans can be put up in acute assessment unit and
elderly wards (3) The physical examination page in the admission pathway can be divided into sections of all the
systems including neurological system to help remind doctors to do a full assessment Audit of the Use of Antibiotics for Treatment of Urinary Tract Infections
Medical Elderly (1) Re-audit to ensure improvements are continued
Re-audit of Antipsychotic Prescribing in Acute Hospitals for Patients with Dementia
Medical Elderly (1) Adhere to further National Audit Cycles through the National Audit of Dementia
Dementia Screening: Has the dementia diagnostic assessment tool improved patient care
Medical Elderly
(1) Redesign of DDA tool (2) Training (3) Re-audit (4) Arrange meeting with SPA to develop a referral form for referral of patient’s with a suspected dementia diagnosis to SPA
Record Keeping Audit Nephrology / Renal (1) Clear identification of person signing name (2) Two sided identification of patient 3. 24 hour clock
Recording of Transplant Status in Notes of new RRT Patients
Nephrology / Renal (1) Re-audit (2) Refer patients with type 1 diabetes for work-up with e-GFR = 20
Vascular Access -Patients Commencing HD via Catheters
Nephrology / Renal (1) Re-audit in six months
Record Keeping Audit Rheumatology (1) Record Keeping training for nursing and clerical staff (2) Review the guidelines for ward 1 as no bleep carried by junior staff and no procedures on ward
one

54
EULAR Recommendations for Vaccinations in Adult Patient with Inflammatory Rheumatic Conditions
Rheumatology (1) GP awareness by incorporating a foot note in clinic letters (2) Re-audit
Use of Golimumab According to NICE Guidelines in Inflammatory Arthritis
Rheumatology (1) Ensure follow up appointments offered timely (2) Re-audit in 2015
Record Keeping Audit Dermatology
(1) Re-audit (2) Disseminate and discuss results of this audit with Dermatology Team and Service Managers (3) Ensure familiarity and compliance with the Trust “Patient Documentation Policy” and related
policies (4) Clinicians should be encouraged to use a stamp bearing their name and grade (5) Enhanced support should be made available to the non-clinical staff (6) Prepare a list of the documentation required, as an aide-memoire, for clinicians who perform
minor surgical procedures.
Consent Audit Dermatology
(1) Re-audit. (2) Disseminate and discuss results of this audit with Dermatology Team and Service Managers. (3) Ensure familiarity and compliance with the Trust “Policy on consent to examination or treatment”
and related policies. (4) All patients should receive verbal and written information about their minor surgical procedure
and it should be documented on the consent form that this has been done. (5) The Dermatology Patient Information Leaflet, “Minor Surgery”, should be reviewed and if
necessary updated. (6) Ideally, the clinician carrying out the minor procedure should complete the consent form. (7) Collate a register of those clinicians who:
a) Have been trained in each type of minor surgical procedure and are able to carry out consent for each type of procedure, or who b) are authorised to obtain consent for each type of minor surgical procedure but who are not capable of performing the procedure.
(8) Liaise with the clinicians on an individual basis who completed the consent forms used in this audit to discuss with them the areas where they need to meet the required standards.
(9) All patients should be given a telephone number to contact in the event of a problem post-operatively.
(10) Clinicians should be encouraged to use a stamp bearing their name and grade. (11) A list of abbreviations for use in Dermatology records should be drawn up and approved. (12) The first page of the Trust consent form could be re-designed so that the details of responsible
health professional are separate from the patient details.

55
(13) The specific risks of the minor surgical procedures could be pre-printed on the consent form with adjacent tick boxes.
Isotretinoin Compliance Regional Audit
Dermatology
(1) Re-audit (February 2014) (2) Disseminate and discuss results of audit with Dermatology Team and Senior Managers (3) Ensure the clinicians who prescribe isotretinoin are familiar with the current BAD national
guideline and comply with this (4) Explore development of proformas based on the BAD guidelines 2010 which could be used pre-
treatment, at each follow up visit and at the patients’ final visit
Record Keeping Audit Cardiology (1) Clinicians to sign documentation with full name (not initials) (2) Patient ID on both sides of clinical document
Audit into the Use of Myocardial Perfusion Imaging in Patients Being Considered for Renal Transplantation
Cardiology (1) Complete analysis of data
Record Keeping Audit Cardiothoracic Surgery (1) Printing of name and designation (2) 24 hour clock time of entry (3) Importance of writing in tests requested and results
Record Keeping Audit Neurology
(1) Present the audit findings and recommendations at departmental Governance and educational meetings
(2) Consultant responsible for departmental induction to include record keeping in issues discussed with any new medical staff
(3) Re-audit Re-audit of compliance with NICE Guidelines for Natalizumab Treatment in Multiple Sclerosis
Neurology (1) All Neurology Consultants to be made aware of the recommendations
Record Keeping Audit Ophthalmology
(1) Patient admin to look at front sheet completion (2) Medical staff update on record keeping standards - results of audit and standards to be circulated
to medical staff. (3) Nursing staff update on record keeping standards - results of audit and standards to be circulated
to nursing staff.
Consent Audit Ophthalmology (1) Encourage clinicians and patients to print name, sign and date (2) Patient gender added to label

56
(3) Contact number to be pre-printed on consent form
Screening Plus Pathway
Ophthalmology (1) Obtain DES Programme Board ratification to cease this pathway. (2) Cease entry of new patients into this pathway - HEY Trust agreement. (3) Phase out re-screening of existing Screening Plus patients as agreed with NDESP.
Record Keeping Audit Stroke (1) Improved results from initial audit. Re-audit at a later date
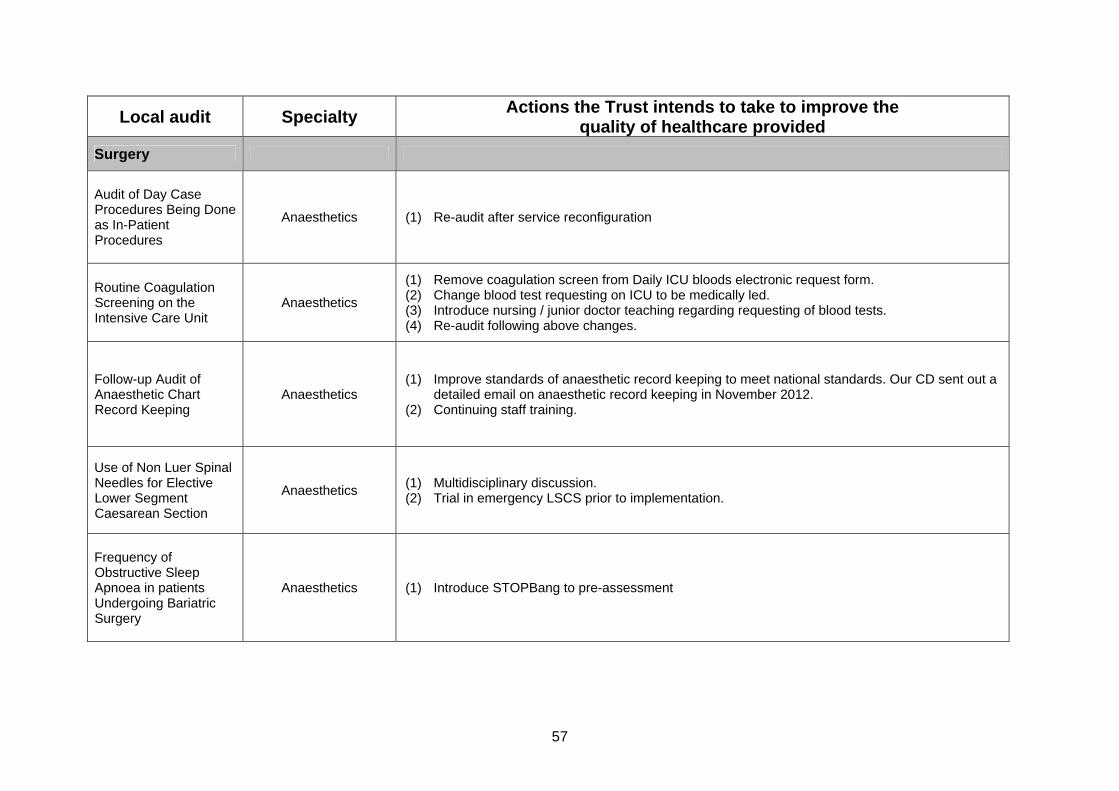
57
Local audit Specialty Actions the Trust intends to take to improve the
quality of healthcare provided
Surgery
Audit of Day Case Procedures Being Done as In-Patient Procedures
Anaesthetics (1) Re-audit after service reconfiguration
Routine Coagulation Screening on the Intensive Care Unit
Anaesthetics
(1) Remove coagulation screen from Daily ICU bloods electronic request form. (2) Change blood test requesting on ICU to be medically led. (3) Introduce nursing / junior doctor teaching regarding requesting of blood tests. (4) Re-audit following above changes.
Follow-up Audit of Anaesthetic Chart Record Keeping
Anaesthetics (1) Improve standards of anaesthetic record keeping to meet national standards. Our CD sent out a
detailed email on anaesthetic record keeping in November 2012. (2) Continuing staff training.
Use of Non Luer Spinal Needles for Elective Lower Segment Caesarean Section
Anaesthetics (1) Multidisciplinary discussion. (2) Trial in emergency LSCS prior to implementation.
Frequency of Obstructive Sleep Apnoea in patients Undergoing Bariatric Surgery
Anaesthetics (1) Introduce STOPBang to pre-assessment

58
Re-audit of Anaesthetic Documentation of Practice During Elective and Emergency Lower Segment Caesarean Section
Anaesthetics (1) Continue to raise awareness of new anaesthetists as to the importance of good documentation
Oxygen Prescription Audit
Critical Care (ICU/HDU)
(1) Amend oxygen prescription chart
Smoking Cessation Advice at Pre-assessment for Colorectal Surgical Patients
Colorectal Surgery (1) To incorporate NHS Stop Smoking services in Pre-assessment Booklet
Record Keeping Audit Colorectal Surgery (1) Introduce ward round pro-forma
Consent Audit Colorectal Surgery (1) Raise awareness at medical local induction
AAA Screening Programme Patient Satisfaction Survey
Vascular Surgery
(1) Ensure there is a chair or appropriate storage area for men’s possessions at Cromwell PCC venue.
(2) Present findings to the NEYNL AAA Screening Programme Director/Business Manager and Divisional General Manager.
(3) Present findings to the NEYNL AAA Screening Programme Team. (4) Present findings to the HEYHT Vascular Surgeons and registrars. (5) Disseminate the report to the NEYNL AAASP Project Board/ Steering Group. (6) Present findings to PCT Leads via project Board members. (7) Share with PCT audit departments and other key stakeholders. (8) Repeat survey bi-annually
Record Keeping Audit Vascular Surgery (1) Ensure all patients have case-note sheets.
Consent Audit Vascular Surgery (1) Minimise use of abbreviations.

59
Consent Audit Urology (1) Encourage everyone to use BMA guidance
Audit to Assess the Efficacy of Management of Post-Operative Hypercalcaemia in Patients Undergoing Total Thyroidectomy
ENT - Head and Neck (1) Roll-out of hypoglycaemia management protocol
Record Keeping Audit ENT - Head and Neck (1) Ensure enough patient identifier labels are available and encourage their use on every sheet. (2) Adopt a consistent approach to documentation. (3) Stopping the use of abbreviations on consent forms
Consent Audit ENT – Head and Neck (1) Staff to write legibly. (2) There should be access to patient information leaflets. (3) Patients should be given copies of the forms (pink sheets).
Gastroenterology and Endoscopy
Record Keeping Audit (1) Education to junior doctors - add to induction for junior doctors.
Gastroenterology and Endoscopy
Consent Audit
(1) Raise awareness regarding lack of demographic information
Proportion of Radiographs Repeated When Original Supplied as Paper Printout of Digital Image
Oral Maxillofacial Surgery
(1) Local guidelines and cover letter to be sent to local practitioners (2) Contact Driffield re PACs image drop box precedent (3) Re-audit in 6 months
Consent Audit Oral Maxillofacial
Surgery (1) To look into the possibility of a dedicated Orthodontic treatment consent form
Mortality After Hip Fracture Surgery: Rates and Causes
Orthopaedics and Trauma
(1) Disseminate findings especially preventable causes of death to the staff caring for hip fracture patients.
(2) Plan re-audit for 2010-2011 fiscal year in order to see if mortality rate has improved. (3) Present findings of audit at international meeting in order to disseminate results to the wider
research community

60
Audit on Delays and Theatre Time Loss for Elective Neurosurgical Cases
Orthopaedics and Trauma
(1) The first patient on the list should be admitted the night before and the pre-admission process to be completed at the latest by 8am on the day of surgery.
(2) Poster to highlight audit findings to be placed in neurosurgical theatres and wards. (3) Cranial cases to be scheduled second on the list where possible
Repatriation of Neurosurgical Patients
Neurosurgery (1) To escalate to senior management
Audit of Flexor Tendon Rupture Rates for 2011
Plastic Surgery (1) Increased consultant level input for tendon procedures
An Audit of Vaginal Melanomas Managed by Plastic Surgery
Plastic Surgery (1) Ensure new patients continue to be seen in a timely fashion

61
APPENDIX III The reports of 33 national clinical audits were reviewed by the provider in 2012/13 and Hull and East Yorkshire Hospitals NHS Trust intends to take the following actions to improve the quality of healthcare provided:
National audits Proposed actions
Neonatal intensive and special care (National Neonatal Audit Programme - NNAP)
Recommendations are being formulated by the Yorkshire Neonatal Network Board. These will be disseminated and implemented across all the networks within the Yorkshire region.
Paediatric pneumonia (British Thoracic Society)
To review the pneumonia guidelines to include: › Admission criteria › Investigations › Antibiotic choice › Management & investigation of complications › Follow-up
Paediatric asthma (British Thoracic Society)
To revise the current asthma pathway and documentation.
To ensure staff are aware of the new pathway and documentation to be completed.
To re-audit when asthma pathway has been adapted and fully implemented.
Paediatric intensive care Audit (Paediatric Intensive Care Audit Network - PICANet)
To develop written information for parents regarding the service.
Diabetes (Royal College of Paediatrics and Child Health - RCPCH National Paediatric Diabetes Audit)
To develop a system of automated text reminders 48 hrs prior to appointment.
The MDT and Retinal screening service to monitor and enrol in the screening programme.
To re-establish the 24 hour telephone support service for children and families.
To aim to extend current support to all children in the care of the Paediatric Diabetes team.
To develop collaborative networking with teams in Yorkshire and aim to attend 80% of meetings.
To establish regular education programme for children and parents.
To hold regular teaching / training sessions for ward staff and junior doctors.
A parent representative to attend MDT meetings. To collect information from 80% of service users
about the current provision of the service. Emergency use of oxygen (British Thoracic Society)
To change the position of the pre-printed oxygen prescription on the drug card
To ensure staff receive ongoing training To continue the Quality Monitoring Programme
which will look at the implementation of changes.

62
Non invasive ventilation (NIV) – adults (British Thoracic Society)
To improve documentation around the mode of ventilation
To issue oxygen alert cards for patients with type 2 respiratory failure. This needs addressing to avoid over-oxygenation by ambulance crews
To look at levels of oxygen given to patients prior to hospital admission, excess oxygen being a contributory factor in respiratory failure
Adult critical care (Case Mix Programme) *No annual report - service receives quarterly reports per ward HICU GICU1, GICU2.
A local audit using CMPD data is proposed to identify management issues of Sepsis and Ventilator Associated Pneumonia in relation to the Standardised Mortality Ratio score for Hull Royal Infirmary and Castle Hill Hospital.
Feedback regarding the increasing figure of delayed discharges has been escalated to senior management and planners.
A local audit is currently underway to assess staff knowledge of Critical Care Minimum Data Set definitions in order to create an education programme to support achievement of maximum funding.
Potential donor audit (NHS Blood and Transplant)
To continue to address education needs, and disseminate guidance and policies, update hospital policies to achieve 100% referral rate and 100% Brain Stem death testing rate.
To update all guidance and policies relating to Organ and tissue donation.
Seizure management (National Audit of Seizure Management)
To produce a guideline and a proforma for patients presenting to the Acute Assessment Unit and Emergency Department with a seizure.
Diabetes (National Adult Diabetes Audit)
The diabetes specialist team will continue to work with commissioners both existing, and emerging CCGs, through the Hull & East Riding Diabetes Network to support commissioners in the planning of service design and delivery to meet the increasing prevalence recognising that over 90% of diabetes contacts for adult services occur within primary care
The diabetes specialist team will review the pathway for individuals with Type 1 diabetes who repeatedly fail to attend outpatient appointments and have not engaged with diabetes services as they are a group at very high risk of poor outcome.
To develop initiatives to investigate the high rate of amputations, understand the underlying causes and work to reduce amputations involve: - Root cause analysis of major amputations - Competency assessment of podiatry services - Launch of e-learning package on foot examination supported by Yorkshire & Humber SHA including risk assessment in accordance with NICE and appropriate referral to foot protection team launched April 2012 as joint work of specialist diabetes podiatrists employed by Humber Mental Health Trust and HEY diabetes team
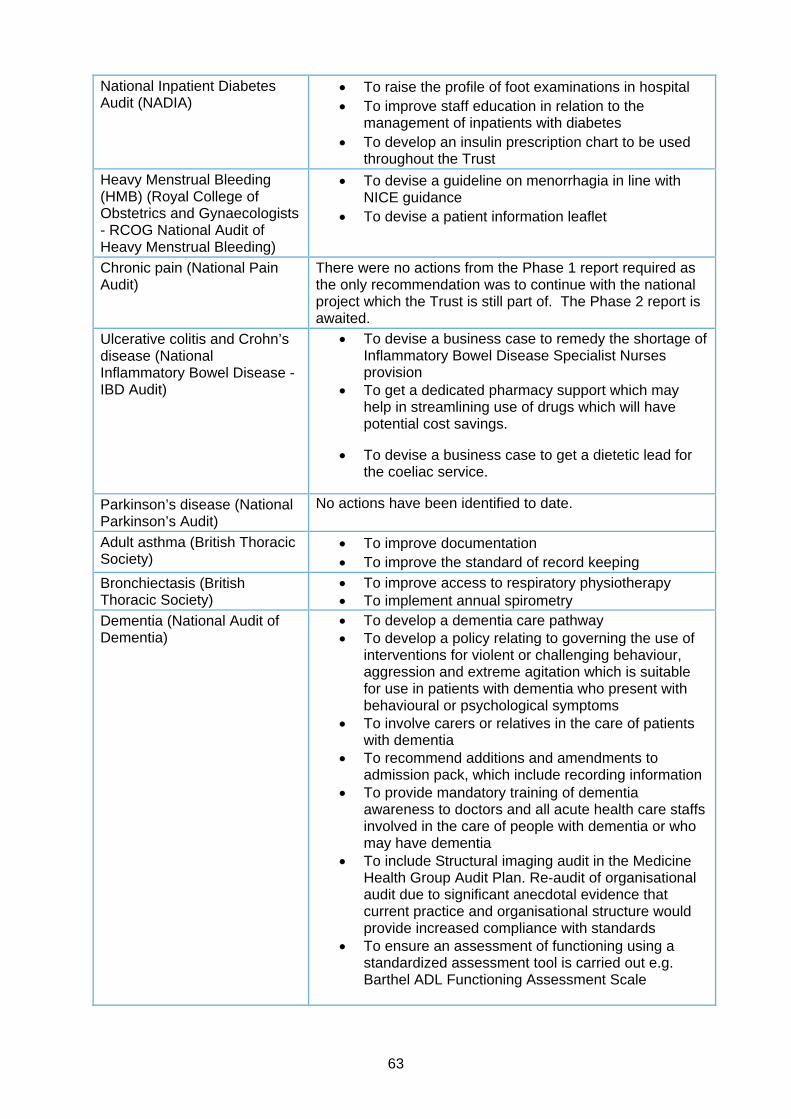
63
National Inpatient Diabetes Audit (NADIA)
To raise the profile of foot examinations in hospital To improve staff education in relation to the
management of inpatients with diabetes To develop an insulin prescription chart to be used
throughout the Trust
Heavy Menstrual Bleeding (HMB) (Royal College of Obstetrics and Gynaecologists - RCOG National Audit of Heavy Menstrual Bleeding)
To devise a guideline on menorrhagia in line with NICE guidance
To devise a patient information leaflet
Chronic pain (National Pain Audit)
There were no actions from the Phase 1 report required as the only recommendation was to continue with the national project which the Trust is still part of. The Phase 2 report is awaited.
Ulcerative colitis and Crohn’s disease (National Inflammatory Bowel Disease - IBD Audit)
To devise a business case to remedy the shortage of Inflammatory Bowel Disease Specialist Nurses provision
To get a dedicated pharmacy support which may help in streamlining use of drugs which will have potential cost savings.
To devise a business case to get a dietetic lead for the coeliac service.
Parkinson’s disease (National Parkinson’s Audit)
No actions have been identified to date.
Adult asthma (British Thoracic Society)
To improve documentation To improve the standard of record keeping
Bronchiectasis (British Thoracic Society)
To improve access to respiratory physiotherapy To implement annual spirometry
Dementia (National Audit of Dementia)
To develop a dementia care pathway To develop a policy relating to governing the use of
interventions for violent or challenging behaviour, aggression and extreme agitation which is suitable for use in patients with dementia who present with behavioural or psychological symptoms
To involve carers or relatives in the care of patients with dementia
To recommend additions and amendments to admission pack, which include recording information
To provide mandatory training of dementia awareness to doctors and all acute health care staffs involved in the care of people with dementia or who may have dementia
To include Structural imaging audit in the Medicine Health Group Audit Plan. Re-audit of organisational audit due to significant anecdotal evidence that current practice and organisational structure would provide increased compliance with standards
To ensure an assessment of functioning using a standardized assessment tool is carried out e.g. Barthel ADL Functioning Assessment Scale

64
Hip, knee and ankle replacements (National Joint Registry)
Total Hip Replacements The Orthopaedic Surgeons no longer routinely
perform Hip Resurfacing Surgery or Metal on Metal Hip Replacements, as per report recommendations. The only cases performed within the Trust are on male patients who are requesting another Resurfacing Joint Replacement after a successful resurfacing on the other side. These patients are being warned of the potential problems and that the surgery is not to be undertaken lightly.
As per report recommendations the Trust is showing a growing trend within the Elective Orthopaedic Department for Cemented Hip Replacements being performed on men and women over 70 years of age. This will be discussed and encouraged further in Clinical Governance meetings.
Total Knee Replacements One of the main points discussed in this years report
appertaining to Total Knee Replacements is the use of Fixed Bearing Prosthesis. This Trust does not use any Mobile Bearing Prosthesis and uses fixed bearings for all Total Knee Replacements.
Data Inputting As per a new requirement of the National Joint
Registry, the Trust will begin to input all the Shoulder Replacements performed.
Carotid interventions (Carotid Intervention Audit)
A recent visit around the Stroke Service provided the following actions:-
The Trust will continue to provide acute stroke lysis/acute carotid surgery and image predominantly through duplex rather than MRA.
All patients will be seen by a dedicated stroke physician following pathways of care.
Dedicated daily sessions for duplex in lab will be provided for the TIA service.
QA process for imaging in place. Acute Myocardial Infarction and other Acute Coronary Syndrome (Myocardial Ischaemia National Audit Project – MINAP)
To review the management of patients with STEMI who initially present to HRI.
To develop a pathway with emergency medicine to ensure prompt management of patients with STEMI who are not directly transferred for primary angioplasty.
Heart failure (Heart Failure Audit)
The provision of the heart failure service will be reviewed as part of a strategic review of cardiac services.

65
Acute stroke (Stroke Improvement National Audit Programme – SINAP)
To educate all staff, work on the Trust pathway and produce posters for awareness that all stroke patients should be directly admitted to a stroke unit equipped to manage acute stroke patients.
To ensure patients receive the same standard of care whether admission to hospital is in or out of hours. There is a 24/7 on call for stroke service and thrombolysis.
To improve co-ordination of care to reduce the delays within hospital control. On arrival, patients to be triaged rapidly to a specialist stroke team, undergo brain scanning, be thrombolysed where appropriate and be admitted to a stroke bed in a designated stroke unit.
To improve education across the Trust regarding stroke symptoms and how to contact the stroke team. This will reduce the current unacceptable delays.
To ensure that all stroke patients have access to a stroke service that can deliver thrombolysis safely and effectively. Any patients who are eligible for thrombolysis should receive it.
To place all incontinent patients onto a clear plan for continence management within 72 hours of admission.
To regularly maintain public awareness campaigns to reinforce the message that stroke needs to be treated as a medical emergency. The Act F.A.S.T campaign has been suggested to the commissioners
Stroke care (National Sentinel Stroke Audit)
The direct stroke unit admission policy has been extended to direct admissions 24/ 7. To ensure the RMO2 reviews the patients after midnight to ensure that transfers to the stroke unit are safe.
To produce a business case for dedicated in-reach neuropsychology support and a dedicated discharge liaison support worker
Nursing staff, occupational therapy assistants and physiotherapy assistants have been appointed and a business case will be put forward for further positions.
The Trust was accredited as a level one hyper acute stroke unit in September 2011. There will be another visit from the Peer Reviewers to monitor the process. Hull was the first Trust to be accredited in Humberside and Yorkshire region.
Renal replacement therapy (Renal Registry)
To continue to supply data on all Renal Replacement Therapy patients as per the Renal Registry
Lung cancer (National Lung Cancer Audit)
To ensure CT scan performed first/ pre-booking, to streamline diagnostic cancer pathway
To ensure specialist nurse is present at diagnosis To consolidate patient flow through specialist multi-
professional clinic
Bowel cancer (National Bowel Cancer Audit Programme)
This data will be looked at during our AGM in May 2012 but there are no current existing actions and mortality is in an acceptable range.

66
Head and neck cancer (Data for Head and Neck Oncology - DAHNO)
To increase input from allied specialties to the Somerset database and thus to DAHNO.
The MDT manager is to meet monthly with Consultants, Speech and Language Therapists and Dieticians to input patients into DAHNO.
To review whether additional resources are required to ensure the following national targets are met - 100% newly diagnosed patients should have been assessed by 1) Clinical Nurse Specialist 2) Dietician 3) Speech and Language Therapist before their treatment starts. Also, 85% of histopathology reports for suspected cancer should be reported within 7 days.
Hip fracture (National Hip Fracture Database)
Through discussion with the Yorkshire Ambulance Service, a protocol will be put in place to provide an early warning of hip fracture patients to ensure prioritisation of bed and theatre slots
To write a business case for the recruitment of a Nurse Practitioner to be prepared to early optimise patients for theatre
To increase investment to orthogeriatrician cover of wards, particularly at weekends and holiday periods
To increase flexibility of theatre sessions through peak times to ensure timely management of patients.
Falls and non-hip fractures (National Falls and Bone Health Audit)
To ensure orthogeriatricians undertake falls assessments and to treat underlying causes.
To ensure nurses, physiotherapists and occupational therapists undertake falls assessment.
For Osteoporosis assessments to be done by orthogeriatricians and to provide secondary prophylaxis of osteoporosis.
Bedside transfusion (National Comparative Audit of Blood Transfusion)
Provide results to Nurse Directors and Medical Directors with a requirement for each Nurse Director to provide reassurances to the Hospital Transfusion Committee as to how they will action the findings.
Transfusion Nurse Specialist to attend Nurse Directors meeting in March 2012, for feedback on Health Group response to the audit.
Recommend that each Health Group undertakes a 5 patient mini-audit to identify if compliance has improved.
Hospital Transfusion Committee to review the Transfusion policy in relation to the recording of observations for demonstrating compliance regarding forthcoming NHSLA assessment.
Re-audit as per national comparative audit plan.Care of dying in hospital (NCDAH)
To roll out training in care of the dying for all staff. To recruit an End of Life Facilitator to support
education and training.

67
APPENDIX IV ANNUAL REPORT ACTION TRACKER
Action Lead Date to be completed by RAG Status
To transfer the audit plan and project documentation to Covalent to enable more efficient monitoring and reporting of the implementation of the plan
Clinical Audit and Effectiveness Manager
September 2013
To devise a new template to record the results of national audits, which includes the action plan
Clinical Audit and Effectiveness Manager
June 2013
To increase the number of outcomes forms for completed clinical audits
Health Group Medical Directors / Quality Facilitators / Quality and Safety Managers
March 2014
To improve the quality of outcome forms, including the requirement to state the reason for a re-audit being the only identified action
Health Group Medical Directors / Quality Facilitators / Quality and Safety Managers
March 2014
The effectiveness of the policy to be monitored via quarterly reports to the Clinical Audit and Effectiveness Committee.
Clinical Audit and Effectiveness Manager
Ongoing
To monitor the actions identified in relation to national audit reports via the corporate action tracking template.
Clinical Audit and Effectiveness Manager / project leads
Ongoing
To email the Clinical Leads the revised BCR form for the NICE
Clinical Audit and Effectiveness Manager
Ongoing

68
guidelines to determine compliance
To monitor the identified actions from the NCEPOD studies via the corporate action tracking template and report to the Clinical Audit and Effectiveness Committee.
Clinical Audit and Effectiveness Manager
Ongoing