hsb examples from finland nea malila mass screening registry, cancer society of finland and...
TRANSCRIPT
HSB examples from Finland
Nea Malila Mass Screening Registry,
Cancer Society of Finland and University of Tampere,
Tampere School of Public Health
Purpose of screening
Main aim is to reduce mortality– From the disease screened
Sometimes also to reduce incidence– E.g. Cervix cancer
To improve quality of life– Evaluation?
Means of screening– early diagnosis– finding pre-invasive lesions
Evidence needed
General proof on efficacy: – Screening works in principle– In ideal conditions screening results in reduction of mortality
as demonstrated by a randomised screening trial
Specific proof on effectiveness: – Screening as a public health policy (or as a routine health
service) results in reduction in mortality in the target population as shown preferably by a randomised design

What is the evidence for public health policy?
Direct evidence, conclusive– randomised allocation of screening within the
routine
Indirect evidence, inconclusive– time trends– geographical differences– survival difference between localised and
nonlocalised disease
Evaluation of public health activities
Effects on health often small – design to identify even small differencesTraditionally before-after comparisons – crude Case-control studies - biasedContradictory effect, e.g. screening can reduce both mortality and quality of lifeTherefore, for practical reasons, mortality is regarded as the most important effectMeans not to be intermixed with effects (e.g. finding of early cases is not sufficient evidence)Common misunderstandings:– Not enough cancers found – bad programme (cervix)– Late stages found – bad programme (colorectal)
Breast cancer screeningNationwide population based screening introduced in Finland in 1987
A group randomised design was used: Women born in odd years were controls during the first years of the programme
Women born in even years (aged 50-64) were invited for screening starting with 3 age cohorts and expanding gradually over the next four years to cover the target population
Over the years 1987-89 76400 women were screened, 13500 invited but not screened and 68800 were controls
References: – Hakama M et al. BMJ, 1997, 314:864-867– Hakama M et al. J Med Screen, 1999, 6:209-216
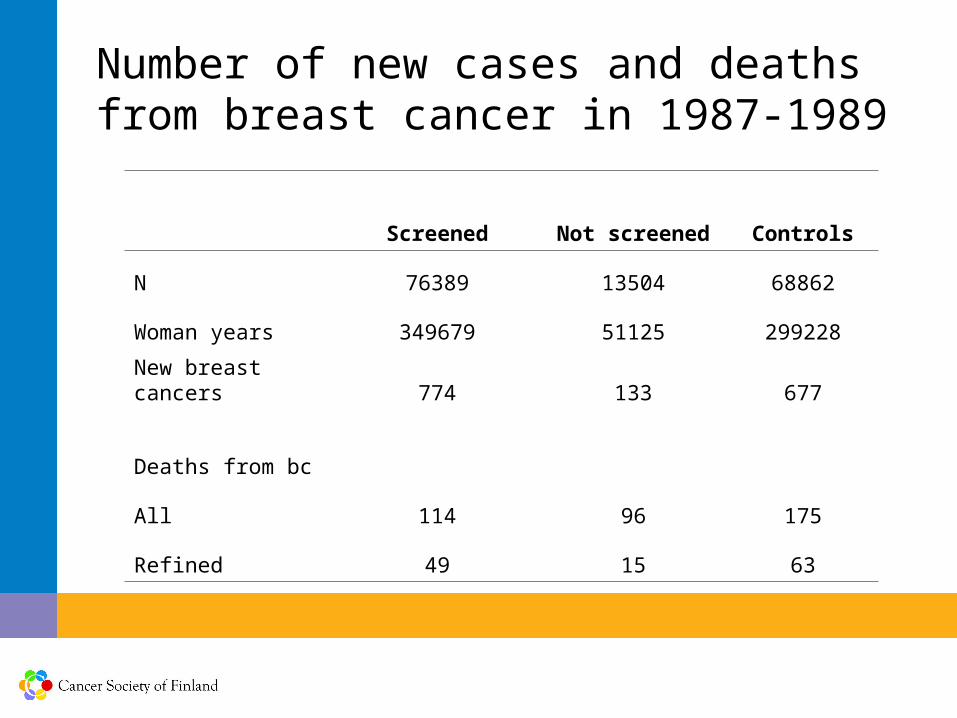
Number of new cases and deaths from breast cancer in 1987-1989
Screened Not screened Controls
N 76389 13504 68862
Woman years 349679 51125 299228
New breast cancers 774 133 677
Deaths from bc
All 114 96 175
Refined 49 15 63
Analysing at the individual level
External control – total bc mortality in the invited compared to all Finland– Biased, participating municipalities not fully representative– Weakened by inclusion of deaths from cancers diagnosed
before screening
Internal control – total mortality– Removes bias from self selection but still weakened by the
inclusion of deaths from cancers diagnosed before screening
Internal control – refined mortality– Confining deaths to cancers diagnosed after onset of
screening removes both bias and dilution of effect
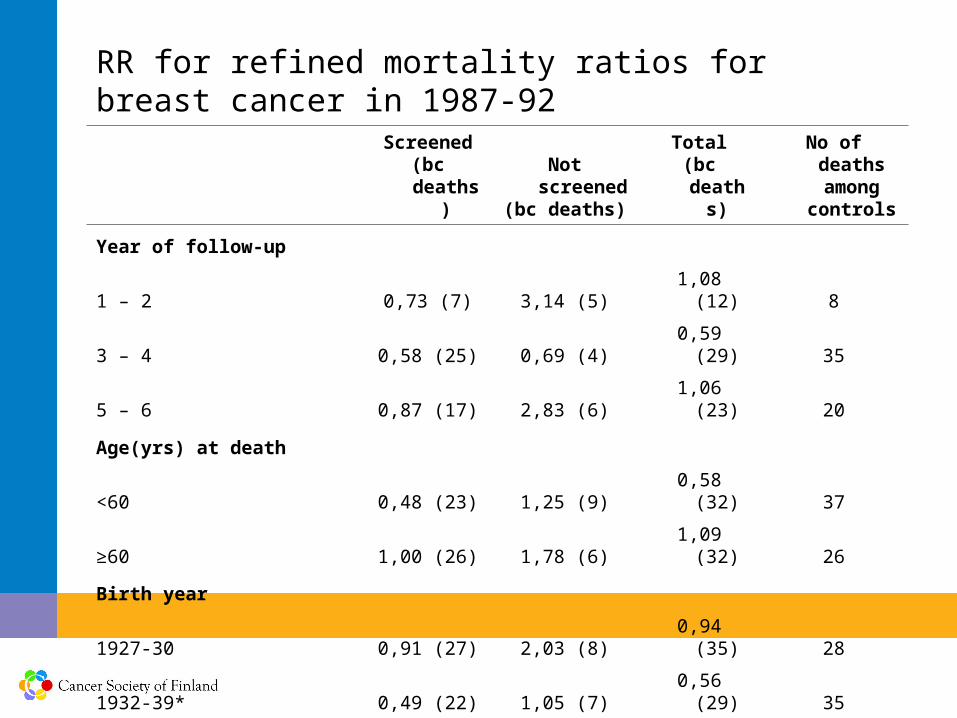
RR for refined mortality ratios for breast cancer in 1987-92
Screened
(bc deaths)Not screened(bc deaths)
Total(bc deaths)
No of deaths among
controls
Year of follow-up
1 – 2 0,73 (7) 3,14 (5) 1,08 (12) 8
3 – 4 0,58 (25) 0,69 (4) 0,59 (29) 35
5 – 6 0,87 (17) 2,83 (6) 1,06 (23) 20
Age(yrs) at death
<60 0,48 (23) 1,25 (9) 0,58 (32) 37
≥60 1,00 (26) 1,78 (6) 1,09 (32) 26
Birth year
1927-30 0,91 (27) 2,03 (8) 0,94 (35) 28
1932-39* 0,49 (22) 1,05 (7) 0,56 (29) 35
Total 0,67 (49) 1,42 (15) 0,76 (64) 63
*excluding 1936 and 1937
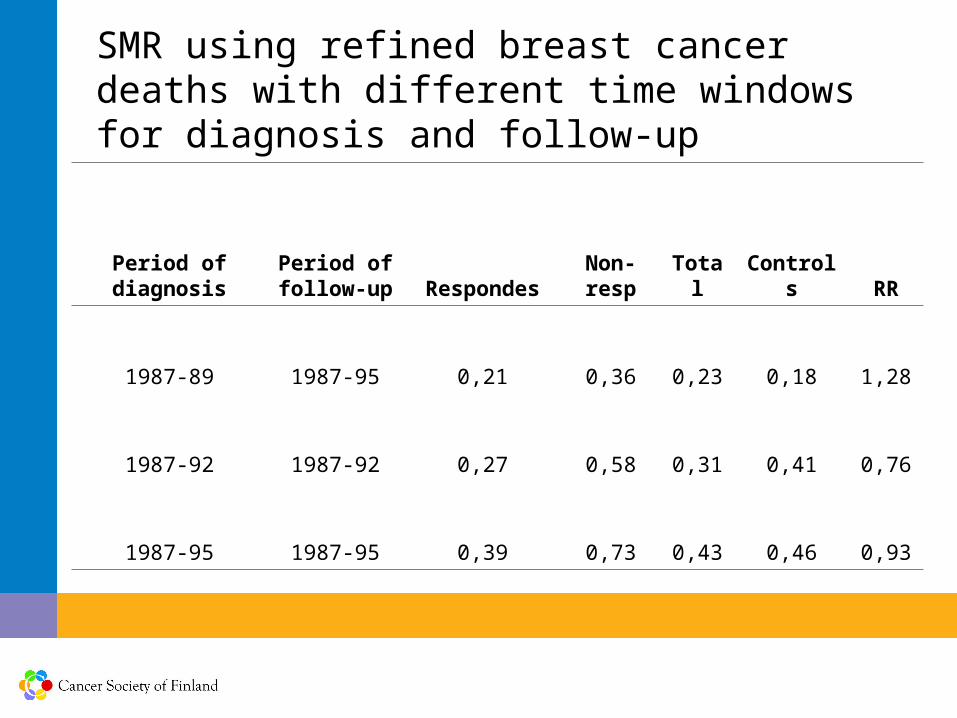
SMR using refined breast cancer deaths with different time windows for diagnosis and follow-up
Period of diagnosis
Period of follow-up Respondes
Non-resp Total Controls RR
1987-89 1987-95 0,21 0,36 0,23 0,18 1,28
1987-92 1987-92 0,27 0,58 0,31 0,41 0,76
1987-95 1987-95 0,39 0,73 0,43 0,46 0,93
Colorectal cancer screening
A population based routine programme for CRC screening– is it feasible and effective in Finland (effectiveness)? – gradual implementation in the target population– Individual level randomisation: screening and control groups
Open questions:– Acceptance of the population – attendance rates – Colonoscopies, need, acceptance, and quality– Need of information and guidance– Programme costs in Finland– Effectiveness in Finland as a public health policy

The effects of screening during the first two years
Invited to screening: 15% of the target population (60-69-year olds) by yearIn Finland the entire target population 500 000 Maximally 80 000 invited /yearAt present the colonoscopy capacity roughly 50 000 (to even 100 000)colonoscopies/yearNeed of colonoscopies c.1100/year in the entire country (if 2% positive) – only marginal increase in resources
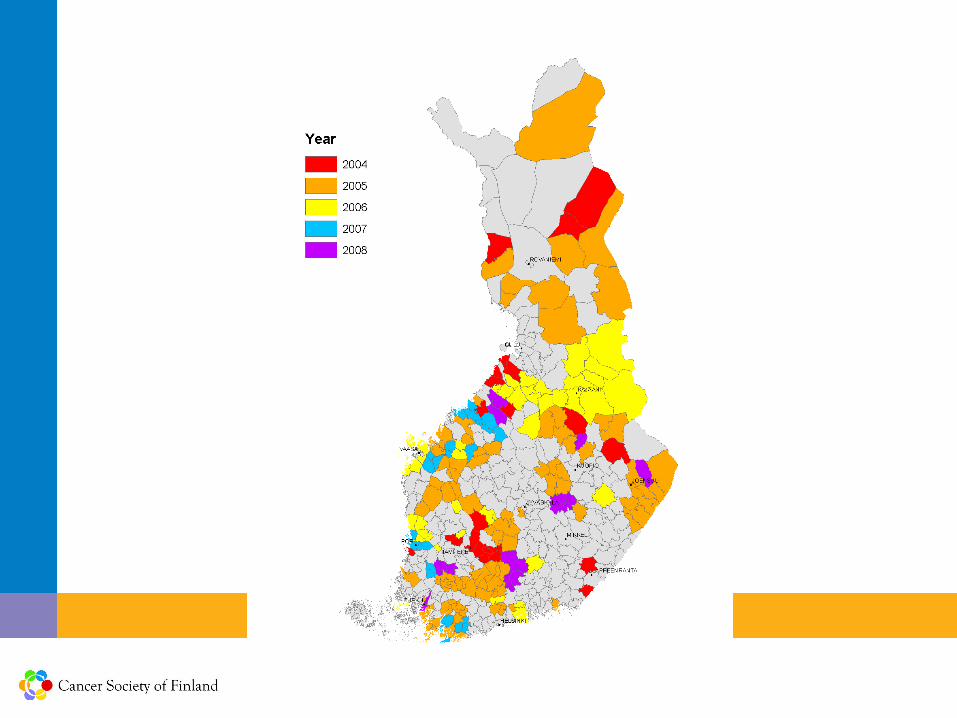
Launch of screening in 2004
A population-based screening programme in 22 pilot municipalitiesIn 2008, 190 municipalities had joined inCentrally planned, organised and runGradual implementation in the target population over time (randomisation into screening and control popul.)Gradual expansion over regions Main aim to reduce colorectal cancer mortalityEvaluation (until effectiveness) of the programme built inTesting feasibility (practical issues, compliance, test results, colonoscopy process) within the public health care system in Finland
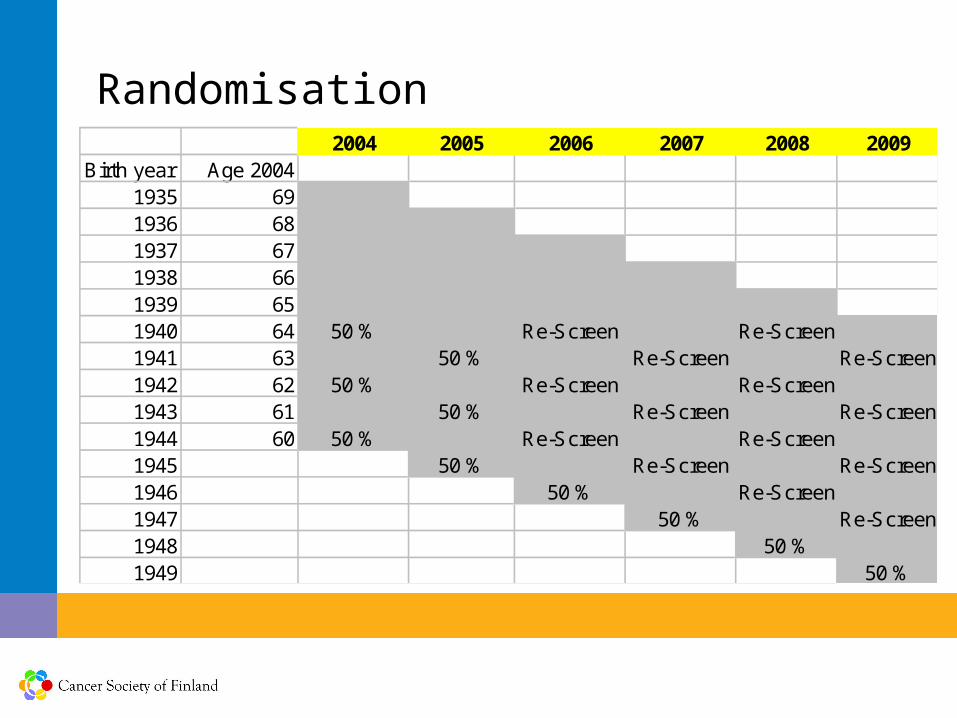
2004 2005 2006 2007 2008 2009Birth year Age 2004
1935 691936 681937 671938 661939 651940 64 50 % Re-Screen Re-Screen1941 63 50 % Re-Screen Re-Screen1942 62 50 % Re-Screen Re-Screen1943 61 50 % Re-Screen Re-Screen1944 60 50 % Re-Screen Re-Screen1945 50 % Re-Screen Re-Screen1946 50 % Re-Screen1947 50 % Re-Screen1948 50 %1949 50 %
Randomisation
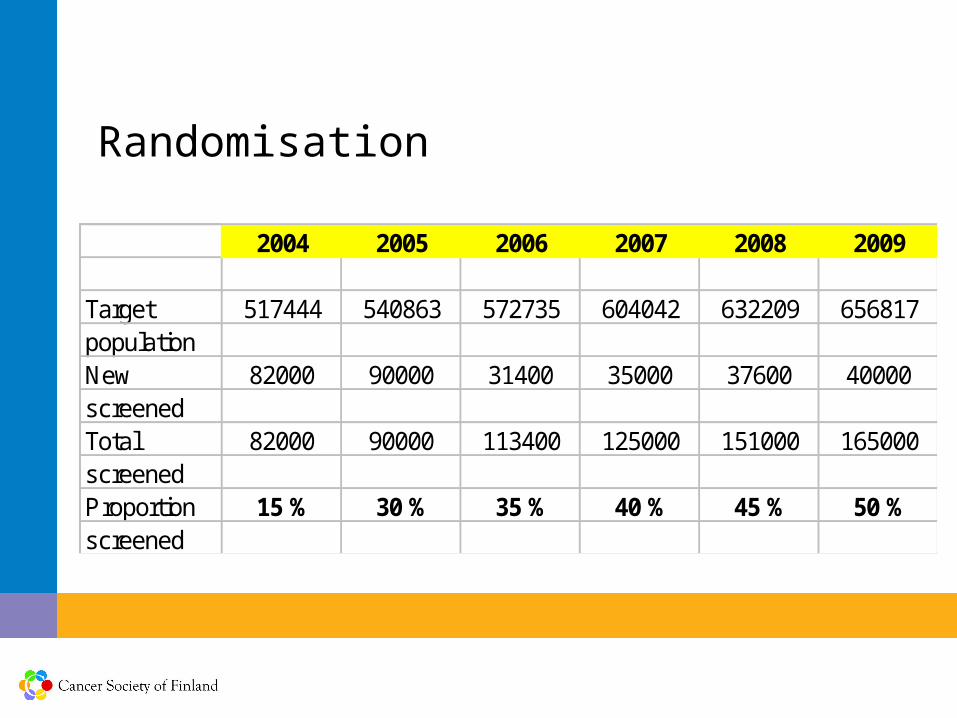
2004 2005 2006 2007 2008 2009
Target 517444 540863 572735 604042 632209 656817populationNew 82000 90000 31400 35000 37600 40000screenedTotal 82000 90000 113400 125000 151000 165000screenedProportion 15 % 30 % 35 % 40 % 45 % 50 %screened
Randomisation
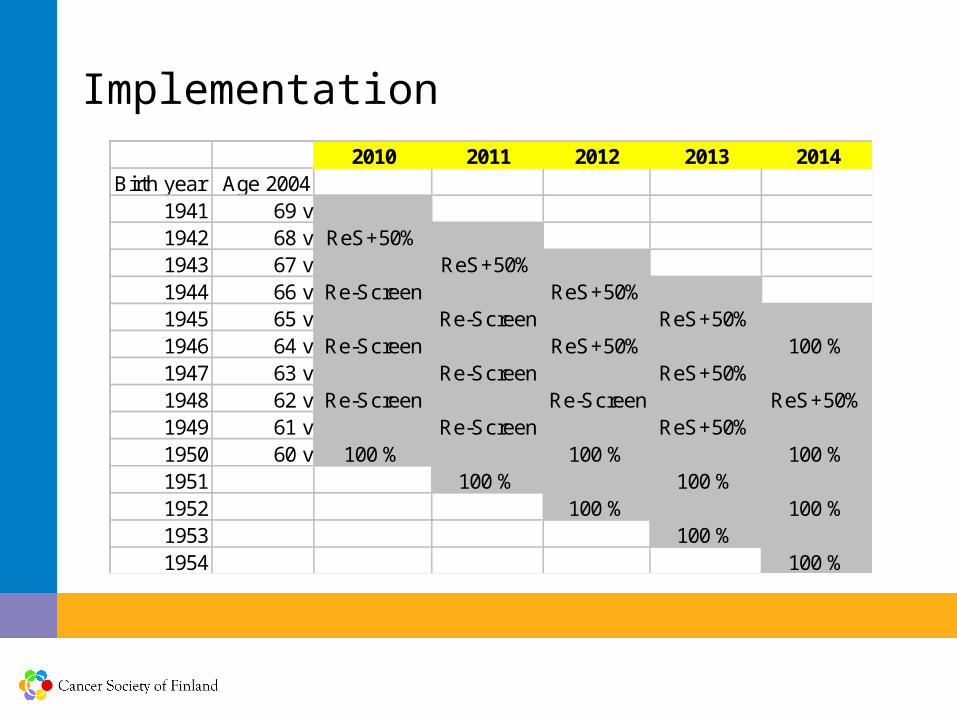
2010 2011 2012 2013 2014Birth year Age 2004
1941 69 v1942 68 v ReS+50%1943 67 v ReS+50%1944 66 v Re-Screen ReS+50%1945 65 v Re-Screen ReS+50%1946 64 v Re-Screen ReS+50% 100 %1947 63 v Re-Screen ReS+50%1948 62 v Re-Screen Re-Screen ReS+50%1949 61 v Re-Screen ReS+50%1950 60 v 100 % 100 % 100 %1951 100 % 100 %1952 100 % 100 %1953 100 %1954 100 %
Implementation
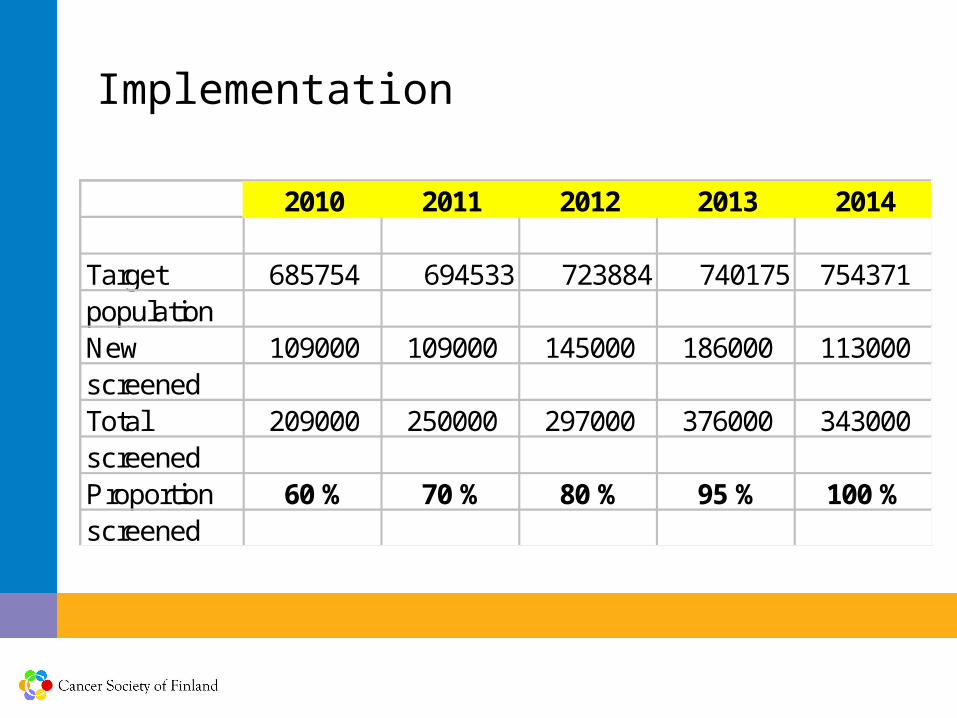
Implementation
2010 2011 2012 2013 2014
Target 685754 694533 723884 740175 754371populationNew 109000 109000 145000 186000 113000screenedTotal 209000 250000 297000 376000 343000screenedProportion 60 % 70 % 80 % 95 % 100 %screened
Why was this kind of programme designed?
Also any routine activity e.g. screening needs to be evaluated without bias
Evaluation should be done when the program is new and randomisation is still possible
Later if established as routin, it could be considered unethical not to offer screening to all, at this point resurces are not sufficient to screen everybody + we are not yet sure about the effect
Spontaneous screening (unorganised) cannot be evaluated and effectiveness cannot be determined
Costs less if organised (total cost + resource allocation)
An organised programme can be stopped if needed
Evaluation
The randomised design allows comparison between the screening and control arms
Cancers and deaths followed through national registries (statistics Finland, Finnish Cancer Registry)
Both screened and controls can be followed through register linkage with practically no loss to follow-up (personal id)
First years: performance, compliance, positivity rate, colonoscopy performance
After 10-15 years mortality will be compared between screened and controls
References
Malila N, Anttila A, Elovainio L, Hakulinen T, Jarvinen H, Paimela H, Pikkarainen P, Rautalahti M, and Hakama M: [Screening of colorectal cancer in Finland and analysis of its cost-effectiveness]. Duodecim 2003; 119: 1115-1123. In Finnish.Malila N, Anttila A, Hakama M: Colorectal cancer screening in Finland: details of the national screening programme implemented in Autumn 2004. J Med Screen 2005; 12:28-32.Malila, N., Oivanen, T., Rasmussen M. and Malminiemi, O.: Suolistosyövän väestöseulonnan käynnistyminen Suomessa. Suom. Lääkäril. 2006: 61: 1963-1967 (in Finnish).Malila, N., Oivanen, T. and Hakama, M.: Implementation of colorectal cancer screening in Finland: Experiences from the first three years of a public health programme. Z Gastroenterol 2007; 46 Suppl 1: S25-8.Malila N, Oivanen T, Malminiemi O, Hakama M. Test, episode, and program sensitivities of screening for colorectal cancer as a public health policy in Finland. BMJ 2008;337:a2261.